Practical Dentistry Dental Radiology Series · PRACTICAL DENTISTRY Peer Reviewed 19 Figure 2....
8
TODAY’S VETERINARY PRACTICE | May/June 2015 | tvpjournal.com PRACTICAL DENTISTRY Peer Reviewed 18 The knowledge gained from dental radiographs not only improves patient care, it increases client compliance with treatment recommendations. Most important, the information gained via these radiographs speeds dental procedures and decreases complications. This article is the first in a 3-part series on dental radiology, which will discuss: • The importance of dental radiography • Dental radiography techniques • Interpretation of dental radiography images. This article reviews indications for dental radiographs based on clinical presentation, demonstrating that radiographs are often critical for proper diagnosis and treatment of oral disease. These conditions are present in many patients and, therefore, are seen on an almost daily basis. PERIODONTAL DISEASE Periodontal disease is by far the most common problem in small animal veterinary medicine. 1,2 By the age of 2, 70% of cats and 80% of dogs have some form of periodontal disease. 3 Periodontal probing is a critical first step in the evaluation of periodontal disease. 4,5 However, there are 2 reasons dental radiographs are required for a complete evaluation: 6 1. Periodontal pockets can easily be missed due to narrow pocket width, a tight interproximal space (Figure 1A), or ledge of calculus. 7 Tight interproximal spaces are normal in the molar teeth, especially in small and toy breed dogs, 8 and dental radiographs should elucidate these pathologic pockets (Figure 1B). 2. Radiographs are absolutely critical in cases of periodontal disease of the mandible of small and toy breed dogs (especially in the area of the canine and first molar teeth). In these patients, periodontal disease can cause marked weakening of the mandible, creating risk for a pathologic fracture. 9,10 In small breed dogs, the teeth, especially the mandibular first molar, extend across a much larger percentage of the bone of the mandible than in other breeds (Figure 2). 11 The periodontal aspect of these pathologic fractures is often missed on skull films, but PRACTICAL DENTISTRY Dental Radiology Series The Importance of Dental Radiography Brook A. Niemiec, DVM, FAVD, Diplomate AVDC Southern California Veterinary Dental Specialties, San Diego, California FIGURE 1. Intraoral image of right mandibular first and second molars (409 and 410) in a dog (A). The tight occlusion does not allow the periodontal probe to pass easily between the teeth, which may prevent a pathologic periodontal pocket from being identified. The subsequent dental radiograph (B) reveals a significant bony defect (red arrow). A B
Transcript of Practical Dentistry Dental Radiology Series · PRACTICAL DENTISTRY Peer Reviewed 19 Figure 2....

Today’s VeTerinary PracTice | May/June 2015 | tvpjournal.com
PracTical denTisTryPeer reviewed
18
The knowledge gained from dental radiographs not only improves patient care, it increases client compliance with treatment recommendations. Most important, the information gained via these radiographs speeds dental procedures and decreases complications.
This article is the first in a 3-part series on dental radiology, which will discuss:• The importance of dental radiography• Dental radiography techniques• Interpretation of dental radiography images.
This article reviews indications for dental radiographs based on clinical presentation, demonstrating that radiographs are often critical for proper diagnosis and treatment of oral disease. These conditions are present in many patients and, therefore, are seen on an almost daily basis.
PERIODONTAL DISEASE Periodontal disease is by far the most common problem in small animal veterinary medicine.1,2 By the age of 2, 70% of cats and 80% of dogs have some form of periodontal disease.3
Periodontal probing is a critical first step in the evaluation of periodontal disease.4,5 However, there are 2 reasons dental radiographs are required for a complete evaluation:6
1. Periodontal pockets can easily be missed due to narrow pocket width, a tight interproximal space (Figure 1A), or ledge of calculus.7 Tight interproximal spaces are normal in the molar teeth, especially in small and toy breed dogs,8 and dental radiographs should elucidate these pathologic pockets (Figure 1B).
2. Radiographs are absolutely critical in cases of periodontal disease of the mandible of small and toy breed dogs (especially in the area of the canine and first molar teeth). In these patients, periodontal disease can cause marked weakening of the mandible, creating risk for a pathologic fracture.9,10 In small breed dogs, the teeth, especially the mandibular first molar, extend across a much larger percentage of the bone of the mandible than in other breeds (Figure 2).11 The periodontal aspect of these pathologic
fractures is often missed on skull films, but
Practical Dentistry
Dental Radiology Series The Importance of Dental RadiographyBrook A. Niemiec, DVM, FAVD, Diplomate AVDC Southern California Veterinary Dental Specialties, San Diego, California
Figure 1. Intraoral image of right mandibular first and second molars (409 and 410) in a dog (A). The tight occlusion does not allow the periodontal probe to pass easily between the teeth, which may prevent a pathologic periodontal pocket from being identified. The subsequent dental radiograph (B) reveals a significant bony defect (red arrow).
A B

tvpjournal.com | May/June 2015 | Today’s VeTerinary PracTice
PracTical denTisTry Peer reviewed
19
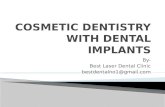
Figure 2. Intraoral dental radiograph of left mandibular fourth premolar and first molar (308 and 309) of a 7-pound dog (A). In this case, minimal bone apical to the tooth roots (red arrows) is present, especially the mesial root of the mandibular first molar, which creates a high risk for iatrogenic jaw fracture during an extraction attempt, even if the bone is normal. Significant periodontal disease greatly worsens the risk for jaw fracture (see Figure 4, page 20). Intraoral dental radiograph of left mandibular first molar (309) of a 65-pound dog (B). In this case, a considerable amount of bone is present apical to the root apices (blue arrows). Therefore, there is minimal risk for jaw fracture during extraction of this tooth, provided that proper technique is utilized.
A B
Figure 3. Lateral skull radiograph of a dog with bilateral distal mandibular jaw fracture (A). Overlapped mandibles make diagnosis of the bone loss that weakened the bone, which subsequently resulted in pathologic fracture, difficult. Intraoral dental radiograph of the same patient (B) that demonstrates obvious alveolar bone loss on the distal aspect of the first molar. If the tooth is not extracted, healing cannot occur.
A B
can seriously complicate healing (Figure 3). Therefore, dental radiographs are important in assessing mandibular fractures.12 In addition, this weakening significantly increases the possibility of iatrogenic fracture during extraction attempts (Figure 4, page 20).10,12 Preoperative dental radiographs can help practitioners avoid this complication.
FELINE TOOTH RESORPTIONDental radiographs are absolutely critical for proper dental care in feline patients due to the potential for resorptive lesions, which are very common in cats.7,13 Intraoral dental radiographs are required for proper diagnosis and treatment.6,14
Types of ResorptionThere are 3 recognized types of tooth resorption:13,15 • Type 1 lesions do not undergo replacement
resorption.13,15 These teeth typically retain sufficient normal root and pulp structure such that, because the roots are retained, pain and infection result. If dental radiographs reveal intact root structure (Figure 5, page 20) or worse, an active infection, complete root extraction is required.6,13,14
• Type 2 lesions demonstrate replacement resorption of the roots. The lost tooth structure is replaced by bone, which makes extraction very difficult (Figure 6, page 20).15 The resorption in these patients often continues until no recognizable

Today’s VeTerinary PracTice | May/June 2015 | tvpjournal.com
PracTical denTisTryPeer reviewed
20
tooth structure remains (ghost roots) (Figure 7). In these cases, endodontic infection does not occur.16 This finding has resulted in the accepted therapy of crown amputation for treating these teeth.13,14
• Type 3 lesions are seen in teeth that have evidence of Type 1 in one root and Type 2 in the other.17 Dental radiographs save the practitioner time and frustration by
directing his or her efforts appropriately.18 Premolar teeth in cats without ankylosis can typically be extracted closed (without a flap).
In patients with ankylosis, a surgical approach with buccal bone removal is often necessary..
Teeth with advanced replacement resorption can be crown amputated, rather than delving after retained/ankylosed roots.6,18 Crown amputation is indicated only if there is significant ankylosis and root resorption, with no evidence of periodontal ligaments, the endodontic system, or infection (endodontic or periodontal) (Figure 6).7,13,14 Patients with caudal stomatitis should not be treated by crown amputation.13
Figure 4. Intraoral dental radiograph of right mandibular first molar in a 5-pound dog with advanced periodontal bone loss (blue arrows). Only 0.3 mm of ventral cortex remains (yellow arrow), which greatly predisposes the area to a pathologic mandibular fracture, especially during an extraction attempt. Note that the third premolar is only held in place by a calculus bridge (red arrow). Figure 5. Type 1 tooth resorption on left mandible of a cat, with significant resorptive lesions in the crowns of the teeth (blue arrows). However, intact endodontic systems and periodontal ligaments are present (red arrows), mandating complete extraction. Figure 6. Type 2 tooth resorption in maxillary left canine of a cat, with significant replacement resorption (dentoalveolar ankylosis) evidenced by lack of a radiographically identifiable periodontal ligament (red arrows). This condition makes extraction by standard elevation difficult to impossible. Figures reprinted from Importance of Dental Radiographs client educational poster.
Figure 7. Advanced Type 2 tooth resorption in left mandibular third premolar (307) in a cat, with no radiographically identifiable root canal or periodontal ligament (red arrow). In addition, no radiographic evidence of periodontal or endodontic infection is present. This tooth is a candidate for crown amputation provided that the patient is not being treated for caudal stomatitis. Figure 8. Intraoral image of a patient with an uncomplicated crown fracture of left maxillary fourth premolar (208). In this case, the dentin is exposed, but not the root canal system directly. In most hospitals, these teeth are not evaluated further. Figure 9. Intraoral dental radiograph of the tooth in Figure 8 that reveals periapical rarefaction of all 3 roots (red arrows), which indicates the tooth is nonvital and significantly infected (similar to a tooth with direct pulp exposure). Root canal therapy or extraction is required to relieve the infection. Figures reprinted from Importance of Dental Radiographs client educational poster.
4 5 6
7 8 9

tvpjournal.com | May/June 2015 | Today’s VeTerinary PracTice
PracTical denTisTry Peer reviewed
21
ENDODONTIC DISEASE Even in cases of obvious endodontic disease, such as a complicated crown fracture or discolored (nonvital) tooth, radiographs may convince clients to consent to the recommended treatment. However, dental radiographs are even more critical in cases where endodontic disease has either subtle or no clinical signs.
Uncomplicated Crown FracturesThe most common cases of camouflaged endodontic disease are uncomplicated crown fractures. These teeth have dentinal, but not direct pulp, exposure (Figure 8). Most of these teeth are vital; however, there is a possibility that the endodontic system has been infected through the dentinal tubules, which can result in tooth nonvitality and infection/abscessation, similar to a tooth with direct pulp exposure.13,19,20
This painful endodontic infection generally cannot be diagnosed without dental radiographs, as clinical abscessation is very rare. Therefore, every tooth with direct dentin exposure should be radiographed to rule out endodontic disease.20,21 Further therapy is always indicated, depending on the results of the dental radiograph. If the dental radiographs reveal no signs of endodontic disease, the tooth should be treated with a bonded sealant, and the patient should have dental radiographs repeated in 9 months to ensure the tooth is/was not subclinically infected.13,20–22
If there is evidence of tooth death (wide root canals or periapical lucency) (Figure 9), root canal therapy or extraction is mandated.7,19,22
Worn TeethAnother scenario in which teeth appear healthy but may be endodontically abnormal is worn teeth.7,13 If a tooth has been worn to the point of direct pulp
exposure, either root canal therapy or extraction is required. If there is adequate reparative (tertiary) dentin (Figure 10A), the majority of these teeth remain vital and pain free.23
However, teeth can become nonvital and infected despite visibly sufficient reparative dentin, and can only be elucidated by dental radiographs.23 If radiographic evidence of endodontic disease is present (ie, wide root canals or periapical lucency) (Figure 10B), root canal therapy or extraction is indicated.7,20,23
Figure 10. Intraoral image of a canine patient with moderate attrition of mandibular incisors (A). Adequate tertiary dentin is present; therefore, direct pulp exposure should not be a concern. Intraoral dental radiograph of these teeth reveals 3 nonvital and infected incisors (B); infection is evidenced by widened endodontic spaces (blue arrows) and periapical rarefaction (red arrows).
Figure 11. Intraoral dental radiograph of retained deciduous left maxillary canine (604). The vast majority of the root is normal (blue arrows), which means that, in all likelihood, the tooth will not resorb, indicating the necessity of complete extraction. However, resorption—caused by pressure from an erupting adult tooth—is present in the cervical region of the tooth (red arrow), which greatly increases the risk of fracturing the tooth during extraction. Therefore, careful elevation apical to this point allows for complete extraction of the tooth; a surgical approach may be advised. Reprinted from Importance of Dental Radiographs client educational poster.
A
B

Today’s VeTerinary PracTice | May/June 2015 | tvpjournal.com
PracTical denTisTryPeer reviewed
22
Teeth with Hidden InfectionThe final scenario of camouflaged endodontic disease is clinically normal teeth that are actually infected.6,7 These teeth, like all endodontically infected teeth, rarely have clinical signs, and the infection can only be diagnosed on radiographs.
PERSISTENT DECIDUOUS TEETHExtraction of persistent deciduous teeth is a common procedure; however, without dental radiographs, this can be a challenging and frustrating endeavor.
Incomplete ResorptionIn some cases, the root and attachment of the deciduous tooth are normal, and extraction—if performed correctly—is straightforward, without root fracture occurring.24 In most cases, however, the deciduous teeth have undergone some to significant resorption due to the pressure applied by the erupting permanent dentition (Figure 11, page 21).6 Resorption and secondary ankylosis make extraction very difficult, commonly resulting in a fractured root.24 In these cases, as in resorptive lesions, beginning with a surgical approach may be advised. Regardless, if an identifiable root canal or signs of infection are present, these roots require complete extraction to avoid inflammation and infection.24,25
Complete ResorptionThere are occasional cases in which the root structure of the deciduous tooth has been completely resorbed, with the crown only held by ankylosis at the alveolar crest (Figure 12).16,24 Proper therapy requires that only the crown and the very small retaining root segment be removed. With this knowledge from the start, the practitioner saves time by not: • Searching for the root• Worrying about a problem that does
not exist• Causing unnecessary trauma to the
patient.
“MISSING” TEETH Incomplete dental arches are quite common in veterinary patients. In some
cases, the tooth is truly missing; however, often the tooth/root is actually present and may be pathologic.
Possible etiologies for “missing” teeth include:24
1. Congenitally missing teeth26 are common in small, toy, and brachycephalic breeds.27 The premolars, maxillary second and mandibular third molars, and incisors are typically absent. No specific therapy is necessary.
2. Previously extracted or exfoliated teeth, while rare in young patients, are quite common in mature animals. Tooth loss can occur secondary to trauma, but occurs most commonly due to periodontal disease or previous extraction. With extraction, radiographs usually reveal evidence of a healing alveolus. Again, no therapy is necessary.
3. Teeth fractured below the gum line (Figure 13) may be a result of trauma or an incomplete extraction attempt. Retained roots following extraction attempts are quite common: one study evaluating carnassial teeth in dogs and cats revealed that almost 90% of these teeth had retained roots.28 Dental radiographs confirm retained roots and, in most cases (57%), an infectious lesion.28 If the root appears relatively normal (ie, not significantly resorbed), surgical extraction is generally the recommended course of action to alleviate pain and endodontic infection.
Figure 12. Intraoral dental radiograph of retained deciduous right mandibular canine (804). In this case, the root is completely resorbed (red arrows), making extraction easy. Without this knowledge, however, the practitioner may delve after roots that are not present, creating unnecessary surgical trauma.
Figure 13. Intraoral dental radiograph of a feline patient with a “missing” right mandibular canine (404). Dental radiographs revealed a retained root (blue arrow) with associated periapical (red arrow) and cervical (yellow arrow) rarefaction, which indicates severe infection. This tooth was causing significant pain in the patient. A significant Type 1 resorptive lesion is present on the contralateral canine (white arrow).
Figure 14. Intraoral dental radiograph of a feline patient with a “missing” right mandibular first premolar (405). The radiograph reveals the embedded tooth (red arrow); the small lucency in the crown is an early dentigerous cyst.

tvpjournal.com | May/June 2015 | Today’s VeTerinary PracTice
PracTical denTisTry Peer reviewed
23
4. Impacted or embedded teeth (Figure 14) can be malformed or normal, but do not erupt into the dentition, often because they are blocked by a structure, such as bone, teeth, or, most commonly, an area of thick and firm gingiva called the operculum. While this condition is most common in the first and second premolars of brachycephalic breeds, any tooth can be embedded.
Dentigerous CystsThe biggest concern with unerupted or impacted teeth is the development of dentigerous cysts, which arise from the enamel forming organ of the unerupted tooth. The incidence of dentigerous cysts is unknown in veterinary medicine, but anecdotally is estimated to be approximately 50% of all unerupted teeth. In addition, pathologic changes were noted in 32.9% of cases in one human study.29
As the cyst grows it causes bone loss by pressure, and these cysts can grow quite large in a short period of time, resulting in a significant bony defect (Figure 15). In addition, malignant transformation can occur and the cysts can become infected, creating significant swelling and pain.26
Therapeutic ApproachThe recommended therapy for impacted teeth is
Figure 15. Large dentigerous cyst (white arrows) in left mandible of a dog with an embedded first premolar (305) (red arrow); no clinical signs were present.

TODAY’S VETERINARY PRACTICE | May/June 2015 | tvpjournal.com
PRACTICAL DENTISTRYPeer Reviewed
24
surgical extraction. If cyst formation has occurred, en bloc removal or extraction of the tooth and meticulous curettage of the lining should prove curative. Following curettage, a biopsy of the lining and bone augmentation is recommended. Referral to a veterinary dentist is recommended for larger lesions.
It is critical to note that 2 of the causes for “missing” teeth require no therapy, while the other 2 can lead to signifi cant pathology. Therefore, all “missing” teeth should be radiographed to determine the correct cause and, therefore, the correct approach to management.
EXTRACTIONS Pre- and postoperative dental radiographs should be exposed for all extraction procedures.18 Pre-extraction radiographs allow the practitioner to determine the amount of disease present as well as any root abnormalities, such as curved (Figure 16) or extra roots. Ten percent of maxillary third premolars in cats have a third root (Figure 17).30
One of the more important fi ndings on pre-operative dental radiographs is the presence and degree of ankylosis.7,19 In addition, the level of remaining bone is elucidated. In the case of a mandibular fi rst molar or canine extraction, knowledge of the amount of remaining mandibular bone can be critical with regard to avoiding an iatrogenic pathologic
fracture.6,10,18 Radiographs also serve as legal evidence, documenting the need for extraction.
Postextraction dental radiographs are equally important. Despite the appearance of complete extraction, there is still a possibility of retained roots or other pathology. One study evaluating extraction of carnassial teeth in dogs and cats revealed that almost 90% of these teeth had retained roots.28 Therefore, postoperative radiographs are critical in all cases (Figure 18). In addition, radiographs serve as legal documents in cases with complications.
IN SUMMARYThe conditions and therapeutic options discussed in this article emphasize the value—especially the patient benefi ts—of full-mouth radiographs for all veterinary patients.30 Nearly every veterinary patient has some form of oral disease. Dental radiographs are a critical piece of information for the veterinarian for both diagnosing and treating oral disease.
Figure 16. Intraoral dental radiograph of left mandibular fi rst molar (309) of a 7-pound dog. The apex is very close to the ventral cortex and has a marked curve (red arrow), which signifi cantly complicates extraction.
Figure 17. Intraoral dental radiograph of maxillary left third premolar in a cat. This tooth has a supernumerary root (red arrow), which greatly complicates the extraction process.
Figure 18. Retained roots of left mandibular fi rst molar (309) after “extraction” at a clinic without dental radiography. Note the retained tooth roots (red arrows).
BROOK A. NIEMIECBrook A. Niemiec, DVM, FAVD, Diplomate AVDC, is Chief of Staff of Southern California Veterinary Dental Specialties, with offi ces in San Diego and Murrieta, California, and Las Vegas, Nevada. He lectures extensively at national and international conferences. He received his DVM from University of California–Davis.

tvpjournal.com | May/June 2015 | Today’s VeTerinary PracTice
PracTical denTisTry Peer reviewed
25
References1. University of Minnesota Center for Companion Animal Health. National
companion animal study. Uplinks 1999; p 3.2. Lund EM, Armstrong PJ, Kirk CA, et al. Health status and population
characteristics of dogs and cats examined at private veterinary practices in the United States. JAVMA 1999; 214:1336-1341.
3. Wiggs RB, Lobprise HB. Periodontology. In Wiggs RB, Lobprise HB (eds): Veterinary Dentistry Principles and Practice. Philadelphia: Lippincott—Raven, 1997, pp 186-231.
4. Niemiec BA. Periodontal disease. Top Comp Anim Med 2008; 23(2):72-80.5. Huffman LJ. Oral examination. In Niemiec BA (ed): Small Animal Dental,
Oral and Maxillofacial Disease—A Color Handbook. London: Manson Publishing, 2010, pp 39-61.
6. Niemiec BA. The importance of dental radiology. Eur J Comp Anim Pract 2011; 20(3):219-229.
7. Niemiec BA. Case based dental radiology. Top Companion Anim Med 2009; 24(1):4-19.
8. Niemiec BA. Advanced non-surgical therapy. In Niemiec BA (ed): Veterinary Periodontology. Ames, IA: John Wiley and Sons, 2012, pp 154-169.
9. Taney KG, Smith MM. Problems with the bones, muscles and joints. In Niemiec BA (ed): Small Animal Dental, Oral and Maxillofacial Disease—A Color Handbook. London: Manson Publishing, 2010, pp 199-224.
10. Niemiec BA. Local and regional consequences of periodontal disease. In Niemiec BA (ed): Veterinary Periodontology. Ames, IA: John Wiley and Sons, 2012, pp 69-80.
11. Gioso MA, Shofer F, Barros PS, Harvey CE. Mandible and mandibular first molar tooth measurements in dogs: Relationship of radiographic height to body weight. J Vet Dent 2001; 18(2):65-68.
12. Mulligan T, Aller S, Williams C. In: Atlas of Canine and Feline Dental Radiography. Trenton, NJ: Veterinary Learning Systems, 1998, pp 176-183.
13. Dupont GA. Pathologies of the dental hard tissue. In Niemiec BA (ed): Small Animal Dental, Oral and Maxillofacial Disease—A Color Handbook. London: Manson Publishing, 2010, pp 127-157.
14. DuPont GA. Crown amputation with intentional root retention for dental resorptive lesions in cats. J Vet Dent 2002; 19(2):107-110.
15. DuPont GA, Debowes LJ. Comparison of periodontitis and root replacement in cat teeth with resorptive lesions. J Vet Dent 2002; 19(2):71-76.
16. Bellows J. Treatment of tooth resorption. In: Feline Dentistry: Oral Assessment, Treatment, and Preventitive Care. Ames, IA: Wiley Blackwell, 2010, pp 222-241.
17. Lommer MJ, Verstraete FJ. Prevalence of odontoclastic resorption lesions and periapical radiographic lucencies in cats: 265 cases (1995-1998). JAVMA 2000; 217(12):1866-1869.
18. Niemiec BA. Dental Extractions Made Easier. Tustin, CA: Practical Veterinary Publishing, 2012.
19. Startup S. Tooth response to injury. In Niemiec BA (ed): Veterinary Endodontics. Tustin, CA: Practical Veterinary Publishing, 2011.
20. Theuns P, Niemiec BA. Bonded sealants for uncomplicated crown fractures. J Vet Dent 2011; 28(2):130-132.
21. Woodward TM. Bonded sealants for fractured teeth. Top Comp Anim Med 2008; 23(2):91-96.
22. Theuns P. Endodontic anatomy. In Niemiec BA (ed): Veterinary Endodontics. Tustin, CA: Practical Veterinary Publishing, 2011.
23. Trowbridge H, Kim S, Suda H. Structure and functions of the dentin and pulp complex. In Cohen S, Burns RC (eds): Pathways of the Pulp, 8th ed. St. Louis: Mosby, 2002, pp 441-456.
24. Niemiec BA. Pathology in the pediatric patient. In Niemiec BA (ed): Small Animal Dental, Oral and Maxillofacial Disease—A Color Handbook. London: Manson Publishing, 2010, pp 89-126.
25. Wiggs RB, Lobprise HB. Pedodontics. In: Veterinary Dentistry, Principals and Practice. Philadelphia: Lippincott Raven, 1997, pp 169-174.
26. Neville BW, Damm DD, Allen CM, Bouquot JE. Abnormalities of teeth. In: Oral and Maxillofacial Pathology, 2nd ed. Philadelphia: Saunders, 2002, pp 49-106.
27. Harvey CE, Emily PP. Occlusion, occlusive abnormalities, and orthodontic treatment. Small Animal Dentistry. St. Louis: Mosby, 1993, pp 266-296.
28. Moore JI, Niemiec BA. Evaluation of extraction sites for retained roots in dogs and cats. JAAHA 2014; 50(2):77-82.
29. Raghoebar GM, Boering G, Vissink A. Clinical, radiographic, and histological characteristics of secondary retention of permanent molars. J Dent 1991; 19:164-170.
30. Verstraete FJ, Kass PH, Terpak CH. Diagnostic value of full-mouth radiography in cats. Am J Vet Res 1998; 59(6):692-695.