Pregnancy induced Hypertension- Pathogenesis and pathological changes
15
PATHOGENESI S & PATHOLOGICA L CHANGES Ameer Salman
-
Upload
ameer-salman -
Category
Health & Medicine
-
view
133 -
download
5
Transcript of Pregnancy induced Hypertension- Pathogenesis and pathological changes

PATHOGENESIS &
PATHOLOGICAL CHANGES
Ameer
Salman
PATHOGENESIS OF PRE-ECLAMPSIA/
ECLAMPSIAChanges that occur during pregnancy contribute to the
development of preeclampsia:
➤ Vasospasm
➤ Absence of remodelling of spiral arteries
➤ Increased production of anti-angiogenic factors
➤ Retention of sodium

VASOSPASM
➤ resistance to blood flow
➤development of arterial
hypertension
➤also exerts damaging
effects on vessels

ABSENCE OF REMODELLING OF
SPIRAL ARTERIES In preeclampsia,
➤ cytotrophoblast cells infiltrate the decidual portion of
the spiral arteries, but fail to penetrate the
myometrial segment
➤ spiral arteries fail to develop into large, tortuous
vascular channels- resulting in placental
hypoperfusion (hypoperfused, ischemic placenta
releases several factors into maternal bloodstream
causing maternall endothelial dysfunction
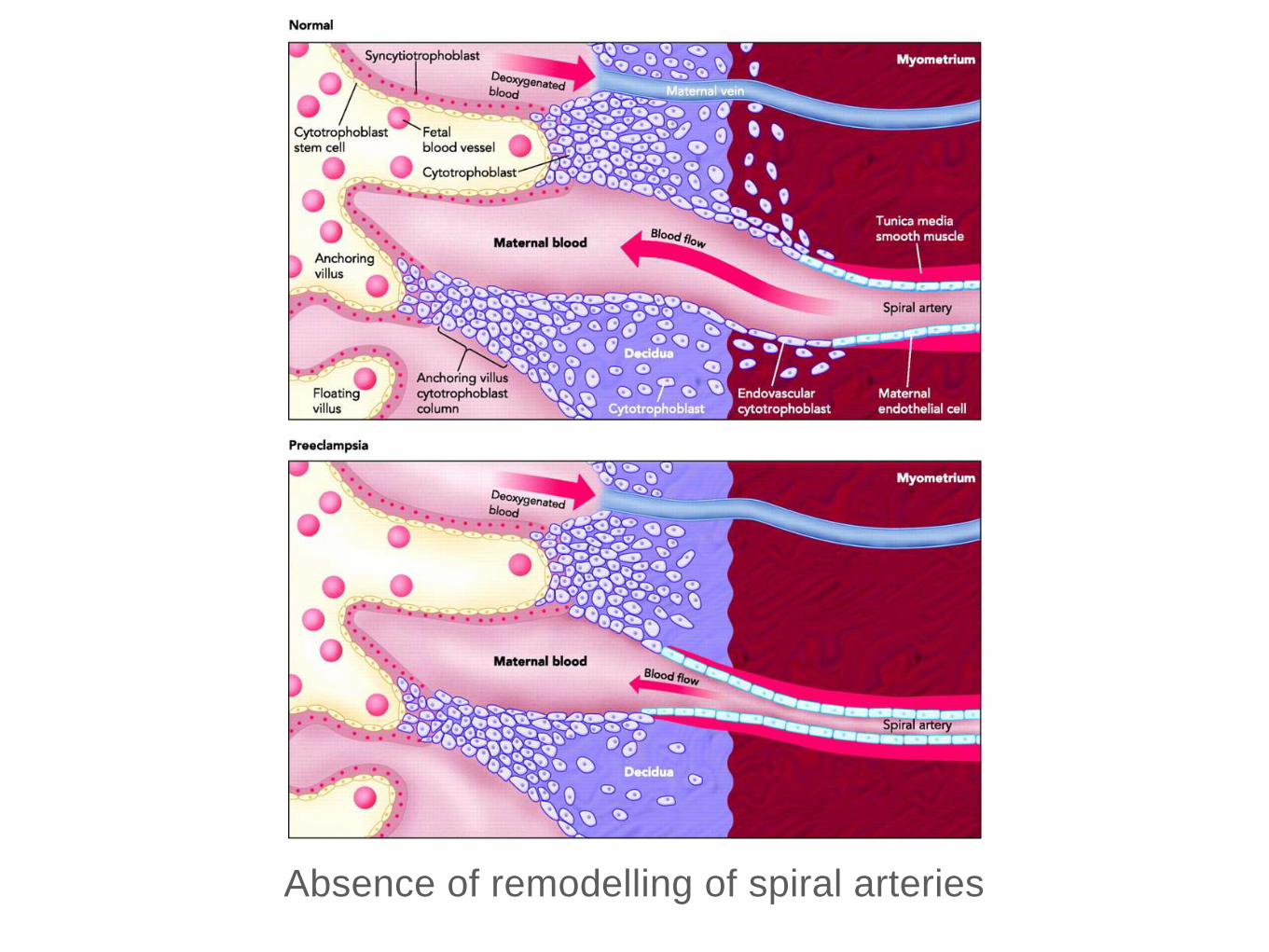
Absence of remodelling of spiral arteries
INCREASED PRODUCTION OF
ANTI-ANGIOGENIC FACTORS• A number of pro-angiogenic factors are elaborated by
placenta, like:
➤ VEGF- Vascular endothelial growth factor
➤ P1GF- Placental growth factor
➤ sEng- Soluble endoglins
• Balance among the above factors play a vital role for
normal placental development.
• Increased production antiangiogenic factors- disturbs
the balance-systemic endothelial dysfunction.
RETENTION OF SODIUM
• In normal pregnancy, there is marked increase in-
plasma volume, GFR & renal blood flow.
• Whereas in preeclampsia, it is characterised by-
➤ Reduced plasma volume
➤ Reduced GFR
➤ Reduced renal blood flow
➤ Hence, there is sodium retention and shift of
sodium into the arterial walls- increased sensitivity
to press or agents in preeclampsia.
PATHOLOGICAL
CHANGES

Impact of preeclampsia/eclampsia can be seen in most of
the vital structures, such as:
➤ Liver
➤ Kidneys
➤ Placenta
➤ Brain
LIVER
• Smooth surface with mottled appearance- numerous
scattered areas of subcapsular hemorrhage.
• Microscopically,
➤ Fibrin thrombi in the portal capillaries (periphery of
the lobules)
➤ Surrounding peripheral thrombi- areas of
haemorrhage and necrosis (periportal hemorrhagic
necrosis)
KIDNEYS
• In PID, there is an association with renal lesion.
• Enlarged glomeruli invading into the neck of the tubules
(Renal biopsy & electron microscopy)
• Microscopically,
➤ Endothelial cells are swollen, possibly blocking the
lumen of the capillaries.
➤ Cytoplasm shows vacuolation, droplet formation &
deposition.
➤ These causes glomerular endotheliosis
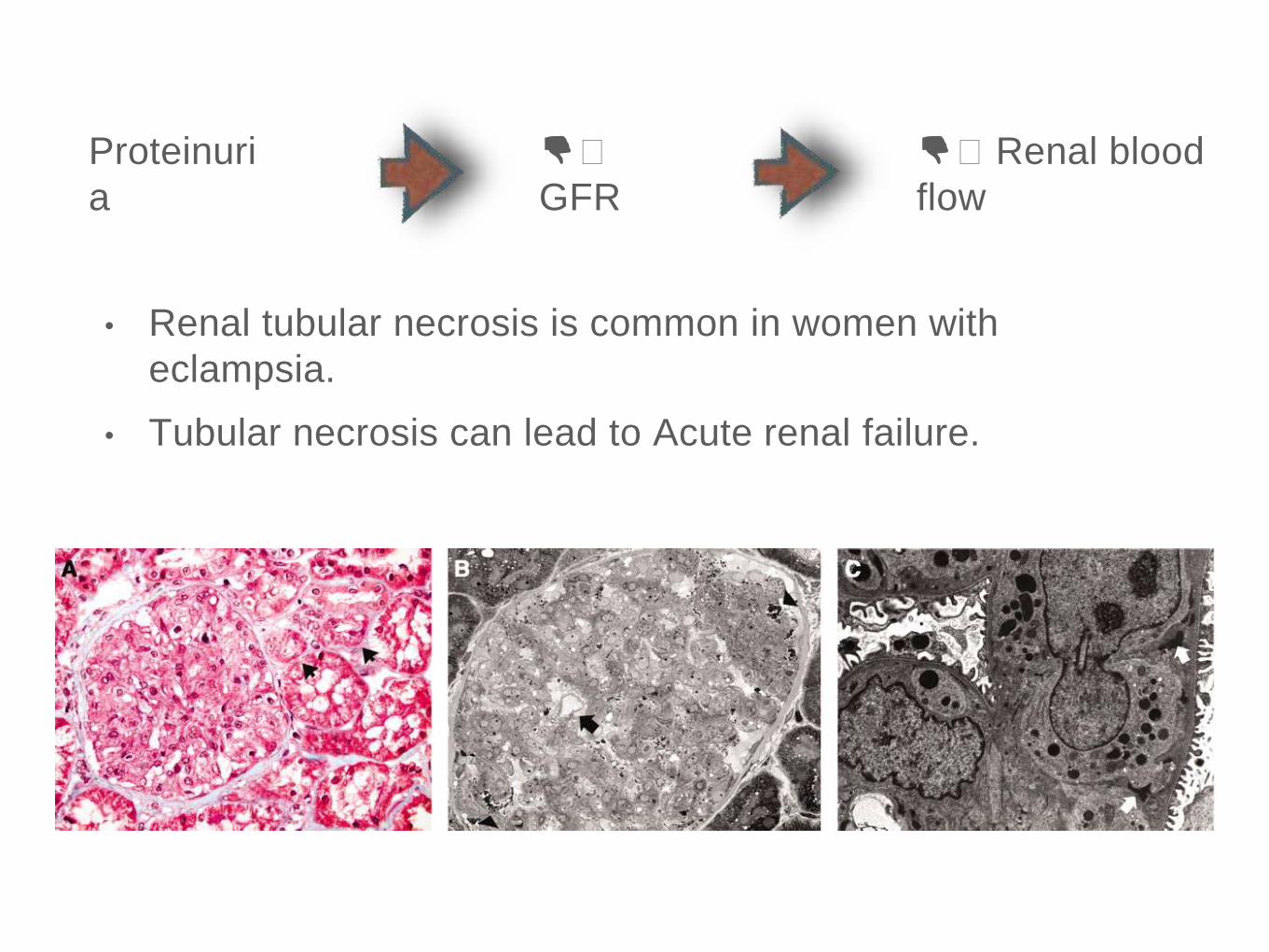
👎🏼
GFR
Proteinuri
a
👎🏼 Renal blood
flow
• Renal tubular necrosis is common in women with
eclampsia.
• Tubular necrosis can lead to Acute renal failure.
PLACENTA
• Vasospasm--->decreased uteroplacental blood flow-->
Anoxia--->liberation of thromboplastic substances--->
intravascular coagulation
BRAIN
• Gross haemorrhages due to ruptured arteries caused
by severe hypertension can be seen.
• Other findings that can be found include:
➤ Cerebral edema
➤ Hyperaemia
➤ Focal anemia
➤ Thrombosis
THANK YOU