PPT
49
Increasing Survival in Sudden Cardiac Arrest (SCA): The Role of ICD Therapy
description
Transcript of PPT

Increasing Survival in Sudden Cardiac Arrest
(SCA): The Role of ICD Therapy

ObjectivesUpon completion of this activity, participants will be able to:
• Describe current trends in the epidemiology and etiology of sudden cardiac arrest (SCA).
• Assess the risk of SCA in ischemic and non-ischemic populations, including post-MI patients and HF patients.
• Describe the current evidence underlying the most recent ACC/AHA/ESC guidelines (2006) for the use of ICDs in patients at risk of SCA, and apply those guidelines.
• List risk-assessment tools being used in clinical practice or under investigation, and describe the current evidence for each.
• Describe the current CMS coverage for use of ICDs in patients at risk of SCA, and compare the economics of such use to other medical interventions.
• Assess their current use of ICDs in patients at risk for SCA.

Patient CaseHistory
76-y.o. white male
Type II DM, low-grade renal dysfunction; both well-controlled
3 years post-MI, successfully revascularized
NYHA functional class II; stable
LVEF is 32% (echo)
Compliant with meds: antiplatelet, beta-blocker, ACE-I, statin, DM regimen

Patient Case
Clinical Decisions
Should this patient be referred for an ICD evaluation?
What factors enter into your decision?
Is there anything else you'd want to know before making the decision?

Epidemiology and Etiology

Cardiovascular Disease Mortality Trends for Males and Females: United States: 1979-2003*
Heart Disease and Stroke Statistics — 2006 Update. CDC/NCHS. * Preliminary. AHA. www.americanheart.org
State-Specific Mortality from Sudden Cardiac Death. www.cdc.gov
400
420
440
460
480
500
520
79 80 85 90 95 00 03
Years
Dea
ths
in T
hous
ands
Males Females
0

SCA Mortality Trends
Age-adjusted cardiovascular deaths have
declined; however mortality due to Sudden
Cardiac Death has not.
Over 60% of coronary artery deaths are
attributable to sudden cardiac arrest
Goraya TY, et al. Am J Epidemiol. 2003; 157:763-770.
Centers for Disease Control. 1999. MMWR Morb Mortal Wkly Rep 2002; 57: 123-126

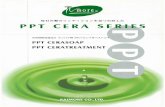
Leading Causes of Death in the US
National Vital Statistics Report. 2001;49;11.MMWR. 2002;51:123-126.
Sudden Cardiac Arrest (SCA)
0% 5% 10% 15% 20% 25%
Septicemia
Nephritis
Alzheimer’s Disease
Influenza/Pneumonia
Diabetes
Accidents/Injuries
Chronic Lower Respiratory Diseases
Cerebrovascular Disease
Other Cardiac Causes
All Cancers
SCA is a leading cause of death in the U.S., second to all cancers combined.

SCA Survival & Mortality Data
• At least 335,000 SCA deaths in the U.S. each year
• Only 5 to 10% survive first episode of SCA
• Roughly two-thirds of SCA deaths occur out-of-hospital
Seidl K, Senges J. Card Electrophysiol Rev. 2003;7:5-13.
Heart Disease and Stroke Statistics — 2005 Update. AHA. www.americanheart.org
Crespo EM, Kim J, Selzman KA. Am J Med Sci. 2005;329:238-246.
Zheng ZJ, et al. Circulation. 2001;104:2158-2163.
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484.

Secondary Prevention of
Sudden Cardiac Arrest

Patient Case
History • 54-y.o. African-American female• Ischemic cardiomyopathy• NYHA functional class I• LVEF = 28% per echo at your institution• Long-time heavy smoker; has COPD• Compliant and stable on optimal medical therapy• Syncopal episodes

Patient Case
Clinical Decisions
Should this patient be referred for an ICD evaluation?
What factors enter into your decision?
Is there anything else you'd want to know before making the decision?

Key Randomized Clinical Trials
Adapted from: DiMarco JP. N Engl J Med. 2003;349:1836-47. www.medscape.com
Young JB. Sudden cardiac death in heart failure. www.medscape.com
ICD therapy for the secondary prevention of SCA
Mortality
(%)
Trial N Age (yrs) Mean LVEF (%)
Follow-up (mos)
Control Therapy
Control ICD P
AVID 1016 65 ± 10 35 18 ± 12 Amiodarone or sotalol
24.0 15.8 .02
CIDS 659 64 ± 9 34 36 Amiodarone 29.6 25.3 .14
CASH 288 58 ± 11 45 57 ± 34 Amiodarone or metoprolol
44.4 36.4 .08

2006 ACC/AHA/ESC Guidelines for the Management of Ventricular
Arrhythmias: Secondary Prevention of SCD
ICD Class I Recommendation:• Patients with a history of SCA, VF, hemodynamically
unstable VT, or unexplained syncope
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484

Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.
Patients with a previous cardiac arrest are at high risk for subsequent SCA events but account for a small percentage
of annual sudden deaths
MADIT I, MUSTT
AVID, CASH, CIDS
SCD-HeFT,MADIT II

Primary Prevention of Sudden Cardiac
Arrest

Patient Case
History • 52 year old woman• Moderate alcohol consumption, has stopped
since MI• Lives alone in rural community; manages on-line
content for a large dog food manufacturer• PMHX: MI 1 year ago, echo on discharge
was 35%• Medications: BB, ACE-I, lipid-lowering agent,
clopidorgrel, omega-3

Patient Case
Clinical Decisions
Should this patient be referred for an ICD evaluation?
What factors enter into your decision?
Is there anything else you'd want to know before making the decision?

SCA Relationship to MI
• A previous MI can be identified in as many as 75% of SCA patients.
• A previous MI as a single risk-factor raises the one-year risk of SCA by 5%.
• The five-year risk of SCA is 32% for patients with all of these risk-factors:• history of MI • non-sustained, inducible, non-suppressible VT• LVEF ≤ 40%
Sudden Cardiac Arrest Fast Facts. HRS. www.hrsonline.org
Risk factors for sudden cardiac death. www.heartinstitute.org.au/Community/scdMain.asp
Buxton AE, et al. N Engl J Med. 1999;341:1882-1890.

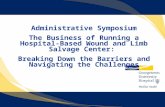
Time Dependence of Mortality Risk Post-MI
Prediction of Sudden Cardiac Death After Myocardial Infarction in the Beta-Blocking Era1
• 700 post-MI patients; ~ 95% on beta-blockers 2 years after discharge.
• The epidemiologic pattern of SCD was different from that reported in previous studies.
Arrhythmia events did not concentrate early after the index event; most occurred > 18 months post-MI.
1 Huikuri HV. J Am Coll Cardiol. 2003;42:652-658.
TotalMortality
CardiacMortality
Non-SCD
SCDCu
mu
lati
ve
Ev
en
ts (
%)
18
15
12
9
6
3
18
15
12
9
6
3
20 40 60 20 40 60
Follow-Up (months) Follow-Up (months)

14
11.6
8.47.89
8.2
4.9
7.2
0
2
4
6
8
10
12
14
16
1-17 mo 18 - 59 mo 60 - 119 mo > 120 mo
ConvICD
(n = 300) (n = 283) (n = 284) (n = 292)Hazard Ratio .98
(p = 0.92)0.52
(p = 0.07)0.50
(p = 0.02)0.62
(p = 0.09)
Wilber, D. Circulation. 2004;109:1082-1084.
Relation of Time from MI to ICD Benefit
in the MADIT-II Trial
Time from MI
% M
ort
alit
y fo
r E
ach
T
ime
Per
iod

SCA Relationship to HF
• Patients with HF are overall at 6-9 times higher risk for SCD than general population
• As HF progresses, pump failure (rather than SCA) becomes relatively more likely as the cause of death
Heart Disease and Stroke Statistics – 2005 Update. AHA. www. americanheart.org

Severity of Heart FailureModes of Death
MERIT-HF Study Group. Lancet.1999;353:2001-2007.
12%
24%64%
CHF
Other
SuddenDeath(N = 103)
NYHA II
26%
15%59%
CHF
Other
SuddenDeath(N = 103)
NYHA III
56%
11%
33%
CHF
Other
SuddenDeath(N = 27)
NYHA IV SCA Pump Failure
NYHA Class II 64% 12%
NYHA Class III 59% 26%
NYHA Class IV 33% 56%

SCA Relation to LVEF
0
1
2
3
4
5
6
7
8
0-30% 31-40% 41-50% >50%
Gorgels PMA. European Heart Journal. 2003;24:1204-1209.
LVEF
% S
CA
Vic
tim
s
7.5%
5.1%
2.8%
1.4%
EF is an Important Risk Stratifier

Key Randomized Clinical Trials
Adapted from: DiMarco JP. N Engl J Med. 2003;349:1836-47. www.medscape.comKadish A, et.al. N Engl J Med 2004;350:2151-8.Young JB. Sudden cardiac death in heart failure. www.medscape.com
ICD therapy for the primary prevention of SCA
Mortality (%)
Trial N Age (yrs)
Mean LVEF (%)
Follow-up (mos)
Control Therapy
Control ICD P
SCD-HeFT
2521 60.1 25 45.5 Optimal Medical Therapy
36.1 28.9 .007
MADIT 196 63 ± 9 26 27 Conventional 38.6 15.7 .009
MADIT II 1232 64 ± 10 23 20 Optimal Medical Therapy
19.8 14.2 .007
MUSTT 704 67 ± 12 30 39 No EP-guided therapy
48 24 .06
DEFINITE 458 58 21 29.0±14.4 Optimal Medical Therapy
14.1 7.9 .08

Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.
Heart Failure and Left Ventricular Dysfunction are indicators of SCA risk
MADIT I, MUSTT
AVID, CASH, CIDS
SCD-HeFT,MADIT II

2006 ACC/AHA/ESC Guidelines for the Management of Ventricular
Arrhythmias: Primary Prevention of SCD
ICD Class I Recommendations:• Patients with ischemic cardiomyopathy who are at least 40 days post-
MI with an LVEF ≤ 30 - 40% and NYHA functional class II or III
• Patients with NYHA Class II-III, LVEF ≤ 30 - 35%, non-ischemic cardiomyopathy
• Patients who are at high risk of SCA due to genetic disorders such as long QT syndrome, Brugada syndrome, hypertrophic cardiomyopathy and arrhythmogenic right ventricular dysplagia (ARVD).
ICD Class II Recommendation:• Ischemic and non-ischemic patients with NYHA functional class I,
LVEF ≤ 30-35%
Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484

Current CMS ICD Coverage*• In brief, this policy expands coverage for:
1) Patients with ischemic dilated cardiomyopathy (IDCM), prior MI, NYHA Class II & III heart failure, LVEF less than or equal to 35%
2) Patients with non-ischemic dilated cardiomyopathy (NIDCM) > 3 months, NYHA Class II & III heart failure, LVEF less than or equal to 35%
Overall, this NCD covers the SCD-HeFT population and all the MADIT II population.
* ICD coverage expanded in January 2005 and updated in April 2006.

Discussion: ICD Contraindications
• Standard Contraindications for ICD Therapy– Hospitalized patients with advanced age– Advanced (NYHA class IV) HF and limited life expectancy– Patients whose VT’s may have transient or reversible causes– Patients with incessant VT or VF– Patients who have a unipolar pacemaker
• Questions
Are there patients who are indicated but who should not get an ICD?Who makes the decision on whether or not an ICD is offered?

Beyond EF

Microvolt T-Wave Alternans
• Noninvasive, ECG-based test• HR elevation by exercise, atrial pacing,
or dobutamine infusion• Measures beat-to-beat microvolt
variations in the shape, amplitude, or timing of the ECG T-wave

Microvolt T-Wave Alternans• Sometimes used as a risk-stratification tool
• Negative result may suggest low risk of SCA• High negative-predictive value, low positive-
predictive value• CMS has approved Medicare coverage when
spectral-analytic method used• Microvolt T-wave alternans has received a Class IIa
recommendation in the 2006 ACC/AHA/ESC Guidelines
• The guidelines do not state that an ICD is not recommended if the T-wave test is negative.
• The outcome of the test also does not change the indication for ICD.
Bloomfield DM, et al. J Am Coll Cardiol. 2006:47:456-463Gehi AK, et al. J Am Coll Cardiol. 2005:46(1):75-82Zipes, DP, et al. 2006 ACC/AHA/ESC Practice Guidelines 5. Circulation. 2006;114;385-484CMS: Decision Memorandum for Microvolt T-wave Alternans Testing. www.cms.hhs.gov

Microvolt T-Wave Alternans: Issues
• Patients must be in sinus rhythm (but up to 30% of patients at risk have AF)
• A patient must sustain a heart rate of 105 for 10 minutes, which may be difficult for patients on beta-blockers.
• Can be indeterminate• Non-sustained MTWA in up to 10% of normals• Value beyond LVEF not fully established, further
studies underway• Cost-effectiveness being assessed

Many methods to further risk stratify patients at risk for SCA have been studied...
Test Objective Sensitivity
(%)
Specificity
(%)
Limitations
Echo Measurement of LVEF
55–65 75–80
HR
variability
Assessment of low heart rate variability
38–62 75–88 Multiple non-standardized methods
EP Study Induction of VA’s 48–73 65–93 Invasive, expensive
Signal
Averaged ECG
(SAECG)
Induction of late potentials
56-68 74–81 Not useful in non-ischemic cardiomyopathy
Microvolt
T-Wave
Alternans (MTWA)
Identification of repolarization abnormalities
77–93 37–83 Cannot be used in AF
Siddiqui A, Kowey PR. Curr Opin Cardiol. 2006;21:517-25.
Prior SG, et al. Eur Heart J, Vol 22:16:August 2001
But a reduced EF remains the single most important risk factor for overall mortality and sudden cardiac death.

The Economics of Therapy

$0
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
$140,000
$160,000
$180,000
$200,000
Incremental Cost-EffectivenessCardiovascular Interventions
HypertensionTherapy(diastolic95 - 104mmHg)
Expensive
BorderlineCost-Effective
Cost-Effective
HighlyCost-Effective
Incr
emen
tal
Co
st p
er L
ife-
Yea
r S
aved
EconomicallyUnattractive
Lovastatin(chol. =
290 mg/dL,50 yrs old,
male, no riskfactors)
PTCA(chronic CAD,severe angina
1 VD)
CABG(chronic
CADmild angina,
3 VD)
End Stage Renal
Disease Treatment
Exercise SPECT (atypical
angina who can walk
on treadmill)
RoutineCoronary
Angiography(35 - 84 yrs
old, low risk MI,has CHF)
$8,461$17,701
$40,750
$67,000
$135,000
$150,000
Carotid Disease
Screening(65 yrs old,
male, no
symptoms)
$1,000,000
$120,000
Moss AJ. Satellite Symposium, 2003.
Kupersmith J. Progress in Cardiovascular Diseases. 1995;37:5:307-346.
Stanton M. Circulation. 2000;101:1067-1074.

Incremental Cost-Effectiveness
of ICD Therapies
Al-Khatib SM, et al. Ann Intern Med. 2005;142:593-600.Larsen G, et al. Circulation. 2002;105:2049-2057.Mark DB. Circulation. 2006;114:135-142. http://circ.ahajournals.org
Incr
emen
tal
Co
st p
er L
ife-
Yea
r S
aved
MADIT-IIICD2
AVIDICD3
$50,000$67,000
Expensive
BorderlineCost-Effective
Cost-Effective
HighlyCost-Effective
EconomicallyUnattractive
SCD-HeFTICD1
$38,000
$0
$20,000
$40,000
$60,000
$80,000
$100,000
$120,000
$140,000
$160,000
$180,000
$200,000

Number-Needed-to-Treat (NNT) to Save One Life for ICDs and
Various Drugs
Camm J, Klein H, Nisam S. European Heart Journal. doi:10.1093/eurheart/eji166; 2006
MADIT II(3 year)
Incr
emen
tal
Co
st p
er L
ife-
Yea
r S
aved
SAVE(3.5 year)
MUSTT(5 year)
MADIT(2.4 year)
AVID(3 year)
SCDHeFT(5 year)
Merit-HF(1 year)
4S(6 year)
4
11
9
20
26
28
14
0
5
10
15
20
25
30

Implications for Real-World Practice

Patient CaseHistory • 78 year old man• Wheelchair bound due to automobile accident• Plays bridge competitively• Lives in assisted-living• PMHX: NIDCM, HF class II, sinus node
dysfunction treated with a pacemaker, EF measured in 2000 was 30%
• Medications: ACE-I, BB, Diuretic

Patient Case
Clinical Decisions Should this patient be referred for an ICD
evaluation?
What factors enter into your decision?
Is there anything else you'd want to know before making the decision?

Myerburg RJ, et al. Circulation. 1998. 97:1514-1521.
Sudden Death Risk
MADIT I, MUSTT
AVID, CASH
SCD-HeFT,MADIT II
How can a practice effectively identify patients at-risk?

Discussion: Practice Realities
• QuestionsIf you were to implement a new SCA algorithm
in your practice, what would happen?
What do you see as possible problems in
implementing the guidelines?
Are there situations that are unique to your
practice?

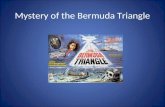
ICD Treatment Algorithms

EF Clinic Program Patient Screening Pathway
(The Ohio Heart & Vascular Center)
Determine EF
Does patient havehistory of cardiac
arrest, VF, orsymptomatic VT?
Non-Ischemic
Consult EP for possible CRT-D
Optimize therapies or consult HF specialist
EF ≤ 35%
Ischemic
PATIENT
40 days post MI with EF ≤ 30%
NYHA Class I CHF
EF > 35%
40 days post MI OR
3 months post revascularization
Consult EP for possible ICD
3 months post diagnosis
1. Consider referral to HF Specialist or HF Program.
2. Repeat diagnostics with change of symptoms.
Class III or IV CHFand QRS > 120 ms
Consult EP for possible ICD
Consult EP for possible ICD
Is patient on optimal medical
therapy?YES
YES
NO
Note: Pathway only begins after optimal medical therapy & coronary evaluation / intervention as appropriate
Consult EP for possible ICD
NYHA Class II or III CHF
This is a general protocol to assist in the management of patients. This protocol is not designed to replace clinical judgment or individual patient needs.

ICD
ICD Practical FlowchartLVEF ≤ 35% Optimal Medical Therapy
NYHA Class III – IV, Wide QRS? YESNO
CRT-D
NO
Prior MI No Prior MI
EF ≤30%MADIT II
NYHA II/III
EPS + MADIT-1
NYHA II/III
Syncope
OROR
Source: Narayan SM. Current Issues in Cardiology. 2005:32:3.
COMPANION
SCD-HeFT

Key Points
• The majority of cases are in patients with:– Coronary artery disease, previous MI– Low left ventricular ejection fraction– Dilated cardiomyopathy and heart failure
• Defibrillation is the only effective treatment option• High-risk patients can be evaluated for known
risk factors before they experience a Sudden Cardiac Arrest– EF remains a key indicator

In Summary…
• SCA is a leading cause of death
• There is solid clinical evidence for ICDs as:– The only effective means to prevent SCD– Superior to optimal medical therapy
• ICDs are cost-effective
• There are practical ways to assess SCA risk in ischemic and non-ischemic populations
Sudden Cardiac Death CAN be Prevented With an ICD

Brief Statement
Medtronic ICDs
IndicationsMedtronic implantable cardioverter defibrillators (ICDs) are indicated for ventricular antitachycardia pacing and ventricular defibrillationfor automated treatment of life-threatening ventricular arrhythmias.
ContraindicationsMedtronic ICDs are contraindicated in patients whose ventricular tachyarrhythmias may have transient or reversible causes, patientswith incessant VT or VF, patients who have a unipolar pacemaker, and patients whose primary disorder is bradyarrhythmia.
Warnings/PrecautionsChanges in a patient¹s disease and/or medications may alter the efficacy of the device¹s programmed parameters. Patients shouldavoid sources of magnetic and electromagnetic radiation to avoid possible underdetection, inappropriate sensing and/or therapydelivery, tissue damage, induction of an arrhythmia, device electrical reset, or device damage. Do not place transthoracic defibrillationpaddles directly over the device.
Potential ComplicationsPotential complications include, but are not limited to, rejection phenomena, erosion through the skin, muscle or nerve stimulation,oversensing, failure to detect and/or terminate tachyarrhythmia episodes, acceleration of ventricular tachycardia, and surgicalcomplications such as hematoma, infection, inflammation, and thrombosis.
See the device manual for detailed information regarding the implant procedure, indications, contraindications, warnings, precautions,and potential complications/adverse events. For further information, please call Medtronic at 1 (800) 328-2518 and/or consultMedtronic¹s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.