
Preparation for transplantation dr ahmed kamal
59
PREPARATION FOR KIDNEY TRANSPLANTATION Ahmed I. Kamal, MD, FISN Mansoura Urology and Nephrology Center Mansoura University
Transcript of Preparation for transplantation dr ahmed kamal

PREPARATION FOR KIDNEY TRANSPLANTATION
Ahmed I. Kamal, MD, FISN
Mansoura Urology and Nephrology Center
Mansoura University

Rational for living donation
• Better out come
• Shorter waiting time
• Elective planning and optimization of the recipient health status
• Realistic chance for pre-emptive kidney transplantation
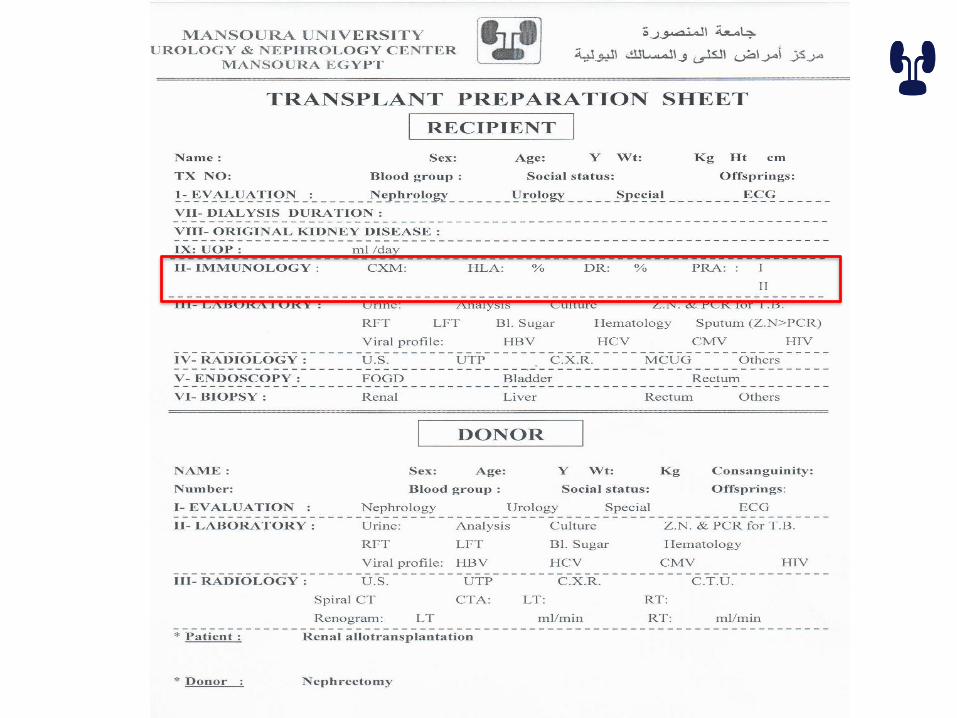
Preparation
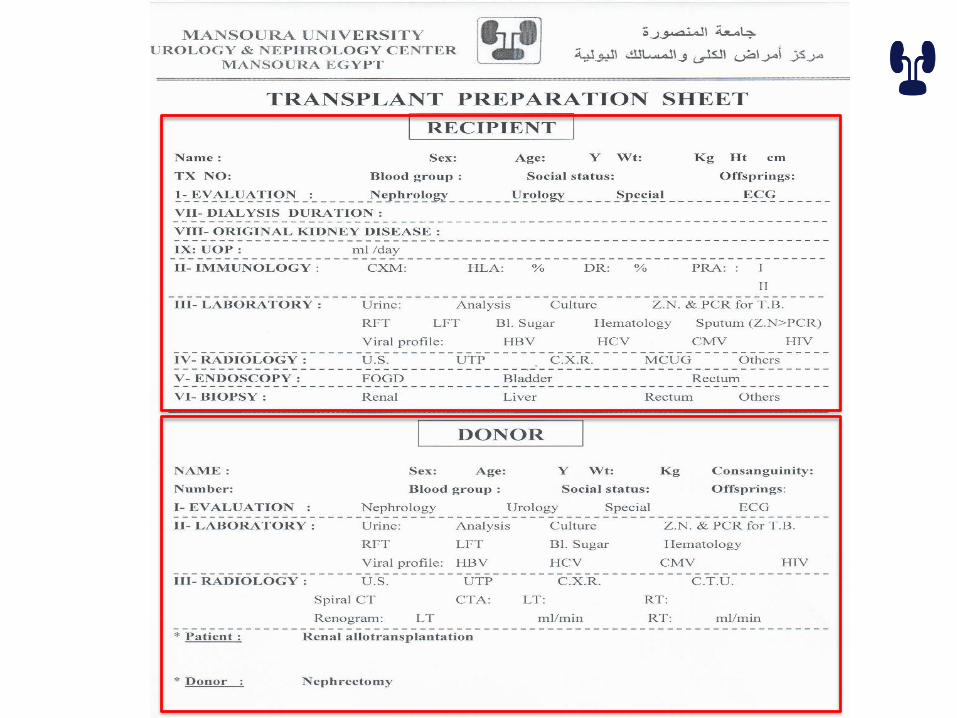

Donor evaluation process
• Education, counseling and consenting
• Psychological evaluation
• Medical screening process
• Identification of transmissible infections
• Evaluation of renal anatomy
Education, counseling and consenting
• Complications
• Blood grouping and HLA
• Medical evaluation steps
• Stress of the right to withdraw at any time
• Follow up
• Informed consent
Erratum in: Am J Transplant. 2015 May;15(5):1447
Psychological evaluation
• Psychiatrist, psychologist or social worker
• For :
– Psychological evaluation and identification of active mental health problems
– Social assessment including high risk behavior
– Assessment of consenting ability
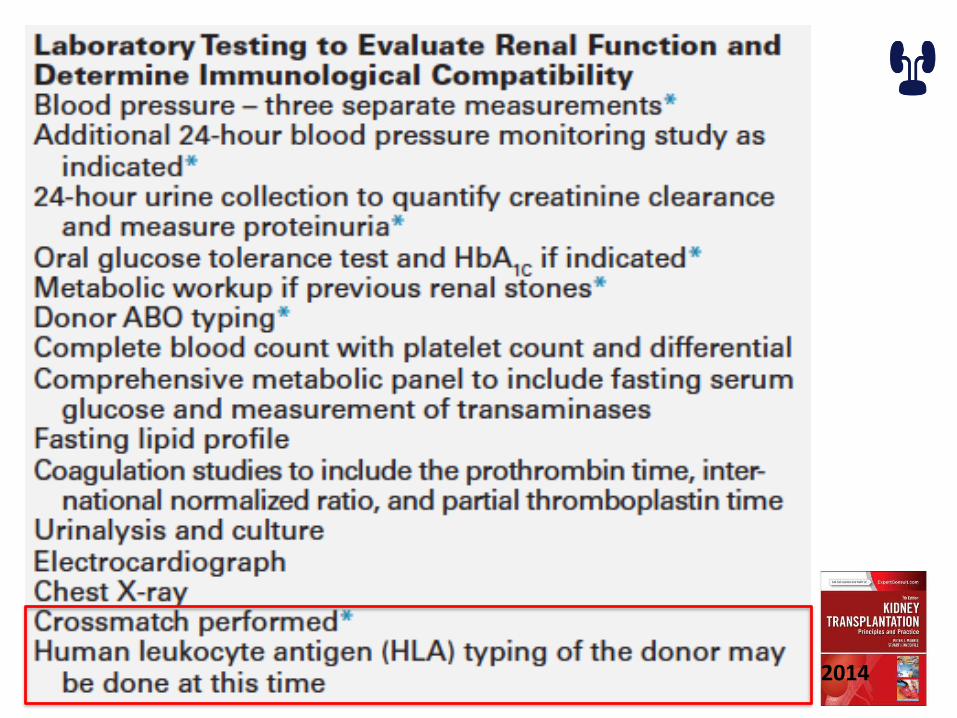
Medical screening process
• History of physical examination
• Laboratory testing
• Identification of transmissible infection
• Evaluating renal anatomy and function

2014


COUPLE EVALUATION
• Education, counseling and consenting• Detailed history • Medical evaluation• Identification of active infections• Evaluation of urinary tract• Hematological and full chemistry • Virology screening • Microbiology
– Urine culture – TB ZN and PCR
2014
Immunological work up
• Cross Match
• HLA genotyping
• (PRA) panel reactive antibodies


Role of the NIH Standard Crossmatch in Kidney Transplant Outcomes
Graft SurvivalRecipients with Anti-HLA Antibodies Recipients
without Anti-HLA
AntibodiesPositive
CrossmatchNo
CrossmatchNegative
Crossmatch
ImmediateFailure
24 (80%) 6 (26%) 4 (15%) 4 (2.4%)
Failure < 3months
0 6 4 32
Failure > 3months
1 3 7 22
Survival < 3months
2 2 1 6
Survival > 3months
3 (10%) 6 (26%) 11 (41%) 104 (62%)
Total Patients 30 23 27 168
80
Patel and Terasaki, NEJM 280:735, 1969

Donor
HanksMononuclear
cell layer
Ficoll
Recipient
Serum
23o
C
30
23o
C
60
Standard NIH Crossmatch
Rabbit
complement

Antiglobulin-Enhanced Technique
• More sensitive
• Can detect non-complement binding antibodies
• Can detect antibodies present in small amounts

Donor
Hanks
Mononuclear
cell layer
Ficoll
Recipient
Serum
Anti-human
globulin
antibodies
23o
C30
23o
C
60
Anti-human Globulin Enhanced Crossmatch
Wash x 3Rabbit
complementC

Laser
Cells
Flow chamber
Laser activated fluorochromes
emit light in red or green spectrum
Flow Crossmatch
Donor cells are incubated with
recipient serum and then fluorochrome-coated antihuman
antibodies

Flow cytometry cross match
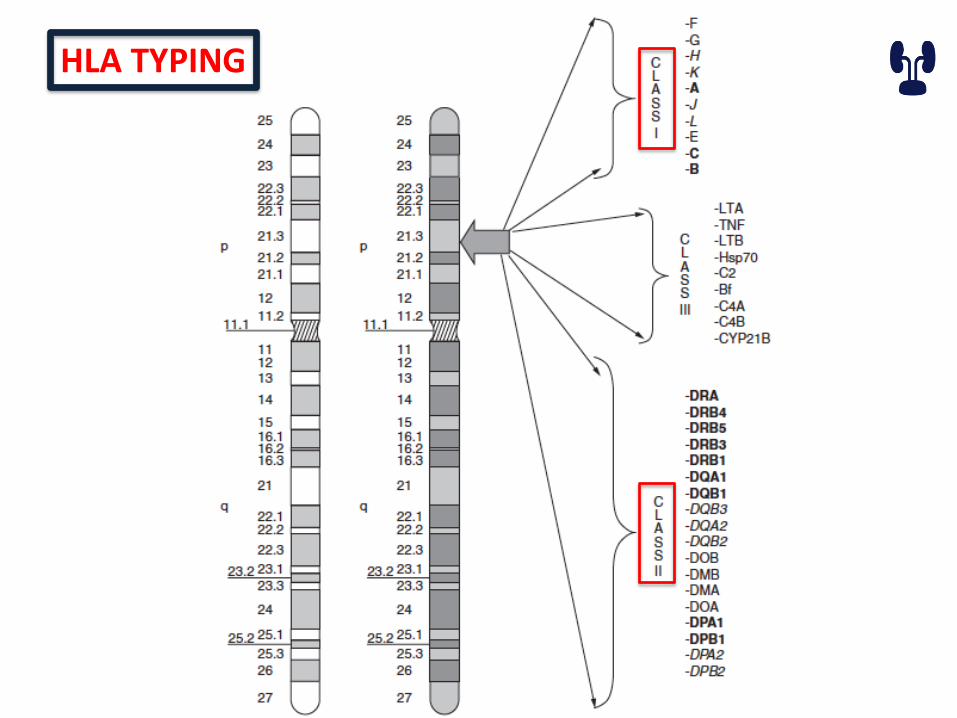
HLA TYPING
•MHC class I molecules•HLA A, B, C•found on all nucleated cells
•MHC class II molecules•HLA DP, DQ, DR•Expressed on antigen presenting cells (and inducible)
•Nomenclature • according to the techniques “ serological or DNA sequencing “
Immunological work up
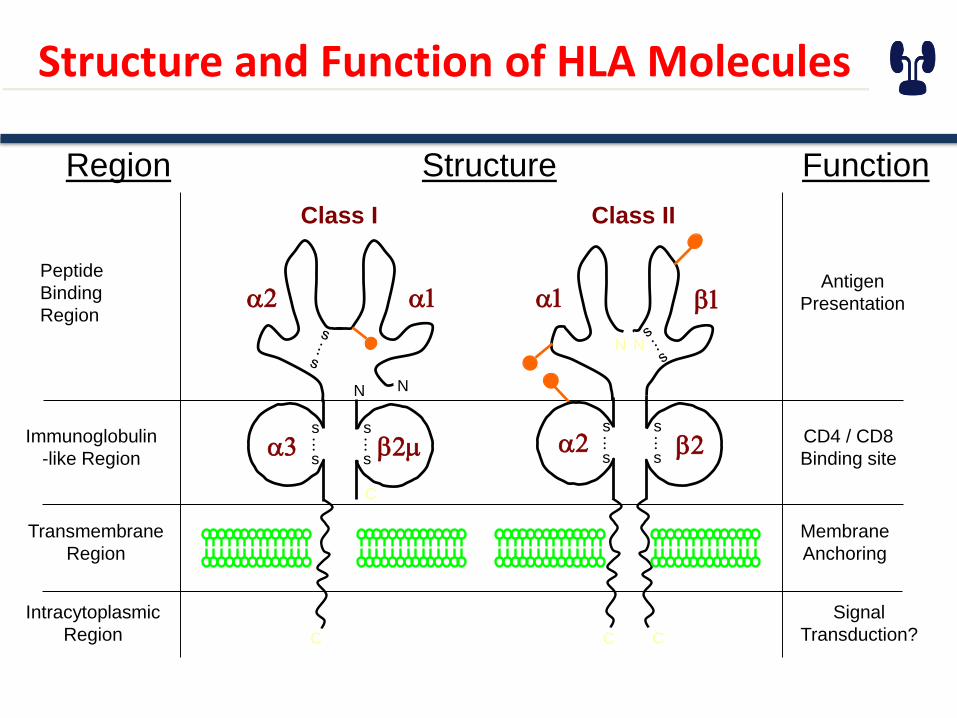
Structure and Function of HLA Molecules
StructureRegion
Peptide
Binding
Region
Immunoglobulin
-like Region
Transmembrane
Region
Intracytoplasmic
Region
Function
Antigen
Presentation
CD4 / CD8
Binding site
Membrane
Anchoring
Signal
Transduction?
C
C
Class I
a2 a1
NN
a3 b2ms
.
..s
s
.
..s
C C
Class II
NN
a1 b1
a2 b2s
.
..s
s
.
..s


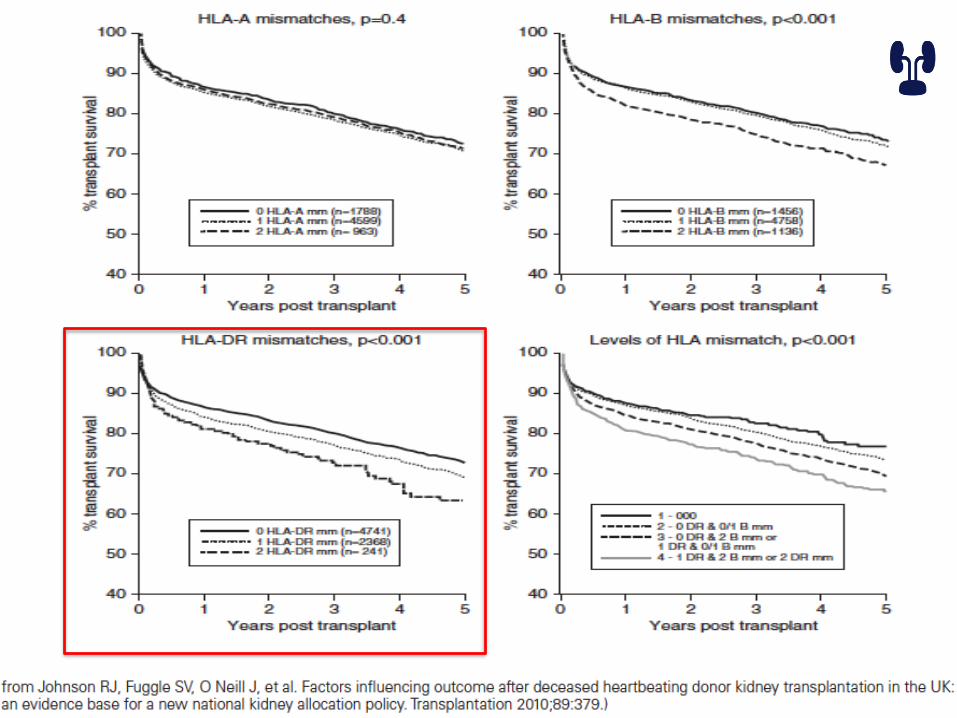
Match v. Mismatch
A2A7
B7
B8
DR15
DR3
Samy
A1
A2
B27
B8DR3
DR4 Mai
A1
A2
B27
B8DR11
DR4
Seif
PRA
• Panel Reactive Antibodies
• Donor non specific
• Donor specific
• Different limit across centers
Why Do Patients Make Anti-HLA Antibodies?
Antibodies occur due to exposure to:
-- blood product
-- pregnancies
-- transplants
-- idiopathic

Identification of transmissible infection
• Identification of transmissible infection
– HCV, HBV, HIV and CMV
– TB
– Rapid plasma reagin
– Strongleloids, Trypanosoma cruzi and West Nile virus
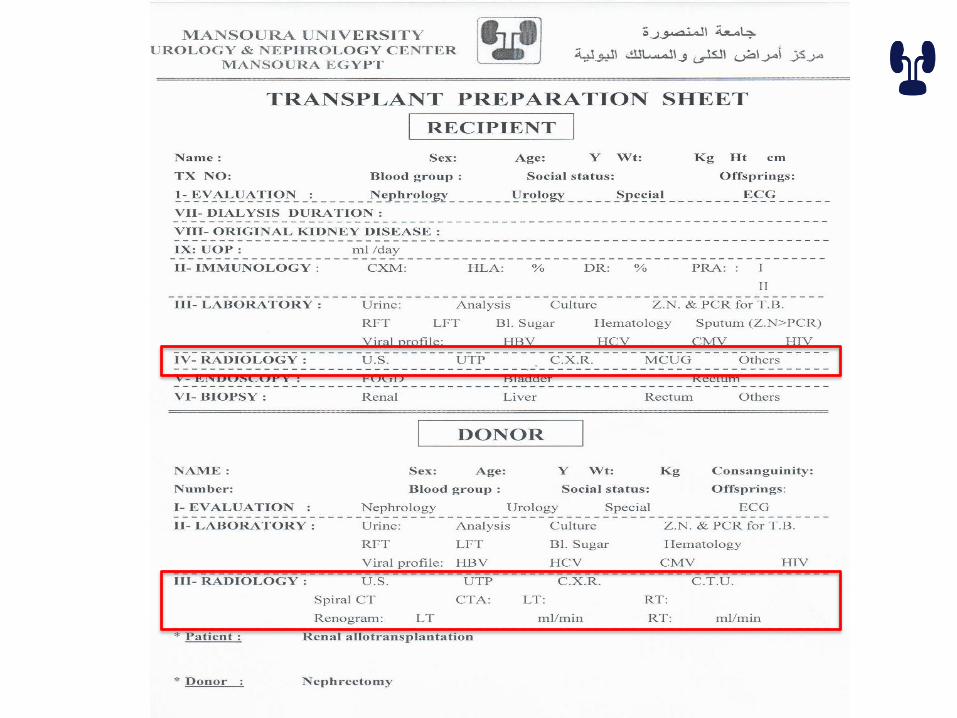
DONOR RADIOLOGICAL ASSESSMENT

US Chest x ray

Spiral CT CTA

Renogram

RECIPIENT RADIOLOGICAL ASSESSMENT

MCUG FOGD

ENDOSCOPY
• Cystoscopy
– Exclude any bladder lesion
–Any uretheral narrowing
–Assessment of bladder capacity
–Biopsy any suspicious lesions

SURPRISES

SURPRISES
• FINAL CROSS MATCH
• INEVITABLE BLOOD TRANSFUSIONS
• CATCHING INFECTIONS
• DONOR HESITATION
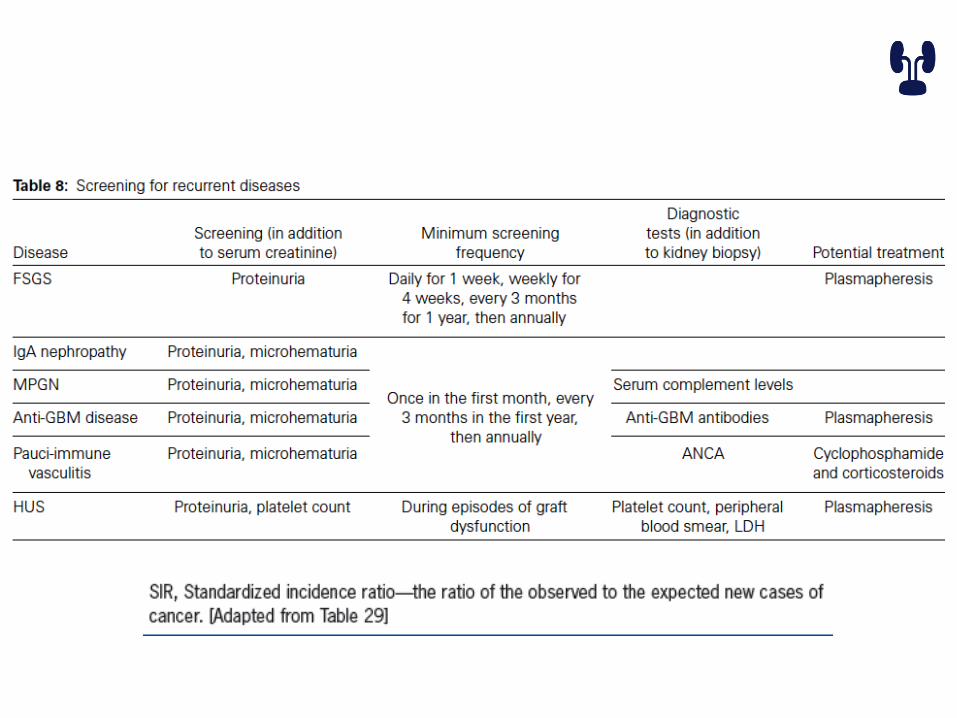
• RECURRENT DISEASES “MODIFIED PROTOCOL”
• MISSED DATA “HISTORY”


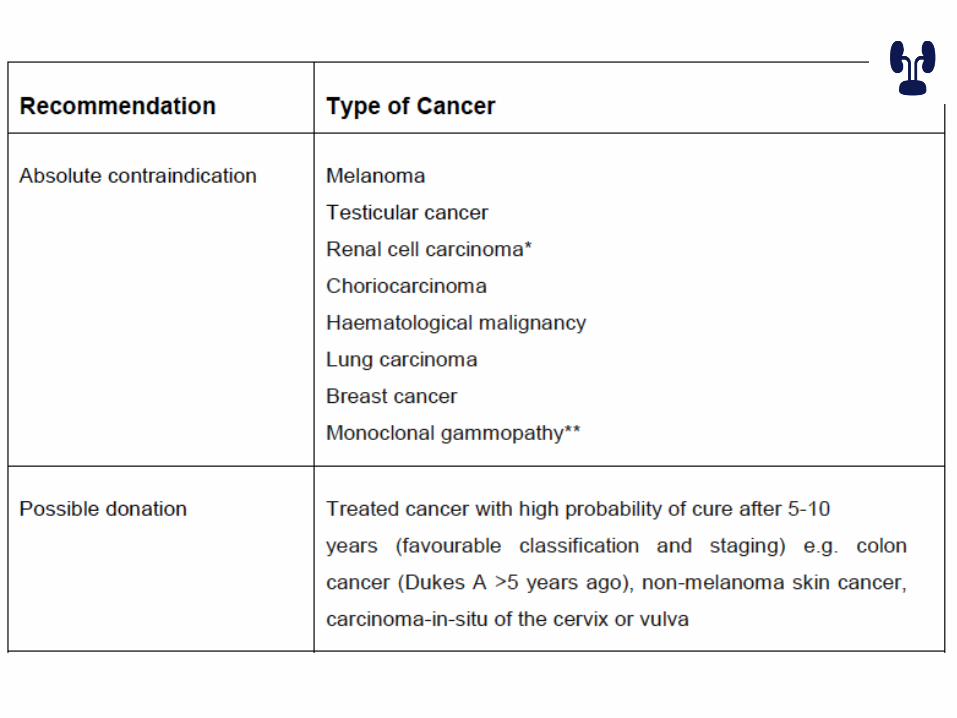
Contraindication for donation
• Absolute – <18 year-old – Active substance abuse– Impaired ability ta make a decision– Hypertension – DM– Morbid obesity– Renal disease– Renal stones – Inherited renal disease– Infections – Cancer – Cardiovascular disease – Significant size discrepancy
Contraindication for donation
• Relative
– Age > 65
– Controlled Hypertension
– Impaired glucose tolerance
– Obesity
– Borderline line renal function
– Microscopic hematuria
– Single renal stone
SPECIFIC SITUATIONS
• Re-transplant patient
– Cause of the first graft loss
– Duration of the first transplant
– Nephrectomy
– Malignancy, cardiovascular risk
SPECIFIC SITUATIONS
• pre-sensitized patient


How we detect it
• Serology
• DNA sequencing
– SSOP (sequence specific oligonucleotide probe)
– SSP (sequence specific primer)
– SBT (sequencing based typing)
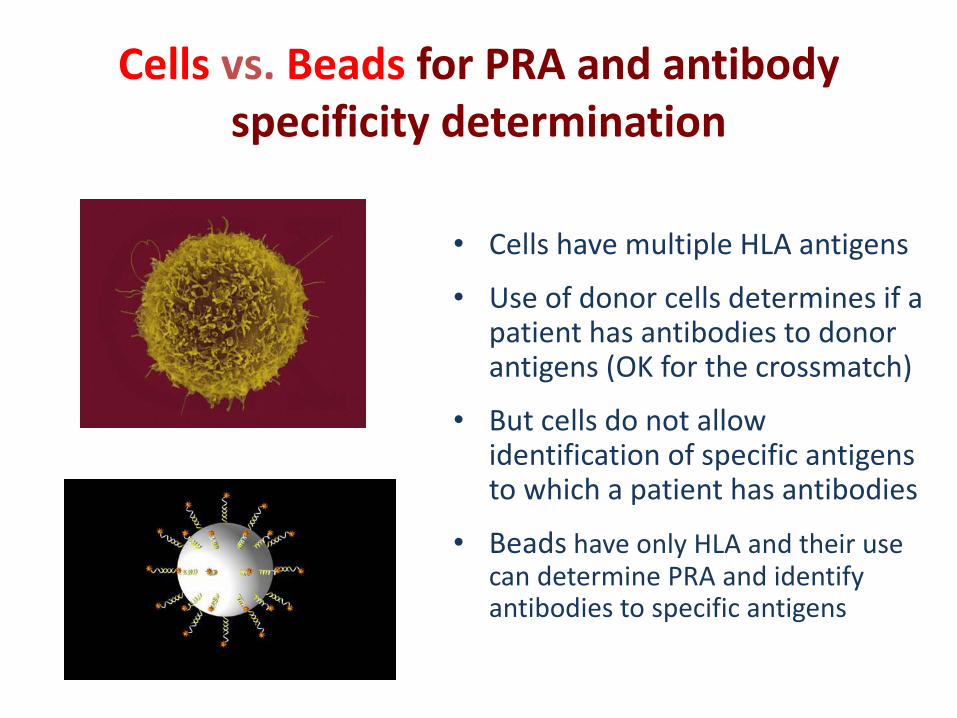
Cells vs. Beads for PRA and antibody specificity determination
• Cells have multiple HLA antigens
• Use of donor cells determines if a patient has antibodies to donor antigens (OK for the crossmatch)
• But cells do not allow identification of specific antigens to which a patient has antibodies
• Beads have only HLA and their use can determine PRA and identify antibodies to specific antigens

FLOW PRA value
• Percentage of HLAantigen coatedbeads in a pool thatreact withantibodies in apatient’s serum
Negative control
Patient Serum
Background fluorescenceof a negative control
Increased fluorescenceindicatespresence of antibodies
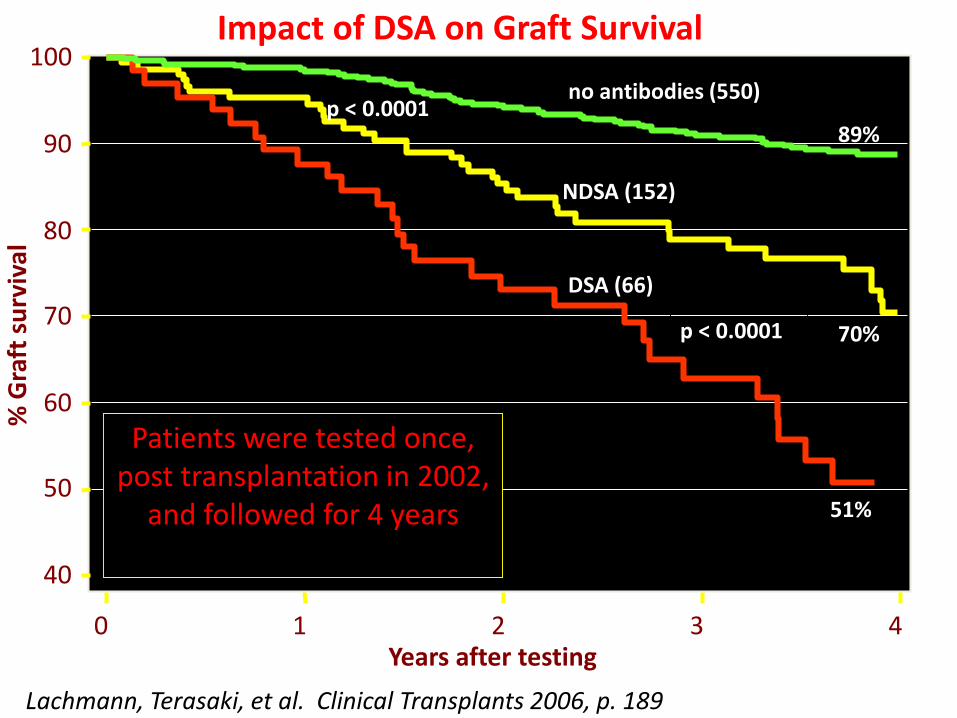
40
50
60
70
80
90
100
0 1 2 3 4
NDSA (152)
DSA (66)
no antibodies (550)
89%
Years after testing
% G
raft
su
rviv
al
p < 0.0001
p < 0.0001 70%
51%
Lachmann, Terasaki, et al. Clinical Transplants 2006, p. 189
Impact of DSA on Graft Survival
Patients were tested once, post transplantation in 2002,
and followed for 4 years
HLA Antibody Identification
•Using Luminex Single Antigen Beads
•Beads have HLA molecules of a single specificity
•Can identify unacceptable donor antigens
•Can identify acceptable donor antigens