Prediction and prevention of OHSS - an evidence-based approach Hassan N. Sallam, MD, FRCOG, PhD...
116
Prediction and prevention of OHSS - an evidence-based approach Hassan N. Sallam, MD, FRCOG, PhD (London) Professor in Obstetrics and Gynaecology The University of Alexandria, and Clinical and Scientific Director, Alexandria Fertility Center, Alexandria, Egypt 3rd Congress of Society of Reproductive Medicine, 5 – 9 October 2011, Antalya / Turkey
-
date post
18-Dec-2015 -
Category
Documents
-
view
214 -
download
0
Transcript of Prediction and prevention of OHSS - an evidence-based approach Hassan N. Sallam, MD, FRCOG, PhD...

Prediction and prevention of OHSS -
an evidence-based approachHassan N. Sallam,
MD, FRCOG, PhD (London)Professor in Obstetrics and Gynaecology
The University of Alexandria, andClinical and Scientific Director,
Alexandria Fertility Center, Alexandria, Egypt
3rd Congress of Society of Reproductive Medicine, 5 – 9 October
2011, Antalya / Turkey

The old Alexandria medical school

The uterus (after Soranos of Ephesus)

Ovarian hyperstimulation syndrome (OHSS)
Rabau et al, Am J Obstet Gynecol 98: 92, 1967

Ovarian hyperstimulation syndrome
Ovarian hyperstimulation syndrome (OHSS) is a rare iatrogenic
complication of ovarian stimulation occurring during the luteal phase or
during early pregnancy. It is potentially fatal and is difficult to predict. Fortunately, the reported prevalence of the severe form of
OHSS is small, ranging from 0.5 to 5%.

OHSS – a potentially fatal complication
Figueroa-Casas. Extraordinary ovarian reaction to gonadotropins: fatal case. Ann Circ (Rosario): 23: 116,
1958
Schenker and Weinstein. Ovarian hyperstimulation syndrome: a current survey. Fertil Steril 30: 255, 1978
Fineschi et al. An immunohistochemical study in a fatality due to ovarian hyperstimulation syndrome. Int
J Legal Med 120: 293, 2006
Madill et al. Ovarian hyperstimulation syndrome: a potentially fatal complication of early pregnancy. J
Emerg Med 35: 283, 2008

Early and late OHSS
Early onset OHSS3 to 7 days after HCG
Excessive response to stimulation
Late onset OHSS12 to 17 days after HCG
Due to pregnancy
Lyons et al, Hum Reprod. 9: 792, 1994; Mathur et al, Fertil Steril 73: 901, 2000
Classification (grading) of OHSS
• Rabau et al, 1967• Schenker and Weinstein, 1978
• Golan et al, 1989• Navot et al, 1992
• Rizk and Aboulghar, 1999
Rabau et al, Am J Obstet Gynecol 98: 92, 1967; Schenker and Weinstein, Fertil Steril 30: 155, 1978; Golan et al, Obstet Gynecol Surv 44: 430, 1989; Navot et al, Fertil Steril 58: 249, 1992; Rizk and Aboulghar,
Textbook of IVF and ART 9: 131, 1999

OHSS grading (Golan et al, 1989)
Ovary Symptoms/ signs
Grade 1 Abdominal distension
Grade 2 5-10 cm Nausea/ vomiting
Grade 3 >10 cm Ascites
Grade 4 > 12 cm Pleural effusion
Grade 5 Haemoconcentration oliguria
Mild
Moderate
Severe

Pathophysiology of OHSSPathophysiology of OHSSPathophysiology of OHSS
Prevention of OHSS
1. Prediction of OHSS2. Primary prevention (before
starting HMG/FSH)3. Secondary prevention (after
starting HMG/FSH and before HCG administration)

Evidence-based medicine
Level A – The recommendation based on good and
consistent scientific evidence (RCT)
Level B – The recommendation is based on limited or inconsistent scientific evidence (CT, cohort,
case control)
Level C – The recommendation is based primarily on consensus and expert opinion

Prevention of OHSS
1. Prediction of OHSS2. Primary prevention (before
starting HMG/FSH)3. Secondary prevention (after
starting HMG/FSH and before HCG administration)

Prediction of OHSS
(A) Risk factors: PCOS, young patients, low BMI, previous OHSS, pregnancy,
genetic predisposition(B) Biochemical indices: Plasma oestradiol peak, insulin resistance, serum VEGF, von Willebrand factor,
FSH, AMH(C) Ultrasound indices: PCO pattern, high
AFC, ovarian volume, low intra-ovarian vascular resistance

Prediction of OHSS
(A) Risk factors: PCOS, young patients, low BMI, previous OHSS, pregnancy,
genetic predisposition(B) Biochemical indices: Plasma oestradiol peak, insulin resistance, serum VEGF, von Willebrand factor,
FSH, AMH(C) Ultrasound indices: PCO pattern, high
AFC, ovarian volume, low intra-ovarian vascular resistance

Polycystic ovary syndrome(Chereau, 1844; Stein and Leventhal, 1934)
Read at a meeting of the Central Association of Obstetricians and Gynecologists, November 1 to 3, 1934, New Orleans, La

Relationship between PCOS and OHSS
Study Patients with OHSS
Controls P value
Smitz et al, 1990
50% (5/10) None (0/1663) <0.0001
MacDougall et al, 1992
63 % (5/8) None (0/1287) <0.0001
Delvigne et al, 1993
37 % (47/128) 15 % (38/256) <0.0001
Smitz et al, Hum Reprod 5: 933, 1990; MacDougall et al, Hum Reprod 7: 597, 1992; Delvigne et al, Hum Reprod 8:
1361, 1993
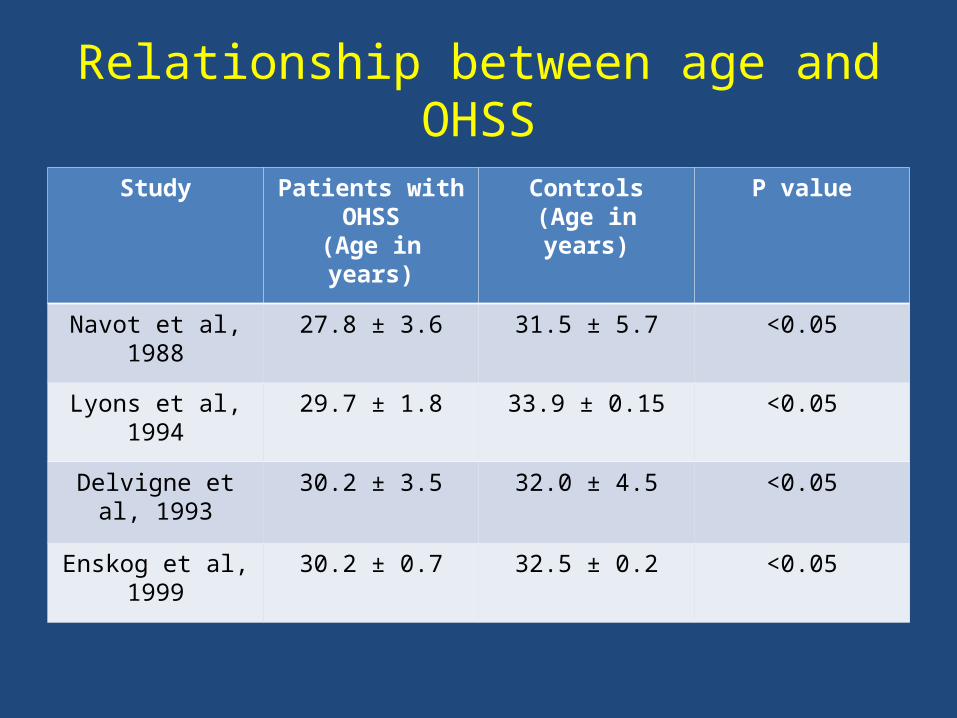
Relationship between age and OHSS
Study Patients with OHSS
(Age in years)
Controls(Age in years)
P value
Navot et al, 1988
27.8 ± 3.6 31.5 ± 5.7 <0.05
Lyons et al, 1994
29.7 ± 1.8 33.9 ± 0.15 <0.05
Delvigne et al, 1993
30.2 ± 3.5 32.0 ± 4.5 <0.05
Enskog et al, 1999
30.2 ± 0.7 32.5 ± 0.2 <0.05

Relationship between BMI and OHSS
Study Number of patients with
OHSS
Number of control
subjects
P value
Papanikolau et al, 2006
23.13 ± 0.8 23.05 ± 0.1 NS
Delvigne et al, 1993
22.0 ± 3.4 21.9 ± 3.2 NS
Enskog et al, 1999
23.2 ± 0.92 23.0 ± 0.16 NS
Papnikolau et al, Fertil Steril 85: 112, 2006; Delvigne et al, Hum Reprod 9: 1361, 1993; Enskog et al, Fertil Steril 71: 808,
1999

Genetic predisposition to predict OHSS
FSH receptor
FSH
FSH

Genetic predisposition to predict OHSS
Allelic frequencies
Genotypic frequencies
A T AA AT TT
Caucasian
controls
40% (78)
60 % (118)
17 % (17)
45 % (44)
38 % (37)
IVF controls
48 % (121)
52 % (131)
25 % (31)
47 % (59)
28 % (36)
OHSS patients
55 % (41)
45 % (33)
30 % (11)
51 % (19)
19 % (7)
P value NS NS NS NS NS
Daelemans et al, J Clin Endocrinol Metab 89:6310, 2004
Prediction of OHSS
(A) Risk factors: PCOS, young patients, low BMI, previous OHSS, pregnancy,
genetic predisposition(B) Biochemical indices: Plasma oestradiol peak, insulin resistance, serum VEGF, von Willebrand factor,
FSH, AMH(C) Ultrasound indices: PCO pattern, high
AFC, ovarian volume, low intra-ovarian vascular resistance

Plasma E2 concentration to predict OHSS
Cut-off valueFor E2 = 2560 ng/L
For follicles >12
Papanikolau et al, Fertil Steril 85: 112, 2006

Insulin resistance to predict OHSS in PCOS
Normo-insulinaemic
(n = 21)
Hyper-insulinaemic
(n = 31)
P value
Mean total dose of HMG ± SD
(IU)
1395 ± 472 1507 ± 727 NS
Mean dose/BMI ± SD (IU/BMI)
57.7 ± 18.7 54 ± 18 NS
Ovulation rate(n/cycle)
85.7 % (18/21) 83.8% (26/31) NS
OHSS rate(n/cycle)
23.8 % (5/21) 64.5 % (20/31) <0.05 *
Pregnancy rate(n/cycle)
28.5 % (6/21) 16% (5/31) NS
Abortions(n/pregnancies)
16.6 % (1/6) 20% (1/5) NS
Felghesu et al. JCEM 82: 644, 1997

Serum VEGF to predict OHSS
Early onset OHSS
Ludwig et al, Hum Reprod 13: 30, 1998
Late onset OHSS

Von Willebrand factor to predict OHSS
Todorow et al, Hum Reprod 8: 2039, 1993

Day 3 FSH to predict OHSS
Onagawa et al, Gynecol Endocrinol 18:335-40, 2004
Pregnant Non-pregnant P value
4.4+/-1.3 mIU/ml
6.1+/-2.9 mIU/ml
0.001
OHSS No OHSS P value
4.5+/-1.2 mIU/ml
5.9+/-2.8 mIU/ml
0.003
Cut-off point = 5.25 mIU/ml
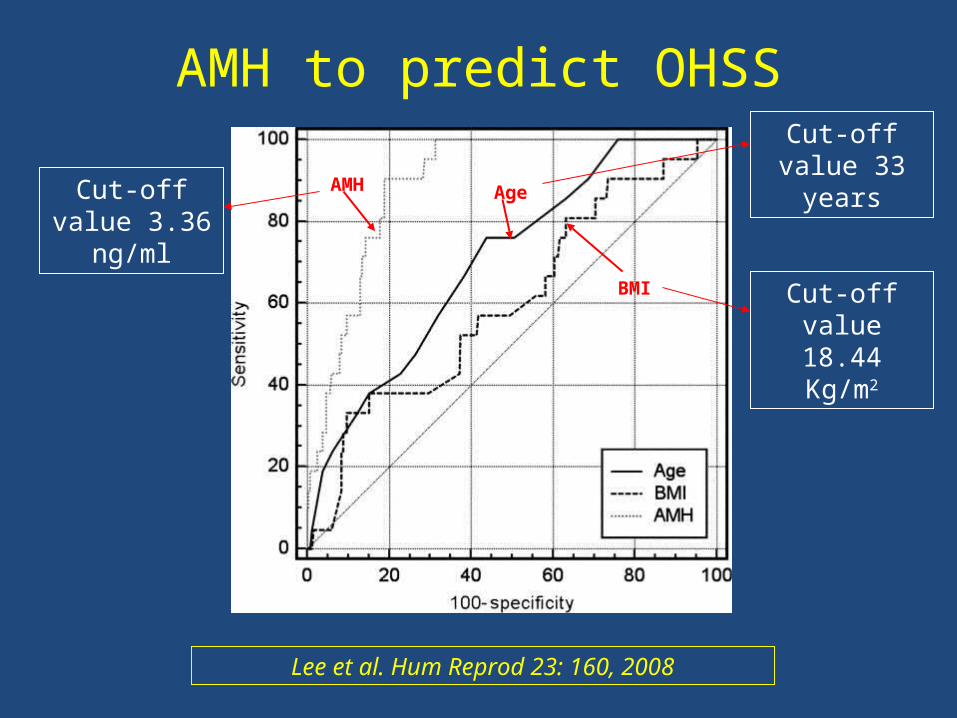
AMH to predict OHSS
Lee et al. Hum Reprod 23: 160, 2008
AMH Age
BMI
Cut-off value 3.36
ng/ml
Cut-off value 33
years
Cut-off value 18.44
Kg/m2

AMH to predict ovarian response
Early follicular Mid-luteal
Cut-off (ng/mL) 2.7 2.7
Sensitivity (%) 83.3 91.7
Specificity (%) 82.4 88.2
PPV (%) 76.9 84.6
NPV (%) 87.2 93.8
Accuracy (%) 82.8 89.6
Elgindy et al, Fertil Steril 89:1670, 2008

Prediction of OHSS
(A) Risk factors: PCOS, young patients, low BMI, previous OHSS, pregnancy,
genetic predisposition(B) Biochemical indices: Plasma oestradiol peak, insulin resistance, serum VEGF, von Willebrand factor,
FSH, AMH(C) Ultrasound indices: PCO pattern, high
AFC, ovarian volume, low intra-ovarian vascular resistance

PCO pattern to predict OHSS
Rizk and Smitz, Hum Reprod 7: 320, 1992; Delvigne et al, Hum Reprod 8: 1353,
1993

Antral follicle count(Tomas et al, 1997)
• Transvaginal ultrasound• After ovarian suppression with GnRHa and before starting FSH
• Follicles 2 to 5 mm in both ovaries• Patients with <5 follicles in both
ovaries were poor responders
Tomas et al, Hum Reprod 12(2):220, 1997

Trans-vaginal scan showing antral follicles
Right ovary Left ovary

AFC to predict ovarian response
Kwee et al, RBEJ 5:9, 2007
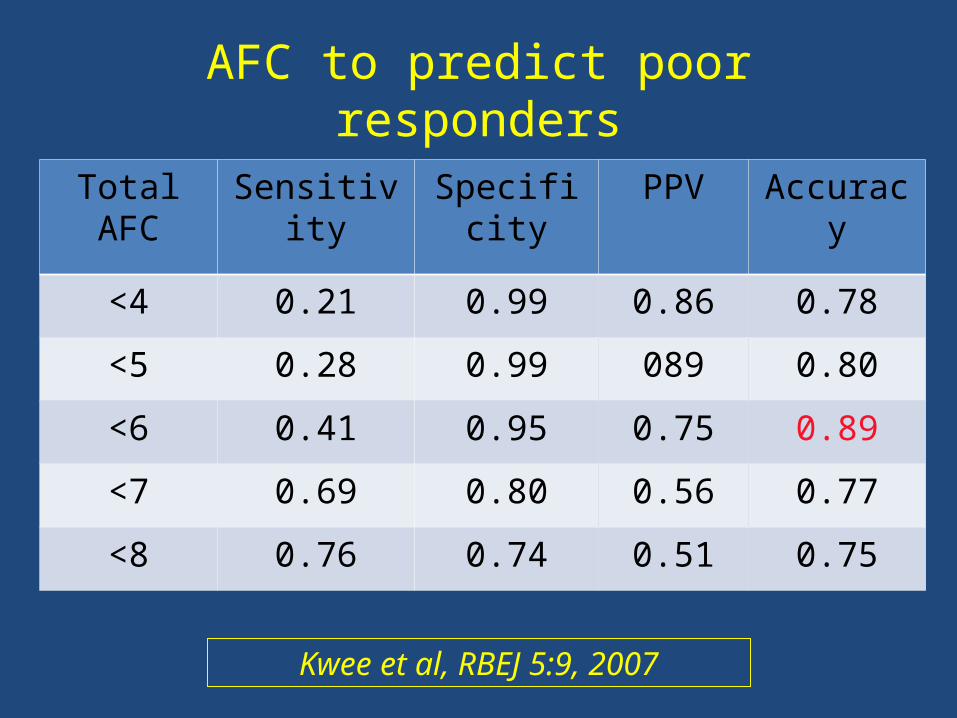
Total AFC
Sensitivity
Specificity
PPV Accuracy
<4 0.21 0.99 0.86 0.78
<5 0.28 0.99 089 0.80
<6 0.41 0.95 0.75 0.89
<7 0.69 0.80 0.56 0.77
<8 0.76 0.74 0.51 0.75
AFC to predict poor responders
Kwee et al, RBEJ 5:9, 2007

Total AFC
Sensitivity
Specificity
PPV Accuracy
<10 0.94 0.71 0.36 0.76
<12 0.88 0.80 0.44 0.81
<14 0.82 0.89 0.58 0.88
<16 0.47 0.96 0.67 0.88
<18 0.29 0.98 0.71 0.87
AFC to predict hyper responders
Kwee et al, RBEJ 5:9, 2007

AFC versus AMH to predict poor response
Hendricks et al, Fertil Steril 83(2): 291, 2005Broer et al, Fertil Steril 91: 705, 2009
AMH
AFC

AFC v/s AMH to predict hyper-response
Broer et al, Hum Reprod Update 17: 46, 2011
AFC
AMH

Predictors of OHSS (Sallam et al, 2011)
OHSS No OHSS P value
No. of cycles 11 22
Day 3 FSH (mIU/ml) 5.97 (2.05) 9.31 (3.01) 0.204
Day 3 LH (mIU/ml) 6.70 (3.14) 5.74 (3.64) 0.230
Day 3 E2 (pg/ml) 38.67 (14.41) 34.66 (9.00) 0.33
Day 3 leptin (ng/ml) 40.27 (28.06) 44.77 (25.71) 0.324
Day 3 VEGF (pg/ml) 438.00 (178.08)
448.27 (216.81)
0.446
Day 3 AFC 21.64 (3.20) 14.32 (3.81) < 0.0002*
Day 3 AMH (ng/ml) 4.50 (2.87) 2.17 (1.55) < 0.005*
E2 on HCG day (pg/ml)
5965.82 (1191.99)
2207.27 (659.32)
< 0.0001*
Sallam et al, Predictors of OHSS, submitted for publication

ROC curves comparing AMH and AFC
Sallam et al, Predictors of OHSS, submitted for publication
AFC
AMH
Cut-off value =>14
Cut-off value 3.36
ng/ml

Ovarian volume
Age Group
Mean Ovarian volume
(ml)
SD (ml)95%
Confidence Interval
% Ovaries Imaged
1 day to 3 months
1.06 0.96 0.03-3.56 70
4-12 months 1.05 0.67 0.18-2.71 100
13-24 months
0.67 0.35 0.15-1.68 90
2 -12 years 0.46 - 0.13-0.9 (range) -
13-20 years 4.0 - 1.8-5.7 (range) -
Cohen et al, AJR 160: 583, 1993; Orsini et al, Radiology 153:113, 1984; Sample et al. Radiology 125:477, 1977; Ivarsson et al, Arch
Dis Child 58, 352, 1983

Ovarian volume
Ivarsson et al, Arch Dis Child 58, 352, 1983

3-D U/S in obstetrics and gynaecology

Ovarian volume to predict OHSS
OHSS Controls P value
No. of patients 8 86
Days of stimulation 10.5 ± 2.5 10.5 ± 1 8 NS
Oestradiol (pg/ml) 2439 ± 1350 937 ± 686 0.0001
No. of follicles 23.3 ± 4.3 13.8 ± 7.5 0.0025
No. of oocytes 164 ± 26 5.9 ± 3 0 0.0001
Cycle length 34.1 ± 5.8 28.7 ± 2 2 0.0001
Body wt before stimulation
55.4 ± 3.8 62.8 ± 11 0.011
Body wt after stimulation 54 3 ± 4.5 62.9 ± 10. 7 0.03
Ovarian volume (ml) 13.2 ± 5 8.9 ± 3.7 0.035
Danninger et al, Hum Reprod 11: 1597, 1996

Perifollicular blood flow to predict OHSS
Oyesanya, Fertil Steril 65: 874, 1996

Intrafollicular hemodynamics to predict OHSS
OHSS Controls P value
Mean age (years) 32.63 ± 1.77 31.48 ± 3.87 NS
Mean duration of infertility (years)
6.00 ± 2.19 5.29 ± 2.73 NS
Maximal peak systolic velocity
0.15 ± 0.04 0.21 ± 0.10 NS
Mean minimal pulsatility index
0.89 ± 0.30 0.79 ± 0.14 NS
Mean minimal resistance indexes
0.56 ± 0.05 0.53 ± 0.06 NS
Oyesanya, Fertil Steril 65: 874, 1996

Combination of indices to predict OHSS
Regression analysis showed that the dependent factors were: (1) Log oestradiol, (2) Slope of log oestradiol, (3) HMG dosage, (4) No. of oocytes
retrieved and (5) LH/FSH ratio. The following formula was devised:
Delvigne et al, Hum Reprod 8: 1353, 1993
PPV = 78.5 %; FNR = 18.1%
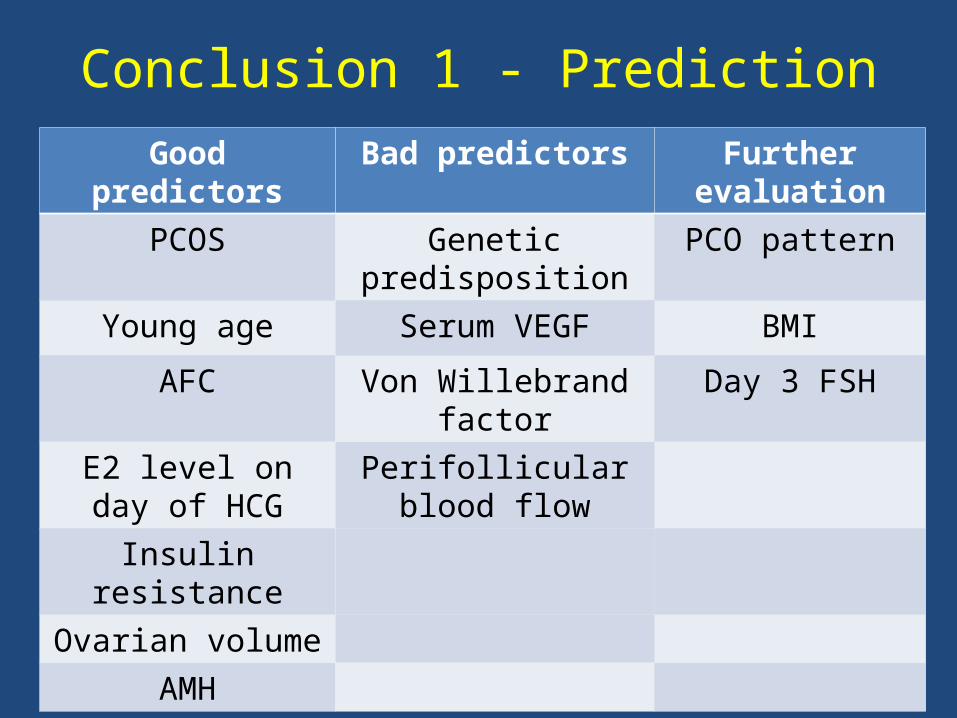
Conclusion 1 - PredictionGood
predictorsBad predictors Further
evaluation
PCOS Genetic predisposition
PCO pattern
Young age Serum VEGF BMI
AFC Von Willebrand factor
Day 3 FSH
E2 level on day of HCG
Perifollicular blood flow
Insulin resistance
Ovarian volume
AMH
Prevention of OHSS
1. Prediction of OHSS2. Primary prevention (before
starting HMG/FSH)3. Secondary prevention (after
starting HMG/FSH and before HCG administration)

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

Nugent et al, Cochrane Database: Issue 1, 2009
FSH versus HMG to prevent OHSS
Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

Chronic low-dose step-up protocol
Homburg et al, Fertil Steril 63: 729, 1995

Low dose step-up protocol (RCT)
Conventional Step-up P value
No. of cycles 48 49
Oestradiol on the day of HCG (pg/ml)
1258.6 ± 1003 533.5 ± 525
0.001
No. of pregnancies 7 (14.6%) 7 (14.3%) NS
No. of abortions 1 (14.3%) 1 (14.3%) NS
No. of multiple pregnancies
2 (28.6%) 1(14.3%) NS
No. of OHSS 13 (27.1%) 4 (8.3%) 0.05
Mild OHSS 5 (10.4%) 4 (8.3%) NS
Moderate OHSS 8 (16.7%) 0 (0%) 0.01
Sengoku et al, Hum Reprod 14: 349, 1999

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists
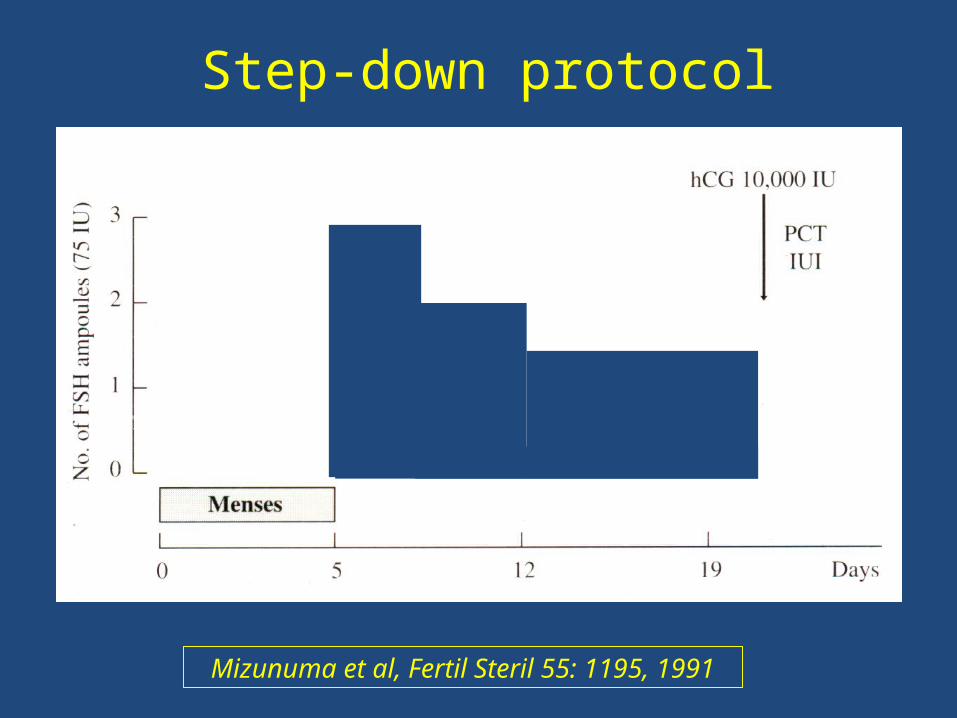
Step-down protocol
Mizunuma et al, Fertil Steril 55: 1195, 1991

Step-up, step-down and conventional protocols (RCT)
Protocol Conventional (n =
19)
Step down (n = 24)
Step up
(n = 25)
P value
Small follicles 7.6 ± 1.9 * 6.3 ± 1.0 3.1 ± 0.7 *
<0.05
Medium follicles
5.7 ± 1.2 * 5.0 ± 0.8 2.3 ± 0.6 *
<0.05
Large follicles 1.5 ± 0.3 1.2 ± 0.2 1.3 ± 0.3 NS
Andoh et al, Fertil Steril 70: 840, 1998

Santbrink and Fauser, J Clin Endocrinol Metab 82: 3597, 1997
Step-up versus step-down protocol (RCT)
Step-up (n=18) Step down (n=17)p

Step-up versus step-down protocol (RCT)
Low dose step-up
Step down P value
No. of patients 19 18
Duration of treatment
(days)
18 9 0.003
No. of ampoules 20 14 NS
Monofollicle growth
6 (39%) 17 (100 %) < 0.001
Ovulation rate 84 % 89 % NS
Ongoing pregnancies
2 5 NS
OHSS 0 0 NS
Santbrink and Fauser, J Clin Endocrinol Metab 82: 3597, 1997

Chronic low-dose step-up versus step-down protocol (RCT)
Low dose step-up
Step down P value
No. of patients 85 72
Duration of treatment
(days)
15.2 ± 7 9.7 ± 3.1 < 0.001
Total dose of rec-FSH (IU)
951 ± 586 967 ± 458 NS
Mono-follicular growth
68.2% 32% < 0.0001
Ovulation rate 70.3% 61.7% 0.02
Pregnancies/cycle
18.7% 15.8% NS
OHSS 2.25% 11% <0.001
Christian-Maitre et al, Hum Reprod 18:1626, 2003

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

Alternate day HMG to prevent OHSS
Nugent et al, Cochrane Database: Issue 1, 2009

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

Sequential FSH regimen to prevent OHSS (RCT)
Step-up protocol
step-down
protocol
Sequential protocol
P value
No. of cycles 75 75 75
No. of clinicalpregnancies (rate)
18 20 33 <0.05
Pregnancy rate 31.0 % 32.2 % 48.5 % NS
No. of multiplepregnancies (rate)
4 (22.2%) 5 (25.0%) 8 (24.0%) NS
NS
Rate of hyperstimulation
5.2 % 13 % * 5.9 % <0.05
Koundouros, Fertil Steril 90: 569, 2009

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

In-vitro maturation to prevent OHSS (CCT)IVM IVF OR (95% CI)
No. of cycles 107 107
Implantation rate (%) 9.5 17.1 0.51 (0.31, 0.84) *
Clinical pregnancy [n (%)]
23 (21.5) 36 (33.7) 0.54 (0.28, 1.04)
Live birth [n (%)] 17 (15.9) 28 (26.2) 0.53 (0.26, 1.10)
Multiple live births [n (% of total live births)]
7 (41.2) 10 (37.0) 1.26 (0.30, 5.11)
Moderate or severe OHSS
0 12 (11.2%)
0.036 (0.002-0.608) *
Child et al, Obstet Gynecol 100: 665, 2002

Primary prevention (before starting HMG/FSH)
• FSH or HMG• Low dose step-up protocol
• Step-down protocol• Alternate day HMG/FSH
• Sequential protocol• In-vitro maturation (IVM)
• GnRH antagonists

GnRHa v/s antagonists to prevent OHSS, 2009
Al-Inany et al, Cochrane Database: Issue 1, 2009

LBR in GnRH agonists v/s antagonists, 2009
Al-Inany et al, Cochrane Database: Issue 1, 2009

GnR a v/s antagonists to prevent OHSS, 2011
Al-Inany et al, Cochrane Database Syst Rev 11;(5):CD001750, 2011

LBR in GnRH agonists v/s antagonists, 2011
Al-Inany et al, Cochrane Database Syst Rev 11;(5):CD001750, 2011

Conclusion 2 – Primary prevention
The following approaches are associated with a lower incidence of OHSS:
• FSH compared to HMG (without GnRHa) (A)• Step-up compared to conventional protocol
(A)• GnRH antagonists compared to agonists (A)• IVM compared to IVF but with a lower LBR
(B)• Sequential compared to step down protocol
(A)

Conclusion 2 – Primary prevention
(cont…)The following approaches are equivocal in
the primary prevention of OHSS:• Alternate days compared to conventional
protocol (A) • Sequential compared to step-up protocol
(A)
The following approaches need further evaluation:
• Step-up compared to step down protocol

Prevention of OHSS
1. Prediction of OHSS2. Primary prevention (before
starting HMG/FSH)3. Secondary prevention (after
starting HMG/FSH and before HCG administration)

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Cancellation of the cycle - attitude of 141 physicians
High risk patient
Moderate risk
patient
Low risk patient
P value
Proceed with IVF 8 % 22 % 38 % <0.001
Cancel cycle 14 % 14 % 7 % NS
Take some preventive measures
78 % 64 % 55 % <0.01
Delvigne and Rozenberg, Hum Reprod 16: 2491, 2001

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Coasting to prevent OHSS - Guidelines
1. Start at • Serum E2 >4,500 pg/mL
• E2 production >150 pg/follicle 16–18 mm • >15 mature follicles
2. Measure E2 on a daily basis3. Give hCG when E2 level falls to <3,500
pg/mL 4. Abandon if
• E2 level rises to >6,500 pg/mL• >30 mature follicles
• Coasting takes >4 daysGarcia-Velasco et al, Fertil Steril 85:
547, 2006

Incidence of OHSSOR = 0.53 (95% CI = 0.23 to 1.23)
Live birth rateOR = 0.48 (95% CI = 0.14 to 1.62)
Clinical pregnancy rate
OR = 0.69 (95% CI = 0.44 to 1.08)
Oocytes retrieved OR = -3.92 (95% CI -4.47 to -3.37) *
Coasting to prevent OHSS (Cochrane)
D’Angelo et al, Cochrane Database Syst Rev 15;(6):CD002811, 2011

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Diminish HCG dose (OS)
• 21 infertile patients at risk of OHSS • Low dose of HCG (i.e. 2500 IU)• No moderate or severe OHSS• 13 women (61.9%) conceived
• Three twin pregnancies
Nargund et al. RBMOnline 14: 682, 2007

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Incidence of OHSS after GnRH agonists to trigger ovulation (MA)
Reference
No patients
with agonist trigger
No of patients with hCG trigger
Patients with OHSS post
agonist
Patients with OHSS
post hCG (%)
P value
Babayof et al, 2006
(RCT)15 13 0/15 4/13 (31%) <0.05
Engmann et al, 2008
(RCT)33 32 0/33
10/32 (31%)
<0.001
Acevedo et al, 2006
(RCT)30 30 0/30 5/30 (17%) <0.05
TOTAL 78 75 0/7819/75 (25%)
<0.001
Kol and Solt, JARG 25: 63, 2008

GnRH agonists to trigger ovulation
Griesinger et al, Human Reprod Update 12: 159, 2006

GnRH agonists to trigger ovulation
Youssef et al, Cochrane Database Syst Rev 10;(11):CD008046, 2010
OHSS incidence per randomised woman OR =
0.10 (95% CI = 0.01 to 0.82) *
GnRH agonist versus HCG (LBR)
OR = 0.44 (95% CI = 0.29 to 0.68) *
GnRH agonist versus HCG (OPR) OR = 0.45 (95% CI = 0.31 to 0.65) *

GnRH agonists to trigger ovulation with modified luteal support (OS)
No OHSS after GnRHa triggering 5% risk
difference (with 95% CI: -0.07 to 0.02)
Delivery rate after modified luteal support 6% risk difference (95% CI: -0.14 to 0.2)
Delivery rate after conventional luteal support 18% risk difference (95% CI: -0.36 to 0.01)
Humaidan, Hum Reprod Update 17(4):510-24, 2011

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Costello et al. Hum Reprod 21:1387, 2006
Metformin versus placebo or no treatment in IVF for to prevent OHSS in PCOS
patients
OR = 0.21; 95% CI = 0.11–0.41, P < 0.00001

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Albumin for the prevention of OHSS
Aboulghar et al, Cochrane Database: Issue 1, 2009

Hydroxyethyl starch (HES) to prevent OHSS (CCT)
HES Control group P value
No. of patients 100 82
No. of pregnancies
28 24 NS
Moderate OHSS 10 32 <0.00001
Severe OHSS 2 7 NS
Graf et al, Hum Reprod 12: 2599, 1997

HES versus albumin to prevent OHSS (RCT)
HES (n = 85)
Albumin (n =82)
Control group (n =
83)
P value
Moderate OHSS
5 (5.9 %) 4 (4.9 %) 12 (14.5 %) <0.05
Severe OHSS
0 0 4 (4.8 %) <0.05
Overall cases of
OHSS
5 (5.9 %) 4 (4.89 %) 16 (19.2 %) <0.01
Gokmen et al, Eur J Obstet Gyn Reprod Biol 96: 187, 2001

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Effect of cabergoline on rats with OHSS
A = Vascular permeabilityB = Serum prolactinC = Plasma progesteroneGomez et al, Endocrinol 147:
5400, 2006
Cabergoline inactivates the VEGF receptor 2 (VEGFR-2)
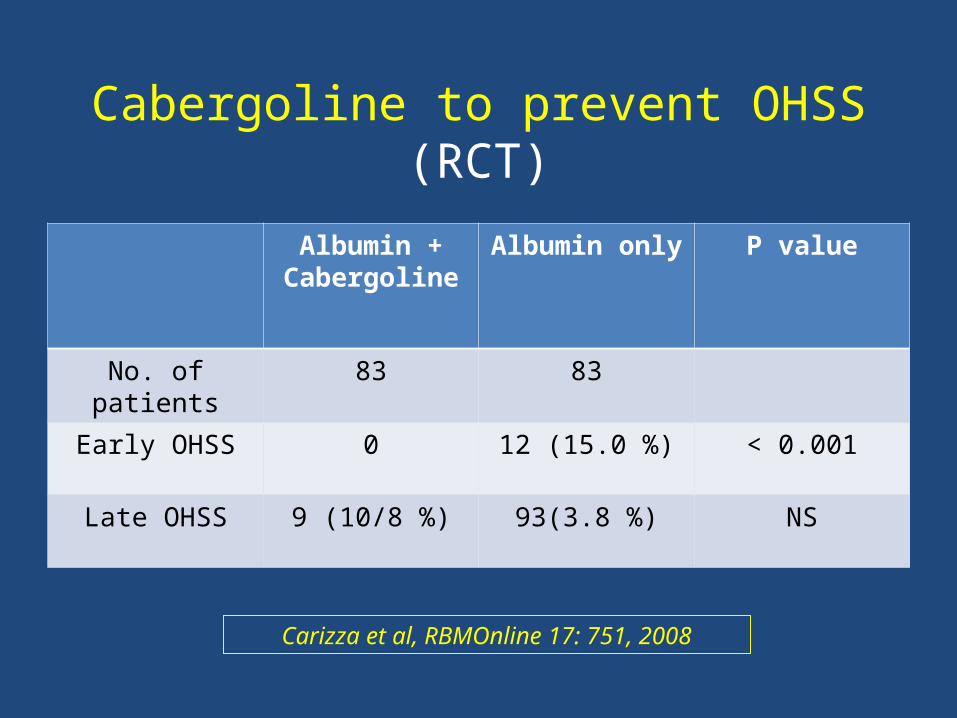
Cabergoline to prevent OHSS (RCT)
Albumin + Cabergoline
Albumin only
P value
No. of patients 83 83
Early OHSS 0 12 (15.0 %) < 0.001
Late OHSS 9 (10/8 %) 93(3.8 %) NS
Carizza et al, RBMOnline 17: 751, 2008

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

I.V. Calcium to prevent OHSS (CCT)
I.V. Calcium Control group
P value
No. of patients 84 371
OHSS 3 (3.6%) 60 (16.2%) <0.01
Pregnancies (CPR)
34 (40.5%) 107 (28.8%) <0.05
Deliveries (LBR) 32 (38.1%) 92 (24.8%) <0.02
Gurgan et al, Fertil Steril 96: 53-7, 2011

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Embryo freezing to prevent OHSS
D’Angelo and Amso, Cochrane Database: Issue 2, 2002

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

GnRH agonists + embryo freezing to prevent OHSS (OS)
% (n) 95% CI
Biochemical PR/patient 5.3 % (1/19) 0.9 % – 24.6 %
Ongoing PR/patient 36.8 % (7/19) 19.1 % – 59.0 %
Ongoing PR/first ET 31.6 % (6/19) 15.4 % – 54.0 %
Cumulative ongoing PR/ET
29.2 % (7/24) 14.9 % – 49.2 %
OHSS 0 % (0/24)
Griesinger et al, Human Reprod 22: 1348, 2007

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Unilateral follicle aspiration before HCG (RCT)
Unilateral follicle
aspiration (n = 16)
Controls (n = 15)
P value
Oestradiol (pmol/l)
15 982 ± 827 16 243 ± 593 NS
Mild OHSS 1 3 NS
Moderate OHSS 1 1 NS
Severe OHSS 2 1 NS
Clinical pregnancy rate
6/16 (37.5%) 7/15 (46.6%) NS
Egbase et al, Hum Reprod 12: 2603, 1997

Late prevention (after starting HMG/FSH and before HCG)
• Cancellation of the cycle• Coasting
• Diminish HCG dose• GnRHa to trigger ovulation
• Metformin• Albumin
• Cabergoline• I.V. Calcium
• Cryopreservation of embryos• GnRH agonists + embryo freezing• Unilateral follicle aspiration before
HCG• Laparoscopic ovarian electro-
cautery

Laparoscopic ovarian electro-cautery (RCT)Conventional
IVF(n = 25)
LOE + IVF(n = 25)
P value
Cancellations due to OHSS risk
5 0 0.025 *
Moderate OHSS 4 1 0.174
Mean number of oocytes 7.37 10.28
Mean embryos transferred 2.5 2.6
Pregnancy rate/cycle 8/25 (32.0 %) 9/25 (36.0 %)
0.765
Rimington et al, Hum Reprod 12: 1443, 1997
Conclusion 3 – Secondary prevention
The following approaches prevent OHSS:• Triggering ovulation with GnRH agonists (A)
• Metformin administration (A)• Intravenous albumin (A)• Hydroxyethyl starch (A)
• Cabergoline for early OHSS (A)• Laparoscopic ovarian electrocautery (A)
The following approaches do not prevent OHSS
• Coasting (A)• Cabergoline for late OHSS (A)

Conclusion 3 – Secondary prevention (cont…)
The following approaches are equivocal in preventing OHSS:
• Coasting versus unilateral oocyte aspiration (A)
• GnRH antagonists versus coasting (A)
The following approaches await further evaluation:
• Cancellation of the cycle•Diminishing the dose of HCG
• Embryo freezing• Triggering with GnRHa + embryo freezing

Prediction and prevention of OHSS -
an evidence-based approachHassan N. Sallam,
MD, FRCOG, PhD (London)Professor in Obstetrics and Gynaecology
The University of Alexandria, andClinical and Scientific Director,
Alexandria Fertility Center, Alexandria, Egypt
3rd Congress of Society of Reproductive Medicine, 5 – 9 October
2011, Antalya / Turkey

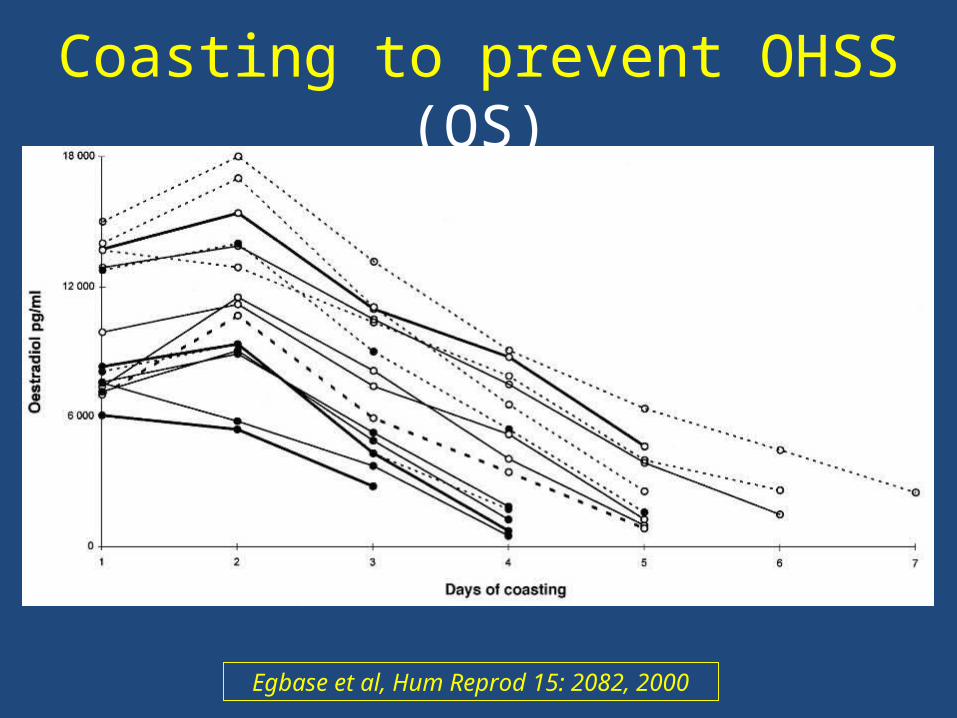
Coasting to prevent OHSS (OS)
Egbase et al, Hum Reprod 15: 2082, 2000

Coasting to prevent OHSS (OS)
Characteristic Outcome
No. of patients 15
Mean age (years ) ± SD 33.5 ± 2.8
Body mass index ± SD 34.8 ± 5.2
No. of ampoules ± SD 50.2 ± 16.5
Moderate OHSS (%) 3 (20 %)
Severe OHSS 3 (20 %)
Clinical pregnancy rate 5/15 (33.3 %)
Egbase et al, Hum Reprod 15: 2082, 2000

Coasting versus early unilateral follicular aspiration to prevent
OHSS
D’Angelo and Amso, Cochrane Database Issue 1, 2009

GnRH antagonists versus coasting to prevent OHSS (RCT)
Coasting(n = 96)
GnRH antagonist
(n = 94)
P value
No. of high quality embryos (SD)
2.21 ± 1.1 2.87 ± 1.2 <0.0001
Mean number of oocytes (SD)
14.06 ± 5.20 16.5 ± 7.60 <0.02
Clinical pregnancy rate
47.9 % 55.3 % NS
Severe OHSS None None NS
Aboulghar et al, RBMOnline 15: 271, 2007

Conclusion 1 - Prediction
Good predictors Bad predictors
PCOS BMI
Young age Genetic predisposition
PCO pattern Serum VEGF
AFC Von Willebrand factor
E2 level on day of HCG Perifollicular blood flow
Insulin resistance
Large ovarian volume
AMH