Preoperative Assessment Decision Support S Lake, B Murthy*, A Fisher Department of Clinical...
23
Preoperative Assessment Decision Support S Lake, B Murthy*, A Fisher Department of Clinical Engineering * Department of Anaesthesia & Theatres
-
Upload
roberta-oliver -
Category
Documents
-
view
216 -
download
0
Transcript of Preoperative Assessment Decision Support S Lake, B Murthy*, A Fisher Department of Clinical...

Preoperative Assessment Decision Support
S Lake, B Murthy*, A FisherDepartment of Clinical Engineering
* Department of Anaesthesia & Theatres

The Journey BEFORE Pre-op
Patient seen by G.P Referred to / seen by surgeon
Lists the patient for an operationGoes on waiting List
Secretary/Clerk sends for the patient (appointment letter)
Patient comes to the hospital the day before or on the day of the operation
Investigations done
Examined by Anaesthetist
Unfit for surgery (D.M, ↑BP) Fit for surgery
Refer back to G.P Goes to operating theatre

Source of all day case cancellations. Aug 01 - Jun 02
Hospital clinical8% (986)
Hospital non-clinical
24% (2980)
Patient68% (8309)

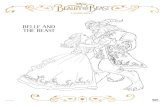
Reasons for day case cancellations on the day & the day before surgery
Aug 01 - Jun 02
23%
(96
6)
19%
(80
3)
12%
(49
9)
8% (
337)
6% (
246)
5% (
234)
5% (
224)
5% (
222)
4% (
187)
4% (
163)
2% (
81)
2% (
79)
1% (
62)
1% (
61)
1% (
49)
1% (
34)
0.4%
(19
)
0
100
200
300
400
500
600
700
800
900
1000
1100
DN
A
Unf
it fo
r su
rger
y (p
atie
ntca
ncel
latio
n)
App
oint
men
t in
conv
enie
nt
Ope
ratio
n no
t re
quire
d(p
atie
nt c
ance
llatio
n)
Unf
it du
e to
acu
te il
lnes
s(h
ospi
tal c
ance
llatio
n)
Sur
geon
una
vaila
ble
War
d be
ds u
nava
ilabl
e
Ope
ratio
n no
t ne
cess
ary
(hos
pita
l can
cella
tion)
Em
erge
ncie
s /
trau
ma
List
ove
rrun
Adm
inis
trat
ive
erro
r
Equ
ipm
ent
failu
re/u
nava
ilabl
e
Ana
esth
etis
t un
avai
labl
e
Pre
exi
stin
g m
edic
alco
nditi
on
Uns
uita
ble
for
day
surg
ery
Pre
-ope
rativ
e gu
idan
ce n
otfo
llow
ed
The
atre
sta
ff un
avai
labl
e
Reason for cancellation
Nu
mb
er
of
ca
nc
ella
tio
ns
Reasons for day case cancellations on the day & the day before surgery.
Aug 01 – Jun 02

The Patient’s Journey Now Patient seen by G.P Refer to/seen by surgeon
Lists the patient for operation
Goes on waiting ListPre-op assessment 4 weeks before
surgery, and investigations
Unfit for surgery Fit for surgery
Patient comes to the hospital on the day of
surgery
Goes to theatre Discharge
Refer back to G.P Seen by Anaesthetist
in the clinic
Referred to Specialist (e.g Cardiologist)
Listed for operation once fit for surgery

Electronic Pre-operative Assessment Pathway
• Mile stone
• Intranet based
• Present Pathways
• Greater Accessibility, Accuracy and
• Completeness of clinical information

OSCAR(Optimised Surgery Care and Anaesthesia Record)
Intranet based recording system of: -• Pre-operative anaesthetic assessment, medication
and scoring.• Complete peri-operative anaesthetic chart
including vital signs.• Post-operative monitoring, medication etc...
Now includes: Pre-admission assessment.

Decision Support
• Must predict investigations and provide advice based on: -– Details from patient history– Details about the operation– Local policies & guidelines

Patient History
• What does the prediction routine have to work with: -
– The patient suffers from occasional, constant, infrequent headaches.
– Patient has chest pain if she lies on her left side for over a year.
– Skin: somewhat pale but present.
– She stated that she had been constipated for most of her life until 1989 when she got a divorce.
Richard Lederer’s list taken from “The Bride of Anguished English (2000)” where entries were described as real-life doctors’ dictations submitted by the American Association of Medical Transcriptionists.

Pre-operative and anaesthetic assessmentBase Line Observations Temp
Weight(kg) Height(m) BMI (kgm-2) Urinalysis
BP Pulse Respirations Skin integrity
Patient Health Questionnaire
General health Good Poor Elaborate as necessary
Nutrition problem or weight change No Yes
Medication eg –HRT, Oral Contraceptive, Anti-coagulants or steroids (including non prescription drugs)
No Yes Identify on page 4. If HRT or Oral Contraceptive inform medical staff before admission.
Previous steroid therapy No Yes When? Identify on page 4
Have you had an operation or anaesthetic before?
No Yes
Did you/your relatives have any problems associated with the anaesthetic?
No Yes Refer below
Do you smoke? No Yes Amount
Do you drink alcohol? No Yes Units per week
Do you have high blood pressure? No Yes
Do you have any heart problems? No Yes Angina Heart attacks Heart murmur
Palpitations Fainting attacks/ blackouts
Do you have any chest problems? No Yes Asthma Bronchitis Emphysema
Any other problems
………………… “ ……………………….. … “ ….. … “ .. …………………… “ …………………………

Guidelines for Pre-operative InvestigationsTEST INDICATION
FBC •All patients over 60 years and all menstruating females
•Patients undergoing major surgery with likelihood of significant peri-operative blood loss.
•H/O blood loss (acute or chronic), anaemia, renal disease, disseminated malignancy, malnutrition.
•Patients likely to have regional anaesthesia.
Coagulation screen •Patient taking anticoagulants
•Patients with bleeding disorder or chronic hepatobiliary disease or on haemodialysis
•Patients likely to have regional anaesthesia
•Consumption >21 units alcohol / week.
U&E •H/O cardiovascular disease or renal or hepatic impairment or malignancy.
•Any cardiovascular drugs including diuretics.
•Diabetes, asthmatics on inhalers, patients on steroids.
•All patients over 50 years and in all patients undergoing major surgery
Glucose •All diabetic patients. In patients undergoing peripheral vascular surgery or pancreatic surgery or liver surgery.
•In obese patients and patients taking steroids.
HbA1C •All diabetic patients
LFTs •Any patient undergoing major abdominal surgery.
•H/O malignancy or chronic liver disease or jaundice or cardiac failure
•Consumption >21 units alcohol / week.
………. “ …………… ………………………………… “ ………………………………………………
Arterial blood gases Patients with known respiratory disease who are listed for major surgery like thoracic surgery or oesophageal surgery.

Association• Would the program know that asthma in the
patient history is a respiratory disease, indicated in the guidelines for investigations.
• Or can we predict all occurrences of this now so it can be programmed in.

Solution1. Introduce an intermediary, ‘Fact Code’, that can
be attributed to a patient and used with the guidelines to predict the investigation.
– E.g. Has asthma or On Steroids
2. Three levels of action if fact code present: -• Recommend test : direct evidence in history
• Suggest test : indirect evidence in history
• Advice : Not a test but administration – e.g. put patient first on list due to allergy.

Next problem• Anaesthetist wrote guidelines but Pre-op nurses
carry them out. Guidelines need to evolve.
• Surgeons have ‘likes’
• Flexible way to adjust prediction algorithm– Defined by rules in a database– Template used to specify questions for history
taking and which rules to apply.

Database Structure

Rule Structure• Each assessment can have one or more rules
• Rule trigger: -
Applicable age range
Level of surgery, minor, intermediate, major, major+
Specific operation procedure codes
Type of anaesthetic: GA, LA
Physiological measurement range (Fact Code), e.g. BMI >= 30
Medication (Fact Code), e.g. thyroxine
Condition (Fact Code), e.g. asthma
• Rule output: -
Action: Recommend, Suggest, Advise only
Investigation to trigger
Patient information

Rule Application

Pre-Admission Assessment


Management list
Shows which assessments are still waiting for test results. Those past the pre-assigned panic date turn red

Anaesthetic Assessment

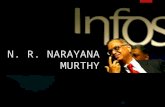
Communications
Web Server
Web Browser
(Internet Explorer)
ProgramsWeb Pages
Other systems
Web Page / Scripts
SOAP call (W3C standard)
By splitting the layout of the web page from the programming we can have different web pages calling the same program and even have other systems call the same program without the results being buried inside the web page source.
Database

Benefits
• Encourages a consistent approach to pre-operative assessment.
• Quality of record.• May flag up tests missed by the Nurse.• Highlights missing test results before it becomes a problem.• Anaesthetist is better informed.
• A catalyst to improvement by providing a focus on: -
Optimising Surgery Care