Ppt mri brain
108
BASICS OF MRI BRAIN BASICS OF MRI BRAIN PRESENTER:DR. ARSHAD YAHYA MODERATOR: DR. K S ANAND
-
Upload
arshad-yahya -
Category
Health & Medicine
-
view
132 -
download
23
Transcript of Ppt mri brain

BASICS OF MRI BRAINBASICS OF MRI BRAIN
PRESENTER:DR. ARSHAD YAHYA
MODERATOR: DR. K S ANAND

HISTORY HISTORY ►Dr Isidor Rabi (Nobel in 1944!) He succeeded in
detecting and measuring single states of rotation of atoms and molecules, and in determining the magnetic moments of the nuclei .
►CJ Gorter, coined the term ‘Nuclear Magnetic Resonance’ in 1942.
►Bloch and Purcell were awarded the Nobel Prize for Physics in 1952
►Found that when certain nuclei were placed in magnetic field they absorbed energy in electromagnetic spectrum and re emit energy when regained their original position.

““We are so close to the man We are so close to the man behind MRI”behind MRI”
►Prof Peter Mansfield was awarded Nobel in 2003 for his discoveries in MRI (with Prof Paul C Lauterbur of USA)
►Peter Mansfield is from Nottingham University, UK
►Described the use of magnetic field gradients to acquire spatial information in NMR experiments

MRI principleMRI principle
MRI is based on the principle of nuclear magnetic resonance (NMR)
Two basic principles of NMR1.Atoms with an odd number of protons or
neutrons have spin 2.A moving electric charge, be it positive or
negative, produces a magnetic field

We all are made up of We all are made up of elementselements
►92 elements occur naturally on earth.
►Human body is built of only 26 elements.
►Oxygen, hydrogen, carbon, nitrogen elements constitute 96 % of human body mass.
►Oxygen is 65 % of body mass; carbon is 18.5 %, hydrogen 9.5 %, nitrogen 3.2 %.

Nucleus needs to have 2 properties:◦ Spin
◦ charge
Nuclei are made of protons(3 quark) and neutrons◦ Both have spin ½
◦ Protons have charge
Pairs of spins tend to cancel, so only atoms with an odd number of protons or neutrons have spin ◦ Good MR nuclei are 1H, 13C, 19F, 23Na, 31P

SPIN!!SPIN!!• Protons and neutron spins
are known as nuclear spins.
• An unpaired component has a spin of ½ and two particles with opposite spins cancel one another.
• In NMR it is the unpaired nuclear spins that produce a signal in a magnetic field

Why Hydrogen ions are used Why Hydrogen ions are used in MRI? in MRI?
Hydrogen nucleus has an unpaired proton which is positively charged
Hydrogen is abundant in the body in the form of water and fat
Every hydrogen nucleus is a tiny magnet which produces small but noticeable magnetic field
Hydrogen atom is the only major species in the body that is MR sensitive
Proton is not only positively charged, but also has magnetic spin (wobble)!
MRI utilizes this magnetic spin property of protons of hydrogen to elicit images
Essentially all MRI is hydrogen (proton) imaging

But why we can’t act like But why we can’t act like magnets?magnets?
The protons (i.e. Hydrogen ions) in body are spinning in a haphazard fashion, and cancel all the magnetism. That is our natural state!

When placed in a large magnetic field, hydrogen atoms have a strong tendency to align in the direction of the magnetic field
Inside the bore of the scanner, the magnetic field runs down the center of the tube in which the patient is placed, so the hydrogen protons will line up in either the direction of the feet or the head.
The majority will cancel each other, but the net number of protons is sufficient to produce an image.
5-spin down 7spin up

Net magnetizationNet magnetization Half of the protons align along the magnetic field and rest are
aligned opposite. At room temperature, the population ratio of anti- parallel versus parallel protons is roughly 100,000
to 100,006 per Tesla of B0
These extra protons produce net magnetization vector (M)
Net magnetization depends on B0 and temperature

PrecessionPrecession The static field causes the spinning
proton to ‘wobble’ in a regular manner from it’s original axis to axis of magnetic field called ‘PRECESSION’

Larmor frequencyLarmor frequencyNatural precession frequency of
proton with in a magnetic field of given strength

Manipulating the net Manipulating the net magnetizationmagnetization
Magnetization can be manipulated by changing the magnetic field environment (static, gradient, and RF fields)
Static field vary in space but not over time during image acquisation.by magnet itself or perturbation by materials with different magnetic permeability.
RF waves are used to manipulate the magnetization of H nuclei
Externally applied RF waves perturb magnetization into different axis (transverse axis). Only transverse magnetization produces signal.
When perturbed nuclei return to their original state they emit RF signals which can be detected with the help of receiving coils

IN A NUT SHELLIN A NUT SHELL

Measuring the MR Signal:◦ the moving proton vector
induces a signal in the RF antenna
◦ The signal is picked up by a coil and sent to the computer system.
the received signal is sinusoidal in nature
◦ The computer receives mathematical data, which is converted through the use of a Fourier transform into an image.
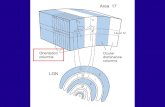
Measuring the MR Signalz
y x
RF signal from precessing protons
RF antenna

Now, we re-transmit the Now, we re-transmit the energy for image processingenergy for image processing►The emitted energy is too small
(despite 2500 times the magnetic field with resonance RF pulse) to convert them into images.
►Hence, repeated “ON-OFF” of RF pulses are required.
►The emitted energy is stored (K-space), analysed and converted into images.

RESONANCE?RESONANCE?
►When the radio frequency pulse frequency matches the precession frequency of proton

Energy Absorption:◦The MRI machine applies radio frequency (RF) pulse that is specific to hydrogen.
◦The RF pulses are applied through a coil that is specific to the part of the body being scanned.

T1 and T2 relaxationT1 and T2 relaxationWhen RF pulse is stopped higher energy gained by
proton is retransmitted and hydrogen nuclei relax by two mechanisms
T1 or spin lattice relaxation- by which original magnetization (Mz) begins to recover.
T2 relaxation or spin spin relaxation - by which magnetization in X-Y plane decays towards zero in an exponential fashion. It is due to incoherence of H nuclei.
T2 values of CNS tissues are shorter than T1 values

T1 relaxationT1 relaxationAfter protons are
Excited with RF pulse
They move out of
Alignment with B0
But once the RF Pulse
is stopped they Realign
after some Time And
this is called t1 relaxation
T1 is defined as the time it takes for the hydrogen nucleus to recover
63% of its longitudinal magnetization

T2 relaxation time is the time for 63% of the protons to become dephased owing to interactions among nearby protons.

T2* RelaxationT2* RelaxationDue to combined loss of phase coherence from both
static and time varying magnetic field in homogenity.
Static magnet field in homogenity are constant in time
signal loss can be recovered by use of 2nd 180* pulse..rephasing the nuclei
Time varying magnetic field-water molecule move rapidly …acquire different area of different magnetic field…precess at different rate..goes out of phase
Not static so can’t be reversed in to phase of coherence

TR and TETR and TE TR (repetition time) : the time between two excitations is called repetition
time TE (echo time) : time interval in which signals are measured after RF
excitation
By varying the TR and TE one can obtain T1WI and T2WI
In general a short TR (<1000ms) and short TE (<45 ms) scan is T1WI
Long TR (>2000ms) and long TE (>45ms) scan is T2WI
Long TR (>2000ms) and short TE (<45ms) scan is proton density image

ParametersParametersImage contrast controlled by:
1- Extrinsic Contrast parameters:TR, TE.
2- Intrinsic Contrast parameters:T1 Recovery, T2 Decay, Proton
Density, Flow & Apparent Diffusion Coefficient

T1 RecoveryT1 Recovery
Caused by EXCHANGE OF ENERGY FROM
NUCLEI TO THEIR SURROUNDING ENVIRONMENT OR LATTICE
"Spin Lattice Energy Transfer"and realign in B0this occur in exponential processat different rates in different tissue
NB: Molecules are constantly in motion; Rotational and Transitional

Excited dipole can relax only if it can transfer energy into lattice.
These molecular energy are present in the form of rotational and vibrational motion of molecules.
Certain types and structures of molecules will be far more efficient in accepting these energies as it will correspond more closely to larmour frequency

Frequencies that are too high or too low will not interact efficiently with nuclear dipole, T1 relaxation….slowed.
When proton dipole undergo faster T1 relaxation more of their longitudinal vector is available with each succeeding pulse…..more signal.

T1 RecoveryT1 Recovery
T1 in FatT1 in Fat T1 in WaterT1 in Waterabsorb energy absorb energy quicklyquickly
T1 is very shortT1 is very short
i.e. nuclei dispose i.e. nuclei dispose their energy to their energy to surrounding fat surrounding fat tissue and return to tissue and return to B0 in very short B0 in very short time time
FATFAT
inefficient at inefficient at receiving energyreceiving energy
T1 is longerT1 is longer
i.e. nuclei take a lot i.e. nuclei take a lot longer to dispose longer to dispose energy to energy to surrounding water surrounding water tissuetissue
WATERWATER

Myelin has slowing effect on motion of adjacent H2O….relatively bright on T1W
Very large, solid structure such as bone or protein(ligament) have proton …..immobile
Low signal, because rotational and vibrational frequencies have been slowed to point, they are no longer optimal for relaxation.

Proton on cholesterol and lipid membrane have poor mobility …long T1 as opposed to adipose fat having molecule in oil, mobile relax more quickly
Paramagnetic material also decreases T1 relaxation as can non paramagnetic calcium salts


T2 DecayT2 DecayThose tissues having constituent
which moves fast loses coherence very late ….long T2 (water)
Water tumbles rapidly in space..any magnetic field distortion are rapidly averaged out.
Adjacent water molecule have similar magnetic field …nuclear dipole dephase very slowly.

Fat being larger molecule than water moves slowly in space…loses coherence early than free water.
Less coherent movement give low signal on T2.
Paramagnetic substances(iron)distort magnetic field…..loss of coherence

Different tissues have different relaxation times. These relaxation time differences is used to generate image contrast.

Types of MRI imagingsTypes of MRI imagings
T1WIT1WI T2WIT2WI FLAIRFLAIR STIRSTIR DWIDWI ADCADC GREGRE MRSMRS MTMT Post-Gd imagesPost-Gd images
MRAMRA MRVMRV

Vector diagram of SE Vector diagram of SE SequenceSequence

T1 & T2 W IMAGINGT1 & T2 W IMAGING

CT SCAN
MRI T1 Weighted
MRI T2 Weighted
MRI T2 Flair

T1W PULSE SEQUENCE

Shorter the TE less decay of signalBest signal to noise ratio with short
TET1 and proton-W ….highest
anatomical detailT1 field strength dependentAlso varies in different instrument
and investigatorNot useful for absolute comparison
with disease process.

T1 RecoveryT1 Recovery
Short TR T1 contrast
(T1 Weighted)
TR 300-600 msTE 10-30 ms

T2W PULSE SEQUENCE

Most pathologic process exhibit prolonged T2
Utilizing long TE discrimination of normal vs abnormal tissue is enhanced

T2 DecayT2 Decay
Long TE T2 contrast
(T2 Weighted)
TR 2000 msTE 70 ms



Confusing…evolution of Confusing…evolution of hematomahematomaHyper acute(mts…hrs):oxyHb…O2
binds to 6th location on iron in heme of HbO2…strong ligand, significantly split energy
level of iron….in low spin state…not paramagnetic
O2Hb blood will have long T1…dark on T1W image
Any T1 shortening occurs due to water binding transiently to hydration layer of protein..shortening T1…iso intense
Due to free flowing without paramagnetic property T2 is long….bright on T2W.



Acute phase deoxyHb(hrs….days):
Fe in deoxyHb is in ferrous state….no O2 present
High spin state, paramagnetic because of presence of 4 unpaired electron….should cause shortening of T2 with brightness on T1W.
When O2 falls of Hb , iron molecule retract slightly inside the porphyrin ring…allosteric shift of HB


Iron is pulled out of plane of porphyrin, water is excluded from sensing the paramagnetic effects of iron.
For significant paramagnetic effect water must transiently bind to iron…
On T1W deoxy Hb …isointense with water.
Immobilization of fibrin,Hb, paramagnetic iron molecule with in semisolid gelatinaous clot reduces the mobility of these substances….disturbing local magnetic field
Rapid dephasing and loss of signal inT2W


MetHb-subacute phase(3d…18 month)
metHb is formed with oxidation of iron from ferrous to ferric form
With loss of additional electron, smaller ferric ion moves back into porphyrin ring…
Available to exchange with relax bound water molecules
Paramagnetic effect …relaxation of T1 becomes short…bright onT1W


In early stage red cell membrane is still intact and paramagnetic substance remain in RBC …immobilized in space
Due to early loss of coherence T2 short…dark in T2W.
In later part as clot dissolve local variation in magnetic field averaged out by tumbling of water and iron
Dephasing lessened…image bright on T2W because of increased water content



Chronic phase hemosiderin formation
Blood breakdown occurs..iron falls off the heme molecule….hemosiderin formed with microglia
Hemosiderin insoluble and rigidly held in space…little effect on T1 relaxation….minimal darkening on T1W
With al SE imaging,T1W image have contribution of T2 W because of echo time..minimal darkening onT1W.
On T2W due to interferance of local magnetic field by large immoble fibrin…dephasing occurs early …dark on T2W

Infarct Infarct Acute : T1W –Isointense hypo
intense T2W-Hyper intenseSub acute: T1W-Low
signal,increasedsignal in peripheral region..hemorrhage(metHb)
T2W- High signal Chronic:T1W-low signal T2W-High siignal

Dark on T1Dark on T1Edema, tumor, infection,
inflammation, hemorrhage(hyperacute, chronic)
Low proton density, calcification
Flow void

Bright on T1Bright on T1Fat, subacute hemorrhage, melanin, protein rich fluid.
Slowly flowing blood
Paramagnetic substances(gadolinium,copper,manganese)
9

Bright on T2Bright on T2Edema, tumor, Infection,
inflammation, subdural collection
Met hemoglobin in late sub acute hemorrhage

Dark on T2Dark on T2Low proton
density,calcification,fibrous tissueParamagnetic substances(deoxy
hemoglobin,methemoglobin(intracellular),ferritin,hemosiderin,melanin.
Protein rich fluidFlow void

Which scan best defines the Which scan best defines the abnormalityabnormalityT1 W Images:Subacute HemorrhageFat-containing structuresAnatomical Details
T2 W Images:EdemaDemyelinationInfarctionChronic Hemorrhage
FLAIR Images:Edema, Demyelination Infarction esp. in Periventricular location

Proton density imagingProton density imaging
A proton density image is one where the difference in the numbers of protons per unit volume in the patient is the main determining factor in forming image contrast.
Proton density weighting is always present to some extent.

Long TR and short TE

In order to achieve proton density weighting, the effects of T1 and T2 contrast must be diminished,
so that proton density weighting can dominate.
A long TR allows tissues e.g. fat and water to fully recover their longitudinal magnetisation and therefore diminishes T1 weighting.
A short TE does not give fat or water time to decay and therefore diminishes T2 weighting

T1PD T2

FLAIR & STIRFLAIR & STIR

Short TI inversion-recovery Short TI inversion-recovery (STIR) sequence (STIR) sequence In STIR sequences, an inversion-
recovery pulse is used to null the signal from fat (180° RF Pulse).
When NMV of fat passes its null point , 90° RF pulse is applied.
As little or no longitudinal magnetization is present and the transverse magnetization is insignificant.
It is transverse magnetization that induces an electric current in the receiver coil so no signal is generated from fat.

Longer TE used..both long T1 and T2 …bright

STIR allows only short time between 180 deg. Pulse and second 90 deg. Pulse.
If TE is kept prolonged, effect of T1 and T2 on lesion detection can be additive.
T1 and T2 of most pathologic lesion are prolonged.
Long TE selection…substances having both LONG T1 and T2 will be bright.
STIR also suppress substances with short T1….hemorrhage, gd-enhancement.


Fluid-attenuated inversion Fluid-attenuated inversion recoveryrecovery(FLAIR)(FLAIR)First described in 1992 and has
become one of the corner stones of brain MR imaging protocols
An IR sequence with a long TR and TE and an inversion time (TI) that is tailored to null the signal from CSF


Particularly helpful in evaluating periventricular white matter lesion.
Water bound to complex molecule with in plaque has relatively shorter T1 than free water with in ventricle.
Long inversion time effectively suppress free water…csf….nulled.
Lesion that contain complex, partially bound water (less mobile)…shorter T1 than free water….not nulled.

Long TE …used…result in T2W Sequence…..additional effect for contrast effect of tissue with prolonged T2 and short T1(White matter lesion)
Effective in high lightening lesion…demyelination, stroke, Ischemic gliosis and tumor
Sensitive but less specific

Normal partially myelinated white matter tract….highlighted
Protein rich pituitary stalk….normally bright on FLAIR.
More sensitive for detection of acute infarct…differentiate it from cystic encephalomalacia
Useful in SAH …removes CSF signal


T2 WFLAIR

FLAIR
FLAIR


GREGRE

GREGRE In a GRE sequence, an RF pulse is
applied that partly flips the NMV into the transverse plane (variable flip angle).
Gradients, as opposed to RF pulses, are used to dephase (negative gradient) and rephase (positive gradients) transverse magnetization.
Because gradients do not refocus field inhomogeneities, GRE sequences with long TEs are T2* weighted (because of magnetic susceptibility) rather than T2 weighted like SE sequences


GRE Sequences contd:
This feature of GRE sequences is exploited- in detection of hemorrhage, as the iron in Hb becomes magnetized locally (produces its own local magnetic field) and thus dephases the spinning nuclei.
The technique is particularly helpful for diagnosing hemorrhagic contusions such as those in the brain .
SE sequences, on the other hand- relatively immune from magnetic susceptibility artifacts, and also less sensitive in depicting hemorrhage and calcification.

GREFLAIR
Hemorrhage in right parietal lobe

Gradient EchoGradient Echo
Pros:fast technique
Cons: More sensitive to magnetic
susceptibility artifacts Clinical use:eg. Hemorrhage , calcification

DWI & ADCDWI & ADC

Diffusion-weighted MRIDiffusion-weighted MRI Diffusion-weighted MRI is a example of
endogenous contrast, using the motion of protons to produce signal changes
DWI images is obtained by applying pairs of opposing and balanced magnetic field gradients (but of differing durations and amplitudes) around a spin-echo refocusing pulse of a T2 weighted sequence.
Stationary water molecules are unaffected by the paired gradients, and thus retain their signal.
Non stationary water molecules acquire phase information from the first gradient, but are not re phased by the second gradient, leading to an overall loss of the MR signal

The normal motion of water molecules within living tissues is random (brownian motion).
In acute stroke, there is an alteration of homeostasis
Acute stroke causes excess intracellular water accumulation, or cytotoxic edema, with an overall decreased rate of water molecular diffusion within the affected tissue.
Reduction of extracellular space
Tissues with a higher rate of diffusion undergo a greater loss of signal in a given period of time than do tissues with a lower diffusion rate.
Therefore, areas of cytotoxic edema, in which the motion of water molecules is restricted, appear brighter on diffusion-weighted images because of lesser signal losses
Restriction of DWI is not specific for stroke

The primary application of DW MR imaging has been in brain imaging, mainly because of its exquisite sensitivity to early detection of ischemic stroke

The increased sensitivity of diffusion-weighted MRI in detecting acute ischemia is thought to be the result of the water shift intracellularly restricting motion of water protons (cytotoxic edema)
whereas the conventional T2 weighted images show signal alteration mostly as a result of vasogenic edema

Core of infarct = irreversible damage
Surrounding ischemic area may be salvaged
DWI: open a window of opportunity during which Tt is beneficial
Regions of high mobility “rapid diffusion” dark
Regions of low mobility “slow diffusion” bright



T2 shine throughT2 shine throughT2 shine-through refers to high
signal on DWI images that is not due to restricted diffusion,
high T2 signal which 'shines through' to the DWI image.
T2 shine through occurs because of long T2 decay time in some normal tissue.
This is most often seen with subacute infarctions due to vasogenic edema but can be seen in other pathologic abnormalities i.e epidermoid cyst.

Apparent Diffusion Apparent Diffusion CoefficientCoefficient It is a measure of diffusion Calculated by acquiring two or more
images with a different gradient duration and amplitude .
To differentiate T2 shine through effects or artifacts from real ischemic lesions.
The lower ADC measurements seen with early ischemia,
An ADC map shows parametric images containing the apparent diffusion coefficients of diffusion weighted images. Also called diffusion map

The ADC may be useful for estimating the lesion age and distinguishing acute from subacute DWI lesions.
Acute ischemic lesions can be divided into hyperacute lesions (low ADC and DWI-positive) and subacute lesions (normalized ADC).
Chronic lesions can be differentiated from acute lesions by normalization of ADC and DWI.
a tumour would exhibit more restricted apparent diffusion compared with a cyst because intact cellular membranes in a tumour would hinder the free movement of water molecules

Nonischemic causes for decreased Nonischemic causes for decreased ADCADC Abscess
Lymphoma and other tumors
Multiple sclerosis
Seizures
Metabolic (Canavans )

65 year male- Rt ACA Infarct

Evaluation of acute stroke on Evaluation of acute stroke on DWIDWIThe DWI and ADC maps show changes
in ischemic brain within minutes to few hours
The signal intensity of acute stroke on DW images increase during the first week after symptom onset and decrease thereafter, but signal remains hyper intense for a long period (up to 72 days in the study by Lausberg et al)
The ADC values decline rapidly after the onset of ischemia and subsequently increase from dark to bright 7-10 days later .

This property may be used to differentiate the lesion older than 10 days from more acute ones .
Chronic infarcts are characterized by elevated diffusion and appear hypo, iso or hyper intense on DW images and hyperintense on ADC maps


DW MR imaging characteristics of Various Disease Entities
MR Signal Intensity
Disease DW Image ADC Image ADC Cause
Acute Stroke High Low Restricted Cytotoxic edema
Chronic Strokes Variable High Elevated Gliosis
Hypertensive
encephalopathy
Variable High Elevated Vasogenic edema
Arachnoid cyst Low High Elevated Free water
Epidermoid mass High Low Restricted Cellular tumor
Herpes encephalitis High Low Restricted Cytotoxic edema
CJD High Low Restricted Cytotoxic edema
MS acute lesions Variable High Elevated Vasogenic edema
Chronic lesions Variable High Elevated Gliosis

References References Bradley’s text book of neurology-
6th editionRobert A Ziemarman’s
Neuroimaging clinical and physical principle.