Prescription Drug Abuse Steve Hanson Director, Bureau of Treatment NYS OASAS.
45
Prescription Drug Abuse Steve Hanson Director, Bureau of Treatment NYS OASAS
-
Upload
margery-reynolds -
Category
Documents
-
view
223 -
download
0
Transcript of Prescription Drug Abuse Steve Hanson Director, Bureau of Treatment NYS OASAS.

Prescription Drug Abuse
Steve HansonDirector, Bureau of Treatment
NYS OASAS

Why Prescription Drugs
• They work• They are fairly easily available• The culture of Prescription Drugs– Advertising– Patient Expectations– Pharmaceutical Company Promotion
• The Internet• The Mail

Basic Facts
• 48 million (age 12 and over) used Rx meds for non-medical purpose - 20% of U.S. population
• 2007 – 1.9 million ED visits related to Drug misuse/abuse (DAWN report)
• 31% - 582,000 – Rx drugs alone• 8% - 144,000 – Rx drug + illicit drugs• 10% - 189,000 – Rx + alcohol• 52% - 611,000 – involved Rx drugs

Non Medical Use of Rx ED VisitsPer 100,000 (2007)

ED Visits Non-Med use of Rx Drugs2004-2005
2004 2005 2006 20070
100,000
200,000
300,000
400,000
500,000
600,000
700,000

Past Month Illicit Drug Use among Persons Aged 12 or Older: 2009

Past Month Use of Selected Illicit Drugs among Persons Aged 12 or Older: 2002-2009

Past Month Use of Selected Illicit Drugs among Young Adults Aged 18 to 25: 2002-2009
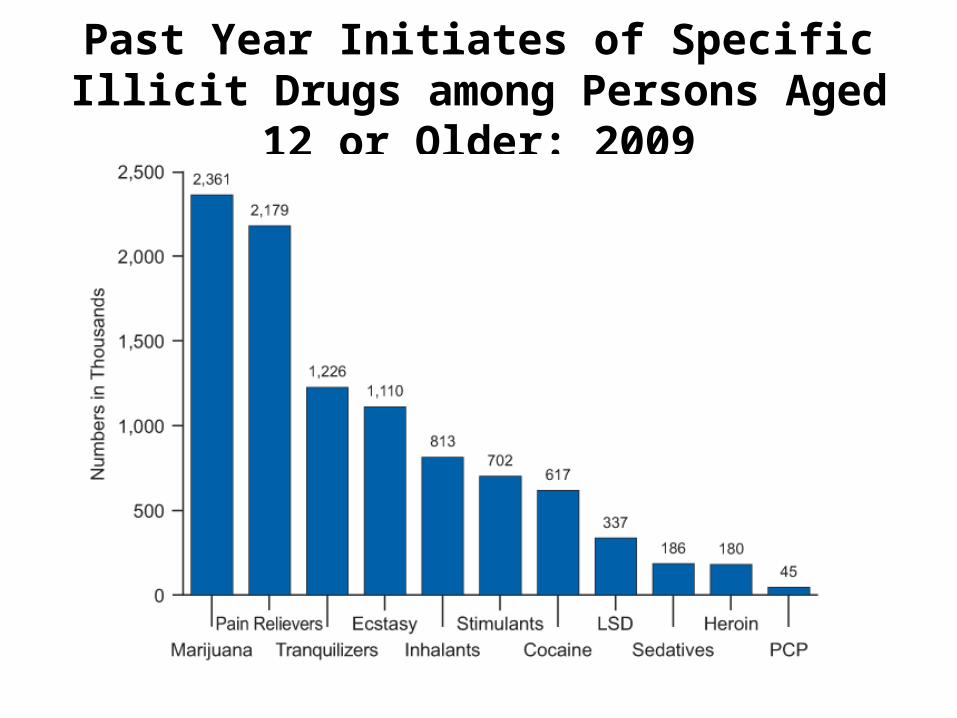
Past Year Initiates of Specific Illicit Drugs among Persons Aged 12 or Older: 2009

Past Month Nonmedical Use of Types of Psychotherapeutic Drugs among Persons Aged 12 or Older: 2002-2009

ED visits non-med use of Rx drugs

Source Where Psychotherapeutics Were Obtained for Most Recent Nonmedical Use among Past Year Users
Aged 12 or Older: 2005Percent of Past Year Users
0
20
40
60
80
100
Pain Relievers Tranquilizers Methamphetamine Stimulants
Other
Bought on Internet
Drug Dealer/ Stranger
1 or More Doctors
Bought/Took from Friend/ Relative
Free from Friend/Relative
8

Two “Types” of Rx Drug Abusers
• The Drug Abuser who likes Rx drugs.– Frequently use other
drugs (cocaine, alcohol, heroin, other non-Rx drugs)
– Fits the “model” of a drug abuser.
– “addicted” to high
• The Patient who becomes dependent on their medication– Infrequent use of other
substances – unless can’t get Rx.
– Don’t fit “model” of drug user – age, other behaviors.
– “dependent” on the drug

Addiction vs. Dependency
• Addiction – use the drug for the high, euphoria
• Dependent – use the drug to avoid withdrawal effects
• Can be both

Commonly Abused Rx Drugs
• Opiates/pain killers• Depressant/anti-anxieties• Stimulants

Nonmedical Use of Pain Relievers in Past Year among Persons Aged 12 or Older, by Substate Region: Percentages,
Annual Averages Based on 2004-2006
The Action ofOpiates

Natural Pain Suppression

Artificial Pain Suppression

Opiate Effects
• Analgesia - change in pain perception• Euphoria - whole body orgasm• Sedation - “on the nod”• Respiratory Depression - OD• Cough Suppression• Nausea/vomiting• Constipation

Tolerance
• Rapid tolerance with continued use• Cell sensitivity thought to be the tolerance
mechanism.• User now needs to find additional amounts• Multiple doctors• Asking friends/relatives
Addiction/Dependency
• Opioids trigger reward system – euphoria – leads to continued use – addiction
• Withdrawal symptoms are significant – regular use to avoid withdrawal - dependence
Withdrawal
• Pain• Depression• Alert• Rapid Breathing• Coughing• Nausea/Vomiting• Diarrhea• 3-5 days

Oxycontin
• Oxycodone – synthesized from thebaine (part of opium)
• Oxycontin – 1995– Crush the tablet for quicker high– Oral, snort, inject
• Percocet – oxycodone & acetominophen• Percodan – oxycodone & aspirin

Vicodin
• Hydrocodone and acetominophen• Lorcet, Lortab• Schedule III – high psychological/medium
physical• Pain and post-surgical use (pain)

Issues with Rx Opiate Dependence
• Presence of real pain• “I’m addicted to vicodin, not alcohol, why do I
have to quit that too?”• Drug Testing – make sure you test for drug of
choice as well as alternatives.

Anti-anxietals/Anxiolytics
• Panic Disorder• Phobias / social phobia• Obsessive Compulsive Disorder (OCD)• Post-Traumatic Stress Disorder (PTSD)• Generalized Anxiety Disorder• The neuroses – treated by Freud

Benzodiazepines
• Share a chemical structure• Librium – 1960• Valium - #1 Rx drug 1972-78, 3x #2• Xanax• Ativan• Very profitable

BenzodiazepinesVery Long Acting Short ActingHalazepam (Paxipam) Alprazolam (Xanax )Prazepam (Centrax ) Temazepam (Restoril ) Flurazepam (Dalmane ) Oxazepam (Serax )
Lorazepam (Ativan )
Intermediate Acting Very Short ActingClonazepam (Klonipin ) Triazolam (Halcion )Chlordiazepoxide (Librium )Diazepam (Valium )
Effects of BenzodiazepinesAnxiety control (e.g., panic attack)RelaxationDrowsiness & sleepControl seizuresReduced muscular coordinationDulled physical sensationsTolerance to effects develops

Benzodiazepines (cont.)
• Action – most increase GABA• Safe – Ld very high• Anticipation/placebo effect• Problems – work so well, people don’t want to
stop.• Side effects – dose related – cognitive
impairment, amnesia, slurred speech• Long Withdrawal

Drug Court/Treatment Issues
• People with true anxiety disorder• Anxiety can be a major relapse trigger• Stressful situations in early recovery• Strong craving for relief• To medicate or not to medicate…

Why Prescription Drug Users May Believe That They Are “Different”
• “I had/have real pain, I wasn’t using these to get high like those drug addicts”
• “My doctor prescribed these for me. It wasn’t my idea”
• “I never robbed anyone or did those things that addicts do.”
• “I have to take something for this pain!”

What the Rx Drug User Might Have Trouble Relating To
• “Hitting Bottom”• Changing People, Places & Things• Change your “Lifestyle”• You must be completely abstinent from
everything else – alcohol included• Going to meetings all of the time.

Drug Court/Treatment Issues
• Urine testing – ensuring that the panel used includes the drugs that the participants take
• Medication needs – people suffering from a medical/psychiatric condition that needs to be medicated – which medications are “okay”
• Withdrawal risks

COMMUNITY SUPERVISION
• Difficult population to supervise
• Unique strategies of supervison
• Training needs of the supervision officer.

Supervision
• Must be unrelenting in the monitoring of prescription drug use
• All prescriptions must be reported• Must work with physician to determine need
for medication.• Connect with addictionologist to monitor
withdrawal, medication assisted treatment, and on-going pain treatment.

Letter for Physician• To Medical Treatment Provider/Doctor:• Your patient, ___________________________ is a participant in the Drug Court Program, a
court ordered substance abuse treatment program. He/She has been assigned to this program due to ongoing and significant substance dependence.
• Your patient has provided documentation indicating that you have prescribed medication with addictive properties as part of his/her treatment. Please verify your knowledge and approval of this patient’s prescribed medication and that you feel the current course of treatment is necessary and no other alternative form of treatment exists.
• To ensure that this is a valid prescription and you have received this letter, the participant must return this letter with the information below completed.
• Physicians Name_________________________________ (Please print and/or type)• Address ___________________________________• Phone Number___________________________________• DEA# _________________________________________• Signature_______________________________________• Sincerely,

Supervision
• Monitoring prescription pills. • Random searches of person and property.• Monitor DEA database to determine multiple
prescriptions.• Obtain release of information from each
physician to facilitate communication between Dr. and team.
Supervision
• On-going communication between supervision officer and treatment
• Monitoring of drug use through random, frequent drug testing
• Not only testing for illegal drug use, but for MAT drugs.

Skills for Supervision Officer
• Must understand the disease model of addiction.
• Be aware of relapse signs and/or triggers.• Motivational Interviewing- to engage clients
buy in, by developing discrepancies and gauging client’s readiness to change.

Skills of Supervision Officer
• Clear communication with treatment provider.• Provide immediate sanction/incentive for
each drug test.
Opiate Addicts in Drug Court
• Decision must be made by entire team that the person will be allowed in the program.
• Understanding that some clients will be on pain medication for the rest of their lives, and our job is to monitor that client is taking medicine as prescribed.

Opiate Addicts in Drug Court
• This population is a growing threat to the safety of our community. The availability of prescription drugs and the on-going abuse must be addressed.
• Drug Courts are here to change the lives of addicts, while offering protection to the community through accountability and on-going collaboration of the courts and treatment.

• While the opioid client is difficult to monitor, choosing to not deal with them is not the answer.
• Drug Courts must continue to develop methods to monitor these clients and not allow them to go unsupervised just because they are hard to monitor.