Practical Approaches to Overcoming Vaccine...
44
1 Practical Approaches to Overcoming Vaccine Hesitancy Brought to you as a public health service by Sanofi Pasteur Inc. MKT26560 7/13
Transcript of Practical Approaches to Overcoming Vaccine...
1
Practical Approaches to Overcoming Vaccine Hesitancy
Brought to you as a public health service by Sanofi Pasteur Inc.
MKT26560 7/13

2
What Is Vaccine Hesitancy?
• Intent to skip or delay at least 1 of the vaccines recommended by the
Advisory Committee on Immunization Practices (ACIP)1,2
• Uncertainty as to whether a vaccine should be administered in
accordance with the ACIP recommended immunization schedule1,2
– In spite of that uncertainty, some vaccine-hesitant parents will allow their
children to be immunized anyway2
Such parents are at risk for skipping or delaying other vaccines down the road3
• Steps that health care professionals (HCPs) can take to minimize the
impact of vaccine hesitancy4:
– Establish trusting relationships with parents/patients
– Provide appropriate educational materials
References: 1. Heller G, Roberts M. Turning the tide: addressing vaccine hesitancy and timely immunizations through a
social marketing campaign. Presented at: 44th National Immunization Conference, Atlanta, Georgia, April 21, 2010.
Abstract 22697. 2. Opel DJ, et al. Hum Vaccines. 2011;7(4):419-425. 3. Dempsey AF, et al. Pediatrics. 2011;128(5):848-
856. 4. Gust DA, et al. Pediatrics. 2008;122(4):718-725.

3
Vaccine Hesitancy: Not a New Problem
• Turn of the 19th century: Vaccination is introduced in the
United States (US)1
• 1809: Massachusetts is the first state to make smallpox
vaccination compulsory1,2
• 1850s: US anti-vaccination movement arises in response to
the proliferation of smallpox vaccination mandates1,2
– Activists object to regulations requiring submission to a procedure
that involves discomfort and that might not be safe 2
• 1870s: Smallpox re-emerges in the US, as a result of a
decline in vaccination rates1
– Opposition to vaccination increases as new laws are passed and old
ones to control smallpox are reinforced1
References: 1. Omer SB, et al. N Engl J Med. 2009;360(19):1981-1988. 2. Colgrove J. State of Immunity: The Politics
of Vaccination in Twentieth-Century America. Berkeley, CA: University of California Press; 2006.

4
Impact of Non-medical Exemptions on Vaccination Rates
• Overall mean state-level rates of non-medical exemptions
have increased; pace of that increase has accelerated1-3
• Vaccination coverage rates are lower in states with personal
belief exemptions (PBEs) than in states permitting only
religious exemptions1,3
• Children with non-medical exemptions tend to aggregate
within schools and communities2,4
• Vaccine-preventable diseases tend to cluster in areas
where exemption rates are highest5-7
References: 1. Omer SB, et al. N Engl J Med. 2012;367(12):1170-1171. 2. Omer SB, et al. N Engl J Med.
2009;360(19):1981-1988. 3. Omer SB, et al. JAMA. 2006;296(14):1757-1763. 4. Buttenheim A, et al. Am J Public
Health. 2012;102(8):e59-e67. 5. Feikin DR, et al. JAMA. 2000;284(24):3145-3150. 6. Centers for Disease Control
and Prevention (CDC). MMWR. 2008;57(8):203-206. 7. Omer SB, et al. Am J Epidemiol. 2008;168(12):1389-1396.

5
High Incidence of Pertussis in States That Allow PBEs: US, 2012a
a States shown in purple allow religious exemptions but not PBEs, whereas states shown in green allow both religious exemptions and PBEs. In Missouri, PBEs are permitted only for children in day care, preschool, and nursery school.2,3 Map adapted from Harrington JW.3
References: 1. CDC. Data on file (2012 Provisional Pertussis Surveillance Report), March 2013. MKT26422. 2. National Conference of State Legislatures. States with religious and philosophical exemptions from school immunization requirements. http://bit.ly/14m1gjt. Accessed June 7, 2013. 3. Harrington JW. Consultant Ped. 2011;10(11):S17-S21.
White check marks indicate states where the documented incidence of pertussis exceeded the national average during 2012.1
Allow religious exemptions but not PBEs
Allow medical exemptions only
Allow religious exemptions and PBEs
In 12 of 19 (63%) states
permitting PBEs and
9 of 31 (29%) states not
allowing PBEs, the
documented incidence of
pertussis was higher than
average.2

6
High Incidence of Measles in States That Allow PBEs: US, 2011
a Import-associated describes cases brought into the US from other countries; cases linked epidemiologically to importations of measles into the US; cases with virologic evidence suggesting recent importation; and cases linked to patients with virologic evidence of recent importation. Map reproduced from CDC.1
References: 1. CDC. MMWR. 2012;61(15):253-257. 2. National Conference of State Legislatures. States with religious and philosophical exemptions from school immunization requirements. http://bit.ly/14m1gjt. Accessed June 7, 2013.
Red check marks indicate states that allow PBEs and had a high incidence of measles during 2011.1,2
Import-associateda
Unknown source

7
Factors That Contribute to Vaccine Hesitancy
• Increase in:
– Number of new vaccines for various diseases
– State-level school entry immunization mandates
• Continued success of vaccines in controlling diseases that parents/patients
no longer remember and rarely see1
• Rise in consumerism, which has2:
– Encouraged parents/patients to shop around for an HCP and actively search
for information about vaccines
– Eroded parents’/patients’ trust in HCPs
• Spread of misinformation via mass media and the internet3
• Growing willingness to question the integrity of scientists, public health officials,
and anyone else involved in formulating immunization policies4
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Timmermans S, Oh H. J Health Soc Behav.
2010;51(suppl):S94-S106. 3. Opel DJ, et al. Arch Pediatr Adolesc Med. 2009;163(5):432-437. 4. Colgrove J. State of
Immunity: The Politics of Vaccination in Twentieth-Century America. Berkeley, CA: University of California Press; 2006.

8
Vaccine-Hesitant Parents Are Not All the Same1
• In a study by Gust and colleagues, 28% of parents
had doubts about vaccination
• Concern about vaccine safety was a predictor of
vaccine delay or refusal
• Parents with doubts about immunizations differ in
their reasons for those doubts
Reference: 1. Gust DA, et al. Pediatrics. 2008;122(4):718-725.

9
Types of Vaccine-Hesitant Parents1,2
• Uninformed but educable
– Want education to counter anti-vaccine information
• Misinformed but correctable
– Need information about vaccine benefits
• Well-read and open-minded
– Want to intelligently discuss pros and cons
• Strongly vaccine-hesitant
– Willing to listen but not likely to change their mind right away
• Strong-willed and committed against vaccines
– Want to sway the HCP to their line of thinking
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Halperin SA. Canadian J CME. 2000;12(1):
62-74.
10
The ASK Approach for Effective Immunization Communication1
• Acknowledge the parent’s/patient’s concerns
– Ask for clarification to understand their needs; sometimes a simple
fact is all that’s needed to dispel a myth or misunderstanding
• Steer the conversation
– Refute the myth or misunderstanding with facts
– If the parent/patient is not already committed against vaccines,
continue your conversation to identify additional obstacles
• Know your facts; be confident and prepared
– Recommend or provide reading material
– Refer the parent/patient to reliable internet resources
– Make your professional recommendation crystal clear
Reference: 1. Morgana T, Pringle J. Approaches to families questioning vaccines—the ASK approach for effective
immunization communication. Presented at: 48th Annual Meeting of the Infectious Diseases Society of America, Vancouver,
BC, October 23, 2010. Abstract 92.
11
The CASE Framework for Conversations about Vaccines1
• Corroborate
– Acknowledge the parent’s/patient’s concern
– Find some point on which you and the parent/patient can agree
– Set the tone for a respectful conversation
• About me
– Talk about what you’ve done to enhance your knowledge and expertise (eg, attended a conference)
• Science
– Describe what science has to say about the topic in question
• Explain and advise
– Offer your recommendation, based on the science
Reference: 1. Singer A. Making the CASE for vaccine communication: a new model for talking to parents about
vaccines. November 2011. http://bit.ly/14lKlh4. Accessed June 7, 2013.

12
Tips for Handling Vaccine Hesitancy
• Take a (or another) deep breath – Listen to the parents/patients
– Identify their questions or problems
– Make no assumptions
• Have a plan – What is your practice philosophy?
– Will you see families who outright refuse all vaccines for
their children?
• Tailor your advice to each individual
parent/patient, based on his or her concerns

13
Tips for Handling Vaccine Hesitancy (cont)
• Document your discussion with the parent/patient
• Revisit the discussion at each subsequent visit
– Inform the parent/patient that you will be doing so
• For parents/patients who refuse, provide the Vaccine Information
Statement and consider using a Refusal to Vaccinate form
• For unimmunized or partially immunized patients, flag the chart for the
benefit of yourself and other HCPs, in the event that those patients
require sick visits
• Be direct, clear, and authoritative with respect to your office’s philosophy
and policy vis-à-vis a parent’s/patient’s ongoing refusal to vaccinate
– Know the plan, and maintain a consistent approach within your practice

14
Concerns That Have Been Raised Regarding Vaccines
• “Overloading of the immune system”1,2
• “Autism or other neurologic side effects”1
• “Mercury exposure and brain damage”1,3
• “Aluminum toxicity and brain damage”1,3
• “Formaldehyde injection”3
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Offit PA, et al. Pediatrics. 2002;109(1):124-
129. 3. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.
15
Concerns That Have Been Raised Regarding Vaccines
• “Overloading of the immune system”1,2
• “Autism or other neurologic side effects”1
• “Mercury exposure and brain damage”1,3
• “Aluminum toxicity and brain damage”1,3
• “Formaldehyde injection”3
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Offit PA, et al. Pediatrics. 2002;109(1):124-
129. 3. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.

16
Key Facts About Multiple Vaccines and the Immune System
• An infant’s immune system has the capacity to respond to thousands of
antigens at any given time1
– Immune system is constantly replenished; it cannot be overloaded by the
antigens (ie, proteins and polysaccharides) in vaccines1
– In fact, children are exposed to thousands of antigens every day (on toys,
doorknobs, and playground equipment)2
• Although the number of recommended vaccines has increased over the
years, children today typically receive fewer antigens than their parents
did in the past1,2
• The response to multiple vaccines given during a single visit is similar
to the response that occurs when individual vaccines are administered
separately1
References: 1. Offit PA, et al. Pediatrics. 2002;109(1):124-129. 2. Harrington JW. Consultant Ped. 2011;10(11):S17-S21.

17
Concerns That Have Been Raised Regarding Vaccines
• “Overloading of the immune system”1,2
• “Autism or other neurologic side effects”1
• “Mercury exposure and brain damage”1,3
• “Aluminum toxicity and brain damage”1,3
• “Formaldehyde injection”3
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Offit PA, et al. Pediatrics. 2002;109(1):124-
129. 3. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.
18
Debunking of the “Link” Between Vaccines and Neurologic Side Effects
• In 2010, The Lancet retracted the 1998 report alleging a link between
vaccines and autism1
– Numerous studies have demonstrated that no such link exists
• Vaccines are given at around the same time that autism becomes
apparent; however, they do not cause autism2
– To explain the difference between causal and temporal relations, use the
analogy of the rooster that crows every morning
The sun will rise whether or not the rooster crows
• Signs of autism in a child may predate a vaccination but not be noticed
until after a particular vaccine has been given2
• The increased number of vaccines recommended for children has not
resulted in a higher prevalence of neurodevelopmental problems2-4
References: 1. Healy CM, Pickering LK. Pediatrics. 2011;127(suppl 1):S127-S133. 2. Harrington JW. Consultant Ped.
2011;10(11):S17-S21. 3. Institute of Medicine. The childhood immunization schedule and safety: stakeholder concerns,
scientific evidence, and future studies. Washington, DC: National Academies Press; 2013. 4. DeStefano F, et al. J
Pediatrics. 2013. Epub ahead of print.
19
Concerns That Have Been Raised Regarding Vaccines
• “Overloading of the immune system”1,2
• “Autism or other neurologic side effects”1
• “Mercury exposure and brain damage”1,3
• “Aluminum toxicity and brain damage”1,3
• “Formaldehyde injection”3
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Offit PA, et al. Pediatrics. 2002;109(1):124-
129. 3. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.
20
Safety of Thimerosal and Aluminum Salts in Vaccines
• Thimerosal: a mercury-containing preservative that helps prevent
bacterial or fungal contamination in vaccines1
– No scientific evidence that links thimerosal with autism2
– Symptoms of mercury poisoning differ from those of autism3
– Measles, mumps, and rubella vaccine never contained thimerosal or
any other form of mercury2
– As a precautionary measure, thimerosal was removed from nearly all
vaccines (the exception being multidose vials) in 20012
Yet the incidence of neurodevelopmental problems has continued to rise
• Aluminum salts: an adjuvant to enhance the immune response2
– Safety is well established1,2
– All infants are exposed to aluminum in the environment (eg, breast milk,
infant formulas)1
References: 1. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401. 2. Harrington JW. Consultant Ped.
2011;10(11):S17-S21. 3. Healy CM, Pickering LK. Pediatrics. 2011;127(suppl 1):S127-S133.
21
Concerns That Have Been Raised Regarding Vaccines
• “Overloading of the immune system”1,2
• “Autism or other neurologic side effects”1
• “Mercury exposure and brain damage”1,3
• “Aluminum toxicity and brain damage”1,3
• “Formaldehyde injection”3
References: 1. Harrington JW. Consultant Ped. 2011;10(11):S17-S21. 2. Offit PA, et al. Pediatrics. 2002;109(1):124-
129. 3. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.

22
Key Facts About Formaldehyde1
• Is used to inactivate:
– Viruses that cause influenza and polio
– Tetanus and diphtheria toxins
• Is diluted during the manufacturing process
• Is required for the synthesis of thymidine, purines,
and amino acids in all humans
– Quantity of formaldehyde found naturally in an infant’s
blood is 10-fold greater than that contained in any
individual vaccine
Reference: 1. Offit PA, Jew RK. Pediatrics. 2003;112(6):1394-1401.

23
Common Reasons for Vaccine Refusal on Religious Grounds
• “God, not immunity, protects my child from illness”
• “The use of fetal cells in vaccine production is
immoral”
• “The use of vaccines containing pork gelatin is
wrong”

24
“God, not Immunity, Protects my Child from Illness”
• Ask for clarification of that statement
– This will help you determine whether the parent’s refusal of
immunizations is indeed an act of faith
• If a parent states his or her religion specifically prohibits
vaccination, a religious exemption may be in ordera
– Such exemptions are often granted to members of the Christian
Science and Amish faiths1
– Note: Amish religious doctrine does not specifically prohibit
vaccination2
Common non-religious reasons for vaccine hesitancy among the Amish:
– Concerns about vaccine safety and infant’s ability to tolerate vaccines
– Idea that vaccination is not a priority
– Feeling that it’s too difficult to travel to places where vaccinations are offered
a Mississippi and West Virginia do not allow religious exemptions.
References: 1. Calandrillo SP. Univ Mich J Law Reform. 2004;37(2):353-440. 2. Wenger OK, et al. Pediatrics.
2011;128(1):79-85.
25
“The Use of Fetal Cells in Vaccine Production is Immoral”
• Cell lines derived from aborted fetal lung tissue were used to develop vaccines
against diseases such as hepatitis A, polio, rubella, and varicella1,2
– Some Catholics may refuse vaccination in order to express their strong opposition to
abortion1
– Others may believe that vaccination involves some form of cooperation with abortion1
• Bear in mind that the lung tissue for those cell lines was from 2 fetuses that
were aborted during the 1960s2
– The cells used today are grown in culture1
• The Vatican supports use of all vaccines available at this time2
– Administration of those vaccines is morally justified because they:
Avoid a serious risk
Provide for the good of children and all who come in contact with them
– However, alternative vaccines should be used if and when they become available
References: 1. Furton EJ. Ethics & Medics. 1999;24(3):3-4. 2. Vatican Statement on Vaccines Derived from Aborted Human Fetuses. http://bit.ly/11xmRo6. Accessed June 7, 2013.
26
“The Use of Vaccines Containing Pork Gelatin is Wrong”1
• Islam and Judaism accept vaccination
• According to Islamic legal scholars, it is permissible
for observant Muslims to receive vaccines
containing pork gelatin
• According to Orthodox Rabbi Abraham Adler,
Jewish laws do allow receipt of non-oral products
containing porcine ingredients
Reference: 1. Institute for Vaccine Safety, Johns Hopkins Bloomberg School of Public Health. Religious Leaders Approval of Use of Vaccines Containing Porcine Gelatin. http://www.vaccinesafety.edu/Porcine-vaccineapproval.htm. Accessed June 7, 2013.
27
Common Philosophical Objections to Vaccination
• “Too much, too soon?”
• “Natural disease provides better immunity”
• “Most of the vaccine-preventable diseases don’t
even exist anymore”
• “My [fill in the blank] told me not to let you
vaccinate my baby”

28
“Too Much, Too Soon?”1
• Offer reassurance
– Vaccines do not overload the immune system
– Every day an infant encounters thousands of antigens (parts of
germs that cause the immune system to fight disease)
• Explain why it’s best to follow the recommended
immunization schedule
– Goal: To ensure that the child is immune to diseases before he or
she is most likely to be exposed
– The vaccines have been tested at the recommended ages, so we
know they’re safe, even in young children
Reference: 1. CDC. The childhood immunization schedule. February 2013. Available at: http://1.usa.gov/19PrMnT.
Accessed June 7, 2013.
29
“Natural Disease Provides Better Immunity”
• Explain that:
– The cost of natural immunity can be severe1
Fatal disease is not a risk worth taking
– Not vaccinating one’s child puts his or her entire community at risk
• If possible, cite cases of disease from your own
experience as an HCP
Reference: 1. Offit PA, Moser CA. Pediatrics. 2009;123(1):e164-e169.
30
“Most of the Vaccine-preventable Diseases Don’t Even Exist Anymore”
• Explain that once-prevalent vaccine-preventable diseases
may return if high immunization rates are not maintained
• Give examples of recent outbreaks
– Invasive Haemophilus influenzae type b disease1: Minnesota in 2008
– Measles2: California, Pennsylvania, and Washington in 2011 (as
indicated on an earlier slide)
• If possible, cite cases of vaccine-preventable disease from
your own experience as an HCP
References: 1. CDC. MMWR. 2009;58(3):58-60. 2. CDC. MMWR. 2012;61(15):253-257.
31
“My [Fill in the Blank] Told Me not to Let You Vaccinate my Baby”1,2
• Ask for clarification: What are the underlying
concerns of the person who gave that advice?
• Offer your recommendation, based on facts
• Recommend or provide reading material
• Refer the parent to reliable resources
References: 1. Morgana T, Pringle J. Approaches to families questioning vaccines—the ASK approach for effective
immunization communication. Presented at: 48th Annual Meeting of the Infectious Diseases Society of America, Vancouver,
BC, October 23, 2010. Abstract 92. 2. Singer A. Making the CASE for vaccine communication: a new model for talking to
parents about vaccines. November 2011. http://bit.ly/14lKlh4. Accessed June 7, 2013.

32
Ways You Can Encourage Discussion With Vaccine-Hesitant Parents/Patients
• “Help me understand how you came to that
decision”
• “Help me understand your reasons for feeling
that way”
• “What is it about vaccines that worries you?”
• “Share with me what you’ve read”
• “Share with me what you’ve heard about getting
2 or more shots at once”

33
Helpful CDC and AAP Resources for HCPs
• CDC resources for vaccine conversations with parents:
http://1.usa.gov/18TMMbH
• AAP webpage titled Communicating with Families:
http://bit.ly/14lNSM5
• AAP webpage titled Parental Refusal to Vaccinate:
http://bit.ly/11K7cNR
– Refusal to Vaccinate form
– AAP clinical report, titled “Responding to Parental Refusals of Immunization
of Children”1
– Coding resources for vaccine refusal
– Sample office vaccine policy statement (for distribution to parents)
– Sample office poster
– Resources to answer questions
Reference: 1. Diekema DS, Committee on Bioethics. Pediatrics. 2005;115(5):1428-1431.
34
Helpful Resources for Parents
• Vaccine Education Center at The Children’s Hospital of Philadelphia: http://www.vaccine.chop.edu
• AAP’s Childhood Immunization Support Program: http://bit.ly/15FmyHW
• Sanofi Pasteur’s ImmYOUnitySM website:
http://vaccines.com/about-immyounity.cfm
• Vaccinate Your Baby: http://www.vaccinateyourbaby.org
• Offit PA, Bell LM. Vaccines: What Every Parent Should Know. New York, NY:
IDG Books; 1999
• Humiston SG, Good C. Vaccinating Your Child: Questions and Answers for the
Concerned Parent. Atlanta, GA: Peachtree Publishers; 2000
• Fisher MC. Immunizations & Infectious Diseases: An Informed Parent’s Guide.
Elk Grove Village, IL: AAP; 2005
• Myers MG, Pineda D. Do Vaccines Cause That? A Guide for Evaluating Vaccine
Safety Concerns. Galveston, TX: Immunizations for Public Health; 2008

35
Additional Resources for HCPs and/or Parents
• Immunization Action Coalition: http://www.vaccineinformation.org
• Immunization Education Program of the AAP’s Pennsylvania chapter: http://www.paiep.org
• Institute for Vaccine Safety, Johns Hopkins Bloomberg School of Public Health: http://www.vaccinesafety.edu
• National Association of Pediatric Nurse Practitioners: http://bit.ly/13f06Du
• National Network for Immunization Information: http://www.immunizationinfo.org
• Pediatric Infectious Diseases Society position statement on PBEs: http://bit.ly/187OMjv

36
Backup
37
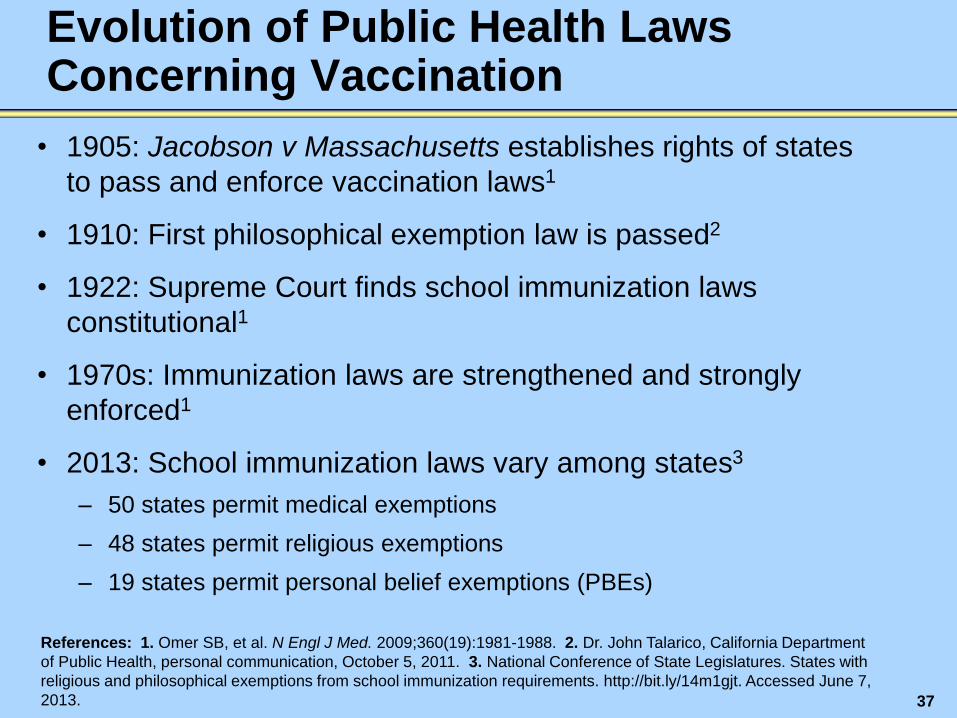
Evolution of Public Health Laws Concerning Vaccination
• 1905: Jacobson v Massachusetts establishes rights of states
to pass and enforce vaccination laws1
• 1910: First philosophical exemption law is passed2
• 1922: Supreme Court finds school immunization laws
constitutional1
• 1970s: Immunization laws are strengthened and strongly
enforced1
• 2013: School immunization laws vary among states3
– 50 states permit medical exemptions
– 48 states permit religious exemptions
– 19 states permit personal belief exemptions (PBEs)
References: 1. Omer SB, et al. N Engl J Med. 2009;360(19):1981-1988. 2. Dr. John Talarico, California Department
of Public Health, personal communication, October 5, 2011. 3. National Conference of State Legislatures. States with
religious and philosophical exemptions from school immunization requirements. http://bit.ly/14m1gjt. Accessed June 7,
2013.
38
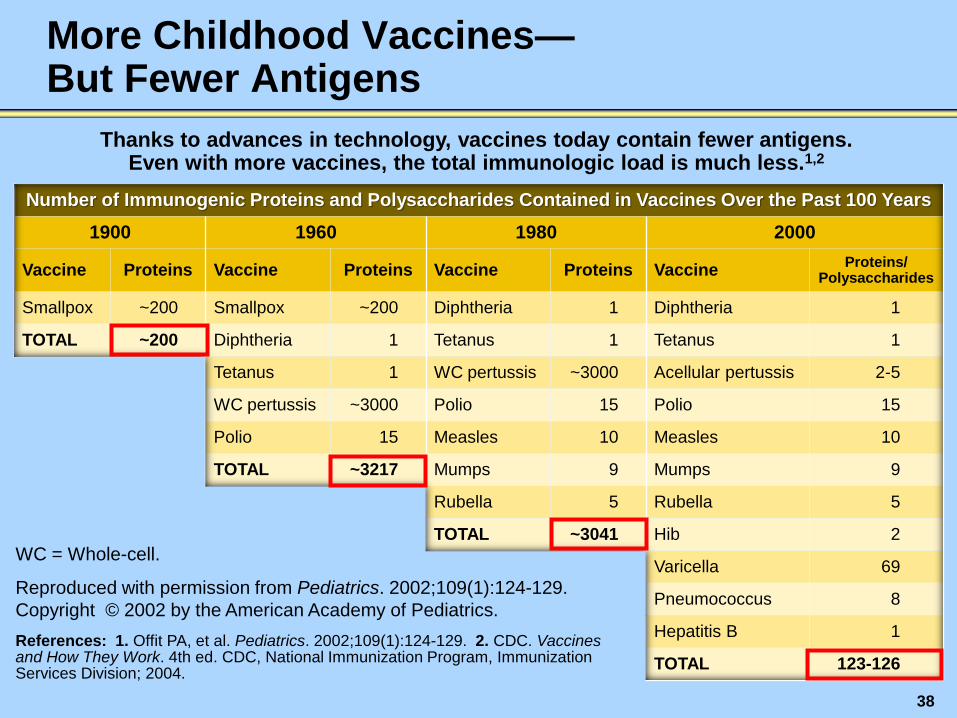
Number of Immunogenic Proteins and Polysaccharides Contained in Vaccines Over the Past 100 Years
1900 1960 1980 2000
Vaccine Proteins Vaccine Proteins Vaccine Proteins Vaccine Proteins/
Polysaccharides
Smallpox ~200 Smallpox ~200 Diphtheria 1 Diphtheria 1
TOTAL ~200 Diphtheria 1 Tetanus 1 Tetanus 1
Tetanus 1 WC pertussis ~3000 Acellular pertussis 2-5
WC pertussis ~3000 Polio 15 Polio 15
Polio 15 Measles 10 Measles 10
TOTAL ~3217 Mumps 9 Mumps 9
Rubella 5 Rubella 5
TOTAL ~3041 Hib 2
Varicella 69
Pneumococcus 8
Hepatitis B 1
TOTAL 123-126
More Childhood Vaccines— But Fewer Antigens
Thanks to advances in technology, vaccines today contain fewer antigens. Even with more vaccines, the total immunologic load is much less.1,2
References: 1. Offit PA, et al. Pediatrics. 2002;109(1):124-129. 2. CDC. Vaccines and How They Work. 4th ed. CDC, National Immunization Program, Immunization Services Division; 2004.
WC = Whole-cell.
Reproduced with permission from Pediatrics. 2002;109(1):124-129.
Copyright © 2002 by the American Academy of Pediatrics.
39
Time-based CPT®a Billing Codes for Office Visits With Vaccine-Hesitant Parents
• When 50% or more of the visit is spent on counseling (as
opposed to patient history or physical examination):
– Use 99214 if the visit lasts at least 25 minutes and less than 40 minutes
– Use 99215 if the visit lasts at least 40 minutes
• Keep in mind that time-based billing codes can be used only
if the topics of counseling are well documented
• If a parent is already known to be vaccine-hesitant and is
scheduling an appointment, be sure to:
– Give that parent a 30-minute slot
– Advise the staff to use a time-based billing code for that visit
a CPT (Current Procedural Terminology) is a registered trademark of the American Medical Association.
40
Providing Parents With Accurate Information
• Most parents seek out information about vaccine safety from
other people and from media outlets before taking their child to
be immunized1
– Parents are increasingly using the internet to obtain vaccine
information
• HCPs remain 1 of the most important sources of information and
advice for parents making immunization decisions and can help
build parental confidence in vaccines1-3
• Assisting HCPs in their efforts to communicate with parents
about vaccines should remain a priority for national, state, and
local immunization programs2
References: 1. Kennedy A, et al. Health Affairs. 2011;30(6):1151-1159. 2. Gust DA, et al. Pediatrics.
2008;122(4):718-725. 3. Freed GL, et al. Pediatrics. 2011;127(suppl 1):S107-S112.

41
Vaccine Hesitancy and Suboptimal Immunization Rates Among Adults
• Coverage rates remain suboptimal for most vaccines that are routinely
recommended for adults1,2
• 2010 National Foundation for Infectious Diseases telephone survey of
1013 adults3:
– 21% believe immunizations are optional for healthy adults
– 27% report refusing a vaccine offered to them by their HCP
Primary reason for refusal is lack of concern about getting the disease
• Many parents—even those whose children are fully vaccinated—may
hesitate to be vaccinated themselves
– Some are skeptical of the need for those immunizations
– Others harbor doubts about the safety and efficacy of 1 or more
immunizations
References: 1. CDC. MMWR. 2013;62(4):66-71. 2. CDC. Flu vaccination coverage, United States, 2011-12
influenza season. http://1.usa.gov/12wMN6y. Accessed June 7, 2013. 3. National Foundation for Infectious
Diseases Survey: Disconnect in What Doctors Think They Say About Vaccines and What Patients Hear.
November 2010. http://bit.ly/11pe9Vu. Accessed June 7, 2013.

42
Sanofi Pasteur’s ImmYOUnitySM Educational Campaign
• Helps answer questions about vaccines for family members of all ages
• Offers online and print material that HCPs can use to supplement discussions
about vaccination with patients and parents

43
“Infographics”: A Simple Way to Understand and Share Key Facts
• Consumer-friendly, balanced, science-based information
• Website content that can be shared via social media and e-mail
44
How ImmYOUnity Can Help
• Public health departments, health systems, clinics,
and others can link to www.vaccines.com from their
own websites
• ImmYOUnity brochures can be disseminated to
clinicians, patients, and parents
• Evolving campaign is open to input from HCPs and
families to further support efforts to educate and
immunize
– For more information, call 1-800-VACCINE (1-800-822-2463),
or contact a Sanofi Pasteur representative