Prematurity, neuropathology virus (HIV)infection · Abbreviations: HIV, human immunodeficiency...
5
Proc. Nati. Acad. Sci. USA Vol. 84, pp. 3826-3830, June 1987 Immunology Prematurity, hypogammaglobulinemia, and neuropathology with human immunodeficiency virus (HIV) infection (acquired immunodeficiency syndrome/human immunodeficiency virus antibody/intracranial calcification) RAJENDRA PAHWA*t, ROBERT A. GOOD*, AND SAVITA PAHWAt *Immunobiology Department, All Children's Hospital, University of South Florida, St. Petersburg, FL 33701; and tPediatric Immunology Division, North Shore University Hospital, Cornell University Medical Center, Manhasset, NY 11030 Contributed by Robert A. Good, February 4, 1987 ABSTRACT Infection with the human immunodeficiency virus (HIV) is characteristically associated with hypergam- maglobulinemia in both adult and pediatric cases. We report herein four infants who had an HIV infection in association with severe hypogammaglobulinemia and did not exhibit antibodies against HIV. HIV was isolated antemortem or postmortem in all four infants from either peripheral blood, cerebrospinal fluid, or body tissues. HIV infection could be presumed to be acquired transplacentally in two infants and by way of infected blood transfusions during the neonatal period in the other two. Each infant became symptomatic within the first year of life and developed rapidly progressive manifesta- tions of the disease. Features that were common to all four infants include premature birth, failure to thrive, hepatomeg- aly, and progressive neurological abnormalities that were associated with intracranial calcifications. We conclude that, when infection occurs early in development either by trans- placental exposure to the virus or from blood transfusion in small premature infants, hypogammaglobulinemia and defi- ciency of antibody production leading to the absence of antibody responses on which diagnosis is usually based can occur. Furthermore, progressive central nervous system dis- ease may be a frequent finding in such infants, and this may lead to cerebral calcifications that must be attributed to the HIV infection itself and not to complicating infections-e.g., toxoplasmosis. It is suggested that patients with hypogamma- globulinemia, antibody deficiency syndrome, and central ner- vous system disease have an extremely bad prognosis. Infection with the retrovirus, human T-lymphotropic virus type III/lymphadenopathy-associated virus (HTLV-III/ LAV), now known as human immunodeficiency virus (HIV), results in a wide spectrum of clinical manifestations, ranging from asymptomatic states to the severest disease forms associated with the acquired immunodeficiency syndrome (AIDS) (1-12). This virus infects preferentially T lympho- cytes bearing the T4 antigen and also seems to exhibit preference for cells, especially macrophages, of the central nervous system (13, 14). Among the immunological distur- bances resulting from infection with HIV, hypergammaglob- ulinemia appears to be a consistent finding in adults as well as in most children (5, 15-17). The presence of antibodies to HIV in serum is considered to be a hallmark of this infection. In this report four infants are described in whom HIV infection was documented by positive virological cultures; they also exhibited profound hypogammaglobulinemia and did not produce HIV antibodies. These infants were born prematurely and had illnesses characterized by severe and progressive neurological disease. Although the protective role of HIV antibodies has not been established, these observations suggest that severe hypogammaglobulinemia that develops in infants with HIV infection may be a bad prognostic feature. Furthermore, neurological complications occur and appear to be severe in such hypogammaglobulin- emic infants. MATERIALS AND METHODS Study Subjects, The four patients described herein were each born prematurely between 26 and 30 weeks of gestation (Table 1). Two infants (patients 1 and 2) were born to HIV antibody-positive, asymptomatic mothers; the first was an intravenous drug user, and the second probably had sexually acquired the infection. The other two infants (patients 3 and 4) were born to healthy mothers. The HIV serology was negative on both parents in each of the latter infants who had, however, been given repeated transfusions in the neonatal period prior to availability of HIV antibody screening. These infants were presumed to be infected by HIV-infected blood transfusions; the blood donor of patient 3 was subsequently proven to have an HIV infection. The clinical manifestations in the four patients are recorded in Table 2. Patient 1 became symptomatic between 7 and 8 months of age. Patient 1 was followed from birth, and patients 2, 3, and 4 were followed from the ages of 5, 8, and 10 months, respectively. Patient 3, who had radiological evidence of interstitial pneumonitis, was found by biopsy to have lymphoid interstitial pneumonitis negative for Pneumocystis carinii pneumonia, bacteria, fungi, and all other identifiable viruses. All infants had progressive retardation of their growth and development, and each exhibited clear evidence of central nervous system (CNS) involvement. Evidence of brain atrophy and CNS calcification was present in the computerized tomographic scans of each of the four patients; examples of the CNS calcifications are illustrated in Fig. 1. Cytomegalovirus was repeatedly isolated from the urine and saliva of only one infant, patient 2. Severe and recurrent bacterial infections resulting in pneumonia, meningitis, or bacteremia ultimately occurred in each of the patients. All patients were treated with intravenous gamma globulin be- cause they exhibited hypogammaglobulinemia. The dose of gamma globulin was gradually increased over a 4-week period from 100 to 300 mg/kg and was given at this dose every 2-4 weeks, depending upon compliance. Patients 1 and 2 were started on intravenous injections of gamma globulin at 6 months of age, whereas patients 3 and 4 first received injections at 13 months of age. Only patient 2 had adverse reactions to the gamma globulin, which often precluded administration of the desired dose. All patients died of sepsis at 7, 22, 21, and 17 months of age, respectively. Autopsy was performed on patient 1. This analysis revealed generalized Abbreviations: HIV, human immunodeficiency virus; AIDS, ac- quired immunodeficiency syndrome; CNS, central nervous system. 1To whom reprint requests should be addressed at: All Children's Hospital, 801 6th Street South, St. Petersburg, FL 33701. 3826 The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. §1734 solely to indicate this fact. Downloaded by guest on July 2, 2020
Transcript of Prematurity, neuropathology virus (HIV)infection · Abbreviations: HIV, human immunodeficiency...

Proc. Nati. Acad. Sci. USAVol. 84, pp. 3826-3830, June 1987Immunology
Prematurity, hypogammaglobulinemia, and neuropathology withhuman immunodeficiency virus (HIV) infection
(acquired immunodeficiency syndrome/human immunodeficiency virus antibody/intracranial calcification)
RAJENDRA PAHWA*t, ROBERT A. GOOD*, AND SAVITA PAHWAt*Immunobiology Department, All Children's Hospital, University of South Florida, St. Petersburg, FL 33701; and tPediatric Immunology Division, NorthShore University Hospital, Cornell University Medical Center, Manhasset, NY 11030
Contributed by Robert A. Good, February 4, 1987
ABSTRACT Infection with the human immunodeficiencyvirus (HIV) is characteristically associated with hypergam-maglobulinemia in both adult and pediatric cases. We reportherein four infants who had an HIV infection in associationwith severe hypogammaglobulinemia and did not exhibitantibodies against HIV. HIV was isolated antemortem orpostmortem in all four infants from either peripheral blood,cerebrospinal fluid, or body tissues. HIV infection could bepresumed to be acquired transplacentally in two infants and byway of infected blood transfusions during the neonatal periodin the other two. Each infant became symptomatic within thefirst year of life and developed rapidly progressive manifesta-tions of the disease. Features that were common to all fourinfants include premature birth, failure to thrive, hepatomeg-aly, and progressive neurological abnormalities that wereassociated with intracranial calcifications. We conclude that,when infection occurs early in development either by trans-placental exposure to the virus or from blood transfusion insmall premature infants, hypogammaglobulinemia and defi-ciency of antibody production leading to the absence ofantibody responses on which diagnosis is usually based canoccur. Furthermore, progressive central nervous system dis-ease may be a frequent finding in such infants, and this maylead to cerebral calcifications that must be attributed to theHIV infection itself and not to complicating infections-e.g.,toxoplasmosis. It is suggested that patients with hypogamma-globulinemia, antibody deficiency syndrome, and central ner-vous system disease have an extremely bad prognosis.
Infection with the retrovirus, human T-lymphotropic virustype III/lymphadenopathy-associated virus (HTLV-III/LAV), now known as human immunodeficiency virus (HIV),results in a wide spectrum of clinical manifestations, rangingfrom asymptomatic states to the severest disease formsassociated with the acquired immunodeficiency syndrome(AIDS) (1-12). This virus infects preferentially T lympho-cytes bearing the T4 antigen and also seems to exhibitpreference for cells, especially macrophages, of the centralnervous system (13, 14). Among the immunological distur-bances resulting from infection with HIV, hypergammaglob-ulinemia appears to be a consistent finding in adults as wellas in most children (5, 15-17). The presence of antibodies toHIV in serum is considered to be a hallmark of this infection.In this report four infants are described in whom HIVinfection was documented by positive virological cultures;they also exhibited profound hypogammaglobulinemia anddid not produce HIV antibodies. These infants were bornprematurely and had illnesses characterized by severe andprogressive neurological disease. Although the protectiverole of HIV antibodies has not been established, theseobservations suggest that severe hypogammaglobulinemia
that develops in infants with HIV infection may be a badprognostic feature. Furthermore, neurological complicationsoccur and appear to be severe in such hypogammaglobulin-emic infants.
MATERIALS AND METHODSStudy Subjects, The four patients described herein were
each born prematurely between 26 and 30 weeks of gestation(Table 1). Two infants (patients 1 and 2) were born to HIVantibody-positive, asymptomatic mothers; the first was anintravenous drug user, and the second probably had sexuallyacquired the infection. The other two infants (patients 3 and4) were born to healthy mothers. The HIV serology wasnegative on both parents in each of the latter infants who had,however, been given repeated transfusions in the neonatalperiod prior to availability of HIV antibody screening. Theseinfants were presumed to be infected by HIV-infected bloodtransfusions; the blood donor of patient 3 was subsequentlyproven to have an HIV infection.The clinical manifestations in the four patients are recorded
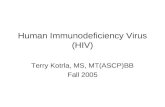
in Table 2. Patient 1 became symptomatic between 7 and 8months of age. Patient 1 was followed from birth, and patients2, 3, and 4 were followed from the ages of 5, 8, and 10 months,respectively. Patient 3, who had radiological evidence ofinterstitial pneumonitis, was found by biopsy to havelymphoid interstitial pneumonitis negative for Pneumocystiscarinii pneumonia, bacteria, fungi, and all other identifiableviruses. All infants had progressive retardation of theirgrowth and development, and each exhibited clear evidenceof central nervous system (CNS) involvement. Evidence ofbrain atrophy and CNS calcification was present in thecomputerized tomographic scans of each of the four patients;examples of the CNS calcifications are illustrated in Fig. 1.Cytomegalovirus was repeatedly isolated from the urine andsaliva of only one infant, patient 2. Severe and recurrentbacterial infections resulting in pneumonia, meningitis, orbacteremia ultimately occurred in each of the patients. Allpatients were treated with intravenous gamma globulin be-cause they exhibited hypogammaglobulinemia. The dose ofgamma globulin was gradually increased over a 4-weekperiod from 100 to 300 mg/kg and was given at this dose every2-4 weeks, depending upon compliance. Patients 1 and 2were started on intravenous injections of gamma globulin at6 months of age, whereas patients 3 and 4 first receivedinjections at 13 months of age. Only patient 2 had adversereactions to the gamma globulin, which often precludedadministration of the desired dose. All patients died of sepsisat 7, 22, 21, and 17 months of age, respectively. Autopsy wasperformed on patient 1. This analysis revealed generalized
Abbreviations: HIV, human immunodeficiency virus; AIDS, ac-quired immunodeficiency syndrome; CNS, central nervous system.1To whom reprint requests should be addressed at: All Children'sHospital, 801 6th Street South, St. Petersburg, FL 33701.
3826
The publication costs of this article were defrayed in part by page chargepayment. This article must therefore be hereby marked "advertisement"in accordance with 18 U.S.C. §1734 solely to indicate this fact.
Dow
nloa
ded
by g
uest
on
July
2, 2
020

Proc. Natl. Acad. Sci. USA 84 (1987) 3827
Table 1. Patient profiles
Gestational Birth weight, Neonatal Neonatal Onset of otherPatient age, wk g complications transfusion symptoms, mo Clinical outcome Route of infection
1 26 1090 IRDS, sepsis + 3 Died, 7 mo.; sepsis Intrauterine/prenatal; HIVAb+ mother; IVDA
2 30 1040 Sepsis - 7 Died, 22 mo.; sepsis Intrauterine/prenatal; HIVAb+ mother; sexuallyacquired infection
3 28 1080 Sepsis + 8 Died, 21 mo.; sepsis; Infected blood transfusionrespiratory failure
4 26 850 IRDS + 7 Died, 17 mo.; sepsis; Infected blood transfusionrespiratory failure
IRDS, idiopathic respiratory distress syndrome; IVDA, intravenous drug abuser; Ab+, antibody-positive.
lymphocyte depletion and the presence of microglial nodules,calcification, and atrophy of cerebral cortex of the brain.Parents refused to permit autopsies on the other threepatients.
Laboratory Methods. Serologic testing for HIV antibodieswas performed by immunological blot analysis (18). Specif-ically, the presence of the anti-p41 antibody to HIV wasconsidered as evidence of HIV infection. HIV cultures wereperformed on peripheral blood lymphocytes of all fourpatients and on cerebrospinal fluid of patient 4. For thesestudies, lymphocytes from peripheral blood or cerebrospinalfluid were cultured with phytohemagglutinin, grown in thepresence of interleukin 2-stimulated lymphocytes, and sub-sequently cocultivated with an uninfected clone of the H-9cell line, as previously described (19). Virus production in theinfected cell clones was monitored by assaying for reversetranscriptase activity in culture supernatants and by electronmicroscopy. In patient 1, tissues obtained at autopsy frombrain and lung were cultured for HIV; the virus was isolatedfrom primary cultures of lung tissue and was propagated inperipheral blood-derived macrophages ofnormal donors (20).Virus expression was tested by an immunofluorescenceassay using a monoclonal antibody to p17 and by measure-ment of reverse transcriptase activity (20).T and B lymphocytes, and cells of the major T-cell subsets
that bear T4 or T8 antigens on their surfaces, were quantifiedin whole blood using monoclonal antibodies (Ortho-immuneand Coulter clone reagents) and flow cytometry (21). Thefunctional capacity of peripheral blood lymphocytes wasassessed by investigating the proliferative responses of thelymphocytes to phytomitogens, namely phytohemagglutinin,concanavalin A, and pokeweed mitogen, as determined byincorporation of [14C]thymidine (New England Nuclear) (22).
Table 2. Clinical characteristics of patients under study
Patient
Manifestation 1 2 3 4
Severe infectionsOpportunistic* - - - +Bacterial + + + +
Lymphocytic interstitial pneumonitist - - +Neurological abnormalities (brain
atrophy, calcifications) + + + +Hepatomegaly + + + +Splenomegaly + - - +Failure to thrive + + + +Growth retardation + + + +Lymnphadenopathy + + + +Thrush + - + +Clubbing of nails - + +
*Pneumocystis carini pneumonia.tBiopsy-proven lymphocytic interstitial pneumonitis.
Quantitative serum immunoglobulin levels were determinedby radial immunodiffusion.
RESULTSSerum immunoglobulin levels and results of HIV antibodytesting are shown in Table 3 for all four infants. In patients 1and 2, serum IgG levels were within normal limits for age at1 and 5 months, respectively, but they were decreased at 3months of age in patient 1 and at 7 months of age in patient2. Patients 3 and 4 had reduced IgG levels at the time ofpresentation (i.e., at 8 and 10 months of age, respectively).Patients 1 and 2, who were initially positive for HIV anti-body, became negative after 6 months of age. It is presumedthat the antibodies in the infants' serum were passivelytransferred to the infants from their HIV-positive mothers.Patients 3 and 4 were negative for HIV antibodies when theywere first tested at 8 and 15 months of age, respectively.Serum IgA levels were ultimately low in all four patients.Serum IgM levels were elevated in patients 2 and 3 at the timeof initial diagnosis and became low after 14 months of age.Sometime during the course of the disease, three of thepatients had low levels of IgM. The fourth patient, patient 2,had elevated or normal IgM levels early in life; these levelsdropped in subsequent months, but they were still in thenormal range prior to death.
All of the children were treated with intravenous gammaglobulin (IgG) for their hypogammaglobulinemia as describedabove.HIV was isolated from peripheral blood lymphocytes of
patients 2, 3, and 4 and from cerebrospinal fluid of patient 4.In patient 1, virus was also isolated from autopsy material inlung macrophages as described above (20).
Table 4 summarizes the results of analyses of lymphocytesurface markers. Absolute lymphocyte counts were de-creased in two patients, and a depression in the number ofT4cells, with absolute counts less than 400/mm3, was noted inthree of the four patients. The T4/T8 ratios were less than 1.0in all four infants. B-cell numbers, which are usually in-creased in HIV infection, were decreased in each of the threeinfants tested. Results of immune testing are summarized inTable 5. Functional lymphoproliferative responses to thephytomitogens phytohemagglutinin, concanavalin A, andpokeweed mitogen were severely depressed in two infants(patients 1 and 2), and response to concanavalin A wasdepressed in patient 3. Normal proliferative responses wereobserved in patient 4 at the time of testing.
DISCUSSIONDocumentation of HIV antibodies in serum has proved to bea reliable and practical means of establishing the presence ofHIV infection (18). On rare occasions, a transient or persis-tent seronegative virus-infected state occurs and poses apotential problem in serodiagnosis of HIV infection (23). In
Immunology: Pahwa et al.
Dow
nloa
ded
by g
uest
on
July
2, 2
020

Proc. Natl. Acad. Sci. USA 84 (1987)
FIG. 1. Computerized tomographs of the brain from patient 3. Cuts at various levels show cortical atrophy, ventricular dilatation, andintracranial calcifications.
this report, we describe four infants with HIV infection, whodeveloped severe hypogammaglobulinemia and were HIVantibody-negative to this virus, although they were clearly
Table 3. Immunoglobulin levels and HIV infection
Patient Test resultsand age IgG, mg/dI IgA, mg/dl IgM, mg/dl HIV-Ab*
Patient 11 mo. 382 9 33 ND3 mo. 133 <7 20 +6 mo. 25 8 147 mo.t 1220 <7 35
Patient 25 mo. 333 26 158 +7 mo.t 181 34 127
11 mo.t 149 25 97 ND14 mo.t 169 14 3718 mo.t 374 <7 55
Patient 38 mo. 147 16 529 mo. 72 ND ND ND10 mo. 42 ND ND14 mo.t 704 <7 18
Patient 410 mo. 100 11 23 ND13 mo.t 364 <4 26 ND)15 mo.t 250 <2 10
Values less than 2 SD for age are in boldface. ND, not done.*Antibodies to HIV in serum, determined by immunological blot.tPatient on intravenous gamma globulin infusions.
infected with HIV. Presumably this immunity status is aconsequence of the hypogammaglobulinemia. The features ofall four of these infants included premature birth and pro-gressive development of severe neurological abnormalities.The latter consisted of intracranial calcifications, cerebralatrophy, and clinical evidence of cerebral palsy.B-lymphocyte dysfunction as an early manifestation of
HIV infection is usually characterized by profound polyclo-nal hypergammaglobulinemia (5, 15-17, 24). In a previousstudy (5), hypergammaglobulinemia was consistently notedin HIV-infected infants, ranging in age from 3 months to 1year, who had typical clinical features of AIDS or AIDS-related complex and were seropositive for HIV antibodies.Hypogammaglobulinemia occurring in association with HIVinfection represents a new phenomenon, and its relationshipto those situations in which HIV-infected patients are sero-negative despite normal or increased levels ofimmunoglobinsneeds to be investigated. Already, however, it has beenshown that the levels of IgG2 and IgG4 subclasses may below in patients with HIV infection, while hypergammaglob-ulinemia attributable to increased levels of IgGi and IgG3occurs in the same patient (25). Furthermore, hypogam-maglobulinemia has been encountered in association withselective T-helper cell immunodeficiency in patients withsevere combined immunodeficiencies or common variableimmunodeficiencies (26, 27). Thus, it seems quite possiblethat the hypogammaglobulinemia seen in these infants maybe attributable to profoundly defective functions of T-helpercells, defective T cell-B cell interactions, or even deficienciesin the function of B cells themselves (24).
In regard to the B-cell pathology in HIV infection, it hasbeen shown already that proliferating B cells infected with
3828 Immunology: Pahwa et al.
Dow
nloa
ded
by g
uest
on
July
2, 2
020

Proc. Natl. Acad. Sci. USA 84 (1987) 3829
Table 4. Lymphocyte markers, percentages, and absolute numbers
Percentage and absolute counts of markers
T3 T4 T8 T11 B1
Patient and age % No. % No. % No. % No. % No. T4/T8 ratio
Patient 13 mo. 35 441 24 307 54 684 75 942 2.1 27 0.4
Patient 27 mo. 68 3002 34 1501 43 1898 76 3356 3.6 159 0.8
Patient 315 mo. 34 275 9 73 52 421 48 389 ND ND 0.2
Patient 415 mo. 38 775 10 204 25 511 36 736 0.9 18 0.4
Values falling outside of the normal range for age are in boldface. For T8, boldface numbers indicate increased values; for all others, boldfacenumbers indicate decreased values. ND, not done.
another virus can grow the HIV (28). It is possible thatdifferent subpopulations of B lymphocytes react differentlyto the influence of the virus; some are stimulated while othersare inhibited. Even in the absence of direct infection ofB cellsby HIV, different components of the HIV might indirectlyexert either stimulatory and/or inhibitory influences (29). Infact, two patients reported herein, in spite of having lowlevels of serum IgG, had high levels IgM at some time duringthe first year of life. This recalls the dysgammaglobulinemiafirst described with virus infections in patients with the inutero infections caused by the rubella virus (30, 31). Theinfants described herein also had a paucity of B cells, whichis unusual in patients with HIV infection. This abnormality inB-cell numbers was unrelated to the mode of acquisition ofthe HIV infection-i.e., whether it occurred as a conse-quence of in utero infection or after birth. It is possible thatin the premature infant infected with HIV the B lymphocytes,which are characteristically immature in the newborn period(32, 33), are more readily compromised in their developmentthan at a later time in life. Only further studies will ascertainjust how and in what cells the primary influence of the virusto inhibit the development of a normal capacity for immu-noglobulin production is exercised.Accumulating clinical, pathological, and virological evi-
dence has firmly established the neurotropic potential ofHIV(3, 13, 14). In brain tissues of AIDS patients, HIV sequenceshave been demonstrated by Southern blot analysis of hostcell DNA. Further, HIV messenger RNA has been detectedby in situ hybridization (13). In a recent study, Popovic andcoworkers (20) demonstrated selective tropism by HIV viralisolates for macrophages obtained either from brain tissue ofan AIDS patient or from lung macrophages ofan infant. It hasbeen suggested that in certain patients, such as patient 1, themacrophages represent a primary target for transmission ofinfection to the CNS. In agreement with this concept isanother report that shows that virus-positive cells in the braintissue ofAIDS patients belong to the mononuclear phagocyte
Table 5. Summary of immunologic abnormalitiesPatient
Abnormality 1 2 3 4
Hypergammaglobulinemia (>2 SD for age) - - -
Hypogammaglobulinemia (<2 SD for age) + + + +Absolute lymphopenia (<1500/mm3) + - +T4 lymphopenia (<400/mm3) + - + +Reversed T4/T8 ratio (<1.0) + + + +Depressed lymphoproliferative responses(<2 SD)* + + + -
*Decrease of more than 2 SD from the normal mean lymphoprolif-erative responses to phytomitogens, phytohemagglutinin, con-canavalin A, or pokeweed mitogen.
series (34). As yet, an association between hypogammaglob-ulinemia and tropism of the HIV for macrophages has notbeen described. It is possible that monocyte dysfunctionmight further contribute to the failure of the development ofa normal capacity to produce antibodies in such patients.An additional concurrent viral infection might be respon-
sible for the CNS disease observed in these children. This is,however, an unlikely possibility, but it is one that cannot beconclusively ruled out in each ofthese patients because of thehypogammaglobulinemia and consequent absence of sero-logical responses that otherwise might be expected-forexample, toxoplasma, rubella, cytomegalovirus, or Epstein-Barr virus. However, cerebrospinal fluid cultures in onepatient were negative for cytomegalovirus and also werenegative for other herpes or enteric viruses and, at the sametime, were positive for HIV. The presence of HIV in thecerebrospinal fluid of patient 4, the autopsy findings of thebrain in patient 1, and the radiological and clinical abnormal-ities of the brain in all these patients raises the likelihood thata primary HIV infection involving the brain has occurred inall four of these children. The mechanism whereby such aninfection would result in intracranial calcifications is as yetunclear, but this finding should be included in the pathologicfeatures of HIV infection.
Thus, these patients who were infected with HIV virusvery early in life present evidence both of a threateningneurotropism of the HIV virus, especially for very youngchildren, and challenging new evidence of the complexity ofthe lymphoid cellular involvement in this disease, which nowmust be recognized as potentially leading to hypogam-maglobulinemia or agammaglobulinemia. Although a protec-tive role for HIV antibodies has not been conclusivelyestablished, the absence of such antibodies in the casesdescribed herein was associated in each instance with rapidlyprogressive clinical deterioration. A heightened awareness ofHIV seronegativity occurring as a consequence of hypogam-maglobulinemia has important consequences for the serodi-agnosis of HIV infection in children.
We are indebted to C. Leombrumo and M. Marecki for technicalassistance and to A. Johnston for secretarial assistance. We thankDrs. L. Resnick and M. Popovic for HIV viral isolation experimentsand Dr. M. Sarngadharan for HIV serology. This work was support-ed by a grant from the New York State AIDS Society (C001545) anda grant from the National Institute of Aging (AG05625).
1. Gallo, R. C., Salahuddin, S. Z., Popovic, M., Kaplan, G. M.,Haynes, M., Palker, B. F., Redfield, T. J., Oleske, R., Safai,J., White, G., Foster, R. & Markham, P. D. (1984) Science224, 500-502.
2. Broder, S. & Gallo, R. C. (1984) N. Engl. J. Med. 511,1292-1297.
Immunology: Pahwa et al.
Dow
nloa
ded
by g
uest
on
July
2, 2
020

Proc. Natl. Acad. Sci. USA 84 (1987)
3. Fauci, A. S., Macher, A. M., Longo, D. L., Lane, H. C.,Rook, A. H., Masur, H. & Gelmann, E. P. (1984) Ann. Intern.Med. 100, 92-106.
4. Levy, J. A. & Shimabukuro, J. (1985) J. Infect. Dis. 152,734-738.
5. Pahwa, S., Kaplan, M., Fikrig, S., Pahwa, R., Sarngadharan,M. G., Popovic, M. & Gallo, R. C. (1986) J. Am. Med. Assoc.255, 2299-3305.
6. Thomas, P. A., Jaffe, H. W., Spira, T. J., Reiss, R., Guerrero,I. C. & Auerbach, D. (1984) J. Am. Med. Assoc. 252, 639-644.
7. Levy, J. A., Kaminsky, L. S., Morrow, W. J., Steimer, K.,Luciw, P., Dina, D., Hoxie, J. & Oshiro, L. (1985) Ann.Intern. Med. 103, 694-696.
8. Oleske, J., Minnefor, A., Cooper, R., Thomas, K., Dela Cruz,A., Ahdieh, H., Guerrero, I., Joshi, V. V. & Desposito, F.(1983) J. Am. Med. Assoc. 249, 2345-2349.
9. Scott, G. B., Buck, B. E., Leterman, J. G., Bloom, F. L. &Parks, W. P. (1984) N. Engl. J. Med. 310, 76-81.
10. Rubinstein, A. (1983) Am. J. Dis. Child. 137, 825-827.11. Rogers, M. F. (1985) Pediatr. Infect. Dis. 4, 230-236.12. Ammann, A. J., Cowan, M. J., Wara, D. W., Weintrub, P.,
Dritz, S., Goldman, H. & Perkins, H. (1983) Lancet i, 956-958.13. Shaw, G. M., Harper, M. E., Hahn, B. M., Epstein, L. G.,
Gajdusek, D. C., Price, R. W., Navia, B. A., Petito, C. K.,O'Hara, C. J., Cho, E., Oleske, J. M., Wong-Staal, F. &Gallo, R. C. (1985) Science 227, 177-181.
14. Epstein, L. G., Sharer, L. R., Joshi, V. V., Fojas, M. M.,Koenigsberger, M. R. & Oleske, J. M. (1985) Ann. Neurol. 17,488-4%.
15. Seligmann, M., Chess, J. L., Fahey, A. S., Fauci, A. S.,Lachmann, P. J., L'Age-Stehr, J., Ngu, J., Pinching, A. J.,Rosen, F. S., Spira, T. J. & Wybran, J. (1984) N. Engl. J.Med. 311, 1286-1292.
16. Lane, C. H., Masur, H., Edgar, L. C., Whalen, G., Rook,A. H. & Fauci, A. S. (1983) N. Engl. J. Med. 309, 453-458.
17. Pahwa, S. G., Quilop, M. T. J., Lange, M., Pahwa, R. &Grieco, M. (1984) Ann. Intern. Med. 101, 757-763.
18. Sarngadharan, M. G., Popovic, M., Schupback, J. & Gallo,R. C. (1984) Science 224, 506-508.
19. Popovic, M., Sarngadharan, M. G., Read, E. & Gallo, R. C.(1984) Science 224, 497-500.
20. Gartner, S., Marcovits, P., Markovitz, D. M., Kaplan, M. H.,Gallo, R. C. & Popovic, M. (1986) Science 233, 215-219.
21. Pahwa, S., Sia, C., Te, C. & Pahwa, R. (1985) Pediatrics 76,914-917.
22. Cunningham-Rundles, S., Hanson, J. A. & Dupont, B. (1976)in Clinical Immunology, eds. Bach, F. H. & Good, R. A.(Academic, New York), Vol. 3, pp. 646-672.
23. Salahuddin, S. Z., Groopman, J. E., Markham, P. D., Sarn-gadharan, M. G., Redfield, R. R., McLane, M. F., Essex, M.,Sliski, A. & Gallo, R. C. (1984) Lancet fi, 1418-1420.
24. Pahwa, S. G., Fikrig, S., Menez, R. & Pahwa, R. (1986)Diagn. Immunol. 4, 20-24.
25. Aucouturier, A., Bremard-Oury, C., Clauvel, J. P., Debre,M., Griscelli, C., Seligmann, M., Preud'homme, J. L. (1986) inMonographs in Allergy, eds. Dukor, P., Kallos, P., Trnka, Z.& Klaksman, B. H. (Krager, Basel), Vol. 20, pp. 203-225.
26. Pahwa, S. G., Pahwa, R. N. & Good, R. A. (1980) J. Clin.Invest. 66, 543-550.
27. Siegal, F. P., Siegal, M. & Good, R. A. (1978) N. Engl. J.Med. 299, 172-177.
28. Montagnier, L., Gruest, J., Chamaret, S., Dauguet, C., Axler,C., Guetard, D., Nugeyre, M. T., Barre-Sinoussi, F., Cher-mann, J. C., Brunet, J. B., Klatzmann, D. & Gluckman, J. C.(1984) Science 225, 63-66.
29. Pahwa, S., Pahwa, R., Saxinger, C., Gallo, R. C. & Good,R. A. (1985) Proc. Natl. Acad. Sci. USA 82, 8198-8202.
30. Dent, P. B., Olson, G. B., Good, R. A., Rawls, W. E., South,M. A. & Melnick, J. L. (1968) Lancet i, 291-293.
31. Soothill, J. E., Haynes, K. & Dudgeon, J. A. (1966) Lancet i,1385-1387.
32. Wu, L. Y., Bianco, A., Cooper, M. D. & Lawton, A. R.(1976) Clin. Immunol. Immunopathol. 5, 208-217.
33. Tosato, G., Magrath, I. T., Koski, I. R., Dooley, N. J. &Blaese, M. R. (1980) J. Clin. Invest. 66, 383-388.
34. Koenig, S., Gendelman, H. E., Orenstein, J. M., Dal Canto,M. C., Pezeshkpour, Yungbluth, M., Janotta, F., Aksamit, A.,Martin, M. & Fauci, A. S. (1986) Science 233, 1089-1093.
3830 Immunology: Pahwa et al.
Dow
nloa
ded
by g
uest
on
July
2, 2
020