Preauriculer Sinuses
3
Indian Journal of Otolaryngology and Head and Neck Surgery Vol. 58, No. 1, January-March 2006 6 Main Article ABSTRACT: A retrospective review of preauricular sinuses operated in Sundaram Medical Foundation, a 140-bedded tertiary care hospital during the period 1995 to 2000 is presented. Patients were operated six to eight weeks after control of infection. Magnification with an operating microscope was always used. A team of ENT and Plastic surgeons was involved in all the cases. Involvement of a Plastic and Reconstructive surgeon permitted primary closure after surgery without any drains, individualised incisions in every patient, and early discharge from hospital. A follow up of all operated patients for a period of 18 months revealed good results without any recurrence. Key Words: Preauricular sinus, microscope, plastic surgeon, primary closure PREAURICULAR SINUS: OPERATING MICROSCOPE IMPROVES OUTCOME Krishna K. Kumar, V. B. Narayanamurthy*, V. Sumathi, R. Vijay Department of Otorhinolaryngology and *Plastic surgery, Sundaram Medical Foundation, IV Avenue, Shanthi Colony, Anna Nagar, Chennai-600040, India INTRODUCTION Patients with preauricular sinuses present to the clinician with persistent discharge, recurrent infections or recurrence after surgery. Surgery has always been regarded as the treatment of choice. Ancillary methods, adopted to improve success rates, include probing and methylene blue injection, diathermy cauterization and excision followed by secondary healing. The objective of this study is to analyze our methods and results with preauricular sinus excisions. Background Lau JT (1983) have shown that preoperative injection of methylene blue into the tract followed by purse-string closure of the orifice, 3 days prior to surgery, together with addition of a posterior drain, improves outcome. If complete excision of the gland and duct is done, the recurrence rate should be substantially reduced. Joseph V T and Jacobsen A S (1995) have reported recurrences due to incomplete excision of the gland. Lam H C and colleagues (2001) have shown that the supraauricular approach for excision of a preauricular sinus has a statistically lower recurrence rate in comparison with sinectomy. Surgery done in the presence of infection results in higher recurrence. Gur E and co-workers (1998) have reported a recurrence of 8.22% without any infection as compared to 15.79% in patients with active infection present at surgery. Use of blunt probing and injection of methylene blue dye simultaneously to delineate the sinus ramifications have resulted in no postoperative recurrence as reported by Gur E and co-workers (1998). Currie A R and colleagues (1996) have shown that previous history of excision, the use of a probe to delineate the sinus and operating under local anaesthesia all increase the chances of recurrence. Postoperative wound asepsis is also mandatory to facilitate good healing without recurrence. Currie A R and colleagues (1996) have reported higher recurrence in patients who developed postoperative wound sepsis. Results are always better in primary preauricular sinus excisions. Ellie M and co-workers (1998) have reported a recurrence rate of 14% in first operations and 42% in patients operated for a recurrence. MATERIALS AND METHODS The hospital medical records of all nine patients operated for a preauricular sinus in our hospital during the period 1995 to 2000 were studied. Details of the patients are given in [Table 1]. Method Infection is controlled and a period of 6 weeks allowed before surgery is undertaken. [Table 1] gives the details of the antibiotics used. Co-amoxiclav is the preferred antibiotic but Ciprofloxacin was used in patients with proven sensitivity patterns. General anaesthesia was used in all cases. The team
-
Upload
andri-wijaya -
Category
Documents
-
view
10 -
download
0
description
Jurnal of otology, desrciption of preauriculer sinus in children, how to make diagnosis and treatment
Transcript of Preauriculer Sinuses

Indian Journal of Otolaryngology and Head and Neck Surgery Vol. 58, No. 1, January-March 2006
6
Main Article
ABSTRACT: A retrospective review of preauricular sinuses operated in Sundaram Medical Foundation,
a 140-bedded tertiary care hospital during the period 1995 to 2000 is presented. Patients were operated
six to eight weeks after control of infection. Magnification with an operating microscope was alwaysused. A team of ENT and Plastic surgeons was involved in all the cases. Involvement of a Plastic and
Reconstructive surgeon permitted primary closure after surgery without any drains, individualised
incisions in every patient, and early discharge from hospital. A follow up of all operated patients for aperiod of 18 months revealed good results without any recurrence.
Key Words: Preauricular sinus, microscope, plastic surgeon, primary closure
PREAURICULAR SINUS: OPERATING MICROSCOPEIMPROVES OUTCOME
Krishna K. Kumar, V. B. Narayanamurthy*, V. Sumathi, R. Vijay
Department of Otorhinolaryngology and *Plastic surgery, Sundaram Medical Foundation, IV Avenue, Shanthi Colony, Anna Nagar, Chennai-600040, India
INTRODUCTIONPatients with preauricular sinuses present to the clinician withpersistent discharge, recurrent infections or recurrence aftersurgery. Surgery has always been regarded as the treatmentof choice. Ancillary methods, adopted to improve successrates, include probing and methylene blue injection, diathermycauterization and excision followed by secondary healing. Theobjective of this study is to analyze our methods and resultswith preauricular sinus excisions.
BackgroundLau JT (1983) have shown that preoperative injection ofmethylene blue into the tract followed by purse-string closureof the orifice, 3 days prior to surgery, together with additionof a posterior drain, improves outcome. If complete excisionof the gland and duct is done, the recurrence rate should besubstantially reduced. Joseph V T and Jacobsen A S (1995)have reported recurrences due to incomplete excision of thegland.
Lam H C and colleagues (2001) have shown that thesupraauricular approach for excision of a preauricular sinushas a statistically lower recurrence rate in comparison withsinectomy. Surgery done in the presence of infection resultsin higher recurrence.
Gur E and co-workers (1998) have reported a recurrence of8.22% without any infection as compared to 15.79% inpatients with active infection present at surgery. Use of blunt
probing and injection of methylene blue dye simultaneouslyto delineate the sinus ramifications have resulted in nopostoperative recurrence as reported by Gur E and co-workers(1998).
Currie A R and colleagues (1996) have shown that previoushistory of excision, the use of a probe to delineate the sinusand operating under local anaesthesia all increase the chancesof recurrence. Postoperative wound asepsis is also mandatoryto facilitate good healing without recurrence. Currie A R andcolleagues (1996) have reported higher recurrence in patientswho developed postoperative wound sepsis. Results arealways better in primary preauricular sinus excisions. EllieM and co-workers (1998) have reported a recurrence rate of14% in first operations and 42% in patients operated for arecurrence.
MATERIALS AND METHODSThe hospital medical records of all nine patients operated fora preauricular sinus in our hospital during the period 1995 to2000 were studied. Details of the patients are given in [Table1].
MethodInfection is controlled and a period of 6 weeks allowed beforesurgery is undertaken. [Table 1] gives the details of theantibiotics used. Co-amoxiclav is the preferred antibiotic butCiprofloxacin was used in patients with proven sensitivitypatterns. General anaesthesia was used in all cases. The team

Indian Journal of Otolaryngology and Head and Neck Surgery Vol. 58, No. 1, January-March 2006
7Preauricular sinus
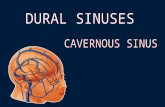
of ENT and Plastic surgeons jointly operated all cases. Gentleprobing with a blunt ended malleable probe is done first todelineate the extent and presence of multiple ramifications.[Figure 1] Local infiltration of 2% lignocaine and adrenalinearound the delineated area is done. An elliptical incisionincluding the sinus opening was used. A zigzag incision wasused where multiple openings were present, to give maximumexposure. Magnification with an operating microscope,bipolar dissecting forceps and local infiltration of adrenalineprovides a bloodless field. All ramifications could bemeticulously dissected and excised in Toto [Figure 1]. Asmeticulous haemostasis is always attained, no drain is usedand primary closure is done.
RESULTSNine patients were operated, of which 5 were females. Sevenof them were less than 21 years, one of them was 68 years
old. Sinuses were more common on the left[5] than on theright,[3] one of them was bilateral with more discharge on theleft side. Eight of our patients were primary preauricular sinusexcisions while 1 had undergone a previous sinus incisionand drainage outside. Sinus tracts were single in 7 patientsand multiple in 2. All patients were followed up for a minimumperiod of 18 months, the longest being 36 months.
None of the operated patients have had a postoperativerecurrence to date.
DISCUSSIONA preauricular sinus is a congenital anomaly. It may be aninclusion dermoid resulting from epithelium trapped betweenthe developing auricular tubercles or it may be a remnant offirst branchial groove epithelium, which has failed to resorb.Recurrence in preauricular sinus excision is due to incompleteexcision of the sinus tract and presence of residual viablesquamous epithelium. Recurrence can manifest in the formof persistence of sepsis, resurgence of swelling, repeated sinusdischarge or recurrence of a preauricular mass. However, inour series, we have had extremely gratifying results withouta single recurrence in any of the nine patients operated so far.
General anaesthesia is preferred to ensure patient co-operation.Magnification with an operating microscope enables precisedissection without any epithelial breach. Copious localinfiltration with adrenaline facilitates a bloodless field for thesurgeon, making dissection more easy and fruitful. Blunt metalprobing to delineate the sinus ramifications, should be gentleand meticulous to avoid the creation of new false passages.Bipolar diathermy cauterization and use of diathermy
Table 1: Patient profile
S. No. Age Sex Presentation Unilateral/ Primary/ Antibiotics Followbilateral recurrent up
1 20 F Discharge Right Primary Co-Amoxiclav 18 months
2 68 M Discharge and pain Left Primary Co-Amoxiclav 18 months
3 29 F Discharge Left Primary Co-Amoxiclav 18 months
4 9 F Swelling and Discharge, Left Primary Co-Amoxiclav 24 months
Multiple tract sinus5 8 M Discharge Left Primary Co-Amoxiclav 24 months
6 16 M Bilateral discharge L > R, Bilateral Primary Ciprofloxacin 24 months
Multiple tract sinus7 15 F Discharge and pain Right Recurrent Ciprofloxacin 24 months
8 5 F Discharge and swelling Left Primary Co-Amoxiclav 36 months
9 5 M Swelling and discharge Right Primary Cloxacillin 36 months
Figure 1: Preauricular sinus: Initial step of gentle probing with a bluntended malleable probe

Indian Journal of Otolaryngology and Head and Neck Surgery Vol. 58, No. 1, January-March 2006
8
dissection ensures a clean bloodless field. Involvement of anexperienced plastic and reconstructive surgeon, with a soundknowledge of wound healing and meticulous planningpreoperatively and preoperatively, helps minimise the scar.
REFERENCES1. Lau JT. Towards better delineation and complete excision of
Preauricular sinus. Aust N Z J Surg 1983;53:267–9.
2. Joseph VT, Jacobsen AS. Single stage excision of Preauricular sinus.
Aust N Z J Surg 1995;65:254–6.
3. Lam HC, Soo G, Wormald PJ, Van Hasselt CA. Excision of the
Preauricular sinus: a comparison of two surgical techniques.
Laryngoscope 2001;111:317–9.
4. Gur E, Yeung A, Al–Azawwi M, Thomson H. The excised preauricular
sinus in 14 years: Is there a problem? Plastic Reconstr Surg
1998;102:1405–8.
5. Currie AR, King WW, Vlantis AC, Li AK. Pitfalls in the management
of Preauricular sinuses. Br J Surg 1996;83:1722–4.
6. Ellie M, Lakswaki R, Anglebe C, Altrogge C. Clinical evaluation and
surgical management of congenital Preauricular fistulas. J Oral
Maxillofac Surg 1998;56:827–30.
Address for CorrespondanceDr. K. Krishna Kumar,Department of Otolaryngology,Sundaram Medical Foundation,IV Avenue, Shanthi Colony,Anna nagar,Chennai – 600 040, IndiaE-mail: [email protected]
Preauricular sinus