Predictive Value of Preoperative Alpha-Fetoprotein and Des ... · Backgound • Milan criteria have...
19
Predictive Value of Preoperative Alpha-Fetoprotein and Des-gamma-Carboxy Prothrombin on Hepatocellular Carcinoma Recurrence after Liver Transplantation Juhan Lee 1 , Hyung Soon Lee 1 , Gi Hong Choi 1,2 , Dae Ryong Kang 3 , Dong Jin Joo 1,2 , Myoung Soo Kim 1,2 , Jin Sub Choi 1,2 , Soon Il Kim 1,2 The 38 th Congress of the Korean Association of HPB surgery Department of Surgery 1 , The Research Institute for Transplantation 2 and Graduate School of Public Health 3 Yonsei University Health System, Seoul, Korea
Transcript of Predictive Value of Preoperative Alpha-Fetoprotein and Des ... · Backgound • Milan criteria have...
Predictive Value of Preoperative Alpha-Fetoprotein
and Des-gamma-Carboxy Prothrombin
on Hepatocellular Carcinoma Recurrence after
Liver Transplantation
Juhan Lee1, Hyung Soon Lee1, Gi Hong Choi1,2, Dae Ryong Kang3,
Dong Jin Joo1,2, Myoung Soo Kim1,2, Jin Sub Choi1,2,
Soon Il Kim1,2
The 38th Congress of the Korean Association of HPB surgery
Department of Surgery1,
The Research Institute for Transplantation2 and
Graduate School of Public Health3
Yonsei University Health System, Seoul, Korea
Backgound
• Milan criteria have been accepted gold standard in LT for patients with HCC
• Radiological aspects alone are not fully able to select candidates
• Too restrictive and could be improved.
- more advanced HCCs either by expanding selection criteria or by offering
down-staging protocols.
Merani et al. J Hepatol. 2011;55(4):814-9
Backgound
• AFP and DCP seem to be a better surrogate markers for unfavorable tumor biology than
radiologic criteria.
• AFP and DCP are independently produced from HCC show no correlation with each other.
• These two markers might complement each other.
• Combined measurement of these two markers appears to be useful in predicting the
prognosis of HCC.
Tumor marker
Chon et al. Int J Cancer. 2012 15;131(10):2332-41

Purpose
• To assess whether the combined use of preoperative serum AFP and DCP levels
improve predictive performance of the Milan criteria for HCC recurrence after LT
- Design the Milan criteria based predictive model for HCC recurrence
- This model incorporated pre-transplant AFP and DCP respectively or simultaneously
Methods
• Retrospectively review with medical records
• Duration : 2001.10 - 2012.10
Inclusion criteria
Patients with HCC that received LT
Pathologically proven HCC
Exclusion criteria
Incidental HCC
Combined HCC-CCC
Without elevation of AFP and DCP
(AFP <9 ng/mL, DCP <35 mAU/mL)
Immediate post-op. mortality

Methods
: Base model (Quasi-Milan criteria) with adjusted age, sex, MELD score and pre-transplant treatment
Model 1. Base model + AFP
Model 2. Base model + DCP
Model 3. Base model + AFP + DCP
We compared a global concordance probability of the each models.
(integrated area under the curve, or iAUC)
New predictive model for HCC recurrence incorporating AFP and DCP
Methods
• To evaluate the predictive performance of each predictive model
: we employed the time-dependent receiver operating characteristic (ROC) curve
• As the recurrence is time dependent, time-dependent ROC curves are more
appropriate than conventional ones.
: disease onset usually varies by length of observation period

Results

Scheme of Patients Selection
LT for HCC
(n=210)
Post-op. mortality
(n=20)
Without
AFP and DCP elevation
(n=6)
HCC-CCC
(n=9)
Incidental HCC
(n=13)
Study population
(n=162)
Within the Milan criteria
(n=129)
Beyond the Milan criteria
(n=33)
Duration : 2001.10 - 2012.10
Median follow-up time: 23.5 months (range, 1-132)

Patient Characteristics
Characteristic Categories Patients (n=162)
Age (yrs) * 53 (37-67)
Gender Male/Female 137/25
Etiology of cirrhosis HBV 137 (84.5%)
HCV 15 (9.3%)
Non-B, Non-C 10 (6.2%)
Living donor LT 123 (75.9%)
Pre-transplant treatment No treatment 45 (27.8%)
TACE 75 (46.3%)
RFA 18 (11.1%)
Resection 17 (10.5%)
CCRT 7 (4.3%)
Within Milan criteria 129 (79.6%)
MELD score* 10 (5-34)
Tumor size (cm)* Radiologic 2.0 (0.8-8.3)
Tumor number* Radiologic 1.0 (1-7)
AFP (ng/mL)* 12.2 (0.8-3900)
DCP (mAU/mL)* 33.0 (5-2017)
E-S grade (major) I 46 (28.4%)
II 80 (49.4%)
III 11 (6.8%)
Total necrosis 100% necrosis 25 (15.4%)
Satellite nodule 20 (12.3%)
Microscopic vascular invasion 39 (24.1%)

Base model (Quasi-Milan criteria with adjusted variables)
: Age + Sex + MELD score + Pre-transplant treatment + Milan criteria
Model 1. Base model + AFP
Model 2. Base model + DCP
Model 3. Base model + AFP + DCP
Estimated ROC curves at 1 year after LT
1- specificity
Se
ns
itiv
ity
New predictive model of HCC recurrence incorporating AFP and DCP

Comparison of iAUC up to 40 months after LT in Each Models at Time-dependent ROC curve
• Model 0. Base
: iAUC = 0.794
• Model 1. Base + AFP
: iAUC = 0.826
• Model 2. Base + DCP
: iAUC = 0.821
• Model 3. Base + AFP + DCP
: iAUC = 0.855
Time after LT (Months)

Comparison of iAUC up to 40 months after LT in Each Model at Time-dependent ROC curve
Base model vs Model 1
: Not significant
(Estimated difference = -0.044, 95% CI = -0.131 to 0.004)
Base model vs Model 2
: Not significant
(Estimated difference = -0.032, 95% CI = -0.098 to 0.001)
Base model vs Model 3
: Significant
(Estimated difference = -0.069, 95% CI = -0.159 to -0.007)
Time after LT (Months)
Cut-off point of AFP and DCP
AFP = 140 ng/mL
DCP = 65 mAU/mL

Univariate Cox Regression Analysis of Recurrence (n = 162)
Variable Categories
Disease-free Survival
Hazard Ratio 95% Confidence Interval P
Age (continuous) 1-year increase 0.936 0.869-1.007 0.076
Gender Female vs Male 1.587 0.517-4.868 0.415
Type of transplantation Living donor vs Deceased donor 0.591 0.218-1.599 0.295
MELD score (continuous) 1 unit increase 0.987 0.902-1.079 0.766
Etiology of cirrhosis Other vs HBV 3.201 0.424-24.145 0.233
Milan criteria Within Milan vs Beyond Milan 8.276 3.118-21.966 <0.001
Pre-transplant treatment No vs Yes 2.759 0.631-12.067 0.160
AFP (ng/mL) and DCP (mAU/mL) AFP ≤140, DCP ≤65 vs AFP >140 and/or DCP >65 10.984 3.152-38.282 <0.001
Satellite Nodule No vs Yes 11.495 4.353-30.358 <0.001
Microscopic vascular invasion No vs Yes 11.651 3.795-35.770 <0.001
Total necrosis No vs Yes 0.292 0.039-2.206 0.204
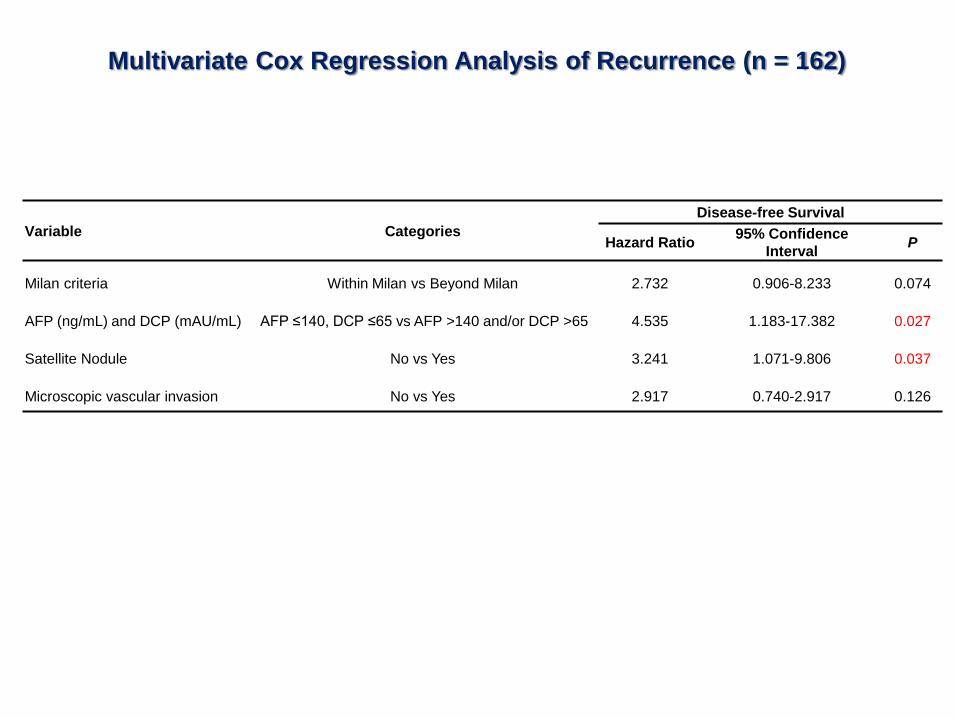
Multivariate Cox Regression Analysis of Recurrence (n = 162)
Variable Categories
Disease-free Survival
Hazard Ratio 95% Confidence
Interval P
Milan criteria Within Milan vs Beyond Milan 2.732 0.906-8.233 0.074
AFP (ng/mL) and DCP (mAU/mL) AFP ≤140, DCP ≤65 vs AFP >140 and/or DCP >65 4.535 1.183-17.382 0.027
Satellite Nodule No vs Yes 3.241 1.071-9.806 0.037
Microscopic vascular invasion No vs Yes 2.917 0.740-2.917 0.126
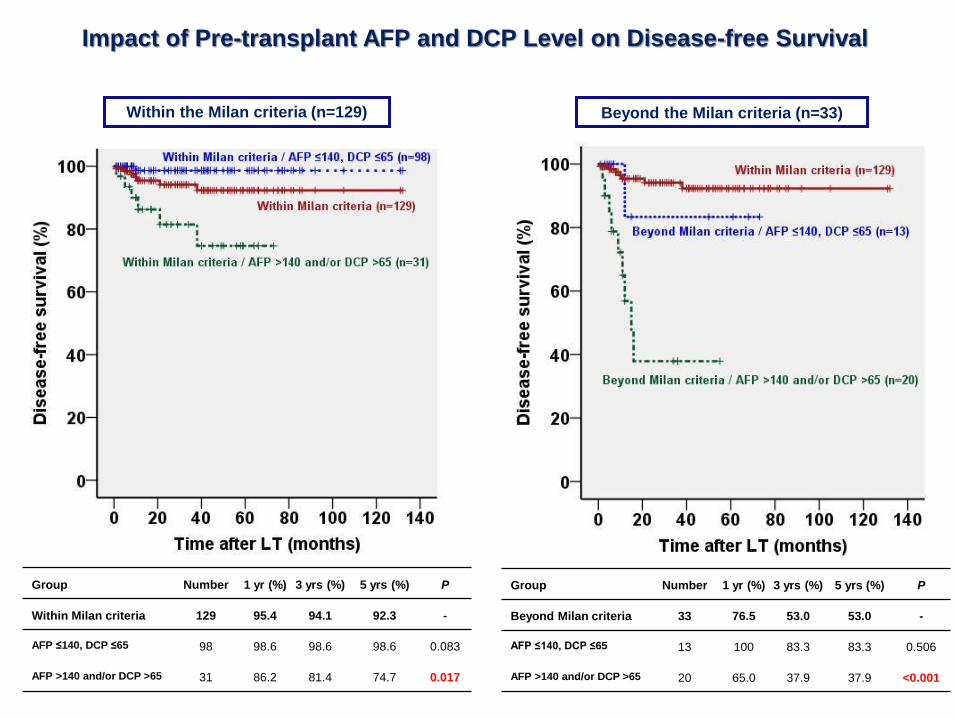
Impact of Pre-transplant AFP and DCP Level on Disease-free Survival
Within the Milan criteria (n=129) Beyond the Milan criteria (n=33)
Group Number 1 yr (%) 3 yrs (%) 5 yrs (%) P
Within Milan criteria 129 95.4 94.1 92.3 -
AFP ≤140, DCP ≤65 98 98.6 98.6 98.6 0.083
AFP >140 and/or DCP >65 31 86.2 81.4 74.7 0.017
Group Number 1 yr (%) 3 yrs (%) 5 yrs (%) P
Beyond Milan criteria 33 76.5 53.0 53.0 -
AFP ≤140, DCP ≤65 13 100 83.3 83.3 0.506
AFP >140 and/or DCP >65 20 65.0 37.9 37.9 <0.001
Combined use of preoperative serum AFP and DCP levels better predict the HCC
recurrence after LT when compared with the other predictive model.
Our results show that combined use of preoperative serum AFP and DCP is an
important prognostic factor for HCC recurrence after LT.
Summary
Thus, LT candidates with HCC can be assessed more accurately by adding pre-
transplant AFP and DCP levels to the Milan criteria.
Conclusion
Thank you for your attention