Precision Dosing of Immunosuppression: A Pharmacogenomics Perspective · 2019-07-22 ·...
58
Medhat Askar, MD, PhD, MSHPE, FRCPath Transplant Immunology & Cell Processing Laboratories Baylor University Medical Center Professor, Pathology & Lab Medicine Texas A & M HSC College of Medicine Precision Dosing of Immunosuppression: A Pharmacogenomics Perspective
Transcript of Precision Dosing of Immunosuppression: A Pharmacogenomics Perspective · 2019-07-22 ·...

Medhat Askar, MD, PhD, MSHPE, FRCPathTransplant Immunology & Cell Processing Laboratories
Baylor University Medical Center
Professor, Pathology & Lab MedicineTexas A & M HSC College of Medicine
Precision Dosing of Immunosuppression: A
Pharmacogenomics Perspective

Outline• Background• Pharmacogenomics (PGx) as a tool for
precision medicine (PM) in solid organ transplantation
• Direct-To-Consumer PGx testing

Precision Medicine
Integration of molecular research with clinical data from individual patients to develop a more accurate molecular taxonomy of diseases that enhances diagnosis and treatment and tailors disease management to the individual characteristics of each patient (US Nat Acad of Sciences report, 2011)

Pharmacogenomics (PGx)
Pharmacogenomics is the field that combines pharmacology (the science of drugs) and genomics (the study of genes and their functions) to understand how genes affect a person’s response to drugs, develop effective and safe medications and determine the doses tailored to a person’s genetic makeup (US NCI Online Dictionary)

Problem Statement
Ø 2.2 million adverse drug reactions occur in the United States annually
Ø Medication efficacy rates vary considerably
Ø Unpredictable serious side effects

Existing PM tools
Ø Kidney function Ø And/or combination of:
– Weight – Age – Population-based nomograms

Strategies & Consequences
Ø Frequent dose monitoring and titration
Ø Iteration among medicationsØ Significant burdens on the patient,
the provider, and the health care system as a whole


Fig. 6. Newmodel (do we explain or predict?). The diamond box indicates the location of thePGx information in the decision making process. (From Brockmoller J, Kirchheiner J, Meisel C,Roots I. Pharmacogenetic diagnostics of cytochrome P450 polymorphisms in clinical drugdevelopment and in drug treatment. Pharmacogenomics 2000;1(2):137; with permission.)
Fig. 7. Genotype affects accumulation and time to steady state of blood drug concentra-tions. Example of warfarin concentrations for 3 genotypes with genetic variants ofCYP2C9. Note the time to reach steady state (vertical arrows) and accumulated concentra-tion of drug (horizontal arrows) are genotype variant-dependent. (From Linder MW, LooneyS, Adams JE, et al. Warfarin dose adjustments based on CYP2C9 genetic polymorphisms. JThromb Thrombolysis 2002;14(3):231; with permission.)
Fundamentals of Pharmacogenetics 455
Valdes & Yin, 2016

annotated pharmacogenomics resource that includes clinicalguidelines, FDA labeling, and pharmacogenomics-relatedpathways (5). Organizations that compile pharmacogeno-mics evidence to develop clinical guidelines include theClinical Pharmacogenetics Implementation Consortium(CPIC; www.cpicpgx.org) and the Dutch PharmacogeneticsWorking Group (15). The CPIC was created to overcomeimplementation barriers by developing standardized clinicalpharmacogenomics guidelines. Over 20 guidelines have beenpublished since 2012, and they are publicly available to aidclinicians in translating genetic laboratory test results intoactionable prescribing decisions (16).
Clinical Pharmacogenomics for the NephrologistIn the following sections, drug-gene pairs with clinical
guidelines and a high level of evidence in conditionscommonly treated by the nephrologist are presented. Thefocus is on cardiovascular disease and transplantationversus an exhaustive list of drugs and genes. Readers areencouraged to investigate the primary literature describedherein as a means to further learn about pharmacogeno-mics in relevant therapeutic areas. A summary of the gene-drug pairs and clinical guidelines discussed is provided inTable 2.
Cardiovascular DiseaseCardiovascular disease is a leading cause of death for
patients suffering from CKD. Hallmarks of cardiovascular
disease secondary to CKD are cardiac remodeling, athero-sclerosis, and arteriosclerosis (17). Pharmacogenomics ofcardiovascular disease is an active area of research andclinical implementation, with evidence-based guidelinesfor antiplatelets, anticoagulation, and hyperlipidemia(16,18,19).
Antiplatelet Agents and AnticoagulantsWarfarin. Warfarin is a vitamin K antagonist that in-
hibits coagulation by inhibiting the formation of coagu-lation factors II, VII, IX, and X and proteins C and S (20). Itis a narrow therapeutic index drug with high interpatientvariability and a delayed time to action (i.e., dose changesare not reflected in laboratory values for approximately72 hours) (21). Frequent monitoring of the internationalnormalized ratio (INR) over days to weeks is needed todetermine the right dose. Patients with impaired kidneyfunction are further known to require lower dosages ofwarfarin, have worse control of anticoagulation, and areat a higher risk for major hemorrhage (22).Warfarin pharmacokinetics and pharmacodynamics are
affected by multiple genotypes. Genetic variations affectingCYP2C9 and CYP4F2 metabolism and VKORC1 sensitivityare known to predict the dose needed to attain optimalanticoagulation (a therapeutic INR) but are not withoutcontroversy (23). In 2013, divergent clinical trial resultssignificantly diminished enthusiasm for routine warfarinpharmacogenomics in all patients. Although the EuropeanPharmacogenetics of Anticoagulation Therapy Studyshowed that use of a pharmacogenomics algorithm
Figure 3. | Simulated dosing data for drug X after patient titration toeffect shows distinct subpopulations based on genetics. A shows thedistribution of total daily dose among the aggregate population,suggesting a mostly normal distribution of doses. B shows populationsubstructure on the basis of genetic variants in the gene responsible formetabolism of drug X for poor metabolizers (PMs), intermediatemetabolizers (IMs), normal metabolizers (NMs), rapid metabolizers(RMs), and ultrapid metabolizers (UMs). Patients with decreasedmetabolism of drug X (PMs and IMs) have a lower effective dose,whereas patients with increased metabolism (RMs and UMs) requirehigher doses. This shows the utility of pharmacogenomics-baseddosing in addition to clinical factors to identify subpopulations.
Table 1. Selected gene alleles, their causative variations, andassociated phenotypes
Gene and Allele CausativeVariation(s) Phenotype
CYP2C9*2 rs1799853 (T) Decreased function*3 rs1057910 (C) Decreased function
CYP4F2*3 rs2108622 (T) Decreased function
CYP3A5*3 rs776746 (C) Decreased function
CYP2C19*2 rs4244285 (A) Decreased function*3 rs4986893 (A) Decreased function*17 rs12248560 (T) Increased function
TPMT*2 rs1800462 (G) Decreased function*3A rs1800460 (T);
rs1142345 (C)Decreased function
*3B rs1800460 (T) Decreased function*3C rs1142345 (C) Decreased function*4 rs1800584 (T) Decreased function
VKORC121639G.A rs9923231 (T) Increased sensitivity
to warfarinSLCO1B1*5 rs4149056 (C) Decreased function
HLA-B*58:01 N/A Increased SCAR risk
TPMT, thiopurine methyltransferase; N/A, not applicable;SCAR, severe cutaneous adverse reaction.
1564 Clinical Journal of the American Society of Nephrology
Adams et al, 2018

PGx in Solid Organ Tx
http://www.phaeurope.org/

ORIGINAL ARTICLE
Higher calcineurin inhibitor levels predict betterkidney graft survival in patients with de novodonor-specific anti-HLA antibodies: a cohort study
Marc-Antoine B!eland1, Isabelle Lapointe1, R!eal No€el1, Isabelle Cot!e1, Eric Wagner2, Julie Riopel3, EvaLatulippe3, Olivier D!esy1, St!ephanie B!eland1, Ciara N. Magee4, Isabelle Houde1 & Sacha A. De Serres1
1 Transplantation Unit, RenalDivision, Department of Medicine,Faculty of Medicine, UniversityHealth Center of Quebec, LavalUniversity, Quebec, QC, Canada
2 Immunology andHistocompatibility Laboratory,Faculty of Medicine, UniversityHealth Center of Quebec, LavalUniversity, Quebec, QC, Canada
3 Department of Pathology, Facultyof Medicine, University HealthCenter of Quebec, Laval University,Quebec, QC, Canada
4 Department of Nephrology &Renal Transplantation, UCL Centrefor Nephrology, Royal Free LondonNHS Foundation Trust, London, UK
CorrespondenceSacha A. De Serres MD SM FRCPC,
Transplantation Unit, Renal Division,
Department of Medicine, Faculty of
Medicine, University Health Center of
Quebec, Laval University, 11 Cote du
Palais, Quebec, QC, Canada, G1R
2J6.
Tel.: 418-691-5464;
fax: 418-691-5757;
e-mail:
SUMMARYThe development of de novo anti-HLA donor-specific antibodies (dnDSA)is associated with poorer outcomes in kidney transplant recipients. Despitethis, antibody screening post-transplant is not widespread, largely becausethe optimal management of patients with dnDSA remains undetermined.We hypothesized that in this population, calcineurin inhibitor blood levelswould be an independent predictor of graft loss. We analyzed a cohort ofunsensitized patients for whom anti-HLA antibody screening was per-formed prospectively post-transplant. During the screening period betweenJanuary 2005 and April 2016, 42 patients developed dnDSA. There was nodifference in the clinical characteristics or the histological scores of patientsbiopsied for clinical indication versus those biopsied solely due to detec-tion of dnDSA. Cox modeling revealed a strong relationship between meantacrolimus levels following dnDSA detection and graft loss, with a hazardratio of 0.49 (95% CI, 0.33–0.75), which persisted following adjustment forestablished independent predictors (HR, 0.52, 95% CI, 0.30–0.89). Kaplan–Meier analysis by tertiles of tacrolimus levels and receiver operating curveanalysis concurred to show that a threshold of 5.3 ng/ml could be predic-tive of graft loss. These data suggest that anti-HLA antibody monitoringpost-transplant could guide maintenance immunosuppression and improvegraft outcomes.
Transplant International 2017; 30: 502–509
Key wordscalcineurins antagonists, histocompatibility, HLA-antibody post-transplantation, immunogenetics,
immunosuppression clinical, immunosuppression kidney clinical
Received: 16 January 2017; Revision requested: 23 January 2017; Accepted: 31 January 2017;
Published online: 5 March 2017
Introduction
The association between the appearance of donor-specific anti-HLA antibodies (DSA) after kidney trans-plantation, referred to as de novo DSA (dnDSA), andpoor graft outcome is clearly established [1,2]. How-ever, the optimal management for patients whodevelop dnDSA has yet to be determined. Different
protocols have been described for the treatment ofacute antibody-mediated rejection (ABMR), but veryfew studies have reported on the treatment of patientswith dnDSA in the context of chronic ABMR, andthere is no clear therapeutic strategy for patients whodevelop dnDSA in the absence of rejection [2,3].Given the lack of such data, there is reluctance to useplasma exchange, IVIG and rituximab in the absence
ª 2017 Steunstichting ESOTdoi:10.1111/tri.12934
502
Transplant International
of acute ABMR, due to the toxicity associated withthese treatments.
It is also unclear if escalation of maintenance immuno-suppression, in particular increased target levels of cal-cineurin inhibitors (CNIs), would improve the outcomesof these patients. We recently reported that patients withtransplant glomerulopathy were more likely to have beenprescribed reduction or withdrawal of immunosuppres-sion, most frequently characterized by reduced CNIs [4].Indeed, many CNI-sparing clinical trials have resulted inhigher rejection rates [5–9]. From an immunologicalstandpoint, the detection of dnDSA indicates plasma cellsecretion of high-affinity alloantibodies, a process notreversible by CNIs. However, it is has long been knownthat CNIs can inhibit B-cell activation both directly, pre-dominantly by blocking cell cycle progression throughlate G1 [10], and indirectly, by inhibiting T-cell activationand consequent B-cell activity. It is not yet established ifeither mechanism is sufficient to reduce ongoingimmunologic damage to the graft and improve outcomesin patients with dnDSA.
We hypothesized that, in patients with dnDSA, higherblood CNI levels would be associated with better clinicaloutcomes. The aim of this study was to examine the rela-tionship between CNI blood levels and graft loss in a con-secutive cohort of kidney transplant recipients in whomdnDSA were detected prospectively and longitudinally byroutine clinical protocol. We show that there is a stronglypositive, independent association between higher CNIblood levels and graft survival, suggesting that DSA mon-itoring is clinically beneficial and can direct optimalpatient management to improve graft outcome.
Materials and methods
Study design and population
This is a single-center, observational cohort study withprospective detection of circulating anti-HLA alloanti-bodies and prospective collection of follow-up clinicaldata. The study population consisted of consecutivepatients in whom alloantibodies were detected duringthe screening period from January 2005 to April 2016,which corresponds to the time during which alloanti-body detection was carried out using sensitive tech-niques for screening and identification, as detailedbelow. All incident kidney transplant recipients wereroutinely monitored for anti-HLA alloantibody develop-ment at 1, 3, 6 and 12 months in the first year post-transplant and yearly thereafter. Antibody monitoringwas also conducted at the time of any protocol or
indication biopsy, and 2–4 weeks following any signifi-cant sensitizing event. Any patient demonstrating atleast one dnDSA was included. No patient was sensi-tized at the time of transplantation, and no patientswere lost to follow-up. The study was approved by theinstitutional ethics committee. The clinical and researchactivities reported are consistent with the Principles ofthe Declaration of Istanbul.
Anti-HLA antibody assessment
Serum samples were screened for anti-HLA antibodiesby flow cytometry using FlowPRA beads (One Lambda,Canoga Park, CA, USA). Whenever antibody screeningwas positive, samples were tested for anti-HLA antibodyidentification by flow cytometry using flow single anti-gen beads from 2005 to 2012. Starting in 2012, HLAantibody identification was performed using LABScreensingle antigen beads (One Lambda) on a Luminex plat-form. Antibody specificities were identified based onnormalized mean fluorescence intensity (nMFI) ≥1500.However, HLA specificities falling below the establishednMFI cutoff were also considered positive if a reactivitypattern consistent with a commonly shared expressedepitope was seen. Such was the case in two patients.Analysis of epitope reactivity is verified using the HLAepitope registry (http://epregistry.ufpi.br).
Donor HLA-DQ typing data were not available forthree of seven patients with anti-DQ antibodies. Unfor-tunately, typing could not be repeated retrospectively asno stored donor DNA or cell sample was available. AsHLA-DR typing was available for all donors, HLA-DQtyping was assigned based on frequency associationswithin the donor ethnic group. This was performedusing NMDP data (Haplostats). Whenever initialpatient HLA-DQ typing was unavailable, it was per-formed retrospectively to rule out any nonspecific reac-tivity or autoreactivity.
Pathologic classification
Biopsies were prospectively graded by the local attend-ing pathologists (J.R. and E.L.) according to the Banff1997 criteria, which were updated in 2003, 2008 and2013 [11–13]. Pathologists were blinded to the resultsof antibody monitoring.
Measurement of CNI exposure
Exposure to tacrolimus was defined as the mean ofblood levels measured at 1, 3, 6, 12 and 24 months
Transplant International 2017; 30: 502–509 503ª 2017 Steunstichting ESOT
DSA, tacrolimus levels and graft loss

Importantly, the hazard ratio was similar when the anal-ysis was restricted to the patients who were biopsied(Table 2, adjusted model 2), and the analysis was robustto the adjustment for arteriolar hyalinosis (ah score)and interstitial fibrosis/tubular atrophy (IFTA score).Overall, these results indicate that the mean tacrolimuslevel in the first 2 years post-dnDSA detection is astrong, independent predictor of graft survival, and thisassociation persists when only biopsied patients are ana-lyzed.
To further assess the relevance of the associationbetween tacrolimus levels and graft survival in the realclinical setting, we next categorized tacrolimus levels bytertiles, which generated cutoffs at 5.3 and 6.3 ng/ml.There was a significant difference between the threegroups, with eight events in the lowest tertile, three inthe middle tertile and one in the highest tertile(P = 0.005 by log-rank; Fig. 2). An analysis restricted tothe biopsied patients showed similar results (Fig. S1).Categorizing the cohort into quartiles, with cutoffs at5.0, 6.0 and 7.2 did not improve the identification of anoptimal level (Fig. S2a). A receiver operating curve
(ROC) analysis built to identify graft survival as theevent concurred with the Kaplan–Meier plot shown inFig. 2 to indicate that a tacrolimus level of 5.3 had thebest predicting accuracy for graft survival (area under
Figure 1 Tacrolimus levels over time.
(a) Histogram showing the
distribution of individual mean
tacrolimus levels post-dnDSA
development. (b) Tacrolimus levels at
the time of dnDSA, and mean
tacrolimus levels post-dnDSA
development. Each line represents a
single patient.
Table 2. Univariate and multivariate risk estimates for graft loss associated with tacrolimus levels post-dnDSA detection
Hazard ratio (95% CI) P-value
TAC levels as continuous variable (ng/ml)Unadjusted (n = 42) 0.49 (0.33–0.75) 0.001Adjusted model 1 (n = 42)* 0.45 (0.27–0.76) 0.003Adjusted model 2 (n = 23)†,‡ 0.52 (0.30–0.89) 0.019Adjusted model 3 (n = 23)‡,§ 0.26 (0.07–0.99) 0.049
*Adjusted for delayed graft function and nonadherence.
†Adjusted for delayed graft function and nonadherence, tubulitis score and transplant glomerulopathy score.
‡Analyzed restricted to the 23 patients who had a biopsy.
§Adjusted for delayed graft function and nonadherence, tubulitis, transplant glomerulopathy, interstitial fibrosis, tubular atro-phy and arteriolar hyaline thickening scores.
Figure 2 Kaplan–Meier plots for graft loss by tertile of mean tacroli-
mus levels post-dnDSA development. Comparison was assessed using
log-rank test.
506 Transplant International 2017; 30: 502–509ª 2017 Steunstichting ESOT
B!eland et al.
Béland et al, 2017

SPECIAL FEATURE
Effect on Kidney Graft Survival of Reducing orDiscontinuing Maintenance Immunosuppression After
the First Year PosttransplantGerhard Opelz and Bernd Dohler
Background. Data are scarce concerning the impact of maintenance immunosuppression dose reductions posttransplant.Methods. Graft survival according to dose reduction or discontinuation of calcineurin inhibitors or mycophenolatemofetil (MMF) after the first year posttransplant was evaluated in 25,045 patients undergoing kidney transplantationduring 1996 to 2005. No patient in this analysis had experienced a rejection and all had good graft function before dosereduction.Results. Reduction of cyclosporine (CsA) dose to less than or equal to 150 mg/day, tacrolimus to less than or equal to2 mg/day, or MMF to less than or equal to 1.0 g/day in patients on CsA or less than or equal to 0.5 g/day in patients ontacrolimus during the second year posttransplant was associated with a statistically significant reduction in graftsurvival (hazard ratios between 1.37 and 1.65). Withdrawal of CsA, tacrolimus, or MMF during year 2 was alsoassociated with an increase in the risk of graft loss compared with continuing treatment (hazard ratio 1.52–1.73).Conclusions. This observational analysis indicates that in kidney transplant patients with good graft function, with-drawing maintenance CsA, tacrolimus or MMF, or reducing the dose of these agents below certain thresholds after thefirst year posttransplant is associated with a significant risk of graft loss.
Keywords: Maintenance immunosuppression, Dose reduction, Calcineurin inhibitors, Mycophenolic acid, Kidneytransplant.
(Transplantation 2008;86: 371–376)
The current emphasis in posttransplant immunosuppres-sion is to minimize the risk of long-term complications
that can threaten either graft survival (e.g., nephrotoxicity) orpatient survival (e.g., hypertension, diabetes mellitus, infec-tion, or malignancy) (1). Accordingly, maintenance immu-nosuppression doses in kidney transplant recipients arereduced and even complete withdrawal of calcineurin inhib-itor (CNI) therapy is becoming more common in an attemptto avoid these complications and, in particular, chronic allo-graft nephropathy (2).
It remains unclear, however, at what point the benefitsof less intensive immunosuppression are balanced or evenoutweighed by insufficient protection against acute or sub-clinical rejection. It is already well-established that patientsreceiving high CNI doses experience worse graft functionthan those on lower doses (3), in part because the dose ishigher in at-risk patients or after rejection, and in part be-
cause of greater risk of CNI-related nephrotoxicity (4). Thereis, however, a noticeable lack of evidence relating to graftoutcome associated with reduced CNI doses.
The Collaborative Transplant Study (CTS) collects in-formation on the daily dose of immunosuppressive agents atintervals from year 1 posttransplant onwards. We have pre-viously published CTS data from kidney transplants under-taken during a previous era of transplantation (1985–1998)showing that low doses of cyclosporine (CsA) are associatedwith worse graft survival (5). Immunosuppressive practicehas evolved in more recent years with, among other changes,use of lower CNI doses and adoption of mycophenolic acid(MPA) as routine adjunctive therapy (6).
Here, we evaluate graft outcomes in kidney transplantpatients according to the maintenance dose of the immuno-suppressive agents most frequently reported to the CTS inthis population: CsA, tacrolimus, and mycophenolate mofetil(MMF). Our objective was to determine whether patientswhose dose of maintenance immunosuppression is reducedbelow a certain threshold experience impaired long-termoutcomes.
MATERIALS AND METHODSPatients reported to the CTS who received a kidney
transplant from a deceased donor during 1996 to 2005 wereincluded in the analysis if they were more than or equal to 18years at time of transplant. All patients were required to be
Department of Transplantation Immunology, University of Heidelberg,Heidelberg, Germany.
Address correspondence to: Gerhard Opelz, M.D., Department of Trans-plantation Immunology, University of Heidelberg, Im NeuenheimerFeld 305, D-69120 Heidelberg, Germany.
E-mail: [email protected] 29 February 2008. Revision requested 7 April 2008.Accepted 30 April 2008.Copyright © 2008 by Lippincott Williams & WilkinsISSN 0041-1337/08/8603-371DOI: 10.1097/TP.0b013e31817fdddb
Transplantation • Volume 86, Number 3, August 15, 2008 371
SPECIAL FEATURE
Effect on Kidney Graft Survival of Reducing orDiscontinuing Maintenance Immunosuppression After
the First Year PosttransplantGerhard Opelz and Bernd Dohler
Background. Data are scarce concerning the impact of maintenance immunosuppression dose reductions posttransplant.Methods. Graft survival according to dose reduction or discontinuation of calcineurin inhibitors or mycophenolatemofetil (MMF) after the first year posttransplant was evaluated in 25,045 patients undergoing kidney transplantationduring 1996 to 2005. No patient in this analysis had experienced a rejection and all had good graft function before dosereduction.Results. Reduction of cyclosporine (CsA) dose to less than or equal to 150 mg/day, tacrolimus to less than or equal to2 mg/day, or MMF to less than or equal to 1.0 g/day in patients on CsA or less than or equal to 0.5 g/day in patients ontacrolimus during the second year posttransplant was associated with a statistically significant reduction in graftsurvival (hazard ratios between 1.37 and 1.65). Withdrawal of CsA, tacrolimus, or MMF during year 2 was alsoassociated with an increase in the risk of graft loss compared with continuing treatment (hazard ratio 1.52–1.73).Conclusions. This observational analysis indicates that in kidney transplant patients with good graft function, with-drawing maintenance CsA, tacrolimus or MMF, or reducing the dose of these agents below certain thresholds after thefirst year posttransplant is associated with a significant risk of graft loss.
Keywords: Maintenance immunosuppression, Dose reduction, Calcineurin inhibitors, Mycophenolic acid, Kidneytransplant.
(Transplantation 2008;86: 371–376)
The current emphasis in posttransplant immunosuppres-sion is to minimize the risk of long-term complications
that can threaten either graft survival (e.g., nephrotoxicity) orpatient survival (e.g., hypertension, diabetes mellitus, infec-tion, or malignancy) (1). Accordingly, maintenance immu-nosuppression doses in kidney transplant recipients arereduced and even complete withdrawal of calcineurin inhib-itor (CNI) therapy is becoming more common in an attemptto avoid these complications and, in particular, chronic allo-graft nephropathy (2).
It remains unclear, however, at what point the benefitsof less intensive immunosuppression are balanced or evenoutweighed by insufficient protection against acute or sub-clinical rejection. It is already well-established that patientsreceiving high CNI doses experience worse graft functionthan those on lower doses (3), in part because the dose ishigher in at-risk patients or after rejection, and in part be-
cause of greater risk of CNI-related nephrotoxicity (4). Thereis, however, a noticeable lack of evidence relating to graftoutcome associated with reduced CNI doses.
The Collaborative Transplant Study (CTS) collects in-formation on the daily dose of immunosuppressive agents atintervals from year 1 posttransplant onwards. We have pre-viously published CTS data from kidney transplants under-taken during a previous era of transplantation (1985–1998)showing that low doses of cyclosporine (CsA) are associatedwith worse graft survival (5). Immunosuppressive practicehas evolved in more recent years with, among other changes,use of lower CNI doses and adoption of mycophenolic acid(MPA) as routine adjunctive therapy (6).
Here, we evaluate graft outcomes in kidney transplantpatients according to the maintenance dose of the immuno-suppressive agents most frequently reported to the CTS inthis population: CsA, tacrolimus, and mycophenolate mofetil(MMF). Our objective was to determine whether patientswhose dose of maintenance immunosuppression is reducedbelow a certain threshold experience impaired long-termoutcomes.
MATERIALS AND METHODSPatients reported to the CTS who received a kidney
transplant from a deceased donor during 1996 to 2005 wereincluded in the analysis if they were more than or equal to 18years at time of transplant. All patients were required to be
Department of Transplantation Immunology, University of Heidelberg,Heidelberg, Germany.
Address correspondence to: Gerhard Opelz, M.D., Department of Trans-plantation Immunology, University of Heidelberg, Im NeuenheimerFeld 305, D-69120 Heidelberg, Germany.
E-mail: [email protected] 29 February 2008. Revision requested 7 April 2008.Accepted 30 April 2008.Copyright © 2008 by Lippincott Williams & WilkinsISSN 0041-1337/08/8603-371DOI: 10.1097/TP.0b013e31817fdddb
Transplantation • Volume 86, Number 3, August 15, 2008 371

was 50.4% and 62.1%, respectively. In total, 6395 patients(25.5%) were receiving azathioprine (5167 CsA, 1228 tacroli-mus) and 21,220 patients (84.7%) were receiving steroids(14,484 CsA, 6736 tacrolimus) at 1 year after transplantation.
Influence of Dose on Graft SurvivalMultivariate analysis to determine reasonable cut-offs
for studying the effect of dose reduction showed that, with theexception of MMF dose in association with tacrolimus, therewere cut-offs in daily dose below which graft survival wassignificantly impaired: CsA less than or equal to 150 mg/day(HR 1.20, 95% CI 1.09 –1.32, P!0.001), tacrolimus less thanor equal to 2.0 mg/day (HR 1.34, 95% CI 1.06 –1.69,P"0.015), and MMF in combination with CsA less than orequal to 1.0 g/day (HR 1.32, 95% CI 1.05–1.65, P"0.016).The increased risk associated with low-dose MMF treatment(!0.5 g/day) in patients receiving tacrolimus did not reach
statistical significance (HR 1.13, 95% CI 0.82–1.55, P"0.47).Based on these results, different cut-offs were used for thesubsequent dose reduction analysis of MMF: 1.0 g/day forpatients on CsA and 0.5 g/day for patients on tacrolimus.
Influence of Dose Reduction on Graft SurvivalThe effect of dose reduction during the second post-
transplant year on graft survival during the subsequent 5years (i.e., years 3–7 posttransplant) is shown in Table 1. Forboth CsA and tacrolimus, a reduction in dose to below the“cut-off” points of 150 and 2.0 mg/day, respectively, was as-sociated with a significant reduction in graft survival and as-sociated HR values of 1.37 and 1.65, respectively. The clinicalimpact, in terms of progressively deteriorating graft survivalover time, is illustrated in Figure 2. Reducing the dose of CsAfrom higher doses to doses more than 150 mg/day or tacroli-mus to doses more than 2.0 mg/day was not associated withimpaired graft survival (data not shown).
Reducing the dose of MMF in CsA-treated patients toless than or equal to 1.0 g/day or to less than or equal to 0.5g/day in tacrolimus-treated patients was also associated withimpaired graft survival (HR 1.51, Table 1, Fig. 2).
There was no evidence that concomitant steroidswere simultaneously increased to compensate for CNI orMMF dose reductions. Similarly, there was no evidencethat MMF dose was increased in patients in whom CsA ortacrolimus dose was decreased.
Influence of Drug WithdrawalComplete withdrawal of CsA, tacrolimus or MMF dur-
ing the second posttransplant year was associated with anincrease in the risk of graft loss compared with continuingtreatment (Fig. 2, Table 1). None of the patients included inthis study was switched from one CNI to another. We did notobserve concomitant dose increases for steroids or MMF inpatients in whom CsA or tacrolimus was reduced to belowthreshold levels, or in patients in whom CNIs were with-drawn altogether. Interestingly, of patients in whom CNIwere withdrawn during the second posttransplant year, 31%were once again receiving CNI treatment at the end of thethird year, suggesting that CNI withdrawal was not successfulin these individuals.
CsA
0
100
95
90
85
80
75
70
65
% G
raft
Sur
viva
l
0 1 2 3 4 5 6 7
6,507 n=Continuation991 n=Reduction218 n=Withdrawal
Tacrolimus
0
100
95
90
85
80
75
70
65
0 1 2 3 4 5 6 7
Years post-transplant
1,736 n=Continuation352 n=Reduction296 n=Withdrawal
MMF
0
100
95
90
85
80
75
70
65
0 1 2 3 4 5 6 7
4,759 n=Continuation 589 n=Reduction614 n=Withdrawal
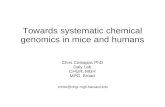
FIGURE 2. Graft survival during years 3 to 7 posttransplant according to dose reductions or withdrawal of CsA, tacroli-mus, and MMF during the second posttransplant year, compared with patients continuing to receive an unchanged dose. AllP values less than 0.001 for reduction or withdrawal vs. continuation (log rank).
TABLE 1. Graft survival during years 3 to 7 afterkidney transplantation according to dose reduction (atyear 2 after transplantation: CsA !150 mg/day,tacrolimus !2.0 mg/day, MMF with CsA !1.0 g/day, MMFwith tacrolimus !0.5 g/day) or withdrawal of medicationduring second posttransplant year
Change in dosage N
Graft survival
P HR 95% CI
CsAContinuation 6507 1.00Reduction 991 !0.001 1.37 1.16–1.61Withdrawal 218 0.005 1.53 1.14–2.06
TacrolimusContinuation 1736 1.00Reduction 352 0.004 1.65 1.18–2.32Withdrawal 296 0.027 1.52 1.05–2.21
MMFContinuation 4759 1.00Reduction 589 !0.001 1.51 1.19–1.92Withdrawal 614 !0.001 1.73 1.38–2.18
© 2008 Lippincott Williams & Wilkins 373Opelz and Dohler
Opelz and Döhler, 2008
Years post-transplant

Higher Initial Tacrolimus Blood Levels and Concentration-Dose Ratiosin Kidney Transplant Recipients Who Develop Diabetes Mellitus
E. Rodrigo, M.A. de Cos, G. Fernández-Fresnedo, B. Sánchez, J.C. Ruiz, C. Pinera, R. Palomar,J.G. Cotorruelo, C. Gómez-Alamillo, S. Sanz de Castro, A.L.M. de Francisco, and M. Arias
ABSTRACTPosttransplantation diabetes mellitus (PTDM) is a common complication of kidneytransplantation, associated with poorer graft and patient outcomes. Tacrolimus is a strongimmunosuppressive drug associated with low acute rejection rates, but a higher risk forPTDM. High trough levels of tacrolimus during the first month after transplantation havebeen found to be a significant risk factor for the development of PTDM. The aim of thissingle-center study was to identify the risk factors for the development of PTDM amongkidney transplant recipients under tacrolimus therapy. We examined 73 cadaveric kidneytransplant recipients receiving tacrolimus between 1994 and 2003. Age, donor and recipientgender, dialysis method, body mass index (BMI), first year weight gain, mismatches, incidenceof acute rejection and delayed graft function, hepatitis C serology, first year cumulativesteroid dose, first tacrolimus blood level, first tacrolimus blood level !15 ng/mL, andcorresponding tacrolimus daily doses and concentration/dose ratios (CDR) were alsocollected. PTDM was defined as at least 2 fasting blood glucose values !126 mg/dL,according to the World Health Organization criteria. Incidence of first year PTDM was27.4%. Patients with PTDM showed significantly higher age, BMI, first tacrolimus bloodlevel, first tacrolimus CDR, and CDR with tacrolimus blood level !15 ng/mL as well as less1-year weight gain. After logistic regression, age (relative risk [RR] 1.060, confidenceinterval [CI] 95%, 1.001–1.122; P " .043) and first tacrolimus blood level (RR 1.154; CI95%, 1.038–1.283; P " .008) remain significant risk factors for developing PTDM. Olderage and initial tacrolimus blood levels were the main risk factors for PTDM among ourgroup of patients. Kidney transplant recipients who develop PTDM maintain a high CDRof tacrolimus.
POSTTRANSPLANTATION diabetes mellitus (PTDM),an increasingly common complication of kidney trans-
plantation, is associated with poorer graft and patientsurvival as well as increased incidence of infections andcardiovascular events.1,2 Tacrolimus is a strong immuno-suppressive drug that affords reduced acute rejection ratesas well as frequency of hyperlipidemia and hypertensionafter kidney transplantation. However, it is associated witha higher risk of PTDM, particularly when used as the initialimmunosuppressant.3,4 High trough levels of tacrolimusduring the first month after transplantation have beenshown to be a significant risk factor for the development ofPTDM.5 The aim of this single-center study was to assessthe risk factors for the development of PTDM amongkidney transplant recipients under tacrolimus therapy.
MATERIALS AND METHODS
Tacrolimus-treated renal transplant recipients engrafted in ourcenter between 1994 and 2003 were included in the study if theyhad a first blood level after at least 5 equal doses of tacrolimus andadequate data. We excluded patients with a known history ofglucose metabolism abnormalities. Among the 73 included pa-tients, tacrolimus trough concentrations were measured usingmicroparticle enzyme immunoassay (MEIA). The data set also
From the Services of Nephrology (E.R., G.F.-F., J.C.R., C.P.,R.P., J.G.C., C.G.-A., S.S.C., A.L.M.F., M.A.) and Clinical Phar-macology (M.A.C., B.S.), Hospital Valdecilla, University of Cant-abria, Santander, Spain.
Address reprint requests to Dr E. Rodrigo, Service of Nephrol-ogy, Hospital Valdecilla, Avda. Valdecilla s/n 39008, Santander,Spain. E-mail: [email protected]
© 2005 by Elsevier Inc. All rights reserved. 0041-1345/05/$–see front matter360 Park Avenue South, New York, NY 10010-1710 doi:10.1016/j.transproceed.2005.09.196
Transplantation Proceedings, 37, 3819–3820 (2005) 3819
Higher Initial Tacrolimus Blood Levels and Concentration-Dose Ratiosin Kidney Transplant Recipients Who Develop Diabetes Mellitus
E. Rodrigo, M.A. de Cos, G. Fernández-Fresnedo, B. Sánchez, J.C. Ruiz, C. Pinera, R. Palomar,J.G. Cotorruelo, C. Gómez-Alamillo, S. Sanz de Castro, A.L.M. de Francisco, and M. Arias
ABSTRACTPosttransplantation diabetes mellitus (PTDM) is a common complication of kidneytransplantation, associated with poorer graft and patient outcomes. Tacrolimus is a strongimmunosuppressive drug associated with low acute rejection rates, but a higher risk forPTDM. High trough levels of tacrolimus during the first month after transplantation havebeen found to be a significant risk factor for the development of PTDM. The aim of thissingle-center study was to identify the risk factors for the development of PTDM amongkidney transplant recipients under tacrolimus therapy. We examined 73 cadaveric kidneytransplant recipients receiving tacrolimus between 1994 and 2003. Age, donor and recipientgender, dialysis method, body mass index (BMI), first year weight gain, mismatches, incidenceof acute rejection and delayed graft function, hepatitis C serology, first year cumulativesteroid dose, first tacrolimus blood level, first tacrolimus blood level !15 ng/mL, andcorresponding tacrolimus daily doses and concentration/dose ratios (CDR) were alsocollected. PTDM was defined as at least 2 fasting blood glucose values !126 mg/dL,according to the World Health Organization criteria. Incidence of first year PTDM was27.4%. Patients with PTDM showed significantly higher age, BMI, first tacrolimus bloodlevel, first tacrolimus CDR, and CDR with tacrolimus blood level !15 ng/mL as well as less1-year weight gain. After logistic regression, age (relative risk [RR] 1.060, confidenceinterval [CI] 95%, 1.001–1.122; P " .043) and first tacrolimus blood level (RR 1.154; CI95%, 1.038–1.283; P " .008) remain significant risk factors for developing PTDM. Olderage and initial tacrolimus blood levels were the main risk factors for PTDM among ourgroup of patients. Kidney transplant recipients who develop PTDM maintain a high CDRof tacrolimus.
POSTTRANSPLANTATION diabetes mellitus (PTDM),an increasingly common complication of kidney trans-
plantation, is associated with poorer graft and patientsurvival as well as increased incidence of infections andcardiovascular events.1,2 Tacrolimus is a strong immuno-suppressive drug that affords reduced acute rejection ratesas well as frequency of hyperlipidemia and hypertensionafter kidney transplantation. However, it is associated witha higher risk of PTDM, particularly when used as the initialimmunosuppressant.3,4 High trough levels of tacrolimusduring the first month after transplantation have beenshown to be a significant risk factor for the development ofPTDM.5 The aim of this single-center study was to assessthe risk factors for the development of PTDM amongkidney transplant recipients under tacrolimus therapy.
MATERIALS AND METHODS
Tacrolimus-treated renal transplant recipients engrafted in ourcenter between 1994 and 2003 were included in the study if theyhad a first blood level after at least 5 equal doses of tacrolimus andadequate data. We excluded patients with a known history ofglucose metabolism abnormalities. Among the 73 included pa-tients, tacrolimus trough concentrations were measured usingmicroparticle enzyme immunoassay (MEIA). The data set also
From the Services of Nephrology (E.R., G.F.-F., J.C.R., C.P.,R.P., J.G.C., C.G.-A., S.S.C., A.L.M.F., M.A.) and Clinical Phar-macology (M.A.C., B.S.), Hospital Valdecilla, University of Cant-abria, Santander, Spain.
Address reprint requests to Dr E. Rodrigo, Service of Nephrol-ogy, Hospital Valdecilla, Avda. Valdecilla s/n 39008, Santander,Spain. E-mail: [email protected]
© 2005 by Elsevier Inc. All rights reserved. 0041-1345/05/$–see front matter360 Park Avenue South, New York, NY 10010-1710 doi:10.1016/j.transproceed.2005.09.196
Transplantation Proceedings, 37, 3819–3820 (2005) 3819

An analysis of tacrolimus-related complications inthe first 30 days after liver transplantationLucas Souto Nacif, Andre Ibrahim David, Rafael Soares Pinheiro, Marcio Augusto Diniz,
Wellington Andraus, Ruy Jorge Cruz Junior, Luiz A. Carneiro D9Albuquerque
Faculdade de Medicina da Universidade de Sao Paulo, Department of Gastroenterology, Liver and Gastrointestinal Transplant Division, (LIM 37), Sao
Paulo/SP, Brazil.
OBJECTIVES: Orthotopic liver transplantation has improved survival in patients with end-stage liver disease;however, therapeutic strategies that achieve ideal immunosuppression and avoid early complications are lacking.To correlate the dose and level of Tacrolimus with early complications, e.g., rejection, infection and renalimpairment, after liver transplantation. From November 2011 to May 2013, 44 adult liver transplant recipientswere studied in this retrospective comparative study.
RESULTS: The most frequent indication for liver transplantation was hepatitis C cirrhosis (47.7%), with a higherprevalence observed in male patients (68.18%). The ages of the subjects ranged from 19-71 and the median agewas 55.5 years. The mean length of the hospital stay was 16.1¡9.32 days and the mean Model for End-stage LiverDisease score was 26.18¡4.28. There were five cases of acute cellular rejection (11.37%) and 16 cases of infection(36.37%). The blood samples that were collected and analyzed over time showed a significant correlationbetween the Tacrolimus blood level and the deterioration of glomerular filtration rate and serum creatinine(p,0.05). Patients with infections had a higher serum level of Tacrolimus (p = 0.012). The dose and presence ofrejection were significantly different (p = 0.048) and the mean glomerular filtration rate was impaired in patientswho underwent rejection compared with patients who did not undergo rejection (p = 0.0084).
CONCLUSION: Blood Tacrolimus levels greater than 10 ng/ml were correlated with impaired renal function. Dosesgreater than 0.15 mg/kg/day were associated with the prevention of acute cellular rejection but predisposedpatients to infectious disease.
KEYWORDS: Liver Transplantation; Renal Failure; End-Stage Liver Disease; Tacrolimus; Rejection.
Nacif LS, David AI, Pinheiro RS, Diniz MA, Andraus W, Cruz-Junior RJ, et al. An analysis of tacrolimus-related complications in the first 30 days afterliver transplantation. Clinics. 2014;69(11):745-749.
Received for publication on February 25, 2014; First review completed on April 14, 2014; Accepted for publication on August 14, 2014
E-mail: [email protected]
Tel.: 55 11 2661-3323
& INTRODUCTION
Orthotopic liver transplantation (OLT) has markedlyimproved survival in patients with end-stage liver disease,especially due to advances in surgical techniques, anesthesiaand immunosuppressive therapy. Calcineurin inhibitors(CNIs) (1-3) have dramatically improved patient survivalafter OLT; however, nephrotoxicity, renal dysfunction withchronic renal injury and end-stage kidney disease occur in3-20% of recipients taking CNIs post-transplant and theseconditions contribute to the high morbidity and mortalityassociated with this course (2-4). Thus, CNI therapy must beclosely monitored. Furthermore, the development of ther-
apeutic strategies that achieve effective immunosuppressionwhile limiting early complications, such as infection, rejectionor renal failure, remains a real challenge after OLT (5,6).
The purpose of this study was to determine the relation-ship between the dose and blood level of Tacrolimus withearly complications post-OLT.
& MATERIALS AND METHODS
Study designWe analyzed 44 adult OLT recipient patients in the Liver
GI Transplant Division within the Department of Gastroen-terology, University of Sao Paulo School of Medicine duringthe first 30 post-operative days, from November 2011 to May2013. We retrospectively studied their demographic, clinicaland laboratory data. Rejection episodes were biopsied anddefined by the Banff criteria (7). Complications from bacterial,fungi or viral infections at any site were determined. Bloodsamples were collected daily during hospitalization and atleast weekly during the first month after OLT to analyze thecreatinine level and glomerular filtration rate (GFR). GFR wasestimated according to the Cockcroft-Gault equation (8).
Copyright ! 2014 CLINICS – This is an Open Access article distributed underthe terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided theoriginal work is properly cited.
No potential conflict of interest was reported.
DOI: 10.6061/clinics/2014(11)07
CLINICAL SCIENCE
745
Inclusion and exclusion criteriaThe following parameters were excluded from analysis:
living donor recipients, severe acute hepatitis, combinedliver-kidney transplantation, split liver, use of immunosup-pressants other than Tacrolimus and prednisone, very illpatients (MELD.40) and those who died before the 30-dayfollow-up. These patients exhibited multifactorial variablesand no linear use of immunosuppression. Demographicparameters were evaluated in these patients. The mean,standard deviation, median, range, number and percentagewere calculated for each parameter. The graphics wereanalyzed over time and compared with the blood level anddose of Tacrolimus, GFR and serum creatinine.
Immunosuppression regime, diagnostic criteria andgroup definitions
In all cases, transplants were performed via the piggybacktechnique (9). The preservation solutions most commonlyused were ViaspanH and CustodiolH. These immunosup-pressive regimens followed a general protocol, but each wascustomized as necessary. All patients received a steroid (ST)bolus during the anhepatic phase (500 mg), which wasdecreased to 20 mg/day and tapered to a complete stopwithin 3 to 6 months of transplantation. Tacrolimus wasorally administered and maintained in all patients (0.10-0.15 mg/kg/day administered via two daily doses admi-nistered every 12 hours). All patients with acute cellularrejection (n = 5) were included in the rejection group withestablished evidence in laboratory analysis, histologicalfindings (Banff criteria) and the treatment used. Episodesof infection were confirmed in patients (n = 16) by positivecultures from any site and laboratory abnormalities (leuko-cytosis and increased C-reactive protein).
Statistical analysisResults are expressed using descriptive measures (means
¡ standard error) for the following variables: Tacrolimusdose (mg/kg/day), serum level of Tacrolimus (ng/ml) andGFR (ml/min). The Student t-test and Mann-Whitney testwere used to compare quantitative and categorical vari-ables, respectively, among groups. These variables werecompared between groups with and without occurrence ofinfection or between groups with or without rejection byanalysis of variance (ANOVA) with repeated measuresusing a nonparametric statistical program in R (Version
2.15.1). Differences were considered statistically significantwhen p,0.05.
Ethical aspectsThe study was approved by the Ethics Committee of
Human Experimentation.
& RESULTS
Clinical and Demographic Population ProfileWe observed a higher prevalence of male gender (68.18%)
compared with female gender. The mean age of the patientswas 52.43 years old (¡12.33); the median age was 55.5 yearsold and the range was 19-71 years old. The mean weight was75.15 kg (¡18.61); the mean of body max index (BMI) was25.94¡4.58 and the mean length of hospital stay was 16.1¡9.32days. The major cause for transplantation was hepatitis Cvirus-induced cirrhosis (47.7%), followed by alcoholic cirrhosis(13.6%), primary sclerosing cholangitis (6.8%), cryptogeniccirrhosis (6.8%), autoimmune hepatitis (6.8%), hepatitis B viruscirrhosis (6.8%), nonalcoholic fatty liver disease (4.7%) andother (6.8%). The mean MELD score was 26.18¡4.28 (Table 1).
Overall patient characteristicsThe patients were evaluated over time (3, 5, 7, 10 and 15
days post-transplant) and then divided into groups based onthe presence or absence of infection or rejection. The numberand percentage of patients in each group are as follows:infection (n = 16/36.37%), no infection (n = 28/63.63%), rejec-tion (n = 5/11.37%) and no rejection (n = 39/88.64%) (Table 2).We observed that the mean age of patients with rejection waslower than that of the other groups and the weight of thisgroup was higher than that of the other groups. The meanhospital stay was longer in patients with infection than inthose without infection (p = 0.003) and those with rejection(p = 0.043). Patients without early complications (rejection orinfection) had a mean hospital stay of 12 days after OLT. Ahigher MELD score was observed in patients with infection(27.14¡6.05) compared with those without infection.
Comparison groups - early complicationThe mean dose of Tacrolimus was lower on the third day
after transplantation in both groups with early complications(infection and rejection), marking a statistically significantlevel of difference (p,0.05). However, when the blood level
Table 1 - Demographic parameters for all liver transplantation patients.
Parameter Liver Transplantation (n = 44)
Sex (n/%) M = 30 (68.18%)/F = 14 (31.82%)Mean age (years) 52.43 (¡12.33)Median age (years) 55.5 (range, 19-71)Mean hospital stay (days) 16.1¡9.32MELD score 26.18¡4.28Cause of transplantation HCV cirrhosis (47.7%) alcoholic cirrhosis (13.6%) primary sclerosing cholangitis
(6.8%) cryptogenic cirrhosis (6.8%) autoimmune hepatitis (6.8%) hepatitis Bvirus cirrhosis (6.8%) nonalcoholic fatty liver disease (4.7%) other (6.8%)
Mean body max index 25.94¡4.58Acute cellular rejection (ACR) n = 5 (11.37%)ACR without infection n = 3 (6.82%)Infection n = 16 (36.37%)Infection without ACR n = 14 (31.82%)
Abbreviations: ACR: acute cellular rejection, GFR: glomerular filtration rate; Creat: creatinine; Tacrolimus dose (mg/kg/day), serum level of Tacrolimus (ng/ml) and days after transplant (t).
Tacrolimus Complications in Liver TransplantationNacif LS et al.
CLINICS 2014;69(11):745-749
746
• Blood Tacrolimus levels > 10 ng/ml correlated with impaired renal function
• Doses > 0.15 mg/kg/day were associated with the prevention of acute cellular rejection but predisposed patients to infectious disease

Cascorbi, 2018

Chen & Prasad, 2018
Pharmacogenomics and Personalized Medicine 2018:11 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
25
CYP3A5 and tacrolimus in renal transplant
early stop codon that results in a nonfunctional protein. In the seminal study by Kuehl et al,22 all Caucasian and most African American patients with low concentrations of intestinal or hepatic CYP3A5 (<21 pmol/mg protein) were homozygous for CYP3A5 *3. Those with higher CYP3A5 content (between 21 and 204 pmol/mg protein) possessed at least 1 copy of CYP3A5 *1. Carriers of the *1 allele have higher overall CYP3A content by approximately three-fold (p=0.001 for Caucasians, p=0.01 for African Americans). In these patients, CYP3A5 represents at least 50% of the total hepatic CYP3A content.
SNPs usually do not occur independently in a given individual. Rather, one observes linkage disequilibrium, in which two or more SNPs interact because genetic material is passed on to the next generation in blocks of DNA known as haplotypes. Studies show that the CYP3A5 *1 wild-type allele is linked to the CYP3A4 *1B allele. In one study, 67% of Caucasians and 100% of African Americans possessing CYP3A4 *1B also possessed CYP3A5 *1.24 CYP3A4 *1B
affects tacrolimus clearance in the same direction. Individu-als possessing the CYP3A4*1B allele have lower C0 by 35% after adjustment for tacrolimus dose compared to wild-type individuals.25
Effect of CYP3A5 genotype on tacrolimus pharmacokineticsThe wild-type CYP3A5 *1 allele is associated with greater production of functional CYP3A5 enzyme, thus leading to higher drug-metabolizing activity by CYP3A overall. The CYP3A45*1/*1 genotype increases tacrolimus clearance by 2-fold, while the heterozygous CYP3A5*1/*3 genotype results in approximately 1.7-fold greater clearance compared to the CYP3A5*3/*3 population.17,26–27 CYP3A5 *3/*3 has 48% lower oral clearance compared to CYP3A5 express-ers11 (Table 3).
In 2012, Terrazino et al28 published a meta-analysis to estimate the effect of CYP3A5 6986A>G polymorphism on tacrolimus dose-adjusted trough concentration in kidney transplant patients. Nineteen studies involving 2,028 patients were included in the meta-analysis. Overall, patients with the *3/*3 genotype had significantly higher dose-adjusted trough concentrations (weighted mean difference: 63.57 ng/mL per mg/kg, 95% confidence interval [CI]: 50.85–76.30) compared with the combined group of *1/*3 and *1/*1 patients. This effect was maintained when stratified by ethnic group (Caucasian and Asian) and by time since transplant (≤1 month, 3–6 months, 12–24 months). The authors addi-tionally compared the effect of *1/*1 genotype versus *1/*3 genotype in 10 studies. The difference in dose-adjusted trough concentration was smaller at 19.83 ng/mL per mg/kg (95% CI: 13.86–25.80).
Table 1 CYP3A5 alleles
Allele Nucleotide variation Effect on CYP3A5 proteina
*1 Wild type Normal function*2 27289G>T Limited/no data*3 6986T>C Loss of function*4 14665T>C Limited/no data*5 12952A>G Limited/no data*6 14690C>T Loss of function*7 27131_27132insA Loss of function*8 3699G>A Limited/no data*9 19386C>T
6986T>CLimited no data
Notes: aNote that “normal” function is not indicative of the most common phenotype within the general population. In most ethnic groups, absence of functional CYP3A5 is most frequent. Adapted from Birdwell et al.13 For any updates to this table or CPIC guideline see: https://cpicpgx.org/guidelines/guideline-for-tacrolimus-and-cyp3a5/.
Table 2 Frequency of CYPA5 alleles in different ethnic populations
Frequency of CYP3A5 allele
Ethnic population CYP3A5 *1/*1 (%) CYP3A5 *1/*3 (%) CYP3A5 *3/*3 (%)
Caucasian 1 13–17 82–86Black 37–45 40–54 9–15Indian 2.5–11 38–57 32–60Chinese 7.7 44.8 47.4
Notes: Data from Barry and Levine,11 Rojas et al,14 Tang et al,15 Chen et al,16 Boughton et al,17 Niioka et al,18 Chandel et al,19 and Satoh et al.20
Table 3 Key terminology and definitions
Patient profile Allele SNP Effect Tacrolimus trough level
Tacrolimus dose requirement
CYP3A5 expressers *1/*1 rs6986 AA mRNA splices correctly, leading to greater quantity of CYP3A5 enzyme
↓ ↑*1/*3 rs6986 AG ↓ ↑
CYP3A5 nonexpressers
*3/*3 rs6986 GG Incorrect mRNA splicing leading to nonfunctional CYP3A5 protein
↑ ↓
Abbreviation: SNP, single-nucleotide polymorphism.

Zhang et al, 2018(alleles numbered *1–*9) [32]. Kuehl et al. reported that the wild-typeallele for CYP3A5 was CYP3A5*1, with variant alleles (*3, *6, or *7)that may result in truncated mRNA with the loss of expression of thefunctional protein or encode nonfunctional protein [33]. TheCYP3A5*3 allele is the most common polymorphism across all ethnicgroups studied (Table 1). The CYP3A5*6 and CYP3A5*7 variant allelesare rare or absent in Asian or Caucasian populations, but are commonlyfound in African populations [30].
Since 2004, many studies have investigated the relationship be-tween the genotype of CYP3A5 and tacrolimus pharmacokinetics[34–39]. Several studies have found that the CYP3A5*1 allele was as-sociated with a significantly higher tacrolimus clearance (CL) and lowersystemic exposure. The patients that are substantially more likely to beCYP3A5 expressors, such as the African-American cohort, may be athigher risk for both rejection as well as poor clinical outcomes relatedto inadequate immunosuppression [40,41], although these individualshave a high dose requirement for tacrolimus, irrespective of CYP3A5genotype [42]. The prevalence of CYP3A5 polymorphisms has becomean important pharmacotherapeutic dosing consideration.
To evaluate whether adaption of tacrolimus dosing according toCYP3A5 genotype would allow earlier achievement of target bloodconcentrations of tacrolimus in renal transplant recipients, Thervetet al. conducted a randomized controlled trial in a cohort of 280 kidneytransplant patients to compare two dosing strategies: the 0.2 mg/kg/day regimen and the CYP3A5*3 allele-guided dosing, in which CYP3A5expressors received 0.30mg/kg/day, whereas CYP3A5 nonexpressors(CYP3A5*3/*3 genotype) received 0.15mg/kg/day (adapted-dosegroup). All patients were received a potent induction therapy and weresubjected to TDM. The results showed that genotype-guided dosing didincrease the proportion of patients on target and required significantlyfewer dose modifications, a lower number of dose modifications and ashorter delay between tacrolimus introduction and achievement oftarget C0 were observed. However, no difference was found in theclinical end points between the two groups over a 3-month follow-upperiod. As the population studied was at low risk of acute rejection orother clinical events, with less than 5% of patients identifying as black,the demonstration of the association between CYP3A5 genotype andclinical outcome was not achieved. Although higher rates of biopsy-proven acute rejection have not been observed in CYP3A5 expressors,rejection did occur earlier in CYP3A5*1/*3 or *1/*1 group comparedwith non-expressors [43]. When a potent immunosuppressive regimenis used in an immunologically low-risk transplant population, a delay inreaching the target tacrolimus exposure may not significantly influencerejection risk [44]. In contrast to the study by the Thervet group,Shuker et al.’s study based on a prospective, randomized, controlled,parallel group, single-center clinical trial including 240 patients sug-gested that the CYP3A5 genotype-guided tacrolimus starting dose didnot lead to earlier achievement of the target tacrolimus C0 range orsuperior clinical outcome compared with standard, body-weight-baseddosing after kidney transplantation [44]. The discrepancies between thetwo studies may be the initiation time point of tacrolimus treatment(the
night following transplant surgery vs. day 7 after transplantation).Higher between-patient tacrolimus concentrations variability in the fewfirst days and early postoperative changes in gastrointestinal motilityand glucocorticoid dose may have diluted the pharmacogenetic effect[45,46]. Focusing on evaluating the role of CYP3A5, neither of thesestudies accounted for other genetic variants, such as CYP3A4*22,ABCB1, POR*28, and CYP3A4*26, which may explain some of the inter-individual differences in tacrolimus exposure.
4.2. CYP3A4
The newly identified CYP3A4*22 allele is an intronic variant asso-ciated with reduced CYP3A4 mRNA levels and CYP3A4 activity in thehuman liver. It was estimated to be responsible for 7% of the variabilityin mRNA expression [47]. Elens et al. were the first to describe that theCYP3A4*22 polymorphism downregulates tacrolimus metabolism andtherefore increases the risk of supratherapeutic tacrolimus concentra-tions soon after transplantation [48,49]. The fast metabolizers(CYP3A5*1/ POR*28T carriers) require two-to-three-fold higher ta-crolimus doses compared with slow metabolizers (CYP3A5*3/*3/CYP3A4*22 carriers) and the combined genotype is the strongest singledeterminant of tacrolimus dose requirement throughout the first year.Based on their research, Elens et al. suggested that it might be moreoptimal to establish multiple genotype-based algorithms that considerthe status of both CYP3A5*3 and CYP3A4*22 alleles. However, nosignificant differences for Tacrolimus normalized values among theCYP3A4*22 genotypes was observed in other researchers’ study [50].Therefore, the exact value of CYP3A4*22 in tacrolimus dose require-ment predicting is uncertain and deeper investigations are needed.CYP3A4*26 was recently identified: a complete failure of CYP3A en-zyme activity was reported in a patient homozygous for CYP3A5*3 andCYP3A4*26 treated with standard tacrolimus dosing [51]. This ob-served pattern might have severe consequences for tacrolimus intake.CYP3A4*1B (rs2740574) allele was reported to have a 35% lower Tacdose-adjusted C0 concentration compared to individuals having theCYP3A4 wild-type allele, but its influence on tacrolimus dose require-ment remains in debate as this SNP is in linkage disequilibrium with theCYP3A5*1 allele [52,53].
4.3. ABC family
ABC transporters, in particular P-gp, are widely distributed andexpressed in the intestinal epithelium, liver cells, and the proximaltubule of the kidney [54]. They may influence the absorption, excre-tion, and distribution of tacrolimus. The relationship between ABCB1polymorphisms and tacrolimus pharmacokinetisc has been extensivelyinvestigated, whereas the results are still controversial [55]. Kurzawskiet al. found no significant difference between the differentABCB1(rs1045642) genotypes [38,56], whlie other investigators foundthat patients homozygous for allele C (rs1045642) would require higherdaily doses of tacrolimus to achieve target range when compared withthe T allele carriers [57]. There are other considerations suggesting thatdonor CC genotype at C3435T (rs1045642) within ABCB1 was asso-ciated with an increased risk for long-term graft failure compared withnon-CC genotype [58], and ABCB1 allelic arrangement is a strongerregulator of P-gp activity than single polymorphisms. Banduret al.suggested that ABCB1 haplotypes modify the risk of acute rejection[59]. The ABCB1 3435C > T (rs1045642), 1236C > T (rs1128503)and 2677G > T/A (rs2032582) SNPs are in linkage disequilibrium. Astudy involving 832 Czech renal transplant recipients demonstratedthat the 1236C-2677G-3435T haplotype was associated with a 1.4-foldincreased risk of acute rejection compared with the homozygous variant((T-T-T)) or wild-type ((C-G-C)) haplotypes [59]. The effect that thesepolymorphisms exerted is small but combined, and is additive to theeffects of the CYP3A5 6986A > G SNP [60].
ABCC2 gene encoding multidrug resistance associated protein 2
Table 1Frequencies of CYP3A5 alleles in major race/ethnic groups [6].
Ethnicity Frequencies of Alleles
*1 *3 *6 *7
African 0.558 0.298 0.172 0.077African American 0.605 0.316 0.111 0.120South East African 0.744 0.157 0.194 0.142Asian 0.258 0.742 0.001 0.000Southwest Asian 0.342 0.659 0.000 NACaucasian 0.078 0.921 0.001 0.000Middle Eastern 0.105 0.881 0.019 0.002Latin American 0.202 0.765 0.037 0.025
X. Zhang et al. %LRPHGLFLQH��3KDUPDFRWKHUDS\���������������²���
���
Pharmacogenomics and Personalized Medicine 2018:11 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
25
CYP3A5 and tacrolimus in renal transplant
early stop codon that results in a nonfunctional protein. In the seminal study by Kuehl et al,22 all Caucasian and most African American patients with low concentrations of intestinal or hepatic CYP3A5 (<21 pmol/mg protein) were homozygous for CYP3A5 *3. Those with higher CYP3A5 content (between 21 and 204 pmol/mg protein) possessed at least 1 copy of CYP3A5 *1. Carriers of the *1 allele have higher overall CYP3A content by approximately three-fold (p=0.001 for Caucasians, p=0.01 for African Americans). In these patients, CYP3A5 represents at least 50% of the total hepatic CYP3A content.
SNPs usually do not occur independently in a given individual. Rather, one observes linkage disequilibrium, in which two or more SNPs interact because genetic material is passed on to the next generation in blocks of DNA known as haplotypes. Studies show that the CYP3A5 *1 wild-type allele is linked to the CYP3A4 *1B allele. In one study, 67% of Caucasians and 100% of African Americans possessing CYP3A4 *1B also possessed CYP3A5 *1.24 CYP3A4 *1B
affects tacrolimus clearance in the same direction. Individu-als possessing the CYP3A4*1B allele have lower C0 by 35% after adjustment for tacrolimus dose compared to wild-type individuals.25
Effect of CYP3A5 genotype on tacrolimus pharmacokineticsThe wild-type CYP3A5 *1 allele is associated with greater production of functional CYP3A5 enzyme, thus leading to higher drug-metabolizing activity by CYP3A overall. The CYP3A45*1/*1 genotype increases tacrolimus clearance by 2-fold, while the heterozygous CYP3A5*1/*3 genotype results in approximately 1.7-fold greater clearance compared to the CYP3A5*3/*3 population.17,26–27 CYP3A5 *3/*3 has 48% lower oral clearance compared to CYP3A5 express-ers11 (Table 3).
In 2012, Terrazino et al28 published a meta-analysis to estimate the effect of CYP3A5 6986A>G polymorphism on tacrolimus dose-adjusted trough concentration in kidney transplant patients. Nineteen studies involving 2,028 patients were included in the meta-analysis. Overall, patients with the *3/*3 genotype had significantly higher dose-adjusted trough concentrations (weighted mean difference: 63.57 ng/mL per mg/kg, 95% confidence interval [CI]: 50.85–76.30) compared with the combined group of *1/*3 and *1/*1 patients. This effect was maintained when stratified by ethnic group (Caucasian and Asian) and by time since transplant (≤1 month, 3–6 months, 12–24 months). The authors addi-tionally compared the effect of *1/*1 genotype versus *1/*3 genotype in 10 studies. The difference in dose-adjusted trough concentration was smaller at 19.83 ng/mL per mg/kg (95% CI: 13.86–25.80).
Table 1 CYP3A5 alleles
Allele Nucleotide variation Effect on CYP3A5 proteina
*1 Wild type Normal function*2 27289G>T Limited/no data*3 6986T>C Loss of function*4 14665T>C Limited/no data*5 12952A>G Limited/no data*6 14690C>T Loss of function*7 27131_27132insA Loss of function*8 3699G>A Limited/no data*9 19386C>T
6986T>CLimited no data
Notes: aNote that “normal” function is not indicative of the most common phenotype within the general population. In most ethnic groups, absence of functional CYP3A5 is most frequent. Adapted from Birdwell et al.13 For any updates to this table or CPIC guideline see: https://cpicpgx.org/guidelines/guideline-for-tacrolimus-and-cyp3a5/.
Table 2 Frequency of CYPA5 alleles in different ethnic populations
Frequency of CYP3A5 allele
Ethnic population CYP3A5 *1/*1 (%) CYP3A5 *1/*3 (%) CYP3A5 *3/*3 (%)
Caucasian 1 13–17 82–86Black 37–45 40–54 9–15Indian 2.5–11 38–57 32–60Chinese 7.7 44.8 47.4
Notes: Data from Barry and Levine,11 Rojas et al,14 Tang et al,15 Chen et al,16 Boughton et al,17 Niioka et al,18 Chandel et al,19 and Satoh et al.20
Table 3 Key terminology and definitions
Patient profile Allele SNP Effect Tacrolimus trough level
Tacrolimus dose requirement
CYP3A5 expressers *1/*1 rs6986 AA mRNA splices correctly, leading to greater quantity of CYP3A5 enzyme
↓ ↑*1/*3 rs6986 AG ↓ ↑
CYP3A5 nonexpressers
*3/*3 rs6986 GG Incorrect mRNA splicing leading to nonfunctional CYP3A5 protein
↑ ↓
Abbreviation: SNP, single-nucleotide polymorphism.
Chen & Prasad, 2018

1019Pharmacogenomics (2016) 17(9), 1019–1027 ISSN 1462-2416
part of
PharmacogenomicsResearch Article
10.2217/pgs-2016-0005 © 2016 Future Medicine Ltd
Aim: The once daily tacrolimus formulation (Tac-OD) has been associated with better patient adherence and low variability in exposure. Patients carrying the CYP3A5*1 allele show accelerated clearance of Tac. Authors prospectively evaluate a simplified strategy for Tac-OD administration. Patients & methods: After grafting, 151 patients were divided into four groups and received a daily dose calculated according to CYP3A5 genotypes and unchanged for the first three days: CYP3A5*3/*3: 0.20 mg/kg/day, CYP3A5*3/*3: 0.25 mg/kg/day, CYP3A5*1/*3: 0.30 mg/kg/day and CYP3A5*1/*1: 0.35 mg/kg/day. The dose was adaptated on day 4 and remained unchanged a further three days and so on. Results: On day 3, median Cmin fell within the therapeutic range in all study groups. CYP3A5 expressors require significantly higher Tac-OD throughout the follow-up period to achieve a comparable Cmin. Conclusion: This simplified strategy does not hamper treatment efficacy.
First draft submitted: 6 January 2016; Accepted for publication: 26 February 2016; Published online: 8 June 2016
Keywords:�EXTENDED�RELEASE�TACROLIMUS�s�IMMUNOSUPPRESSION�s�KIDNEY�TRANSPLANT�s��PHARMACOGENOMICS
Immunosuppression is the cornerstone of treatment to avoid rejection and sustain renal function after kidney transplanta-tion. Patients are expected to adhere to a lifelong therapeutic regimen designed to preserve the graft in the long term. Thus, the primary goal after transplantation is to individualize patient therapy to maintain a good balance between efficacy and toxicity. However, predicting the starting dose of immuno suppressant and adjusting it over time remains challenging. The once daily formulation of the immuno suppressive agent tacro limus (Tac-OD; Advagraf®, Astellas Pharma Europe, Ltd, Staines, UK) has been associated with enhanced adher-ence after kidney transplantation [1] and lower intrapatient variability in drug expo-sure [2]. Conversion studies have shown Tac-OD to have a similar safety profile to the widely established twice daily Tac adminis-
tration [3]. According to de novo studies on Tac-OD, excellent survival rates and com-parable safety profiles have been achieved with both formulations [4,5].
Genetic testing for CYP3A biotrans-formation enzymes is currently thought to be a potential benefit for dose individualiza-tion and target Tac concentrations predic-tion [6]. Indeed, individuals expressing the CYP3A5 enzyme (CYP3A5*1 allele carriers) need higher Tac doses to reach the same Tac trough concentration values (Cmin ) [7–9]. The recommended Tac-OD dose for de novo use after kidney transplantation was set by the manufacturer at 0.20 mg/kg/day, starting within the first 24 h of transplantation [10], with dose adjustment performed according to daily Tac Cmin levels.
To the best of our knowledge, no other guidelines have been proposed for initial Tac-OD administration.
Pharmacogenetic-based strategy using de novo tacrolimus once daily after kidney transplantation: prospective pilot study
Martine De Meyer1, Vincent Haufroid2,3, Nada Kanaan4, Tom Darius1, Antoine Buemi1, Luc De Pauw1, Djamila Chaïb Eddour1, Pierre Wallemacq2 & Michel Mourad*,1
1$EPARTMENT�OF�3URGERY��3URGERY���!BDOMINAL�4RANSPLANTATION�$IVISION��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM 2$EPARTMENT�OF�#LINICAL�#HEMISTRY��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM 3 ,OUVAIN�#ENTRE�FOR�4OXICOLOGY���!PPLIED�0HARMACOLOGY��,4!0��)NSTITUT�DE�2ECHERCHE�%XPÏRIMENTALE�ET�#LINIQUE��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��"RUSSELS��"ELGIUM 4$EPARTMENT�OF�.EPHROLOGY��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM !UTHOR�FOR�CORRESPONDENCE�� 4EL������������������� &AX������������������ MICHEL�MOURAD UCLOUVAIN�BE
For reprint orders, please contact: [email protected]
1019Pharmacogenomics (2016) 17(9), 1019–1027 ISSN 1462-2416
part of
PharmacogenomicsResearch Article
10.2217/pgs-2016-0005 © 2016 Future Medicine Ltd
Aim: The once daily tacrolimus formulation (Tac-OD) has been associated with better patient adherence and low variability in exposure. Patients carrying the CYP3A5*1 allele show accelerated clearance of Tac. Authors prospectively evaluate a simplified strategy for Tac-OD administration. Patients & methods: After grafting, 151 patients were divided into four groups and received a daily dose calculated according to CYP3A5 genotypes and unchanged for the first three days: CYP3A5*3/*3: 0.20 mg/kg/day, CYP3A5*3/*3: 0.25 mg/kg/day, CYP3A5*1/*3: 0.30 mg/kg/day and CYP3A5*1/*1: 0.35 mg/kg/day. The dose was adaptated on day 4 and remained unchanged a further three days and so on. Results: On day 3, median Cmin fell within the therapeutic range in all study groups. CYP3A5 expressors require significantly higher Tac-OD throughout the follow-up period to achieve a comparable Cmin. Conclusion: This simplified strategy does not hamper treatment efficacy.
First draft submitted: 6 January 2016; Accepted for publication: 26 February 2016; Published online: 8 June 2016
Keywords:�EXTENDED�RELEASE�TACROLIMUS�s�IMMUNOSUPPRESSION�s�KIDNEY�TRANSPLANT�s��PHARMACOGENOMICS
Immunosuppression is the cornerstone of treatment to avoid rejection and sustain renal function after kidney transplanta-tion. Patients are expected to adhere to a lifelong therapeutic regimen designed to preserve the graft in the long term. Thus, the primary goal after transplantation is to individualize patient therapy to maintain a good balance between efficacy and toxicity. However, predicting the starting dose of immuno suppressant and adjusting it over time remains challenging. The once daily formulation of the immuno suppressive agent tacro limus (Tac-OD; Advagraf®, Astellas Pharma Europe, Ltd, Staines, UK) has been associated with enhanced adher-ence after kidney transplantation [1] and lower intrapatient variability in drug expo-sure [2]. Conversion studies have shown Tac-OD to have a similar safety profile to the widely established twice daily Tac adminis-
tration [3]. According to de novo studies on Tac-OD, excellent survival rates and com-parable safety profiles have been achieved with both formulations [4,5].
Genetic testing for CYP3A biotrans-formation enzymes is currently thought to be a potential benefit for dose individualiza-tion and target Tac concentrations predic-tion [6]. Indeed, individuals expressing the CYP3A5 enzyme (CYP3A5*1 allele carriers) need higher Tac doses to reach the same Tac trough concentration values (Cmin ) [7–9]. The recommended Tac-OD dose for de novo use after kidney transplantation was set by the manufacturer at 0.20 mg/kg/day, starting within the first 24 h of transplantation [10], with dose adjustment performed according to daily Tac Cmin levels.
To the best of our knowledge, no other guidelines have been proposed for initial Tac-OD administration.
Pharmacogenetic-based strategy using de novo tacrolimus once daily after kidney transplantation: prospective pilot study
Martine De Meyer1, Vincent Haufroid2,3, Nada Kanaan4, Tom Darius1, Antoine Buemi1, Luc De Pauw1, Djamila Chaïb Eddour1, Pierre Wallemacq2 & Michel Mourad*,1
1$EPARTMENT�OF�3URGERY��3URGERY���!BDOMINAL�4RANSPLANTATION�$IVISION��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM 2$EPARTMENT�OF�#LINICAL�#HEMISTRY��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM 3 ,OUVAIN�#ENTRE�FOR�4OXICOLOGY���!PPLIED�0HARMACOLOGY��,4!0��)NSTITUT�DE�2ECHERCHE�%XPÏRIMENTALE�ET�#LINIQUE��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��"RUSSELS��"ELGIUM 4$EPARTMENT�OF�.EPHROLOGY��5NIVERSITÏ�CATHOLIQUE�DE�,OUVAIN��#LINIQUES�UNIVERSITAIRES�3AINT ,UC��"RUSSELS��"ELGIUM !UTHOR�FOR�CORRESPONDENCE�� 4EL������������������� &AX������������������ MICHEL�MOURAD UCLOUVAIN�BE
For reprint orders, please contact: [email protected]

www.futuremedicine.com 1021future science group
Pharmacogenetic-based strategy using de novo tacrolimus once daily Research Article
tion rate [GFR; ml/min] estimated by Modification of diet in renal disease [MDRD]) was evaluated daily during the first week after transplantation and twice during the second postoperative week. Delayed graft function is defined as the need for at least one dialysis session during the first week after transplantation. After hospital discharge, they were followed as outpatients. Serum creatinine, GFR, Tac Cmin and proteinuria were determined at 6 and 12 months. Graft biopsy was per-formed in case of renal function deterioration. Fasting glycemia and glycated hemoglobin levels were evalu-ated before grafting and then 6 and 12 months after transplantation.
Statistical analysisStatistical analysis was carried out using the JMP®Pro (version 12.1.0, SAS Institute, NC, USA). Groups were compared using nonparametric tests. To compare two groups, we applied the Mann–Whitney U test, and to compare several groups, the Kruskal–Wallis test. When appropriate, multiple comparisons testing (post-hoc analysis) was performed on all possible pairwise using Steel–Dwass All Pairs test. P-values less than 0.05 were considered statistically significant. All values are expressed as median and range, unless otherwise stated.
ResultsPatientsOut of 170 subjects eligible for this study, 151 were considered (89%). Nineteen patients were excluded for different reasons: eight were undergoing immu-nosuppression for a previous graft at the time of transplantation, six had a history of malignancy for whom immuno suppressive regimen has to be changed 3 months after transplantation, five lost their graft within the first month (two nonprimary function, two early graft thrombosis, one recurrence of oxalate deposition). Ninety-six percent of the study population were of Caucasian origin. Age, gender, origin of the graft, primary kidney disease, rank of the pro cedure and the CYP3A5 genotype are summarized in Table 1. Mean follow-up was 21 ± 9 months (6–38). The geno-type frequencies were not significantly different from that predicted by the Hardy–Weinberg equation.
Tacrolimus oral doses & blood concentrations according to study groupsDuring the first week after transplantation, all patients underwent Tac Cmin determination twice, on days 3 and 6, followed by dose adjustment on days 4 and 7, respectively. Tac-OD doses (mg/kg b.w./day) are
Table 1. Population characteristics.
Population Expressors Non-expressors
Total
CYP3A5 *1/*1 *1/*3 *3/*3 –
n 7 16 128 151
Recipients Mean age ± SD (y) 48 ± 14* 45 ± 12* 50 ± 13* 49 ± 12
Sex (F/M) 4/3 9/7 43/85 56/95
Donors Deceased 5 10 101 116 (77%)
Living 2 6 27 35 (23%)
Mismatch Median 3 3 3 3
Range 2–5 0–6 0-6 0-6
Transplantation rank First 6 16 123 145
Second 1 0 5 6
Primary kidney disease Glomerulonephritis 1 5 20 26
Interstitial nephritis 0 3 17 20
APKD 0 2 37 39
Hereditary disease 1 1 12 14
Systemic disease 0 2 12 14
Vascular disease 1 0 6 7
Diabetes 0 1 5 6
Unknown 4 2 19 25
*P�������!0+$��!UTOSOMAL�DOMINANT�POLYCYSTIC�KIDNEY�DISEASE��&��&EMALE��-��-ALE��3$��3TANDARD�DEVIATION�
Byun et al, 2016

1020 Pharmacogenomics (2016) 17(9)
Figure 1. Scheme of the study.
CYP3A5
CYP3A5*3/*3 CYP3A5*1/
Group 1CYP3A5*3/*30.20 mg/kg/d
Group 2CYP3A5*3/*30.25 mg/kg/d
Group 3CYP3A5*1/*30.30 mg/kg/d
Group 4CYP3A5*1/*10.35 mg/kg/d
future science group
Research Article De Meyer, Haufroid, Kanaan et al.
We therefore designed this study to assess the feasi-bility and safety of a simplified new strategy for admin-istration of the first Tac-OD dose, individualized according to CYP3A5 polymorphism and less frequent trough level determination.
Patients & methods From January 2011 to October 2013, all single renal transplant recipients aged from 18 to 70 years, receiv-ing a first or second kidney transplant from a living or deceased donor, were considered for this study. Patients requiring plasma exchange because of a high immuno-logical risk were excluded from the analysis as well as patients treated with drugs potentially interacting with tacrolimus (e.g., anti-epileptic, anti-arrhythmic, antibiotics).
Study design & immunosuppressive therapyA triple-drug-based immunosuppressive regimen com-bining Tac-OD (Advagraf®, Astellas Pharma Europe, Ltd), mycophenolate mofetil (Cellcept®, F Hoffmann-La Roche SA, Basel, Switzerland) at a fixed low dose (500 mg twice a day) and methylprednisolone (tapered to 4 mg by 6 weeks) was administered to all patients. Twenty milligrams of an anti-CD25 monoclonal anti-body (Basiliximab®, Novartis Pharmaceuticals Corpo-ration, Basel, Switzerland ) was given on days 1 and 5 to recipients of living donor kidneys as induction therapy.
A simplified new strategy for Tac-OD administra-tion was followed in all cases, with all patients receiv-ing a fixed pretransplant dose of 0.10 mg/kg admin-istered at any time within 6 h before reperfusion. An unchanged daily dose of Tac was then administered at 8 a.m. during the first 3 days after transplantation. The first Tac Cmin was determined on the third day after transplantation, and the first dose adjustment made on day 4. This dose remained unchanged for a further three days and so on until the patient was dis-charged from hospital. The initial unchanged 3-day daily dose was calculated according to the recipient’s CYP3A5 genotype (Figure 1). CYP3A5 nonexpressors (CYP3A5*3/*3) were given either 0.20 mg/kg/day (group 1) or 0.25 mg/kg/day (group 2). CYP3A5
expressors bearing only one wild-type CYP3A5*1 allele received 0.30 mg/kg/day (CYP3A5*1/*3, group 3), while those homozygous for the wild-type allele (CYP3A5*1/*1, group 4) received 0.35 mg/kg/day. The target therapeutic window for Cmin was 10–15 ng/ml until day 21, 8–12 ng/ml from day 22 to day 90 and 5–8 ng/ml thereafter.
CYP3A5 nonexpressor patients were randomized into group 1 and group 2 on a 1/1 basis randomization method.
The local ethics committee approved the proto-col and informed consent was obtained from each recipient.
Tacrolimus concentration measurement & genetic analysisTacrolimus blood concentrations were obtained rou-tinely by liquid chromatography-tandem mass spec-trometry (LC-MS/MS) using the Agilent HPLC 1290 Infinity system, coupled to the 6460 Triple Quadru-pole instrument. Calibrators and quality controls were from Recipe®, Germany. Briefly, 100 Pl EDTA whole blood was pretreated and vortexed with 100 Pl zinc sulfate 0.1 M, and 250 Pl internal standard (ascomy-cin) in methanol. Samples were sonicated for 5 min, before 10 min of centrifugation at 11,000 rpm. Forty microliters of the supernatant was injected into the system. The precolumn used was the 10 × 4 mm Mercury Phenomenex, and the analytical column the 4.6 × 50 mm Agilent Zorbax Eclipse XDB C18, maintained at 60°C. The mobile phase of pump 1 contained a mixture of H2O/methanol (40/60%), and pump 2 2 mM NH4+ acetate, and aqueous 0.5% for-mic acid/methanol (5/95%). Tac retention time was 1.59 min. The method was fully validated in terms of analytical performance (LOQ: 0.5 ng/ml; imprecision <5%) and ion suppression effects. Our laboratory par-ticipates to the Tac International Proficiency Testing Scheme (ASI, London, UK).
DNA was extracted from peripheral blood leuko-cytes using a blood DNA kit QI Asymphony® (Qia-gen, Hilden, Germany) in accordance with standard protocols. Genotyping of the CYP3A5*3 allele was performed using TaqMan Assay reagents for allelic dis-crimination with a Light Cycler® 480 Instrument II (Roche, Switzerland) thermal cycler. This genotyping test is ISO15189 certified. Genotypes were determined before transplantation, once patients were considered for the waiting list for grafting.
Follow-upAll patients were followed up according to standard care norms used in our transplant unit. Renal func-tion (serum creatinine [mg/dl] and glomerular filtra-
Byun et al, 2016

www.futuremedicine.com 1023future science group
Pharmacogenetic-based strategy using de novo tacrolimus once daily Research Article
the ratio between infratherapeutic, therapeutic and supratherapeutic levels did not show any significant difference between the two groups (Chi-square test). Similar results were obtained on day 6 (Figure 2). The same analysis is also done for groups 3 and 4. The low number of patients in these two last groups does not allow an appropriate statistical analysis.
OutcomeDelayed graft function was observed in 17 patients (11.25%). Nine patients (7 CYP3A5 nonexpressors and 2 expressors) presented with ten biopsy-proven acute rejection episodes within the first year of trans-plantation. In five patients, acute rejection occurred within the first 2 weeks of grafting and was not asso-ciated with infratherapeutic Tac Cmin values. In one homozygous CYP3A5 expressor, acute cellular rejec-tion occurred 3 weeks after transplantation and was concomitant with an infratherapeutic Tac Cmin level despite a higher Tac-OD oral dose. Acute cellular rejec-tion episodes were treated by polyclonal antithymocyte serum in seven cases (Banff IIA in 6 cases and Banff IA in 1), and by corticosteroid pulses in three cases (Banff borderline).
In the study population, 11 patients (7.2%) pre-sented with diabetes mellitus at the time of trans-plantation. Out of the remaining 117 patients who achieved 1-year follow-up, eight nonexpressors (6.8%) developed post-transplant diabetes.
Renal function remained stable and comparable between study groups throughout the follow-up period (Table 5).
No mortality was observed during follow-up. Two grafts were lost due to acute rejection because of nonadherence and chronic nephropathy related to malignant disease therapy, respectively.
DiscussionThe results of this pilot study demonstrate that the reported simplified strategy for administration of Tac-OD is both feasible and efficient. It is essentially based on the once daily Tac administration, which has proved to be superior to the twice daily regimen in terms of adherence [1]. A standard first pretransplant dose was given to all patients, as previously suggested by phar-macokinetic studies on de novo use [11]. Indeed, despite a similar correlation between AUC0–24 and Cmin with both formulations, pretransplant administration helps to reduce the difference in exposure between Tac-OD and twice daily Tac formulations [12].
This new strategy is also based on pretransplant genotyping for CYP3A5 biotransformation enzymes. Whatever the formulation, Tac is characterized by a narrow therapeutic index and interindividual vari-ability in its bioavailability. Factors affecting Tac vari-ability include patient age, ethnicity, albumin, hema-tocrit, liver function, gastrointestinal motility, food intake, drug interactions and genetic polymorphisms in biotransformation enzymes and transporters [13]. During this last decade, numerous studies have evi-denced the impact of CYP3A5 genetic polymorphism on Tac oral clearance. Consequently, CYP3A5*1 car-riers have higher dose requirements than CYP3A5 non expressors [14–16]. On the basis of genetic test-
Table 4. Tacrolimus doses-adjusted blood concentrations according to study groups.
Patient groups
Dose-adjusted Tac Cmin (ng.ml-1/mg/kg b.w.)
Day 3 Day 6 Day 14 Month 1 Month 3 Month 6 Month 12
Group 1 72.6 (29.1–162.3)†, n = 66
70.0 (24.8–161.5)†, n = 66
65.8 (23.5–212.8)†, n = 66
85.1 (21.2–293.8)†, n = 64
97.3 (29.2–372.3)†, n = 66
110.7 (26.8–327.4)†, n = 64
122.6 (19.5–270.0)†, n = 50
Group 2 65.5 (23.8–124.5)†, n = 62
65.9 (21.6–312.0)†, n = 62
58.2 (21.2–285.6)†, n = 61
67.9 (18.1–214.1)†, n = 61
88.0 (25.2–263.5)†, n = 62
97.1 (21.3–292.4)†, n = 62
103.7 (33.3–360.8)†, n = 60
Group 3 45.6 (15.6–95.1)‡, n = 16
37.3 (10.8–83.1)‡, n = 15
34.3 (11.7–90.0)‡, n = 15
38.4 (14.9–118.4)‡, n = 16
43.8 (13.5–70.0)‡, n = 16
38.0 (17.8–118.8)‡, n = 16
38.1 (21.3–103.7)‡, n = 14
Group 4 37.7 (23.9–51.8)‡, n = 7
22.3 (12.8–36.7)‡, n = 7
21.3 (17.0–34.5)‡, n = 7
27.8 (20.9–33.3)‡, n = 7
30.0 (18.1–46.3)‡, n = 7
25.1 (20.6–37.0)‡, n = 7
32.9 (13.7–40.9)‡, n = 6
Kruskal–Wallis test
p < 0.001 p < 0.001 p < 0.001 p < 0.001 p < 0.001 p < 0.001 p < 0.001
6ALUES�ARE�EXPRESSED�AS�MEDIAN��RANGE�;+RUSKALn7ALLIS�TEST=�o�p6ALUES�WITH�THE�SAME�SUPERSCRIPT�LETTER�DO�NOT�DIFFER�SIGNIlCANTLY�FROM�EACH�OTHER��ACCORDING�TO post-hoc�ANALYSIS�
Byun et al, 2016

1024 Pharmacogenomics (2016) 17(9)
Figure 2. Distribution of Tac levels on day 3 and 6 into therapeutic, infratherapeutic or supratherapeutic rates according to the differents groups. *Not significant, Chi-square test.
Proportion (%) of patients in therapeutic range
Day 3Day 6
*
*
0
10
20
30
40
50
60
Proportion (%) of patients in infratherapeutic range
Day 3Day 6
*
*
0
10
20
30
40
50
60
Proportion (%) of patients in supratherapeutic range
Group 1 Group 2 Group 3 Group 4
Group 1 Group 2 Group 3 Group 4
Group 1
Pat
ient
s (%
)P
atie
nts
(%)
Pat
ient
s (%
)
Group 2 Group 3 Group 4
Day 3Day 6
**
0
10
20
30
40
50
60
future science group
Research Article De Meyer, Haufroid, Kanaan et al.
ing before transplantation looking to optimize ini-tial twice daily Tac formulation dosing in a previ-ous study, we proposed a reduction in the starting Tac dose to 0.075 mg/kg in CYP3A5 nonexpressors and an increase to 0.150 mg/kg in expressors [7]. As a result, target Cmin levels were more rapidly reached with fewer dose adjustments than by following the manufacturer’s recommended dose of 0.10 mg/kg [17].
However, no impact was observed on graft rejection or survival [17].
The expression of CYP3A enzymes is not con-stant over the length of the small intestine and this may have a differential effect on the exposure to the two formulations. However, despite a differential impact of the CYP3A5 polymorphism on Cmin values, CYP3A5*3/*3 patients required significantly lower
1024 Pharmacogenomics (2016) 17(9)
Figure 2. Distribution of Tac levels on day 3 and 6 into therapeutic, infratherapeutic or supratherapeutic rates according to the differents groups. *Not significant, Chi-square test.
Proportion (%) of patients in therapeutic range
Day 3Day 6
*
*
0
10
20
30
40
50
60
Proportion (%) of patients in infratherapeutic range
Day 3Day 6
*
*
0
10
20
30
40
50
60
Proportion (%) of patients in supratherapeutic range
Group 1 Group 2 Group 3 Group 4
Group 1 Group 2 Group 3 Group 4
Group 1
Pat
ient
s (%
)P
atie
nts
(%)
Pat
ient
s (%
)
Group 2 Group 3 Group 4
Day 3Day 6
**
0
10
20
30
40
50
60
future science group
Research Article De Meyer, Haufroid, Kanaan et al.
ing before transplantation looking to optimize ini-tial twice daily Tac formulation dosing in a previ-ous study, we proposed a reduction in the starting Tac dose to 0.075 mg/kg in CYP3A5 nonexpressors and an increase to 0.150 mg/kg in expressors [7]. As a result, target Cmin levels were more rapidly reached with fewer dose adjustments than by following the manufacturer’s recommended dose of 0.10 mg/kg [17].
However, no impact was observed on graft rejection or survival [17].
The expression of CYP3A enzymes is not con-stant over the length of the small intestine and this may have a differential effect on the exposure to the two formulations. However, despite a differential impact of the CYP3A5 polymorphism on Cmin values, CYP3A5*3/*3 patients required significantly lower
Byun et al, 2016

Clinical Transplantation. 2018;32:e13162. clinicaltransplantation.com | 1 of 9https://doi.org/10.1111/ctr.13162
© 2017 John Wiley & Sons A/S.
Published by John Wiley & Sons Ltd
Accepted: 15 November 2017
DOI: 10.1111/ctr.13162
O R I G I N A L A R T I C L E
Impact of CYP3A5 genomic variances on clinical outcomes among African American kidney transplant recipients
Tomefa E. Asempa1 | Lorita M. Rebellato2 | Suzanne Hudson3 | Kimberly Briley2 | Angela Q. Maldonado4
1Department of Pharmacy, Vidant Medical
Center, Greenville, NC, USA
2Department of Pathology & Laboratory
Medicine, The Brody School of Medicine at
East Carolina University, Greenville, NC, USA
3Department of Biostatistics, East Carolina
University, Greenville, NC, USA
4Department of Surgery, Vidant Medical
Center, Greenville, NC, USA
CorrespondenceAngela Q. Maldonado, PharmD, CPP, BCPS,
FAST, Clinical Pharmacy Specialist (Transplant
Services), Vidant Medical Center, Greenville,
NC, USA.
Email: [email protected]
Funding informationBrody School of Medicine, Grant/Award
Number: Brody Brothers Seed Grant 2016
AbstractLittle is known about the impact of CYP3A5 polymorphisms on transplantation out-
comes among African American (AA) kidney transplant recipients (KTRs). To assess
this issue, clinical outcomes were compared between AA CYP3A5*1 expressers and
nonexpressers. This retrospective cohort study analyzed AA KTRs. Biopsy- proven
acute rejection (BPAR), delayed graft function (DGF), glomerular filtration rate (GFR),
infections, and tacrolimus dosing requirements were examined in 106 immunologically
high- risk AA kidney transplant patients over a 2- year follow- up period. In CYP3A5*1
expressers compared to nonexpressers, the incidence of BPAR was significantly higher
in the first 6 months (13% vs 0%; P = .016) compared to 24 months (13% vs 7%;
P = .521). Tacrolimus total daily dose at first therapeutic level was significantly higher
in CYP3A5*1 expressers (12 mg/day) compared to nonexpressers (8 mg/day; P < .001).
Compared to CYP3A5*1 nonexpressers, DGF incidence was significantly higher
among CYP3A5*1 expressers (27.6% vs 6.7%; P = .006). By contrast, median GFR was
significantly higher in CYP3A5*1 expressers compared to nonexpressers (54.5 mL/
min vs 50.0 mL/min; P = .003) at 24 months. The findings from this retrospective
study suggest that AAs with CYP3A5*1 expression require 50% more tacrolimus and
have an increased incidence of DGF and acute rejection.
K E Y W O R D S
calcineurin inhibitor: tacrolimus, genomics, immunosuppressant, rejection: acute
1 | INTRODUCTION
Interest in new transplant immunosuppressive therapies continues to
grow; however, calcineurin inhibitors (CNI) remain the cornerstone
of drug therapy with tacrolimus the preferred CNI in recent years.1,2
Tacrolimus is metabolized by the CYP3A system, in particular the
CYP3A5 enzyme, which exhibits polymorphism resulting in signifi-
cant interindividual variability.3-6
As a result, there is growing interest
in the utility of therapeutic dosing strategies based on an individual’s
CYP3A5 profile.7,8
Recent studies conducted in predominantly Caucasian cohorts,
point to a lack of benefit when preemptive pharmacogenetic testing
or tacrolimus dose adaptation was utilized.9-11
Pallet et al report no
difference in the incidence of biopsy- proven acute rejection (BPAR)
and graft survival between the control and the genomic- adapted tac-
rolimus dose group.9 However, a meta- analysis of tacrolimus- treated
kidney transplant patients with CYP3A5 data demonstrated an in-
creased risk of acute rejection and chronic nephrotoxicity among pa-
tients who were CYP3A5*1 expressers.10
Of primary concern is the
relatively low proportion of CYP3A5 expressers and lack of ethnic
diversity in these studies. Whether the racial prevalence of CYP3A5
genotypes is relevant to clinical outcomes is largely unknown.
What is known is that African American (AA) kidney transplant re-
cipients (KTRs) continue to demonstrate inferior outcomes compared
to other races. In a recent analysis, the scientific registry of transplant
recipients reported an approximately 5% lower 5- year graft survival for

4 of 9 | ASEMPA Et Al.
nonexpressers in prior dialysis, cold ischemia time, HLA mismatches, DQ mismatches, cPRA, or induction agents received.
3.2 | Acute rejection
Incidence of first BPAR was compared between CYP3A5*1 express-ers and nonexpressers (Figure 1). At 6 months post- transplantation, CYP3A5*1 expressers had a significantly higher incidence of BPAR compared to nonexpressers (13.2% vs 0%, P = .016). At the 24 month follow- up, there was no statistically significant difference in the in-cidence of BPAR between CYP3A5*1 expressers and nonexpressers (13.2% vs 6.7%, P = .521). Table 2 highlights the clinical characteristics of all patients with BPAR. No rejection was observed among patients expressing noncommon variants (CYP3A5*6; n = 6), CYP3A5*7; n = 1) during the follow- up period (Table 3).
3.3 | Tacrolimus TDD and trough characteristics
Tacrolimus was titrated to therapeutic levels according to interdiscipli-nary transplant team discussions. This study showed that mean TDD at first therapeutic level differed significantly between CYP3A5*1 expressers (12.2 mg/day; SD = 4.04) and nonexpressers (8.3 mg/day; SD = 2.37; P < .001) (Figure 2A). Adjusting for body weight, mean TDD (mg/kg) in patients with and without the CYP3A5*1 allele (0.14 mg/kg per day vs 0.11 mg/kg per day, respectively; P < .001), still differed significantly (Figure 2B). In addition, the median time to therapeutic trough for CYP3A5*1 expressers was 12 days in contrast to 8.5 days for nonexpressers (P = .051) (Figure 3). There was no significant differ-ence regarding mean trough levels at 6 or 24 months between both groups (Figure 4).
3.4 | Renal function
Compared to CYP3A5*1 nonexpressers, the incidence of DGF was significantly higher in CYP3A5*1 expressers (27.6% vs 6.7%; P = .006). At 6 months post- transplant, GFR was comparable between both groups. However, at 24 months, GFR was significantly higher among CYP3A5*1 expressers compared to the nonexpressers (57 mL/min vs 47 mL/min; P = .003) (Table 4).
3.5 | Infections
Opportunistic and nonopportunistic infections were assessed based on CYP3A5*1 expression. The leading infections in patients with CYP3A5*1 expression and nonexpression were urinary tract infec-tion (42% and 37%, respectively) and CMV (28% and 27%, respec-tively). There was no significant difference in the incidence of any infection between CYP3A5*1 expressers and nonexpressers at 6 and 24 months post- transplantation (Table 4).
4 | DISCUSSION
In our study, we evaluated the impact of the genetic polymorphisms of CYP3A5 on tacrolimus daily dose requirements and time to thera-peutic trough in a cohort of AA KTRs. Most importantly, we also re-port patient outcomes including biopsy proven acute rejection, DGF, GFR, and incidence of infections at 2 time points: 6 and 24 months.
Our results indicate that either homozygous or heterozygous carri-ers of the CYP3A5*1 allele (CYP3A5*1 expressers) needed significantly higher doses of tacrolimus on average, that is, 50% more tacrolimus per
F IGURE 1 Kaplan- Meier survival analysis. Time to first rejection episode between CYP3A5*1 expressers and nonexpressersAsempa et al, 2017

6 of 9 | ASEMPA Et Al.
The pooled effect estimate in a meta- analysis of 37 trials demon-strates a higher risk of acute rejection with the CYP3A5*1 expresser genotype (OR: 1.32, 95% CI 1.02- 1.71).10 However, studies evaluat-ing acute rejection in AA patients are limited. In a retrospective single
center study, Taber et al evaluated the time to development of acute rejection based on tacrolimus trough concentrations. By multivariate analysis, AA patients with tacrolimus levels lower than 8 ng/mL ex-perienced a significantly higher risk of acute rejection, which was not demonstrated in non- AAs. Although CYP3A5 genotype was not eval-uated, the authors largely attributed the results to racial differences in pharmacogenomics.31 In a more recent retrospective analysis utilizing the UNOS registry database, Taber et al highlight contemporary racial disparities in kidney transplantation outcomes. Similarly, a significantly higher incidence of acute rejection was reported among AA compared to Caucasians. This study is commendable, given the large number of patients identifying as AA (n = 19 269).32 In recognition of this phar-macogenomic and racial disparity, Sanghavi et al33 proposed and val-idated a tacrolimus dosing model to encompass common CYP3A5 variants prevalent in AAs.
In line with these studies, our findings suggest that targeted phar-macogenomic dosing interventions in AA patients with CYP3A5*1 expression have the potential to improve transplantation outcomes. The few randomized trials evaluating the impact of CYP3A5 gen-otypes on clinical outcomes lacked racial diversity and included pa-tients with low immunological risk.9,34 For example, Shuker et al in a single center prospective trial conducted in the Netherlands and Pallet et al in a multicenter prospective trial conducted in France both concluded that tacrolimus dose adjustments based on CYP3A5 geno-type did not influence acute rejection or renal function.9,34 Although
TABLE 3 Biopsy- proven acute rejection among all CYP3A5 allele variants at 24 months post- transplantation
CYP3A5 allele (%)
*1/*1 (n = 28)
*1/*3 (n = 26)
*1/*6 (n = 9)
*1/*7 (n = 13)
*3/*3 (n = 6)
*3/*6 (n = 10)
*3/*7 (n = 7)
*6/*6 (n = 1)
*6/*7 (n = 5)
*7/*7 (n = 1)
BPAR
ACR 2 (7.1) 5 (19.2) 1 (11.1) 0 (0.0) 1 (16.7)a 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
AMR 0 (0.0) 0 (0.0) 0 (0.0) 2 (15.4) 0 (0.0) 0 (0.0) 1 (14.3) 0 (0.0) 0 (0.0) 0 (0.0)
ACR+AMR 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (16.7)a 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
BPAR,biopsy proven acute rejection; ACR, acute cellular rejection; AMR, antibody- mediated rejection.aSame individual.
F IGURE 2 (A) Therapeutic total daily dose (TDD) (mg) between CYP3A5*1 expressers and nonexpressers. (B) Therapeutic TDD (mg/kg) between CYP3A5*1 expressers and nonexpressers
F IGURE 3 Days to therapeutic trough among CYP3A5*1 expressers and nonexpressers
Asempa et al, 2017

6 of 9 | ASEMPA Et Al.
The pooled effect estimate in a meta- analysis of 37 trials demon-strates a higher risk of acute rejection with the CYP3A5*1 expresser genotype (OR: 1.32, 95% CI 1.02- 1.71).10 However, studies evaluat-ing acute rejection in AA patients are limited. In a retrospective single
center study, Taber et al evaluated the time to development of acute rejection based on tacrolimus trough concentrations. By multivariate analysis, AA patients with tacrolimus levels lower than 8 ng/mL ex-perienced a significantly higher risk of acute rejection, which was not demonstrated in non- AAs. Although CYP3A5 genotype was not eval-uated, the authors largely attributed the results to racial differences in pharmacogenomics.31 In a more recent retrospective analysis utilizing the UNOS registry database, Taber et al highlight contemporary racial disparities in kidney transplantation outcomes. Similarly, a significantly higher incidence of acute rejection was reported among AA compared to Caucasians. This study is commendable, given the large number of patients identifying as AA (n = 19 269).32 In recognition of this phar-macogenomic and racial disparity, Sanghavi et al33 proposed and val-idated a tacrolimus dosing model to encompass common CYP3A5 variants prevalent in AAs.
In line with these studies, our findings suggest that targeted phar-macogenomic dosing interventions in AA patients with CYP3A5*1 expression have the potential to improve transplantation outcomes. The few randomized trials evaluating the impact of CYP3A5 gen-otypes on clinical outcomes lacked racial diversity and included pa-tients with low immunological risk.9,34 For example, Shuker et al in a single center prospective trial conducted in the Netherlands and Pallet et al in a multicenter prospective trial conducted in France both concluded that tacrolimus dose adjustments based on CYP3A5 geno-type did not influence acute rejection or renal function.9,34 Although
TABLE 3 Biopsy- proven acute rejection among all CYP3A5 allele variants at 24 months post- transplantation
CYP3A5 allele (%)
*1/*1 (n = 28)
*1/*3 (n = 26)
*1/*6 (n = 9)
*1/*7 (n = 13)
*3/*3 (n = 6)
*3/*6 (n = 10)
*3/*7 (n = 7)
*6/*6 (n = 1)
*6/*7 (n = 5)
*7/*7 (n = 1)
BPAR
ACR 2 (7.1) 5 (19.2) 1 (11.1) 0 (0.0) 1 (16.7)a 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
AMR 0 (0.0) 0 (0.0) 0 (0.0) 2 (15.4) 0 (0.0) 0 (0.0) 1 (14.3) 0 (0.0) 0 (0.0) 0 (0.0)
ACR+AMR 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 1 (16.7)a 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
BPAR,biopsy proven acute rejection; ACR, acute cellular rejection; AMR, antibody- mediated rejection.aSame individual.
F IGURE 2 (A) Therapeutic total daily dose (TDD) (mg) between CYP3A5*1 expressers and nonexpressers. (B) Therapeutic TDD (mg/kg) between CYP3A5*1 expressers and nonexpressers
F IGURE 3 Days to therapeutic trough among CYP3A5*1 expressers and nonexpressers
Asempa et al, 2017

A Randomized Controlled Trial Comparing theEfficacy of Cyp3a5 Genotype-Based With Body-Weight-Based Tacrolimus Dosing After Living DonorKidney Transplantation
N. Shuker1,2,*,†, R. Bouamar2,†, R. H. N. vanSchaik3, M. C. Clahsen-van Groningen4,J. Damman5, C. C. Baan1, J. van de Wetering1,A. T. Rowshani1, W. Weimar1, T. van Gelder1,2
and D. A. Hesselink1
1Department of Internal Medicine, Erasmus MedicalCentre, Rotterdam, The Netherlands2Department of Hospital Pharmacy, Erasmus MedicalCentre, Rotterdam, The Netherlands3Department of Clinical Chemistry, Erasmus MedicalCentre, Rotterdam, The Netherlands4Department of Pathology, Erasmus Medical Centre,Rotterdam, The Netherlands5Department of Pathology, Academic Medical Centre,Amsterdam, The Netherlands*Corresponding author: Nauras Shuker,[email protected]†Both authors contributed equally to this study.This study was registered in the Dutch national trialregistry (number NTR2226).
Patients expressing the cytochrome P450 (CYP) 3A5gene require a higher tacrolimus dose to achievetherapeutic exposure compared with nonexpressers.This randomized-controlled study investigatedwhether adaptation of the tacrolimus starting doseaccording to CYP3A5 genotype increases the propor-tion of kidney transplant recipients being withinthe target tacrolimus predose concentration range(10–15 ng/mL) at first steady-state. Two hundredforty living-donor, renal transplant recipients wereassigned to either receive a standard, body-weight-based or a CYP3A5 genotype-based tacrolimus start-ing dose. At day 3, no difference in the proportion ofpatients having a tacrolimus exposure within the tar-get range was observed between the standard-doseand genotype-based groups: 37.4% versus 35.6%,respectively; p = 0.79. The proportion of patientswith a subtherapeutic (i.e. <10 ng/mL) or asupratherapeutic (i.e. >15 ng/mL) Tac predose con-centration in the two groups was also not signifi-cantly different. The incidence of acute rejection wascomparable between both groups (p = 0.82). Pharma-cogenetic adaptation of the tacrolimus startingdose does not increase the number of patientshaving therapeutic tacrolimus exposure early after
transplantation and does not lead to improved clini-cal outcome in a low immunological risk population.
Abbreviations: ACMIA, antibody-conjugated mag-netic immunoassay; AE, adverse event; BPAR,biopsy-proven acute rejection; C0, predose concentra-tion; CYP, cytochrome P450; DGF, delayed graftfunction; EMIT, enzyme multiplied immunoassaytechnique; GBG, genotype-based group; MMF, my-cophenolate mofetil; PTDM, posttransplant diabetesmellitus; RTRs, renal transplant recipients; SDG,standard-dose group; SNP, single-nucleotide poly-morphism; Tac, tacrolimus; TDM, therapeutic drugmonitoring
Received 25 October 2015, revised 06 December 2015and accepted for publication 20 December 2015
Introduction
Tacrolimus (Tac) is the cornerstone of immunosuppres-sive therapy after kidney transplantation (1). The clinicaluse of Tac is difficult due to its toxicity, narrow therapeu-tic range, and highly variable pharmacokinetics betweenindividuals (2). The exposure to Tac correlates with theexpression and activity of the Tac-metabolizing enzymescytochrome P450 (CYP) 3A4 and CYP3A5 (3,4). Theseenzymes are polymorphically expressed, which is in partexplained by the presence of single-nucleotide polymor-phisms (SNPs) in the CYP3A4 and CYP3A5 genes (5–8).
A SNP at position 6986 of the CYP3A5 gene (rs776746;6986A>G) causes a splicing defect, resulting in theabsence of functional CYP3A5 protein. Patients who arehomozygous for the 6986 G allele (designated asCYP3A5*3) are therefore expected to lack CYP3A5 activ-ity (6). Renal transplant recipients (RTRs) carrying one ortwo CYP3A5*1 alleles (so-called CYP3A5 expressers)require a significantly higher Tac dose compared withCYP3A5 nonexpressers (9,10). In theory, the earlier ther-apeutic blood concentrations of Tac are attained aftertransplantation, the more effective the drug is likely tobe in preventing acute rejection (11). The higher doserequirement of patients expressing CYP3A5 may cause adelay in reaching the desired Tac target concentrations.
2085
© Copyright 2015 The American Society of Transplantationand the American Society of Transplant Surgeons
doi: 10.1111/ajt.13691
American Journal of Transplantation 2016; 16: 2085–2096Wiley Periodicals Inc.

between the SDG and GBG. Among the CYP3A5expressers, 39.1% (95% CI 22.2–59.2%) of the patientsin the SDG (n = 23) and 26.9% (95% CI 15.3–47.1%) ofthe patients in the GBG (n = 28) were within the targetTac C0 range (p = 0.62). A comparable situation was
found among the CYP3A5 nonexpressers: 36.8% (95%CI 26.9–48.1%) of the patients in the SDG (n = 76) and38.2% (95% CI 28.1–49.4%) of the patients in the GBG(n = 76) were within the target Tac C0 range (p = 1.00;Figure 4B).
Table 2: Tacrolimus dose, predose concentration, and dose-corrected predose concentration according to the treatment group
Whole group Standard-dose group n Genotype-based group N
Tacrolimus dose (mg/day)
Day 3 14.0 (7.0–32.0) 15.0 (8.0–26.0) 119 13.0 (7.0–32.0) 117
Day 7 12.5 (0.0–32.0) 12.0 (0.0–26.0) 119 13.0 (4.0–32.0) 117
Day 10 12.0 (0.0–36.0) 11.0 (0.0–26.0) 117 12.0 (3.0–36.0) 117
Day 14 11.0 (0.0–36.0) 10.0 (1.0–30.0) 117 12.0 (0.0–36.0) 116
Day 30 9.0 (2.0–34.0) 8.0 (2.0–22.0) 115 10.0 (3.0–34.0) 118
Day 60 6.0 (0.0–34.0) 6.0 (0.0–18.0) 114 6.0 (0.0–34.0) 117
Day 90 5.5 (0.0–34.0) 5.0 (0.0–16.0) 114 6.0 (0.0–34.0) 116
Tacrolimus C0 (ng/mL)
Day 3 12.2 (2.6–30.0) 13.3 (2.6–30.0) 99 11.6 (4.1–30.0) 104
Day 7 12.5 (5.0–30.0) 12.7 (5.4–30.0) 96 11.9 (5.0–30.0) 96
Day 10 11.8 (4.3–23.9) 12.1 (5.9–22.7) 79 11.5 (4.3–23.9) 89
Day 14 11.0 (5.1–19.9) 11.1 (5.1–19.9) 44 10.6 (5.6–18.3) 41
Day 30 9.6 (2.9–30.0) 9.3 (2.9–30.0) 104 10.3 (3.6–23.2) 114
Day 60 8.2 (3.3–20.3) 8.6 (3.3–20.3) 110 8.1 (3.8–19.7) 109
Day 90 7.6 (2.7–16.8) 7.5 (2.7–16.7) 103 7.9 (3.4–16.8) 110
Tacrolimus C0/dose (ng/mL per mg/kg)
Day 3 67.8 (13.8–195.3) 64.6 (13.8–162.0) 97 72.0 (23.4–195.3) 104
Day 7 74.9 (20.2–355.6) 76.0 (23.5–355.6) 93 72.8 (20.2–275.6) 96
Day 10 75.6 (22.4–678.3) 80.9 (31.6–678.3) 77 74.5 (22.4–467.0) 88
Day 14 79.6 (10.8–531.6) 82.9 (10.8–531.6) 41 74.3 (15.8–255.9) 41
Day 30 84.6 (16.5–647.5) 90.5 (19.1–647.5) 101 79.5 (16.5–390.6) 113
Day 60 106.7 (14.4–439.2) 109.8 (25.7–439.2) 106 100.2 (14.4–415.7) 106
Day 90 114.2 (19.6–775.0) 114.7 (19.6–775.0) 100 113.3 (22.6–444.0) 109
Figure 2: Boxplots depicting the pre-dose tacrolimus (Tac) concentrations(C0) on day 3 after transplantation in thestandard-dose and genotype-basedgroups. The boxes depict the median and
the 25th and 75th percentiles. The whiskers
depict the 5th and 95th percentiles. The
dots represent the outliers. The shaded
area represents the target Tac C0 range
(10–15 ng/mL).
2090 American Journal of Transplantation 2016; 16: 2085–2096
Shuker et al
Shuker et al, 2017

Shuker et al, 2017
However, on day 3 after transplantation, a trend towardsmore frequent subtherapeutic Tac exposure wasobserved among CYP3A5 expressers in the SDG com-pared with CYP3A5 expressers in the GBG. The reversewas observed for CYP3A5 nonexpressers who were sig-nificantly less frequently below the target Tac C0 in theSDG compared with the GBG (Figure 4B).
SafetyIn total, 728 AEs occurred in the SDG and 750 in theGBG (p = 0.56; Tables 3 and 4). Of these, 148 and 167were judged to be serious (p = 0.40). One patient in theSDG died of bacterial peritonitis. Overall kidney allograftsurvival (including death with a functioning transplant)was 96.6% in the SDG and 99.2% in the GBG(p = 0.370). Kidney allograft survival censored for deathwas 97.5% in the SDG and 99.2% in the GBG(p = 0.62). Three patients in the SDG and one in theGBG lost their graft as a result of vascular complications.
The overall incidence of BPAR was 10.5% (n = 25). TheBPAR rate was comparable between the SDG and GBG:10.1% (n = 12) versus 11.0% (n = 13); p = 0.82. Also,the severity and subtype of BPAR were not differentbetween both treatment groups (Table 3). The rate ofpresumed acute rejection was not significantly different:SDG 4.2% (n = 5) versus GBG 5.1% (n = 6); p = 1.00.
The incidence of DGF was comparable between the twogroups (Table 4). At month 3 after transplantation, renalfunction was similar in the SDG and GBG: median eGFR47 (20–60) versus 50 mL/min per 1.73 m2 (18–60),respectively (p = 0.80). There was no difference in renalfunction recovery or the amount of proteinuria betweenthe SDG and GBG (Figure S4 and Table S6).
There were no significant between-group differences inthe incidence of all other AEs, including PTDM
(p = 0.49), acute Tac-associated nephrotoxicity, and neu-rotoxicity (Table 4). Tac was tolerated well, and onlythree patients (all in the GBG) discontinued Tac. Tac wasdiscontinued because of neurotoxicity (n = 2) and throm-botic microangiopathy (n = 1).
Discussion
In this study, adaptation of the Tac starting dose basedon an individual’s CYP3A5 genotype did not lead to ahigher percentage of patients reaching the desired TacC0 range on day 3 after kidney transplantation, as com-pared to a standard, body-weight-based dosing approach.In addition, CYP3A5 genotype-based Tac dosing did notresult in a lower number of Tac dose modifications, ashorter time to achieve the Tac target C0, or improvedclinical outcome.
This study confirms that CYP3A5 expressers require asignificantly higher Tac dose to reach the same targetexposure compared with nonexpressers (9,10). Using astandard, body-weight-based dosing approach, the firstmedian Tac C0 of CYP3A5 expressers was lower thanthat of nonexpressers. With CYP3A5 genotype-baseddosing, the proportion of patients with subtherapeuticTac exposure tended to decrease among CYP3A5expressers, whereas it increased significantly amongCYP3A5 nonexpressers. The reverse was observed withregard to supratherapeutic Tac exposure (Figure 4B). Asa result, the CYP3A5 genotype-based adjustment of theTac starting dose did not change the overall proportion ofpatients within the target Tac C0 range.
In a randomized-controlled study that included 280 RTRs,Thervet et al demonstrated that CYP3A5-based adapta-tion of the Tac starting dose does increase the proportionof patients on target compared with a standard, body-weight-based dosing approach. Three days after the startof Tac treatment, significantly more RTRs were withinthe target Tac C0 range if Tac was individualized accord-ing to CYP3A5 genotype as compared with standard Tacdosing (43.2% vs. 29.1%, respectively; p = 0.03) (18). Inaddition, CYP3A5-based Tac dosing was associated withfewer dose modifications and a shorter time to reach thetarget C0. However, and in line with the present findings,CYP3A5 genotype-based Tac dosing did not improve clin-ical outcomes (18).
It is unknown why the CYP3A5-based Tac dosingapproach of Thervet et al was beneficial in terms of earlyTac exposure, whereas this was not the case in the pre-sent study. In both studies, the same Tac starting doseswere prescribed and the number of included patients iscomparable. However, in contrast to the current study, inwhich Tac was started directly after transplantation, theinitiation of Tac treatment was delayed until day 7 aftertransplantation in the French trial, in which recipients of
Figure 3: Time to achieve the target tacrolimus C0 range(10.0–15.0 ng/mL).
American Journal of Transplantation 2016; 16: 2085–2096 2091
Pharmacogenetic Adaptation of the Tacrolimus Starting Dose

Shuker et al, 2017
No significant between-group difference was found inthe frequency of being markedly underexposed duringthe first month after transplantation. During this timeperiod, 12 patients (10.3%; 95% CI 6.0–17.1%) in theSDG and 13 patients (11.1%; 95% CI 6.6–18.1%) in theGBG had one or more Tac C0 <5.0 ng/mL (p = 0.83).Likewise, the number of patients experiencing markedTac overexposure was comparable between the SDGand GBG: 38 patients (32.5%; 95% CI 24.7–41.4%) inthe SDG and 28 (23.9%; 95% CI 17.1–32.4%) patients inthe GBG (p = 0.15).
Post-hoc pharmacokinetic analyses: To investigatewhether CYP3A5 expressers do require a higher Tacdose to achieve target concentrations compared withCYP3A5 nonexpressers, the whole study population wasanalyzed. On day 3 after transplantation, CYP3A5expressers (n = 50) had a 36.3% higher Tac doserequirement (C0/D) compared with nonexpressers(n = 151): 49.1 ng/mL per mg/kg (13.8–150.9) versus77.1 ng/mL per mg/kg (25.8–195.3); p < 0.001(Table S4). The difference in Tac C0/D between CYP3A5expressers and nonexpressers persisted throughout the3-month follow-up period (Table S4 and Figure S3).
Repeated measurements analysis confirmed that theoverall Tac C0/D was significantly lower in CYP3A5expressers than in nonexpressers, indicating a higherdose requirement of the former group (p < 0.001).
Tac exposure on day 3 of the patients in the SDG and GBGwas analyzed according to their CYP3A5 genotype (Fig-ure 4A). The median Tac C0 in patients homozygous forCYP3A5*1 was not statistically significantly differentbetween patients in the SDG and GBG: median 6.8 ng/mL(4.6–10.6 ng/mL) versus 9.4 ng/mL (8.1–25.7 ng/mL);p = 0.40 (Figure 4A and Table S5). HeterozygousCYP3A5*1 carriers in the SDG had a significantly lowerTac C0 compared with their counterparts in the GBG: med-ian 10.4 ng/mL (2.6–30.0) versus 14.7 ng/mL (6.5–30.0);p = 0.024. Among CYP3A5 nonexpressers (those with theCYP3A5*3/*3 genotype), Tac C0 was significantly higherin the SDG than in the GBG: 14.5 ng/mL (5.5–30.0) versus11.3 ng/mL (4.1–30.0); p < 0.001 (Table S5; Figure 4A).
When the proportion of patients within the target TacC0 range on day 3 after transplantation was analyzedaccording to CYP3A5 genotype (expressers and nonex-pressers), no significant differences were found
Table 1: Baseline characteristics
Standard-dose group Genotype-based group p
Recipient gender
Male/female 73 (61.3%)/46 (38.7%) 75 (63.6%)/43 (36.4%) 0.73
Age of recipient (years) 57 (19–79) 55 (19–79) 0.55
Ethnicity 0.89
White 93 (78.2%) 93 (78.8%)
Asian 13 (10.9%) 10 (8.5%)
Black 11 (9.2%) 12 (10.2%)
Other 2 (1.7%) 3 (2.5%)
Body weight (kg) 75.7 (37.6–132.0) 81.2 (43.6–123.1) 0.21
Length (cm) 173.0 (145.0–203.0) 174.0 (151.0–196.0) 0.77
BMI (kg/m2) 25.5 (17.2–37.8) 26.2 (18.1–42.2) 0.21
Primary kidney disease
Diabetic nephropathy 21 (17.6%) 23 (19.5%)
Polycystic kidney disease 17 (14.3%) 18 (15.3%)
Glomerulonephritis 16 (13.3%) 27 (22.6%)
Hypertensive nephropathy 16 (13.3%) 13 (11.0%)
Reflux disease/Chronic pyelonephritis 7 (5.8%) 6 (5.0%)
Other 6 (5.0%) 4 (3.2%)
Unknown 36 (30.3%) 27 (22.9%)
Number of kidney transplantations 0.46
1st 111 (93.3%) 107 (90.7%)
2nd 7 (5.9%) 9 (7.6%)
3rd 1 (0.8%) 2 (1.7%)
RRT prior to kidney transplantation 0.55
Hemodialysis 46 (38.7%) 44 (37.3%)
Peritoneal dialysis 20 (16.8%) 24 (20.3%)
Pre-emptive 53 (44.5%) 49 (41.5%)
Donor type
Living-related/Living-unrelated 48 (40.3%)/71 (59.7%) 47 (39.8%)/71 (60.2%) 0.94
PRA% (<15%/≥15%) 111 (93.3%)/8 (6.7%) 109 (92.4%)/8 (6.8%) 0.97
Peak PRA% (<15%/≥15%) 100 (84%)/19 (16.0%) 93 (78.8%)/24 (20.3%) 0.37
BMI, body mass index; RRT, renal replacement therapy; PRA, panel reactive antibodies.
American Journal of Transplantation 2016; 16: 2085–2096 2089
Pharmacogenetic Adaptation of the Tacrolimus Starting Dose

Birdwell et al, 2012
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
Birdwell et al. Page 24
Table 3
Results for fixed effects in the mixed-effects model for CYP3A5*3 in the longitudinal data analysis for log-transformed tacrolimus C/D ratio.
Covariate Coefficienta (S.E.) P value
CYP3A5*3 0.54 (0.044) 7.15 × 10−29
Albuminb (x) −0.17 (0.04) 2.07 × 10−5
(x') 0.12 (0.04) 0.005
Age 0.007 (0.002) 1.80 × 10−5
Weightb (x) −0.007 (0.002) 3.24 × 10−4
(x') 0.006 (0.002) 0.004
Hemoglobin 0.015 (0.006) 0.012
Days post transplantb (x) 0.0004 (6.2 × 10−5) 2.97 × 10−9
(x') −0.0012 (2.5 × 10−4) 2.44 × 10−6
Sex (Male vs. Female) 0.034 (0.043) 0.431
Principal components (PCs)
PC1 −0.85 (0.59) 0.155
PC2 0.28 (0.40) 0.487
PC3 −0.34 (0.40) 0.404
PC4 −0.25 (0.40) 0.535
PC5 −0.20 (0.40) 0.616
PC6 −0.74 (0.40) 0.064
PC7 0.09 (0.40) 0.816
PC8 −0.27 (0.40) 0.504
PC9 0.57 (0.40) 0.157
PC10 0.48 (0.40) 0.228
aFor coefficients with a positive value, the covariate results in an increase in log-transformed tacrolimus C/D ratio, whereas a negative values
results in a decrease in log-transformed tacrolimus C/D ratio.
bRestricted cubic spline functions with 3 knots were used to model nonlinear time trend and relationships, and x and x' are the corresponding linear
and nonlinear terms.
Pharmacogenet Genomics. Author manuscript; available in PMC 2013 January 1.

increased time in therapeutic range versus fixed dosing at12 weeks in a predominantly white population, the Clar-ification of Optimal Anticoagulation through Genetics Trialshowed no improvement of a pharmacogenomics algo-rithm over a clinical algorithm at 4 weeks in a more diverseAmerican population (24,25). Most recently, however, themulticenter, randomized Genetics Informatics Trial(GIFT) showed that genotype-guided warfarin dosingimproved clinical outcomes versus clinically guided dos-ing. The rate of a composite of major bleeding, INR of fouror greater, venous thromboembolism, or death was re-duced from 14.7% to 10.8% in elderly patients undergoingelective hip or knee arthroplasty (26). Collectively, thesetrials show the importance of generalizability of results;measuring hard clinical outcomes versus surrogates, likeINR; ethnic diversity in clinical trials; and the genotypecoverage of pharmacogenomics testing. Future work willno doubt study cost-effectiveness and the effect of broadergenotyping. In fact, in a recent prospective observationaltrial, de Oliveira Almeida et al. (27) found that othergenetic variants (in APOE, ABCB1, and UGT1A1) were alsoassociated with warfarin dose.Current evidence-based CPIC guidelines for warfarin
dosing include CYP2C9, VKORC1, and CYP4F2, and theyare specific to patient self-identified ancestry. In non-African ancestry patients, the highest evidence is availablefor patients who carry at least one reduced functionCYP2C9 allele (e.g., *2, *3), which predicts decreasedhepatic clearance and lower dose requirements. Patientscarrying a VKORC1–1639G.A allele are expected to havehigher sensitivity to warfarin, thus requiring a lower dose.Individuals who have both of these variations requiremuch lower doses of warfarin. Carriers of CYP4F2 *3 allelemay also require a 5%–10% increase in dose. In patientswith African ancestry, because nearly one half of individ-uals may carry CYP2C9 *5, 6, *8, *11, or rs12777823variants, genotype-guided warfarin dosing is only recom-mended if testing covers these variants (23).The FDA-approved product labeling contains recom-
mendations for initial dosing with a convenient table onthe basis of CYP2C9 and VKORC1 (28). Finally, Gageet al. (29), who led the GIFT, also maintain a web-based
application (www.warfarindosing.org), which incorporatesadditional clinical and genetic data to provide tailoredwarfarin dosing in an easy-to-use interface. Neither toolcurrently incorporates kidney function in these recommen-dations.Clopidogrel. Antiplatelet medications (prasugrel, ticagrelor,
and clopidogrel) are indicated for patients who receivecoronary artery stenting (30). They may also be used afterkidney artery stenting, although the evidence for thisis less robust (31). These drugs carry differing risksfor bleeding, treatment failure, and cost, and their use ischallenged by the lack of a well validated biomarker oftreatment response. The most commonly prescribed drug,clopidogrel, is a prodrug that requires metabolic activationby CYP2C19 among other enzymes. Patients with de-creased metabolic activity at CYP2C19 have decreasedgeneration of the active metabolite and decreased plateletinhibition (32,33). Conversely, patients with increasedCYP2C19 activity (rapid and ultrarapid metabolizers) mayhave increased generation of the active metabolite forclopidogrel and thus, a theoretically higher platelet in-hibition and increased risk for bleeding. The NationalInstitutes of Health–funded Implementing Genomics in Prac-tice network’s multicenter observational trial investigatedpatient outcomes with pharmacogenomics-guided antiplatelettherapy after percutaneous coronary intervention and stenting.Patients carrying at least one nonfunctional allele at CYP2C19whowere treatedwith clopidogrel versus alternative therapywere at higher risk for major adverse cardiovascularevents (hazard ratio, 2.26; 95% CI: 1.18 to 4.32; P50.01) (34).This suggests that pharmacogenomics testing for CYP2C19may provide a significant clinical benefit in real world clinicaluse. The CPIC guideline for clopidogrel therapy recommendsthat patients with at least one decreased function allele (*2, *3,etc.) receive an alternative agent due to risk for decreasedresponse. Additionally, the guideline recommends thatpatients with increased metabolism (*1/*17 and *17/*17) bemonitored for increased bleeding risk, although it does notrecommend different dosing (35). Implementation of rou-tine CYP2C19 testing in cardiac catheterization laboratoriesis feasible and has been a popular first pharmacogenomicsimplementation at several health systems (9).
Table 2. Summary of the gene-drug pairs and clinical guidelines relevant to nephrology
Drug Gene Clinical Guidance Summary Ref.
Warfarin CYP2C9 Use lower dose if a poor or intermediate metabolizer (e.g., *2/*2, *1/*2) 23Warfarin CYP4F2 Use lower dose if decreased activity (*3) 23Warfarin VKORC1 Use lower dose if increased sensitivity (21639G.A) 23Clopidogrel CYP2C19 Use alternative antiplatelet agent if poor or intermediate metabolizer
(e.g., *2/*2, *1/*2); monitor for bleeding if ultrarapid metabolizer (*1/*17, *17/*17)35
Simvastatin SLCO1B1 Use lower dose or alternative agent in patients with decreased transporter activity(*5, *15, *17)
37
Azathioprine TPMT Patients with decreased TPMT function have higher risk for toxicity 39Tacrolimus CYP3A5 Carriers of at least one functional (*1) allele may require higher doses 13Voriconazole CYP2C19 Use an alternative agent in CYP2C19 rapid/ultrarapid metabolizer (*1/*17, *17/*17);
use alternative agent or lower dose in CYP2C19 poor metabolizer (*2/*2, *3/*3)40
Allopurinol HLA-B User an alternative uric acid–lowering agent in patients who carry at least one *58:01 allele 53
TPMT, thiopurine methyltransferase.
Clin J Am Soc Nephrol 13: 1561–1571, October, 2018 Pharmacogenomics in Nephrology, Adams et al. 1565
Adams et al, 2018
Metformin: rs11212617 Patients with at least one “A” allele require higher doses for adequate hemoglobin A1c control



RESEARCH ARTICLE Open Access
Pharmacogenetic testing through thedirect-to-consumer genetic testingcompany 23andMeMengfei Lu1, Cathryn M. Lewis1,2 and Matthew Traylor1*
Abstract
Background: Rapid advances in scientific research have led to an increase in public awareness of genetic testingand pharmacogenetics. Direct-to-consumer (DTC) genetic testing companies, such as 23andMe, allow consumersto access their genetic information directly through an online service without the involvement of healthcareprofessionals. Here, we evaluate the clinical relevance of pharmacogenetic tests reported by 23andMe in theirUK tests.
Methods: The research papers listed under each 23andMe report were evaluated, extracting information on effectsize, sample size and ethnicity. A wider literature search was performed to provide a fuller assessment of thepharmacogenetic test and variants were matched to FDA recommendations. Additional evidence from CPICguidelines, PharmGKB, and Dutch Pharmacogenetics Working Group was reviewed to determine current clinicalpractice. The value of the tests across ethnic groups was determined, including information on linkagedisequilibrium between the tested SNP and causal pharmacogenetic variant, where relevant.
Results: 23andMe offers 12 pharmacogenetic tests to their UK customers, some of which are in standard clinicalpractice, and others which are less widely applied. The clinical validity and clinical utility varies extensively betweentests. The variants tested are likely to have different degrees of sensitivity due to different risk allele frequencies andlinkage disequilibrium patterns across populations. The clinical relevance depends on the ethnicity of the individualand variability of pharmacogenetic markers. Further research is required to determine causal variants and providemore complete assessment of drug response and side effects.
Conclusion: 23andMe reports provide some useful pharmacogenetics information, mirroring clinical tests that arein standard use. Other tests are unspecific, providing limited guidance and may not be useful for patients withoutprofessional interpretation. Nevertheless, DTC companies like 23andMe act as a powerful intermediate step tointegrate pharmacogenetic testing into clinical practice.
BackgroundRecent advances in technology have enabled comprehen-sive characterization of the genetic component underlyingmany complex diseases, traits, and responses to medica-tion. This new information has enabled genetic testing tobecome more widely available in healthcare, and can beused to assess risk of inherited conditions and predictresponse to medication. Such testing has the potential toreduce drug-related adverse events, as well as to increase
the effectiveness of drugs by assessing how sensitive anindividual might be to a given pharmaceutical. Severalpharmacogenetic tests have become standard clinicalpractice and others are supported by strong research evi-dence. However, challenges exist in moving pharmacoge-netic testing from a research endeavor to point-of-careimplementation.Traditionally, genetic tests have been ordered in clinical
settings but direct-to-consumer (DTC) genetic testingcompanies allow consumers to access their genetic infor-mation through an online service without the intermedi-ary of a healthcare professional. A 2012 review of onlinecompanies offering pharmacogenetic testing identified
* Correspondence: [email protected] of Medical and Molecular Genetics, King’s College London, 8thFloor Tower Wing, Guy’s Hospital, Great Maze Pond, London SE1 9RT, UKFull list of author information is available at the end of the article
© The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Lu et al. BMC Medical Genomics (2017) 10:47 DOI 10.1186/s12920-017-0283-0

as abacavir hypersensitivity reactions which are associatedwith HLA-B*57:01. All reports are for variants in a singlegene, except for warfarin which combines genotypes fromthree SNPs in CYP2C9 and VKORC1. The report foracetaldehyde toxicity, leading to increased risk ofoesophageal squamous cell carcinoma in people ofEast Asian ancestry, is a curious entry in the list,
since the toxicity arises from a breakdown of alcohol,a recreational drug, and not a pharmaceutical com-pound as in the other 11 tests.The FDA considers that pharmacogenetic tests for five
of the 12 drugs provide actionable results (fluorouracil,peginterferon alpha, phenytoin, pseuodocholinesterasedeficiency and warfarin); genetic testing is required for
Table 1 Pharmacogenetic tests provided by 23andMeDrugs Gene Variant SNP Purpose of test FDA/PharmGKB
GuidanceaGuidelinesb
Abacavir HLA-B *57:01 rs2395029 Hypersensitivity reactions Genetic testing requiredCPIC, DPWG
CPIC, DPWG
Acetaldehyde ALDH2 *2 rs671 Toxicity and risk of oesophageal squamous cellcarcinoma
No recommendation -
Clopidogrel (Plavix®) CYP2C19 *2 rs4244285 Efficacy and ADRs Genetictesting recommendation
CPIC, DPWG
*3 rs4986893
*4 rs28399504
*8 rs41291556
*17 rs12248560
Fluorouracil (Adrucil®) DPYD *2A rs3918290 Toxicity and ADRs Actionable PGx CPIC, DPWG
Peginterferon alpha(PEG-IFN-alpha) &ribavirin (RBV)
19q13region
rs8099917 Hepatitis C treatment failure Actionable PGx CPIC
Phenytoin CYP2C9 *2 rs1799853 Sensitivity and Dosage adjustment Actionable PGx CPIC, DPWG
*3 rs1057910
Proton Pump Inhibitor(PPI)
CYP2C19 *2 rs4244285 Efficacy and Dosage adjustment Informative PGx DPWG
*3 rs4986893
*4 rs28399504
*8 rs41291556
*17 rs12248560
Pseudocholinesterase BCHE F1 rs28933389 ADR - extended paralysis and apnoea Actionable PGx -
Deficiency F2 rs28933390
A rs1799807
Simvastatin SLCO1B1 *5 rs4149056 ADR - Myopathy No recommendation CPIC
Sulfonylurea CYP2C9 *2 rs1799853 Efficacy and Dosage adjustment No recommendation DPWG
*3 rs1057910
ThiopurineMethyltransferase
TPMT c.460G > A,*3B
rs1800460 Toxicity and ADRs Genetictesting recommended
CPIC, DPWG
c.238G > C,*2
rs1800462
c.719A > G,*3C
rs1142345
Warfarin CYP2C9 *2 rs1799853 Efficacy and Dosage adjustment Actionable PGx CPIC
*3 rs1057910
VKORC1 rs9923231aPharmGKB evaluated the pharmacogenetic (PGx) information provided by U.S. FDA approved drug labels, and assigned each test with a level ofrecommendation according to the level of clinical evidence, [7] The levels begin from genetic testing required, genetic test recommended,Actionable PGx to Informative PGx.b: Guidelines from https://www.pharmgkb.org/view/dosing-guidelines.do published by the Clinical Pharmacogenetics Implementation Consortium(CPIC) or the Royal Dutch Association for the Advancement of Pharmacy - Pharmacogenetics Working Group (DPWG)*used to indicate that these values represent a given variant in the literature
Lu et al. BMC Medical Genomics (2017) 10:47 Page 3 of 8

as abacavir hypersensitivity reactions which are associatedwith HLA-B*57:01. All reports are for variants in a singlegene, except for warfarin which combines genotypes fromthree SNPs in CYP2C9 and VKORC1. The report foracetaldehyde toxicity, leading to increased risk ofoesophageal squamous cell carcinoma in people ofEast Asian ancestry, is a curious entry in the list,
since the toxicity arises from a breakdown of alcohol,a recreational drug, and not a pharmaceutical com-pound as in the other 11 tests.The FDA considers that pharmacogenetic tests for five
of the 12 drugs provide actionable results (fluorouracil,peginterferon alpha, phenytoin, pseuodocholinesterasedeficiency and warfarin); genetic testing is required for
Table 1 Pharmacogenetic tests provided by 23andMeDrugs Gene Variant SNP Purpose of test FDA/PharmGKB
GuidanceaGuidelinesb
Abacavir HLA-B *57:01 rs2395029 Hypersensitivity reactions Genetic testing requiredCPIC, DPWG
CPIC, DPWG
Acetaldehyde ALDH2 *2 rs671 Toxicity and risk of oesophageal squamous cellcarcinoma
No recommendation -
Clopidogrel (Plavix®) CYP2C19 *2 rs4244285 Efficacy and ADRs Genetictesting recommendation
CPIC, DPWG
*3 rs4986893
*4 rs28399504
*8 rs41291556
*17 rs12248560
Fluorouracil (Adrucil®) DPYD *2A rs3918290 Toxicity and ADRs Actionable PGx CPIC, DPWG
Peginterferon alpha(PEG-IFN-alpha) &ribavirin (RBV)
19q13region
rs8099917 Hepatitis C treatment failure Actionable PGx CPIC
Phenytoin CYP2C9 *2 rs1799853 Sensitivity and Dosage adjustment Actionable PGx CPIC, DPWG
*3 rs1057910
Proton Pump Inhibitor(PPI)
CYP2C19 *2 rs4244285 Efficacy and Dosage adjustment Informative PGx DPWG
*3 rs4986893
*4 rs28399504
*8 rs41291556
*17 rs12248560
Pseudocholinesterase BCHE F1 rs28933389 ADR - extended paralysis and apnoea Actionable PGx -
Deficiency F2 rs28933390
A rs1799807
Simvastatin SLCO1B1 *5 rs4149056 ADR - Myopathy No recommendation CPIC
Sulfonylurea CYP2C9 *2 rs1799853 Efficacy and Dosage adjustment No recommendation DPWG
*3 rs1057910
ThiopurineMethyltransferase
TPMT c.460G > A,*3B
rs1800460 Toxicity and ADRs Genetictesting recommended
CPIC, DPWG
c.238G > C,*2
rs1800462
c.719A > G,*3C
rs1142345
Warfarin CYP2C9 *2 rs1799853 Efficacy and Dosage adjustment Actionable PGx CPIC
*3 rs1057910
VKORC1 rs9923231aPharmGKB evaluated the pharmacogenetic (PGx) information provided by U.S. FDA approved drug labels, and assigned each test with a level ofrecommendation according to the level of clinical evidence, [7] The levels begin from genetic testing required, genetic test recommended,Actionable PGx to Informative PGx.b: Guidelines from https://www.pharmgkb.org/view/dosing-guidelines.do published by the Clinical Pharmacogenetics Implementation Consortium(CPIC) or the Royal Dutch Association for the Advancement of Pharmacy - Pharmacogenetics Working Group (DPWG)*used to indicate that these values represent a given variant in the literature
Lu et al. BMC Medical Genomics (2017) 10:47 Page 3 of 8

PGx in HCT
http://www.huffingtonpost.com

Influence of Absorption, Distribution, Metabolism, andExcretion Genomic Variants on Tacrolimus/Sirolimus BloodLevels and Graft-versus-Host Disease after AllogeneicHematopoietic Cell Transplantation
Samer K. Khaled 1,2,*, Joycelynne M. Palmer 3, Josef Herzog 4, Tracey Stiller 3, Ni-Chun Tsai 3,David Senitzer 5, Xueli Liu 3, Sandra H. Thomas 1, Sepideh Shayani 6, Jeffrey Weitzel 4,Stephen J. Forman 1, Ryotaro Nakamura 1
1Department of Hematology and Hematopoietic Cell Transplantation, City of Hope, Duarte, California2Gehr Family Center for Leukemia Research of the Hematologic Malignancies and Stem Cell Transplantation Institute of the City of Hope, Duarte, CA3Division of Biostatistics, City of Hope, Duarte, California4Division of Clinical Cancer Genetics, City of Hope, Duarte, California5Division of Histocompatibility (HLA Laboratory), City of Hope, Duarte, California6Department of Pharmacy, City of Hope, Duarte, California
Article history:Received 7 May 2015Accepted 19 August 2015
Key Words:ImmunosuppressantDrug absorption, distribution,metabolism, and excretion(ADME)Pharmacogenetics
a b s t r a c tAllelic variants of genes implicated in drug absorption, distribution, metabolism, and excretion (ADME)determine the pharmacokinetic variability of many medications and are increasingly recognized as importantfactors determining the success or failure of medical treatments. Both tacrolimus and sirolimus have narrowtherapeutic ranges maintained by therapeutic drug monitoring (TDM). Using an ADME panel that covers>99% of the PharmaADME working group core list (188 single nucleotide polymorphism [SNP] and 12 copynumber variant [CNV] assays in 36 pharmacogenetically relevant genes), we studied 177 patients who un-derwent allogeneic hematopoietic cell transplantation (HCT) using tacrolimus/sirolimusebased graft-versus-host disease (GVHD) prophylaxis. We tested for possible associations between ADME variants and tacrolimus/sirolimus drug levels, concentration/dose (C/D) ratio, and clinical endpoints, including acute GVHD. A total of62 SNP and 6 CNV assays were evaluable after removing the variants, which were homozygous in (nearly) allsamples. For sirolimus, rs2032582 (ABCB1) T-carriers versus noneT-carriers were associated with higher bloodlevels (P ¼ .01), with similar results for C/D ratio. Generalized estimating equation analysis supported thesefindings. For tacrolimus, rs776746 CYP3A5*3/*3 and CYP3A5*3/*1 were associated with higher blood levelsthan CYP3A5*1/*1 (P ¼ .002). By multivariable analysis, rs776746 CYP3A5*3/*3 and CYP3A5*3/*1 were inde-pendently associated with decreased acute GVHD compared with CYP3A5*1/*1, after adjustment for condi-tioning, donor type, race/ethnicity, and age. We demonstrated association of specific ADME geneticpolymorphisms with blood levels of tacrolimus/sirolimus, and incidence of acute GVHD after HCT, in spite ofTDM and dose adjustment. A larger ongoing study will determine whether these associations have clinicalutility beyond TDM.
! 2016 American Society for Blood and Marrow Transplantation.
INTRODUCTIONAllogeneic hematopoietic cell transplantation (HCT) is an
effective and potentially curative therapy for a variety ofmalignant and nonmalignant hematologic diseases [1];
however, graft-versus-host disease (GVHD) remains a majorcomplication and a leading cause of morbidity and mortalityafter transplantation [2]. We and others have evaluated thecombination of 2 immunosuppressive drugs, tacrolimus andsirolimus, as a GVHD prophylactic regimen, demonstratingthat the combination is associated with reduced incidence/severity of acute GVHD and transplantation-related mortal-ity [3-6]. A randomized phase III trial, conducted by theBlood and Marrow Transplant Clinical Trials Network,compared tacrolimus/methotrexate versus tacrolimus/
Financial disclosure: See Acknowledgments on page 275.* Correspondence and reprint requests: Samer K. Khaled, MD, Depart-
ment of Hematology/HCT, City of Hope, 1500 E. Duarte Rd., Duarte,CA 91010.
E-mail address: [email protected] (S.K. Khaled).
http://dx.doi.org/10.1016/j.bbmt.2015.08.0271083-8791/! 2016 American Society for Blood and Marrow Transplantation.
Biol Blood Marrow Transplant 22 (2016) 268e276
Biology of Blood andMarrow Transplantationjournal homepage: www.bbmt.org

at days 7 and 14 after HCT. None of the polymorphisms forthe 3 genes of interest gave indications of association withincreased serum creatinine levels (Table S4). Among addi-tional genes in the ADME PGx Panel, 6 gene polymorphismstrended toward association (P ! .05) with either day 7 or day14 increased creatinine levels, with NAT2 (rs1799931)attaining P< .01 over the first 7 days and P¼ .02 over the first14 days after transplantation. All observed increased creati-nine levels were 1.4-fold or less.
TMA outcomesWe analyzed all evaluable polymorphisms for association
with cumulative incidence of TMA after HCT. None of thepolymorphisms for the 3 genes of interest gave indications ofassociation with TMA incidence (Table S5). In the additionalgenes from the ADME PGx Panel, 6 variants in 4 genestrended toward association with TMA (P ! .05), including3 SNPs from the NAT2 gene, rs1041983 (P ¼ .03), rs1799930(P ¼ .02), and rs1799931 (P < .01).
Other clinical outcomesWe also evaluated the impact of ADME genetic variants
on 100-day nonrelapse mortality; however, none of the 3genes of interest showed an association.
DISCUSSIONPossible associations between abnormal drug reactions
and individual inherited factors were first noted in the early20th century; however, the term “pharmacogenetics” wascoined by the German physician Friedrich Vogel in 1959 [33].Since then, the field of pharmacogenetics has evolved andnumerous reports have been published on the influence ofspecific SNPs on multiple medications across medical disci-plines. These reports have prompted the Food and DrugAdministration to revise drug labels to include relevantpharmacogenetic information and recommendations forcertain drugs, such as clopidogrel and warfarin [34]. Despitethe advances in this field, we are still in an exploratory era,with many influential genetic variants still to be uncovered.
The use of immunosuppressive therapy is essential in HCTto prevent potentially lethal GVHD reactions. Our institutionand others utilize the combination of tacrolimus and siroli-mus for GVHD prophylaxis. Vigilant monitoring of targetblood levels is necessary to avoid adverse reactions andprovide adequate immunosuppression because of the nar-row therapeutic ranges of both tacrolimus and sirolimus.Pharmacogenetic association studies can help us to predicttarget doses of these medications and assist clinicians inoptimizing patient management. The association betweenthe ADME genotype and immunosuppressant blood con-centration is illustrated in solid organ transplantation bymultiple reports. For instance, Zhang et al. report that pa-tients with CYP3A5*1/*1 and *1/*3 have lower dose-adjustedtacrolimus concentrations compared with patients withCYP3A5 *3/*3, in patients undergoing kidney transplantation[35]. Anglicheau and colleagues describe a similar effect ofCYP3A4 and CYP3A5 polymorphisms on the bioavailability ofsirolimus [36]. These genomic variations can also affect theclinical outcome in renal transplantation. Patients who areCYP3A5*3 expressers show a reduced incidence of acuterejection [37] and longer time to first rejection episode [38].On the other hand, patients who are CYP3A5*3 homozygoteshave higher nephrotoxicity: 47% compared with 17% in pa-tients who carried at least 1 CYP3A5*1 allele [39].
In contrast, studies in HCT are scarce because of thecomplexity of the conditioning regimens and GVHD regi-mens and the many drug-drug interactions. Not only arepatients recovering from myeloablative chemotherapy, butthey are also on a host of supportive care medications, suchas antifungal drugs that may affect immunosuppressant druglevels. Despite the difficulty in obtaining clear cut results inthis setting, we believe that this analysis will spark interest infuture studies examining the role of ADME in HCT regimensand possible pharmacogenetic associations with trans-plantation outcomes.
To our knowledge, this is the first study to demonstratethe use of a comprehensive ADME panel in the setting of HCT.This study used the iPLEX ADME PGx Panel (Agena Biosci-ence), allowing us to economically explore a large number ofpolymorphisms in a relatively short period of time. Wefocused our analyses on the early post-transplantationperiod, specifically the first 7 days after transplantation fortacrolimus and the first 14 days for sirolimus (because of itslonger half-life), because we expected a greater impact fromADME genetic variants before physician TDM had stabilized
0 2 4 6 8 10 12 14
05
1015
2025
30
0 2 4 6 8 10 12 14
05
1015
2025
30
Siro
limus
Lev
els
(ng/
ml)
Tacr
olim
us L
evel
s (n
g/m
l)
Time post-HCT (days)
Time post-HCT (days)
A
B
Figure 2. Association of SNPS immunosuppressant drug levels over time.Repeated drug level measurements over time were plotted for individual pa-tients and a Loess smoothed curve was fitted. (A) depicts the association ofABCB1 rs2032582 on sirolimus drug levels over time after infusion of stem cellsat allogeneic hematopoietic cell transplantation (alloHCT). Red lines indicate T-carrier variants (TT, TA, GT) and black lines indicate non-T carriers (AA, GG, GA).(B). depicts the association of CYP3A5 rs776746 on tacrolimus drug levels overtime post alloHCT. Red lines are GG variants, blue are GA, and black are AA.
S.K. Khaled et al. / Biol Blood Marrow Transplant 22 (2016) 268e276 273
*3/*3, *1/*3, *1/*1
Khaled et al, 2016

Khaled et al, 2016
polymorphism is present in about 70% of the Caucasianpopulation, whereas it accounts for 27% to 50% of CYP3A5alleles in African Americans, 65% to 85% in Asians, and 75% inMexican populations [40]. Although our sample populationhas low African American and Asian representation, wewereable to demonstrate an association in our population mix.This result is corroborated by reports published in solid or-gan transplantation [37-39,41]. Association of the rs776746polymorphismwith tacrolimus at 7 days after HCT, was seenat a significance level of P ¼ .002. This trend was maintainedwhenwe analyzed the C/D ratio to account for TDM and dosemodification by the treating physician (P ¼ .01). Additionalpolymorphisms in the ADME panel, such as 2 CNV assaysfrom the UGT2B17 gene, exhibited possible associations withtacrolimus blood levels that will be evaluated further infuture studies.
In comparison to our finding with tacrolimus, we did notfind a significant difference in sirolimus blood levels associ-ated with the rs776746 (CYP3A5) in the first 14 days afterHCT. Although some reports from solid organ transplantationindicate that there is an influence of CYP3A5 on the sirolimusblood level [42,43], these studies were conducted in theabsence of tacrolimus. In a study by Anglicheau et al., theassociation of CYP3A4 and CYP3A5 with sirolimus levels waseliminated when sirolimus was combined with a calcineurininhibitor [36], which may explain our results. On the otherhand, we observed a possible association in the blood levelsof sirolimus in relation to rs2032582 (ABCB1) (P ¼ .01) at 14days after HCT, with a similar trend toward association of C/Dratio (P ¼ .05). In the additional polymorphisms from theADME panel, several variants were associated with eithersirolimus blood levels or C/D ratio, but none gave a signal forboth blood levels and C/D ratio.
Genetic polymorphisms in ADME genes may not onlyimpact drug levels but can also impact clinical outcomes dueto enhanced or reduced pharmacologic efficacy/toxicity ofany given drug. In fact, we found that that the CYP3A5*1/*1(rs776746, AA) associated with lower tacrolimus blood levelswas also associated with an increased risk of acute GVHD(P¼ .04). However this association is based on only 8 patientsin the AA group, and although it is consistent with results
from the solid organ transplantation literature, it could be anartifact of the small sample size. In a previous study, we re-ported a significant association between day 14 sirolimusdrug levels and risk of TMA [8]; however, this analysis did notfind any association between ADME genetic polymorphismsand TMA. This is likely due to the relatively small sample sizeand other clinical variables influencing sirolimus drug levels.
In conclusion, our study indicates a statistically significantassociation of specific ADME genetic polymorphisms withelevated blood levels of tacrolimus and sirolimus when usedin combination as GVHD prophylaxis, in spite of vigilant TDMand dose adjustment. We also demonstrated an associationbetween ADME genetic polymorphisms and a post-HCTclinical outcome: acute GVHD. Whether these associationsare clinically meaningful in light of mitigating TDM is un-clear. We have undertaken a larger confirmatory study todetermine whether there is clinical utility for ADME-basedpersonalized dosing of immunosuppressive medications inHCT recipients.
ACKNOWLEDGMENTSFinancial disclosure: Agena Bioscience (Sequenom) pro-
vided the iPLEX ADME PGx Panel including reagents foranalysis of DNA samples and assistance with interpretationof the Admet report tables. This study utilized the City ofHope Cancer Center Biostatistics Core funded by NCI grantCA33572. This project was funded in part by the AmericanSociety of Blood and Marrow Transplantation New Investi-gator Award.
Authorship statement: S.K.K., R.N., J.M.P., and S.J.F.designed the study. J.H. performed assays and collected ge-netic data with oversight by J.W. D.S. collected and preparedDNA samples. S.S. collected drug dosing and drug level data.J.M.P., T.S., N.T., and X.L. performed data analysis. S.K.K., R.N.,J.M.P., and S.H.T. interpreted data and wrote the manuscript.All authors read and approved the final manuscript.
SUPPLEMENTARY DATASupplementary data related to this article can be found
online at 10.1016/j.bbmt.2015.08.027.
REFERENCES1. Baron F, Storb R. Allogeneic hematopoietic cell transplantation as
treatment for hematological malignancies: a review. Springer SeminImmunopathol. 2004;26:71-94.
2. Ferrara JL, Reddy P. Pathophysiology of graft-versus-host disease. SeminHematol. 2006;43:3-10.
3. Cutler C, Kim HT, Hochberg E, et al. Sirolimus and tacrolimus withoutmethotrexate as graft-versus-host disease prophylaxis after matchedrelated donor peripheral blood stem cell transplantation. Biol BloodMarrow Transplant. 2004;10:328-336.
4. Cutler C, Li S, Ho VT, et al. Extended follow-up of methotrexate-freeimmunosuppression using sirolimus and tacrolimus in related andunrelated donor peripheral blood stem cell transplantation. Blood.2007;109:3108-3114.
5. Rodriguez R, Nakamura R, Palmer JM, et al. A phase II pilot study oftacrolimus/sirolimus GVHD prophylaxis for sibling donor hematopoi-etic stem cell transplantation using 3 conditioning regimens. Blood.2010;115:1098-1105.
6. Pidala J, Kim J, Jim H, et al. A randomized phase II study to evaluatetacrolimus in combination with sirolimus or methotrexate after allo-geneic hematopoietic cell transplantation. Haematologica. 2012;97:1882-1889.
7. Cutler C, Logan B, Nakamura R, et al. Tacrolimus/sirolimus vs tacroli-mus/methotrexate as GVHD prophylaxis after matched, related donorallogeneic HCT. Blood. 2014;124:1372-1377.
8. Shayani S, Palmer J, Stiller T, et al. Thrombotic microangiopathy asso-ciated with sirolimus level after allogeneic hematopoietic cell trans-plantation with tacrolimus/sirolimus-based graft-versus-host diseaseprophylaxis. Biol Blood Marrow Transplant. 2013;19:298-304.
Table 5Multivariable Model for Acute GVHD
Factor No. ofaGVHDEvents
Hazard Ratio(95% CI)
P
rs776746 (CYP3A5)AA 8 7 referenceGA 40 20 .40 (.19-.86) .02GG 122 52 .32 (.16-.61) <.01
Reduced-intensityconditioning
No 72 39 referenceYes 98 40 .60 (.37-.98) .04
Donor typeMatched related donor 81 35 referenceMUD 89 44 1.26 (.77-2.06) .37
Age<46.8 86 40 reference"46.8 84 39 1.24 (.79-1.94) .35
Race/ethnicityWhite 90 40 referenceHispanic 51 25 .97 (.53-1.76) .92Asian 22 10 .88 (.43-1.80) .72Other 7 4 .80 (.27-2.35) .68
aGVHD indicates acute GVHD.Bold typeface indicates that the P value is #.05.
S.K. Khaled et al. / Biol Blood Marrow Transplant 22 (2016) 268e276 275
*1/*1*1/*3*3/*3

Khaled et al, 2016
tacrolimus/sirolimus blood levels. Although a relatively smallnumber of samples were used in this study, we were able toidentify multiple SNPs that could potentially influence theblood levels of tacrolimus and sirolimus.
Our study confirms the influence of rs776746 (CYP3A5*3)on tacrolimus blood levels in the post-HCT setting. rs776746(CYP3A5*3/*3) GG is a common polymorphism of CYP3A5
leading to a pre-mRNA splicing site alteration, which in turnleads to a nonfunctional enzyme that decreases the meta-bolism of substrate drugs including tacrolimus, resulting inincreased drug blood levels. In other words, patients withhaplotype CYP3A5*3 (nonexpressers) tend to have higherblood levels of tacrolimus at the same drug dose comparedwith those who express the CYP3A5*1 (wild-type) allele. This
Acu
te G
VH
DC
umul
ativ
e In
cide
nce
0.0
0.2
0.4
0.6
0.8
1.0
Time (Days) from Transplant0 10 20 30 40 50 60 70 80 90 100
rs776746 AA
rs776746 GA
rs776746 GG
rs776746 Days from Transplant 10 20 30 40 50 60 70 80 90 100AA (n=8) # of Events 2 3 4 5 5 5 6 7 7 7
# of Competing risk 0 0 0 0 0 0 0 0 1 1# of At risk 6 5 4 3 3 3 2 1 0 0
GA (n=40) # of Events 2 13 15 17 19 19 19 19 20 20# of Competing risk 0 1 2 2 5 5 6 6 6 6# of At risk 38 26 23 21 16 16 15 15 14 14
GG (n=122) # of Events 10 25 37 44 46 51 51 51 52 52# of Competing risk 1 2 3 4 7 9 9 9 10 11# of At risk 111 95 82 74 69 62 62 62 60 59
Figure 3. Cumulative incidence of acute GVHD stratified by CYP3A5 rs776746 genotypic variant. Cumulative incidence of grade II to IV acute graft-versus-host disease(GVHD) is plotted from day of transplantation stem cell infusion (day 0) with curves for each genotypic variant of rs776746. Solid line is AA variants (n ¼ 8), narrowdash is GA variant (40), and wide dash is GG variant (122) of rs776746 from CYP3A5 gene.
Table 4Cumulative Incidence of Acute GVHD by Gene Variant
Variants Acute GVHD Cumulative Incidence
Selected Genes SNP Genotypic Group* n No. of Events 100-Day Estimate 95% CI P
Genes of InterestABCB1 rs1045642 CC 54 24 44.4 30.8-57.2 .81
TT 41 18 43.9 28.2-58.4TC 76 35 46.1 34.4-56.8
rs1128503 CC 45 21 46.7 31.4-60.5 .98TT 45 21 46.7 31.4-60.5TC 78 36 46.2 34.7-56.8
rs2032582 AA/GG/GA 60 29 48.3 35.1-60.3 .67TT/TA/GT 110 50 45.5 35.9-54.4
rs3213619 CT 18 9 50.0 24.9-70.7 .77TT 154 70 45.5 37.4-53.1
CYP3A4 rs35599367 CC 161 76 47.2 39.2-54.6 .32CT 11 3 27.3 5.74-55.3TT 1 0 0.0 N/A
CYP3A5 rs776746 AA 8 7 87.5 17.2-98.9 .04GA 40 20 50.0 33.4-64.4GG 122 52 42.6 33.7-51.2
Additional GenesCYP2C19 rs12248560 CC 121 50 41.3 32.4-49.9 .04
CT 45 27 60.0 43.9-72.8TT 6 1 16.7 .47-54.8
VKORC1 rs7294 AA 15 9 60.0 30.0-80.5 .05GG 78 39 50.0 38.3-60.5GA 79 31 39.2 28.4-49.8
CI indicates confidence interval.Bold typeface indicates that the value is P value is " .05.
* Paired letters in the Genotypic Group column refer to the identity of the nucleotides at this position in the 2 gene alleles.
S.K. Khaled et al. / Biol Blood Marrow Transplant 22 (2016) 268e276274
*1/*1
*1/*3
*3/*3

ORIGINAL ARTICLE
Relationship between tacrolimus blood concentrations and clinical outcomeduring the first 4 weeks after SCT in children
N Watanabe1, K Matsumoto1, H Muramatsu2, K Horibe3, T Matsuyama4, S Kojima2 and K Kato1
1Division of Hematology and Oncology, Children’s Medical Center, Japanese Red Cross Nagoya First Hospital, Nagoya, Japan;2Department of Pediatrics, Nagoya University Graduate School of Medicine, Nagoya, Japan; 3Clinical Research Center, NationalHospital Organization Nagoya Medical Center, Nagoya, Japan and 4Nagoya Nishi Clinic Hospital, Nagoya, Japan
The relationship between tacrolimus concentration andacute GVHD is not well known, with few published dataavailable for lower target levels. We hypothesized thatlower levels of tacrolimus would correlate with higherincidence of acute GVHD and poorer prognosis. Receiveroperator characteristic curves (ROC) were used toquantify tacrolimus blood levels as predictors of gradeII–IV acute GVHD. A total of 97 pediatric patients withhematological malignancies met the study criteria. On theROC, a cutoff of 7 ng/ml provided the best balancebetween sensitivity and specificity (62.8 vs 68.2%,respectively). Cumulative incidence of acute GVHD was65.9% (range 58.5–73.3%) in patients with meantacrolimus concentration of p7 ng/ml and 34.8% (range27.8–41.8%) in patients with mean tacrolimus concentra-tion of 47 ng/ml (P¼ 0.002). Incidence of non-relapsemortality (NRM) was higher in patients with tacrolimusof p7 ng/ml (42.9%; range 35.6–50.2%) than in patientswith tacrolimus of 47 ng/ml (28.3%; range 17.4–39.2%;P¼ 0.008). This translated into better EFS in patientswith tacrolimus of 47 ng/ml (48.9%; range 39.8–58.0%)than in patients with tacrolimus of p7 ng/ml (31.8%;range 25.0–38.6%; P¼ 0.031). Multivariate analysisshowed that tacrolimus concentration was significantlyassociated with clinical outcomes. Mean whole-blood levelof tacrolimus as continuous infusion should be maintainedat X7 ng/ml for pediatric patients.Bone Marrow Transplantation (2010) 45, 1161–1166;doi:10.1038/bmt.2009.327; published online 16November 2009Keywords: tacrolimus; whole-blood levels; SCT
Introduction
The correlations of tacrolimus blood concentration withclinical efficacy and toxicity have been studied since the
introduction of tacrolimus into clinical use. Previousstudies have shown a sharp increase in nephrotoxicity forwhole-blood levels of 420 ng/ml. In one study, the risk forcreatinine 42mg/dl increased by 84.4% when meantacrolimus level was 420 ng/ml, compared with a meanlevel of p20 ng/ml.1 According to those results, tacrolimusconcentration should be kept at o20 ng/ml. However, noconsensus has been reached regarding the lower limits ofeffective tacrolimus concentration, as no clear relationshiphas been identified between blood concentration oftacrolimus and occurrence of acute GVHD. In particular,although Przepiorka et al.2 reported that tacrolimus levelsof o5 ng/ml were associated with an increased risk of acuteGVHD in adult patients, no reports have addressed thisissue in pediatric patients. We therefore analyzed therelationship between tacrolimus blood levels and clinicaloutcomes after SCT in 97 pediatric patients. Specialattention was given to analyzing the relationship betweenblood concentrations and occurrence of acute GVHD todetermine the lower target concentration of tacrolimus.
Patients and methods
PatientsThis retrospective study included 97 pediatric patients withhematological malignancies who received tacrolimus aspart of GVHD prophylaxis from December 1997 toSeptember 2007 at the Japanese Red Cross Nagoya FirstHospital. Treatment was approved by the institutionalreview board, and written informed consent was obtainedfrom the guardians of each patient. Patients were classifiedwith standard- or high-risk disease according to thepreviously described criteria.3 In brief, 49 patients werecategorized as standard risk, based on a diagnosis of ALL,AML or malignant lymphoma in the first or second CR.The remaining 48 patients, including 23 patients who hadreceived a second transplantation, were categorized as highrisk. Only eight patients received HLA-matched relateddonor grafts. All other patients received grafts fromalternative donors, including HLA-mismatched relateddonors, unrelated BM donors or unrelated cord blooddonors.
Received 22 June 2009; revised 1 October 2009; accepted 1 October 2009;published online 16 November 2009
Correspondence: Dr N Watanabe, Clinical Research Center, NationalHospital Organization Nagoya Medical Center, 4-1-1 Sannomaru,Naka-ku, Nagoya, Aichi 461-0001, Japan.E-mail: [email protected]
Bone Marrow Transplantation (2010) 45, 1161–1166& 2010 Macmillan Publishers Limited All rights reserved 0268-3369/10 $32.00
www.nature.com/bmt

Receiver operator characteristic analyses in this studyindicated that a cutoff value of 7 ng/ml resulted in the bestsensitivity and specificity for predicting the development ofacute GVHD. A mean blood level of tacrolimus p7 ng/mlwas identified as an independent risk factor for acuteGVHD, TRM, EFS and OS in multivariate analysis.Indeed, a 2.164-fold increase in grade II–IV GVHD wasobserved for tacrolimus levels of p7 ng/ml compared with47 ng/ml, using mean concentrations at 14 days after SCTand a 3.017-fold increase was observed at 28 days afterSCT. Maintaining mean blood levels of tacrolimus47ng/mlfor 28 days after SCT in continuous infusion may thus beimportant.A total of 21 patients stopped receiving tacrolimus
at o28 days after SCT because of various complications.The main reason for discontinuation of tacrolimus wasTAM, occurring in 11 patients. TAM can be a fatal
complication after SCT and immunosuppressants havebeen indicated as one of the causative agents for micro-angiopathy.6,7 To prevent deterioration of TAM, westopped administration of tacrolimus in patients who werediagnosed with TAM. Grade II–IV acute GVHD haddeveloped at the time of stopping the administrationof tacrolimus in all of these patients. In patients whostopped receiving tacrolimus at o28 days after SCT, meanwhole-blood level was 5.88±3.07 ng/ml, significantly lowerthan that of patients without early discontinuation. Wholetacrolimus level of p7 ng/ml at 14 days after SCTrepresented a significant risk factor for acute GVHD, eventhough the mean concentration in patients with earlycessation of tacrolimus was evaluated at a time point beforethe onset of acute GVHD or other complications. AcuteGVHD caused by lower blood levels of tacrolimus mightwell contribute to the development of TAM, as somereports have identified grade II–IV acute GVHD as one ofthe risk factors for TAM.8,9
Przepiorka et al.2 reported that a tacrolimus whole-bloodlevel of o5 ng/ml in the early post transplantation period issubtherapeutic, and dosages of tacrolimus should beadjusted to maintain whole-blood steady-state or troughlevels at 5–15 ng/ml. Since that report, a target rangemaintaining the level at 45 ng/ml has been recom-mended.10 We showed that mean whole-blood level oftacrolimus should be maintained at 47 ng/ml in contin-uous infusion for pediatric patients, as well as in adults.Wong et al.11 also insisted that the optimal range of bloodtacrolimus levels during the first 15 days would be 7–9 ng/ml in adult patients with refractory or relapsed myeloidleukemia.In a recent study using the new pharmacokinetic
parameter of area under the trough level, the calculatedtarget blood trough level for orally administered tacrolimuswas 0.71 times that for continuous infusion, which wasalmost equal to the clinical concentration for continuousinfusion.12 Blood trough levels of tacrolimus when admi-nistered orally should thus be maintained at X5 ng/ml, asour results suggest that mean whole-blood levelof tacrolimus should be maintained at X7 ng/ml whilereceiving continuous infusion.In summary, although little published data are available
regarding relationships between tacrolimus blood levelsand risk of GVHD, our study clearly showed thattacrolimus levels at p7 ng/ml with continuous infusionare significantly associated with an increased risk of acuteGVHD and lower survival, identifying 7 ng/ml as the lowerlimit of the therapeutic range.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
This work was supported by a grant from the Ministryof Health, Labour, and Welfare of Japan, Tokyo.
Table 4 Predictors of OS, EFS, NRM, relapse and acute GVHDby multivariate analysis, the Cox proportonal hazard model
RR 95.0% CI P-value
OSPatient age X8 years/o8 years 2.035 1.114 3.717 0.021X2nd SCT/first SCT 2.330 1.072 5.061 0.033HR/SR 2.623 1.244 5.533 0.011Reduced intensity/conventional 0.609 0.292 1.267 0.184HLA mismatch/match 2.075 1.168 3.686 0.013TAC p7 (ng/ml)/47 (ng/ml) day 14 2.240 1.198 4.190 0.012TAC p7 (ng/ml)/47 (ng/ml) day 28 4.146 2.216 7.757 o0.001
EFSPatient age X8 years/o8 years 1.713 0.972 3.018 0.062X2nd SCT/first SCT 1.209 0.616 2.372 0.582HR/SR 3.219 1.658 6.250 0.001HLA mismatch/match 1.952 1.123 3.395 0.018TAC p7 (ng/ml)/47 (ng/ml) day 14 1.859 1.044 3.312 0.035TAC p7 (ng/ml)/47 (ng/ml) day 28 2.815 1.639 4.836 0.005
NRMPatient age X8 years/o8 years 1.821 0.817 4.056 0.143X2nd SCT/first SCT 2.415 0.967 6.035 0.059HR/SR 1.479 0.579 3.783 0.414HLA mismatch/match 3.072 1.383 6.824 0.006TAC p7 (ng/ml)/47 (ng/ml) day 14 3.021 1.339 6.816 0.008TAC p7 (ng/ml)/47 (ng/ml) day 28 5.071 2.369 10.857 o0.001
RelapseHR/SR 3.684 1.593 8.519 0.002TAC p7 (ng/ml)/47 (ng/ml) day 14 1.174 0.543 2.537 0.683TAC p7 (ng/ml)/47 (ng/ml) day 28 0.895 0.385 2.080 0.797
Acute GVHD (II–IV)Donor sex F/M 1.560 0.685 3.555 0.290Female donor to male recipient/others 1.019 0.447 2.320 0.965HLA mismatch/match 1.396 0.752 2.591 0.291TAC p7 (ng/ml)/47 (ng/ml) day 14 2.164 1.128 4.153 0.020TAC p7 (ng/ml)/47 (ng/ml) day 28 3.017 1.619 5.624 o0.001
Acute GVHD (III–IV)X2nd SCT/first SCT 2.086 0.919 4.735 0.079Donor sex F/M 1.428 0.644 3.168 0.381HLA mismatch/match 1.400 0.653 3.002 0.387TAC p7 (ng/ml)/47 (ng/ml) day 14 3.228 1.399 7.451 0.006TAC p7 (ng/ml)/47 (ng/ml) day 28 4.445 2.039 9.690 0.005
Abbreviations: F¼ female; HR¼ high risk; M¼male; NRM¼ non-relapsemortality; SR¼ standard risk; TAC¼mean tacrolimus concentration.
Consequences of tacrolimus blood concentrationN Watanabe et al
1165
Bone Marrow Transplantation
Receiver operator characteristic analyses in this studyindicated that a cutoff value of 7 ng/ml resulted in the bestsensitivity and specificity for predicting the development ofacute GVHD. A mean blood level of tacrolimus p7 ng/mlwas identified as an independent risk factor for acuteGVHD, TRM, EFS and OS in multivariate analysis.Indeed, a 2.164-fold increase in grade II–IV GVHD wasobserved for tacrolimus levels of p7 ng/ml compared with47 ng/ml, using mean concentrations at 14 days after SCTand a 3.017-fold increase was observed at 28 days afterSCT. Maintaining mean blood levels of tacrolimus47ng/mlfor 28 days after SCT in continuous infusion may thus beimportant.
A total of 21 patients stopped receiving tacrolimusat o28 days after SCT because of various complications.The main reason for discontinuation of tacrolimus wasTAM, occurring in 11 patients. TAM can be a fatal
complication after SCT and immunosuppressants havebeen indicated as one of the causative agents for micro-angiopathy.6,7 To prevent deterioration of TAM, westopped administration of tacrolimus in patients who werediagnosed with TAM. Grade II–IV acute GVHD haddeveloped at the time of stopping the administrationof tacrolimus in all of these patients. In patients whostopped receiving tacrolimus at o28 days after SCT, meanwhole-blood level was 5.88±3.07 ng/ml, significantly lowerthan that of patients without early discontinuation. Wholetacrolimus level of p7 ng/ml at 14 days after SCTrepresented a significant risk factor for acute GVHD, eventhough the mean concentration in patients with earlycessation of tacrolimus was evaluated at a time point beforethe onset of acute GVHD or other complications. AcuteGVHD caused by lower blood levels of tacrolimus mightwell contribute to the development of TAM, as somereports have identified grade II–IV acute GVHD as one ofthe risk factors for TAM.8,9
Przepiorka et al.2 reported that a tacrolimus whole-bloodlevel of o5 ng/ml in the early post transplantation period issubtherapeutic, and dosages of tacrolimus should beadjusted to maintain whole-blood steady-state or troughlevels at 5–15 ng/ml. Since that report, a target rangemaintaining the level at 45 ng/ml has been recom-mended.10 We showed that mean whole-blood level oftacrolimus should be maintained at 47 ng/ml in contin-uous infusion for pediatric patients, as well as in adults.Wong et al.11 also insisted that the optimal range of bloodtacrolimus levels during the first 15 days would be 7–9 ng/ml in adult patients with refractory or relapsed myeloidleukemia.
In a recent study using the new pharmacokineticparameter of area under the trough level, the calculatedtarget blood trough level for orally administered tacrolimuswas 0.71 times that for continuous infusion, which wasalmost equal to the clinical concentration for continuousinfusion.12 Blood trough levels of tacrolimus when admi-nistered orally should thus be maintained at X5 ng/ml, asour results suggest that mean whole-blood levelof tacrolimus should be maintained at X7 ng/ml whilereceiving continuous infusion.
In summary, although little published data are availableregarding relationships between tacrolimus blood levelsand risk of GVHD, our study clearly showed thattacrolimus levels at p7 ng/ml with continuous infusionare significantly associated with an increased risk of acuteGVHD and lower survival, identifying 7 ng/ml as the lowerlimit of the therapeutic range.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
This work was supported by a grant from the Ministryof Health, Labour, and Welfare of Japan, Tokyo.
Table 4 Predictors of OS, EFS, NRM, relapse and acute GVHDby multivariate analysis, the Cox proportonal hazard model
RR 95.0% CI P-value
OSPatient age X8 years/o8 years 2.035 1.114 3.717 0.021X2nd SCT/first SCT 2.330 1.072 5.061 0.033HR/SR 2.623 1.244 5.533 0.011Reduced intensity/conventional 0.609 0.292 1.267 0.184HLA mismatch/match 2.075 1.168 3.686 0.013TAC p7 (ng/ml)/47 (ng/ml) day 14 2.240 1.198 4.190 0.012TAC p7 (ng/ml)/47 (ng/ml) day 28 4.146 2.216 7.757 o0.001
EFSPatient age X8 years/o8 years 1.713 0.972 3.018 0.062X2nd SCT/first SCT 1.209 0.616 2.372 0.582HR/SR 3.219 1.658 6.250 0.001HLA mismatch/match 1.952 1.123 3.395 0.018TAC p7 (ng/ml)/47 (ng/ml) day 14 1.859 1.044 3.312 0.035TAC p7 (ng/ml)/47 (ng/ml) day 28 2.815 1.639 4.836 0.005
NRMPatient age X8 years/o8 years 1.821 0.817 4.056 0.143X2nd SCT/first SCT 2.415 0.967 6.035 0.059HR/SR 1.479 0.579 3.783 0.414HLA mismatch/match 3.072 1.383 6.824 0.006TAC p7 (ng/ml)/47 (ng/ml) day 14 3.021 1.339 6.816 0.008TAC p7 (ng/ml)/47 (ng/ml) day 28 5.071 2.369 10.857 o0.001
RelapseHR/SR 3.684 1.593 8.519 0.002TAC p7 (ng/ml)/47 (ng/ml) day 14 1.174 0.543 2.537 0.683TAC p7 (ng/ml)/47 (ng/ml) day 28 0.895 0.385 2.080 0.797
Acute GVHD (II–IV)Donor sex F/M 1.560 0.685 3.555 0.290Female donor to male recipient/others 1.019 0.447 2.320 0.965HLA mismatch/match 1.396 0.752 2.591 0.291TAC p7 (ng/ml)/47 (ng/ml) day 14 2.164 1.128 4.153 0.020TAC p7 (ng/ml)/47 (ng/ml) day 28 3.017 1.619 5.624 o0.001
Acute GVHD (III–IV)X2nd SCT/first SCT 2.086 0.919 4.735 0.079Donor sex F/M 1.428 0.644 3.168 0.381HLA mismatch/match 1.400 0.653 3.002 0.387TAC p7 (ng/ml)/47 (ng/ml) day 14 3.228 1.399 7.451 0.006TAC p7 (ng/ml)/47 (ng/ml) day 28 4.445 2.039 9.690 0.005
Abbreviations: F¼ female; HR¼ high risk; M¼male; NRM¼ non-relapsemortality; SR¼ standard risk; TAC¼mean tacrolimus concentration.
Consequences of tacrolimus blood concentrationN Watanabe et al
1165
Bone Marrow Transplantation
Watanabe et al, 2016

Clinical Research: Pediatric
Genotype-Directed Dosing Leads to Optimized VoriconazoleLevels in Pediatric Patients Receiving Hematopoietic StemCell Transplantation
Ashley Teusink 1,*, Alexander Vinks 2, Kejian Zhang 3, Stella Davies 4, Tsuyoshi Fukuda 2,Adam Lane 4, Shannon Nortman 3, Diane Kissell 3, Sarah Dell 3, Alexandra Filipovich 4,Parinda Mehta 4
1Division of Pharmacy, Cincinnati Children’s Hospital Medical Center, Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio2Division of Clinical Pharmacology, Cincinnati Children’s Hospital Medical Center, Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati,Ohio3Division of Human Genetics, Cincinnati Children’s Hospital Medical Center, Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio4Division of Bone Marrow Transplantation and Immune Deficiency, Cincinnati Children’s Hospital Medical Center, Department of Pediatrics, University of CincinnatiCollege of Medicine, Cincinnati, Ohio
Article history:Received 23 July 2015Accepted 17 November 2015
Key Words:PharmacogeneticsVoriconazoleHematopoietic stem celltransplant
a b s t r a c tInvasive fungal infections are a significant cause of morbidity and mortality in recipients of hematopoieticstem cell transplantation (HSCT), warranting antifungal prophylaxis as a standard of care in these patients.Voriconazole is commonly used in this setting because of its broad-spectrum activity and available dosageforms. There is wide well-known inter- and intrapatient variability in voriconazole concentrations, in partbecause concentrations are affected by common CYP2C19 polymorphisms. In 2 successive studies we haveoptimized voriconazole dosing to achieve target voriconazole serum concentrations using a genotype-specificdosing algorithm for antifungal prophylaxis in the post-HSCT period. In our pilot study all patients undergoingHSCT who received voriconazole antifungal prophylaxis were prospectively followed. Voriconazole concen-trations were monitored weekly and doses adjusted until concentrations reached between 1 and 5.5 mg/L. Themost common CYP2C19 polymorphisms were determined and correlated with voriconazole dose and timerequired to reach the target concentration range. In the subsequent study patients receiving voriconazoleprophylaxis were dosed based on their CYP2C19 genotype and followed prospectively. In the pilot study 25patients received voriconazole as antifungal prophylaxis for a median of 49 days (range, 15 to 196 days). Themedian time to reach the target concentration was 34 days for extensive metabolizers and 11 days for poormetabolizers. Three patients were genotyped as intermediate metabolizers; they reached the target concen-tration in amedian of 56 days. Similarly, 2 patients whowere genotyped as ultrarapidmetabolizers reached thetarget range in 18 and 25 days. The time and dose required to reach the adequate concentration showed a trendtoward correlation with individual CYP2C19 genotype, although voriconazole concentrations showed largeinterpatient variability in wild-type patients (extensive metabolizers). In our follow-up study, 20 patientsreceived voriconazole prophylaxis prospectively dosed based on their CYP2C19 genotype. The median times toreach the target concentration using genotype-guided dosing were 9, 6.5, and 4 days for ultrarapid, extensive,and intermediate metabolizers, respectively. Overall, the median time to reach the target concentration withgenotype-guided dosing was 6.5 days compared with a median time of 29 days when all patients were startedon the same dose regardless of CYP2C19 genotype (P< .001). Our data show that traditional voriconazole dosingdoes not lead to timely achievement of target levels for fungal prophylaxis. However, a genotype-directeddosing algorithm allows patients to reach the voriconazole target range significantly sooner, providing betterprophylaxis against fungal infections in the immediate post-transplant period.
! 2016 American Society for Blood and Marrow Transplantation.
INTRODUCTIONDisseminated fungal infections cause significant
morbidity and mortality in immunocompromised children.Children with leukemia (eg, acute myelogenous leukemia,
Financial Disclosure: See Acknowledgments on page 486.* Correspondence and reprint request: Dr. Ashley Teusink, Cincinnati
Children’s Hospital Medical Center, 3333 Burnet Ave, Cincinnati, OH 45229.E-mail address: [email protected] (A. Teusink).
http://dx.doi.org/10.1016/j.bbmt.2015.11.0111083-8791/! 2016 American Society for Blood and Marrow Transplantation.
Biol Blood Marrow Transplant 22 (2016) 482e486
Biology of Blood andMarrow Transplantationjournal homepage: www.bbmt.org

Teusink et al, 2016
than standard dosing (29 days) for all patients; this differ-ence was statistically significant (P < .001) (Figure 1).
In terms of safety and adverse effects, 1 patient hadelevation of LFTs (greater than 3 times the upper limit ofnormal). No patients experienced neurotoxicity. There was 1breakthrough Rhizopus infection in this follow-up study(Table 2).
DISCUSSIONVoriconazole is a broad-spectrum antifungal agent with
activity against Aspergillus and non-Aspergillus moldinfections as well as activity against many Candida species. Itis well established that successful outcomes in both thetreatment and prevention of fungal infections have beenassociatedwith sustained voriconazole concentrations abovethe minimum inhibitory concentration for the organism.Trifilio et al. [8] described their experience with 71 HSCTrecipients receiving voriconazole prophylaxis. A total of 10breakthrough fungal infections were seen in patients onvoriconazole prophylaxis. Six of the 10 patients developedcandidiasis and 4 experienced zygomycosis. In 5 of 6 patientswith candidiasis, voriconazole trough concentrations werebelow 1 mg/mL. Smith et al. [9] reported 17 patients withinvasive aspergillosis who were not improving clinicallydespite voriconazole treatment. In this cohort, all patientswith voriconazole trough concentration of greater than 2 mg/mL survived, whereas only 50% of those with concentrationsof less than 2 mg/mL survived, emphasizing the importance oftherapeutic drug monitoring when using voriconazole forprophylaxis and/or treatment.
Several studies show that voriconazole adverse effects aredose related and associated with trough concentrationsexceeding 6 mg/mL [8-11]. High trough concentrations ofvoriconazole have been linked to visual disturbances,including altered visual perception, blurred vision, colorvision changes, and photophobia. Additionally, neurologicside effects (encephalopathy, hallucinations, peripheralneuropathy, and anxiety) and alterations in LFTs (hepatitisand jaundice) have also been described.
Based on previous reports, the target range for vor-iconazole trough concentrations for prophylaxis is between 1and 5.5 mg/mL, and the desired range for treatment of fungaldisease is between 2 and 5.5 mg/mL [8,9]. This classifiesvoriconazole as a drug with a narrow therapeutic window.This classification combined with a great deal of unpredict-ability and wide inter- and intrapatient variability empha-sizes the importance of therapeutic drug monitoring inpatients receiving voriconazole.
Voriconazole is cleared by hepatic metabolism primarilyby the CYP2C19 pathway. Functional genetic polymorphismsof CYP2C19, such as CYP2C19*2, *3, and *17, have beenreported to result in either increased (*17) or decreased (*2and *3) metabolic activity [10,11]. It is believed that thesepolymorphisms could play an important role in the largeinterpatient variability [10,11], and therefore patients shouldbe dosed based on their CYP2C19 genotype to ensure thetarget range is reached as quickly as possible. The resultsfrom our pilot study showed a significant difference in dosesrequired and the time required to achieve the desired troughconcentrations for different CYP2C19 genotypes, furthersupporting the idea that patients may need different initialdosing based on their CYP2C19 genotype. These observationsare in agreement with other studies suggesting higher initialdosing in children based on therapeutic drug monitoring orCYP genotyping [15,16]. However, the most concerningfinding from our pilot study was the median time of 29 days(range, 3 to 65) that intermediate and extensivemetabolizersneeded to achieve the desired trough concentration, leavingthese high-risk patients vulnerable to invasive fungalinfections during the critical early post-transplantneutropenic period. Based on the pilot study results, wedeveloped a dosing algorithm according to individualCYP2C19 genotype. By prospectively validating the algorithm,we showed a statistically significant decrease in time totarget voriconazole concentration from 29 to 6.5 days.Although there was no statistically significant difference inthe number of breakthrough fungal infections, because thenumber of events was small, these results are still compellingand clinically relevant.
In our studies 2 patients had 1 level each that were abovethe desired target range. Of note, both supratherapeutictroughs were seen in patients included in the initial pilotstudy compared with none in the genotype-directed dosingstudy. Similarly, in contrast to our pilot study, where 5patients had elevated liver enzymes, only 1 patient in thegenotype-directed dosing study experienced elevations inLFTs, which may or may not have been related to vor-iconazole, as his voriconazole trough concentrations werebelow the target range at the time of liver enzyme elevation.Additionally, this patient remained on voriconazole therapyand LFTs returned to baseline within next 9 days, suggestinga probable alternate cause for liver enzyme elevation.
In conclusion, our studies demonstrate the value ofCYP2C19 genotyping in selecting appropriate initial vor-iconazole dosage for pediatric patients undergoing HSCT.These data also emphasize the need and value of an effectivetherapeutic drug monitoring strategy for this high-riskpatient population to reach the target serum voriconazoleconcentrations in a timely manner. Our hospital, CCHMC, hascontinued to use the algorithm described in the prospectivestudy to direct our voriconazole therapy with great success.It should be mentioned that CYP2C19 genotyping andvoriconazole concentration monitoring are both routinelyperformed at CCHMC laboratory facilities. At CCHMC, the
Figure 1. Time to target voriconazole concentration for the pilot and pro-spective genotype-directed studies.
A. Teusink et al. / Biol Blood Marrow Transplant 22 (2016) 482e486 485

RESEARCH ARTICLE
The Impact of MethylenetetrahydrofolateReductase C677T Polymorphism on PatientsUndergoing Allogeneic Hematopoietic StemCell Transplantation with MethotrexateProphylaxisJa Min Byun1☯, Hea-Lim Kim2☯, Dong-Yeop Shin1,3, Youngil Koh1,3, Sung-Soo Yoon1,3,Moon-Woo Seong4, Sung Sup Park4, Jin Hee Kim5, Yun-Gyoo Lee6*, Inho Kim1,3*
1 Department of Internal Medicine, Seoul National University College of Medicine, Seoul National UniversityHospital, Seoul, Korea, 2 Graduate School of Public Health, Seoul National University, Seoul, Korea,3 Cancer Research Institute, Seoul National University, Seoul, Korea, 4 Department of LaboratoryMedicine, Seoul National University Hospital, Seoul, Korea, 5 Department of Integrative Bioscience andBiotechnology, Sejong University, Seoul, Korea, 6 Department of Internal Medicine, Kangbuk SamsungHospital, Sungkyunkwan University School of Medicine, Seoul, Korea
☯ These authors contributed equally to this work.* [email protected] (IK); [email protected] (Y-GL)
Abstract
Pharmacogenomics can explain the inter-individual differences in response to drugs,
including methotrexate (MTX) used for acute graft-versus-host disease (aGVHD) prophy-
laxis during hematopoietic stem cell transplantation (HSCT). In real-world practice, pre-
planned MTX dose is arbitrarily modified according to observed toxicity which can lead to
unexpected and severe aGVHD development. We aimed to validate the influence of
MTHFR C677T polymorphism on the outcomes of allogenic HSCT in a relatively under-rep-
resented homogenous Asian population. A total of 177 patients were divided into 677TT
group versus 677C-carriers (677CT+677CC), and clinical outcomes along with baseline
characteristics were analyzed and compared. Although there was a tendency towards
increased peak liver function test results and accordingly greater delta values between the
highest and the baseline in 677TT group, we found no associations between genotypes
and hepatotoxicity. However, the incidence of acute liver GVHD (� grade 2) was signifi-
cantly higher in the 677TT group than in the 677CC + 677CT group (P = 0.016). A total of
25 patients (14.1%) expired due to transplantation related mortality (TRM) during the first
180 days after HSCT. Patients carrying 677TT genotype were more likely to experience
early TRM than 677C-carriers. The same pattern was observed in the cumulative TRM
rate, and 677TT genotype patients were more prone to cumulative TRM (P = 0.010). This
translated into shorter OS for patients with 677TT compared to 677C-carriers (P = 0.010).
The 3-year survival after HSCT was 29.9% for 677TT cases and 47.1% for 677C-carriers.
The multivariate analysis identified 677TT genotype (HR = 1.775. 95% CI 1.122–2.808, P =
0.014) and non-CR state (HR = 2.841. 95% CI 1.627–4.960, P<0.001) as predictors for
PLOS ONE | DOI:10.1371/journal.pone.0163998 October 26, 2016 1 / 11
a11111
OPENACCESS
Citation: Byun JM, Kim H-L, Shin D-Y, Koh Y,Yoon S-S, Seong M-W, et al. (2016) The Impact ofMethylenetetrahydrofolate Reductase C677TPolymorphism on Patients Undergoing AllogeneicHematopoietic Stem Cell Transplantation withMethotrexate Prophylaxis. PLoS ONE 11(10):e0163998. doi:10.1371/journal.pone.0163998
Editor: Masaru Katoh, National Cancer Center,JAPAN
Received: June 14, 2016
Accepted: September 19, 2016
Published: October 26, 2016
Copyright:© 2016 Byun et al. This is an openaccess article distributed under the terms of theCreative Commons Attribution License, whichpermits unrestricted use, distribution, andreproduction in any medium, provided the originalauthor and source are credited.
Data Availability Statement: All relevant data arewithin the paper and its Supporting Informationfiles.
Funding: This research was supported by BasicScience Research Program through the NationalResearch Foundation of Korea (NRF) funded by theMinistry of Education (NRF-2016-0024046, NRF-2011-0024046).
Competing Interests: The authors have declaredthat no competing interests exist.
serum measurements total bilirubin, aspartic transaminase (AST), alanine transaminase(ALT), and alkaline phosphatase (ALP). The baseline liver function levels, peak level and dif-ferences between highest and baseline were taken into consideration. Veno-occlusive disease(VOD) was diagnosed based on development of hepatomegaly, weight gain and jaundice asdescribed elsewhere [14]. Clinical outcomes measured included veno-occlusive disease (VOD),acute GVHD, transplantation-related mortality (TRM), chronic GVHD, relapse free survival(RFS) and overall survival (OS). Acute GVHD (aGVHD) was graded from 0 to 4 according topublished data [15] from day 1 after HSCT, while chronic GVHD (cGVHD) was evaluated inpatients who survived with sustained engraftment from day 100 after HSCT [16]. TRM wascalculated from the time of transplantation to death related to transplant without relapse. EarlyTRM was calculated at day 180 after HSCT. OS was defined as the time from the date of HSCTto death of any cause while RFS was derived from the date of HSCT to that of relapse or deathfrom any cause.
Statistical analysis
The primary outcome of interest of this study was the development of MTX related toxicity inpatients with different polymorphism status. By univariate analysis, odds ratios (OR) and 95%confidence intervals (95% CI) were used to estimate the risk of developing toxicity. By multivari-ate logistic regression analysis, adjusted OR were calculated, with the dependent variable beingspecific toxicity per involved site. The multivariate model included sex, age, primary diagnosis,conditioning regimen, donor status and the MTHFR polymorphisms as covariates and they werechecked for possible interaction or confounding effects. If a covariate had an effect of 10% ormore, then it was considered a confounding factor and the model was adjusted for it.
Univariate and multivariate proportional hazards regression models were used to identifyindependent risk factors of overall survival and treatment-related mortality by means of log-rank tests and Cox proportional hazards models, respectively. The survival curves were esti-mated using the Kaplan-Meier method. A stepwise backward procedure was used to constructa set of independent predictors of each end points. All predictors achieving a P value below0.10 were considered, and sequentially removed if the P value in the multiple model was above0.05. Differences between groups were assessed using a Student’s t-test or one-way analysis ofvariance for continuous variables, and Pearson chi-square test for categorical variables, as indi-cated. All data were analyzed using the Statistical Package for the Social Sciences software(IBM1 SPSS1 Statistics, version 22.0). P values of < 0.05 were considered statisticallysignificant.
Results
Patient characteristics
The baseline characteristics of 177 Korean patients enrolled are described in Table 1. The fre-quency of MTHFR genotypes in decreasing order is as follows: 46.3% (82/177) for 677CT,32.2% (57/177) for 677CC, and 21.5% (38/177) for 677TT. The mean age at HSCT was 37.8±12.5 years old, and there were more males (108, 61%) in the total cohort. Acute myeloid leuke-mia was the most common etiology (87, 49.2%) and acute leukemias including blast crisis ofchronic myeloid leukemia constituted 90.4% (160/177) of the cohort.
Liver toxicity and graft-versus-host disease
The results of serum liver function test results are presented in Table 2. There were no associa-tions between differences in the baseline liver function between the groups. Although the peak
MTHFR C677T Polymorphism and Methotrexate Toxicity
PLOS ONE | DOI:10.1371/journal.pone.0163998 October 26, 2016 3 / 11

Overall survival according to MTHFR C677T genotype (P = 0.036)
Byun et al, 2016

Patient Information CardThis is a summary genetic report for your patient to share with other healthcare providers. The card can be cut out along the dashed line and carried with the patient.
Apolipoprotein E ε3/ε3 Normal APOE function
COMT Val158Met A/G Intermediate COMT Activity
CYP1A2 *1A/*1J Normal Metabolizer- Possible Inducibility
CYP2B6 *1/*1 Normal MetabolizerCYP2C19 *1/*1 Normal MetabolizerCYP2C9 *1/*1 Normal MetabolizerCYP2D6 *1/*1 Normal MetabolizerCYP3A4 *1B/*22 Intermediate MetabolizerCYP3A5 *3/*3 Poor MetabolizerFactor II 20210G>A GG Normal Thrombosis RiskFactor V Leiden 1691G>A GG Normal Thrombosis RiskMTHFR 677C>T CT Reduced MTHFR ActivityMTHFR 1298A>C AC Reduced MTHFR ActivitySLCO1B1 521T>C T/T Normal FunctionVKORC1 -1639G>A A/A High Warfarin Sensitivity
Pharmacogenetic Test Summary
Name: Patient TILAB3
ACC #:DOB:
REPORT DETAILS
1/1/1900TILAB3
For a complete report contact Baylor University Medical Center
DO NOT DISTRIBUTE
PATIENT INFORMATION
NAME: Patient TILAB3
DOB: 1/1/1900SEX:
ACC #: TILAB3
Genetic Test Results For Patient TILAB3Page 11 of 11Lab Director: Medhat Askar, M.D., Ph.D. | CLIA: 45D0051832 | 3500 Gaston Avenue, 4th Floor, Y Wing, Room L-0470, Dallas, TX 75246 | | 214.820.2119



Very Convincing!
Ø Right?

but it does not provide a recommendation on whether to testpatients preemptively (48,49).
Growing Evidence for Diabetes TreatmentsDiabetic nephropathy is a leading cause for CKD and
ESKD (55). As such, nephrologists treat many patients withcomorbid type 2 diabetes mellitus who are managed onmetformin. Although there are no clinical guidelines for theuse of pharmacogenomics to tailor therapy with metformin,evidence has been growing that supports the use of the SNPrs11212617 in an intergenic (nongene) region of the genome
called the chromosome 11 open reading frame 65 region. At thisSNP, the presence of at least one “A” allele is associated withdecreased response to metformin (56). In the future, thisvariation or others affecting pharmacokinetics (e.g., transporters)may be useful for predicting which patients will require altereddoses of metformin for adequate hemoglobin A1c control.
Clinical Decision Making and the Use ofPharmacogenomics in PracticeSeveral barriers prevent more widespread pharmacoge-
nomics clinical implementation in everyday practice
Figure 4. | Pharmacogenomics implementation is limited by challenges in testing, informatics, clinical constraints, lack of education, andELSI. ELSI, ethical, legal, and social implications.
Clin J Am Soc Nephrol 13: 1561–1571, October, 2018 Pharmacogenomics in Nephrology, Adams et al. 1567
Adam
s et
al,
2018
Bar
riers

Summary• PGx testing yields clinically
actionable results that are conducive to the practice of precision medicine
• Nephrologists are well positioned to leverage PGx in managing patients with significant comorbidities