[PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks...
17
Pediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013
Transcript of [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks...
![Page 1: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/1.jpg)
Pediatric Neurology Quick Talks
HypotoniaMichael Babcock
Summer 2013
![Page 2: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/2.jpg)
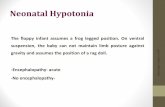
Scenario
• 2 do M in the NICU• Poor feeding and “weakness”• Not intubated• Delivered 37 weeks by C/S – failure to progress• Poor maternal pre-natal care• HC ~50%• Exam – axillary slippage, reduced spontaneous movements, +head lag,
normal suck. +awake
![Page 3: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/3.jpg)
Hypotonia – Localize –> Central or Peripheral
• Central (brain/spinal cord)– Normal/mild weakness– normal bulk– normal/increased reflexes– Dysmorphisms– encephalopathy
• Peripheral (Anterior horn, peripheral nerve, NMJ, muscle)
– Marked weakness– decreased bulk– decreased reflexes– no dysmorphisms– Awake, alert
![Page 4: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/4.jpg)
![Page 5: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/5.jpg)
Central Causes
• Sepsis• Maternal narcotics• Hypothyroid• Prematurity• HIE• Down's Syndrome• Prader-Willi• Inborn Errors of Metabolism
– Zellweger• Cerebral dysgenesis
![Page 6: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/6.jpg)
Peripheral Causes
• Anterior Horn– SMA– Pompe
• Peripheral Nerve (uncommon)– Inflammatory – GBS– Demyelinating– Axonal– Metabolic- Leigh
• Neuromuscular Junction– Myasthenias– Infantile botulism– Hypermagnesemia
• Muscle– Myopathy– Muscular dystrophy– Myotonic dystrophy– Metabolic myopathy
![Page 7: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/7.jpg)
Perkowski's top 5 not to miss causes of floppy baby
• Down's syndrome• Prader Willi• Pompe (have heart problems)• Zellweger• Spinal Muscular Atrophy• However, most common is HIE
![Page 8: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/8.jpg)
History
• Mother – systemic illness, fever, substance abuse• Pregnancy – polyhydramnios, fetal movement, abnormal lie• Delivery – complicated/prolonged, trauma, Apgars• Family history – delayed milestones, weakness, myotonia
![Page 9: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/9.jpg)
Exam – Assess Tone
• Tone is resistance to stretch forces, develops with nervous system development, low tone is normal for premature infants – Ballard testing.
• Resting posture – assess resting posture when infant is quiet/drowsy– Hypotonic infant – frog leg position– Long-standing immobility can cause joint contractures – arthrogryposis
• Passive manipulation– Infants develop increasing flexor tone in extremities – causes increased
recoil after limb is extended– Head control in vertical/horizontal suspension– Vertical suspension
![Page 10: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/10.jpg)
Ballard Testing – Testing tone
![Page 11: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/11.jpg)
Work Up
• Central– Electrolytes (Mg, Ca, Gluc)– TFT's– Brain imaging – U/S vs MRI– EEG– Karyotype, CMA– Metabolic work-up
• Peripheral– CK– EMG/NCS– muscle/nerve bx
![Page 12: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/12.jpg)
Spinal Muscular Atrophy (SMA)
• AR – SMN1 gene – SMN protein (survival motor neuron); SMN2 gene regulates severity
• Weakness and atrophy of muscles, including tongue
• Symmetric weakness, more proximal than distal, more severe in LE
• Tongue fasciculations• Absent DTRs• Normal intellectual capacity• Facial muscles typically spared
early on
• Types– Type 1 – infantile - Werdnig
Hoffman - <6mo. - never sit– Type 2 – intermediate -
Dubowitz – 6-18 months – never walk
– Type 3 – juvenile - Kugelberg-Welander – 18mo- 17 years. - able to walk initially, often lose this.
– Type 4 – adult-onset
![Page 13: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/13.jpg)
Myasthenias
• Congenital– Genetic disorder of NMJ– Hypotonia, weakness (ocular, bulbar, respiratory)
• Variable onset, sometimes in utero – arthrogryposis– Recurrent ALTEs– Fatigability, weak cry, feeding difficulties, episodic apnea– Sometimes respond to AchE inhibitors
• Transient neonatal– Transplacental transfer of AchR Antibodies.– 10-15% of infant of myasthenic mothers– Hypotonia, weakness—bulbar and respiratory, within 4 days of birth– Good response to AchE inhibitors
![Page 14: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/14.jpg)
Infant Botulism
• Weakness and hypotonia• Can have hx of honey ingestion; though contamination from soil is most
common• Constipation is often first sign• Eye findings, ophthalmoplegia – botulism is descending paralysis• Can test stool• Can give Human boutlinum immunoglobulin – 50mg/kg in first few days
shortens course• Often severe respiratory weakness requiring ventilation, prolonged course.
![Page 15: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/15.jpg)
Prep Question
During the health supervision visit for a 6 week old boy, his father expresses concern that his son “doesn’t look like” his other children. Growth parameters are normal except for a head circumference of 35.5 cm (<5th percentile).
On PE, you note that the infant does not appear to fixate or track your face visually. There is a “slip through” on vertical suspension and “draping over” on horizontal suspension. DTRs are brisk. Moro reflex is present and brisk. Of the following, the MOST likely cause of this infants hypotonia is:
• Anterior horn cell disease• Congenital brain malformation• Congenital myasthenic syndrome• Congenital myopathy• Spinal cord disease
![Page 16: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/16.jpg)
B. Congenital brain malformation
• Hypotonia– Localize! UMN vs. LMN signs, axial vs appendicular– Take into account growth parameters, especially HC, as well as
features such as tracking• Regarding other choices:
– A. anterior horn cell disease – wouldn't cause microcephaly or increased reflexes
– C. Congenital myasthenic syndrome – wouldn't cause microcephaly or brisk reflexes
– D. Congenital myopathy – no microcephaly or poor visual tracking– E. Spinal cord disease – wouldn't cause microcephaly or poor visual
tracking.
![Page 17: [PPT]PowerPoint Presentation - Vanderbilt University … · Web viewPediatric Neurology Quick Talks Hypotonia Michael Babcock Summer 2013 * * Scenario 2 do M in the NICU Poor feeding](https://reader031.fdocuments.in/reader031/viewer/2022022516/5aff90fd7f8b9a256b8eb9fa/html5/thumbnails/17.jpg)
References
Paediatr Child Health. 2005 September; 10(7): 397–400.; PMCID: PMC2722561; A schematic approach to hypotonia in infancy
Respiratory update.com







![How to Treat the Child with Hypotonia Presentation[1]](https://static.fdocuments.in/doc/165x107/61fc859d8d33c02b785e2618/how-to-treat-the-child-with-hypotonia-presentation1.jpg)