Premalignant conditions omr
41
-
Upload
cyriacjohn -
Category
Health & Medicine
-
view
256 -
download
1
Transcript of Premalignant conditions omr

BY
CYRIAC JOHN PART 1 4th year BDS
PRECANCEROUS CONDITION
• Generalized state of the body, which is associated with a significantly
increased risk of cancer
DEFINITION
PREMALIGNANT CONDITIONS ARE……
• ORAL SUBMUCOUS FIBROSIS
• ORAL LICHEN PLANUS
• SIDEROPENIC DYSPHAGIA
• DYSKERATOSIS CONGENITA
• DISCOID LUPUS ERYTHEMATOSIS

ORAL SUBMUCOUS FIBROSISDEFINITION
“It is a slowly progressing chronic fibrotic disease of the oral cavity
&oropharynx, characterized by fibro elastic change and inflammation leading
To a progressive inability to open the mouth, swallow or speak”
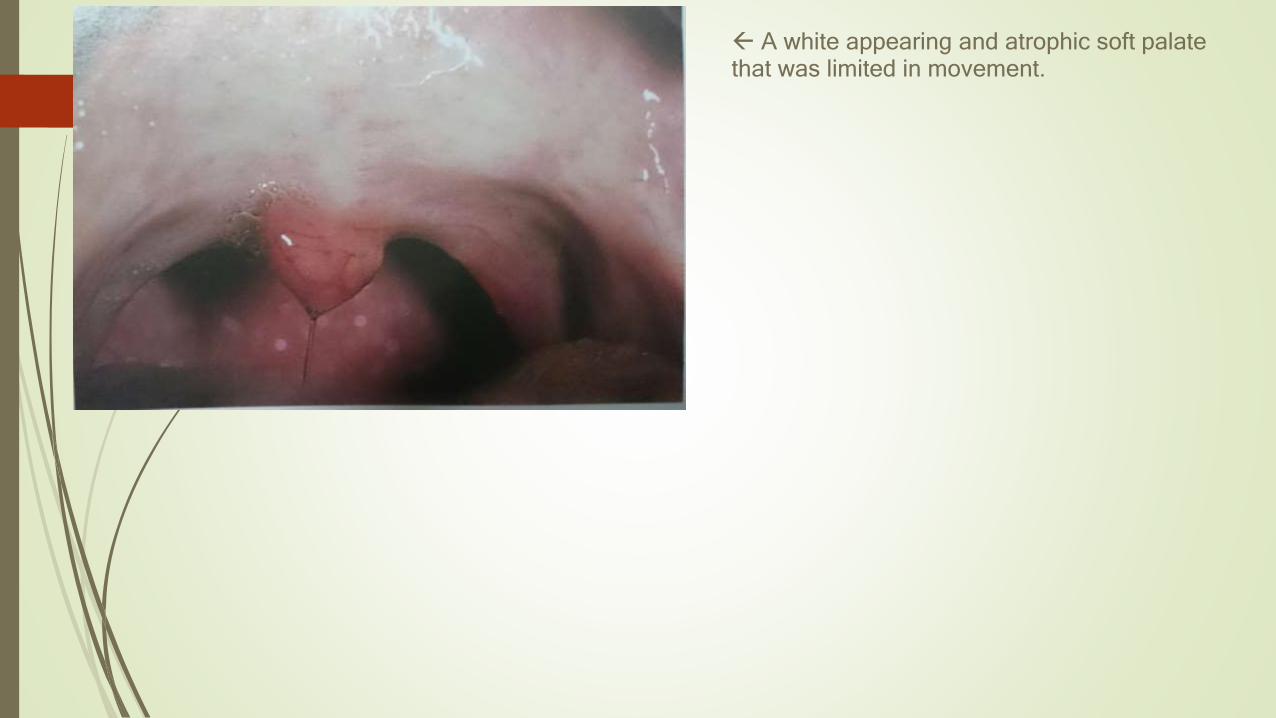
A white appearing and atrophic soft palate that was limited in movement.
ETIOLOGY
• Intially classified as idiopathic,now
• Betel quid & its components(arecoline,an active alkaloid found in betel nuts,stimulatesfibroblasts to increase production of collagen by 150%)
• Capsaicin—chilles(hypersensitivity reaction)
• Nutritional factors
• Immunological factors
CLINICAL FEATURES
AGE
11-- 60 years ,prevalent among teenagers in India
Sex
From 0.2 -- 0.3% in males to 1.2--4.5% in females in Indian communities
Race
South – East Asian countries, in Indian immigrants to other countries
Mortality/morbidity
• High rate of morbidity – progressive inability to open mouth, resulting
in difficulty in eating & consequent nutritional deficiencies
• Significant Mortality rate – can transform into oral cancer , particularly
Squamous cell carcinoma 7.6%
Clinical presentation
• Common site – buccal mucosa, retro molar area, uvula, palate etc
• Initially pain and burning sensation upon consumption of hot and spicy food
• Vesicle and ulcers are present
• EXcessive or reduced salivation and defective gustation
• Hearing loss
• Depapillation and atrophy of tongue and uvula
• Depigmentation and loss of stippling over gingiva
• Nasal tone in voice
• Difficulty in deglutition
• Impaired mouth movements e.g.: eating, whistling, blowing, sucking
Clinical stages
3 stages (pindborg 1989) vased on physical findings
• Stage 1 : stomatitis includes erythematous mucosa, vesicles, mucosal ulcers, melanotic mucosal pigmentation and mucosal petechiae
• Stage 2 : fibrosis occurs on ruptured vesicles and ulcers when they heal . It is a hallmark of stage
• Stage 3 : sequelae of osmfleukoplakia is found in more than 25% individuals with osmfspeech and hearing deficits may occur because of involvement of
tongue and the Eustachian tubes

Management
• Behavioural therapy : patient counseling, stoppage of habit
• Medicinal therapy :
• hyaluronidase: topically shown to improve symptoms more quickly than steroids alone
• Mild cases : intra- lesional injection dexamethasone 4mg to reduce symptoms and surgical
splitting / excision of fibrous bands
• Recent study : intralesional injection of gamma interferon 3 times a week improves mouth
opening significantly

Oral lichen planus“a common chronic immunologic inflammatory mucocutaneous disorder that varies in appearance from keratotic(reticular/plaque like) to erythematous and ulcerated, affecting the stratified squamous epithelium”
• Affects .5—1% of worlds population• Approximately half patients with cutaneous lp, have oral involvement• Peak incidence– middle age• Female : male 2:1• Characteristically associated with persistent clinical course and resistance to most
conventional treatments

On Skin
• Flat-topped purple polygonal and pruritic popular rash
• Koebner phenomenon
ETIOLOGY AND PATHOGENESIS
• Both antigen specific and non specific mechanisms maybe involved in pathogenesis of OLP
• Antigen specific mechanism :
• Antigen presentation by basal keratinocyte
• Antigen specific keratinocyte killing by cd8+ cytotoxic t-cell
• Non specific mechanism:
• Mast cell degranulation
• Matrix metalloproteinase activation
• these mechanisms may combine to cause
T-cell accumulation in superficial lamina propria
Basement membrane disruption
Intra epithelial t- cell migration
Keratinocyte apoptosis
CLINICAL FEATURES
• Lesions usually symmetrical
• Frequently affects buccal mucosa ,tongue,gingiva,lip &palate
• Extra oral mucosal involvements –anogenital area ,conjunctiva,esophagus/larynx
• Approx 1.2 –5.3% lesion undergo malignant changes
• Hence regular follow up mandatory
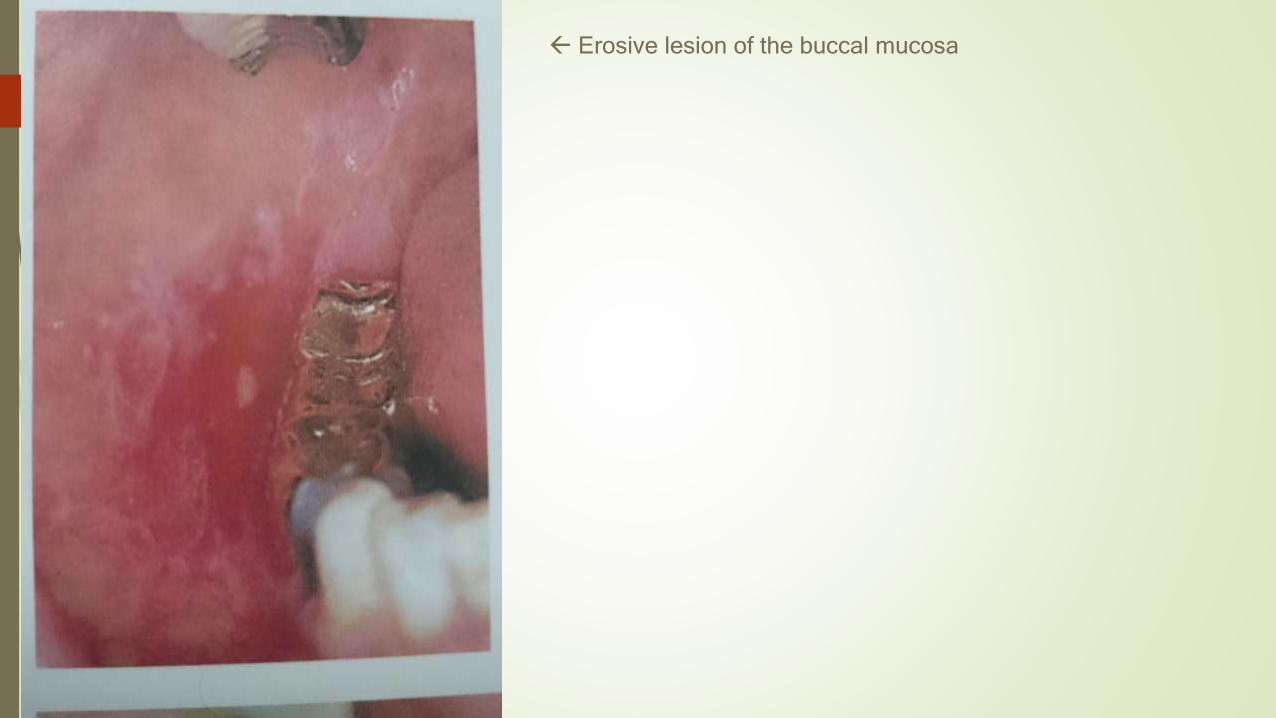
Erosive lesion of the buccal mucosa

ASYMPTOMATIC
• Reticular-wickham’s striae with or without discrete erythematous border
• Plaque like—resemble leukoplakia,common in smokers
SYMPTOMATIC
• Atrophic—diffuse red patch,peripheral radiating white striae
• Errosive --- irregular erosion covered with a pseudomembrane
• Bullous– small bullae /vesicles that may rupture easily
DIAGNOSIS
• ORAL BIOPSY
• DIRECT IMMUNOFLUORESCENCE
MANAGEMENT
• Reticular type is asymptomatic and treatment often unnecessary
• Errosive type presents significant management problems
• All patients should optimize oral hygiene
• Oral candiasis should be excluded/treated
• Corticosteroids is the treatment of choice e.g fluocinonide or clobestasol gel for 2 weeks with
months follow up

• In symptomatic patients with apparent contact dental factor , patch test with replacement of
amalgam
• In those with no apparent contact factor,topical or intra lesional steroid is the first line treatment. a
short course of systemic steroids for more rapid control
SIDEROPENIC DYSPHAGIAAKA “PLUMMER –VINSON SYNDROME,PATERSON –KELLY SYNDROME”
Definition
“Sideropenic dysphagia consists of iron deficiency anemia with associated dysphagia
the development of webs or strictures in the lower part of the hypopharynx or the upper part of the
esophagus.”
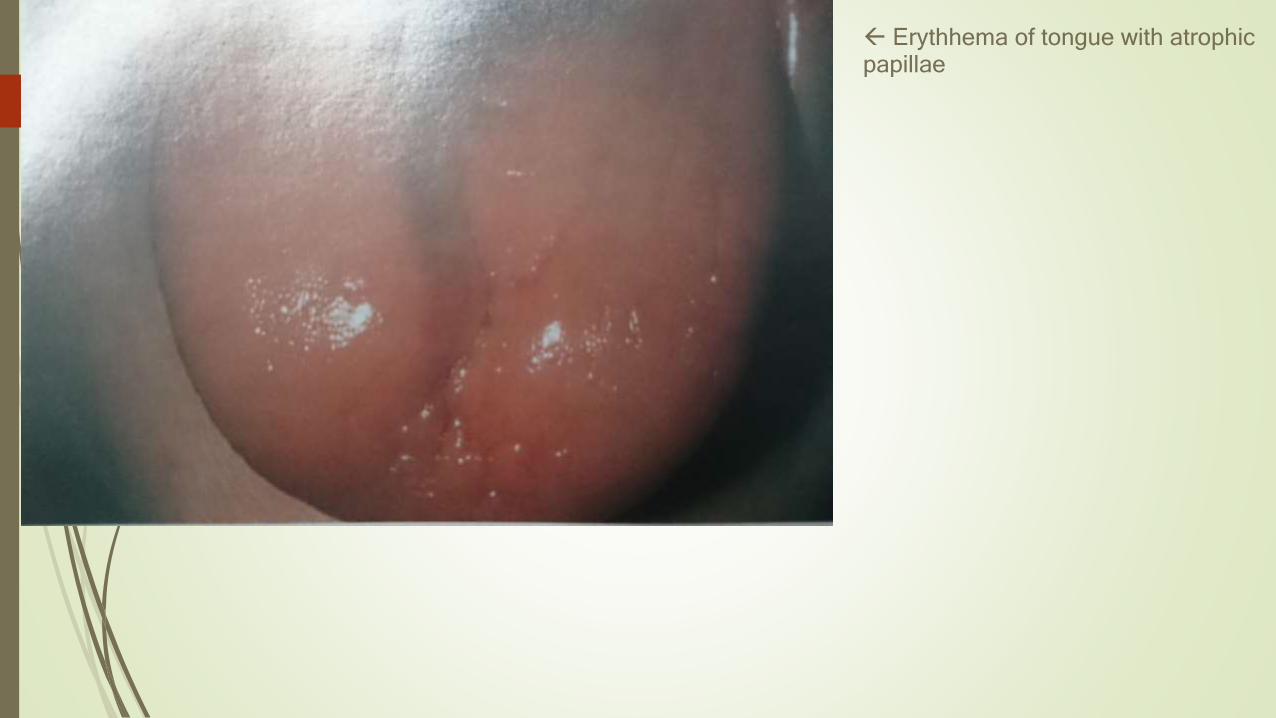
Erythhema of tongue with atrophic papillae
ETIOLOGY
• Chronic blood loss: Menstrual or post menopausal bleeding,parturition,bleeding hemorrhoids
• Decreased rate of absorption of iron: malabsorption syndromes,subtotal or complete gastrectomy
• Inadequate dietary intake of iron : poor economic status, anorexia and elderly individuals
• Increased requirements : growth spurts in infancy ,childhood and adolescence, prematurity
,pregnancy and lactation

CLINICAL FEATURES & PRESENTATION
• Almost exclusively in middle aged women, now uncommon due to improved nutritional conditions in
the community
• Presents with hypochromic, microcytic anemia with resultant pallor of the skin and atrophy of the
mucous membrane
• Atrophy of the tongue pappilae may lead to a smooth,red,painful glossitis.
• Angular chelitis also frequently seen.
• The condition is significant in that patients exhibit a significantly increased prevalence of carcinoma
of the esophagus,hypopharynx and oral cavity
TREATMENT AND PROGNOSIS
• The anemia responds well to iron therapy and a high protein diet
• Because of the predisposition to development of carcinoma of oral mucous membranes, early
diagnosis and treatment is necessary
• Dysphagia may improve with iron replacement in patients whose webs are not substantially
obstructive
• Advanced webs is unlikely to respond to iron replacements alone thus mechanical dilation is done
DYSKERATOSIS CONGENITA
DEFINITION
“Dyskeratosis congenital is a rare syndrome that is characterized by
defects of ectodermal structures plus bone marrow hypofunction”

Dystrophic nail changes
Atrophy of the dorsal tongue mucosa

CLINICAL FEATURES
• More than 80% of cases have occurred in males
• Transmitted most frequently as an X—linked recessive trait
• Despite the name ,it is not congenital begin to be noticed between 5 and 10 years of age.
• Reticulate hyperpigmentation is seen on the skin, especially face ,neck, upper arms and chest
• Nails become dystrophic
• Palms and soles show hyperhidrosis ,mostly associated with hyperkeratosis
• Progressive bone marrow failure occurs in half of all the cases causing thrombocytopenia,anemia
and leucopenia
• Oral involvement--- development of vesiculoerosive lesions on the tongue and buccal mucosa
• The dorsum of tongue may exhibit atrophy of the papillae smooth & shiny
• Most significant feature is frequent development of leukoplakia, which may involve tongue ,buccal
mucosa and labial mucosa
• Predisposition to malignancies, like carcinomas of gi system
TREATMENT
• Short term treatment options for bone marrow failure in patients with DKC
Include Erythropoietin and granulocytes colony—stimulating factor,howerver the only long term
curative option is allogeneic bone marrow transfer
• The frequency of malignant transformation of oral lesions would necessitate careful periodic
examination of patient for such an occurrence

DISCOID LUPUS ERYTHEMATOSISDEFINITION
“It is a chronic scarring,atrophy producing,photosensitive dermatosis”
• DLE may occur in patients with sle• Lesions may produce scarring or atrophy.scarring alopecia is particularly disturbing

ETIOLOGY
• In genetically predisposed individuals, but the exact genetic connection has not been
determined
• A heat shock protein is induced in the keratinocyte following ultraviolet(UV) light
exposure or stress, and this protein may act as a target for t cell mediated epidermal
cytotoxicity

CLINICAL FEATURES
• Relatively common• Occurs commonly in the 3rd and 4th decades• Women > Men• Sites: Face, Oral mucous membrane, chest, back and extremities• Lesions are slightly elevated red/purple macules that are often covered by gray or yellow adherent
scales• Forcefull removal of theses scales reveals numerous ‘carpet tack’ extension which had dipped into
enlarged pilosebaceous canalsORAL MANIFESTATION• More frequently seen associated with systemic form of DLE• The discoid form begins as erythematous area,elevated,desperesed ,without induration with white
spots• The margins of the lesions are not sharply demarcated but frequently the formation is a narrow
zone of keratinization
• Often,fine white striae radiate out from the margins
• In case of the tongue , atrophy of the papillae and severe fissuring are also seen
• The vermillion border,particularly the lower, is very common site
• The erythematous,atrophic plaques,surrounded by a keratotic border may involve the entire lip and
extend into the skin surface
TREATMENT/MANAGEMENT
• Goal of management is
to improve the appearance of the patient
To control existing lesions and limiting scarring
To prevent development of further lesions
• The prognosis of patients with chronic DLE is favorable regarding mortality; however many
patients continue to experience pain in their lesions or may experience disfigurement from the
scars or atrophy that can develop
REFERENCE
• Burket’s oral medicine diagnosis and treatment
• Textbook of oral pathology –shaefer
• Neville’s oral and maxillofacial pathology
• Emedicine-oral submucous fibrosis