
Prescription Drug Utilization & Opioid Abuse July 16, 2013 Mona Chitre, PharmD, CGP Vice President,...
33
Prescription Drug Utilization & Opioid Abuse July 16, 2013 Mona Chitre, PharmD, CGP Vice President, Pharmacy Management Excellus BlueCross BlueShield
-
Upload
megan-miller -
Category
Documents
-
view
213 -
download
1
Transcript of Prescription Drug Utilization & Opioid Abuse July 16, 2013 Mona Chitre, PharmD, CGP Vice President,...
Prescription Drug Utilization & Opioid AbuseJuly 16, 2013
Mona Chitre, PharmD, CGPVice President, Pharmacy Management
Excellus BlueCross BlueShield

Pharmacy Management: Market Landscape
• Impact of Prescription Benefits
• Specialty Medications
• Price Increases
• Trend Management Opportunities
• Opioids

Service Bucket PMPM Allowed: Rx extracted from buckets and consolidated
Drug (Rx and Medical Benefits) $ 94.03
Physician $ 93.44
Outpatient $ 70.93
Inpatient $ 60.96
Why are Prescriptions important:
•#1 Benefit: Most commonly used benefit
• 67-70% use the drug benefit each year• 12-15 prescription fills per person per year
•#1 Cost: Drugs are the top cost driver
How does Rx affect benefit plans?
Medical Benefit• Hospital • Physician Office• Outpatient Facility• Clinics• Infusion centers • Home Infusion• DME
• Drug Costs: 5-8% of total medical cost ($20-$25 pmpm)
Pharmacy Benefit• Retail Pharmacy• Mail Pharmacy • Specialty Pharmacy
• Drug Cost : 20-25% of total health care cost ($75-$85 pmpm)

Prescription Benefit Medical Benefit
Cancer
Rheumatology
Psoriasis
Contraceptives
Multiple Sclerosis
Osteoarthritis
Asthma
Pulmonary Arterial
Hypertension
Diabetes
Antidepressants
Hypertension
Hyperlipidemia
PPIs
Glaucoma
Hemophilia
Vaccines
Immunoglobulins
Enzyme Replacement

Today’s pharmaceutical benefit reality
$20 – generic Rx
$2,200 – specialty Rx
$200 – brand Rx

7
SPECIALTY PHARMACEUTICALS
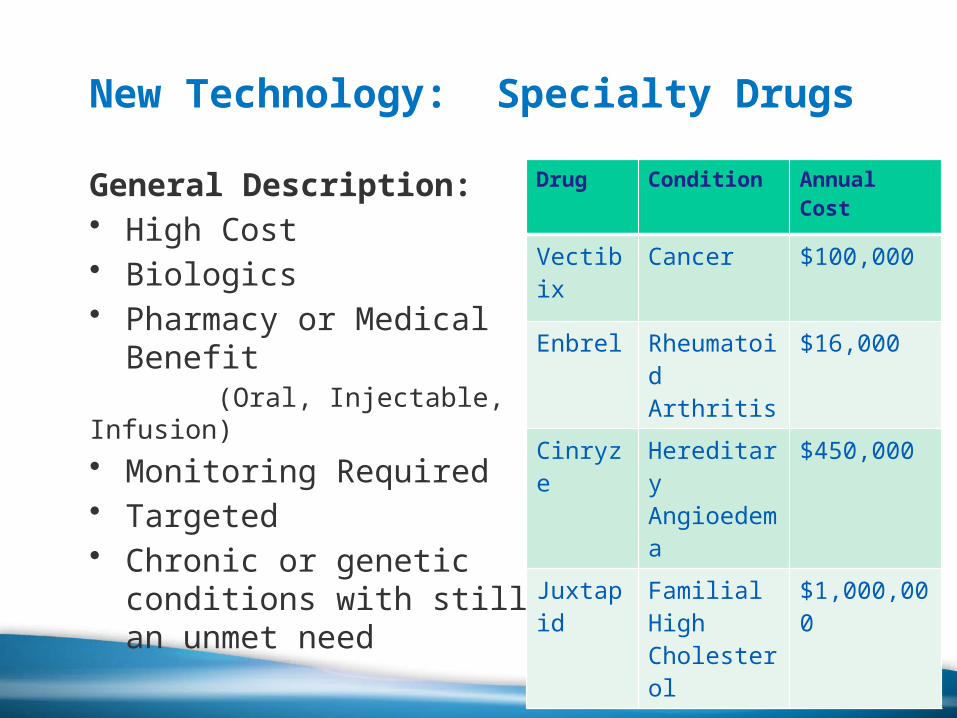
New Technology: Specialty Drugs
General Description: • High Cost • Biologics • Pharmacy or Medical
Benefit (Oral, Injectable, Infusion)• Monitoring Required• Targeted• Chronic or genetic
conditions with still an unmet need
Drug Condition Annual Cost
Vectibix
Cancer $100,000
Enbrel Rheumatoid Arthritis
$16,000
Cinryze Hereditary Angioedema
$450,000
Juxtapid
Familial High Cholesterol
$1,000,000
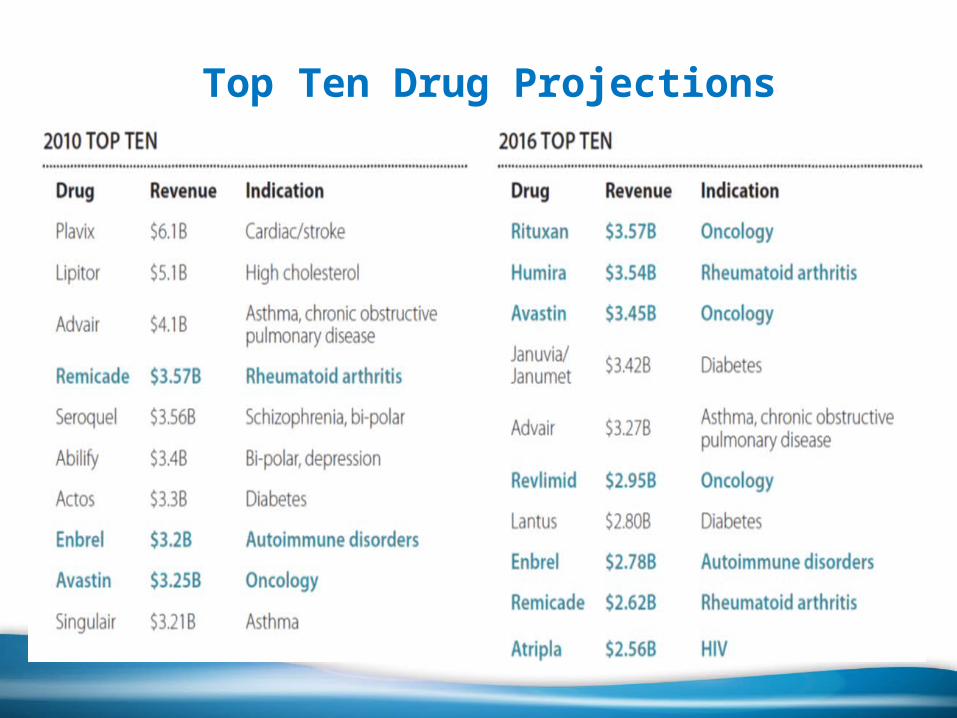
Top Ten Drug Projections
10
Specialty Drug: Employer Impact
Employer: 200 employees (450 total with coverage)• 5300 Prescriptions/ year • Average employer cost/Rx: $60• Total Annual Rx cost for employer: $320,000
Specialty Drug Impact: Tykerb • Oral drug used in combination for breast cancer.• Incremental Added Cost: $55,000/ year
15% increase in Rx expense that year

11
Specialty Drug: Employer Impact
Large multiple employer coalition: • 41,000 covered lives • Medical Drug PMPM: $14.47 (07-08)• Medical Drug Trend: 50% over 2 years• Specialty Drug Impact:
– 2 of the covered members treated with Fabrazyme – Annual cost of > $518,000
This drug accounted for 8% of the medical expense
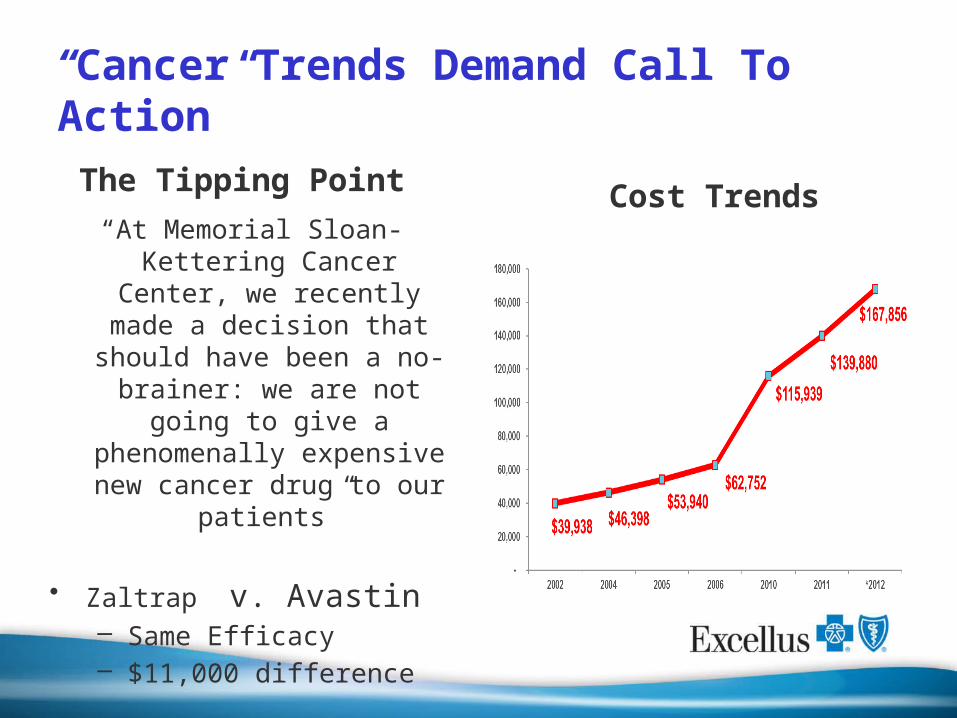
“Cancer Trends Demand Call To Action”
The Tipping Point
“At Memorial Sloan-Kettering Cancer Center, we recently
made a decision that should have been a no-
brainer: we are not going to give a phenomenally
expensive new cancer drug to our patients”
• Zaltrap v. Avastin – Same Efficacy – $11,000 difference
Cost Trends

DrugManufacture
rRout
eIndication Approval
Launch (est)
Annual Cost
Inlyta (axitnib)
Pfizer OralAdvanced renal cell carcinoma
1/27/2012 2/1/2012 $75,000/yr
Erivedge (vismodegib
)Genentech Oral Basal cell carcinoma 1/30/2012 2/7/2012 $75,000/yr
Kalydeco (ivacaftor)
Vertex Oral Cystic Fibrosis 1/31/2012 2/7/2012$294,000/
yrKorylm
(mifepristone)
Corcept Oral Cushings Disease 2/17/2012 5/1/2012$180,000/
yr
Elelyso (taligluceras
e alfa)Pfizer/Protalix IV Gaucher Disease 5/2/2012 5/3/2012
$180,000/yr
Perjeta (pertuzuma
b)Genentech IV
HER2-positive Breast CA
6/11/2012 6/25/2012 $71,000/yr
Juxtapid (pertuzuma
b)Aegerion Oral
Familial High Cholersterol
12/21/2012
2/1/2013 $1,000,000
Kadylca(traztuzuma
b emtansine)
Genentech IV HER2-positive Breast CA 2/22/2013 $94,000
2012/2013 Sample Specialty Rx Approvals

Pricing and Price Increases

15
Case Study: Multiple Sclerosis New Technology: 2010: 2 New agents - 1st Combination drug and 1st Oral Agent
Significant Price Increases: • 2006 Price - $ 15,000• 2010 Price - $37,000
Mean Ingredient Cost Copaxone Compared with CPI
$1,000
$1,200
$1,400
$1,600
$1,800
$2,000
$2,200
$2,400
$2,600
$2,800
$3,000
2004Q
1
2004Q
2
2004Q
3
2004Q
4
2005Q
1
2005Q
2
2005Q
3
2005Q
4
2006Q
1
2006Q
2
2006Q
3
2006Q
4
2007Q
1
2007Q
2
2007Q
3
2007Q
4
2008Q
1
2008Q
2
2008Q
3
2008Q
4
2009Q
1
2009Q
2
2009Q
3
2009Q
4
2010Q
1
2010Q
2
COPAXONE
Consumer Price Index
METRIC EHP 2 year Trend
COST 40%
USE 16%
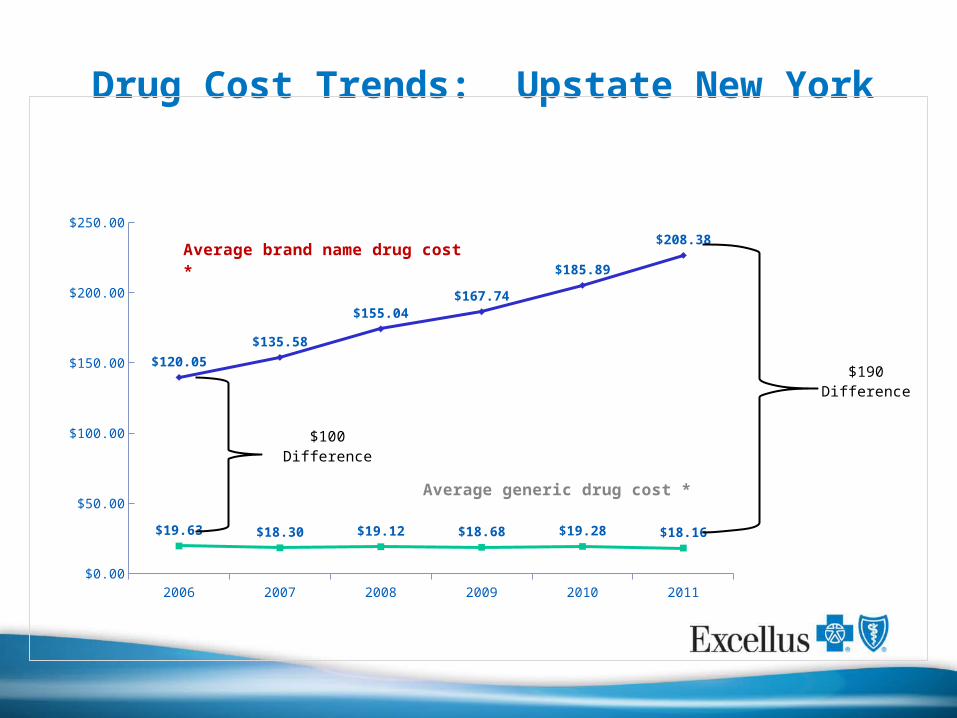
Drug Cost Trends: Upstate New York
2006 2007 2008 2009 2010 2011$0.00
$50.00
$100.00
$150.00
$200.00
$250.00
$19.63 $18.30 $19.12 $18.68 $19.28 $18.16
$120.05
$135.58
$155.04$167.74
$185.89
$208.38
$100 Difference
$190 Difference
Average brand name drug cost *
Average generic drug cost *

Trend Management: GENERICS
“Ask your doctor if a generic is right for you”
Each 1 point increase in GFR can reduce Rx spend by 2-3%
Employer Impact: Case Study
• Employer: 200 employees (450 total with coverage)• Avg 12 Rx/person/yr: approx. 5,300 Rx• Avg employer cost/Rx: $60• Generic Fill Rate: 65% (3,445 of the Rx are for generic)• Total Annual Rx cost for employer: $318,000
• Generic Opportunity: Increase GFR to 70%• 265 brand drug Rx changed to a generic option.• Cost saving per Rx: $100• Savings to employer: $26,500 (8% of spend)• Savings to employee: 200-$400+/year

201301 201302 201303 201304$0.00
$40.00
$80.00
$120.00
$160.00
Managed Managed Trend
Unmanaged Unmanaged Trend
To
tal
$ P
MP
M 20.5%
• Rx management programs: Generic Trial Program, Prior Authorization and Step Therapy encourage equally effective lower cost options to help manage trend and lower member out of pocket cost.
• Groups with unmanaged Rx are incurring significantly higher Per Member Per Month (PMPM) costs than groups with managed Rx benefits
Measure Managed Rx Unmanaged Rx
Generic Fill Rate 85.6% 74.2%
Brand PMPM $54.38 $102.09Brand PMPM Trend 0.4% 26.7%
Generic PMPM $24.42 $30.11
Generic PMPM Trend -9.2% 2.5%
Total PMPM $78.80 $132.20Total PMPM Trend -2.6% 20.5%Est Annual Spend $2,124,289 $3,237,091 Data based on claims incurred January – April 2013
Trend Management: Use Management
Opioid Impact

“Overdoses involving prescription painkillers are at epidemic levels and now kill more Americans than heroin and cocaine combined.
States, health insurers, health care providers and individuals have critical roles to play in the national effort to stop this epidemic of overdoses while we protect patients who need prescriptions to
control pain.”
CDC Director Thomas Friedan M.D., M.P.H.
Although evidence is limited, chronic opioid therapy (COT) can be an effective therapy for carefully selected and monitored patients
with chronic non-cancer pain (CNCP).
The American Pain Society and the American Academy of Pain Medicine expert panel
Balancing the need for opioids
21

Statistics• Overdose deaths involving opioid pain
relievers (OPR) have increased and now exceed deaths involving heroin and cocaine combined. OPR involved in 14,800 deaths in 2008
• More ED visits related to misuse or abuse of pharmaceuticals compared to use of illicit drugs
• By 2010, enough OPR were sold to medicate every American adult with a typical dose of 5 mg of hydrocodone every 4 hours for 1 month
• 17 percent of teens say they have used a prescription medicine at least once in their lifetime to get high or change their mood.
22
74%
26%
Prescription Drug Overdose Deaths,
2008
OPR Overdose Deaths
Other Rx Drugs
* Significantly lower than 2009 levels

Impact to Stakeholders in Healthcare
• 40 people die every day from overdoses involving opioids such as hydrocodone, oxycodone and oxymorphone
• The average annual cost per capita for opioid abusers has been calculated at $16,000 compared to $1,800 for non-abusers
• Nonmedical use of OPR costs insurance companies up to $72.5 billion annually in health-care costs
23
Wasted healthcare dollars

Excellus BlueCross Blue Shield Team
24
ClinicalPharmacy ManagementMedical DirectorBehavioral Health
Non-ClinicalSpecial Investigations UnitData AnalyticsCommunications

25
Integrated
Approach
Identification and
Stratification
Opioid Mailing
Suboxone® Initiative
Align Formulary

26
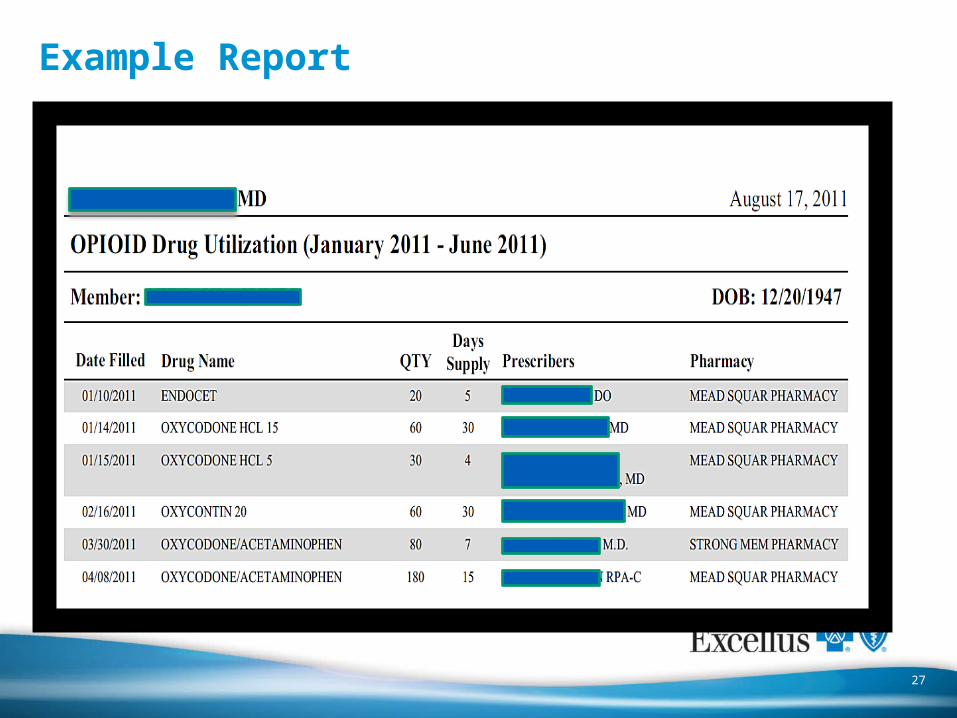
Prescribing Summary - Cover Letter
27
Example Report
Results of Opioid Mailing
28
Pharmacy Billing Errors
Fraudulent RXs by MD
staff
Stolen Prescriptio
n Pads
Negative Urine Drug
Screen
Suboxone® Provider testament

Provider survey
29
88%
12%
Was mailing helpful?
Yes
No
41%
59%
Did you take action?
Yes
No
Contacted other pre-
scriber
Contacted insurance company
Contacted patient listed
Contacted pharmacy
0%
5%
10%
15%
20%
25%
18.50%
1.50%
21.60%
9.10%
Action Taken
32.4%
61.3%
6.3%
What frequency of mailing is appropriate?
More frequently
Same
Less frequently
Based on 330 respondents

Step Three - Promoting Outpatient Detoxification• Suboxone® - Under the Drug Addiction Treatment Act (DATA), limited to
physicians who meet certain qualifying requirements (authorized training, addiction medicine specialty)
• Physician Engagement: – Upstate New York has a shortage of physicians who can prescribe Suboxone®
for opioid dependence
• Advantages of therapy:– Withdrawal symptoms can be managed safely and effectively in their home
environment that incorporates support from the family.– Significant MEDICAL cost savings. Medical costs associated with inpatient
detox can cost upwards of $1,200/day. Outpatient detox costs the health plan less than $300/day (excluding drug costs).
• Disadvantages of therapy:– High cost– Inappropriate use
30

Results
Decrease in inpatient detoxification by 10 percent over a two year time period (2009 – 2011)
Approximate 22% savings in Medical costs for the same time period
Significant increase in members utilizing Suboxone® therapy.
31
2009 2010 2011, est $-
$1,000,000
$2,000,000
$3,000,000
$2,194,857
$2,016,609
$1,718,065
Detox Medical Claims Expense

Last Thoughts
Insurers — the bad guys in so many policy debates — can do a lot of good, keeping better track of the
number and types of controlled substances policyholders are receiving.
The New Drug Crisis: Addiction by Prescription
Time Magazine
Monday, Sept. 13, 2010
32



















