
PPM in Myanmar - · PDF filePresentation overview •NTP Myanmar background •PPM...
34
9 th Meeting of the Subgroup on Public-Private Mix for TB Care and Control & Global Workshop on Engaging Large Hospitals 28-30 August 2013, Bangkok, Thailand PPM in Myanmar Dr Thin Thin Nwe, NTP
Transcript of PPM in Myanmar - · PDF filePresentation overview •NTP Myanmar background •PPM...

9th Meeting of the Subgroup on Public-Private Mix for TB Care and Control
&
Global Workshop on Engaging Large Hospitals
28-30 August 2013, Bangkok, Thailand
PPM in Myanmar Dr Thin Thin Nwe, NTP

Presentation overview
• NTP Myanmar background
• PPM Background
• Engagement of GPs (PSI and MMA)\
• Public-public mix (hospitals)
• Engagement of implementing partners
• PPM results
• Future plans

CHINA
LAOS
THAILAND
INDIA
BANGLA
DESH
KACHIN
SHAN
SAGAING
CHIN
RAKHINE
MANDALAY
MAGWE
BAGO
AYARWADDY
YANGON
KAYIN
KAYAH
MON
TANINTHARYI
Area (km2) - 676,578
Regions/States - 17
Districts - 69
Townships - 330
Sub Townships - 82
Wards - 3,040
Village tracts - 13,267
Villages - 67,285
Population - 59.78 m
Urban - 30%
Rural - 70%
Myanmar

Magnitude of TB in Myanmar • TB is a major public health problem
• Myanmar is one of the 22 HBCs 27 high MDR-TB countries 41 high TB/HIV countries
. Est. Annual Risk of TB Infection (ARTI)
1972 - 1.66%,
1994 - 1.5%
• 2011 disease burden (2012 Global TB Report): – Est. incidence (all forms): 381/100,000/year – Est. prevalence (all forms): 506/100,000 – Est. mortality: 48/100,000
• HIV prevalence in TB (2012 HIV sentinel survey): 9.7%

TB epidemiology, Myanmar (2011)
Mortality
Prevalence
Incidence

6 6
39 43 44
55
66
70 73
83
95
86
89 87 95
76 77
84 82
83 81 82 82 82 81 84
85
85
85 85 85
86 86
0
10
20
30
40
50
60
70
80
90
100
2000 2005 2010
%
Year
Trend in Case Detection Rate & Treatment Success Rate of the Myanmar NTP, 1997-2012
CDR New SS+
TSR
Target reset
Achievements in 2012: Total case notification: 148,149 (or 251/100,000) Smear-positive case notification: 42,910 (or 73/100,000)

PPM in Myanmar: background • Policy on PPM DOTS: 2003 • Operational guidelines for PPM DOTS: 2005 • Engagement of GPs through (2) NGOs [PSI and MMA]
and (3) schemes: – Scheme 1: health education and suspect referral – Scheme 2: health education, suspect referral, DOT – Scheme 3: referral, diagnosis, treatment, DOT
• Engagement of private laboratories: – 79 labs under EQA (plus 386 public labs)
• Engagement of public hospitals: – 4 in 2007 → 23 in 2013
• Other ministries: Labour, Home Affairs, Defence

Partners of NTP 1. Myanmar Women Affairs Federation (MWAF).
2. Myanmar Maternal & Child Welfare Association (MMCWA)
3. Myanmar Medical Association (MMA)
4. Myanmar Red Cross Society (MRCS)
5. Myanmar Health Assistant Association (MHAA)
International NGOs 1. Population Services International (PSI) 2. MSF - Holland 3. Malteser International 4. World Vision Myanmar 5. Japan Anti-TB Association (JATA) 6. International Organization of Migration (IOM) 7. Asia Harm Reduction Network (AHRN) 8. Merlin 9. Pact Myanmar 10. Union 11. Progeto 12. Cesvi 13. MSF – Switzerland 14. MDM 15. FHI 360
Local NGOs
UN Agencies
Bilateral Agencies
1. World Health Organization (WHO)
1. Japan International Cooperation Agency (JICA)

PPM by PSI • Population Services International or PSI is US-based
NGO
• Collaboration with NTP since 2004
• PSI organized GPs through “Sun Quality Clinic” as DOT unit
• Coverage: 189 townships in 13 states/regions
894 GPs in Scheme 3
• Achievements: contributed 16% of national case finding (2012) Treatment success rate 85%

PSI: service delivery for PPM DOTS 2004 2008
Scheme 3 Scheme 1 HE, DOT, contact tracing

PSI: Area coverage of PPM-DOTS (2012)
Channel Townships No. of
providers
SQHC 185 894
SPH 68 1627
TB REACH (IPC) 38 60
TB REACH (Pharmacy)
38 526
No. of private lab
No. of NTP lab
Total
53 152 205 SQH only
SUN (SQH/SPH)

0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
2004 2005 2006 2007 2008 2009 2010 2011 2012
PSI contribution on new smear (+) TB patients notified to NTP in project area (2004-2012)
PSI
NTP
8%
13%
15%
14% 14%
16%
19%

PPM by MMA • Myanmar Medical Association or MMA
started PPM activities in 2005 • MMA uses (3) Schemes:
– Scheme 1: health education, suspect referral – Scheme 2: health education, referral, DOT – Scheme 3: referral, diagnosis, treatment, DOT
• Coverage in 2012: – 116 townships in 11 states/regions – Scheme 1 by 1266 GPs – Scheme 2 by 2 GPs – Scheme 3 by 175 GPs

PPM coverage by MMA


0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
2009 2010 2011 2012
3015 3506
70068401
557651
797
864
MMA (Scheme III) contribution on new smear( +) TB patients notified to NTP in project area (2009-2012)
MMA S III
NTP+other unit
(16%) (16%)
(10%)
(11 %)
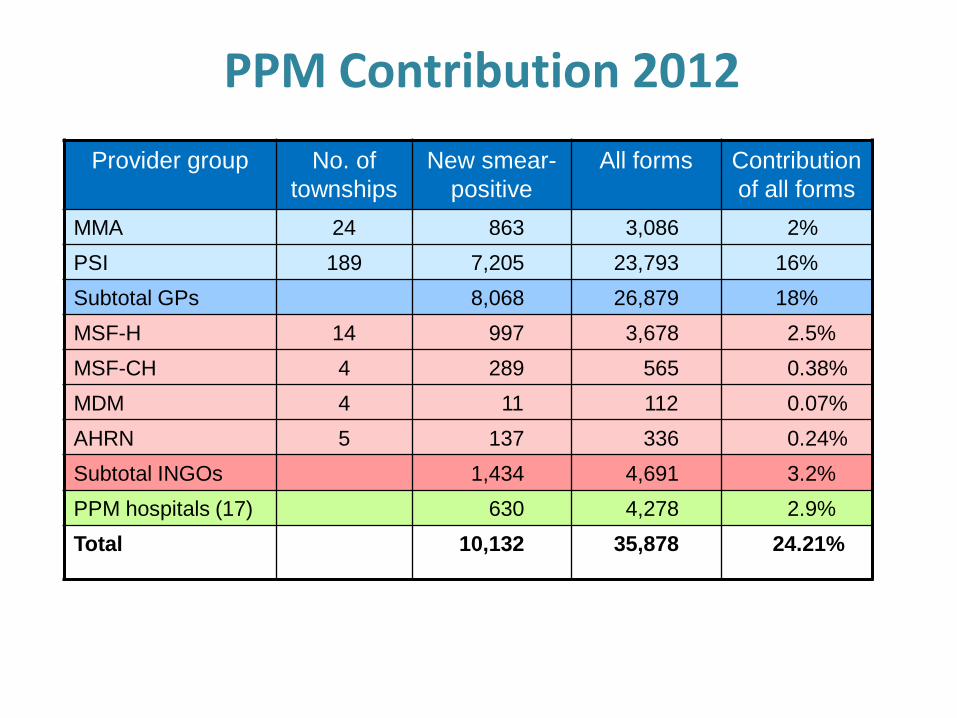
PPM Contribution 2012
Provider group No. of
townships
New smear-
positive
All forms Contribution
of all forms
MMA 24 863 3,086 2%
PSI 189 7,205 23,793 16%
Subtotal GPs 8,068 26,879 18%
MSF-H 14 997 3,678 2.5%
MSF-CH 4 289 565 0.38%
MDM 4 11 112 0.07%
AHRN 5 137 336 0.24%
Subtotal INGOs 1,434 4,691 3.2%
PPM hospitals (17) 630 4,278 2.9%
Total 10,132 35,878 24.21%
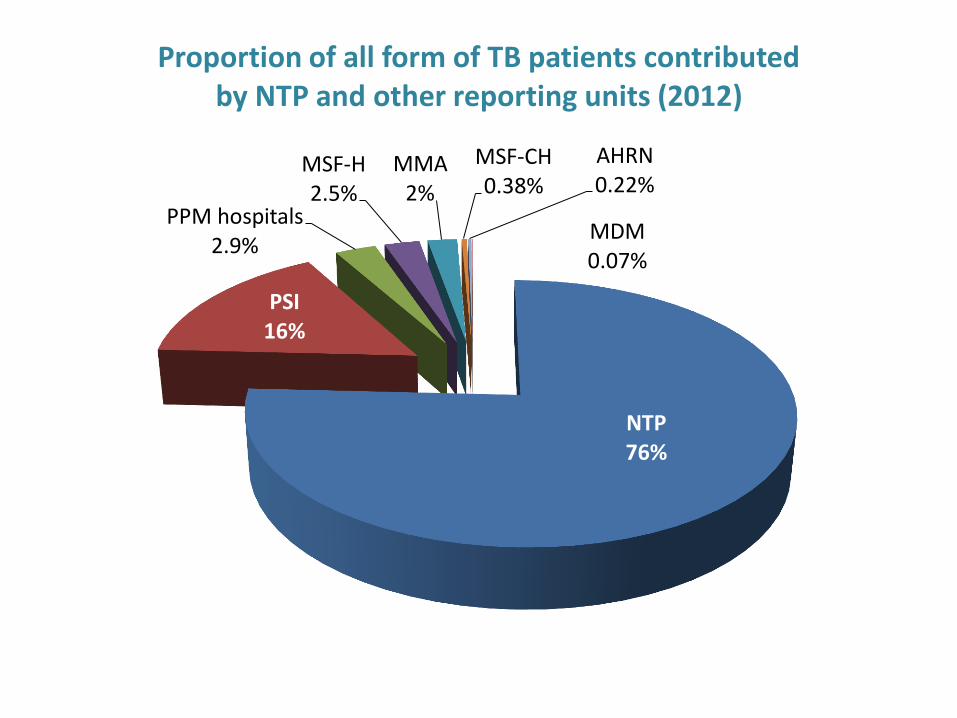
NTP 76%
PSI 16%
PPM hospitals 2.9%
MSF-H 2.5%
MMA 2%
MSF-CH 0.38%
AHRN 0.22%
MDM 0.07%
Proportion of all form of TB patients contributed by NTP and other reporting units (2012)

0%
20%
40%
60%
80%
100%
120%
Treatment outcomes of new smear positive TB patients, by PPM partner, 2011 cohort
Transfer
Defaulter
Failure
Died
Completed
Cured
Public-public mix DOTS

Hospital engagement
• Aim: – to strengthen link between public TB centres and public
hospitals within framework of DOTS strategy
• 4 hospitals in 2007 → 23 hospitals in 2013
– General hospitals: 12 – TB hospitals: 3 (including workers hospitals) – HIV hospitals: 2 – Military hospitals: 2 – Prison hospital: 1 (Mandalay) – Children hospitals: 3

Hospital engagement: process
• Advocacy meeting in each hospital
• Two-day training for relevant hospital staff
• Set-up of Hospital DOTS Committee
– Chair: Medical Superintendent
– Members: Heads of clinical departments
• Set-up of Hospital PPM DOTS Unit
– Coordinator: Assistant Medical Superintendent
– Roles identified of laboratory technician, nurses, pharmacist, social worker
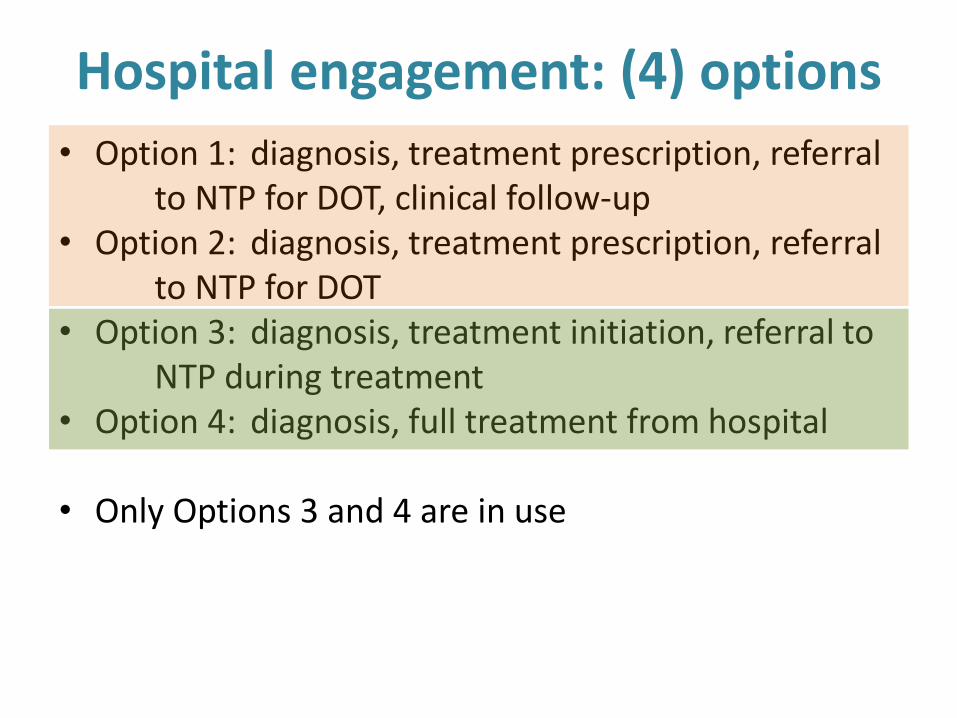
Hospital engagement: (4) options
• Option 1: diagnosis, treatment prescription, referral to NTP for DOT, clinical follow-up • Option 2: diagnosis, treatment prescription, referral to NTP for DOT • Option 3: diagnosis, treatment initiation, referral to NTP during treatment • Option 4: diagnosis, full treatment from hospital
• Only Options 3 and 4 are in use

Hospital engagement: functioning
• DOTS corner • Logistics management • Recording and reporting • Monitoring • Supervision • EQA for hospital laboratory
• → improved accessibility and reduced out-of pocket expenditures

0
5000
10000
15000
20000
25000
30000
35000
40000
45000
2004 2005 2006 2007 2008 2009 2010 2011 2012
30977 36212 39874 42120 40703 40742 41706 41762
42402
431
329 367 468 545
647 612 573
597
No
of
NS(
+) T
B c
ase
s
Years
Hospital Contribution in NTP of NS(+) TB cases (2004-2012)
Hospital total cases NTP total cases

0
20
40
60
80
100
2004 2005 2006 2007 2008 2009 2010 2011 2012
98.6 99.1 99.1 98.9 98.7 98.4 98.5 98.6 98.1
1.4 0.9 0.9 1.1 1.3 1.6 1.5 1.4 1.9
(%
)
Years
Hospital Contribution in NTP of NS(+) TB cases by Percentage (2004-2012 )
Hospital
NTP

0
20000
40000
60000
80000
100000
120000
140000
160000
2004 2005 2006 2007 2008 2009 2010 2011 2012
95977 106684 121878 131090 125157 130217 133316 139351
143999
1932
1307
1715
2457 3582 3806 4087
3813
4150
No
of
All
typ
e TB
cas
es
Years
Hospital Contribution in NTP of All type TB cases (2004-2012 )
Hospital total cases NTP total cases

0
20
40
60
80
100
2004 2005 2006 2007 2008 2009 2010 2011 2012
98 98.8 98.6 98.1 97.1 97.1 96.9 97 97
2 1.2 1.4 1.9 2.9 2.9 3.1 3 3
(%)
Years
Hospital Contribution in NTP of All type TB cases by percentage (2004-2012)
Hospital NTP

0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
2004 2005 2006 2007 2008 2009 2010 2011 2012
36615 41559 45614 48531 46508 46969 47866 48112 48789
746
579743
720795 908 917 900 870
No
of
All
S(+
) T
B c
ase
s
Years
Hospital Contribution in NTP of All S(+) TB cases (2004-2012)
Hospital total cases NTP total cases
0
20
40
60
80
100
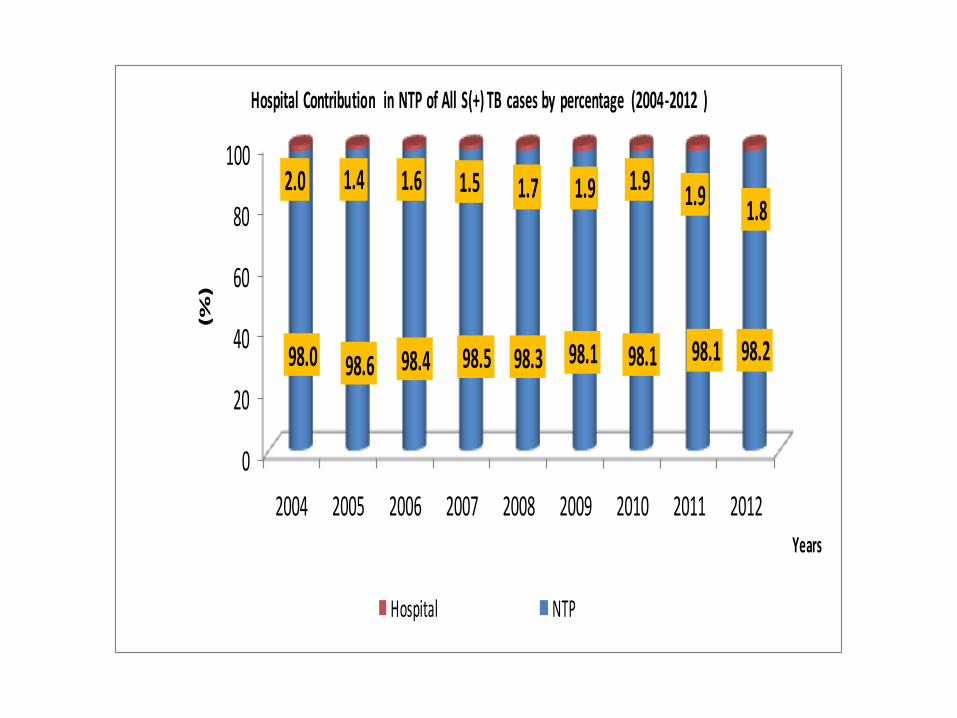
2004 2005 2006 2007 2008 2009 2010 2011 2012
98.0 98.6 98.4 98.5 98.3 98.1 98.1 98.1 98.2
2.0 1.4 1.6 1.5 1.7 1.9 1.9 1.9 1.8
(%
)
Years
Hospital Contribution in NTP of All S(+) TB cases by percentage (2004-2012 )
Hospital NTP

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
%Treatment outcome of new smear positive TB patients from PPM-DOTS
hospitals by percentage (2011 tri quarter cohort)
Transfer out
Defaulter
Failure
Died
completed
Cured
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
%Treatment outcome of new smear positive TB patients from PPM-DOTS
hospitals by percentage (2011 tri quarter cohort)
Transfer out
Defaulter
Failure
Died
completed
Cured
PPM: weaknesses • Human resources: shortage of staff (medical doctors,
laboratory technicians) in public hospitals
• Turnover of medical doctors and staff
• No regular refresher training
• Non adherence to treatment guidelines
• Weakness in coordination
• Weakness in supported supervision
• Problems with recording and reporting
• Fund flow

Future Plan
• Refresher training will be provided for expanded PPM hospitals
• Regular supervision for newly expanded townships
• Strengthen EQA system to ensure laboratory quality
• Strengthen referral system from GPs
• Start MDR-TB management through GPs

Thank you!


















