Prepared by J. Mabbutt & C. Maynard NaMO September 2008 8.2: Managing Benzodiazepine, Cannabis,...
35
Prepared by J. Mabbutt & C. Maynard NaMO September 2008 8.2: Managing Benzodiazepine, Cannabis, Nicotine and other Withdrawal
-
Upload
robyn-fitzgerald -
Category
Documents
-
view
215 -
download
0
Transcript of Prepared by J. Mabbutt & C. Maynard NaMO September 2008 8.2: Managing Benzodiazepine, Cannabis,...

Prepared by J. Mabbutt & C. MaynardNaMO
September 2008
8.2: Managing Benzodiazepine, Cannabis, Nicotine and other Withdrawal

1. During the session nurses & midwives will learn how to identify, assess & manage a patient in benzodiazepine, cannabis, nicotine & other drug withdrawal
2. At the end the session, nurses will have a basic understanding & knowledge to safely & effectively identify, monitor & manage benzodiazepine, cannabis, nicotine & other drug withdrawal
8.2: Managing other drug withdrawal: Objectives

This presentation gives general guidelines for managing withdrawal. Refer to Section 9 for specific details of withdrawal symptoms and management for the most commonly used substances
For further information, refer to the New South Wales Drug and Alcohol Withdrawal Clinical Practice Guidelines (2007) http://www.health.nsw.gov.au/policies/gl/2008/GL2008_011.html
8.2: Managing drug withdrawal

Present the post natal case study for benzodiazepine and other drug withdrawal from Guidelines CD Rom Section 01
Discuss each section in small groups or as a large group and feedback
8:2 Indications and guidelinesBenzodiazepine Withdrawal – Option – Case Study

Onset of withdrawal depends on the half-life of the particular benzodiazepine used by the person
Withdrawal from short-acting benzodiazepines generally occurs earlier & is more severe
Withdrawal symptoms do not necessarily decrease steadily from a peak, but can follow a fluctuating course with good & bad periods
Eventually the good periods will last longer & become more frequent
8:2 Indications and guidelines – Benzodiazepine withdrawal – Onset & duration of benzodiazepine withdrawal

* Based on manufacturer’s product information. †Elimination half-life: time for the plasma drug concentration to decrease by 50%. ‡ Equivalent dose: approximate dose equivalent to diazepam 5 mg.
Generic name Trade name Time to peak concentration
Elimination half life † Equivalent dose ‡
Diazepam AntenexDuceneValiumValpam
30-90 min Biphasic: rapid phase half-life, 3 hours; elimination half-life, 20-48 hours
5 mg
Alprazolam AlpraxXanaxKalma
1 hour 6-25 hours 0.5-1.0 mg
Bromazepam Lexotan 0.5-4 hours 20 hours 3-6 mg
Clobazam Frisium 1-4 hours 17-49 hours 10 mg
Clonazepam PaxamRivotril
2-3 hours 22-54 hours 0.5 mg
Flunitrazepam Hypnodorm 1-2 hours 20-30 hours 1-2 mg
Table 9.9: Absorption rates, half-life, & equivalent daily doses of common benzodiazepines**

* Based on manufacturer’s product information. †Elimination half-life: time for the plasma drug concentration to decrease by 50%. ‡Equivalent dose: approximate dose equivalent to diazepam 5 mg.
Generic name Trade name Time to peak concentration
Elimination half life † Equivalent dose ‡
Lorazepam Ativan 2 hours 12–16 hours 1 mg
Nitrazepam AlodormMogadon
2 hours 16–48 hours 2.5–5 mg
Oxazepam AlepamMurelaxSerepax
2–3 hours 4–15 hours 15–30 mg
Temazepam EuhypnosNormisonTemazeTemtabs
30–60 min after tablets, 2 hours after capsules
5–15 hours 10–20 mg
Triazolam Halcion 1–3 hours Biphasic: rapid phase half-life, 2.5–3.5 hours; elimination half-life, 6–9 hours
0.25 mg
Zolpidem Stilnox 0.5–3 hours 2.5 hours Not known
Table 9.9: Absorption rates, half-life, & equivalent daily doses of common benzodiazepines**

Subjective symptoms with few observable signs of withdrawal are a feature, particularly of low dose withdrawal
Individuals may report feeling extremely mentally distressed (as though they are “going mad”), although they may not have any obvious signs of physical discomfort
This may result in the person not receiving the care that would be appropriate during this time
8:2 Indications and guidelines – Benzodiazepine withdrawal – Signs & symptoms of benzodiazepines withdrawal

NSW Health (2007)
Common symptoms Less common symptoms Uncommon symptoms
Anxiety Nightmares, agoraphobia Delusions
Insomnia Feelings of unreality Paranoia
Restlessness Depersonalisation Hallucinations
Agitation Panic attacks Seizures
Irritability Nausea, dry retching, decreased
Persistent tinnitus
Poor concentration Increased sensory perception, Confusion
Poor memory Increased temperature, ataxia
Depression Gastrointestinal unrest
Muscle tension, aches and twitching
Menstrual changes
Table 9.10: Symptoms of benzodiazepine withdrawal

The major complications of withdrawal are:
Progression to severe withdrawal
Delirium with risk of injury (to self or others)
Risk of dehydration or electrolyte imbalance
Potential for seizures
Presence of concurrent illness, which masks or mimics withdrawal
Orthostatic hypotension
8:2 Indications and guidelines – Benzodiazepine withdrawal – Major complications of withdrawal
Withdrawal from short-acting benzodiazepines (e.g. oxazepam, temazepam, alprazolam, & lorazepam) typically produces a faster and more severe onset of symptoms
Withdrawal from long-acting benzodiazepines (e.g. diazepam, nitrazepam) may be more difficult to undergo and complete
8:2 Indications and guidelines – Benzodiazepine withdrawal – Course of withdrawal

Adapted from Frank L, Pead J. New concepts in drug withdrawal: a resource handbook© 1995 State of Victoria. Reproduced with permission.
Figure 9.3: Withdrawal from short and long-acting benzodiazepines

Undertake nursing observations to identify & manage withdrawal symptoms & prevent the progression to severe withdrawal
In particular, offer:
Reassurance regarding distorted sensory stimuli
Heat & massage for muscle aches
Symptomatic management to reduce the severity of symptoms
8:2 Indications and guidelines Managing benzodiazepine withdrawal
There is no validated tool for recording benzodiazepine withdrawal symptoms in an inpatient setting
The symptoms previously listed in Table 9.10 need to be monitored
8:2 Indications and guidelines – Managing benzodiazepine withdrawal – Monitoring

Initial stabilisation of dose (preferably with a long-acting benzodiazepine) – a gradual dose reduction preferably as an outpatient
In hospital: patients taking high doses, or polydrug users, should be stabilised on a long-acting benzodiazepine (preferably, diazepam), at a dose about 40% of their regular intake prior to admission (or 80 mg/day, whichever is lower)
Reduction & withdrawal should follow once their other medical condition has been dealt with
From the New South Wales Drug and Alcohol Withdrawal Clinical Practice Guidelines (2007)
8:2 Indications and guidelines – Managing benzodiazepine withdrawal – Pharmacological treatment (1)

Referral to Drug & Alcohol outpatient services or supportive GPs needs to be arranged well in advance of discharge to organise a continued outpatient reduction regime
Please contact a specialist Drug & Alcohol medical officer/nurse practitioner/ senior clinical nurse for advice & support
If patients stabilise on a dose in the range 40–80 mg of diazepam daily, withdrawal should be at the rate of at least 5 mg per week until the dose reaches 40 mg, then 2.5 mg/week
A maximal rate of withdrawal would be to reduce the dose by 10 mg at weekly intervals until 40 mg, then by 5mg at weekly intervals this will take 12 weeks as an outpatient
New South Wales Drug and Alcohol Withdrawal Clinical Practice Guidelines (2007)
8:2 Indications and guidelines – Managing benzodiazepine withdrawal – Pharmacological treatment (2)
Most symptoms commence on day 1, peaking at day 2-3, returning to baseline after a week or two
Can be an onset of aggression (day 4) often peaking after 2 weeks of abstinence and anger (day 6) also being particularly significant
There is a National Cannabis Prevention and Information Centre (NCPIC) with has a range of resources and information regarding cannabis withdrawal, for the workforce, users & families, http://ncpic.org.au/ – 1800 30 40 50
8:2 Indications and guidelines – Managing cannabis withdrawal – Onset & duration of cannabis withdrawal (1)

Special considerations include:
Patients with a comorbid mental health condition as there may be unmasking of the mental illness during withdrawal
Appropriate assessment & management is required
Patients who use cannabis for chronic pain may require assessment for adequate pain management & referral to specialist pain services
Patients with a history of aggression may require closer monitoring and a higher dose of benzodiazepine
8:2 Indications and guidelines – Managing cannabis withdrawal – Onset & duration of cannabis withdrawal (2)

Common symptoms Less common symptoms/equivocal symptoms
Anger or aggression Chills
Decreased appetite or weight loss Depressed mood
Irritability Stomach pain
Nervousness/anxiety Shakiness
Restlessness Sweating
Sleep difficulties, including strange dreams
Table 9.13 Cannabis withdrawal symptoms (Budney et al., 2004:1975)

Cannabis withdrawal can be monitored by using a withdrawal assessment scale such as the Cannabis Withdrawal Assessment Scale (see Appendix 5)
Not all patients will require medication for withdrawal
The following table lists medications for symptomatic relief of cannabis withdrawal
8:2 Indications and guidelines – Managing cannabis withdrawal –Monitoring
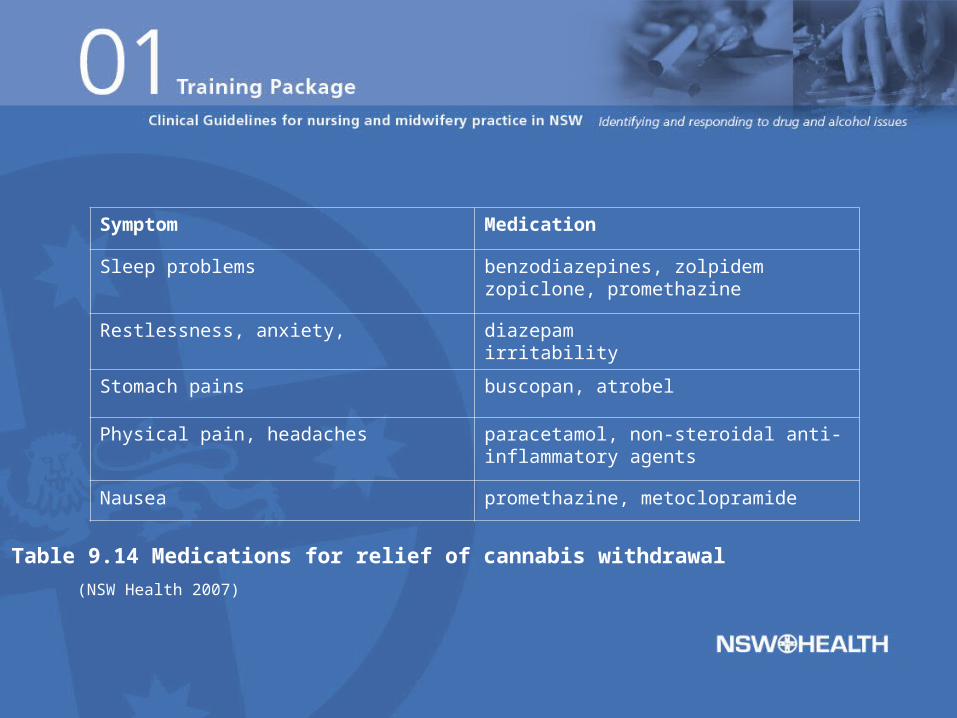
(NSW Health 2007)
Symptom Medication
Sleep problems benzodiazepines, zolpidem zopiclone, promethazine
Restlessness, anxiety, diazepamirritability
Stomach pains buscopan, atrobel
Physical pain, headaches paracetamol, non-steroidal anti-inflammatory agents
Nausea promethazine, metoclopramide
Table 9.14 Medications for relief of cannabis withdrawal

Given the wide interpersonal variability, dosages and prescribing schedules will most effectively be decided upon only after a thorough exploration of the individual patient’s symptom profile and circumstances.
Outpatient regimens might be:
7 days of diazepam 5 mg four times daily, zopiclone 7.5 mg at night, NSAIDs / buscopan as needed, or
7 days of zolpidem 7.5 mg at night
From the New South Wales Drug and Alcohol Withdrawal Clinical Practice Guidelines (2007)
8:2 Indications and guidelines – Managing cannabis withdrawal –Pharmacological Treatment

Onset of withdrawal is usually within a few hours of the last cigarette & withdrawal symptoms peak at 24-72 hours
Withdrawal symptoms vary, but can include the following:
Irritability
Cravings
Increased nervousness and tension
Sleep disturbance
Stomach upsets
8:2 Indications and GuidelinesNicotine withdrawal signs & symptoms (1)

Bowel disturbance
Loss of concentration
Muscle spasm
Changes in taste
Headaches
Cough
Increased appetite
8:2 Indications and GuidelinesNicotine withdrawal signs & symptoms (2)

There is generally no indication for admission into a Drug & Alcohol inpatient facility but may be admitted into hospital & experience withdrawal from nicotine consequently
Patients should be informed of the NSW Health Smoke Free Workplace Policy (1999) & offered support to stop
NRT should be used when not contraindicated
Refer to NSW Health Guidelines GL2005_036: Nicotine Dependent Inpatients http://www.health.nsw.gov.au/policies/GL/2005/pdf/GL2005_036.pdf
8:2 Pharmacological treatment Treatment: Indication for in patient nicotine withdrawal

A holistic approach to smoking cessation is important and a pharmacotherapy should be seen as one part of this approach
Pharmacotherapy options are:
Nicotine Replacement Therapy (NRT)
Bupropion
Other options such as clonidine, & nortriptyline
8:2 Nicotine withdrawal Pharmacological treatment –Pharmacotherapiesc

Type Dose and Duration Side Effects Contraindications
Less than 10 cigs per day
10-20 cigsper day
More than20 cigsper day
Patches None Nicobate®14 mgNicorette®10 mg
Nicobate®21 mgNicorette®15 mg
Transient skin irritation, itching, dreams, sleep disturbance, indigestion,diarrhoea
Relative:• Ischaemicheart diseaseAbsolute:• Recent MI• Seriousarrhythmias• Unstableangina• Pregnancy
Gum None 2 mg, 8-12per day
4 mg, 8-12per day
Jaw discomfort,nausea, indigestion,hiccups, excess saliva, sore throat
Inhaler None Nicorette®6-12cartridgesper day
Not recommended Mouth and throatirritation, cough,nausea andindigestion
Table 9.16 Pharmacotherapy of nicotine replacement therapies

Type Dose and Duration Side Effects Contraindications
Less than 10 cigs per day
10–20 cigs per day
More than 20 cigs per day
Bupropion 150 mg for 3 days, then 150 mg b.d. for 7 weeks
Headaches, dry mouth, impaired sleep, seizures, nausea, anxiety, constipation and dizziness
1. seizure disorders or significant risk of seizure2. bulimia3. anorexia nervosa 4. bipolar disorders
From New South Wales Drug and Alcohol Withdrawal Clinical Practice Guidelines (2007)
Table 9.17 Pharmacotherapy of bupropion (Zyban®)

These drugs are not usually associated with dependence arising from long term, high-level use
There is no evidence of a withdrawal syndrome from hallucinogens even after abrupt cessation or substantial reduction in their use
8:2 HallucinogenDependence and withdrawal

Withdrawal syndrome can occur in some cases, but it is generally mild
Symptoms include:
Anxiety
Depression
Headache
Nausea
Dizziness
8:2 SolventsWithdrawal (1)

Drowsiness
Chills
Abdominal pains
Muscular cramps
Sometimes, confusion & hallucinations can occur after chronic solvent use
8:2 SolventsWithdrawal (2)
Abrupt withdrawal can occur after cessation of long-term daily use (White et al 2002)
There is no validated tool for recording ketamine withdrawal symptoms
Symptoms of withdrawal are:
Fear
Tremors; facial twitches
Craving
Animal studies show seizures, irritability & weight loss during ketamine withdrawal
8:2 Indications and guidelines –Ketamine withdrawal

GHB use should be suspected in particular groups such as clubbers & body builders who present with signs compatible with alcohol intoxication but record a breath alcohol level of zero
– E.g. nystagmus, ataxia, nausea, vomiting, bradycardia & hypotension)
Withdrawal presents as rapid onset, prolonged alcohol withdrawal picture, with less autonomic arousal and risk of seizures, but marked confusion, delirium & hallucinations, waxing & waning over a two week period
8:2 Indications and guidelines Gamma Hydroxybutyrate (GHB) Withdrawal (1)

Management may require the use of both short & long acting benzodiazepines
Additional sedation with propofol may be required in some patients
There is no validated tool for recording GHB withdrawal symptoms
8:2 Indications and guidelines GHB withdrawal (2)

Generally, physical dependence does not appear to occur with steroid use
8:2 SteroidsWithdrawal