Bench-to-bedside review: Mechanisms of critical - BioMed Central

PREECLAMPSIA (VD GAROVIC, SECTION EDITOR)
Prediction of Preeclampsia-Bench to Bedside
Anjali Acharya & Wunnie Brima & Shivakanth Burugu &
Tanvi Rege
Published online: 21 September 2014# Springer Science+Business Media New York 2014
Abstract Hypertensive disorders of pregnancy (HDP) con-stitute the most common medical condition seen during ges-tation, effecting 1 in 10 pregnancies in the USA. Traditionally,preeclampsia (PE) is defined as a new onset of hypertensionand either proteinuria or end-organ dysfunction after 20 weeksof gestation in a previously normotensive woman. Preeclamp-sia is a potentially life-threatening condition with widespreadunderlying endothelial dysfunction, and accompanying in-flammation, vasoconstriction, and platelet activation. Womenwith preeclampsia are at an increased risk for life-threateningcomplications and progression to eclampsia.Worldwide, 10 to15 % of maternal deaths are from preeclampsia and relatedcomplications. Traditionally, diagnosis of preeclampsia ismade based upon presence of risk factors and clinical criteria.Diagnosis is challenging in asymptomatic women early inpregnancy as well as in nulliparous women as they lackobstetric history; however, it is well known that women withprevious preeclampsia have a 14.7 % risk of the condition inthe second pregnancy. Prediction of those at risk and earlydiagnosis is crucial to enable close surveillance of high-riskwomen in order to improve maternal and fetal outcomes.There has been much advance in our understanding of thepathogenesis of PE and in the field of angiogenic markers.However, no one test meets the criteria for a good biomarker.A multiparametric approach appears to be optimal as we await
newer systems biology approaches to give us better insightinto the pathogenesis of the disease.
Keywords Preeclampsia . Early onset preeclampsia (EoPE) .
Late onset preeclampsia (LoPE) . Systems biology .
Multiparametric testing . Epigenetics
Introduction
Hypertensive disorders of pregnancy (HDP) constitute themost common medical condition during gestation, impacting1 in 10 pregnancies in the USA and a much higher number inthe developing countries. The National High Blood PressureEducation Program of the NHLBI and the American Collegeof Obstetricians and Gynecologists (ACOG) [1] classifiesHDP into four major categories: preeclampsia/eclampsia,chronic hypertension, gestational hypertension, and preeclamp-sia superimposed upon chronic/preexisting hypertension.
Hypertension in pregnancy is defined as systolic bloodpressure ≥140 mmHg or diastolic blood pressure ≥90 mmHgon two occasions at least 4 hours apart after 20 weeks ofgestation in a previously normotensive woman [2]. Traditional-ly, preeclampsia (PE) is defined as a new onset of hypertensionand either proteinuria or end-organ dysfunction after 20weeks ofgestation in a previously normotensive woman. Severe hyper-tension and signs/symptoms of end-organ injury are consideredto be severe manifestations of the disease. In 2013, the AmericanCollege of Obstetricians and Gynecologists (ACOG) re-moved proteinuria as an essential criterion for diagnosis ofpreeclampsia. Oliguria and fetal growth restriction were alsoremoved as possible features of severe disease [1]. In patientswith new onset hypertension without proteinuria, the newonset of any of the following is diagnostic of preeclampsia:platelet count <100,000/μl, serum creatinine >1.1 mg/dl ordoubling of serum creatinine in the absence of other renal
This article is part of the Topical Collection on Preeclampsia
A. Acharya (*) : S. Burugu : T. RegeNephrology Division, Jacobi Medical Center, Albert EinsteinCollege of Medicine, Bronx, NY 10461, USAe-mail: [email protected]
W. BrimaAlbert Einstein College of Medicine, Bronx, NY 10461, USA
Curr Hypertens Rep (2014) 16:491DOI 10.1007/s11906-014-0491-3

disease, liver transaminases at least twice the normalconcentrations, pulmonary edema, and cerebral or visualsymptoms [1].
Preeclampsia is a condition with widespread endothelialdysfunction, along with accompanying inflammation, vaso-constriction, and platelet activation. Women with preeclampsiaare at an increased risk for life-threatening events, includingplacental abruption, acute kidney injury, cerebral hemorrhage,hepatic failure or rupture, pulmonary edema, disseminatedintravascular coagulation, and progression to eclampsia.Worldwide, 10 to 15% of maternal deaths are from preeclamp-sia and related complications [3]. In the USA, preeclampsia/eclampsia is one of the four leading causes of maternal deaths[4]. PE can present as late onset (LoPE) after 34 weeks or earlyonset (EoPE) disease, <34 weeks [2] of gestation, reported at2.72 and 0.38 %, respectively, in a population-based study [5].Fetal/neonatal morbidity and mortality are also higher from agreater risk of restricted fetal growth and iatrogenic pretermbirth. Recent epidemiologic data shows that women with HDPare at high risk of long-term cardiovascular consequences, aswell as insulin resistance and hyperlipidemia.
Diagnosis of preeclampsia is largely made based uponpresence of maternal risk factors and clinical criteria. Knownrisk factors for PE include past history of preeclampsia,nulliparity, family history of preeclampsia in a first-degreerelative, race, twin pregnancies, advanced maternal age, met-abolic syndrome, obesity, and underlying medical conditionssuch as gestational diabetes, hypertension, chronic kidneydisease, antiphospholipid antibody syndrome [2], and vascu-lar disease. Fetal trisomy is a well-known fetal risk factor [6].Analysis of the National Institute for Health and ClinicalExcellence (NICE) and Preeclampsia Community Guideline(PRECOG) show the limitations of using clinical maternalfactors in diagnosing PE [7]. Diagnosis is especially challeng-ing in nullipara as shown by the prospective Screening forPregnancy Endpoints (SCOPE) study, a multicenter cohortstudy [8]. The area under the curve (AUC) receiver operatingcharacteristics for clinical criteria was 0.76 and detected 37 %of women who developed preeclampsia with a false-positiverate of 10 %. Risk factor ascertainment thus severely fallsshort of expectations as a screening strategy [9].
There is a thrust for early diagnosis of PE as well asidentification of “at risk” women, with the goal to improvematernal and fetal outcomes by providing close surveillance.Risk stratification and early diagnosis will also enable identi-fication of women for prevention trials such as with aspirin,statins, and apheresis. In addition, differentiating PE fromother hypertensive disorders of pregnancy is equally impor-tant to avoid misdiagnosis and its attendant complications ofiatrogenic premature delivery. Though skeptics challenge theneed for an early biomarker due to lack of treatment other thandelivery, there is surely hope on the horizon for newer treat-ment strategies.
The quest for biomarkers has accelerated with the explo-sion of research in the area of placentology and a betterunderstanding of the molecular processes in placentation.The ideal biomarker should have the following: high sensitiv-ity, specificity, positive predictive, and negative predictivevalues; be easily available; and be minimally invasive, inex-pensive, rapid, and reproducible. It is quite evident that giventhe complex pathophysiology of PE, a single test will notsuffice as a biomarker. There is increasing evidence that thedifferent phenotypes, early vs. late onset and mild vs. severepreeclampsia, have differing pathophysiologies [10] and mayeven have a distinct biomarker profile.
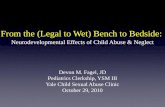
Systems Biology Approach Early on, angiogenic markerswere detected using ELISA assays which are plagued withhigh interassay variability. Newer automated systems over-come this limitation but await validation. With the advent ofhigh-dimensional biology or the “omics,” it is possible to havea holistic view of the molecules that make up an organ [11].Traditionally, the hypothesis-generating science of Omics in-cluded study of genes (genomics), messenger RNA (mRNA)(transcriptomics), proteins (proteomics), and metabolites(metabolomics) in a sample. The newer Omics include meth-ylation profiling (epigenetics), nanovesicles, and lipidomics(Fig. 1). The integration of these techniques called systemsbiology provides us the opportunity to evaluate the complexinteractions at the maternal fetal interface. Using platformtechnologies that can process multivariate and multiplex data,these systems biology approaches create large data requiringmathematical algorithms [12] and use of bioinformatics. Thisfield has tremendously enhanced our understanding of thepathogenesis of PE and advanced biomarker discovery.
Microarrays enable us to measure and analyze DNA se-quence and expression of thousands of genes simultaneously,but it is limited as it cannot measure protein. The tran-scriptome, the total mRNA in a cell or organism, reflectsgenes that are actively expressed at any given moment.RNA sequencing can provide information such as gene ex-pression levels, differential expression, alternative spliceforms, and novel transcripts, and is becoming the techniqueof choice. The proteome is the set of all expressed proteins in acell or organism. It reflects the interaction between genes andthe environment [13, 14] and is a great tool for biomarkerdiscovery. The metabolome, made up of many different mole-cules, is the final downstream product of gene transcription andis closest to the phenotype of the system. Mass spectrometry isthe most commonly used method for the identification ofanalytes in both proteomics and metabolomics. Other analyticalplatforms used in metabolomics include nuclear magnetic reso-nance (NMR) spectroscopy and infra-red spectroscopy.
Normal Placentation The placenta is a very unique and dy-namic organ confined to pregnancy. Precise coordination of
491, Page 2 of 12 Curr Hypertens Rep (2014) 16:491

several vascular processes including angiogenesis at the fetal–maternal interface and adequate cytotrophoblast (CTB) inva-sion with remodeling of the spiral arteries is crucial for normalplacentation. Disturbances in these processes lead to adversepregnancy outcomes and pregnancy-related disorders likepreeclampsia [15].
The current paradigm suggests that PE is a two-stagephenomenon resulting in the preeclampsia phenotype inpredisposed women.
1. Abnormal placentation is the initial insult leading to maldevelopment of uteroplacental perfusion.
2. Placental oxidative stress causes increased inflammatoryresponse, endothelial dysfunction, and an imbalance be-tween angiogenic and antiangiogenic factors.
Established Circulating Angiogenic Biomarkers Since thecrucial discovery of placental angiogenic and antiangiogenicfactors in the preeclampsia syndrome [16], there has beenmuch advance in the field of biomarkers. There has been aplethora of studies highlighting the association of preeclamp-sia with an abnormal pattern of circulating maternal pro an-giogenic and antiangiogenic factors and that the angiogenicimbalance antedates clinical manifestations of PE by at least5–6 weeks [17–21]. Test characteristics of biomarkers de-scribed below are summarized in Table 1.
Vascular Endothelial Growth Factor (VEGF)
VEGF is a potent proangiogenic glycoprotein essential formaintaining endothelial integrity and function. Polliotti et al.
reported that VEGF could be potentially useful as a tool forearly identification of patients at risk for developing severeEoPE [22]. Other studies, however, reported undetectableVEGF levels [23]. Overall, it is unreliable as a biomarker.
Placental Growth Factor (PlGF)
PlGF, a potent proangiogenic factor produced by the placenta,is a member of the VEGF sub-family that acts throughVEGFR1, potentiating the angiogenic activity of VEGF[24]. In normal pregnancy, PlGF levels rise until week 32and then decline [25]. Evidence shows that circulating PlGFlevels decrease early in pregnancy and several weeks beforethe onset of clinical symptoms of preeclampsia [23]. Though,by itself, it has a low sensitivity, Poon et al. show a 90 %detection rate of EoPE vs. 35 % detection of LoPE at a false-positive rate of 5 % when PlGF was used in combinationscreening [26] (described below under multiparametric tests).Myers et al. in the SCOPE study reported a 45 % sensitivity, a95 % specificity, and a positive likelihood ratio of 9 using acombination of clinical risk variables and PlGF measurementat 15 weeks gestation [27].
Soluble fms-Like Tyrosine Kinase 1 (sFlt1)
sFlt-1, produced mainly in the placenta [28], is a splice variantof VEGF receptor, which binds and neutralizes VEGF andPlGF with high affinity [29]. Maynard et al., in their seminalwork, demonstrated that administration of sFlt-1 into pregnantrats results in the preeclampsia phenotype [16]. Hypoxia [30]and oxidative stress from inflammatory stimuli [31] are majortriggers for the release of sFlt-1. Numerous studies havereported upregulation of placental sFlt1 mRNA and
Maternal Phenotype PE Fetal Phenotype
Maternal Clinical Risk Factors
Urine podocytes
Urine protein mRNA
Biophysical
UtAD
MAP
Genomics
Transcriptomics
Proteomics
Metabolomics
AngiogenicMarkers
Epigenetics
cff DNA
Exosomes
Nanovesicles
miRNA
Lipidomics
Multiparametric testing + Omic strategies
Fig. 1 Current biomarker tools inpreeclampsia
Curr Hypertens Rep (2014) 16:491 Page 3 of 12, 491

subsequent increase in circulating sFlt1 levels 5–6 weeks priorto the onset of clinical PE [32]. Myatt et al. reported a sensi-tivity and specificity of 77 % (95 % CI 50–93) and 80 %,respectively, of sFlt-1 in conjunction with clinical character-istics such as race, BMI, and BP to predict EoPE [33]. A casecontrol study by Powers et al., however, reported no suchcorrelation [34].
A superior performance of sFlt-1/PlGF ratio was demon-strated by many, to accurately identify women at risk ofpreeclampsia. Hassan et al. showed it to have an area underthe curve (AUC) from receiver operating characteristic (ROC)of 0.917 compared to the individual factors—0.875 and 0.855for sFlt-1 and PlGF, respectively. At a cutoff value for sFlt-1/PlGF ratio of 24.5, they reported a sensitivity of 91.6 %,specificity of 86.4 %, positive predictive value (PPV) of69.1 %, negative predictive value (NPV) of 96.9 %, positivelikelihood ratio (PLR) of 6.7, negative likelihood ratio (NLR)of 0.1, odds ratio (OD) of 67, and accuracy of 87.7 % [35].Another study showed similar results of high sFlt-1/PlGF ratioup to 4 weeks before clinical diagnosis in women who laterdeveloped preeclampsia when compared to controls. Thus in-creased sFlt-1/PlGF ratio appears to be a robust predictive
marker for the risk of developing preeclampsia and is recom-mended for use in triage of patients [36, 37]. Another screen-ing strategy is urinary screening for PlGF, followed by con-firmation with serum sFlt-1/PlGF ratio. PlGF is readily filteredby the glomerulus and a low concentration (<118 pg/ml) ofPlGF in the urine at midgestation was shown to be stronglyassociated with the subsequent development of preterm pre-eclampsia in a nested case control study [38]. The exact timingof measurement of this marker seems to be relevant as shownin a follow-up study which has questioned the validity ofUPlGF in predicting preterm preeclampsia. The authors showthat urinary PlGF, with or without normalization for urinarycreatinine, does not predict the development of preeclampsia[39]. Another study measuring urinary PlGF in the thirdtrimester demonstrated that a low level of urinary PlGFhelps discriminate different hypertensive disorders ofpregnancy [40].
Soluble Endoglin (sENG)
Endoglin is a co-receptor for transforming growth factor(TGF) beta and is expressed by vascular endothelial cells. Its
Table 1 Test characteristics of the biomarkers in preeclampsia
Biomarker Test characteristics Comments
Podocyte Sensitivity 100 %, specificity 100 % (115)
Sensitivity 38 %, specificity 70 %(116)Differences on population, antigens targeted,and technique
NICE (clinical)(6) Sensitivity 77 %, specificity 54 %, PPVof 7 % Prior history of PE was most discriminatory; notapplicable to nullipara
PRECOG (clinical)(6) Sensitivity 59 %, specificity 81 %, PPVof 11 %
SCOPE (clinical)(7) AUC 0.76, DR 37 % at FPR of 10 % Prospective study of nullipara
UtAD—biophysical(121) Sensitivity 43 %, specificity (67 %), PPVof 10 %,NPVof 93 %
A good rule out test in nullipara
cffDNA—(plasma)(108) Sensitivity 100 % Using RASSF1A hypermethylation; small sample
sFlt(37) Sensitivity 80 %, specificity 70 %
PlGF AUC 0.85, sensitivity for EOPE 90 %
sENG Sensitivity 80 %, specificity 84.6 %, PPV 84 %,NPV 81.5 %
sFlt/PlGF AUC 0.9, sensitivity 91 %, specificity 86 %,PPV 69 %, NPV 96.9 %
Multiparametric tests for EOPE
MAP (11–13 weeks)+MRF AUC 0.85
MRF, UtAD, MAP, PlGF, PAPP-A(25) 95 % DR at FPR 10 % Uses the competing risk model and detect the test withthe highest detection rate at 5 and 10 % FPR
MRF, UtAD, MAP, PAPP-A(25) 95 % DR at FPR 10 % Uses the competing risk model and detect the test withthe highest detection rate at 5 and 10 % FPR
MRF, UtAD, MAP, PAPP-A(125) 81 % DR
NICE National Institute for Health and Clinical Excellence, PlGF placental growth factor, SCOPE Screening for Pregnancy Endpoints, sENG solubleendoglin,DR detection rate, FPR false-positive rate, sFlt soluble fms-like tyrosine kinase-1,CffDNA cell-free fetal DNA, PAPP-A pregnancy-associatedplasma protein-A, PRECOG Preeclampsia Community Guideline, PPV positive predictive value, EOPE early-onset preeclampsia, NPV negativepredictive value, MAP mean arterial pressure, AUC area under the curve, UtAD uterine artery Doppler, MRF maternal risk factors
#(A notch or RI or PI MoM at or above the 75th percentile)
491, Page 4 of 12 Curr Hypertens Rep (2014) 16:491

soluble form, sENG, is known to cause endothelial dysfunc-tion by inhibiting TGF signaling [41, 42]. Circulating mater-nal level of sENG is elevated from 17 weeks of gestation inwomen who develop preeclampsia [17, 43, 44]. Levine et al.in the Calcium for Preeclampsia Prevention trial (CPEP)showed that there is a significant increase in circulating sENGlevels beginning 2 to 3 months before the onset of preeclamp-sia and levels correlate with disease severity [17]; De Vivoet al. [36] demonstrated a sensitivity, specificity, diagnosticaccuracy, PPV, and NPVof 80.8, 84.6, 82.7, 84, and 81.5 %,respectively, with no differential expression between womenwho developed EoPE and LoPE [36]. When used in additionto clinical characteristics such as race, BMI, and blood pres-sure at enrolment, Myatt et al. reported an AUC receiveroperating characteristic of 0.88 (95 % CI 0.83–0.93), and asensitivity and specificity of 88.2 and 80 %, respectively, ofsENG, for prediction of EOPE [33]. Placental protein-13(PP13) and pregnancy-associated plasma protein-A (PAPP-A), both derived from syncytiotrophoblast (STB), have beentested as predictors and show poor sensitivity. However, se-quential testing for PlGF, sENG, and sFlt at 6–15 weeks andagain at 20–25 weeks increased the sensitivity to 100 % andspecificity to 98 %. Of note, lower levels of these biomarkersare found in pregnant women who smoke. These women areknown to be at a lower risk of PE and the enzyme catechol-O-methyltransferase (COMT) is implicated [45].
Newer Candidate Serum Biomarkers In addition to the abovewell-established biomarkers, there are newer candidate bio-markers that are being studied in the clinical context that wereview below.
Proteases facilitate extravillous trophoblast (EVT) inva-sion of the maternal decidua [46]. Many novel proteasesystems such as matrix metalloproteinases (MMPs),galectin, cathepsins, and the serine protease urokinase-type plasminogen activator (uPA) have been identifiedwhich are potential candidates for circulating biomarkers.The syncytiotrophoblast (STB)-derived proteins, on theother hand, are biomarkers of a cellular stress responseand are involved in upregulation of proteins such as vas-cular endothelial growth factor receptor 1 (sVEGFR-1) anddown-regulation of others such as PlGF in the maternalcirculation [47].
Galectin-1 (Gal-1), a conserved protease, peaks in thesecond trimester [48–50], binds to neuropilin-1 (NRP-1) onendothelial cells, and promotes activation of the vascularendothelial growth factor receptor 2 (VEGFR2) signalingpathway [51]. Freitag et al. have shown that galectin inhibitioncauses dysregulated EVT invasion, inhibition of angiogenesis,thereby increasing the levels of AT1AA and sENG, andeventually leads to the PE phenotype. Placental and circulat-ing levels of galactoside-binding soluble 1 (Lgals1), the onlygalectin to be down-regulated in patients with PE, were
different between EoPE and LoPE, making Gal-1 a valuablebiomarker candidate [10].
The matrix metalloproteinases (MMPs), A disintegrin andmetalloproteinase domain (ADAM), and the secretedADAMTS belong to a superfamily of zinc proteinases, themetzincins. Both maternal and fetal MMPs are important forplacentation, and deficiency of either protease contributes todevelopment of PE. CTBs in PE produce less MMP9 [52] andMMP9 inhibition or gene silencing blocks CTB invasionin vitro [53]. Consistently low MMP levels were found inpatients with PE [54] along with recent reports of an MMP9variant in severe and EoPE [55]. Though the optimal thresholdlevel for MMP is unknown, it is a promising biomarker forsusceptibility to EoPE and even as a potential therapeutictarget. ADAM12 and a cathepsin called CTSL are otherpotential candidates under investigation [56].
Global transcriptional profiling [57] of the trophoblastexpression of an angiogenesis inhibitor SEMA3B shows dys-regulation of SEMA3B receptors, neuropilin-1 and 2 (NRP-1,2), in PE. SEMA3B opposes the actions of VEGF onangiogenesis by effecting PI3K/AKT and GSK3 signalingand the downstream targets of SEMA3B signaling such asadrenomedullin, Frizzle-related proteins, Wnt inhibitors arepotential novel targets for biomarker discovery. Using inte-grated proteomics, Myers et al. show insulin-like growthfactor acid labile subunit (IGFALS) to be a very predictivenovel preeclampsia biomarker [12]. This is a promisingadvance in diagnosis of PE in healthy nullipara.
Endothelial Microparticles (EMP) Diffuse endothelial cellinjury is the hallmark in the pathogenesis of PE [58–60].EMPs which are submicroscopic are shed from the endothelialcell wall upon activation or with apoptosis. They are beingexplored as markers of endothelial injury. Elevated levels ofEMPs have been documented in PE and in other disease stateswith known endothelial insult [61–63]. Petrozella et al. [63]showed direct endothelial insult in women with preeclampsia,while in another study, the EMP levels were shown to behigher in women with severe preeclampsia and eclampsiacompared to controls [64]. EMPs originate from various en-dothelial cell antigens with differing functions. CD31expressed at the endothelial cell junction is involved in main-taining the integrity of the endothelium. CD62E, a surfaceadhesion molecule, helps in recruiting leukocytes to the site ofinflammation. On the other hand, CD105, found on the vas-cular endothelium, is the non-soluble form of endoglin. Theantigenic type of the EMP also seems to vary by the patho-logic process involved, i.e., endothelial activation or apoptosis[65]. Though all three types of EMP were elevated in pre-eclampsia suggesting that both inflammation and apoptosisare at play, only apoptosis-associated EMPs exhibited apositive correlation with the sFlt1:PlGF ratio. Interestingly,CD31+/42− EMPs remained elevated at 1 week
Curr Hypertens Rep (2014) 16:491 Page 5 of 12, 491

postpartum suggesting persistent endothelial injury afterdelivery. It may explain the long-term cardiovascular mor-bidity seen in epidemiologic studies in women after HDP.EMPs may also have a role in identifying risk of pre-eclampsia in future gestations.
Exosomes and nanovesicles differ from microparticles intheir size and their mode of generation, and are a burgeoningfield of research [66, 67]. They are active and contain MHC IIantigen presenting molecules and transport mRNAs andmicroRNAs and bioactive lipids. In addition, they also carryfibronectin which plays a role in inflammation [68] andsyncytin which, along withWnt/bcatenin, is involved inmem-brane fusion in syncytiotrophoblasts [69–71]. Placenta-specific microRNAs originating from a “chromosome19microRNA cluster” have also been recovered in exosomesfrom the maternal circulation [72]. Given their structural sta-bility and ease of isolation, circulating exosomes lend them-selves as viable biomarker candidates. In addition, there isincreased shedding of microparticles due to activation ofproapoptotic p38 and SAPK/JNK MAPK and inflammatoryNF-κB pathways.
Their proinflammatory, procoagulant, and antiangiogenicproperties are also enhanced in preeclampsia [73, 74].
Lipidomics Dysregulated lipid metabolism secondary to up-regulation of proinflammatory cytokines and insulin resis-tance is emerging as one of the key players in the pathogenesisof PE. There is evidence that plasma from preeclampsiapatients shows differential expression of lipid metabolism-related proteins [75, 76]. Syncytiotrophoblast membranesshow sphingolipids (SM) to be the major lipid components[77]. SM is involved in inflammation, immune response, andoxidative stress [78], all processes which are upregulated inpreeclampsia. Despite reversal of sphingolipids/phosphatidylcholine (PC) ratio, total levels of PC which isinvolved in coagulation and apoptosis [79] was elevated. It isunknown whether these changes persist after delivery.
Epigenetics The phenotype and function of cells in the humanbody differ despite the same DNA sequence and program-ming. This is called epigenetics and refers to changes in geneexpression through mechanisms other than changes in theDNA nucleotide sequence. During development, differentiat-ed cells of various lineages accumulate epigenetic marks [80].Epigenetics allows phenotypic plasticity to the fetus in re-sponse to stress, nutrition, or other environmental factors[81]. DNA methylation, protein (histone modifications), ge-nomic imprinting, and expression of microRNA (miRNA)[82, 83] are important levels of epigenetic controls on tran-scription. Epigenetic modification at these three levels isimplicated in the defective trophoblast invasion of PE andmight provide critical insight into the pathogenesis of PE.Most of these modifications are studies in placental fetal
trophoblastic tissue, although some of these proteins modifiedin placental disease can be identified in the maternal plasma.
DNA methylation by addition of a methyl group to thecytosine/guanine-rich regions of DNA (“CpG” islands) resultsin transcriptional repression, whereas hypomethylation leadsto overexpression. Epigenetic modification of serine proteaseinhibitor (SERPIN) gene family, which regulates several path-ways of inflammation, coagulation, and complement activa-tion, is seen in PE placentas [84–86]; also, promoter of serineprotease inhibitor, SERPINA3, was significantlyhypomethylated in PE placentas compared to controls [87].Hypomethylation of CpG at the hypoxia-inducible factor(HIF)-1a binding sites leads to transcriptional induction inPE [88] and facilitates interaction of this transcriptional factorwith the SERPINA3 promoter. DNA methylation of variousloci was shown to be different in EoPE placentas compared toLoPE placentas [89, 90]. Kulkarni et al. have also foundincreased global DNA methylation levels in placentae ofwomen with LoPE [91]. These studies illustrate epigeneticalterations seen in the trophoblastic tissue from fetal side ofthe placenta.
Phosphorylation of the histone protein H2AX in responseto oxidative stress results in the formation of γH2AX foci andis a sensitive marker of DNA damage that can be identified byimmunohistochemistry. Both in vivo and in vitro [92] studieson placentas from PE patients have shown significantly higherexpression of γH2AX vs. normotensive controls and theyappear to be localized to the maternal cells of the decidua. Astatistically significant hypomethylation of CpG sites in ma-ternal systemic blood vessels has been shown in preeclampticwomen compared to controls. Hypomethylation of inflamma-tory genes such as thromboxane synthase (TBXAS1) geneand matrix metalloproteinase-1 (MMP-1) gene has also beenshown. These DNA methylation changes seen could predis-pose these women to an increased risk for cardiovasculardisease in later life [93]. There is a an imbalance in maternalcollagen-regulating genes with hypomethylation at MMP-1and MMP-8 genes and normal or hypermethylation of tissueinhibitor of metalloproteinase (TIMP) and collagen (COL)groups, suggesting their role in vascular dysfunction in pre-eclampsia [94]. There is evidence that this change is mani-fested in the maternal plasma as shown by the elegant work ofAuer et al. [95]. Incidentally, they also found elevated levels ofserum homocysteine levels, a key constituent of one-carbonmetabolism which could be epigenetically modified in PE.This has therapeutic implications and may explain the reducedrisk of PE shown with folic acid implying the importance ofmethylation [96]. Methylation alterations of trophoblastic cir-culating DNA in the maternal blood seem to be anotherpromising marker for early detection of preeclampsia [97].
There is abundant expression of miRNA in the placenta;placental miRNAs belong to three highly expressed clusters,C14MC, C19MC, and the miR-371-3 cluster, and play a role
491, Page 6 of 12 Curr Hypertens Rep (2014) 16:491

in gene silencing. miR-210, known to target hypoxia-inducible factor, was shown to be differentially expressed insevere PE [98, 99] compared to controls. On the contrary,Mayor-Lynn et al. [100] found no miR-210 alterations be-tween PE and control placentas. miR-155 which regulatesCYR61 [101, 102] and pri-miR-34a that regulates SERPINAare other candidates shown to be of significance [103]. Withthe current RNA sequencing capabilities, miRNAs hold agreat promise as biomarkers. Imprinting or silencing of eitherthe maternal or the paternal allele in conserved clusters ofgenes regulates trophoblast growth and has been implicated inthe pathogenesis of preeclampsia. Though imprinted Cdkn1cgene has shown to result in features of preeclampsia in mice[104], its role in human preeclampsia is unclear. Paternal H19imprinting was shown to lead to decreased trophoblast inva-sion and preeclampsia [105].
Cell-Free Fetal DNA
Georg Schmorl in 1893 initially described the presence ofplacental cells within the lungs of deceased preeclampticpatients [106]. Cell-free fetal (cff)DNA in maternal blood isnow gaining use for noninvasive prenatal diagnosis in aneu-ploidy; its role in PE is being explored. Lo et al. found afivefold increase in cffDNA by real-time quantitative PCR forthe SRY gene locus on the Y chromosome in maternal plasmaof 20 preeclamptic women and 20 gestational age-matchednormotensive controls from the third trimester [107]. Twoindependent investigators have demonstrated that elevationin maternal plasma cffDNA levels antedate onset of the clin-ical symptoms [108, 109]. It is surmised that placental hyp-oxia alternating with reperfusion triggers oxidative stress andSTB necrosis/apoptosis [110] causes release of fetal DNA intothe maternal circulation in PE [111].
Using DYS 14, a more sensitive assay, Zimmermann et al.demonstrated a 10-fold higher detection rate for cffDNA[112]. cffDNA level was shown to increase early, between11 and 13 weeks of gestation in patients with subsequentEoPE but not in LoPE when compared to controls.Gender-independent approaches using fetal RNA analysis,fetal epigenetic markers, such as DNA methylation, arebeing investigated. The maspin gene, which is specificallyhypomethylated in fetal tissue [113] or the promoter se-quence of RASSF1A [114] which is hypermethylated inthe placenta have been used for detection of fetal DNA inmaternal plasma. In a small retrospective study of 10patients, the sensitivity and specificity of cffDNA usingRASSF1A was 100 % [115]. Larger prospective studiesare awaited.
Podocytes and Preeclampsia Based on our knowledge ofother proteinuric diseases, it is natural that the proteinuria inpreeclampsia is attributed to podocyte injury. However, data
on this seems to show discordant results [116]. Garovic et al.first described a decrease in slit diaphragm proteins in pre-eclamptic kidney tissue on autopsies [117]. However, Redmanet al. have shown preservation of the podocyte foot process onelectron microscopy [15]. Another question that remains un-clear is if the podocyte damage is a cause rather than an effectof proteinuria in these women. Henao et al. have shown thatthe sera from women with preeclampsia directly affectpodocyte function [118]. Podocytes have been identified asthe main source of VEGF within the glomerulus [119]. Thepodocyte expresses the neuropilin-1 receptor that facilitatesVEGF binding on the surface with the plausibility for anautocrine loop in vivo [120]. Eremina et al. in their seminalwork developed knockout mice for podocyte-derived VEGF,with the mice showing a severe glomerular phenotype consis-tent with podocyte injury with dose-dependent effects ofVEGF [121]. Henao’s group also showed that VEGF supple-mentation can recover the barrier-forming capacity of thepodocyte [122].
Can podocytes or their injury markers be used as bio-markers in PE? Garovic’s group cultivated podocytes fromthe urine samples and stained them for podocyte-specificproteins podocin, nephrin, podocalyxin, and synaptopodin.They showed sensitivity and specificity of 100 % forpodocyturia in the urine of women with preeclampsia [123].Our group used synaptopodin to identify podocytes in theurine of high-risk women. We saw that podocyturia had asensitivity of only 38 % and a specificity of 70 % for diag-nosing preeclampsia [124]. These discrepant results could bedue to differing techniques, use of the choice of the podocyte-specific protein, interobserver variability in identifyingpodocytes, and difference in patient characteristics. In addi-tion, podocyturia, resulting from preeclampsia, cannot bedistinguished from podocyturia arising from an unrelatedglomerulopathy.
Clearly, we need more standardized techniques to avoidbias and overcome the limitations of this test. Using an ELISAassay for nephrin and podocalyxin, Wang et al. found thaturinary levels of these podocyte-injury biomarkers are elevat-ed in PE compared to healthy pregnant controls and those withhypertension [125]. Podocyte-specific mRNA for podocin,nephrin, and VEGF as markers have demonstrated elevatedlevels in PE as compared to healthy pregnant and non-pregnant controls. These studies also have indicated that theremay be low-grade podocyte shedding in normal pregnancywhich may explain the result from our group. Mass spectrom-etry method to measure podocyte proteins in the urine couldprovide more insight [126].
Biophysical Markers: Uterine Artery Doppler (UtAD)
Increased impedance to uterine blood flow in PE and ismanifested as an early diastolic notch [127]. The commonly
Curr Hypertens Rep (2014) 16:491 Page 7 of 12, 491

used indices in Doppler evaluation in clinical practice are asfollows:
1. Resistance index (RI) (resistive index or Pourcelot’sindex); RI=systolic-diastolic/systolic;
2. Systolic/diastolic (S/D) ratio, sometimes called the A/Bratio;
3. Pulsatility index (PI); PI=systolic−diastolic/[(systolic+diastolic)]/2.
Doppler assessment of the uteroplacental circulation in theprediction of preeclampsia has been studied extensively formany decades with disappointingly inconsistent results. Theseresults may be the consequence of differences in technique,differences in the populations examined, gestational age atstudy, and use of different clinical criteria for diagnosing PE.Recent studies use a more reproducible technique to assessflow in the uterine artery at the point where it crosses theexternal iliac artery. In several large prospective studies, uter-ine artery Doppler measurements done in the second trimestershowed utility in identifying women who develop preeclamp-sia [128]. It was shown to be most sensitive before 32 weeksof gestation [129].
A planned observational cohort of a larger randomizedcontrolled trial, Combined Antioxidant and Preeclampsia Pre-diction Studies (CAPPS), was conducted using stringent stan-dardized criteria. A notch or RI or PI multiples of median(MoM) at or above the 75th percentile were used as criteria forpredicting preeclampsia in 2,188 women. It yielded a sensi-tivity of 43 % and specificity of 67 %, positive predictivevalue of 10 % (95 % CI 8–12), negative predictive value of93 % (95 % CI 92–95), positive likelihood ratio of 1.29 (95 %CI 1.07–1.55), and negative likelihood ratio 0.86 (95 % CI0.75–0.98). Analyzing for time of onset and the severity ofpreeclampsia, it showed a sensitivity of 78 and 53 %, respec-tively. Doppler ultrasound measurements in the second tri-mester shows poor sensitivity for prediction of preeclampsiain low-risk nullipara in this well-conducted study [130]. Ofnote, the high negative predictive value makes it a useful rule-out test. A meta-analysis conducted by Cnossen et al. of 74studies with 79,547 patients revealed that combining highpulsatility index and early diastolic notch had a good predic-tive value for preeclampsia in the second but not in the firsttrimester of pregnancy [131].
Multiparametric Testing Several studies show improved pre-diction rate in multiparametric testing when UtAD is com-bined with angiogenic biomarkers. Using PAPP-A PlGF incombination with UtAD had a detection rate of more than95 % for EoPE but performed poorly in LoPE in a competingrisks model [26]. Another study, however, showed a detectionrate of only 81 % [132]. Other biomarkers studied in conjunc-tion with uterine artery Doppler are decreased placental
growth factor (PIGF) [133] concentration and elevated solublefms-like tyrosine kinase 1 (sFlt1) [134] showing similar re-sults. These combination tests have been validated in a Span-ish and Australian cohort with good results. The commerciallyavailable Perkins Elmer screening test uses a combination ofPlGF, PAPP-A, and biophysical studies of mean arterial pres-sure (MAP=the sum of the systolic and twice the diastolicblood pressures divided by three) and uterine artery Dopplerpulsatility index (UtAD). Sequential multiparametric testingneeds to be explored as screening tests.
Conclusion
Despite major advances, preeclampsia prediction prior to on-set of symptoms continues to be a challenge. Relying onclinical risk factors has been shown to be suboptimal. Recentyears have seen an enormous progress in the field of predictivemarkers with a plethora of studies but with discordant results.It is becoming increasingly clear that it is unlikely to find asingle screening test that meets the requisite sensitivity andspecificity and cost effectiveness profile. It is also evident thatdiagnosis of EoPE is easier than LoPE. Use ofmultiparametrictests using multiple biomarkers that reflect different aspects ofthe complex pathological processes involved in preeclampsiais a sensible approach. Advances in platform technologies,identifying new cellular pathways, high-content gene expres-sion tools, including microarrays, next generation RNA se-quencing, Bioinformatics tools, and the Omics approach pro-vide the necessary tools for the journey. Multimarker combi-nation tests with high detection rates and low false-positiverates seem very effective. As tools of risk stratification forpreeclampsia become available, wewill need to carefully auditoutcomes and be mindful of the cost effectiveness of thesestrategies. Economic analyses that will enable choice of testingmodalities are crucial in addressing this global health issue.
Compliance with Ethics Guidelines
Conflict of Interest Anjali Acharya, Wunnie Brima, ShivakanthBurugu, and Tanvi Rege declare no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
1. Hypertension in pregnancy. Report of the American College ofObstetricians and Gynecologists’ Task Force on Hypertension inPregnancy. Obstet Gynecol. 2013;122(5):1,122–31. doi:10.1097/01.aog.0000437382.03963.88.
2. Cunningham FG, LindheimerMD. Hypertension in pregnancy. N EnglJ Med. 1992;326(14):927–32. doi:10.1056/nejm199204023261405.
491, Page 8 of 12 Curr Hypertens Rep (2014) 16:491

3. Duley L. The global impact of pre-eclampsia and eclampsia. SeminPerinatol. 2009;33(3):130–7. doi:10.1053/j.semperi.2009.02.010.
4. Chang J, Elam-Evans LD, Berg CJ, Herndon J, Flowers L, SeedKA, et al. Pregnancy-related mortality surveillance—United States,1991–1999. MMWR Surveill Summ. 2003;52(2):1–8.
5. Lisonkova S, Joseph KS. Incidence of preeclampsia: risk factorsand outcomes associated with early- versus late-onset disease. Am JObstet Gynecol. 2013;209(6):544.el–e12.
6. Wright A, Zhou Y,Weier JF, Caceres E, KapidzicM, Tabata T, et al.Trisomy 21 is associated with variable defects in cytotrophoblastdifferentiation along the invasive pathway. Am J Med Genet A.2004;130a(4):354–64. doi:10.1002/ajmg.a.30254.
7. Verghese L, Alam S, Beski S, Thuraisingham R, Barnes I,MacCallum P. Antenatal screening for pre-eclampsia: evaluationof the NICE and pre-eclampsia community guidelines. J ObstetGynaecol. 2012;32(2):128–31. doi:10.3109/01443615.2011.635224.
8. North RA, McCowan LM, Dekker GA, Poston L, Chan EH,Stewart AW, et al. Clinical risk prediction for pre-eclampsia innulliparous women: development ofmodel in international prospec-tive cohort. BMJ. 2011;342:d1875. doi:10.1136/bmj.d1875.
9. Kane SC, Da Silva CF, Brennecke SP. New directions in theprediction of pre-eclampsia. Aust N Z J Obstet Gynaecol.2014;54(2):101–7. doi:10.1111/ajo.12151.
10. Freitag N, Tirado-Gonzalez I, Barrientos G, Herse F, Thijssen VL,Weedon-Fekjaer SM, et al. Interfering with Gal-1-mediated angio-genesis contributes to the pathogenesis of preeclampsia. Proc NatlAcad Sci U S A. 2013;110(28):11451–6. doi:10.1073/pnas.1303707110.
11. Horgan RP, Kenny LC. ‘Omic’ technologies: genomics, transcripto-mics, proteomics and metabolomics. Obstet Gynaecol. 2011;13(3):189–95. doi:10.1576/toag.13.3.189.27672.
12. Myers JE, Tuytten R, Thomas G, Laroy W, Kas K, Vanpoucke G,et al. Integrated proteomics pipeline yields novel biomarkers forpredicting preeclampsia. Hypertension. 2013;61(6):1281–8. doi:10.1161/hypertensionaha.113.01168.
13. Theodorescu D, Mischak H. Mass spectrometry based proteomicsin urine biomarker discovery. World J Urol. 2007;25(5):435–43.doi:10.1007/s00345-007-0206-3.
14. Vlahou A, Fountoulakis M. Proteomic approaches in the search fordisease biomarkers. J Chromatogr B Anal Technol Biomed Life Sci.2005;814(1):11–9. doi:10.1016/j.jchromb.2004.10.024.
15. Redman CW, Sargent IL. Latest advances in understanding pre-eclampsia. Science. 2005;308(5728):1592–4. doi:10.1126/science.1111726.
16. Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, et al.Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) maycontribute to endothelial dysfunction, hypertension, and proteinuriain preeclampsia. J Clin Invest. 2003;111(5):649–58. doi:10.1172/jci17189.
17. Levine RJ, Lam C, Qian C, Yu KF, Maynard SE, Sachs BP, et al.Soluble endoglin and other circulating antiangiogenic factors inpreeclampsia. N Engl J Med. 2006;355(10):992–1005. doi:10.1056/NEJMoa055352.
18. Chaiworapongsa T, Romero R, Kim YM, Kim GJ, Kim MR,Espinoza J, et al. Plasma soluble vascular endothelial growth factorreceptor-1 concentration is elevated prior to the clinical diagnosis ofpre-eclampsia. J Matern Fetal Neonatal Med. 2005;17(1):3–18. doi:10.1080/14767050400028816.
19. Hertig A, Berkane N, Lefevre G, Toumi K, Marti HP, Capeau J,et al. Maternal serum sFlt1 concentration is an early and reliablepredictive marker of preeclampsia. Clin Chem. 2004;50(9):1702–3.doi:10.1373/clinchem.2004.036715.
20. Romero R, Nien JK, Espinoza J, TodemD, FuW, Chung H, et al. Alongitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial
growth factor receptor-1) factors in normal pregnancy and patientsdestined to develop preeclampsia and deliver a small for gestationalage neonate. J Matern Fetal Neonatal Med. 2008;21(1):9–23. doi:10.1080/14767050701830480.
21. Wang A, Rana S, Karumanchi SA. Preeclampsia: the role of angio-genic factors in its pathogenesis. Physiology (Bethesda, Md).2009;24:147–58. doi:10.1152/physiol.00043.2008.
22. Polliotti BM, Fry AG, Saller DN, Mooney RA, Cox C, Miller RK.Second-trimester maternal serum placental growth factor and vas-cular endothelial growth factor for predicting severe, early-onsetpreeclampsia. Obstet Gynecol. 2003;101(6):1266–74.
23. Thadhani R, Mutter WP, Wolf M, Levine RJ, Taylor RN, SukhatmeVP, et al. First trimester placental growth factor and soluble fms-liketyrosine kinase 1 and risk for preeclampsia. J Clin EndocrinolMetab. 2004;89(2):770–5. doi:10.1210/jc.2003-031244.
24. Park JE, Chen HH, Winer J, Houck KA, Ferrara N. Placentagrowth factor. Potentiation of vascular endothelial growth fac-tor bioactivity, in vitro and in vivo, and high affinity binding toFlt-1 but not to Flk-1/KDR. J Biol Chem. 1994;269(41):25646–54.
25. Knudsen UB, Kronborg CS, von Dadelszen P, Kupfer K, Lee S-W,Vittinghus E, et al. A single rapid point-of-care placental growthfactor determination as an aid in the diagnosis of preeclampsia.Pregnancy Hypertens: Int J Women’s Cardiovasc Health.2012;2(1):8–15.
26. Poon LC, Kametas NA, Maiz N, Akolekar R, Nicolaides KH. First-trimester prediction of hypertensive disorders in pregnancy.Hypertension. 2009;53(5):812–8. doi:10.1161/hypertensionaha.108.127977.
27. Myers JE, Kenny LC, McCowan LM, Chan EH, Dekker GA,Poston L, et al. Angiogenic factors combined with clinical riskfactors to predict preterm pre-eclampsia in nulliparous women: apredictive test accuracy study. BJOG. 2013;120(10):1215–23. doi:10.1111/1471-0528.12195.
28. Li H, GuB, ZhangY, Lewis DF,WangY. Hypoxia-induced increasein soluble Flt-1 production correlates with enhanced oxidative stressin trophoblast cells from the human placenta. Placenta. 2005;26(2–3):210–7. doi:10.1016/j.placenta.2004.05.004.
29. Clark DE, Smith SK, He Y, Day KA, Licence DR, Corps AN, et al.A vascular endothelial growth factor antagonist is produced by thehuman placenta and released into the maternal circulation. BiolReprod. 1998;59(6):1540–8.
30. Munaut C, Lorquet S, Pequeux C, Blacher S, Berndt S, FrankenneF, et al. Hypoxia is responsible for soluble vascular endothelialgrowth factor receptor-1 (VEGFR-1) but not for soluble endoglininduction in villous trophoblast. HumReprod. 2008;23(6):1407–15.doi:10.1093/humrep/den114.
31. Redman CW, Sargent IL. Placental stress and pre-eclampsia: arevised view. Placenta. 2009;30 Suppl A:S38–42. doi:10.1016/j.placenta.2008.11.021.
32. Levine RJ,Maynard SE, Qian C, LimKH, England LJ, Yu KF, et al.Circulating angiogenic factors and the risk of preeclampsia. N EnglJ Med. 2004;350(7):672–83. doi:10.1056/NEJMoa031884.
33. Myatt L, Clifton RG, Roberts JM, Spong CY, Wapner RJ, Thorp JrJM, et al. Can changes in angiogenic biomarkers between the firstand second trimesters of pregnancy predict development of pre-eclampsia in a low-risk nulliparous patient population? BJOG.2013;120(10):1183–91. doi:10.1111/1471-0528.12128.
34. Powers RW, Roberts JM, Cooper KM, Gallaher MJ, Frank MP,Harger GF, et al. Maternal serum soluble fms-like tyrosine kinase 1concentrations are not increased in early pregnancy and decreasemore slowly postpartum in women who develop preeclampsia. AmJ Obstet Gynecol. 2005;193(1):185–91. doi:10.1016/j.ajog.2004.11.038.
35. Hassan MF, Rund NM, Salama AH. An elevated maternal plasmasoluble fms-like tyrosine kinase-1 to placental growth factor ratio at
Curr Hypertens Rep (2014) 16:491 Page 9 of 12, 491

midtrimester is a useful predictor for preeclampsia. Obstet GynecolInt. 2013;2013:202346. doi:10.1155/2013/202346.
36. De Vivo A, Baviera G, Giordano D, Todarello G, Corrado F,D’Anna R. Endoglin, PlGF and sFlt-1 as markers for predictingpre-eclampsia. Acta Obstet Gynecol Scand. 2008;87(8):837–42.doi:10.1080/00016340802253759.
37. Schoofs K, Grittner U, Engels T, Pape J, Denk B, Henrich W, et al.The importance of repeated measurements of the sFlt-1/PlGF ratiofor the prediction of preeclampsia and intrauterine growth restric-tion. J Perinat Med. 2014;42(1):61–8. doi:10.1515/jpm-2013-0074.
38. Levine RJ, Thadhani R, Qian C, Lam C, Lim KH, Yu KF, et al.Urinary placental growth factor and risk of preeclampsia. JAMA.2005;293(1):77–85. doi:10.1001/jama.293.1.77.
39. Savvidou MD, Akolekar R, Zaragoza E, Poon LC, Nicolaides KH.First trimester urinary placental growth factor and development ofpre-eclampsia. BJOG. 2009;116(5):643–7. doi:10.1111/j.1471-0528.2008.02074.x.
40. Campbell N, Ogle R, Thornton C, Hennessy A, Abbott J. Urinaryplacental growth factor differentiates the hypertensive disorders ofpregnancy. Aust N Z J Obstet Gynaecol. 2011;51(6):523–6. doi:10.1111/j.1479-828X.2011.01349.x.
41. Venkatesha S, Toporsian M, Lam C, Hanai J, Mammoto T, KimYM, et al. Soluble endoglin contributes to the pathogenesis ofpreeclampsia. Nat Med. 2006;12(6):642–9. doi:10.1038/nm1429.
42. Toporsian M, Gros R, Kabir MG, Vera S, Govindaraju K, EidelmanDH, et al. A role for endoglin in coupling eNOS activity andregulating vascular tone revealed in hereditary hemorrhagic telan-giectasia. Circ Res. 2005;96(6):684–92. doi:10.1161/01.res.0000159936.38601.22.
43. Rana S, Karumanchi SA, Levine RJ, Venkatesha S, Rauh-Hain JA,Tamez H, et al. Sequential changes in antiangiogenic factors in earlypregnancy and risk of developing preeclampsia. Hypertension.2007;50(1):137–42. doi:10.1161/hypertensionaha.107.087700.
44. Masuyama H, Nakatsukasa H, Takamoto N, Hiramatsu Y.Correlation between soluble endoglin, vascular endothelial growthfactor receptor-1, and adipocytokines in preeclampsia. J ClinEndocrinol Metab. 2007;92(7):2672–9. doi:10.1210/jc.2006-2349.
45. Kanasaki K, Palmsten K, Sugimoto H, Ahmad S, Hamano Y, Xie L,et al. Deficiency in catechol-O-methyltransferase and 2-methoxyoestradiol is associated with pre-eclampsia. Nature.2008;453(7198):1117–21. doi:10.1038/nature06951.
46. Pollheimer J, Fock V, Knofler M. Review: the ADAM metallopro-teinases—novel regulators of trophoblast invasion? Placenta.2014;35(Suppl):S57–63. doi:10.1016/j.placenta.2013.10.012.
47. Redman CW, Sargent IL, Staff AC. IFPA Senior Award Lecture:making sense of pre-eclampsia—two placental causes of pre-eclampsia? Placenta. 2014;35(Suppl):S20–5. doi:10.1016/j.placenta.2013.12.008.
48. Tirado-Gonzalez I, Freitag N, Barrientos G, Shaikly V, Nagaeva O,Strand M, et al. Galectin-1 influences trophoblast immune evasionand emerges as a predictive factor for the outcome of pregnancy.Mol Hum Reprod. 2013;19(1):43–53. doi:10.1093/molehr/gas043.
49. Fischer I, Redel S, Hofmann S, Kuhn C, Friese K, Walzel H, et al.Stimulation of syncytium formation in vitro in human trophoblastcells by galectin-1. Placenta. 2010;31(9):825–32. doi:10.1016/j.placenta.2010.06.016.
50. Kolundzic N, Bojic-Trbojevic Z, Kovacevic T, Stefanoska I,Kadoya T, Vicovac L. Galectin-1 is part of human trophoblastinvasion machinery—a functional study in vitro. PLoS ONE.2011;6(12):e28514. doi:10.1371/journal.pone.0028514.
51. Hsieh SH, YingNW,WuMH,ChiangWF, HsuCL,Wong TY, et al.Galectin-1, a novel ligand of neuropilin-1, activates VEGFR-2signaling and modulates the migration of vascular endothelial cells.Oncogene. 2008;27(26):3746–53. doi:10.1038/sj.onc.1211029.
52. Graham CH, McCrae KR. Altered expression of gelatinase andsurface-associated plasminogen activator activity by trophoblast
cells isolated from placentas of preeclamptic patients. Am J ObstetGynecol. 1996;175(3 Pt 1):555–62.
53. Librach CL, Werb Z, Fitzgerald ML, Chiu K, Corwin NM, EstevesRA, et al. 92-kD type IV collagenase mediates invasion of humancytotrophoblasts. J Cell Biol. 1991;113(2):437–49.
54. Kolben M, Lopens A, Blaser J, Ulm K, Schmitt M, Schneider KT,et al. Proteases and their inhibitors are indicative in gestationaldisease. Eur J Obstet Gynecol Reprod Biol. 1996;68(1–2):59–65.
55. Rahimi Z, Rahimi Z, Shahsavandi MO, Bidoki K, RezaeiM.MMP-9 (−1562 C:T) polymorphism as a biomarker of susceptibility tosevere pre-eclampsia. Biomark Med. 2013;7(1):93–8. doi:10.2217/bmm.12.95.
56. Varanou A, Withington SL, Lakasing L, Williamson C, Burton GJ,Hemberger M. The importance of cysteine cathepsin proteases forplacental development. J Mol Med (Berl). 2006;84(4):305–17. doi:10.1007/s00109-005-0032-2.
57. Zhou Y, Gormley MJ, Hunkapiller NM, Kapidzic M, Stolyarov Y,Feng V, et al. Reversal of gene dysregulation in culturedcytotrophoblasts reveals possible causes of preeclampsia. J ClinInvest. 2013;123(7):2862–72. doi:10.1172/jci66966.
58. Davidge ST. Oxidative stress and altered endothelial cell function inpreeclampsia. Semin Reprod Endocrinol. 1998;16(1):65–73. doi:10.1055/s-2007-1016254.
59. Lockwood CJ, Peters JH. Increased plasma levels of ED1+ cellularfibronectin precede the clinical signs of preeclampsia. Am J ObstetGynecol. 1990;162(2):358–62.
60. Nova A, Sibai BM, Barton JR, Mercer BM, Mitchell MD. Maternalplasma level of endothelin is increased in preeclampsia. Am JObstet Gynecol. 1991;165(3):724–7.
61. Gonzalez-Quintero VH, Jimenez JJ, Jy W, Mauro LM, Hortman L,O’Sullivan MJ, et al. Elevated plasma endothelial microparticles inpreeclampsia. Am J Obstet Gynecol. 2003;189(2):589–93.
62. Gonzalez-Quintero VH, Smarkusky LP, Jimenez JJ, Mauro LM, JyW, Hortsman LL, et al. Elevated plasma endothelial microparticles:preeclampsia versus gestational hypertension. Am J ObstetGynecol. 2004;191(4):1418–24. doi:10.1016/j.ajog.2004.06.044.
63. Petrozella L, Mahendroo M, Timmons B, Roberts S, McIntire D,Alexander JM. Endothelial microparticles and the antiangiogenicstate in preeclampsia and the postpartum period. Am J ObstetGynecol. 2012;207(2):140.e20–6. doi:10.1016/j.ajog.2012.06.011.
64. Reyna-Villasmil E, Mejia-Montilla J, Reyna-Villasmil N, Torres-Cepeda D, Pena-Paredes E, Santos-Bolivar J, et al. [Endothelialmicroparticles in preeclampsia and eclampsia]. Med Clin (Barc).2011;136(12):522–6. doi:10.1016/j.medcli.2010.07.026.
65. Jimenez JJ, JyW, Mauro LM, Soderland C, Horstman LL, Ahn YS.Endothelial cells release phenotypically and quantitatively distinctmicroparticles in activation and apoptosis. Thromb Res.2003;109(4):175–80.
66. Record M. Intercellular communication by exosomes in placenta: apossible role in cell fusion? Placenta. 2014;35(5):297–302. doi:10.1016/j.placenta.2014.02.009.
67. Harding C, Heuser J, Stahl P. Receptor-mediated endocytosis oftransferrin and recycling of the transferrin receptor in rat reticulo-cytes. J Cell Biol. 1983;97(2):329–39.
68. Atay S, Gercel-Taylor C, Suttles J, Mor G, Taylor DD. Trophoblast-derived exosomes mediate monocyte recruitment and differentia-tion. Am J Reprod Immunol. 2011;65(1):65–77. doi:10.1111/j.1600-0897.2010.00880.x.
69. Tolosa JM, Schjenken JE, Clifton VL, Vargas A, Barbeau B, LowryP, et al. The endogenous retroviral envelope protein syncytin-1inhibits LPS/PHA-stimulated cytokine responses in human bloodand is sorted into placental exosomes. Placenta. 2012;33(11):933–41. doi:10.1016/j.placenta.2012.08.004.
70. Gross JC, Chaudhary V, Bartscherer K, Boutros M. Active Wntproteins are secreted on exosomes. Nat Cell Biol. 2012;14(10):1036–45. doi:10.1038/ncb2574.
491, Page 10 of 12 Curr Hypertens Rep (2014) 16:491

71. Matsuura K, Jigami T, Taniue K, Morishita Y, Adachi S, Senda T,et al. Identification of a link between Wnt/beta-catenin signallingand the cell fusion pathway. Nat Commun. 2011;2:548. doi:10.1038/ncomms1551.
72. Bullerdiek J, Flor I. Exosome-delivered microRNAs of “chromo-some 19 microRNA cluster” as immunomodulators in pregnancyand tumorigenesis. Mol Cytogenet. 2012;5(1):27. doi:10.1186/1755-8166-5-27.
73. Redman CW, Sargent IL. Pre-eclampsia, the placenta and the ma-ternal systemic inflammatory response—a review. Placenta.2003;24 Suppl A:S21–7.
74. VanWijk MJ, Nieuwland R, Boer K, van der Post JA, VanBavel E,Sturk A. Microparticle subpopulations are increased in preeclamp-sia: possible involvement in vascular dysfunction? Am J ObstetGynecol. 2002;187(2):450–6.
75. Blumenstein M, McMaster MT, Black MA, Wu S, Prakash R,Cooney J, et al. A proteomic approach identifies early pregnancybiomarkers for preeclampsia: novel linkages between a predisposi-tion to preeclampsia and cardiovascular disease. Proteomics.2009;9(11):2929–45. doi:10.1002/pmic.200800625.
76. Liu C, Zhang N, Yu H, Chen Y, Liang Y, Deng H, et al. Proteomicanalysis of human serum for finding pathogenic factors and poten-tial biomarkers in preeclampsia. Placenta. 2011;32(2):168–74. doi:10.1016/j.placenta.2010.11.007.
77. Baig S, Lim JY, Fernandis AZ, Wenk MR, Kale A, Su LL, et al.Lipidomic analysis of human placental syncytiotrophoblastmicrovesicles in adverse pregnancy outcomes. Placenta.2013;34(5):436–42. doi:10.1016/j.placenta.2013.02.004.
78. Lahiri S, Futerman AH. The metabolism and function ofsphingolipids and glycosphingolipids. Cell Mol Life Sci.2007;64(17):2270–84. doi:10.1007/s00018-007-7076-0.
79. Leventis PA, Grinstein S. The distribution and function ofphosphatidylserine in cellular membranes. Annu Rev Biophys.2010;39:407–27. doi:10.1146/annurev.biophys.093008.131234.
80. Reik W. Stability and flexibility of epigenetic gene regulation inmammalian development. Nature. 2007;447(7143):425–32. doi:10.1038/nature05918.
81. Waterland RA, Jirtle RL. Early nutrition, epigenetic changes attransposons and imprinted genes, and enhanced susceptibility toadult chronic diseases. Nutrition. 2004;20(1):63–8.
82. Haluskova J. Epigenetic studies in human diseases. Folia Biol(Praha). 2010;56(3):83–96.
83. Szyf M. Epigenetics, DNA methylation, and chromatin modifyingdrugs. Annu Rev Pharmacol Toxicol. 2009;49:243–63. doi:10.1146/annurev-pharmtox-061008-103102.
84. Chelbi ST, Vaiman D. Genetic and epigenetic factors contribute tothe onset of preeclampsia. Mol Cell Endocrinol. 2008;282(1–2):120–9. doi:10.1016/j.mce.2007.11.022.
85. Silverman GA, Bird PI, Carrell RW, Church FC, Coughlin PB,Gettins PG, et al. The serpins are an expanding superfamily ofstructurally similar but functionally diverse proteins. Evolution,mechanism of inhibition, novel functions, and a revised nomencla-ture. J Biol Chem. 2001;276(36):33293–6.
86. Ness RB, Sibai BM. Shared and disparate components of thepathophysiologies of fetal growth restriction and preeclampsia.Am J Obstet Gynecol. 2006;195(1):40–9. doi:10.1016/j.ajog.2005.07.049.
87. Chelbi ST, Mondon F, Jammes H, Buffat C, Mignot TM, Tost J,et al. Expressional and epigenetic alterations of placental serineprotease inhibitors: SERPINA3 is a potential marker of preeclamp-sia. Hypertension. 2007;49(1):76–83. doi:10.1161/01.HYP.0000250831.52876.cb.
88. Wenger RH, Kvietikova I, Rolfs A, Camenisch G, Gassmann M.Oxygen-regulated erythropoietin gene expression is dependent on aCpG methylation-free hypoxia-inducible factor-1 DNA-bindingsite. Eur J Biochem. 1998;253(3):771–7.
89. Yuen RK, Penaherrera MS, von Dadelszen P, McFadden DE,Robinson WP. DNA methylation profiling of human placentasreveals promoter hypomethylation of multiple genes in early-onsetpreeclampsia. Eur J HumGenet. 2010;18(9):1006–12. doi:10.1038/ejhg.2010.63.
90. Higuchi T, Kanzaki H, Nakayama H, Fujimoto M, Hatayama H,Kojima K, et al. Induction of tissue inhibitor of metalloproteinase 3gene expression during in vitro decidualization of human endome-trial stromal cells. Endocrinology. 1995;136(11):4973–81. doi:10.1210/endo.136.11.7588231.
91. Kulkarni A, Chavan-Gautam P, Mehendale S, Yadav H, Joshi S.Global DNA methylation patterns in placenta and its associationwith maternal hypertension in pre-eclampsia. DNA Cell Biol.2011;30(2):79–84. doi:10.1089/dna.2010.1084.
92. Tadesse S, Kidane D, Guller S, Luo T, Norwitz NG, Arcuri F, et al. Invivo and in vitro evidence for placental DNA damage in preeclampsia.PLoS ONE. 2014;9(1):e86791. doi:10.1371/journal.pone.0086791.
93. Mousa AA, Archer KJ, Cappello R, Estrada-Gutierrez G, IsaacsCR, Strauss 3rd JF, et al. DNA methylation is altered in maternalblood vessels of women with preeclampsia. Reprod Sci.2012;19(12):1332–42. doi:10.1177/1933719112450336.
94. Mousa AA, Cappello RE, Estrada-Gutierrez G, Shukla J, RomeroR, Strauss 3rd JF, et al. Preeclampsia is associated with alterations inDNA methylation of genes involved in collagen metabolism. Am JPathol. 2012;181(4):1455–63. doi:10.1016/j.ajpath.2012.06.019.
95. Auer J, Camoin L, Guillonneau F, Rigourd V, Chelbi ST, Leduc M,et al. Serum profile in preeclampsia and intra-uterine growth restric-tion revealed by iTRAQ technology. J Proteome. 2010;73(5):1004–17. doi:10.1016/j.jprot.2009.12.014.
96. Wen SW, ChenXK, RodgerM,White RR,YangQ, Smith GN, et al.Folic acid supplementation in early second trimester and the risk ofpreeclampsia. Am J Obstet Gynecol. 2008;198(1):45.e1–7. doi:10.1016/j.ajog.2007.06.067.
97. Tong YK, Lo YM. Plasma epigenetic markers for cancer detectionand prenatal diagnosis. Front Biosci. 2006;11:2647–56.
98. Zhu XM, Han T, Sargent IL, Yin GW, Yao YQ. Differential expres-sion profile of microRNAs in human placentas from preeclampticpregnancies vs normal pregnancies. Am J Obstet Gynecol.2009;200(6):661.e1–7. doi:10.1016/j.ajog.2008.12.045.
99. ZhangY, FeiM, Xue G, ZhouQ, Jia Y, Li L, et al. Elevated levels ofhypoxia-inducible microRNA-210 in pre-eclampsia: new insightsinto molecular mechanisms for the disease. J Cell Mol Med.2012;16(2):249–59. doi:10.1111/j.1582-4934.2011.01291.x.
100. Mayor-Lynn K, Toloubeydokhti T, Cruz AC, Chegini N.Expression profile of microRNAs and mRNAs in human placentasfrom pregnancies complicated by preeclampsia and preterm labor.Reprod Sci. 2011;18(1):46–56. doi:10.1177/1933719110374115.
101. Dai Y, Diao Z, Sun H, Li R, Qiu Z, Hu Y. MicroRNA-155 isinvolved in the remodelling of human-trophoblast-derived HTR-8/SVneo cells induced by lipopolysaccharides. Hum Reprod.2011;26(7):1882–91. doi:10.1093/humrep/der118.
102. Zhang Y, Diao Z, Su L, Sun H, Li R, Cui H, et al. MicroRNA-155contributes to preeclampsia by down-regulating CYR61. Am JObstet Gynecol. 2010;202(5):466.e1–7. doi:10.1016/j.ajog.2010.01.057.
103. Doridot L, Houry D, Gaillard H, Chelbi ST, Barbaux S, Vaiman D.miR-34a expression, epigenetic regulation, and function in humanplacental diseases. Epigenetics : Off J DNA Methylation Soc.2014;9(1):142–51. doi:10.4161/epi.26196.
104. Kanayama N, Takahashi K,Matsuura T, Sugimura M, Kobayashi T,Moniwa N, et al. Deficiency in p57Kip2 expression inducespreeclampsia-like symptoms in mice. Mol Hum Reprod.2002;8(12):1129–35.
105. Yu L, Chen M, Zhao D, Yi P, Lu L, Han J, et al. The H19 geneimprinting in normal pregnancy and pre-eclampsia. Placenta.2009;30(5):443–7. doi:10.1016/j.placenta.2009.02.011.
Curr Hypertens Rep (2014) 16:491 Page 11 of 12, 491

106. Lapaire O, HolzgreveW, Oosterwijk JC, Brinkhaus R, Bianchi DW.Georg Schmorl on trophoblasts in the maternal circulation. Placenta.2007;28(1):1–5. doi:10.1016/j.placenta.2006.02.004.
107. Lo YM, Leung TN, Tein MS, Sargent IL, Zhang J, Lau TK, et al.Quantitative abnormalities of fetal DNA in maternal serum in pre-eclampsia. Clin Chem. 1999;45(2):184–8.
108. Leung TN, Zhang J, Lau TK, Chan LY, Lo YM. Increased maternalplasma fetal DNA concentrations in women who eventually devel-op preeclampsia. Clin Chem. 2001;47(1):137–9.
109. Zhong XY, HolzgreveW, Hahn S. The levels of circulatory cell freefetal DNA in maternal plasma are elevated prior to the onset ofpreeclampsia. Hypertens Pregnancy. 2002;21(1):77–83. doi:10.1081/prg-120002911.
110. Huppertz B, Kingdom J, Caniggia I, Desoye G, Black S, Korr H,et al. Hypoxia favours necrotic versus apoptotic shedding of pla-cental syncytiotrophoblast into the maternal circulation. Placenta.2003;24(2–3):181–90.
111. Knight M, Redman CW, Linton EA, Sargent IL. Shedding ofsyncytiotrophoblast microvilli into the maternal circulation inpre-eclamptic pregnancies. Br J Obstet Gynaecol. 1998;105(6):632–40.
112. Zimmermann BG, Holzgreve W, Avent N, Hahn S. Optimized real-time quantitative PCR measurement of male fetal DNA in maternalplasma. Ann N YAcad Sci. 2006;1075:347–9. doi:10.1196/annals.1368.047.
113. Chim SS, Tong YK, Chiu RW, Lau TK, Leung TN, Chan LY, et al.Detection of the placental epigenetic signature of the maspin gene inmaternal plasma. Proc Natl Acad Sci U S A. 2005;102(41):14753–8. doi:10.1073/pnas.0503335102.
114. Chan KC, Ding C, Gerovassili A, Yeung SW, Chiu RW, Leung TN,et al. Hypermethylated RASSF1A in maternal plasma: a universalfetal DNA marker that improves the reliability of noninvasiveprenatal diagnosis. Clin Chem. 2006;52(12):2211–8. doi:10.1373/clinchem.2006.074997.
115. Wang J, Yang J,Wu X,Mu Y, Li S, Cui K, et al. [Predictive value ofplacenta-derived RASSF1A sequence expression in maternal plas-ma for pre-eclampsia]. Zhonghua Yi Xue Yi Chuan Xue Za Zhi.2014;31(1):25–8. doi:10.3760/cma.j.issn.1003-9406.2014.01.006.
116. Henao DE, Mathieson PW, Saleem MA, Bueno JC, Cadavid A. Anovel renal perspective of preeclampsia: a look from the podocyte.Nephrol Dial Transplant. 2007;22(5):1477. doi:10.1093/ndt/gfl804.
117. Garovic VD, Wagner SJ, Petrovic LM, Gray CE, Hall P, SugimotoH, et al. Glomerular expression of nephrin and synaptopodin, butnot podocin, is decreased in kidney sections from women withpreeclampsia. Nephrol Dial Transplant. 2007;22(4):1136–43. doi:10.1093/ndt/gfl711.
118. Henao DE, Arias LF, Mathieson PW, Ni L, Welsh GI, Bueno JC,et al. Preeclamptic sera directly induce slit-diaphragm protein redis-tribution and alter podocyte barrier-forming capacity. Nephron ExpNephrol. 2008;110(3):e73–81. doi:10.1159/000166993.
119. Maharaj AS, Saint-Geniez M, Maldonado AE, D’Amore PA.Vascular endothelial growth factor localization in the adult. Am JPathol. 2006;168(2):639–48. doi:10.2353/ajpath.2006.050834.
120. Harper SJ, Xing CY, Whittle C, Parry R, Gillatt D, Peat D, et al.Expression of neuropilin-1 by human glomerular epithelial cellsin vitro and in vivo. Clin Sci (Lond). 2001;101(4):439–46.
121. Eremina V, Jefferson JA, Kowalewska J, Hochster H, Haas M,Weisstuch J, et al. VEGF inhibition and renal thrombotic
microangiopathy. N Engl J Med. 2008;358(11):1129–36. doi:10.1056/NEJMoa0707330.
122. Henao DE, Cadavid AP, SaleemMA. Exogenous vascular endothe-lial growth factor supplementation can restore the podocyte barrier-forming capacity disrupted by sera of preeclamptic women. J ObstetGynaecol Res. 2013;39(1):46–52. doi:10.1111/j.1447-0756.2012.01889.x.
123. Garovic VD, Wagner SJ, Turner ST, Rosenthal DW, Watson WJ,Brost BC, et al. Urinary podocyte excretion as a marker for pre-eclampsia. Am J Obstet Gynecol. 2007;196(4):320.e1–7. doi:10.1016/j.ajog.2007.02.007.
124. Jim B, Jean-Louis P, Qipo A, Garry D, Mian S, Matos T, et al.Podocyturia as a diagnostic marker for preeclampsia amongst high-risk pregnant patients. J Pregnancy. 2012;2012:984630. doi:10.1155/2012/984630.
125. WangY, Zhao S, Loyd S, Groome LJ. Increased urinary excretion ofnephrin, podocalyxin, and betaig-h3 in women with preeclampsia.Am J Physiol Ren Physiol. 2012;302(9):F1084–9. doi:10.1152/ajprenal.00597.2011.
126. Garovic VD, Craici IM, Wagner SJ, White WM, Brost BC, RoseCH, et al. Mass spectrometry as a novel method for detection ofpodocyturia in pre-eclampsia. Nephrol Dial Transplant. 2013;28(6):1555–61. doi:10.1093/ndt/gfs074.
127. McLeod L. How useful is uterine artery Doppler ultrasonography inpredicting pre-eclampsia and intrauterine growth restriction?CMAJ. 2008;178(6):727–9. doi:10.1503/cmaj.080242.
128. Papageorghiou AT, Yu CK, Nicolaides KH. The role of uterineartery Doppler in predicting adverse pregnancy outcome. BestPract Res Clin Obstet Gynaecol. 2004;18(3):383–96. doi:10.1016/j.bpobgyn.2004.02.003.
129. Papageorghiou AT, Yu CK, Bindra R, Pandis G, Nicolaides KH.Multicenter screening for pre-eclampsia and fetal growth re-striction by transvaginal uterine artery Doppler at 23 weeks ofgestation. Ultrasound Obstet Gynecol. 2001;18(5):441–9. doi:10.1046/j.0960-7692.2001.00572.x.
130. Myatt L, Clifton RG, Roberts JM, Spong CY, Hauth JC,Varner MW, et al. The utility of uterine artery Dopplervelocimetry in prediction of preeclampsia in a low-risk pop-ulation. Obstet Gynecol. 2012;120(4):815–22. doi:10.1097/AOG.0b013e31826af7fb.
131. Cnossen JS, Morris RK, ter Riet G, Mol BW, van der Post JA,Coomarasamy A, et al. Use of uterine artery Doppler ultrasonogra-phy to predict pre-eclampsia and intrauterine growth restriction: asystematic review and bivariable meta-analysis. CMAJ.2008;178(6):701–11. doi:10.1503/cmaj.070430.
132. Scazzocchio E, Figueras F, Crispi F, Meler E, Masoller N, Mula R,et al. Performance of a first-trimester screening of preeclampsia in aroutine care low-risk setting. Am J Obstet Gynecol. 2013;208(3):203.e1–e10. doi:10.1016/j.ajog.2012.12.016.
133. Espinoza J, Romero R, Nien JK, Gomez R, Kusanovic JP,Goncalves LF, et al. Identification of patients at risk for early onsetand/or severe preeclampsia with the use of uterine artery Dopplervelocimetry and placental growth factor. Am J Obstet Gynecol.2007;196(4):326.e1–13. doi:10.1016/j.ajog.2006.11.002.
134. Stepan H, Unversucht A, Wessel N, Faber R. Predictive value ofmaternal angiogenic factors in second trimester pregnancies withabnormal uterine perfusion. Hypertension. 2007;49(4):818–24. doi:10.1161/01.HYP.0000258404.21552.a3.
491, Page 12 of 12 Curr Hypertens Rep (2014) 16:491