Preparation for Percutaneous Ablation Procedures
10
Preparation for Percutaneous Ablation Procedures Ian M. Brennan, MD, Salomao Faintuch, MD, and Muneeb Ahmed, MD Percutaneous tumor ablation is now commonly used to treat a wide range of focal tumors. Patients eligible for ablation often have complex medical problems that preclude them from receiving other treatments. The interventional radiologist needs to perform a careful clinical evaluation of each patient before the procedure to determine which patients are suitable candidates for treatment and to identify patients who may be at a higher risk for complications. The clinical consultation also provides an opportunity to prepare the patient for the ablation and to appropriately plan the procedure. In this article, we discuss key components of the consultation and concepts regarding patient evaluation and preparation for a tumor ablation procedure. Tech Vasc Interventional Rad 16:209-218 C 2013 Elsevier Inc. All rights reserved. KEYWORDS Tumor Ablation, Pre procedure Assessment Introduction The treatment of cancer now involves multiple medical disciplines including medical oncology, radiation oncology, surgery, and interventional radiology. Individual cases should be discussed in a multidisciplinary manner involving all specialties so that an optimal treatment strategy can be decided upon. Once the decision is made to proceed with percutaneous ablation, the responsibility falls to the interven- tional radiologist to formulate a plan culminating in a safe and effective percutaneous treatment. Patients undergoing percu- taneous tumor ablation may have a more advanced disease stage than those undergoing a potentially curative resection. In addition, many patients referred for percutaneous ablation have signi ficant medical comorbidities often precluding more conventional open surgical resection. This article outlines some of the general and patient specific factors requiring consideration when planning a percutaneous tumor ablation on this sometimes challenging patient population. Preprocedural Clinical Assessment The decision to proceed with a percutaneous tumor ablation is ideally made in a multidisciplinary manner with an agreed- upon treatment plan. Most patients are then contacted directly following this to inform them of the consensus decision and the proposed treatment plan. At this point, it is crucial that the patient be referred to the interventional radiology clinic. Although patients often have some understanding of the planned procedure from their primary care physician or medical oncologist, this is their first opportunity to receive detailed background and more in-depth procedural informa- tion from members of the interventional radiology team. The Clinic Consultation The diagnosis of cancer is a life-changing event for the patient and their family. Many patients are referred for percutaneous ablation very soon following their initial diagnosis and it is worth investing time at the beginning of the consultation to empathize and gauge the patient’ s insight into their disease. Although the patient’ s medical imaging and brief clinical history have almost certainly been reviewed at the multi- disciplinary meeting, this often is the first opportunity to obtain the patient’ s full medical history, note relevant physical examination findings, assess performance status, review current medications, and gauge overall treatment expect- ations. In our practice, we strongly encourage family mem- bers to accompany the patient during the clinic visit to both reduce anxiety and optimize the exchange and retention of information. Studies have shown the capacity to absorb educational information is impaired by the presence of fear or anxiety. 1 Very often it is the accompanying family member who would be taking care of the patient in the early postprocedure period and that person should be well informed of what to expect in normal recovery and be instructed to identifying the warning signs of potential 1089-2516/13/$ - see front matter & 2013 Elsevier Inc. All rights reserved. 209 http://dx.doi.org/10.1053/j.tvir.2013.08.004 Section of Interventional Radiology, Department of Radiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA. Address reprint requests to Ian M Brennan, MD, Section of Interventional Radiology, Department of Radiology, Beth Israel Deaconess Medical Center, 1 Deaconess Rd, Boston, MA 02215. E-mail: ibrennan@ bidmc.harvard.edu
Transcript of Preparation for Percutaneous Ablation Procedures
1089-2http://d
SectionDea
AddresRadCenbidm
Preparation for Percutaneous Ablation Procedures
Ian M. Brennan, MD, Salomao Faintuch, MD, and Muneeb Ahmed, MD516/13/$ - seex.doi.org/10.1
of Interventioconess Medics reprint requeiology, Departer, 1 Deacoc.harvard.ed
Percutaneous tumor ablation is now commonly used to treat a wide range of focaltumors. Patients eligible for ablation often have complex medical problems that precludethem from receiving other treatments. The interventional radiologist needs to perform acareful clinical evaluation of each patient before the procedure to determine whichpatients are suitable candidates for treatment and to identify patients who may be at ahigher risk for complications. The clinical consultation also provides an opportunity toprepare the patient for the ablation and to appropriately plan the procedure. In this article,we discuss key components of the consultation and concepts regarding patientevaluation and preparation for a tumor ablation procedure.Tech Vasc Interventional Rad 16:209-218 C 2013 Elsevier Inc. All rights reserved.
KEYWORDS Tumor Ablation, Pre procedure Assessment
IntroductionThe treatment of cancer now involves multiple medicaldisciplines including medical oncology, radiation oncology,surgery, and interventional radiology. Individual cases shouldbe discussed in a multidisciplinary manner involving allspecialties so that an optimal treatment strategy can bedecided upon. Once the decision is made to proceed withpercutaneous ablation, the responsibility falls to the interven-tional radiologist to formulate a plan culminating in a safe andeffective percutaneous treatment. Patients undergoing percu-taneous tumor ablation may have a more advanced diseasestage than those undergoing a potentially curative resection.In addition, many patients referred for percutaneous ablationhave significant medical comorbidities often precluding moreconventional open surgical resection. This article outlinessome of the general and patient specific factors requiringconsideration when planning a percutaneous tumor ablationon this sometimes challenging patient population.
Preprocedural ClinicalAssessmentThe decision to proceed with a percutaneous tumor ablationis ideally made in a multidisciplinary manner with an agreed-
front matter & 2013 Elsevier Inc. All rights reserved.053/j.tvir.2013.08.004
nal Radiology, Department of Radiology, Beth Israelal Center, Harvard Medical School, Boston, MA.sts to Ian M Brennan, MD, Section of Interventionaltment of Radiology, Beth Israel Deaconess Medicalness Rd, Boston, MA 02215. E-mail: ibrennan@u
upon treatment plan. Most patients are then contacted directlyfollowing this to inform them of the consensus decision andthe proposed treatment plan. At this point, it is crucial that thepatient be referred to the interventional radiology clinic.Although patients often have some understanding of theplanned procedure from their primary care physician ormedical oncologist, this is their first opportunity to receivedetailed background and more in-depth procedural informa-tion from members of the interventional radiology team.
The Clinic ConsultationThe diagnosis of cancer is a life-changing event for the patientand their family. Many patients are referred for percutaneousablation very soon following their initial diagnosis and it isworth investing time at the beginning of the consultation toempathize and gauge the patient’s insight into their disease.Although the patient’s medical imaging and brief clinicalhistory have almost certainly been reviewed at the multi-disciplinary meeting, this often is the first opportunity toobtain the patient’s full medical history, note relevant physicalexamination findings, assess performance status, reviewcurrent medications, and gauge overall treatment expect-ations. In our practice, we strongly encourage family mem-bers to accompany the patient during the clinic visit to bothreduce anxiety and optimize the exchange and retention ofinformation. Studies have shown the capacity to absorbeducational information is impaired by the presence of fearor anxiety.1 Very often it is the accompanying family memberwho would be taking care of the patient in the earlypostprocedure period and that person should be wellinformed of what to expect in normal recovery and beinstructed to identifying the warning signs of potential
209

I.M. Brennan, S. Faintuch, and M. Ahmed210
complications. Some patients also find it of benefit to beshown their imaging studies to get a sense of the size andlocation of the lesion undergoing treatment. It is important toprovide contact information at the end of the clinic visit toallow the patient easy access if further questions should ariseor if an appointment needs to be changed at short notice.
Table 1 Eastern Cooperative Oncology Group (ECOG) Scor-ing System
Grade Performance Status
0 Fully active and able to carry on all prediseaseperformance without restriction.
1 Restricted in physically strenuous activity butambulatory and able to carry out work of a lightor sedentary nature, for example, light housework and office work.
2 Ambulatory and capable of all self-care but unableto carry out any work activities; up and aboutmore than 50% of waking hours.
Patient HistoryA detailed clinical history should be obtained for everypatient. This includes a detailed evaluation of currentsymptoms and therapy, a review of systems, obtaining amedical and surgical history, review of all medications andallergies, and a review of family and social history. Somecenters find the use of a printed clinic template helpful inadding structure to the consultation and ensuring no aspectsof the history and physical examination are overlooked.2
Evaluation for cancer-related symptoms should be per-formed, which includes both localized symptoms (such aspain from tumor invasion), symptoms related to dysfunctionof the underlying organ (such as gastrointestinal bleeding orabdominal swelling in patients with hepatocellular carci-noma and cirrhosis or home oxygen requirements inpatients with chronic obstructive pulmonary disease), andconstitutional symptoms (fatigue, weight loss, or anorexia),as these are critical to staging the disease and identifyingpatients who would be good candidates for ablative thera-pies. A detailed oncologic history, including treatments thepatient has previously received or is currently undergoing(such as chemotherapy), should also be obtained. Access toprior medical records and imaging studies, especially thosefrom outside hospitals, are critical to evaluate response fromprevious systemic or regional therapies.The review of systems can give clues to potential prob-
lems during or immediately after the ablation procedure. Forexample, a history of bladder outlet obstruction in an olderman may prompt placement of Foley catheter during theprocedure, whereas a history of rapidly developing ascitescausing orthopnea may require a periprocedural paracent-esis. Involuntary weight loss of 5% or more over a 6-monthperiod in patients with cancer is associated with a shortermedian survival time and should be documented if present.3
A thorough medication history should be obtained, with aparticular focus on drug or contrast allergies, anticoagulant,and diabetic medications (described later). A detailed reviewof the patient’s surgical history is important with previoussurgical resection in the target organ obviously relevant. Inaddition, patients with a previous bilioenteric anastomosisor urinary diversion procedure are at an increased risk ofinfectious complications following hepatic and renal abla-tion, respectively, and such patients may require a longerantibiotic prophylaxis regimen (described later).4 It isimportant to ask about previous anesthesia and any asso-ciated adverse events should be recorded.
3 Capable of only limited self-care, confined to bedor chair more than 50% of waking hours.
4 Completely disabled; cannot carry on any self-care; totally confined to bed or chair.
5 Dead.
Performance StatusOncologists use an assessment of performance status tograde the effect of the patient’s disease and their overall
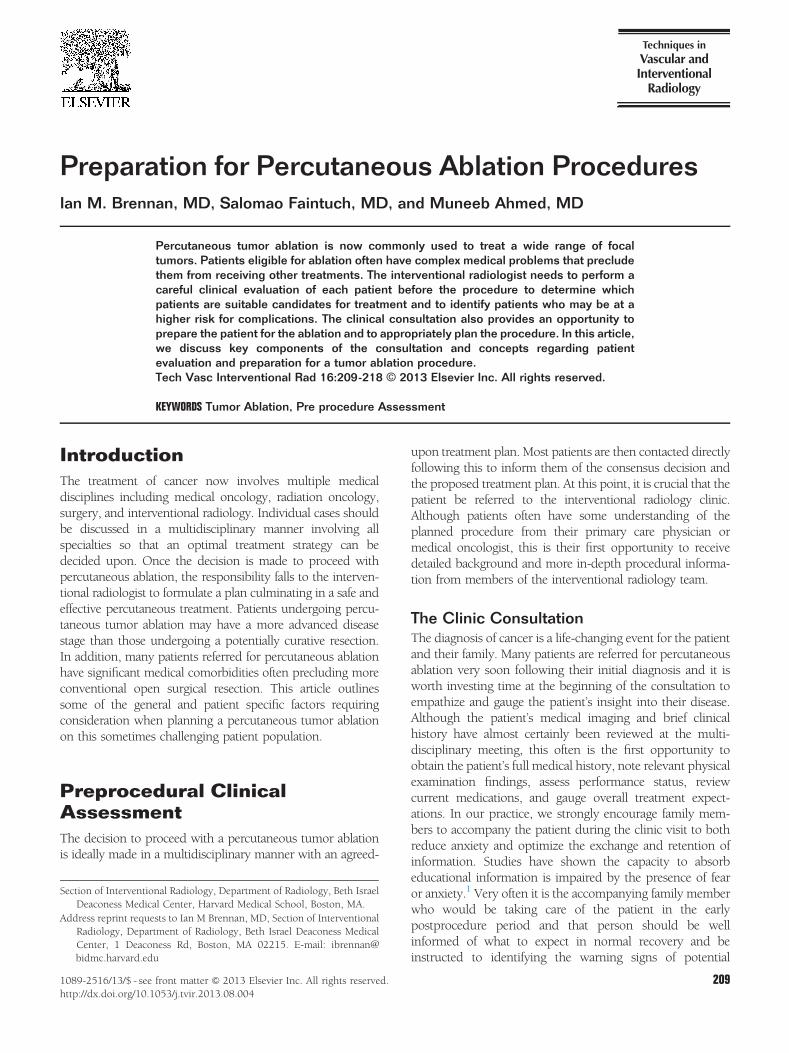
functional status. It has an important role in gaugingprognosis and in patient selection for a particular therapy.The Eastern Cooperative Oncology Group (ECOG) scor-ing system has 5 levels (Table 1).5 Another commonlyused score, the Karnofsky score, has 11 levels (Table 2).6
The Eastern Cooperative Oncology Group system has asuperior predictive value compared with the Karnofskyscore for patient prognosis.7 Overall, a falling performancestatus score is indicative of a poor prognosis and should betaken into consideration when an ablative procedure isplanned in the context of the overall goals of care.
Physical ExaminationThis can be directed toward the ablation procedure. Animportant step in the physical examination is to identifypatients in whom moderate sedation is unlikely to besufficient for a safe and effective ablation procedure. Suchpatients would require monitored anesthesia care (MAC)or general anesthesia (described later). It is also importantto evaluate the patient’s airway and document a Mallam-pati airway score.8 In our practice, a Mallampati score of IVrequires an anesthesia consultation and likely generalanesthesia with airway protection. A thorough cardiovas-cular examination is required to assess patient suitabilityfor conscious sedation. The patient’s American Society ofAnesthesiologists physical status score should be deter-mined (Table 3). An American Society of Anesthesiologistsscore of IV should also prompt an anesthesia consultation.Absent or diminished breath sounds could indicate apleural effusion or atelectasis, conditions that could beoptimized before the ablation procedure. Large-volumeascites impairing respiration may require a preproceduralparacentesis. Patients with cardiac disease should havetheir exercise tolerance classified by the New York HeartAssociation functional classification score (Table 4). Theneed for supplemental home oxygen or a continuouspositive airway pressure (CPAP) mask should also bedocumented. Often, patients need to bring in their bilevelpositive airway pressure (BiPAP) or continuous positive
Table 2 Karnofsky Performance Status Score
Score(%) Performance Status
100 Normal, no complaints, and no signs of disease.90 Capable of normal activity; few symptoms or signs
of disease.80 Normal activity with some difficulty and some
symptoms or signs.70 Caring for self; not capable of normal activity or
work.60 Requiring some help; can take care of most
personal requirements.50 Requires help often; requires frequent medical
care.40 Disabled; requires special care and help.30 Severely disabled; hospital admission indicated
but no risk of death.20 Very ill, urgently requiring admission, requires
supportive measures or treatment.10 Moribund; rapidly progressive fatal disease
processes.0 Death.
Preparation for percutaneous ablation procedures 211
airway pressure machine on the day of the procedure foruse during moderate sedation or MAC anesthesia. Pulmo-nary function testing should be carried out before lungablation to assess pulmonary reserve.9
It is important to evaluate the planned percutaneousaccess route with special attention to the required patientposition and likely skin entry sites, evaluating for evidenceof infection or other abnormality. The presence of fixed-limb flexion or spinal deformities can also impair percuta-neous access. Finally, 25% of patients with cancer have anepisode of severe depression during their illness, and caremust be taken to assess their overall psychological state.10
Severe anxiety may require MAC or even general anes-thesia to allow a successful ablation.
Review of Laboratory Tests and ImagingClose attention should be paid to the patient’s renalfunction as dehydration during the periprocedural period
Table 3 American Society of Anesthesiologists Physical Status ClAnesthesiologists Relative Value Guide)
ASA Score Preoperative Health Status
AzSA 1 Normal healthy patient
ASA 2 Patients with mild systemic disease
ASA 3 Patients with severe systemic disease
ASA 4 Patients with severe systemic disease that isa constant threat to life
ASA 5 Moribund patients who are not expected tosurvive without the operation
ASA 6 A declared brain-dead patient whose organsare being removed for donor purposes
ASA, American Society of Anesthesiologists.
can exacerbate renal impairment. This becomes moreimportant when intravenous (IV) contrast administrationis planned (described later). Total bilirubin levels, pro-thrombin time, and albumin levels are components of theChild-Pugh hepatic function scoring system, whereasbilirubin, international normalized ratio, and serum crea-tinine levels are used to calculate the model for end-stageliver disease (MELD) score.11,12 Both scoring systems givean approximation of hepatic function and predicted lifeexpectancy and should be taken into consideration whencontemplating ablative procedures on patients withadvanced liver disease. Studies have shown worse out-comes in ablation for hepatocellular carcinoma with MELDscores greater than 10.13 Coagulation parameters arediscussed below.All available imaging should be reviewed. This is
important for procedural planning, such as identifyingroutes of access, and allows one to confirm during the visitthat any specific positioning or access requirements can bemet during the procedure. Additionally, depending on thetumor type, one should ensure that all imaging is recent(ideally, obtained within 1 month of the procedure) or thatadditional imaging is planned. Finally, careful review ofimaging ensures that the diagnostic assessment that led tothe initial referral is indeed correct.
Assessment and Establishing Goals of CareAfter a complete clinical consultation, including review ofthe detailed history, a physical examination, and review oflaboratory and imaging data, a determination can be madeas to whether the patient is a candidate for percutaneousablation, both from a technical perspective and basedupon their clinical status.The clinical history allows the patient to describe their
overall symptoms and current quality of life and also tooutline what they hope to gain from the proposed treat-ment. This leads to an important discussion of the patient’sand their family’s expectations from the ablation proce-dure. A clear distinction should be made between apotentially curative ablation and a more palliative proce-dure. The physician should clarify the rationale behind the
assification System (As outlined in the American Society of
Comments
No physiologic or psychiatric disturbance. Healthy withgood exercise tolerance
No functional limitations; well-controlled disease of1 body system
Some functional limitation; controlled disease of morethan 1 body system or 1 major system; no immediatedanger of death
Has at least 1 severe disease that is poorly controlled orat end stage; possible risk of death
Not expected to survive 424 h without surgery;imminent risk of death

Table 4 New York Heart Association Functional Classifi-cation (The Criteria Committee of the New York HeartAssociation. Nomenclature and Criteria for Diagnosis ofDiseases of the Heart and Great Vessels (ed 9). Boston,MA, Little, Brown & Co, 1994:253-256)
A Class Symptoms
I Cardiac disease; but no symptoms orlimitation in ordinary physical activity.
II Mild symptoms (mild shortness of breath orangina or both) and slight limitation duringordinary activity.
III Marked limitation in activity due tosymptomatic cardiac disease, even duringmild activity, for example, walking shortdistances (20-100 m)
Comfortable only at rest.IV Severe limitations in any physical activity;
may experiences symptoms even while atrest; mostly bedbound patients.
I.M. Brennan, S. Faintuch, and M. Ahmed212
proposed procedure, to potentially cure, improve survival,or provide symptom relief, and should ensure the patientunderstands this fully. It should be remembered that formany elderly patients, an improvement in quality of lifecan be as important as overall improved survival. If theprimary goal of the ablation is pain control, an assessmentof the patient’s pain levels and analgesic requirementsusing a linear scale or pain diary is of great benefit,especially in gauging treatment response.
Procedure Discussion and Obtaining InformedConsentThe clinic is the ideal setting in which to discuss theprocedure in detail and provide information to the patientand their family about how to prepare, what to expect onthe day of the procedure (both before and after the actualablation procedure), and outline a plan for post ablationfollow-up and care. Detailed preprocedure instructionscan be provided, including maintaining a nil-by-mouthstatus before the procedure for sedation or anesthesia.Patients often have questions as to what constitutes a nil-by-mouth status, and there may be institution-specificguidelines regarding the time required (eg, at our institu-tion, patients are required to maintain a nil-by-mouthstatus for 6 hours before the procedure with regard to solidor nonclear liquid intake including tube feeds and 2 hoursfor clear liquids). Instructions regarding preproceduremanagement of medication (described later) should alsobe given. Information on arrival and procedure times,instructions on how to get to the preprocedure area (as thisis often separate from clinic locations at many institutions),and instructions for parking are also very helpful.Detailed information on anticipated postprocedure
course should also be provided. This includes expectedsymptoms immediately afterward and how they wouldbe managed, anticipated time spent in recovery, whatthe patient may expect to feel in the postprocedure courseafter going home, and a discussion of when patientsmight need to be admitted for observation. Postprocedure
instructions should also be reviewed, such as any restric-tions on activity or work. This is important in allowingpatients to plan for treatment, take appropriate time offfrom work, or plan travel. This discussion also allows oneto identify patient-specific circumstances that may requirespecial attention, such as whether the patient lives alone, iscomfortable going directly home following the procedure,and can get transportation.During this process, written informed consent should
also be obtained. Again, the presence of family members isusually greatly reassuring for patients and should bedocumented on the consent form. The consent processallows an honest and frank discussion of treatment goals,potential complications, and their treatment, if required.We and other centers have found simple illustrations tobe helpful in explaining interventional procedures and inaiding consent.14 Other groups give printed informationsheets during the clinic visit to further reinforce the pointsmade in the consent process.15 Generally, risks frompercutaneous ablation can be broadly divided into risksthat are related to needle puncture (bleeding, pneumo-thorax, and tract seeding), and those that are related tonontarget thermal injury (injury to adjacent structures,such as colon, stomach, nerves, diaphragm, and gallblad-der). Patients often want specific information about therisks of the procedure. A review of the literature ordedicated reviews of organ- and tumor-specific ablationare readily available and good sources of information.Additionally, societal quality guidelines (such as thosepublished by the Society of Interventional Radiology [SIR])are also an excellent source of specific risk-relatedinformation.The consent should cover the goals of the ablation and
mention other treatment options, outline risks and poten-tial complications and their treatment, and stress the needfor follow-up imaging studies and potential repeat proce-dures.16 It is worth remembering that a sizable proportionof medical malpractice cases relate to perceived poordoctor-patient communication rather than direct proce-dural error.17 If the procedure is being performed as partof a clinical trial, this would require a separate consentform, as usually outlined in the trial protocol. The consentshould also include whether adjunctive or ancillary pro-cedures would be performed at the time of ablation. Forexample, if a percutaneous biopsy is planned, this shouldalso be discussed and mentioned in the consent. For lungablations, the possibility of chest tube placement should bespecifically discussed.
Procedure PlanningThe clinic visit represents an excellent opportunity to planseveral key aspects of the procedure. Careful review ofimaging allows one to plan both the route of percutaneousaccess, what type of ablation modality would be used, andwhether adjunctive procedures (such as hydrodissection)would be required. Based on this, appropriate planningfor type of sedation (general anesthesia or conscious

Preparation for percutaneous ablation procedures 213
sedation) and anticipated procedure length can also beperformed.
Choice of Imaging ModalityThe choice of imaging modality depends on the site of thetarget lesion, lesion conspicuity on that modality, availableequipment and operator preference. Its selection is animportant part of the procedure planning process. Ultra-sound is the modality of choice for probe placement in thesolid abdominal viscera as it allows safe, real-time visual-ization. Once ablation commences however, lesion con-spicuity decreases greatly with gas formation within thetarget lesion. The use of microbubble ultrasound contrastagents has greatly improved the accuracy of this technique,and it is now in common use as a single modality for imageguidance for percutaneous ablation in European and Asiancenters. Contrast-enhanced computed tomography (CT)or magnetic resonance (MR) imaging, when available,continues to have great utility in detection of residualdisease and identification of early postablationcomplications.18
As a result, we perform most visceral ablations usinga combination of ultrasound and contrast-enhanced CTguidance. Following initial probe positioning using ultra-sound, a limited noncontrast CT can be performed withthe probe in situ and correlated with preprocedural cross-sectional imaging. In addition, the CT study allows clearvisualization of the probe position in relation to thesurrounding structures such as the pleura and bowel. Ifthe lesion is not identifiable on ultrasound or CT studies,positioning using landmarks is required. CT is also themodality of choice if hydrodissection or pneumodissectionis required to create a safe path for probe positioning. MR-guided ablation has been described but requires specialequipment and advanced anesthesia planning.19
Sedation PlanningPatients expect and deserve a comfortable experienceduring the ablation procedure. Skilled infiltration of localanesthesia can greatly reduce percutaneous access–relateddiscomfort; however, visceral or osseous pain from theablation itself usually requires systemic medication. Inaddition, percutaneous ablation often requires the patientto remain in a stable position for prolonged periods oftime, which can be a challenge in older or anxious patients.The level of sedation required to perform a safe andeffective procedure with the lowest risk varies greatlyand must be assessed on a case-by-case basis. Minimal-sedation (anxiolysis) and moderate-sedation analgesia(conscious sedation) can be administered to good effectby trained nonanesthesiology personnel. However, ifdeeper sedation is expected to be required (such asdeep-sedation analgesia or general anesthesia), anesthesiaexpertise is needed.On occasion, the patient would have undergone a
previous image-guided biopsy of the target lesion. If thiswas poorly tolerated under moderate sedation, the patient
is unlikely to tolerate a prolonged ablation procedure witha similar sedation strategy. When in doubt, assessment inan anesthesiology preoperative assessment clinic is of greatvalue. The interventionalist should provide the anesthesi-ologist with specific details on the planned procedure type,expected patient position, estimated treatment duration,and importantly, the concerns about performing the caseusing nonanesthesiologist-delivered conscious sedationalone. In selected cases, consideration can be given toregional anesthesia in patients undergoing extremity pro-cedures such as bone ablation or thoracic paravertebralblocks in patients undergoing hepatic ablation.20 Involv-ing anesthesia in the pretreatment planning stage is criticalas requesting assistance in an emergent setting is not ideal.General anesthesia is usually indicated in cases with a
predicted long procedure time (overlapping ablations orchallenging approach), inherently painful (pericapsularliver and osseous lesions), likely poor patient compliance(pediatric patients, old age, claustrophobia, or languagebarrier), patients with a difficult airway (high Mallampatiscore), and those with severe anxiety. In addition, it shouldbe remembered that many patients with cancer are onmultiagent pain management regimens and require signifi-cantly higher narcotic doses than opiate-naive patients.21
If high sedative and narcotic doses are likely to be required,consideration should be given to MAC or general anesthesia.In addition, chemotherapeutic agents can also directly
impair cardiopulmonary function. Pulmonary toxicity is acomplication of many chemotherapeutic agents and is seenin up to 10% of patients.22 The most commonly impli-cated agents include busulfan, bleomycin, methotrexate,and cyclophosphamide. Similarly, patients may developradiation pneumonitis following radiotherapy, which mayeven progress to pulmonary fibrosis. These patients arelikely to have increased supplemental oxygen require-ments and preprocedural pulmonary function test maybe of benefit. In relation to cardiac toxicity, many chemo-therapeutic agents are arrythmogenic (eg, paclitaxel) or canprecipitate myocardial ischemia (fluorouracil).Most centers perform day case percutaneous tumor
ablation even in patients undergoing general anesthesia.However, contingency plans must be in place for overnightadmission in the event of procedural complications or adelayed finish time. Interventional radiology services thatdo not admit directly should have a framework in place toallow postprocedural admission under the referring clini-cian or hospitalist service.Special consideration must be given to the administra-
tion of MAC or general anesthesia in the radiologydepartment, especially when establishing an ablationpractice. General anesthesia performed in C-arm angio-graphic suites may have issues with space and C-armmovement. Ablations performed using intermittent CTimaging require repeated table movement and removal ofall staff from the scanner room during image acquisitions.Lastly, MR-guided ablations require advanced planning toavoid the use of ferromagnetic equipment.23
Finally, studies have defined an important role for non-pharmacologic and behavioral methods in reducing pain

Table 5 Risk Factors for Contrast-Induced Nephropathy(CIN)
Patient-RelatedRisk Factors
Contrast-Related RiskFactors
I.M. Brennan, S. Faintuch, and M. Ahmed214
and anxiety during interventional radiology procedures.24
This is especially true in patients with known high-anxietystates, but it should be considered as a useful adjunctivestrategy in all patients.
Age 470 y High-osmolarity contrastmedium
Chronic kidney disease High viscosityDiabetes mellitus Large contrast volumeCongestive cardiac failure Route of administration (intra-
arterial 4 intravenous)HypertensionLow serum hematocritDehydrationConcurrent use ofnephrotoxic medications(diuretics or NSAIDs)
Periprocedural Antibiotic ProphylaxisThe use of periprocedural prophylactic antibiotics inpercutaneous tumor ablation remains controversial andno randomized controlled trials exist to guide practice.Infectious complications following hepatic ablation arewell described, including periprocedural cholangitis andliver abscess formation. Risk factors for hepatic abscessformation include diabetes mellitus and the presence of abilioenteric anastomosis or common bile duct stent, whichcan result in bacterial contamination of the biliary tree.Similarly, patients with a ureteric stent or ileal conduit areat increased risk of an infectious complication followingrenal ablation. Many groups empirically use prophylaxis inall hepatic ablation cases and may prescribe a longercourse in high-risk patients.25,26 The SIR practice guide-lines from 2010 acknowledge the lack of consensus butrecommend 1.5 g IV of ampicillin/sulbactam for hepaticablation and 1 g of ceftriaxone for renal ablation.27
Management of SpecificClinical IssuesPatients With Impaired Renal FunctionAll periprocedural patients should remain adequatelyhydrated as most would have been fasting from the nightbefore. Isotonic IV fluids such as 0.9% normal salineshould be administered at a rate of 60-80 mL/h, dependingon the patient’s fluid volume status. Following the proce-dure, oral fluid intake should be encouraged as early astolerated.Although not all ablation patients require IV contrast
during or immediately following the procedure, in ourpractice, we routinely perform contrast-enhanced multi-phase CT immediately following renal and liver ablations(described later). Accordingly, it is important to optimizepatients with impaired renal function. Patients with abaseline estimated glomerular filtration rate of less than60 mL/min) or one or more known risk factors should beconsidered to be at high risk of developing contrast-induced nephropathy (CIN) (Table 5).28 Although thereare several risk factors for CIN, patients with both chronickidney disease and diabetes have an overall fourfoldincreased risk.29
A patient with normal renal function and a history ofprevious nephrectomy also warrants judicious use ofiodinated contrast and active hydration. Patients with renalimpairment should avoid angiotensin-converting-enzymeinhibitors, metformin, and nonsteroidal antiinflammatorymedications in the 24-hour period before and following theablation and accompanying contrast-enhanced CT.As a general principle, the smallest volume of low-
osmolar contrast medium required for a diagnostic study
is used. At our institution, multiphase abdominal andpelvic imaging with a single weight-determined contrastbolus is performed; patients weighing 45 kg or less receive80 mL of iodinated contrast, those weighing 46-60 kgreceive 100 mL, those weighing 61-90 kg receive 120 mL,and those weighing more than 90 kg receive 150 mL foroptimal opacification. These values should act as guide-lines only however, and less contrast should be used if it islikely to answer the clinical question.As in patients with normal renal function, periproce-
dural hydration is important when contrast administrationis planned in the setting of renal impairment. Wecommence the administration of isotonic IV fluid rehydra-tion (2-3 mL/kg/h of 0.9% normal saline or ringers lactate)from 1 hour before the ablation and reduce to 1 mL/kg/hfor 4 hours following the procedure. If the patient is athigh risk of CIN, overnight admission for IV hydration andserum creatinine and electrolyte monitoring may berequired. In our practice, patients with a serum creatinineof 1.7 or greater (or 1.3 or greater when the patient hasa single kidney or is a kidney transplant recipient) receivethe iso-osmolar agent iodixanol (Visipaque) in addition tothe IV hydration regimen.There is some evidence to support isotonic bicarbonate
in patients at high risk for CIN. A regimen involving anIV bolus of 3 mL/kg of isotonic bicarbonate administered1 hour before the procedure and continued at a rate of1 mL/kg for 6 hours after the procedure has beendescribed.30
There is conflicting evidence on the role of the anti-oxidant n-acetylcysteine (Mucomyst) in reducing contrast-related nephropathy. The risks of its use are low however,and given a potential benefit, its use may be considered ona case-by-case basis. Supportive studies advocate 600 mgadministered orally twice daily on the day before and theday of the procedure.31
Patients With a Known Adverse Reaction toIodinated ContrastWhen assessing prevalence of all adverse reactions tononionic iodinated contrast medium, Katayama et al

Preparation for percutaneous ablation procedures 215
described a rate of 3.13% but a much lower rate of severereactions (0.04%).32
As mentioned earlier, not all ablation patients requireiodinated contrast medium. In our practice, we do notroutinely perform contrast-enhanced imaging for bone orlung lesions. However, we do perform multiphase post-ablation CT imaging following liver and, sometimes, renalablation as outlined previously. In the presence of adocumented iodinated contrast allergy, the decision mustbe made if contrast is truly required. The identification ofintraperitoneal bleeding can often be made with non-contrast CT alone; however, detection of residual unab-lated tumor is not possible on noncontrast CT imaging andmay require gadolinium-enhanced MR imaging immedi-ately following the ablation.Acute nonrenal adverse reactions to iodinated contrast
are classified as mild (nausea, vomiting, pruritus, andurticaria), moderate (bronchospasm, vasovagal episode,severe vomiting, or urticaria) or severe (severe hypoten-sion, cardiac, or respiratory arrest).33
Patients with a history of mild or moderate contrastreactions can be managed with a steroid-based premed-ication regimen, as outlined in the American College ofRadiology guidelines (Table 6).34
Patients with a history of severe anaphylactic reactionsin whom iodinated contrast is required may require bothpremedication and elective airway protection in the formof an endotracheal tube if the use of IV contrast is deemedessential. As discussed in the American College of Radiol-ogy guidelines, studies have not shown a benefit fromsteroid premedication in patients with a history of severecontrast reactions.
Patients With Coagulopathy or onAnticoagulationCoagulopathy is not uncommon in patients referred forpercutaneous ablation and may be a consequence of
Table 6 American College of Radiology (ACR) Elective Pre-medication Guidelines for Patients with IV Contrast Aller-gies (ACRManual on Contrast Medium v9. ACRCommitteeon Drugs and Contrast Media. 2013 http://www.acr.org/Quality-Safety/Resources/Contrast-Manual)
Prednisone 50 mg PO13, 7, and 1 h Before contrastadministration
ORMethylprednisolone 32 mg PO
12 and 2 h Before contrast mediuminjection
ORHydrocortisone 200 mg IV
13, 7, and 1 h Before contrastadministration
Diphenhydramine 50 mg PO, IV or IM1 h Before contrast administration
PO, per oral; IM, intramuscularly.
underlying disease as in hepatic failure or may result fromanticoagulant medication administration. Optimizing thepatient’s coagulation status is critical in percutaneousprocedures as, in contrast with open surgical procedures,the operator is unable to directly visualize, identify, andtreat the site of bleeding and often must rely on imaging orchanges in patient parameters to recognize.As outlined in the SIR consensus guidelines, there is a
lack of randomized controlled studies or high-level evi-dence to provide firm guidelines and every case must bejudged individually.35 In this document, radio frequencyablation is classified as having a severe risk of bleeding(category III), and it recommends a target internationalnormalized ratio of r1.5 and platelet count greater than50,000. It should be stated that studies have failed to relateabnormal preprocedural coagulation parameters with sub-sequent bleeding complications following image-guidedinterventions.36 In addition, there is considerable contro-versy on the benefit of prophylactic administration of freshfrozen plasma in patients with elevated prothrombin timebefore invasive procedures of any kind, but especially inpatients with hepatic failure.37 The interventionalist mustweigh the risk of potential bleeding with the cost andcomplications (acute lung injury, anaphylaxis, volumeoverload, and blood-borne pathogens) of fresh frozenplasma and platelet transfusion.The management of patients on anticoagulant medica-
tion is complex and can vary greatly given the site ablation,patient comorbidities, and indication for anticoagulation.Following coronary artery stenting, dual-agent antiplateletmedication is routinely commenced in patients, andconsultation with the patient’s cardiologist is critical indeciding whether these medications can be discontinued.A summary of the updated SIR anticoagulant medicationguidelines for high-risk bleeding procedures (includingpercutaneous ablation) is provided (Table 7).38
As cancer is a risk factor for thromboembolic disease,many patients will be on warfarin-based anticoagulantregimens. In patients with a significant risk of throm-boembolic complications, periprocedural admission and“bridging” to an unfractionated heparin infusion or low-molecular-weight heparin regimen may be required.39
Nonsteroidal antiinflammatory drugs (NSAIDS) inhibitplatelet aggregation in a reversible fashion (unlike aspirinor clopidrogel, which irreversibly inhibit platelet function),so their effect is reversible with clearance of the drug. Ingeneral, NSAIDs are thought not to cause significantbleeding problems, except in those patients with a preex-isting coagulopathy. In addition, NSAIDS contribute torenal impairment and should be stopped 48 hours beforeplanned administration of iodinated contrast in at-riskpatients.
Patients With DiabetesDiabetes mellitus is increasing in prevalence globally and isa common comorbidity in patients undergoing percutane-ous tumor ablation.40 These patients present a challenge toboth the interventional radiologist and the anesthesiologist,

Table 7 SIR Consensus Guidelines on Periprocedural Management of Anticoagulant Medications for High-Risk procedures
Anticoagulant Class Recommendation for High-Risk Procedures
Warfarin Withhold for 5 d before procedureINR o 1.5
Aspirin Withhold for 5 d before procedure
Heparin AgentsUnfractionated Heparin Withhold 2-4 h before procedure; aPTT o1.5 baseline valueLow-Molecular-Weight Heparin(Therapeutic)
Withhold 2 doses or 24 h before procedure
Fondaparinux Withhold for 2-3 d if normal renal functionWithhold for 3-5 d if abnormal renal function
ThienopyridinesClopidogrel (Plavix) Withhold for 5 d before procedurePrasugrel (Effient)Ticlopidine (Ticlid) Withhold for 7 d before procedure
NSAIDSShort acting (half-life 2-6 h) Withhold for 24 h before procedureIbuprofenDiclofenacKetoprofenIndomethacin
Intermediate acting (half-life7-15 h)
Withhold for 2-3 d before procedure
NaproxenSulindacDiflunisalCelecoxib
Long acting (half-life 4-20 h) Withhold for 10 d before procedureMeloxicamNabumetonePiroxicam
Glycoprotein IIB/IIIA InhibitorsLong acting Withhold for 24 h before procedureAbciximab (ReoPro) aPTT o50 s
ACT o150 sShort acting Withhold for 4 h before procedureEptifibatide (Integrilin)Tirofiban (Aggrastat)
Direct Thrombin InhibitorsArgatroban Defer procedure until off medication if possible. If procedure is emergent, withhold 4 h
before procedureBivalirudin (Angiomax) Defer procedure until off medication if possible. If procedure is emergent, withhold 2-3 h
before procedure, if renal function is normal. Withhold 3-5 h before procedure if renalfunction is abnormal.
Dabigatran (Pradaxa) Defer procedure until off medication if possible. If procedure is urgent, withhold 2-3 dbefore procedure if normal renal function. Withhold 3-5 d before procedure if abnormalrenal function.
INR, international normalized ratio; aPTT, activated partial thromboplastin time.
I.M. Brennan, S. Faintuch, and M. Ahmed216
given the prevalence of serious diabetic complications, suchas ischemic heart disease, hypertension, renal impairment,stiff joint syndrome, and autonomic neuropathy. It isimportant to remember that a number of patients with type2 diabetes may be unaware of their diagnosis and may onlypresent during the periprocedural period.41 Subsequently,assessment of blood sugar should be incorporated into thepreoperative assessment.
Diabetic patients presenting for percutaneous tumorablation need preprocedural and intraprocedural optimi-zation of their glycemic control. A preprocedure assess-ment from their endocrinologist is usually of benefit andan assessment of the patient’s HbA1c titer gives anapproximation of recent glycemic control and patientcompliance with diet and exercise modifications. Oralhypoglycemic drugs are usually withheld on the day of

Preparation for percutaneous ablation procedures 217
the procedure and up to 48 hours preoperatively forlonger-acting drugs such as chlorpropamide to avoidreactive hypoglycemia and drug interactions.42 It shouldbe recognized that the use of metformin is not a risk factorfor CIN, but its use in the presence of renal dysfunctionmay lead to development of lactic acidosis in the event ofacute renal failure.43 In our practice, we withhold metfor-min for 48 hours before planned iodinated contrastadministration in patients with a glomerular filtration rateof less 60 mL/min. Patients with type 2 diabetes and moresevere hypoglycemia may require conversion to insulintherapy during the perioperative period.Overall, tight glycemic control in perioperative and
critical care patients has been shown to decrease compli-cations and improve survival.44,45 Diabetic patients havea known increased risk of perioperative infection, althoughthere is a paucity of data on infectious complicationsfollowing percutaneous tumor ablation.46 Despite the lackof data, antibiotic prophylaxis should be considered in thisat-risk patient group. Overall, the interventionalist shouldhave a low threshold for the use of MAC and periproce-dural admission for poorly controlled or long-standingdiabetic patients.
Management of Other OutpatientMedicationsA detailed discussion on the perioperative management ofa broad spectrum of medications is beyond the scope ofthis article; however, the general principles can be out-lined. It is advisable to continue medications with anywithdrawal potential (selective serotonin reuptake inhib-itors, β-blockers, clonidine, statins, and corticosteroids).47
Patients should be advised to take their routine medi-cations with a small amount (less than 150 mL) of wateron the day of the procedure. This is especially importantfor chronic narcotic analgesic medications. Whether totake antihypertensive, angiotensin-converting-enzymeinhibitor, or diuretic medications on the morning of theprocedure is controversial with no good data to support orrefute the practice.48 In general, it is probably safe toadminister these medications. However, changes in elec-trolytes can occur with diuretic therapy and the combina-tion of antihypertensive medications and generalanesthesia can result in hypotension. In such cases, adiscussion with the anesthesiologist is advisable.
Planning Postablation Follow-up CarePatients require close postablative follow-up to ensure thebest possible clinical care, allow for the early detection ofpotential procedural complications, and for evaluation oftreatment efficacy. Patients should be provided withinformation on how to easily contact practice representa-tives (either physicians or an answering service) bothduring daytime hours and for after-hour emergencies. Aplan for postprocedural follow-up after discharge should
be established, and may include a phone call or short-termclinic visit. Short-interval follow-up imaging should ideallybe scheduled before the procedure or on discharge.Although imaging follow-up regimens are often tumor-type specific, in our practice, we obtain a 1-month imagingstudy in most cases to allow early identification of patientswho may have residual untreated tumor and need addi-tional treatment. For patients who are undergoing ablationfor symptomatic relief (such as an osteoid osteoma or anadrenal aldosteronoma), follow-up evaluation with appro-priate clinical and laboratory evaluation may suffice.
ConclusionTime invested in careful preprocedural planning andpatient preparation greatly increases the likelihood of asafe and effective percutaneous ablation procedure. Theclinic visit is critical in assessing and clarifying patientexpectations as well as obtaining a fully informed consent.The decision on whether to perform the procedure
using nonanesthesiologist-delivered moderate sedation orto use MAC or general anesthesia depends on a multitudeof factors and should be treated on a case-by-case basis.Patients with coagulopathy, diabetes, and renal impair-ment require close supervision and may benefit fromsubspecialist opinion and periprocedural hospital admis-sion. Planning for follow-up care before performing theprocedure provides patients with seamless periproceduralcare.47,48
References1. Sims MJ, Rilling WS: Psychosocial management of distress in
interventional radiology patients with cancer. Tech Vasc IntervRadiol 9:101-105, 2006 [Review]
2. Tuite CM, Sun W, Soulen MC: General assessment of the patientwith cancer for the interventional oncologist. J Vasc Interv Radiol17:753-758, 2006 [Review]
3. Chen CCH, Kenefick AL, Tang ST, et al: Utilization of comprehen-sive geriatric assessment in cancer patients. Crit Rev Oncol Hematol29:53-67, 2004
4. Georgiades CS, Hong K, Geschwind JF: Pre- and postoperativeclinical care of patients undergoing interventional oncology proce-dures: A comprehensive approach to preventing and mitigatingcomplications. Tech Vasc Interv Radiol 9:113-124, 2006 [Review]
5. Oken MM, Creech RH, Tormey DC, et al: Toxicity and responsecriteria of the Eastern Cooperative Oncology Group. Am J ClinOncol 5:649-655, 1982
6. Karnofsky DA, Burchenal JH: The clinical evaluation of chemo-therapeutic agents in cancer. in MacLeod CM (ed.), Evaluation ofChemotherapeutic Agents. New York, NY: Columbia Univ Press,196, 1949
7. Buccheri G, Ferrigno D, Tamburini M: Karnofsky and ECOGperformance status scoring in lung cancer: A prospective, longitu-dinal study of 536 patients from a single institution. Eur J Cancer32A:1135-1141, 1996
8. Mallampati SR, Gatt SP, Gugino LD, et al: A clinical sign to predictdifficult tracheal intubation: A prospective study. Can Anaesth Soc J32:429-434, 1985 [PubMed PMID: 4027773]
9. Sharma A, Moore WH, Lanuti M, et al: How I do it: Radiofrequencyablation and cryoablation of lung tumors. J Thorac Imaging26:162-174, 2011. http://dx.doi.org/10.1097/RTI.0b013e3182171b75 [Review]

I.M. Brennan, S. Faintuch, and M. Ahmed218
10. Breitbart W: Psychiatric management of cancer pain. Cancer 63:2336-2342, 1989
11. Pugh RN, Murray-Lyon IM, Dawson JL, et al: Transection of theoesophagus for bleeding oesophageal varices. Br J Surg 60:646-649,1973
12. Kamath PS, Kim WR: Advanced Liver Disease Study Group; Themodel for end-stage liver disease (MELD). Hepatology 45:797-805,2007 [Review]
13. Testa R, Testa E, Giannini EG, et al: Trans-catheter arterial chemo-embolization for hepatocellular carcinoma in patients with viralcirrhosis: Role of combined staging systems, Cancer Liver ItalianProgram (CLIP) and Model for End-stage Liver Disease (MELD), inpredicting outcome after treatment. Aliment Pharmacol Ther17:1563-1569, 2003
14. Davies L, Laasch H-U, Wilbraham L, et al: The consent process inInterventional radiology: The role of specialist nurses. Clin Radiol59:246-252, 2004
15. Henry F: Uterine artery embolization for symptomatic uterinefibromas. Informed consent of the patient. J Radiol 82:111-115,2001
16. Mavroforou A, Giannoukas A, Mavrophoros D, et al: Physicians’liability in interventional radiology and endovascular therapy. Eur JRadiol 46:240-243, 2003 [Review]
17. Gann R: The therapeutic partnership: Legal and ethical aspects ofconsumer health information. Health Libr Rev 12:83-90, 1995
18. Choi D, Lim HK, Kim SH, et al: Assessment of therapeutic responsein hepatocellular carcinoma treated with percutaneous radio fre-quency ablation: Comparison of multiphase helical computedtomography and power Doppler ultrasonography with a micro-bubble contrast agent. J Ultrasound Med 21:391-401, 2002
19. Rempp H, Waibel L, Hoffmann R, et al: MR-guided radiofrequencyablation using a wide-bore 1.5-T MR system: Clinical results of 213treated liver lesions. Eur Radiol 22:1972-1982, 2012
20. Cheung Ning M, Karmakar MK: Right thoracic paravertebralanaesthesia for percutaneous radiofrequency ablation of livertumours. Br J Radiol 84:785-789, 2011. http://dx.doi.org/10.1259/bjr/28983063 [Epub 2010 Nov 16]
21. Vainio A, Auvinen A, Ahmedzai S, et al: Prevalence of symptomsamong patients with advanced cancer: An international collaborativestudy. J Pain Symptom Manage 12:3-10, 1996
22. Rosenow EC III, Limper AH: Drug-induced pulmonary disease.Semin Respir Infect 10:86-95, 1995
23. Tatli S, Morrison PR, Tuncali K, et al: Interventional MRI foroncologic applications. Tech Vasc Interv Radiol 10:159-170, 2007[Review]
24. Schupp CJ, Berbaum K, Berbaum M, et al: Pain and anxiety duringinterventional radiologic procedures: Effect of patients’ state anxietyat baseline and modulation by nonpharmacologic analgesia adjuncts.J Vasc Inter Radiol 16:1585-1592, 2005
25. Dupuy DE, Goldberg SN: Image-guided radiofrequency tumorablation: Challenges and opportunities—Part II. J Vasc Interv Radiol12:1135-1148, 2001 [Review]
26. de Baere T, Roche A, Amenabar JM, et al: Liver abscess formationafter local treatment of liver tumors. Hepatology 23:1436-1440,1996
27. Venkatesan AM, Kundu S, Sacks D, et al: Practice guidelines foradult antibiotic prophylaxis during vascular and interventionalradiology procedures. Written by the Standards of Practice Com-mittee for the Society of Interventional Radiology and Endorsed bythe Cardiovascular Interventional Radiological Society of Europe andCanadian Interventional Radiology Association [corrected], J VascInterv Radiol 21:1611-1630, 2010. http://dx.doi.org/10.1016/j.jvir.2010.07.018 [quiz 1631. Review. Erratum in: J Vasc IntervRadiol. 2011 Feb;22(2):263. PubMed PMID: 21029949]
28. Al-Ghonaim M, Pannu N: Prevention and treatment of contrast-induced nephropathy. Tech Vasc Interv Radiol 9:42-49, 2006[Review]
29. Parfrey PS, Griffiths SM, Barrett BJ, et al: Contrast material-inducedrenal failure in patients with diabetes mellitus, renal insufficiency, orboth. A prospective controlled study. N Engl J Med 320:143-149,1989
30. Pannu N, Wiebe N, Tonelli M: Alberta Kidney Disease Network:Prophylaxis strategies for contrast-induced nephropathy. J Am MedAssoc 295:2765-2779, 2006
31. Thornton K: Postprocedure clinical management for the interven-tional radiologist. Tech Vasc Interv Radiol 9:106-112, 2006 [Review.PubMed PMID: 17561213]
32. Katayama H, Yamaguchi K, Kozuka T, et al: Adverse reactions toionic and nonionic contrast media. Radiology 175:270-276, 1990
33. Thomsen HS: Contrast media safety—An update. Eur J Radiol80:77-82, 2011
34. ACR Committee on Drugs and Contrast Media. ACR Manual onContrast Media, Version 9, 8-9, 2013
35. Patel IJ, Davidson JC, Nikolic B, et al: Consensus guidelines forperiprocedural management of coagulation status and hemostasisrisk in percutaneous image-guided interventions. J Vasc IntervRadiol 23:727-736, 2012
36. Segal JB, Dzik WH: Transfusion Medicine/Hemostasis Clinical TrialsNetwork. Paucity of studies to support that abnormal coagulationtest results predict bleeding in the setting of invasive procedures: Anevidence-based review. Transfusion 45:1413-1425, 2005
37. Stanworth SJ, Brunskill SJ, Hyde CJ, et al: Is fresh frozen plasmaclinically effective? A systematic review of randomized controlledtrials. Br J Haematol 126:1139, 2004
38. Patel IJ, Davidson JC, Nikolic B, et al: Addendum of neweranticoagulants to the SIR Consensus Guideline. J Vasc Interv Radiol24:641-645, 2013. http://dx.doi.org/10.1016/j.jvir.2012.12.007
39. Ansell J, Hirsh J, Poller L, et al: The pharmacology and managementof the vitamin K antagonists: The Seventh ACCP Conference onAntithrombotic and Thrombolytic Therapy. Chest 126:204S-233S,2004 (suppl 3)
40. Robertshaw HJ, Hall GM: Diabetes mellitus: Anaesthetic manage-ment. Anaesthesia 61:1187-1190, 2006
41. Lauruschkat AH, Arnrich B, Albert AA, et al: Prevalence and risks ofundiagnosed diabetes mellitus in patients undergoing coronaryartery bypass grafting. Circulation 112:2397-2402, 2005
42. Kadoi Y: Anesthetic considerations in diabetic patients. Part II:Intraoperative and postoperative management of patients withdiabetes mellitus. J Anesth 24:748-756, 2010
43. Thomsen HS, Morcos SK: Contrast media and metformin: guidelinesto diminish the risk of lactic acidosis in non-insulin-dependentdiabetics after administration of contrast media. ESUR ContrastMedia Safety Committee. Eur Radiol 9:738-740, 1999
44. Van den Berghe G, Wouters P, Weekers F, et al: Intensive insulintherapy in critically ill patients. N Engl J Med 345:1359-1367, 2001
45. Lazar HL, Chipkin SR, Fitzerald CA, et al: Tight glycemic control indiabetic coronary artery bypass graft patients improves perioperativeoutcomes and decreases recurrent ischemic events. Circulation109:1497-1502, 2004
46. Peleg AY, Weerarathna T, McCarthy JS: Common infections indiabetes: Pathogenesis, management and relationship to glycemiccontrol. Diabetes Metab Res Rev 23:3-13, 2007
47. Papadopoulos S, Cook AM: You can withdraw from that? The effects ofabrupt discontinuation of medications. Orthopedics 29:413-417, 2006
48. Whinney C: Perioperative medication management: General princi-ples and practical applications. Cleve Clin J Med 76:S126-S132,2009 (suppl 4). http://dx.doi.org/10.3949/ccjm.76.s4.20 [Review]












![Percutaneous image-guided ablation of bone and soft tissue ... · oid osteoma [23, 24]. Ever since, for the therapy of this benign tumour, thermal ablation constitutes a first-line](https://static.fdocuments.in/doc/165x107/5cbf758888c9932c128b8add/percutaneous-image-guided-ablation-of-bone-and-soft-tissue-oid-osteoma-23.jpg)