

PREMERA BLUE CROSS Medicare AdvantageGym membership Silver&Fit Over the counter (OTC) benefit $50...
69
© 2019 Premera Blue Cross 2020 GUIDE FOR PRODUCERS PREMERA BLUE CROSS Medicare Advantage 1
Transcript of PREMERA BLUE CROSS Medicare AdvantageGym membership Silver&Fit Over the counter (OTC) benefit $50...

© 2019 Premera Blue Cross
2020 GUIDE FOR PRODUCERS
PREMERA BLUE CROSS
Medicare Advantage
1

What’s new or improved
3NEW COUNTIES –
12 TOTAL
1FORMULARY
IMPROVED
HEARING BENEFIT
10PLANS
“ENHANCED PLAN” IN EVERY COUNTY
2

Service area:• 3 new counties• 12 total

CurrentWhatcomSkagitSnohomishKing Pierce ThurstonLewisSpokaneStevens
County ExpansionSan Juan
IslandStevens
Walla Walla
Spokane
King
Snohomish
Skagit
Whatcom
PierceThurston
Lewis
New for 2020IslandSan JuanWalla Walla
4

Plan overview• 10 total plans• “Enhanced plan” in every county

Overview of Premera HMO plansENHANCED ENHANCED ENHANCED
Plan Benefits HMOPeak + Rx
Core HMO
Total Health
Sound + Rx
Alpine ClassicCore Plus
NEWCharter +
RxClassic
Plus
DentalOptional
Dental RiderOptional
Dental RiderOptional
Dental RiderEmbedded
DentalEmbedded
DentalNot
AvailableEmbedded
DentalEmbedded
DentalEmbedded
DentalEmbedded
Dental
Premium $0 $0 $12 $24 $40 $42 $55 $75 $150 $190
King, Pierce, Snohomish, Thurston X X X X X X XLewis X XIsland, San Juan, Walla Walla NEW XSkagit X XWhatcom X X X X NEW XSpokane X XStevens X
6

Enhanced plans• One available in each county: Total
Health, Classic, or Core Plus• Offer enhanced medical and pharmacy
benefits

Routine chiropractic and podiatry (6 per year)
Max out-of-pocket
lowered to $5,000 per year
Hearing aids covered in full
through Hearing Care
Solutions (up to $1,000 per ear)
Additional dental services
allowance of $200 per year
Copays reduced to
• $5 for PCP• $20 for
OT/PT• $30 for
specialist visits
“Enhanced plans” – Enhanced medical benefitsTotal Health, Classic, and Core Plus
8

“Enhanced plans” – Enhanced pharmacy benefitsTotal Health, Classic, and Core Plus
Over the counter benefit (per quarter)
Rx deductible(Tiers 1–3)
for 90 days (Tier 1 through mail order)
$50 WAIVED $0 COPAY
9

3 things to know about all Premera plans

Inpatient hospitalcopays apply
once during any admit within the
60-day period
Gym membershipas low as $0
premium or a plan with more
extensive benefits
3
Coverage for worldwide
emergencies or urgent care
21
All Premera plans include:
11

• Now available in Whatcom county• Premium remained the same - $55• Reduced max out of pocket to $5,000• Decreased PCP copay to $5• Decreased specialist copay to $30• Reduced occupational and physical
therapy copay to $20• Added “Additional dental services”
coverage of $200/year• Added OTC benefit of $50/quarter• Added hearing aid benefit• Added routine chiropractic and
podiatry• Diabetic supplies – lower coinsurance
Classic HMO: HighlightsKing, Lewis, Pierce, Snohomish, Thurston and Whatcom counties
PHARMACY• Deductible lowered and only on tiers
4 and 5• Copays lowered on tiers 1-4• $0 copay for 90-day mail order fill
on tier 1 drugs

Plan Benefits 2019 2020
Monthly plan premium $55 $55
Medical deductible $0 $0
Annual out-of-pocket maximum $5,600 $5,000
Primary care provider visit $10 copay $5 copay
Specialist visit $40 copay $30 copay
Occupational/physical therapy $40 copay $20 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5+) $450 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center $250 copay $250 copay
Outpatient hospital center $350 copay $350 copay
Ambulance $300 copay each way $300 copay each way
Worldwide emergency care $75 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $50 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $10 copay $10 copay
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
Classic HMOKing, Lewis, Pierce, Snohomish, Thurston and Whatcom counties
13

Classic HMO
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $150 per calendar year $150 per calendar year
Dental Included Included
Additional dental services Not covered $200
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50 per quarter
Routine hearing exam $40/1 per year $0–$30/1 per year
Hearing aids with Hearing Care Solutions
Not covered $1,000 per ear each year
Routine chiropractic Not covered $30 copay/6 per year
Routine podiatry Not covered $30 copay/6 per year
Diabetic supplies 20% coinsurance 10% coinsurance
24-Hour NurseLine Included Included
NEW
NEW
NEW
14
NEW
NEW

Classic HMO
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $200 on tiers 3-5 $180 on tiers 4-5
Tier 1 – Preferred generic$3 copay/$0 deductible
*$6 for 90-day mail order$2 copay/$0 deductible
*$0 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $10 copay/$0 deductible
Tier 3 – Preferred brand $42 copay $40 copay/$0 deductible
Tier 4 – Non-preferred drug 35% coinsurance 33% coinsurance
Tier 5 – Specialty 29% coinsurance 29% coinsurance
15
• New plan, same as Classic HMO and Total Health HMO
Core Plus HMO: HighlightsIsland, San Juan, Walla Walla, and Skagit counties

Plan Benefits 2020
Monthly plan premium $75
Medical deductible $0
Annual out-of-pocket maximum $5,000
Primary care provider visit $5 copay
Specialist visit $30 copay
Occupational/physical therapy $20 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center $250 copay
Outpatient hospital center $350 copay
Ambulance $300 copay each way
Worldwide emergency care $90 copay (waived if admitted)
Worldwide urgent care $50 copay (waived if admitted)
Lab services/x-rays $10 copay
Preventive care $0 copay
Annual physical exam Covered in full 1 per year
Core Plus HMOIsland, San Juan, Walla Walla, and Skagit counties
NEW
17

Core Plus HMO
Plan Benefits 2020
Annual routine eye exam $20 copay/1 per year
Vision hardware allowance $150 per calendar year
Dental Included
Additional dental services $200
Gym membership Silver&Fit
Over the counter (OTC) benefit $50 per quarter
Routine hearing exam $0 – $30/1 per year
Hearing aids with Hearing Care Solutions $1,000 per ear each year
Routine chiropractic $30 copay/6 per year
Routine podiatry $30 copay/6 per year
Diabetic supplies 10% coinsurance
24-Hour NurseLine Included
NEW
18

Prescription 2020
30-day supply from a preferred network pharmacy
Drug deductible $180 on tiers 4-5
Tier 1 – Preferred generic$2 copay/$0 deductible
*$0 for 90-day mail order
Tier 2 – Generic $10 copay/$0 deductible
Tier 3 – Preferred brand $40 copay/$0 deductible
Tier 4 – Non-preferred drug 33% coinsurance
Tier 5 – Specialty 29% coinsurance
NEWCore Plus HMO
19

• Premium remained the same - $24• Max out of pocket reduced to $5,000• Specialist copay dropped to $30• OT/PT reduced to $20• ASC and outpatient are now copays• Ambulance is now a copay• Labs and x-rays lowered• Added “Additional dental services”
coverage of $200/year• Added OTC benefit of $50/quarter• Added hearing aid benefit• Added routine chiropractic and podiatry• Diabetic supplies – lower coinsurance
Total Health HMO: HighlightsSpokane and Stevens counties
PHARMACY• Deductible lowered and only on tiers
4 and 5• Copays lowered on tiers 1-4• $0 copay for 90-day mail order fill
on tier 1 drugs

Total Health HMO
Plan Benefits 2019 2020
Monthly plan premium $24 $24
Medical deductible $0 $0
Annual out-of-pocket maximum $5,500 $5,000
Primary care provider visit $5 copay $5 copay
Specialist visit $45 copay $30 copay
Occupational/physical therapy $40 copay $20 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5+) $450 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center 15% coinsurance $250 copay
Outpatient hospital center 20% coinsurance $350 copay
Ambulance $300 copay each way $300 copay each way
Worldwide emergency care $75 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $50 copay $50 copay (waived if admitted)
Lab services/x-rays $20 copay $10 copay
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
Spokane and Stevens counties
21

Total Health HMO
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $150 per calendar year $150 per calendar year
Dental Included Included
Additional dental services Not covered $200
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50/quarter
Routine hearing exam $40/1 per year $0-$30/1 per year
Hearing aids with Hearing Care Solutions
Not covered $1,000 per ear each year
Routine chiropractic Not covered $30 copay/6 per year
Routine podiatry Not covered $30 copay/6 per year
Diabetic supplies 20% coinsurance 10% coinsurance
24-Hour NurseLine Included Included
NEW
NEW
NEW
22
NEW
NEW

Total Health HMO
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $180 on tiers 3-5 $180 on tiers 4-5
Tier 1 – Preferred generic$2 copay/$0 deductible
*$4 for 90-day mail order$2 copay/$0 deductible
*$0 for 90-day mail order
Tier 2 – Generic $10 copay/$0 deductible $10 copay/$0 deductible
Tier 3 – Preferred brand $42 copay $40 copay/$0 deductible
Tier 4 – Non-preferred drug 35% coinsurance 33% coinsurance
Tier 5 – Specialty 29% coinsurance 29% coinsurance
23

• Lowered coinsurance on diabetic supplies
HMO: HighlightsKing, Pierce, Snohomish, Thurston, Lewis and Spokane counties

HMO
Plan Benefits 2019 2020
Monthly plan premium $0 $0
Medical deductible $0 $0
Annual out-of-pocket maximum $6,300 $6,300
Primary care provider visit $15 copay $15 copay
Specialist visit $45 copay $45 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5-90+) $450 copay (days 1–4)/$0 copay (days 5-90+)
Ambulatory surgical center 15% coinsurance 15% coinsurance
Outpatient hospital center 20% coinsurance 20% coinsurance
Ambulance $300 copay each way $300 copay each way
Worldwide emergency care $75 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $50 copay $50 copay (waived if admitted)
Lab services/x-rays $20 copay $20 copay
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
King, Pierce, Snohomish, Thurston, Lewis and Spokane counties
25

HMO
Plan Benefits 2019 2020
Annual routine eye exam $45 copay $45 copay
Vision hardware allowance Not covered Not covered
Dental Optional $26 rider Optional $26 rider
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered Not covered
Routine hearing exam Not covered Not covered
Hearing aids with Hearing Care Solutions
Not covered Not covered
Routine chiropractic Not covered Not covered
Routine podiatry Not covered Not covered
Diabetic supplies 20% coinsurance 10% coinsurance
24-Hour NurseLine Included Included
26

HMO
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $300 on tiers 3-5 $300 on tiers 3-5
Tier 1 – Preferred generic$4 copay/$0 deductible
*$8 for 90-day mail order$4 copay/$0 deductible
*$8 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $42 copay $42 copay
Tier 4 – Non-preferred drug 35% coinsurance 33% coinsurance
Tier 5 – Specialty 27% coinsurance 27% coinsurance
27

• Lowered copay on worldwide urgent care• Vision hardware improved, no copay, and
now available annually• Dental benefits now available as additional
rider• OTC benefit - $50/quarter• 24-Hour NurseLine now included
Peak + Rx (HMO): HighlightsKing, Pierce, Snohomish, Thurston and Whatcom counties
PHARMACY• Lowered copay on tier 1 mail order• Lowered copays on tiers 2-4

Plan Benefits 2019 2020
Monthly plan premium $0 $0
Medical deductible $0 $0
Annual out-of-pocket maximum $6,700 $6,700
Primary care provider visit $15 copay $15 copay
Specialist visit $50 copay $50 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $595 copay (days 1–3)/$0 copay (days 4+) $595 copay (days 1–3)/$0 copay (days 4+)
Ambulatory surgical center $395 copay $395 copay
Outpatient hospital center 20% coinsurance 20% coinsurance
Ambulance $280 copay/each way $280 copay/each way
Worldwide emergency care $80 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $80 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $15 copay labs/$20 copay x-rays $15 copay labs/$20 copay x-rays
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
Peak + Rx (HMO)King, Pierce, Snohomish, Thurston and Whatcom counties
29

Peak + Rx (HMO)
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $30 copay/$120 allowance/2 years $150 per calendar year
Dental Not covered Optional $26 rider
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50 per quarter
Routine hearing exam $0-$50 $0-$50
Hearing aids with Hearing Care Solutions
$1,000 per ear each year $1,000 per ear each year
Routine chiropractic Not covered Not covered
Routine podiatry $50 copay/6 per year $50 copay/6 per year
Diabetic supplies 0% coinsurance 10% coinsurance
24-Hour NurseLine Not covered Included
NEW
30
NEW

Peak + Rx (HMO)
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $160 on tiers 3-5 $160 on tiers 3-5
Tier 1 – Preferred generic$3 copay/$0 deductible*$7.50 for 90-day mail
$3 copay/$0 deductible*$6 for 90-day mail order
Tier 2 – Generic $14 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $47 copay $42 copay
Tier 4 – Non-preferred drug 50% coinsurance 33% coinsurance
Tier 5 – Specialty 30% coinsurance 30% coinsurance
31

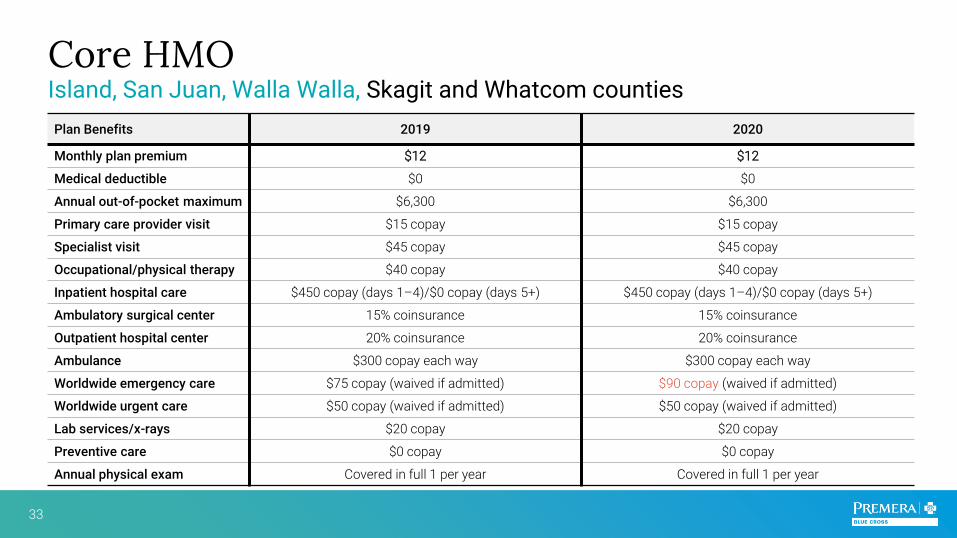
• Now available in Island, San Juan and Walla Walla counties
• Lowered copay on diabetic supplies
Core HMO: HighlightsIsland, San Juan, Walla Walla, Skagit and Whatcom counties
Core HMO
Plan Benefits 2019 2020
Monthly plan premium $12 $12
Medical deductible $0 $0
Annual out-of-pocket maximum $6,300 $6,300
Primary care provider visit $15 copay $15 copay
Specialist visit $45 copay $45 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5+) $450 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center 15% coinsurance 15% coinsurance
Outpatient hospital center 20% coinsurance 20% coinsurance
Ambulance $300 copay each way $300 copay each way
Worldwide emergency care $75 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $50 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $20 copay $20 copay
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
Island, San Juan, Walla Walla, Skagit and Whatcom counties
33

Core HMO
Plan Benefits 2019 2020
Annual routine eye exam $45 copay $45 copay
Vision hardware allowance Not covered Not covered
Dental Optional $26 rider Optional $26 rider
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit
Not covered Not covered
Routine hearing exam Not covered Not covered
Hearing aids with Hearing Care Solutions
Not covered Not covered
Routine chiropractic Not covered Not covered
Routine podiatry Not covered Not covered
Diabetic supplies 20% coinsurance 10% coinsurance
24-Hour NurseLine Included Included
34

Core HMO
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $300 on tiers 3-5 $300 on tiers 3-5
Tier 1 – Preferred generic$4 copay/$0 deductible
*$8 for 90-day mail order$4 copay/$0 deductible
*$8 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $42 copay $42 copay
Tier 4 – Non-preferred drug 34% coinsurance 33% coinsurance
Tier 5 – Specialty 27% coinsurance 27% coinsurance
35

• Lowered worldwide urgent care copay
• Vision hardware benefit now $150 allowance per year
• New OTC benefit - $50/quarter• 24-Hour nurse hotline now included
Sound + Rx (HMO): HighlightsKing, Pierce, Snohomish, Thurston and Whatcom Counties
PHARMACY• Lowered copay for 90-day mail order• Lowered copays on tiers 3 and 4

Sound + Rx HMO
Plan Benefits 2019 2020
Monthly plan premium $40 $40
Medical deductible $0 $0
Annual out-of-pocket maximum $6,500 $6,500
Primary care provider visit $10 copay $10 copay
Specialist visit $50 copay $50 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $595 copay (days 1–3)/$0 copay (days 4+) $595 copay (days 1–3)/$0 copay (days 4+)
Ambulatory surgical center $395 copay $395 copay
Outpatient hospital center $495 copay $495 copay
Ambulance $255 copay each way $255 copay each way
Worldwide emergency care $80 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $80 (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $15 copay labs/$20 copay x-ray $15 copay labs/$20 copay x-ray
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
King, Pierce, Snohomish, Thurston and Whatcom Counties
37

Sound + Rx HMO
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $30 copay/$120 allowance/2 years $150 per calendar year
Dental Included Included
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50 each quarter
Routine hearing exam $0-$50 $0-$50
Hearing aids with Hearing Care Solutions
$1,000 per ear each year $1,000 per ear each year
Routine chiropractic Not covered Not covered
Routine podiatry $50 copay/6 per year $50 copay/6 per year
Diabetic supplies 0% coinsurance 10% coinsurance
24-Hour NurseLine Not covered Included
NEW
38
NEW

Sound + Rx HMO
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $160 on tiers 3-5 $160 on tiers 3-5
Tier 1 – Preferred generic$2 copay/$0 deductible
*$5 for 90-day mail order$2 copay/$0 deductible
*$4 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $47 copay $42 copay
Tier 4 – Non-preferred drug 50% coinsurance 33% coinsurance
Tier 5 – Specialty 30% coinsurance 30% coinsurance
39

• Lowered worldwide urgent care copay
• Vision hardware benefit now $150 allowance per year
• New OTC benefit $50/quarter• 24-Hour nurse hotline now included
Alpine (HMO): HighlightsKing, Pierce, Snohomish, Thurston and Whatcom Counties

Alpine (HMO)
Plan Benefits 2019 2020
Monthly plan premium $42 $42
Medical deductible $0 $0
Annual out-of-pocket maximum $6,500 $6,500
Primary care provider visit $10 copay $10 copay
Specialist visit $50 copay $50 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $595 copay (days 1–3)/$0 copay (days 4+) $595 copay (days 1–3)/$0 copay (days 4+)
Ambulatory surgical center $395 copay $395 copay
Outpatient hospital center $495 copay $495 copay
Ambulance $255 copay each way $255 copay each way
Worldwide emergency care $80 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $80 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $15 copay labs/$20 copay x-ray $15 copay labs/$20 copay x-ray
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
King, Pierce, Snohomish, Thurston and Whatcom Counties
41

Alpine (HMO)
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $30 copay/$120 allowance/2 years $150 per calendar year
Dental Not covered Not covered
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50 per quarter
Routine hearing exam $1,000 per ear each year $1,000 per ear each year
Hearing aids with Hearing Care Solutions
Not covered Not covered
Routine chiropractic Not covered Not covered
Routine podiatry $50 copay/6 per year $50 copay/6 per year
Diabetic supplies 0% coinsurance 10% coinsurance
24-Hour NurseLine Not covered Included
42
NEW

• Lowered worldwide urgent care copay
• Vision hardware benefit now $150 allowance per year
• New OTC benefit $50/quarter• 24-Hour nurse hotline now included
Charter + Rx (HMO): HighlightsKing, Pierce, Snohomish, Thurston, and Whatcom counties
PHARMACY• Lowered copays on tier 1 mail order,
tiers 3 and 4

Charter + Rx (HMO)
Plan Benefits 2019 2020
Monthly plan premium $146 $150
Medical deductible $0 $0
Annual out-of-pocket maximum $4,900 $4,900
Primary care provider visit $10 copay $10 copay
Specialist visit $35 copay $35 copay
Occupational/physical therapy $35 copay $35 copay
Inpatient hospital care $450 copay (days 1–4)/$0 copay (days 5+) $450 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center $190 copay $190 copay
Outpatient hospital center $290 copay $290 copay
Ambulance $315 copay each way $315 copay each way
Worldwide emergency care $80 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $80 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $7 copay labs/$20 copay x-rays $7 copay labs/$20 copay x-rays
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
King, Pierce, Snohomish, Thurston, and Whatcom counties
44

Charter + Rx (HMO)
Plan Benefits 2019 2020
Annual routine eye exam $20 copay $20 copay
Vision hardware allowance $30 copay/$120 allowance/2 years $150 per calendar year
Dental Included Included
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered $50 per quarter
Routine hearing exam $0-$35 $0-$35
Hearing aids with Hearing Care Solutions
$1000 per ear each year $1000 per ear each year
Routine chiropractic Not covered Not covered
Routine podiatry $35 copay/6 per year $35 copay/6 per year
Diabetic supplies 0% coinsurance 10% coinsurance
24-Hour NurseLine Not covered Included
NEW
45
NEW
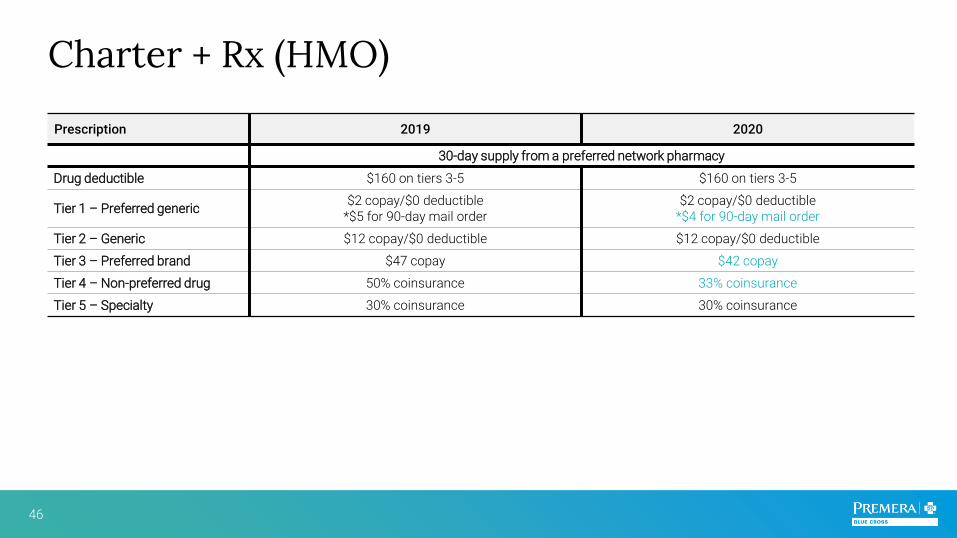
Charter + Rx (HMO)
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $160 on tiers 3-5 $160 on tiers 3-5
Tier 1 – Preferred generic$2 copay/$0 deductible
*$5 for 90-day mail order$2 copay/$0 deductible
*$4 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $47 copay $42 copay
Tier 4 – Non-preferred drug 50% coinsurance 33% coinsurance
Tier 5 – Specialty 30% coinsurance 30% coinsurance
46

• Lowered coinsurance on diabetic supplies
Classic Plus (HMO): HighlightsKing, Pierce, Snohomish and Thurston counties

Classic Plus (HMO)
Plan Benefits 2019 2020
Monthly plan premium $167 $190
Medical deductible $0 $0
Annual out-of-pocket maximum $5,000 $5,000
Primary care provider visit $10 copay $10 copay
Specialist visit $40 copay $40 copay
Occupational/physical therapy $40 copay $40 copay
Inpatient hospital care $350 copay (days 1–4)/$0 copay (days 5+) $350 copay (days 1–4)/$0 copay (days 5+)
Ambulatory surgical center $250 copay $250 copay
Outpatient hospital center $250 copay $250 copay
Ambulance $200 copay each way $200 copay each way
Worldwide emergency care $75 copay (waived if admitted) $90 copay (waived if admitted)
Worldwide urgent care $40 copay (waived if admitted) $50 copay (waived if admitted)
Lab services/x-rays $0 copay $0 copay
Preventive care $0 copay $0 copay
Annual physical exam Covered in full 1 per year Covered in full 1 per year
King, Pierce, Snohomish and Thurston counties
48

Classic Plus (HMO)
Plan Benefits 2019 2020
Annual routine eye exam $40 copay $40 copay
Vision hardware allowance $150 per calendar year $150 per calendar year
Dental Included Included
Additional dental services Not covered Not covered
Gym membership Silver&Fit Silver&Fit
Over the counter (OTC) benefit Not covered Not covered
Routine hearing exam Not covered Not covered
Hearing aids with Hearing Care Solutions
Not covered Not covered
Routine chiropractic Not covered Not covered
Routine podiatry Not covered Not covered
Diabetic supplies 20% coinsurance 10% coinsurance
24-Hour NurseLine Included Included
49
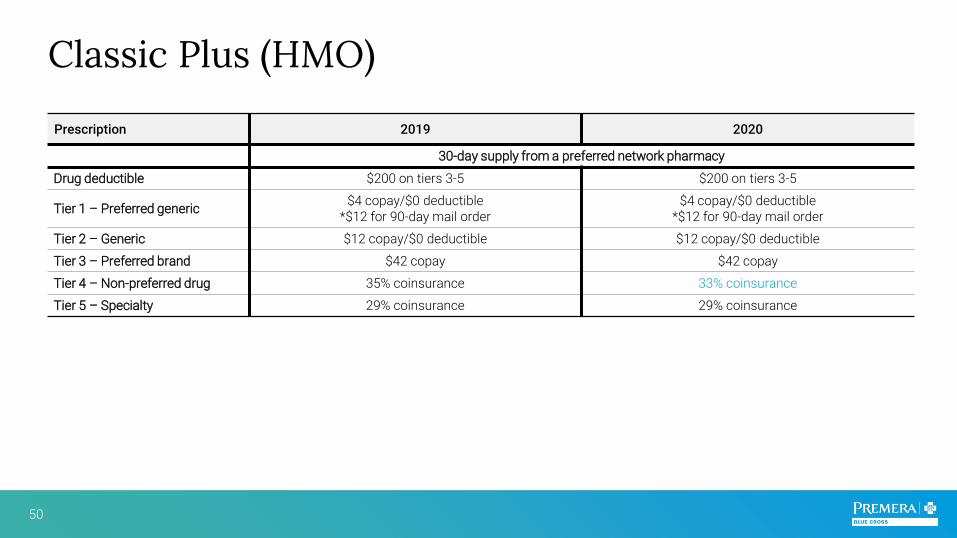
Classic Plus (HMO)
Prescription 2019 2020
30-day supply from a preferred network pharmacy
Drug deductible $200 on tiers 3-5 $200 on tiers 3-5
Tier 1 – Preferred generic$4 copay/$0 deductible
*$12 for 90-day mail order$4 copay/$0 deductible
*$12 for 90-day mail order
Tier 2 – Generic $12 copay/$0 deductible $12 copay/$0 deductible
Tier 3 – Preferred brand $42 copay $42 copay
Tier 4 – Non-preferred drug 35% coinsurance 33% coinsurance
Tier 5 – Specialty 29% coinsurance 29% coinsurance
50

• Included on Charter + Rx, Classic, Classic Plus, Core Plus, Sound + Rx, and Total Health
• Classic, Core Plus and Total Health plans have additional dental services allowance of $200/per year
• Available as a $26 rider for HMO, Peak + Rx, and Core HMO plans
Dental Plan

*Dental Rider – Available as $26 rider on HMO, Peak + Rx, and Core HMO plans. Members may add the optional dental rider within 60
days of enrolling in their Premera Blue Cross Medicare Advantage plans. Coverage starts the first of the month following the date we
receive the completed enrollment form.
Dental Plan
Included on Charter + Rx, Classic, Classic Plus, Core Plus, Sound + Rx, and Total Health*
Monthly dental premium $0 (embedded)/$26 (rider)
Routine oral exams $0 copay (2 per year)
Routine cleanings/periodontal maintenance $0 copay (2 per year)
Fluoride treatments $0 copay (1 per year)
Bitewing x-rays (set of 4) $0 copay (1 set per year)
Panoramic or complete series X-rays $0 copay (1 set per 5 years )
Emergency exam $0 copay (1 per year)
Additional dental services (Classic, Core Plus, and Total Health only)
$200 (per year)
Find providers online at premera.com/ma
52
NEW

Provider Network

Premera Medicare Advantage Provider Network
16,000 providers
across 12 counties
Memberscan see any provider –not limited
to those within their county
Memberscan find providers
online at premera.com/ma
Producerscan find provider
alerts at premera.com/ma
/producers
Memberscan travel with
worldwidecoverage for
emergencies or urgent care
54

This list is not a complete list of standard and/or preferred providers and is subject to change.
CHI Franciscan
EvergreenHealth
Family Care Network
Morton General Hospital
MultiCare
Northwest Physicians Network
Overlake Medical Center & Clinics
PacMed
PeaceHealth
Physicians of Southwest Washington
Providence Health & Services
Seoul IPA
Skagit Valley Hospital
Swedish Health Services
The Everett Clinic
The Polyclinic
UW Medicine
Virginia Mason Medical Center
Western Washington Medical Group
WESTERN WASHINGTON PROVIDERS
Premera Medicare Advantage Provider Network
55

This list is not a complete list of standard and/or preferred providers and is subject to change.
Premera Medicare Advantage Provider Network
EASTERN WASHINGTON PROVIDERS
CHAS Health
MultiCare Rockwood
Providence Health & Services
The Doctors’ Clinic
Vivacity Care Center
56

Telehealth services (virtual care)
Office visits and consultations using interactive 2-way telecommunications (phone, video)
Providence/Swedish Virginia MasonMultiCare
Health System CHI Franciscan
PCP provider virtual visits covered at PCP copay
Specialist provider virtual visits covered at specialist copay
Virtual mental health visits with Optum providers covered at mental health copay
Any contracted in-network provider who offers their services is covered:
Providers who offer telehealth services:
57

Prescription coverage and network

Pharmacy
One formulary
Total Health, Classic, and Core Plus (“Enhanced” plans)
$0 copay for 90 days for Tier 1 through mail order
Rx deductible waived for Tiers 1-3
Lower copays for Tiers 1-3 through preferred pharmacies
59
* Not available on Classic Plus and Core

Prescription Coverage
Non-preferred drugs
Preferred brand (deductible waived on
Classic, Total Health, and Core Plus)
Generic(deductible waived on all plans)
Preferred generic
(deductible waived on all plans)
TIER
1TIER
2TIER
3TIER
4
Specialty
TIER
5
60

Medicare Advantage Pharmacy Network
61 Network may change at any time. You will receive notice of change as necessary.
Preferred Pharmacies
Standard Pharmacies

*Hearing Care Solutions provides hearing aids and services on behalf of Premera Blue Cross. They have been working with Premera since 2013.
Hearing Aids with Hearing Care Solutions*

Comprehensive hearing exam at no charge
60-day evaluation
period
1-year of follow-up service at no charge
Unlimited telehealth and product support following hearing aid
fitting
3-year comprehensive
warranty including loss, damage, and
repair
2-year supply of batteries
(up to 128 cells per ear)
Benefits for membersClassic, Total Health, Core Plus, Charter+Rx, Peak+Rx, Sound+Rx, and Alpine
63

How to enroll your clients• Paper applications• Shop and Enroll tool

Send via secure email to premera_applications@
advantasure.com
Send paper applications via fax to 800-381-4837
Paper applications
OR
For clients who want to change Premera plans: submit a plan change form (rather than a full application)
65

Request a personal URLthrough your FMO or
Register at premera.com/wa/producer
OR
Shop and Enroll: premera.com/wa/producers
66

Your one-stop resource

Everything you need in one place
Premera.com/ma/producers
Customizable sales materials
Supply order formsSales and application forms
Electronic Funds Transfer form, Producer of Record Change form
Benefit Summaries and Evidence of Coverage
bookletsProvider network updates
Link to member welcome site
68


















