predicting maximal grip strength using hand circumference.pdf
7
Original article Predicting maximal grip strength using hand circumference Ke Li a, b , David J. Hewson a , Jacques Duchêne a , Jean-Yves Hogrel c, * a Institut Charles Delaunay, FRE CNRS 2848, Université de Technologie de Troyes, Troyes, France b School of Control Science and Engineering, Shandong University, 73 Jingshi Ave, 250062 Jinan, China c Institut de Myologie, Université Paris 6 UMR S974, Inserm U974, CNRS UMR 7215, GH Pitié-Salpêtrière, Paris, France article info Article history: Received 16 October 2009 Received in revised form 23 June 2010 Accepted 28 June 2010 Keywords: Maximal grip strength Predictive model Outcome assessment Impairment abstract The objective of this study was to analyze the correlations between anthropometric data and maximal grip strength (MGS) in order to establish a simple model to predict “normal” MGS. Randomized bilateral measurement of MGS was performed on a homogeneous population of 100 subjects. MGS was measured according to a standardized protocol with three dynamometers (Jamar, Myogrip and Martin Vigorimeter) for both dominant and non-dominant sides. Several anthropometric data were also measured: height; weight; hand, wrist and forearm circumference; hand and palm length. Among these data, hand circumference had the strongest correlation with MGS for all three dynamometers and for both hands (0.789 and 0.782 for Jamar; 0.829 and 0.824 for Myogrip; 0.663 and 0.730 for Vigorimeter). In addition, the only anthropometric variable systematically selected by a stepwise multiple linear regression analysis was also hand circumference. Based on this parameter alone, a predictive regression model presented good results (r 2 ¼ 0.624 for Jamar; r 2 ¼ 0.683 for Myogrip and r 2 ¼ 0.473 for Vigorimeter; all adjusted r 2 ). Moreover a single equation was predictive of MGS for both men and women and for both non-dominant and dominant hands. “Normal” MGS can be predicted using hand circumference alone. Ó 2010 Elsevier Ltd. All rights reserved. 1. Introduction There are a number of situations in which maximal hand-grip strength references are needed. Individual functional evaluation and follow-up can be considered, for example, within the frame of maturity or aging, injury and rehabilitation, disease and therapy, or medicolegal issues. Maximal grip strength (MGS) has also been shown to be a good indicator of overall upper-limb strength (Bohannon, 1998, 2004) or even of the whole neuromuscular system function (Avlund et al., 1994; Chan et al., 2008). Hand-grip strength is also known to be associated with ability to perform daily living activities (Nybo et al., 2001). MGS is thus implicitly linked to functional autonomy, hence quality of life. This relationship had already been attested in aging people (Sayer et al., 2006) and patients (Ansari et al., 2007). Frederiksen et al. (2002) concluded that “grip strength is a suitable phenotype for identifying genetic variants of importance to mid- and late-life physical functioning”. Most of the prediction regression models for MGS use gender, age, weight and/or height either in children, in adults or in aging people (Balogun et al., 1991; Crosby et al., 1994; Rauch et al., 2002; Niempoog et al., 2007; Gunther et al., 2008). Measurements of the forearm and hand have already been described as better predictors of MGS than height and weight (Rice et al., 1998; Nicolay and Walker, 2005). Kallman et al. previously claimed that forearm circumference provides the most practical index of MGS (Kallman et al., 1990). However, Anakwe et al. recently found that forearm circumference was predictive of MGS for men but not for women (Anakwe et al., 2007). This could be explained by difference in forearm composition, implying that a gender effect could be eliminated as a factor in predicting MGS by using fat-free cross- sectional area (CSA) (Bishop et al., 1987). Indeed, fat-free CSA was found to be highly correlated with MGS (r 2 ¼ 0.788) whatever the gender (Aghazadeh et al., 1993). Thus, many parameters have been used to establish predictive models for MGS and to provide clinicians with a means of computing the deficit in strength or the residual strength of patients or elderly people. This is of particular importance for impairment quantification during aging, pathology, injury, reha- bilitation or therapy. However many anthropological variables are difficult to assess such as fat-free mass (FFM), muscle CSA or even skin-fold measurements. Furthermore, the predictive models previously used tend to be either too general, mainly based on gender and age only, or too complicated, requiring many variables to be measured and calculated. The objective of the present study was to explore if a simple and practical predictive model of MGS * Corresponding author. Institut de Myologie, GH Pitié-Salpêtrière, 75651 Paris Cedex 13, France. Tel.: þ33 1 42 16 58 80; fax: þ33 142 16 58 81. E-mail address: [email protected] (J.-Y. Hogrel). Contents lists available at ScienceDirect Manual Therapy journal homepage: www.elsevier.com/math 1356-689X/$ e see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.math.2010.06.010 Manual Therapy 15 (2010) 579e585
-
Upload
graciela-rodriguez -
Category
Documents
-
view
76 -
download
1
Transcript of predicting maximal grip strength using hand circumference.pdf

lable at ScienceDirect
Manual Therapy 15 (2010) 579e585
Contents lists avai
Manual Therapy
journal homepage: www.elsevier .com/math
Original article
Predicting maximal grip strength using hand circumference
Ke Li a,b, David J. Hewson a, Jacques Duchêne a, Jean-Yves Hogrel c,*
a Institut Charles Delaunay, FRE CNRS 2848, Université de Technologie de Troyes, Troyes, Franceb School of Control Science and Engineering, Shandong University, 73 Jingshi Ave, 250062 Jinan, Chinac Institut de Myologie, Université Paris 6 UMR S974, Inserm U974, CNRS UMR 7215, GH Pitié-Salpêtrière, Paris, France
a r t i c l e i n f o
Article history:Received 16 October 2009Received in revised form23 June 2010Accepted 28 June 2010
Keywords:Maximal grip strengthPredictive modelOutcome assessmentImpairment
* Corresponding author. Institut de Myologie, GHCedex 13, France. Tel.: þ33 1 42 16 58 80; fax: þ33 1
E-mail address: [email protected] (J.
1356-689X/$ e see front matter � 2010 Elsevier Ltd.doi:10.1016/j.math.2010.06.010
a b s t r a c t
The objective of this study was to analyze the correlations between anthropometric data and maximalgrip strength (MGS) in order to establish a simple model to predict “normal” MGS. Randomized bilateralmeasurement of MGS was performed on a homogeneous population of 100 subjects. MGS was measuredaccording to a standardized protocol with three dynamometers (Jamar, Myogrip and Martin Vigorimeter)for both dominant and non-dominant sides. Several anthropometric data were also measured: height;weight; hand, wrist and forearm circumference; hand and palm length. Among these data, handcircumference had the strongest correlation with MGS for all three dynamometers and for both hands(0.789 and 0.782 for Jamar; 0.829 and 0.824 for Myogrip; 0.663 and 0.730 for Vigorimeter). In addition,the only anthropometric variable systematically selected by a stepwise multiple linear regressionanalysis was also hand circumference. Based on this parameter alone, a predictive regression modelpresented good results (r2¼ 0.624 for Jamar; r2¼ 0.683 for Myogrip and r2¼ 0.473 for Vigorimeter; alladjusted r2). Moreover a single equation was predictive of MGS for both men and women and for bothnon-dominant and dominant hands. “Normal” MGS can be predicted using hand circumference alone.
� 2010 Elsevier Ltd. All rights reserved.
1. Introduction
There are a number of situations in which maximal hand-gripstrength references are needed. Individual functional evaluationand follow-up can be considered, for example, within the frame ofmaturity or aging, injury and rehabilitation, disease and therapy, ormedicolegal issues. Maximal grip strength (MGS) has also beenshown to be a good indicator of overall upper-limb strength(Bohannon, 1998, 2004) or even of the whole neuromuscularsystem function (Avlund et al., 1994; Chan et al., 2008). Hand-gripstrength is also known to be associatedwith ability to perform dailyliving activities (Nybo et al., 2001). MGS is thus implicitly linked tofunctional autonomy, hence quality of life. This relationship hadalready been attested in aging people (Sayer et al., 2006) andpatients (Ansari et al., 2007). Frederiksen et al. (2002) concludedthat “grip strength is a suitable phenotype for identifying geneticvariants of importance to mid- and late-life physical functioning”.Most of the prediction regression models for MGS use gender, age,weight and/or height either in children, in adults or in aging people(Balogun et al., 1991; Crosby et al., 1994; Rauch et al., 2002;
Pitié-Salpêtrière, 75651 Paris42 16 58 81.-Y. Hogrel).
All rights reserved.
Niempoog et al., 2007; Gunther et al., 2008). Measurements ofthe forearm and hand have already been described as betterpredictors of MGS than height and weight (Rice et al., 1998; Nicolayand Walker, 2005). Kallman et al. previously claimed that forearmcircumference provides the most practical index of MGS (Kallmanet al., 1990). However, Anakwe et al. recently found that forearmcircumference was predictive of MGS for men but not for women(Anakwe et al., 2007). This could be explained by difference inforearm composition, implying that a gender effect could beeliminated as a factor in predicting MGS by using fat-free cross-sectional area (CSA) (Bishop et al., 1987). Indeed, fat-free CSA wasfound to be highly correlated with MGS (r2¼ 0.788) whatever thegender (Aghazadeh et al., 1993).
Thus, many parameters have been used to establish predictivemodels for MGS and to provide clinicians with a means ofcomputing the deficit in strength or the residual strength ofpatients or elderly people. This is of particular importance forimpairment quantification during aging, pathology, injury, reha-bilitation or therapy. However many anthropological variables aredifficult to assess such as fat-free mass (FFM), muscle CSA or evenskin-fold measurements. Furthermore, the predictive modelspreviously used tend to be either too general, mainly based ongender and age only, or too complicated, requiring many variablesto be measured and calculated. The objective of the present studywas to explore if a simple and practical predictive model of MGS

K. Li et al. / Manual Therapy 15 (2010) 579e585580
could be obtained using a limited number of simple variables withan acceptable reliability. This was performed by using three types ofdynamometers to ensure that the measurement device did notinfluence the model. Moreover a homogeneous population ofyoung healthy subjects was selected to ensure that age was nota factor in the model developed.
2. Methods
2.1. Subject selection
One hundred undergraduate students participated in this study,which was conducted as part of practical work aiming to assess therelationship between some anthropometric data and musclestrength. Prior to any evaluation, each subject was given a detaileddescription of the objectives and requirements of the experiment.The protocol was approved by the university studies committee(CEVU), as part of the course structure. The idea was to geta homogeneous population of healthy subjects in order to obtain an“optimal” MGS that could be considered as independent of age(maturation and aging). People with any prior hand, wrist orforearm injury were not considered for the analyses in order toavoid any bias caused by a possible impairment of grip function.Accordingly, six subjects were not considered for subsequent dataanalysis. Of the remaining 94 subjects, none of them participated insporting and fitness activities more than four times a week. Inaddition, no subjects could be considered to be severely over- orunder-weighted according to their body mass index (BMI).
In order to assess the power of MGS prediction models, 29 addi-tional healthy subjects were selected from a database of MGS usingthe same eligibility criteria and measured according to the sameoperating procedures, by another evaluator in another center. Thisstudywasapprovedby the local ethical committee (CPP Ile-de-FranceVI, Pitié-Salpêtrière).
2.2. Data collection
Subjects completed a questionnaire that provided informationincluding gender, date of birth, and height. Weight was assessed bya conventional scale (0.1 kg precision). Anthropometric data weremeasured by the experimenter using a standard 1000-mmmeasurement tape. The circumference of the forearm was definedas the perimeter of the largest part of forearm, located over the bulkof the brachioradialis muscle, at about the proximal quarter of thewhole forearm length depending on the subject morphology. Thecircumference of the wrist was measured at the joint of the radiusand the ulna which corresponds to the perimeter of the thinnestpart of the forearm. The circumference of the hand was measuredas the perimeter of the middle part of hand, located over the two
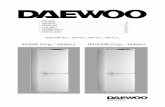
Fig. 1. Materials and standardized positions. A. Picture of the three dynamometers used inthe evaluation. C. Position of the evaluator.
major transverse palmar creases (“heart line” and “head line”).Palm length was defined as the distance from the midline of thedistal wrist crease to the crease of the base of the middle finger.Hand length was defined as the distance from the midline of thedistal wrist crease to the tip of the middle finger. All anthropo-metric data were measured to the nearest millimeter with theforearm and hand relaxed in a supinated position, while the elbowwas supported on a table. A preliminary study has shown that theoperating procedures for measuring these anthropometric vari-ables were highly reliable (unpublished data).
The dominant hand side was defined as the hand that thesubject used to write with.
2.3. Test procedure
Three dynamometers were used to assess MGS: the Jamar(Sammons & Preston, Bolingbrook, IL, USA), the Martin Vigorimeter(MartinMedizintechnik, Tuttlingen, Germany) and the Myogrip(ASICA, Saint-Malo, France) (Fig. 1.A). The Jamar is an isometrichydraulic dynamometer with an adjustable 5-position handle. Itmeasures forces in kilograms (kg) from 6 to 90 kg with a resolutionof 1 kg. The Jamar is considered as the reference tool by theAmerican Society of Hand Therapists. The Martin Vigorimeter isa pseudo-dynamic dynamometer that measures the pressure whensubjects press a rubber bulb connected by a tube to a manometer.Three sizes of bulbs are available. The Vigorimeter measures pres-sures in kiloPascal (kPa) and has been shown to be highly correlatedto grip strength (Desrosiers et al., 1995). The Myogrip dynamom-eter is an isometric electronic device specifically developed formeasuring grip strength in weak patients, but which can also beused in healthy subjects. The Myogrip can directly display thestrength of the subjects or be connected to a computer either byradio-frequency, RS232 or BNC connections. Handle size is adjust-able in a continuous way. It measures forces in decaNewtons (daN)from 0 to 89 daN with a resolution of 0.01 daN.
The measurement sessions took place in a quiet laboratory ata controlled temperature of 22 �C. Tests using the Jamar wereperformed with the handle in the second position, while the largebulb of the Vigorimeter was used. All tests with the Myogrip useda handle position of 1.5, which corresponds to the second positionof the Jamar. No subjects reported any problems with the handlesize chosen. Test mode by RS232 connection was used for allrecordings from the Myogrip. Both Jamar and Myogrip were cali-brated before the recording periods. During the evaluation,subjects were seated on a chair, with their feet flat on the floor,their shoulders adducted, and their testing arm close to their body,with their elbow extended to 180� along the vertical axis and theirwrists in slight extension (Li et al., 2009). The distal part of theforearm was maintained by the evaluator in order to avoid any
the study. 1. Jamar; 2. MyoGrip; 3. Martin Vigorimeter. B. Position of the subject during

K. Li et al. / Manual Therapy 15 (2010) 579e585 581
compensatory movements (Fig. 1.C). Subjects were continuouslygiven standardized verbal encouragements before and during alltrials in order to motivate them to exert their MGS.
Each subject was tested for both right and left hands, and for allthree dynamometers. The order in which each device and the twosides were tested was randomized in order to prevent for anywarm-up or fatigue effects. MGS for each dynamometer wasmeasured twice for each hand, alternating between hands, with15 s between trials (Li et al., 2009). Maximal grip contractions wereperformed until the values measured from two trials were within10% (Nevill and Holder, 2000). The MGS was taken as the largestforce from these two values. Subjects changed dynamometers aftercompleting all measurements for both left and right hands.Subjects were given a 2-min rest between dynamometers.
2.4. Data analysis
All statistical analyses were performed using the StatisticalPackage for Social Sciences (V16, SPSS Inc., Chicago, IL, USA). Datawere assessed for normality using the KolmogoroveSmirnov test.An independent-samples t-test was used to compare grip strengthbetween genders. Paired-samples t-tests were used to analyze theinfluence of hand dominance. Pearson’s correlation analysis wasused to compare the influence of anthropometric data and dyna-mometers on MGS. A stepwise multiple linear regression analysiswith an entry probability of 0.05 and a removal probability of 0.10was applied to determine the importance of anthropometric dataand to establish a predictive regression-based model. Pearson’scorrelation analysis and PeP plot were used for residue analysisfor the initial population as well as for the additional population.Intraclass correlation coefficients (ICC(2,1)) were computed for theadditional population in order to assess the agreement betweenthe values calculated by the prediction models and the truemeasurements. All coefficients of determination are adjusted r2.All statistical test results were considered as statistically signifi-cant for p values less than 0.05. The correlations were character-ized according to Hopkins’ scale whereby correlations can beconsidered to be moderate from 0.3 to 0.5, large from 0.5 to 0.7,very large from 0.7 to 0.9 and nearly perfect from 0.9 to 1(Hopkins, 2000).
Table 1Characteristics and anthropometric data of the subjects.
Men (n¼ 67)
Mean (SD)
Age (y) 20.5 (0.9)Height (cm) 178.6 (5.7)Weight (kg) 71.1 (8.7)BMI (kg/m2) 22.3 (2.2)
Forearm circumference (mm)* D 270.9 (16.6)ND 264.5 (15.7)
Wrist circumference (mm) D 168.0 (8.8)ND 167.6 (8.8)
Hand circumference (mm)* D 215.6 (11.0)ND 208.4 (10.6)
Palm length (mm) D 111.9 (5.9)ND 111.8 (5.4)
Hand length (mm) D 194.3 (9.8)ND 195.4 (9.1)
DominanceRight handed 61 (91.0%)Left handed 6 (9.0%)
D: dominant side; ND: non-dominant side.*Significantly different between sides (p< 0.0001).
3. Results
A final number of 94 subjects was retained for analysis, withcharacteristics of these subjects given in Table 1. Pearson’s corre-lation coefficients between grip strength and anthropometric dataare provided in Table 2. The largest correlations were observed forhand, forearm, and wrist circumference, then for hand and palmlength, followed by weight and height.
Men were significantly stronger than women by similar ratiosfor the three dynamometers (Jamar: 1.50; Myogrip: 1.55; Vig-orimeter: 1.50). The dominant side was significantly stronger thanthe non-dominant side by similar ratios for the three dynamome-ters (Jamar: 1.09� 0.11; Myogrip: 1.08� 0.11; Vigorimeter:1.06� 0.13). In addition, hand and forearm circumferences weresignificantly larger at the dominant side compared with the non-dominant side (ratio for the forearm: 1.025� 0.025; ratio for thehand: 1.035� 0.027). There was a trend toward a larger wristcircumference (p¼ 0.0981) and a smaller hand length (p¼ 0.0796)at the dominant side compared with the non-dominant side. Thecorrelation matrix for the anthropometric data is given in Table 3. Itshould be noted that the correlation between BMI and forearmcircumference is very large, whereas the correlation between BMIand hand circumference is only moderate (Hopkins, 2000).
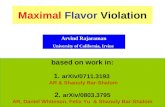
Stepwise multiple linear regression analysis was used toestablish predictive models for MGS for each dynamometer.Table 4 provides the successive parameters entering the regres-sion model in the order defined by the stepwise method. For thethree dynamometers, on the dominant or non-dominant sidestaken separately or together, the only anthropometric parametersystematically included in the regression model was handcircumference. Thus three regression functions were establishedbased on hand circumference only, one for each device (Table 5).A single equation was used for both hands and both genders afterverifying that the 95% confidence intervals of the parameters ofthe models computed separately for each gender and side over-lapped. Adjusted r2 demonstrates that these regression functionshave a good capacity to predict MGS when considering handcircumference alone (Fig. 1). The coefficients of determination(r2) of these correlations were 0.626, 0.685 and 0.481 for Jamar,Myogrip and Vigorimeter, respectively (all p< 0.001).
Women (n¼ 27)
Range Mean (SD) Range
19e24 20.2 (1.1) 19e24169e192 166.7 (5.4) 152e17657e92 57.3 (8.1) 43e81
17.0e26.6 20.6 (2.3) 17.0e26.2
224e302 238.7 (18.1) 200e282234e302 232.3 (17.1) 199e276
147e186 154.2 (9.8) 133e174147e187 153.0 (8.3) 133e170
191e249 190.2 (11.0) 168e213185e237 183.8 (9.5) 163e206
96e122 103.2 (6.9) 89e11697e123 103.4 (7.0) 86e114
171e215 179.7 (10.8) 154e201174e215 179.7 (9.9) 154e194
25 (92.6%)2 (7.4%)

Table 2Pearson correlation coefficients between anthropometric data and grip-strengthscores obtained for the three dynamometers.
Jamar Myogrip Vigorimeter
Handcircumference
D 0.789 0.829 0.663ND 0.782 0.824 0.730
Forearmcircumference
D 0.739 0.764 0.614ND 0.803 0.805 0.729
Wristcircumference
D 0.702 0.730 0.604ND 0.711 0.764 0.652
Hand length D 0.657 0.718 0.617ND 0.630 0.737 0.630
Palm length D 0.600 0.664 0.542ND 0.592 0.678 0.581
Weight D 0.671 0.703 0.525ND 0.667 0.730 0.582
Height D 0.642 0.693 0.559ND 0.611 0.684 0.591
Age D 0.156(p¼ 0.133)
0.152(p¼ 0.145)
0.170(p¼ 0.101)
ND 0.250(p¼ 0.015)
0.138(p¼ 0.186)
0.253(p¼ 0.014)
D: dominant side; ND: non-dominant side.All p< 0.001 except when mentioned.
Table 3Correlation matrix between the anthropometric variables. All correlations aresignificant at p< 0.0001. BMI: Body Mass Index; C: circumference; L: length.
Height Weight BMI Forearm C Wrist C Hand C Palm L Hand L
Height 1.000Weight 0.766 1.000BMI 0.327 0.855 1.000Forearm C 0.641 0.853 0.747 1.000Wrist C 0.637 0.801 0.668 0.884 1.000Hand C 0.690 0.710 0.497 0.849 0.803 1.000Palm L 0.741 0.615 0.321 0.566 0.553 0.618 1.000Hand L 0.772 0.676 0.386 0.621 0.628 0.697 0.935 1.000
K. Li et al. / Manual Therapy 15 (2010) 579e585582
In order to verify these models and to illustrate their ability topredict MGS, 29 additional subjects were tested. Their character-istics are given in Table 6. Fig. 2 shows the results obtained for theMyogrip. Correlation analysis showed that the predicted andobserved values were significantly correlated (r2¼ 0.635;p< 0.0001). The ICC(2,1) between predicted and measured valueswas 0.795. The residuals were normally distributed (Fig. 3).
4. Discussion
The main result of this study shows that MGS can be suitablypredicted using hand circumference alone, indicating that thismeasurement is a relevant body-size dimension associated to gripstrength. Moreover a single equation can be used for both gendersand both hands provided that men have larger hands than womenand the dominant hand is significantly larger than the non-domi-nant hand. The coefficients of determination can be interpreted aslarge for the Martin Vigorimeter and very large for both the Jamarand the Myogrip dynamometers (Hopkins, 2000). Thus, handcircumference is a convenient and practical variable for routinelypredicting MGS since its measurement is easy to perform.
The model developed in the current study was constructedusing a homogeneous young adult population. Such a choice of
Table 4Variables selected for the stepwise multiple linear regression model and corresponding
Jamar Myogrip
Non-dominant Forearm circumference r2¼ 0.641 Hand circumHand circumference r2¼ 0.673 Forearm cir
Hand length
Dominant Hand circumference r2¼ 0.618 Hand circumPalm length r2¼ 0.639 Palm lengthForearm circumference r2¼ 0.651 Gender
Total Hand circumference r2¼ 0.624 Hand circumForearm circumference r2¼ 0.661 Palm lengthGender r2¼ 0.673 Forearm cirPalm length r2¼ 0.679 Gender
All p< 0.0001.
population was performed specifically to ensure that the subjectshad not begun the aging process. The resulting model was thusindependent of age. In addition, a single model can be used for bothgenders and hand sides. The use of a singlemodel was confirmed bycomparing separate models for hand dominance and gender. Theresulting single model will enable simple calculations of expectedgrip strength to be performed. It is clear that additional investiga-tions are needed using both young and elderly populations toconfirm this finding.
Normative data for MGS have been produced for several pop-ulations (Hager-Ross and Rosblad, 2002; Rauch et al., 2002;Kunelius et al., 2007; Gunther et al., 2008; Mitsionis et al., 2009).These normative data depict what is supposed to be a “normal” gripperformance mainly with respect to gender and age. Hence theycan be used to describe the possible loss of functional status duringaging (Robertson et al., 1996) or disease (Chin et al., 1999; Visseret al., 2003) in terms of deficit or residual strength. “Normal” gripstrength may be also defined as the maximal MGS observed in thelife of a “standard” individual, i.e. without any effect of age(maturation and aging), illness, injury, training or obesity.
Age and gender are mainly considered as two main factorsinfluencing MGS. For both genders, MGS presents a curvilinearrelationship to age (Hinson and Gench, 1989), which results ina peak of MGS in the third decade and a decline at an acceleratingrate after age 40 (Kallman et al., 1990; Sinaki et al., 2001; Mitsioniset al., 2009). However, a large study conducted by Hanten et al.concluded that age correlated weakly to grip strength, with theexception of people between 50 and 64 years (Hanten et al., 1999).A poor correlation between age and MGS was also found byMacDermid et al. (2002). Regardless of age, men have significantlyhigher values than women (Hanten et al., 1999). However, whenrelated to muscle CSA or one of its surrogates (forearm circumfer-ence for instance), strength differences between men and womenbecome considerably reduced (Hanten et al., 1999) or even absent(Bishop et al., 1987; Sartorio et al., 2002).
adjusted coefficient of determination.
Vigorimeter
ference r2¼ 0.675 Hand circumference r2¼ 0.527cumference r2¼ 0.712 Forearm circumference r2¼ 0.565
r2¼ 0.744
ference r2¼ 0.683 Hand circumference r2¼ 0.433r2¼ 0.723 Hand length r2¼ 0.473r2¼ 0.738
ference r2¼ 0.683 Hand circumference r2¼ 0.478r2¼ 0.720 Hand length r2¼ 0.511
cumference r2¼ 0.739 Forearm circumference r2¼ 0.530r2¼ 0.750 Weight r2¼ 0.540
Age r2¼ 0.549

Table 5Regression prediction functions by stepwise multiple linear model for three dyna-mometers based on hand circumference (in mm).
Dynamometer Regression prediction equation r Adjusted r2
Jamar (kg) MGS¼�65.477þ 0.524�Hand circumference
0.791 0.624
Myogrip (kg) MGS¼�67.895þ 0.523�Hand circumference
0.827 0.683
Vigorimeter (kpa) MGS¼�147.433þ 1.200�Hand circumference
0.694 0.478
All p< 0.0001.
A
B
C
Women
Men
Jamar
R² = 0.626
01020304050607080
150 160 170 180 190 200 210 220 230 240 250 260
Hand circumference (mm)
)gk(S
GM
MyoGrip
R² = 0.685
0
10
20
30
40
50
60
70
150 160 170 180 190 200 210 220 230 240 250 260
Hand circumference (mm))gk(
SG
M
Vigorimeter
R² = 0.481
020406080
100120140160180
150 160 170 180 190 200 210 220 230 240 250 260
Hand circumference (mm)
)aPk(S
GM
Fig. 2. Correlation between hand circumference and MGS measured by three dyna-mometers: A. Jamar; B. Myogrip; C. Vigorimeter.
K. Li et al. / Manual Therapy 15 (2010) 579e585 583
Besides age and gender, the correlation between severalanthropometric variables and MGS has been explored in severalpopulations of children and adults in various countries. Significantcorrelations were found between MGS and height, weight (Hantenet al., 1999; Hager-Ross and Rosblad, 2002; Schreuders et al., 2003;Gunther et al., 2008; Mitsionis et al., 2009), FFM (Aghazadeh et al.,1993; Innes, 1999; Almuzaini, 2007), forearm volume or circum-ference (Harries, 1985; Fraser et al., 1999; Vaz et al., 2002; Guntheret al., 2008), as well as hand volume, width, circumference orlength (Fraser et al., 1999; MacDermid et al., 2002; Kunelius et al.,2007; Gunther et al., 2008). The effect of hand dominance is stilla subject of debate regarding whether there is a consistent differ-ence in grip strength between dominant and non-dominant hands(Innes, 1999; Mitsionis et al., 2009).
Height andweight are two important anthropometric factors forpredicting MGS. However, they are too global to describe gripstrength with a good reliability. Their importance is evidently lessthan local anthropometric data such as hand, wrist and forearmcircumference, or hand and palm length (see Table 2). Among allthe parameters highly correlated with MGS, the strongest corre-lated one was hand circumference. Consistent results were found(see Table 4) when the stepwise multiple linear regression wasapplied. The only parameter that was systematically selected washand circumference, which was then chosen as the sole parameterto establish the final predictive models (see Table 5). This findingwas the same for both dominant and non-dominant hands.Although grip strength for the dominant hand was significantlyhigher than for the non-dominant hand, hand circumferences werealso larger for dominant hands. Thus a single predictive equationwas able to be used for both hands. Our results are similar to thoseof Nicolay and Walker who found a correlation of 0.826 betweenpalm width and MGS (to be compared to 0.789 for the Jamar and0.829 for the MyoGrip in the present study) (Nicolay and Walker,2005). Desrosiers et al. (1995) found also strong correlationsbetween strength and hand circumference, with stronger correla-tions observed for the Jamar than for the Vigorimeter.
The initial interpretation of selection of hand circumference asthe preferred variable seems counterintuitive since the musclesused to produce grip force are predominantly located in the
Table 6Characteristics and anthropometric data for the additional subject group.
Men (n¼ 17) Women (n¼ 12)
Mean (SD) Range Mean (SD) Range
Age (y) 21.5 (1.8) 19e24 21.5 (1.7) 19e24Height (cm) 179.0 (5.8) 170e190 165.8 (6.3) 153e175Weight (kg) 71.8 (8.3) 60e92 59.9 (7.0) 50e70BMI (kg/m2) 22.4 (1.9) 19.4e25.8 21.8 (2.1) 18.4e25.1Hand circumference
(mm)*D 213.8 (8.3) 201e233 187.8 (7.8) 170e205ND 207.9 (8.0) 195e220 189.7 (8.4) 170e202
D: dominant side; ND: non-dominant side.*Significantly different between sides (p< 0.0001).
forearm (Rice et al., 1998). However, the forearm volume, in addi-tion to the FFM, is also heavily influenced by the amount of fat. Sucha relationship can be seen in the very large correlation found in thepresent study between forearm circumference and BMI (r¼ 0.747).In contrast, hand volume is less related to the amount of fat asshown by the moderate correlation between BMI and handcircumference (r¼ 0.497). In addition, the anatomical landmarksfor hand circumference (palm creases) are easier to standardizethan those of the forearm (largest diameter of the proximal quarterof the forearm).
The population used in the present study was selected in orderto be as homogeneous as possible to eliminate the possible effectsof age, physical activity levels, injuries, and issues related to under-or over-weight. No subjects had prior hand or forearm injuries,while no subjects performed physical activity more than four timesper week. The BMI of subjects fell within 17 and 27 kg/m2. In sucha population, hand and forearm circumferences are stronglycorrelated (r¼ 0.849) and may be seen as a redundant informationif both are used. However, when the subjects are involved ina situation in which the forearm volume is prone to be changed(muscle atrophy or obesity for instance), the relationship betweenhand and forearm circumferences may be modified.

0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1Observed cumulative probability
Pred
icte
dcu
mul
ativ
e pr
obab
ility
A
B
C
y = 1.016xR²=0.683
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60 70Predicted MGS (kg)
Mea
sure
dM
GS
(kg)
-20
-15
-10
-5
0
5
10
15
20
20 30 40 50 60
Predicted MGS (kg)
Res
idua
lMG
S (k
g)
Fig. 3. Results on a population of 29 additional subjects for the Myogrip dynamometer.A. Relation between measured and predicted MGS. B. Residual cumulative probability.C. Relation between residuals and predicted MGS.
K. Li et al. / Manual Therapy 15 (2010) 579e585584
Hand circumference is obviously not the sole determinant ofgrip strength. Many genotypic and phenotypic parameters, as wellas psychological, methodological, environmental variables mayinfluence physical performance. This is the reason why between-and evenwithin-individual variabilities are large. Predictivemodelsare designed to get a statistical picture of the MGS of an individualbut allow impairment detection and follow-up. Maximal strength isonly one aspect of neuromuscular function, but this is a variable
that has been shown to be correlated with global neuromuscularfunctioning (Nybo et al., 2001; Chan et al., 2008).
Indeed, regular measurement of MGS should be performed,preferably at home using a convenient setup, in order to geta robust way of following MGS changes over time, as it can be donefor body weight or blood pressure. As suggested by Kerr et al.(2006) and Bohannon (2006), “grip strength should be measuredroutinely alongside the measurement of blood pressure”.
Themain result of this study is particularly important as it showsthat grip strength is directly proportional to morphological devel-opment andmuscle trophicity. In otherwords, specific grip-strengthcapacities, prior to the onset of aging and sarcopenia, are indepen-dent of gender, dominance or age. Further analyses in children andelderly people obviously need to be performed to support the use ofhand circumference alone to predict grip strength.
Acknowledgements
The authors would like to thank the China Scholarship Council(CSC) for the financial support for Ke Li and all the subjects for theirparticipation in the experiments. This study was partly supportedby the Association Française contre les Myopathies (AFM).
References
Aghazadeh F, Lee K, Waikar A. Impact of anthropomatric and personal variables ongrip strength. J Hum Ergol 1993;22:75e81.
Almuzaini KS. Muscle function in Saudi children and adolescents: relationship toanthropometric characteristics during growth. Pediatr Exerc Sci 2007;19(3):319e33.
Anakwe RE, Huntley JS, McEachan JE. Grip strength and forearm circumference ina healthy population. J Hand Surg Eur 2007;2:203e9.
Ansari K, Shamssain M, Keaney NP, Burns G, FarrowM. Predictors of quality of life inchronic obstructive pulmonary disease patients with different frequency ofexacerbations. Pak J Med Sci 2007;23(4):490e6.
Avlund K, Schroll M, Davidsen M, Løvborg B, Rantanen T. Maximal isometric musclestrength and functional ability in daily activities among 75-year-old men andwomen. Scand J Med Sci Sports 1994;4:32e40.
Balogun JA, Akinloye AA, Adenlola SA. Grip strength as a function of age, height,body weight and Quetelet index. Physiother Theory Pract 1991;7:111e9.
Bishop P, Cureton K, Collins M. Sex difference in muscular strength in equally-trained men and women. Ergonomics 1987;30(4):675e87.
Bohannon RW. Hand-grip dynamometry provides a valid indication of upperextremity strength impairment in home care patients. J Hand Ther 1998;11(4):258e60.
Bohannon RW. Adequacy of simple measures for characterizing impairment inupper limb strength following stroke. Percept Mot Skills 2004;99(3 Pt 1):813e7.
Bohannon RW. Grip strength predicts outcome. Age Ageing 2006;35:320.Chan DC, Lee WT, Lo DH, Leung JC, Kwok AW, Leung PC. Relationship between grip
strength and bone mineral density in healthy Hong Kong adolescents. Osteo-poros Int 2008;19(10):1485e95.
Chin APMJ, Dekker JM, Feskens EJ, Schouten EG, Kromhout D. How to select a frailelderly population? A comparison of three working definitions. J Clin Epidemiol1999;52(11):1015e21.
Crosby CA, Wehbe MA, Mawr B. Hand strength: normative values. J Hand Ther1994;19(4):665e70.
Desrosiers J, Hebert R, Bravo G, Dutil E. Comparison of the Jamar dynamometer andthe Martin vigorimeter for grip strength measurements in a healthy elderlypopulation. Scand J Rehab Med 1995;27(3):137e43.
Fraser A, Vallow J, Preston A, Cooper RG. Predicting ‘normal’ grip strength forrheumatoid arthritis patients. Rheumatology 1999;38(6):521e8.
Frederiksen H, Gaist D, Petersen HC, Hjelmborg J, McGue M, Vaupel JW, et al. Handgrip strength: a phenotype suitable for identifying genetic variants affectingmid- and late-life physical functioning. Genet Epidemiol 2002;23(2):110e22.
Gunther CM, Burger A, Rickert M, Crispin A, Schulz CU. Grip strength in healthyCaucasian adults: reference values. J Hand Surg Am 2008;33(4):558e65.
Hager-Ross C, Rosblad B. Norms for grip strength in children aged 4e16 years. ActaPaediatr 2002;91(6):617e25.
HantenWP, ChenWY, Austin AA, Brooks RE, Carter HC, Law CA, et al. Maximum gripstrength in normal subjects from 20 to 64 years of age. J Hand Ther 1999;12(3):193e200.
Harries AD. A comparison of hand-grip dynamometry and armmuscle size amongstAfricans in North-East Nigeria. Hum Nutr Clin Nutr 1985;39(4):309e13.
Hinson M, Gench BE. The curvilinear relationship of grip strength to age. OccupTher J Res 1989;9:53e60.
Hopkins WG. A new view on statistics. Available from: http://www.sportsci.org/resource/stats/; 2000.

K. Li et al. / Manual Therapy 15 (2010) 579e585 585
Innes E. Handgrip strength testing: a review of the literature. Austr Occup Ther J1999;46:120e40.
Kallman DA, Plato CC, Tobin JD. The role of muscle loss in the age-related decline ofgrip strength: cross-sectional and longitudinal perspectives. J Gerontol 1990;45(3):M82e8.
Kerr A, Syddal HE, Cooper C, Turner GF, Briggs RS, Aihie Sayer A. Does admissiongrip strength predict length of stay in hospitalised older patients? Age Ageing2006;35:82e4.
Kunelius A, Darzins S, Cromie J, Oakman J. Development of normative data for handstrength and anthropometric dimensions in a population of automotiveworkers. Work 2007;28(3):267e78.
Li K, Hewson D, Hogrel JY. Influence of elbow position and handle size on maximalgrip strength. J Hand Surg Eur 2009;34E:692e4.
MacDermid J, Fehr L, Geiger K. The effect of physical factors on grip strength anddexterity. Br J Hand Ther 2002;7:112e8.
Mitsionis G, Pakos EE, Stafilas KS, Paschos N, Papakostas T, Beris AE. Normative dataon hand grip strength in a Greek adult population. Int Orthop 2009;33(3):713e7.
Nevill AM, Holder RL. Modelling handgrip strength in the presence of confoundingvariables: results from the Allied Dunbar National Fitness Survey. Ergonomics2000;43(10):1547e58.
Nicolay CW, Walker AL. Surface EMG and anatomical measurements as predictors ofgrip strength. Int J Ind Ergon 2005;35:605e18.
Niempoog S, Siripakarn Y, Suntharapa T. An estimation of grip strength duringpuberty. J Med Assoc Thai 2007;90(4):699e705.
Nybo H, Gaist D, Jeune B, McGue M, Vaupel JW, Christensen K. Functional status andself-rated health in 2,262 nonagenarians: the Danish 1905 Cohort Survey. J AmGeriatr Soc 2001;49(5):601e9.
Rauch F, Neu CM, Wassmer G, Beck B, Rieger-Wettengl G, Rietschel E, et al.Muscle analysis by measurement of maximal isometric grip force: newreference data and clinical applications in pediatrics. Pediatr Res 2002;51(4):505e10.
Rice VJ, Williamson TL, Sharp M. Using anthropometry and strength values topredict grip strength. In: Kumar S, editor. Adv occup ergonom safety. Amster-dam: IOS Press; 1998. p. 378e81.
Robertson LD, Mullinax CM, Brodowicz GR, Swafford AR. Muscular fatiguepatterning in power grip assessment. J Occup Rehabil 1996;6:71e85.
Sartorio A, Lafortuna CL, Pogliaghi S, Trecate L. The impact of gender, bodydimension and body composition on hand-grip strength in healthy children.J Endocrinol Invest 2002;25(5):431e5.
Sayer AA, Syddall HE, Martin HJ, Dennison EM, Roberts HC, Cooper C. Is gripstrength associated with health-related quality of life? Findings from theHertfordshire Cohort Study. Age Ageing 2006;35(4):409e15.
Schreuders TA, Roebroeck ME, Goumans J, van Nieuwenhuijzen JF, Stijnen TH,Stam HJ. Measurement error in grip and pinch force measurements in patientswith hand injuries. Phys Ther 2003;83(9):806e15.
Sinaki M, Nwaogwugwu NC, Phillips BE, Mokri MP. Effect of gender, age, andanthropometry on axial and appendicular muscle strength. Am J Phys MedRehabil 2001;80(5):330e8.
Vaz M, Hunsberger S, Diffey B. Prediction equations for handgrip strength inhealthy Indian male and female subjects encompassing a wide age range. AnnHum Biol 2002;29(2):131e41.
Visser J, Mans E, de Visser M, van den Berg-Vos RM, Franssen H, de Jong JM, et al.Comparison of maximal voluntary isometric contraction and hand-held dyna-mometry in measuring muscle strength of patients with progressive lowermotor neuron syndrome. Neuromuscular Disord 2003;13(9):744e50.