
Prescribing information is available at this meeting 1 MODULE 2 IDENTIFICATION, SCREENING AND...
17
Prescribing information is available at this meeting 1 MODULE 2 IDENTIFICATION, SCREENING AND DIAGNOSIS DET 808
-
Upload
frederick-mcdaniel -
Category
Documents
-
view
215 -
download
0
Transcript of Prescribing information is available at this meeting 1 MODULE 2 IDENTIFICATION, SCREENING AND...
Prescribing information is available at this meeting1
MODULE 2
IDENTIFICATION, SCREENINGAND DIAGNOSIS
DET 808

Prescribing information is available at this meeting
• Patients do not initiate discussions since they may not see OAB as a legitimate condition or may not understand the terminology
• Patients are often too embarrassed to talk about their symptoms
• Patients learn to accept and cope with their symptoms
– Avoiding social interaction– Mapping toilet locations– Carrying spare clothing
17. Abrams P, et al. Am J Manag Care. 2000;6(suppl):S580-S590.
CHALLENGES TO IDENTIFICATION OF OAB
2

Prescribing information is available at this meeting
• Do you go to the toilet more than 8 times a day?
• Do you often wake up during the night needing to go to the toilet?
• Do you have to hurry to make the toilet in time?
• Do you often not reach the toilet in time?
ASKING THE RIGHT QUESTIONS
3
Prescribing information is available at this meeting
• New patient medical questionnaires
• New patient medical examinations
• Routine cervical smears
• Routine checkups for patients over 40 years old
• Family planning/menopause clinics
• Patient leaflets/posters
• Health visitors/district nurses/practice nurses
• Nursing homes
OPPORTUNITIES FOR SCREENING
4
Prescribing information is available at this meeting
SCREENING IS AN IMPORTANT TOOL
• Reasons for screening
– High prevalence
– Impact on patients’ lives
– Cost to society
– Government initiatives/guidelines such as:
• Good Practice in Continence Services in the UK23
23. Donaldson L, Mullally S. London, England: Department of Health;April 19, 2000.
5

Prescribing information is available at this meeting
• Validated in 1260 patients24
• 8 simple, self-administered questions
• Simple scoring by addition
• Available and linguistically validated in 12 languages25
A NEW SCREENING TOOL – THE OVERACTIVE BLADDER – VALIDATED 8-QUESTION QUESTIONNAIRE
6
24. Coyne K, Matza L ICS 2004.25. Conway K, Uzun V, Vigner S et al. ICS 2004.
Prescribing information is available at this meeting
How bothered have you been by…
• Frequent urination during the day?
• Uncomfortable urge to urinate?
• Sudden urge to urinate with little or no warning?
• Accidental leakage of small amounts of urine?
• Night-time urination?
• Waking up at night because of the need to urinate?
• Uncontrollable urge to urinate?
• Urine leakage associated with a strong desire to urinate?
SCREENING WITH THE OVERACTIVE BLADDER QUESTIONNAIRE
7 14. Coyne K, et al. Qual Life Res. 2002;11:563-574.
Prescribing information is available at this meeting
• Patients complete the screening questions
• Doctor reviews the patient-completed screener
• Doctor makes diagnosis and treats appropriately
HOW TO USE THE OVERACTIVE BLADDER QUESTIONNAIRE
8
Prescribing information is available at this meeting
COMMUNICATION IS THE KEY
• Active listening
• Use of language
• Use of body language
• Questioning techniques
9

Prescribing information is available at this meeting
DIAGNOSIS OF OAB
10
Prescribing information is available at this meeting
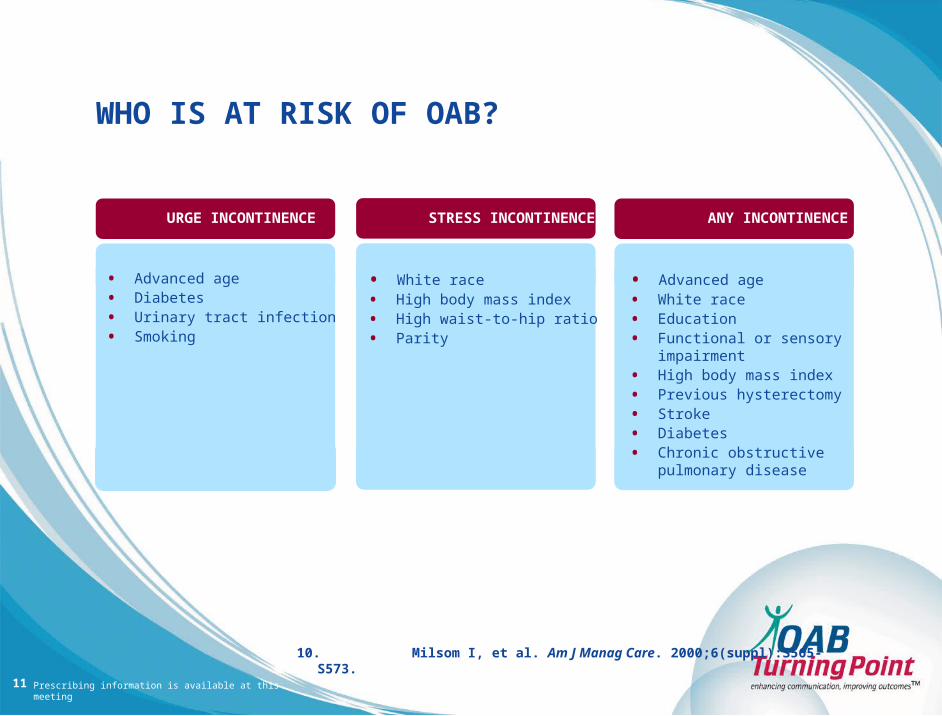
WHO IS AT RISK OF OAB?
10. Milsom I, et al. Am J Manag Care. 2000;6(suppl):S565-S573.11
URGE INCONTINENCE STRESS INCONTINENCE ANY INCONTINENCE
• Advanced age
• Diabetes
• Urinary tract infection
• Smoking
• White race
• High body mass index
• High waist-to-hip ratio
• Parity
• Advanced age
• White race
• Education
• Functional or sensory impairment
• High body mass index
• Previous hysterectomy
• Stroke
• Diabetes
• Chronic obstructive pulmonary disease

Prescribing information is available at this meeting
OTHER CONDITIONS/MEDICATIONS WHICHHAVE AN IMPACT ON SYMPTOMS OF OAB
12
22. Thuroff J. EUR Urol. 2003;2 (Suppl):10-15.26. ASCP website.
http://www.ascp.com/pubs/tcp/1999/special/diagnosing.shtml
COEXISTING CONDITIONS DRUGS ASSOCIATED WITH INCONTINENCE
• Chronic constipation26
• Urinary tract infection26
• Delirium26
• Depression22
• Skin infection22
• Sleep deprivation22
• Diuretics26
• Antidepressants26
• Antihypertensives26
• Sedatives, hypnotics and nacotics26
• Muscle relaxants26
Prescribing information is available at this meeting
• To confirm diagnosis of OAB
– Patient history12
– Overactive Bladder Questionnaire24
– Physical examination12
– Urinalysis12
DIAGNOSIS OF OAB BASED ON SYMPTOMS
1312. Wein AJ, Royner ES. Int J Fertil. 1999;44:56-66.24. Coyne K, Matza L. ICS 2004.
Prescribing information is available at this meeting
• Patient history
– Form a working diagnosis– Assess the impact of symptoms on QoL– Review body systems (neurologic, metabolic)– Identify coexisting conditions and treatments that can cause
incontinence
12. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66.
DIAGNOSIS OF OAB
• Physical examination
– Abdominal– Neurological– Pelvic (women)– Genital/prostate (men)
14

Prescribing information is available at this meeting
• Urinalysis
– Infection
– Tumour
– Haematuria
– Glucosuria
– Proteinuria
12. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66.
DIAGNOSIS OF OAB (CONTINUED)
• Postvoid residual volume (PVR)
– Elderly with voiding symptoms and/or recurrent UTI
– Neurological disease and voiding dysfunction
– Symptoms of poor bladder emptying
15
Prescribing information is available at this meeting
12. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66.
DIFFERENTIAL DIAGNOSIS:OAB AND STRESS INCONTINENCE
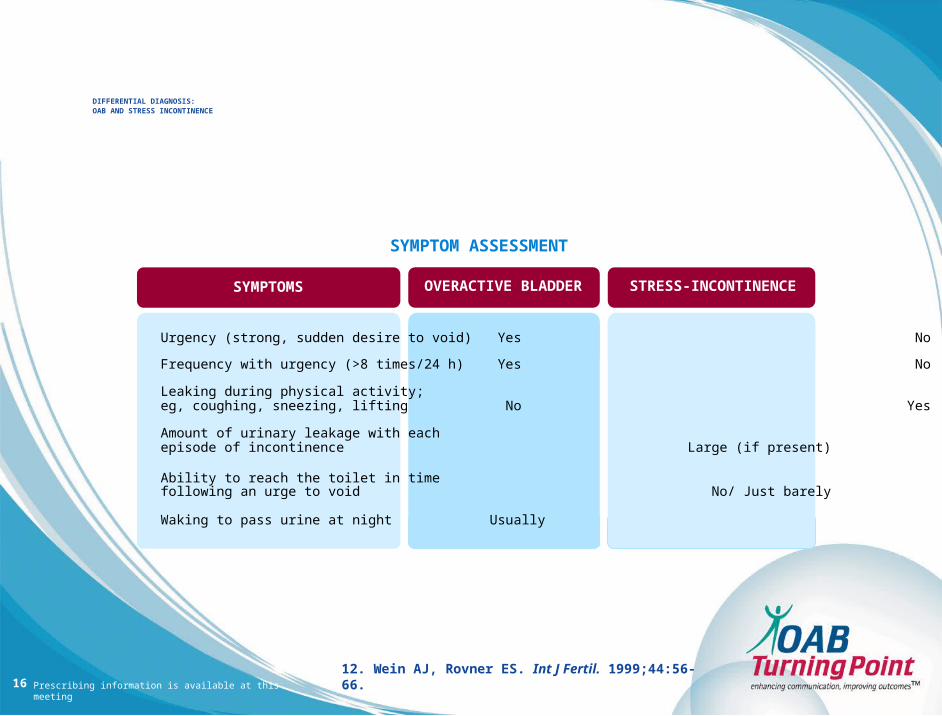
Urgency (strong, sudden desire to void) Yes No
Frequency with urgency (>8 times/24 h) Yes No
Leaking during physical activity; eg, coughing, sneezing, lifting No Yes
Amount of urinary leakage with each episode of incontinence Large (if present) Small
Ability to reach the toilet in time following an urge to void No/ Just barely Yes
Waking to pass urine at night Usually Seldom
SYMPTOMS STRESS-INCONTINENCEOVERACTIVE BLADDER
SYMPTOM ASSESSMENT
16
Prescribing information is available at this meeting
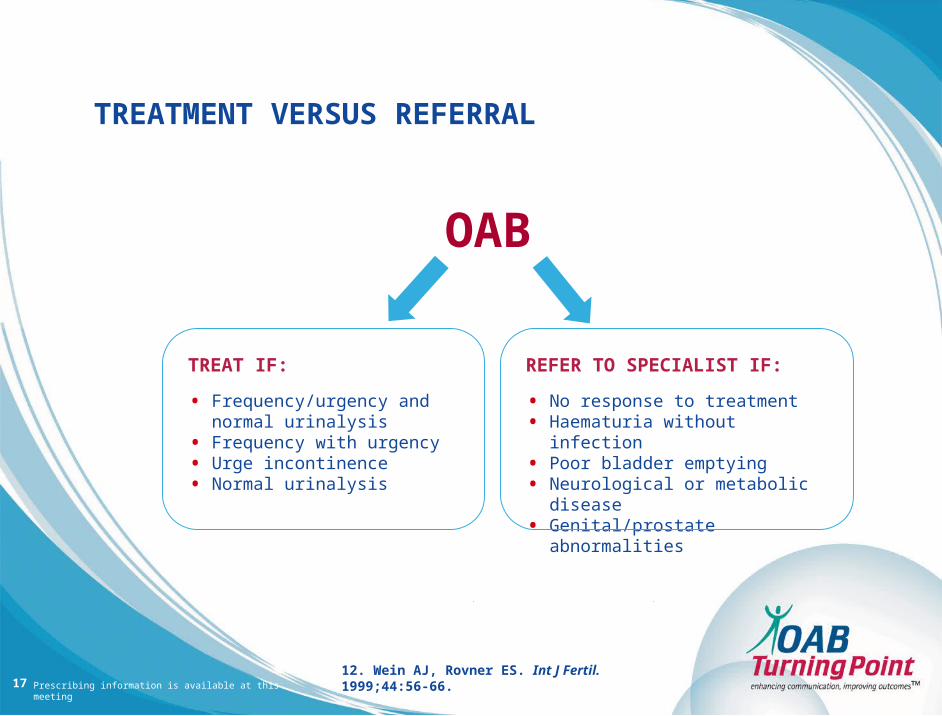
TREAT IF:
• Frequency/urgency and normal urinalysis
• Frequency with urgency• Urge incontinence• Normal urinalysis
REFER TO SPECIALIST IF:
• No response to treatment• Haematuria without infection• Poor bladder emptying• Neurological or metabolic disease• Genital/prostate abnormalities
OAB
12. Wein AJ, Rovner ES. Int J Fertil. 1999;44:56-66.
TREATMENT VERSUS REFERRAL
17


















