Ppi Original

of 16
Transcript of Ppi Original
-
8/8/2019 Ppi Original
1/16
Proton-Pump Inhibitors Are Associated With Increased CardiovascularRisk Independent of Clopidogrel UseA Nationwide Cohort Study
Mette Charlot, MD; Ole Ahlehoff, MD; Mette Lykke Norgaard, MD; Casper H. Jrgensen, MD; Rikke Srensen, MD;
Steen Z. Abildstrm, MD, PhD; Peter Riis Hansen, MD, PhD, DMSc; Jan Kyst Madsen, MD, DMSc; Lars Kber, MD, DMSc;
Christian Torp-Pedersen, MD, DMSc; and Gunnar Gislason, MD, PhD
Background: Controversy remains on whether the dual use ofclopidogrel and proton-pump inhibitors (PPIs) affects clinical effi-cacy of clopidogrel.
Objective: To examine the risk for adverse cardiovascular out-comes related to concomitant use of PPIs and clopidogrel com-pared with that of PPIs alone in adults hospitalized for myo-cardial infarction.
Design: A nationwide cohort study based on linked administrativeregistry data.
Setting: All hospitals in Denmark.
Patients: All patients discharged after first-time myocardial infarc-tion from 2000 to 2006.
Measurements: The primary outcome was a composite of rehos-pitalization for myocardial infarction or stroke or cardiovasculardeath. Patients were examined at several assembly time points,including 7, 14, 21, and 30 days after myocardial infarction.Follow-up was 1 year.
Results: Of 56 406 included patients, 9137 (16.2%) were re-hospitalized for myocardial infarction or stroke or experienced car-diovascular death. Of the 24 702 patients (43.8%) who received
clopidogrel, 6753 (27.3%) received concomitant PPIs. The hazardratio for cardiovascular death or rehospitalization for myocardialinfarction or stroke for concomitant use of a PPI and clopidogrelamong the cohort assembled at day 30 after discharge was 1.29(95% CI, 1.17 to 1.42). The corresponding ratio for use of a PPI inpatients who did not receive clopidogrel was 1.29 (CI, 1.21 to1.37). No statistically significant interaction occurred between a PPIand clopidogrel (P 0.72).
Limitations: Unmeasured and residual confounding, time-varyingmeasurement errors of exposure, and biases from survival effectswere possible.
Conclusion: Proton-pump inhibitors seem to be associated withincreased risk for adverse cardiovascular outcomes after discharge,regardless of clopidogrel use for myocardial infarction. Dual PPI andclopidogrel use was not associated with any additional risk foradverse cardiovascular events over that observed for patients pre-scribed a PPI alone.
Primary Funding Source: The Danish Medical Research Counciland the Danish Heart Foundation.
Ann Intern Med. 2010;153:378-386. www.annals.org
For author affiliations, see end of text.
Clopidogrel is a platelet inhibitor that reduces the riskfor new ischemic cardiovascular events, in combina-tion with aspirin, in patients treated either medically or
with percutaneous coronary intervention (PCI) after myo-cardial infarction (13). Proton-pump inhibitors (PPIs) areoften given in combination with clopidogrel and aspirin toreduce the risk for upper gastrointestinal bleeding. Clopi-dogrel is a prodrug that is metabolized to an active metab-olite primarily by the hepatic P-450 enzyme 2C19 (4).Because PPIs are metabolized by the same hepatic isoen-zyme (5), concern has been raised that PPIs might inhibit
the conversion of clopidogrel to its active metabolite andthereby diminish its clinical benefit.
Recent studies show that PPIs reduce the ex vivo in-hibition of platelet aggregation achieved during treatment
with clopidogrel (6 8). Clinical studies involving selectedpopulations (913) show conflicting results regarding riskfor adverse cardiovascular events associated with the dualuse of clopidogrel and PPIs. The U.S. Food and Drug
Administration (14, 15) and the European MedicinesAgency (16) have recently discouraged the combined use ofthese agents unless strongly indicated, while emphasizingthe need for further studies. We sought to examine the riskfor adverse cardiovascular outcomes related to concomitantuse of PPIs and clopidogrel compared with that of PPIsalone in a large, unselected cohort of patients hospitalized
with first-time myocardial infarction.
METHODSDesign Overview
In Denmark, every resident is provided with a perma-nent and unique civil registration number that enablesindividual-level linkage between different registries. Our
See also:
Print
Editors Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 379
Editorial comment. . . . . . . . . . . . . . . . . . . . . . . . . . 413
Web-Only
Appendix Tables
Appendix Figures
Conversion of graphics into slides
Annals of Internal MedicineArticle
378 2010 American College of Physicians
Original version, published 21 September 2010.
-
8/8/2019 Ppi Original
2/16
nationwide cohort study linked Danish national registrydata relevant to hospitalizations, pharmacy prescriptionclaims, and deaths for 4.65 million people.
For all hospital admissions in Denmark, the DanishNational Patient Registry registers a primary diagnosis and,if appropriate, 1 or more secondary diagnoses, as defined
by the International Classification of Diseases. The DanishRegistry of Medicinal Product Statistics (a national pre-scription registry) records every prescription dispensedfrom pharmacies in Denmark, and each drug is classifiedaccording to the International Anatomical TherapeuticalChemical system. Information on vital status and causes ofdeath were obtained, respectively, from the Danish CivilRegistry and the National Causes of Death Registry.
The Danish Data Protection Agency approved thestudy, and the data made available to us were such thatindividuals could not be identified. Retrospective registrystudies do not require ethical approval in Denmark. The
authors had full access to the data and take full responsi-bility for its integrity.
Patient Population
From the National Patient Registry, we identified allconsecutive patients older than 30 years who were hospi-talized with acute myocardial infarction between 2000 and2006 in Denmark. To ensure the homogeneity of our pop-ulation, patients with previous myocardial infarction andpatients with partially missing data were excluded. We de-pended on patients filling prescriptions to identify users.Our primary analysis included patients who survived atleast 30 days because we reasoned that a 30-day period
would facilitate correct classification of drug use; most pa-tients who filled their prescriptions did so within 30 days(Appendix Figure 1, available at www.annals.org). We alsoexamined the sensitivity of the results to the 30-day cutoffby examining alternative cohorts that included patients
who survived 7, 14, and 21 days after myocardial infarc-tion. Patients who emigrated were censored at the time ofemigration.
Drug Use
Using the national prescription registry, we identifiedall prescriptions of drugs claimed up to 90 days after dis-
charge (Table 1), as well as all prescriptions for PPIs andH
2-antagonists claimed within 1 year after discharge. In-
formation on medication exposure for each day offollow-up was also obtained, including dispensing date,type, quantity, dose of drug, and days of drug supply. Nodata on patient-reported adherence were available. We de-fined current use as the period from the prescription fillingdate to the calculated end of the period drug supply. Ofnote, the national prescription registry has demonstratedaccuracy (17), and the use of clopidogrel is reasonably sta-ble over time in this cohort, with a 1-year persistency of89% after 2004 (18).
Outcomes
The primary outcome was a composite of rehospital-ization for myocardial infarction or stroke or cardiovasculardeath. Secondary outcomes included all-cause death, car-diovascular death, and rehospitalization for myocardial in-farction, stroke, or gastrointestinal bleeding. Follow-up wasup to 1 year after discharge. The diagnoses of acute myo-
cardial infarction and stroke have been validated in theDanish National Patient Registry (19, 20).
Comorbidity
Comorbid conditions were established on the basis ofdiagnoses noted at the time of discharge from the indexmyocardial infarction, as specified in the Ontario acutemyocardial infarction mortality prediction rule (21). Thecomorbidity index was further enhanced by adding diag-noses from the year before the event, as was done by Ras-mussen and colleagues (22).
Concomitant use of loop diuretics or diabetes medica-tion was a proxy for heart failure or diabetes, respectively,
to define high-risk subgroups of patients, as was done byGislason and colleagues (23).
Statistical Analysis
We used 2 statistical methods to estimate the risk as-sociated with PPI treatment with or without concomitanttreatment with clopidogrel.
First, we used Cox proportional hazards models toderive hazard ratios (HRs) and 95% CIs. These models
were adjusted for the variables shown in Table 1, includingage, sex, PCI, income, concomitant medical treatment, andcomorbid conditions. Exposure to PPIs was included as atime-dependent covariate.
Context
Observational studies show mixed signals about risk forcardiovascular events with the dual use of proton-pumpinhibitors (PPIs) and clopidogrel compared with clopidogrel
alone.
Contribution
This observational study, based on administrative data
from all hospitals in Denmark, found that patients whoreceived clopidogrel and PPIs at discharge after a first-timemyocardial infarction had similar risks for cardiovascular
death, myocardial infarction, or stroke as did those ofpatients who received PPIs alone.
Caution
Possible confounding and no information on adherence orover-the-counter drug use limit interpretation.
Implication
Concurrent PPI and clopidogrel use after myocardialinfarction may not be associated with additional risk overthat observed with PPIs alone.
The Editors
ArticleIncreased Cardiovascular Risk With Proton-Pump Inhibitors
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 379
-
8/8/2019 Ppi Original
3/16
Second, we performed a propensity scorematchedanalysis, in which we quantified a propensity score for thelikelihood of receiving a PPI in the first year after dischargeby using multivariate logistic regression analysis, conditionalon the baseline covariates specified in Table 1. Using theGreedy matching macro (http://mayoresearch.mayo.edu/mayo/research/biostat/upload/gmatch.sas; accessed on 27
July 2010), we matched each case patient to a control partic-ipant on the basis of propensity score. Use of PPIs was in-cluded as a time-dependent covariate, and propensity scorematched KaplanMeier estimates were generated to showevent rates and time-to-event curves.
To assess the robustness of our results, we performed a
series of additional analyses, including an analysis that eval-uated how large the effect of an unmeasured confounder
would need to be to explain the results, subgroup analysesof different types of PPIs, and a dose-dependent analysis(24). We also assessed the variation of both PPI use andoutcome between hospitals and performed a stratified anal-ysis according to PCI and aspirin use. All statistical calcu-lations were performed with SAS, version 9.2 (SAS Insti-tute, Cary, North Carolina).
Role of the Funding Source
Our study was funded by the Danish Medical Re-search Council and the Danish Heart Foundation. The
study sponsors had no influence on the study design, datacollection, analysis, data interpretation, or decision to sub-mit the manuscript for publication.
RESULTSPatients
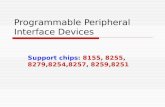
A total of 71 987 patients were admitted with myo-cardial infarction from 2000 to 2006 (Figure 1). Ofthese, we excluded 1889 patients with previous myocar-dial infarction, 13 324 patients who died during hospi-talization or within 30 days of discharge, and 368 pa-tients with partially missing data. Of the 56 406patients included in the study, 24 704 (43.8%) claimeda prescription for clopidogrel within 30 days of dis-charge ( Appendix Figure 1). Of these, 6753 patients(27.3%) claimed at least 1 prescription for PPIs within1 year of discharge. The use of PPIs was equal in the 2cohorts and independent of clopidogrel use (AppendixTable 1, available at www.annals.org).
Table 1 shows baseline characteristics of the studysample at the time of inclusion. Patients who received clo-pidogrel were younger, were more often male, received lessconcomitant medical treatment, had fewer comorbid con-ditions, and more often had PCI than patients who did not
Table 1. Baseline and Propensity ScoreMatched Baseline Characteristics at Inclusion*
Characteristic Patients Not Receiving Clopidogrel Propensity ScoreMatched PatientsNot Receiving Clopidogrel
Patients Receiving Clopidogrel
Patients NotReceiving a PPI
(n
22 815)
PatientsReceiving a PPI
(n
8889)
PValue Patients NotReceiving a PPI
(n
8437)
PatientsReceiving a PPI
(n
8437)
PValue Patients NotReceiving a PPI
(n
17 949)
PatientsReceiving a PPI
(n
6753)
PValue
Mean age (SD), y 70.3 (13.4) 73.3 (12.4) 0.001 73.2 (12.8) 73.1 (12.5) 0.72 64.1 (12.5) 67.5 (12.5) 0.001
Men 13 811 (60.5) 4739 (53.3) 0.001 4535 (53.7) 4516 (53.5) 0.77 12 801 (71.3) 1775 (61.8) 0.001
Income group 0.001 0.25 0.001
0 3630 (15.9) 1482 (16.7) 1527 (18.1) 1405 (16.7) 1456 (8.1) 789 (11.7)
1 4914 (21.5) 2316 (26.1) 2145 (25.4) 2178 (25.8) 2123 (11.8) 1147 (17.0)
2 4717 (20.7) 2108 (23.7) 1966 (23.2) 1986 (23.5) 3421 (19.1) 1649 (24.4)
3 4741 (20.8) 1725 (19.4) 1569 (18.6) 1650 (19.6) 4241 (23.6) 1501 (22.2)
4 4813 (21.1) 1258 (14.2) 1230 (14.6) 1218 (14.4) 6708 (37.4) 1667 (24.7)
Shock 251 (1.1) 196 (2.2) 0.001 146 (1.7) 163 (1.9) 0.33 88 (0.5) 69 (1.0) 0.001
Diabetes with complications 1226 (5.4) 606 (6.8) 0.001 527 (6.3) 565 (6.7) 0.23 663 (3.7) 394 (5.8) 0.001
Peptic ulcer 160 (0.7) 546 (6.1) 0.001 160 (1.9) 172 (2.0) 0.52 40 (0.2) 195 (2.9) 0.001
PCI 2169 (9.5) 727 (8.2) 0.001 665 (7.9) 713 (8.5) 0.177 12 467 (69.5) 4065 (60.2) 0.001
Pulmonary edema 303 (1.3) 145 (1.6) 0.04 114 (1.4) 134 (1.6) 0.20 96 (0.5) 65 (1.0) 0.001
Cerebral vascular disease 1309 (5.7) 709 (8.0) 0.001 583 (6.9) 646 (7.7) 0.062 499 (2.8) 308 (4.6) 0.001
Cancer 69 (0.3) 57 (0.6) 0.001 49 (0.6) 50 (0.6) 0.92 40 (0.2) 36 (0.2) 0.001
Cardiac dysrhythmias 3094 (13.6) 1295 (14.6) 0.092 1160 (13.8) 1212 (14.4) 0.29 1203 (6.7) 616 (9.1)
0.001Acute renal failure 200 (0.9) 209 (2.4) 0.001 147 (1.7) 171 (2.0) 0.174 43 (0.2) 73 (1.1) 0.001
Chronic renal failure 269 (1.2) 314 (3.5) 0.001 240 (2.8) 249 (3.0) 0.68 102 (0.6) 119 (1.8) 0.001
Loop diuretic 10 135 (44.4) 5143 (57.8) 0.001 4838 (57.3) 4804 (56.9) 0.60 4300 (24.0) 2677 (39.6) 0.001
Spironolactone 2665 (11.7) 1324 (14.9) 0.001 1214 (14.4) 1255 (14.9) 0.37 1196 (6.7) 750 (11.1) 0.001
Aspirin 11 218 (49.2) 3953 (44.5) 0.001 3704 (43.9) 3826 (45.4) 0.058 13 079 (72.9) 4402 (65.2) 0.001
Statin 11 492 (50.4) 3970 (44.6) 0.001 3754 (44.4) 3841 (45.4) 0.178 16 002 (89.2) 5684 (84.2) 0.001
-Blocker 16 056 (70.4) 5915 (66.5) 0.001 5645 (66.9) 5655 (67.0) 0.29 15 772 (87.9) 5624 (83.3) 0.001
ACE inhibitor 9761 (42.8) 3754 (42.2) 0.79 3535 (41.9) 3597 (42.6) 0.33 9129 (50.9) 3708 (54.9) 0.001
Diabetes medication 2868 (12.6) 1301 (14.6) 0.001 1152 (13.7) 1235 (14.6) 0.067 1919 (10.7) 928 (13.7) 0.001
ACE angiotensin-converting enzyme; PCI percutaneous coronary intervention; PPI proton-pump inhibitor.* All values are numbers (percentages) unless otherwise indicated.
Article Increased Cardiovascular Risk With Proton-Pump Inhibitors
380 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
4/16
receive clopidogrel. Patients who received PPIs were older,were more often female, received more concomitant med-
ical treatment, and had more comorbid conditions thanthose who did not receive PPIs.
Outcome
In the first year after inclusion, 9137 (16.2%) cardio-vascular deaths and rehospitalizations for myocardial in-farction or strokes were registered ( Appendix Table 2,available at www.annals.org). Clopidogrel was associated
with lower event rates, and PPIs were associated withhigher event rates. The event rates were highest amongpatients who received a PPI but not clopidogrel (26.3%).
Cox Proportional Hazards Regression Analysis
The time-dependent Cox proportional hazards regres-sion analysis (Table 2), based on patients who filled pre-scriptions for clopidogrel within 30 days of discharge,demonstrated an increased risk for the primary end point(cardiovascular death or rehospitalization for myocardialinfarction or stroke) among patients who received bothclopidogrel and a PPI (HR, 1.29 [95% CI, 1.17 to 1.42];P 0.001) compared with those who did not receive aPPI. Among patients who did not receive clopidogrel, PPItherapy was associated with a similar increase in risk (HR,1.29 [CI, 1.21 to 1.37]; P 0.001). Results were consis-tent for the risk for all secondary outcomes (Table 2). Thehazard rate ratio of the effect of the interaction between
PPI and clopidogrel for the primary outcome analysis was0.98 (CI, 0.88 to 1.10; P 0.72).
Time-Dependent, Propensity ScoreMatched CoxProportional Hazards Regression Analysis
Using the propensity score generated from logistic re-gression models conditional on baseline covariates, we
matched 6556 patients who received both clopidogrel anda PPI with the same number of patients who received clo-pidogrel but not a PPI. We also matched 8437 patients
who did not receive clopidogrel but did receive a PPI withthe same number of patients who received neither clopi-dogrel nor a PPI. Use of PPIs was included as a time-dependent covariate. The c-statistics were 0.65 and 0.65for the clopidogrel and nonclopidogrel groups, respec-tively, which indicates an acceptable discriminative powerfor the models. Table 1 shows the baseline characteristicsof the propensity scorematched populations and P valuesfor the between-group differences (Appendix Tables 3 and4 and Appendix Figure 2, available at www.annals.org,provide further details). For use of a PPI in combination
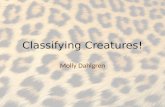
with clopidogrel, with no PPI therapy as the reference, theHR for cardiovascular death or rehospitalization for myo-cardial infarction or stroke was 1.35 (CI, 1.22 to 1.50; P0.001), whereas the HR for use of a PPI without clopi-dogrel was 1.43 (CI, 1.34 to 1.53; P 0.001). Analysis ofthe risk for the secondary outcomes generated similar re-sults (Table 2). The propensity scorematched KaplanMeier analysis (Figure 2) depicts the elevated risk for car-diovascular death or rehospitalization for myocardialinfarction or stroke for patients who received PPIs with or
without clopidogrel.
Subgroup Analyses of Different Types of PPIs
Of the 15 642 patients who claimed at least 1 pre-scription for PPIs, 4698 (30.0%) claimed prescriptionsfor pantoprazole, 2798 (17.9%) for lansoprazole, 2717(17.4%) for omeprazole, 5316 (34.0%) for esomeprazole,and 113 (0.01%) for rabeprazole. Results from the time-dependent, Cox proportional hazards regression analysisand the KaplanMeier cumulative hazard estimates dem-onstrated no difference in risk associated with the type ofPPI independent of clopidogrel treatment ( Appendix Fig-ures 3 and 4, available at www.annals.org). We did notinclude rabeprazole data in this analysis because the cohort
was too small to generate reliable results.Additional Analyses
In the propensity score matching based on baselinecovariates that predicted treatment with a PPI, the riskreduction for gastrointestinal bleeding in patients who re-ceived clopidogrel and a PPI was 0.82 (CI, 0.63 to 1.07;P 0.140) compared with patients who did not receive aPPI. Therapy with a PPI had no effect in the group thatdid not receive clopidogrel (risk reduction, 0.99 [CI, 0.80to 1.22]; P 0.89).
We estimated that an unmeasured confounder wouldhave to elevate risk by 2.5 to 3 to fully explain the in-
Table 1Continued
Propensity ScoreMatched PatientsReceiving Clopidogrel
Patients NotReceiving a PPI
(n
6556)
PatientsReceiving a PPI
(n
6556)
PValue
67.3 (12.6) 67.4 (12.5) 0.66
4028 (61.4) 4066 (62.0) 0.50
0.21
807 (12.3) 746 (11.4)
1133 (17.3) 1102 (16.8)
1562 (23.8) 1598 (24.4)
1410 (21.5) 1470 (22.4)
1644 (25.1) 1640 (25.0)
58 (0.9) 60 (0.9) 0.85
345 (5.3) 364 (5.6) 0.46
40 (0.6) 41 (0.6) 0.91
4024 (60.4) 3984 (60.8) 0.47
55 (0.8) 61 (0.9) 0.58
253 (3.9) 288 (4.4) 0.12
30 (0.5) 33 (0.5) 0.90
578 (8.8) 585 (8.9) 0.8342 (0.6) 49 (0.8) 0.46
85 (1.3) 93 (1.4) 0.55
2545 (38.8) 2546 (38.8) 0.99
713 (10.9) 725 (11.1) 0.74
4341 (66.2) 4334 (66.1) 0.80
5585 (85.2) 5554 (84.7) 0.45
5505 (84.0) 5486 (83.7) 0.193
3682 (56.2) 3604 (55.0) 0.65
855 (13.0) 886 (13.5) 0.43
ArticleIncreased Cardiovascular Risk With Proton-Pump Inhibitors
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 381
-
8/8/2019 Ppi Original
5/16
Figure 1. Study flow diagram.
Included (n = 60 393)
Excluded (n = 11 594)
Previous MI: 1889
Missing data: 368
Died before discharge: 9337
All patients hospitalized with acute MI from 20002006 (n = 71 987)
>7-d cohort (n = 58 582)
No clopidogrel (n = 36 955)
No PPI (n = 27 031) PPI (n = 9924)
Died within 7 d of discharge (n = 1811)
>14-d cohort (n = 57 683)
Died within 714 d of discharge (n = 899)
Clopidogrel (n = 21 627)
No PPI (n = 15 655) PPI (n = 5972)
No clopidogrel (n = 35 130)
No PPI (n = 25 526) PPI (n = 9406)
>21-d cohort (n = 57 044)
Died within 1421 d of discharge (n = 639)
Clopidogrel (n = 22 553)
No PPI (n = 16 327) PPI (n = 6226)
No clopidogrel (n = 33 380)
No PPI (n = 24 135) PPI (n = 9245)
>30-d cohort (n = 56 406)
Died within 2130 d of discharge (n = 638)
Clopidogrel (n = 23 664)
No PPI (n = 17 169) PPI (n = 6495)
No clopidogrel (n = 31 704)
No PPI (n = 22 815) PPI (n = 8889)
Clopidogrel (n = 24 702)
No PPI (n = 17 949) PPI (n = 6753)
MI myocardial infarction; PPI proton-pump inhibitor.
Article Increased Cardiovascular Risk With Proton-Pump Inhibitors
382 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
6/16
creased risk for cardiovascular events observed with eitherPPI or clopidogrel and PPI (Appendix Figure 5, availableat www.annals.org). To ensure the validity of using day 30after discharge as the inclusion day, we examined differ-ences in baseline characteristics at discharge and at day 30.
We found that most patients (83.5%) who died in the first30 days were from the cohort that had not filled prescrip-tions for clopidogrel or a PPI (Appendix Table 5, availableat www.annals.org). Examinations of the study cohort atvarious assembly time points, including 7 and 21 days aftermyocardial infarction, revealed no differences in the hazardrate ratios of the effect of the interaction between PPIs andclopidogrel (Table 3).
An analysis subdivided by patients seen before andafter 2004 provided no evidence of any differences in theeffect of PPIs on outcome (P 0.14). Interaction analysesbetween relevant subgroups of patients, PPI therapy, andoutcome showed interactions (P 0.035) for concomitanttreatment with a PPI and clopidogrel and PCI, with astatistically significant higher risk for cardiovascular deathor rehospitalization for myocardial infarction or stroke in astratified analysis (HR, 1.40 [CI, 1.19 to 1.64]) than in thepatient groups who did not have PCI (HR, 1.21 [CI, 1.07to 1.38]) ( Appendix Figure 6, available at www.annals.org). Stratifying patients by concomitant aspirin treatment
showed no effect. Additional sensitivity analyses demon-strated no evidence of any clustering between hospitals andno evidence of any difference between high and low PPIdoses (Appendix Figure 7 and Appendix Table 6, availableat www.annals.org)
DISCUSSIONWe found no evidence that concomitant PPI therapy
increases risk for adverse cardiovascular events in patientswho receive clopidogrel.
We conducted a MEDLINE search to find majorstudies between 2003 and 2010 that investigated possible
interactions between clopidogrel and PPIs. Gilard and col-leagues (6, 7) first drew attention to a possible interactionin a double-blind study that showed a reduced ex vivoantiplatelet effect of clopidogrel when combined with aPPI. Other studies (8, 14, 20, 21) have confirmed thisfinding.
An intense debate is now occurring about whether thediminished ex vivo antiplatelet effect is of clinically signif-icant importance. Several large observational studies (911, 25) found concomitant use of clopidogrel and a PPI tobe associated with increased risk for death or rehospitaliza-tion for myocardial infarction. However, these studies were
Figure 2. Propensity scorematched KaplanMeier analysis
of risk for cardiovascular death, myocardial infarction, or
stroke.
Risk,%
Time, d
Clopidogrel only
Clopidogrel + PPI
PPI only
No clopidogrel or PPI
30 60 90 120 150 180 210 240 270 300 330 3 60
60
70
80
90
100
PPI proton-pump inhibitor.
Table 2. Association Between PPI Therapy and Risk for Adverse Cardiovascular Outcomes During 1-Year Follow-up*
Outcome Time-Dependent Cox Proportional Hazards Model Time-Dependent, Propensity ScoreMatched CoxProportional Hazards Model
Patients Receiving a PPIbut Not Clopidogrel
Patients Receiving a PPIand Clopidogrel
Interaction Between PPIand Clopidogrel
Patients Receiving a PPIbut Not Clopidogrel
Patients Receiving a PPIand Clopidogrel
Hazard Ratio(95% CI)
PValue Hazard Ratio(95% CI)
PValue Hazard RateRatio (95% CI)
PValue Hazard Ratio(95% CI)
PValue Hazard Ratio(95% CI)
PValue
Cardiovasculardeath, MI, orstroke
1.29 (1.211.37) 0.001 1.29 (1.171.42) 0.001 0.98 (0.881.10) 0.72 1.43 (1.341.53) 0.001 1.35 (1.221.50) 0.001
All-cause death 1.58 (1.481.68) 0.001 1.75 (1.531.99) 0.001 1.19 (1.031.37) 0.017 1.95 (1.822.09) 0.001 2.09 (1.822.41) 0.001
Cardiovasculardeath
1.49 (1.381.60) 0.001 1.57 (1.361.82) 0.001 1.14 (0.981.35) 0.092 1.83 (1.691.98) 0.001 1.91 (1.632.24) 0.28
MI 1.13 (1.021.26) 0.020 1.19 (1.051.35) 0.007 1.06 (0.901.24) 0.50 1.13 (1.011.25) 0.033 1.18 (1.041.35) 0.013
Stroke 1.32 (1.171.49) 0.001 1.43 (1.191.71) 0.001 1.14 (0.921.41) 0.23 1.36 (1.191.55) 0.001 1.78 (1.472.16) 0.001
MI myocardial infarction; PPI proton-pump inhibitor.* Reference was no PPI therapy. Exposure to PPIs was included as a time-dependent covariate.
ArticleIncreased Cardiovascular Risk With Proton-Pump Inhibitors
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 383
-
8/8/2019 Ppi Original
7/16
not based on populations that represent the average patient who has had a myocardial infarction. For example, thestudies from Juurlink and colleagues (9) and Rassen andassociates (25) were based on retired patients older than65 years, and Ho and colleagues (10) presented data from
U.S. veterans (98% of whom were men). In contrast, apost hoc analysis of the randomized TRITON-TIMI 38(Trial to assess Improvement in Therapeutic Outcomes byoptimizing platelet Inhibition with prasugrel ThrombolysisIn Myocardial Infarction 38) (12) found no increased riskfor cardiovascular events with the combined use of PPIsand clopidogrel and no difference in risk between the var-ious types of PPIs. A post hoc analysis of the randomizedCREDO (Clopidogrel for the Reduction of Events DuringObservation) trial (11) also found baseline PPI use to beassociated with increased cardiovascular events, regardlessof whether clopidogrel was used. These studies were based
on selected patients eligible for randomized trials, who were usually younger and less likely to have significantcomorbid conditions than many patients who are pre-scribed both clopidogrel and a PPI. The prospective, ran-domized COGENT (Clopidogrel and the Optimization ofGastrointestinal Events) study (26), which was stopped be-fore inclusion of patients was complete, evaluated the car-diovascular safety of concomitant treatment with omepra-zole and clopidogrel and found no evidence of increasedcardiovascular risk. Similar results were recently reportedby Ray and colleagues (13). Of note, preliminary resultsfrom the COGENT study demonstrated an increased riskfor gastrointestinal bleeding in patients who received dualantiplatelet treatment without PPI therapy. This increasedbleeding risk was confirmed by Yasuda and colleagues (27),
which emphasizes the importance of establishing the car-diovascular safety of concomitant PPI treatment. Ray andcolleagues study (13) also illustrated the efficacy of PPItherapy in combination with dual antiplatelet treatment byshowing a remarkable reduction in risk for gastrointestinalbleeding in patients who received combination therapy.
Our study furthers the research in this area by inves-tigating the risk for cardiovascular events in a nationwide,unselected population that represents the average patient
who has had a myocardial infarction. We demonstrated
that PPI therapy did not modify the effect of clopidogrelon cardiovascular outcomes and that PPI use was associ-ated with increased cardiovascular risk independent of con-comitant use of clopidogrel.
We suspect that the increased cardiovascular risk in all
patients who received a PPI can be explained by differencesin baseline comorbid conditions that were unmeasured ormeasured imperfectly. Such unmeasured confounders
would have to elevate the risk 2.5- to 3-fold to explain theobserved increased risk for cardiovascular events. This is alarge but potentially plausible amount of risk elevation fora confounder or a mix of confounders, particularly becausethese registry data lacked detailed information on risk fac-tors, such as smoking, lipid levels, body mass index, andleft ventricle ejection fraction.
We also demonstrated a reduction in risk for gastroin-testinal bleeding related to PPI therapy for patients who
received clopidogrel, although it did not reach statisticalsignificance. In Denmark, PPIs are prescribed mainly forpatients with a clear indication, such as peptic ulcer. Thus,
we expected the cohort of patients treated with PPIs to beheavily confounded by the indication for PPIs and to havea higher bleeding risk than patients in countries whereguidelines recommend routine use of PPIs in combination
with dual antiplatelet therapy. This may explain why ourstudy did not find a statistically significant protective effectof PPIs on risk for gastrointestinal bleeding.
Previous studies (9, 10) have reported that the risk foradverse cardiovascular outcomes was particularly increasedby concomitant treatment with omeprazole and clopi-dogrel, on the basis of proposed differences in drug-specificmetabolism and diminished antiplatelet effects ex vivo (6,7, 23). Our data set provided no evidence of differences inrisk between the subtypes of PPIs, with or without clopi-dogrel. Sensitivity analyses also provided no evidence ofdifferences in risk related to heart failure, diabetes, age,hospitals, or PPI dosages. However, we did find a statisti-cally significant interaction between PCI and PPIs in thegroup that received clopidogrel.
Several considerations and limitations may affect theinterpretation of our results. We had no self-reported pa-tient data regarding adherence. We were also dependent on
Table 3. Association Between PPI Therapy and Risk for Adverse Cardiovascular Outcomes During 1-Year Follow-up*
TimePoint
Patients Receiving a PPI butNot Clopidogrel
Patients Receiving a PPIand Clopidogrel
Hazard RateRatio (95% CI)
PValue
Hazard Ratio (95% CI) PValue Hazard Ratio (95% CI) PValue
7 d 1.18 (1.101.24) 0.001 1.21 (1.091.34) 0.001 1.01 (0.901.14) 0.84
14 d 1.23 (1.161.30) 0.001 1.22 (1.101.36) 0.001 0.96 (0.861.08) 0.5421 d 1.26 (1.191.34) 0.001 1.24 (1.121.37) 0.001 0.96 (0.851.07) 0.44
30 d 1.29 (1.211.37) 0.001 1.29 (1.171.42) 0.001 0.98 (0.881.10) 0.72
PPI proton-pump inhibitor.* Time-dependent Cox proportional hazards model. Reference was no PPI therapy. Times are in relation to inclusion day after discharge. Assessed outcomes werecardiovascular death, myocardial infarction, or stroke. Patients who filled or did not fill a prescription for clopidogrel.
Article Increased Cardiovascular Risk With Proton-Pump Inhibitors
384 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
8/16
patients filling prescriptions after discharge, and we choseday 30 as the inclusion day for primary analyses to avoid apotential immortal time bias. The comparison of baselinecharacteristics between day 30 and discharge (Table 1 and
Appendix Table 5) illustrates this potential bias, because83.5% of the patients who died in the first 30 days were in
the cohort who did not fill a prescription for either clopi-dogrel or a PPI. The high 30-day mortality rate in thiscohort can be explained by the inclusion of high-risk pa-tients who may not have received clopidogrel or a PPI bythe choice of their physicians, whereas other high-risk pa-tients who were actually given prescriptions at dischargecould have been too sick to fill their prescriptions or couldhave been readmitted to the hospital before they filledthem. Of note, we examined the cohort at various assemblytime points, including 7 and 21 days after myocardial in-farction, and found no differences in the hazard rate ratiosof the effect of the interaction between PPIs and clopi-dogrel in relation to assembly time point.
Our studys strengths include the large size of our co-hort based on a nationwide, unselected population thatrepresents average patients in a contemporary clinical set-ting who have had a myocardial infarction. The DanishNational Patient Registry includes all hospital admissionsin Denmark and is therefore not affected by selection biasstemming from selective inclusion of specific hospitals,health insurance systems, or age groups. The concordancebetween drug dispensing and drug consumption is proba-bly high, because reimbursement of drug expenses is onlypartial, and most drugs, including PPIs, were not availableover the counter in Denmark during the study period (ex-
ceptions include aspirin and H2-antagonists). Because ofthe partial reimbursement of drug expenses by Danish au-thorities, we reasonably assumed that a patient whoclaimed a prescription from the pharmacy intended to takethe drug.
Our study has additional limitations. Clopidogrel re-sistance has been linked to genotype polymorphisms. Al-though we have no knowledge of the precise distribution ofthese polymorphisms in our largely white study popula-tion, several studies (28, 29) based in the countries thatsurround Denmark found variations in relevant genes thatmatched those reported earlier for white populations.However, generalizing these data to other racial and ethnicgroups should be done with caution. Finally, we had noinformation on the indications for PPI therapy.
In conclusion, PPIs seem to be associated with an in-creased risk for adverse cardiovascular outcomes regardlessof clopidogrel use, but concomitant PPI and clopidogreluse was not associated with any additional increase in riskover that observed for patients who received a PPI alone.
We believe that the increased cardiovascular risk associatedwith PPI use independent of clopidogrel is caused by un-measured confounders. These results seem to refute con-cerns about increased risk for ischemic events during con-comitant PPI and clopidogrel therapy.
From Copenhagen University Hospital Gentofte, Hellerup, Denmark,and Copenhagen University Hospital Glostrup, National Institute of
Public Health, University of Southern Denmark, and Copenhagen Uni-
versity Hospital Rigshospitalet, Copenhagen, Denmark.
Grant Support: By the Danish Medical Research Council (grant 271-
06-0572) and the Danish Heart Foundation (grant 10-04-R78-A2865-
22586).
Potential Conflicts of Interest: Disclosures can be viewed at www.acponline
.org/authors/icmje/ConflictOfInterestForms.do?msNumM10-0269.
Reproducible Research Statement: Study protocol and statistical code: Available from Dr. Charlot (e-mail, [email protected]). Data set: Not
available.
Requests for Single Reprints: Mette Charlot, MD, Department ofCardiology, Copenhagen University Hospital Gentofte, PA Research,
Post 67, Niels Andersens Vej 65, 2900 Hellerup, Denmark; e-mail, mc
@heart.dk.
Current author addresses and author contributions are available at www.annals.org.
References1. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE
Jr, et al. ACC/AHA 2007 guidelines for the management of patients with un-stable angina/non-ST-Elevation myocardial infarction: a report of the AmericanCollege of Cardiology/American Heart Association Task Force on PracticeGuidelines (Writing Committee to Revise the 2002 Guidelines for the Manage-ment of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarc-tion) developed in collaboration with the American College of Emergency Phy-sicians, the Society for Cardiovascular Angiography and Interventions, and theSociety of Thoracic Surgeons endorsed by the American Association of Cardio-vascular and Pulmonary Rehabilitation and the Society for Academic Emergency
Medicine. J Am Coll Cardiol. 2007;50:e1-e157. [PMID: 17692738]2. Steinhubl SR, Berger PB, Mann JT 3rd, Fry ET, DeLago A, Wilmer C, et al;CREDO Investigators. Clopidogrel for the Reduction of Events During Obser-vation. Early and sustained dual oral antiplatelet therapy following percutaneouscoronary intervention: a randomized controlled trial. JAMA. 2002;288:2411-20.[PMID: 12435254]3. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK; Clopi-dogrel in Unstable Angina to Prevent Recurrent Events Trial Investigators.Effects of clopidogrel in addition to aspirin in patients with acute coronary syn-dromes without ST-segment elevation. N Engl J Med. 2001;345:494-502.[PMID: 11519503]4. Hulot JS, Bura A, Villard E, Azizi M, Remones V, Goyenvalle C, et al.Cytochrome P450 2C19 loss-of-function polymorphism is a major determinantof clopidogrel responsiveness in healthy subjects. Blood. 2006;108:2244-7.[PMID: 16772608]
5. Ishizaki T, Horai Y. Review article: cytochrome P450 and the metabolism ofproton pump inhibitorsemphasis on rabeprazole. Aliment Pharmacol Ther.1999;13 Suppl 3:27-36. [PMID: 10491726]6. Gilard M, Arnaud B, Cornily JC, Le Gal G, Lacut K, Le Calvez G, et al.Influence of omeprazole on the antiplatelet action of clopidogrel associated withaspirin: the randomized, double-blind OCLA (Omeprazole CLopidogrel Aspirin)study. J Am Coll Cardiol. 2008;51:256-60. [PMID: 18206732]7. Gilard M, Arnaud B, Le Gal G, Abgrall JF, Boschat J. Influence of omeprazolon the antiplatelet action of clopidogrel associated to aspirin [Letter]. J ThrombHaemost. 2006;4:2508-9. [PMID: 16898956]8. Zuern CS, Geisler T, Lutilsky N, Winter S, Schwab M, Gawaz M. Effect ofcomedication with proton pump inhibitors (PPIs) on post-interventional residualplatelet aggregation in patients undergoing coronary stenting treated by dualantiplatelet therapy. Thromb Res. 2010;125:e51-4. [PMID: 19781742]9. Juurlink DN, Gomes T, Ko DT, Szmitko PE, Austin PC, Tu JV, et al. Apopulation-based study of the drug interaction between proton pump inhibitors
ArticleIncreased Cardiovascular Risk With Proton-Pump Inhibitors
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 385
-
8/8/2019 Ppi Original
9/16
and clopidogrel. CMAJ. 2009;180:713-8. [PMID: 19176635]10. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED, et al.Risk of adverse outcomes associated with concomitant use of clopidogrel andproton pump inhibitors following acute coronary syndrome. JAMA. 2009;301:937-44. [PMID: 19258584]11. Dunn SP, Macaulay TE, Brennan DM, Campbell CL, Charnigo RJ,Smyth SS, et al. Abstract 3999: Baseline proton pump inhibitor use is associated
with increased cardiovascular events with and without the use of clopidogrel in
the CREDO Trial. Circulation. 2008;118:S815.12. ODonoghue ML, Braunwald E, Antman EM, Murphy SA, Bates ER,Rozenman Y, et al. Pharmacodynamic effect and clinical efficacy of clopidogreland prasugrel with or without a proton-pump inhibitor: an analysis of two ran-domised trials. Lancet. 2009;374:989-97. [PMID: 19726078]13. Ray WA, Murray KT, Griffin MR, Chung CP, Smalley WE, Hall K, et al.Outcomes with concurrent use of clopidogrel and proton-pump inhibitors: acohort study. Ann Intern Med. 2010;152:337-45. [PMID: 20231564]14. U.S. Food and Drug Administration. Early Communication About an On-going Safety Review of Clopidogrel Bisulfate (Marketed as Plavix). Silver Spring,MD: U.S. Food and Drug Administration; 2009. Accessed at www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm079520.htm on 27 July2010.15. U.S. Food and Drug Administration. Follow-Up to the January 26, 2009, EarlyCommunication About an Ongoing Safety Review of Clopidogrel Bisulfate (mar-
keted as Plavix) and Omeprazole (marketed as Prilosec and Prilosec OTC). SilverSpring, MD: U.S. Food and Drug Administration; 2009. Accessed at www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm190784.htm on 27 July2010.16. European Medicines Agency. Public Statement on Possible Interaction Be-tween Clopidogrel and Proton-Pump Inhibitors. London: European Medicines
Agency; 2009. Accessed at www.emea.europa.eu/humandocs/PDFs/EPAR/Plavix/32895609en.pdf on 27 July 2010.17. Gaist D, Srensen HT, Hallas J. The Danish prescription registries. DanMed Bull. 1997;44:445-8. [PMID: 9377907]18. Srensen R, Gislason GH, Fosbl EL, Rasmussen S, Kber L, Madsen JK,et al. Initiation and persistence with clopidogrel treatment after acute myocardialinfarction: a nationwide study. Br J Clin Pharmacol. 2008;66:875-84. [PMID:18823305]19. Madsen M, Davidsen M, Rasmussen S, Abildstrom SZ, Osler M. The
validity of the diagnosis of acute myocardial infarction in routine statistics: acomparison of mortality and hospital discharge data with the Danish MONICAregistry. J Clin Epidemiol. 2003;56:124-30. [PMID: 12654406]20. Krarup LH, Boysen G, Janjua H, Prescott E, Truelsen T. Validity of strokediagnoses in a National Register of Patients. Neuroepidemiology. 2007;28:150-4.[PMID: 17478969]21. Tu JV, Austin PC, Walld R, Roos L, Agras J, McDonald KM. Develop-ment and validation of the Ontario acute myocardial infarction mortality predic-
tion rules. J Am Coll Cardiol. 2001;37:992-7. [PMID: 11263626]22. Rasmussen S, Zwisler AD, Abildstrom SZ, Madsen JK, Madsen M. Hos-pital variation in mortality after first acute myocardial infarction in Denmarkfrom 1995 to 2002: lower short-term and 1-year mortality in high-volume andspecialized hospitals. Med Care. 2005;43:970-8. [PMID: 16166866]23. Gislason GH, Jacobsen S, Rasmussen JN, Rasmussen S, Buch P, Friberg J,et al. Risk of death or reinfarction associated with the use of selectivecyclooxygenase-2 inhibitors and nonselective nonsteroidal antiinflammatorydrugs after acute myocardial infarction. Circulation. 2006;113:2906-13. [PMID:16785336]24. Schneeweiss S. Sensitivity analysis and external adjustment for unmeasuredconfounders in epidemiologic database studies of therapeutics. Pharmacoepide-miol Drug Saf. 2006;15:291-303. [PMID: 16447304]25. Rassen JA, Choudhry NK, Avorn J, Schneeweiss S. Cardiovascular out-comes and mortality in patients using clopidogrel with proton pump inhibitorsafter percutaneous coronary intervention or acute coronary syndrome. Circula-
tion. 2009;120:2322-9. [PMID: 19933932]26. Bhatt DL. A prospective, randomized, placebo-controlled trial of omeprazolein patients receiving aspirin and clopidogrel. Accessed at www.clinicaltrialresults.org on 8 April 2010.27. Yasuda H, Yamada M, Sawada S, Endo Y, Inoue K, Asano F, et al. Uppergastrointestinal bleeding in patients receiving dual antiplatelet therapy after coro-nary stenting. Intern Med. 2009;48:1725-30. [PMID: 19797827]28. Simon T, Verstuyft C, Mary-Krause M, Quteineh L, Drouet E, MeneveauN, et al; French Registry of Acute ST-Elevation and Non-ST-Elevation Myo-cardial Infarction (FAST-MI) Investigators. Genetic determinants of response toclopidogrel and cardiovascular events. N Engl J Med. 2009;360:363-75. [PMID:19106083]29. Varenhorst C, James S, Erlinge D, Brandt JT, Braun OO, Man M, et al.Genetic variation of CYP2C19 affects both pharmacokinetic and pharmacody-namic responses to clopidogrel but not prasugrel in aspirin-treated patients withcoronary artery disease. Eur Heart J. 2009;30:1744-52. [PMID: 19429918]
Article Increased Cardiovascular Risk With Proton-Pump Inhibitors
386 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
10/16
Current Author Addresses: Drs. Charlot, Ahlehoff, Norgaard, Jr-
gensen, Srensen, Hansen, Madsen, Torp-Pedersen, and Gislason: De-partment of Cardiology, Copenhagen University Hospital Gentofte, PA
Research, Post 67, Niels Andersens Vej 65, 2900 Hellerup, Denmark.
Dr. Abildstrm: Department of Cardiology, Copenhagen UniversityHospital Bispebjerg, Bispebjerg Bakke 23, 2400 Kbenhavn NV,
Denmark.
Dr. Kber: The Heart Centre, Copenhagen University Hospital Rigshos-
pitalet, Blegdamsvej 9, 2100 Copenhagen, Denmark.
Author Contributions: Conception and design: M. Charlot, C. Torp-
Pedersen, G. Gislason.Analysis and interpretation of the data: M. Charlot, O. Ahlehoff, M.L.
Norgaard, C.H. Jrgensen, P.R. Hansen, L. Kber, C. Torp-Pedersen,
G. Gislason.Drafting of the article: M. Charlot, P.R. Hansen, C. Torp-Pedersen, G.
Gislason.
Critical revision of the article for important intellectual content: M.
Charlot, O. Ahlehoff, M.L. Norgaard, C.H. Jrgensen, R. Srensen, S.Z.Abildstrm, P.R. Hansen, J.K. Madsen, L. Kber, C. Torp-Pedersen, G.
Gislason.
Final approval of the article: M. Charlot, O. Ahlehoff, M.L. Norgaard,
R. Srensen, S.Z. Abildstrm, P.R. Hansen, J.K. Madsen, L. Kber, C.Torp-Pedersen, G. Gislason.
Statistical expertise: M. Charlot, S.Z. Abildstrm, L. Kber, C. Torp-
Pedersen, G. Gislason.Obtaining of funding: M. Charlot, J.K. Madsen, C. Torp-Pedersen.
Administrative, technical, or logistic support: M. Charlot, O. Ahlehoff,
J.K. Madsen, C. Torp-Pedersen, G. Gislason.
Collection and assembly of data: M. Charlot, S.Z. Abildstrm, C. Torp-Pedersen, G. Gislason.
Appendix Figure 1. Cumulative claimed prescriptions for
clopidogrel after discharge for first myocardial infarction.
ClaimedPrescriptions,%
Time, d
0 10 20 30 40 50
0
20
40
60
80
100
Annals of Internal Medicine
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 W-125
-
8/8/2019 Ppi Original
11/16
Appendix Table 1. Descriptive Statistics for Clopidogrel and
PPI Therapy During Follow-up
Measure Patients NotReceivingClopidogrel
PatientsReceivingClopidogrel
Mean duration of PPI therapy (SD), d 147 (120) 152 (120)
Median duration of PPI therapy (IQR), d 104 (35269) 113 (38275)
Mean duration of PPI and clopidogrelcombination therapy (SD), d
33 (80)
Mean breaks in PPI therapy (SD), n 1 (1) 1 (1)
Initially receiving a PPI before startingclopidogrel therapy, n
2335
Started PPI therapy after startingclopidogrel therapy, n
5653
Stopped PPI therapy before stoppingclopidogrel therapy, n
4566
Receiving a PPI at end of study, n 4834 3465
Receiving clopidogrel at end of study, n 14 156
Receiving a PPI and clopidogrel at endof study, n
2335
Mean duration of clopidogrel therapy(SD), d
235 (129)
Median duration of clopidogrel therapy(IQR), d 298 (90354)
IQR interquartile range; PPI proton-pump inhibitor.
AppendixTable2.
AdverseOutcomesat1YearAfterInclusion
Outcome
PatientsNotReceivingClopidogrel(n
31
704)
PatientsReceivingClopidogrel(n
24702)
PatientsN
otReceivingaPPI
(n
22815)
PatientsReceivingaPPI
(n
8889)
PatientsN
otReceivingaPPI
(n
17949)
PatientsReceivingaPPI
(n
6753)
Person-Years
Events,
n(%)*
Rate
Person-Years
Events,
n(%)*
Rate
Person-Years
Events,
n(%)*
Rate
Person-Years
Events,
n(%)*
Rate
Cardiovascu
lar
death,
MI,orstro
ke
19453
4232(18.6
)
0.2
18
7074
2341(26.3
)
0.3
32
15583
1506(8
.4)
0.0
96
5540
1058(15.7
)
0.1
91
All-cause
death
20437
3269(14.3
)
0.1
60
7618
1873(21.1
)
0.2
46
16216
603(3
.4)
0.0
37
5986
475(7
.0)
0.0
79
Cardiovascu
lar
death
20437
2678(11.7
)
0.1
31
7618
1442(16.2
)
0.1
89
16216
516(2
.9)
0.0
31
5986
368(5
.5)
0.0
61
MI
19662
1791(7
.9)
0.0
91
7170
1029(11.6
)
0.1
43
15663
978(5
.5)
0.0
62
5596
704(10.4
)
0.1
25
Stro
ke
22815
1509(6
.6)
0.0
66
8889
724(8
.1)
0.0
81
17949
538(3
.0)
0.0
30
6753
298(4
.4)
0.0
44
MI
myocardialinfarction;PPI
proton-pum
pinhibitor.
*CalculatedbyusingtheKaplanMeiermethod.
W-126 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
12/16
Appendix Table 3. Propensity ScoreMatched Model Results of Probability of PPI Therapy During 1-Year Follow-up
Parameter Patients Not Receiving Clopidogrel (n 31 704) Patients Receiving Clopidogrel (n 24 702)
Estimate Odds Ratio (95% CI) P Value Estimate Odds Ratio (95% CI) P Value
Age 0.06 1.06 (1.031.09) 0.001 0.03 1.03 (0.991.06) 0.143
Male sex 0.15 0.85 (0.810.91) 0.001 0.20 0.82 (0.770.87) 0.001
Income group 0.06 0.94 (0.920.96) 0.001 0.13 0.88 (0.850.90) 0.001Shock 0.36 1.43 (1.171.75) 0.001 0.28 1.32 (0.951.85) 0.100
Diabetes with complications 0.01 0.99 (0.871.12) 0.84 0.13 1.14 (0.971.33) 0.115
Peptic ulcer 2.05 7.76 (6.479.31) 0.001 2.35 10.53 (7.4314.92) 0.001
PCI 0.07 1.07 (0.971.17) 0.158 0.10 0.90 (0.850.96) 0.002
Pulmonary edema 0.11 0.89 (0.731.10) 0.28 0.03 0.96 (0.701.35) 0.85
Cerebral vascular disease 0.16 1.17 (1.061.29) 0.002 0.17 1.18 (1.021.38) 0.031
Cancer 0.30 1.36 (0.941.95) 0.102 0.63 1.88 (1.182.98) 0.008
Cardiac dysrhythmias 0.17 0.84 (0.780.91) 0.001 0.01 1.01 (0.901.12) 0.91
Acute renal failure 0.47 1.62 (1.312.00) 0.001 0.93 2.53 (1.703.79) 0.001
Chronic renal failure 0.75 2.11 (1.762.52) 0.001 0.51 1.67 (1.252.13) 0.001
Loop diuretic 0.38 1.60 (1.291.98) 0.001 0.43 1.53 (1.431.65) 0.001
Spironolactone 0.12 1.13 (1.041.22) 0.003 0.17 1.18 (1.061.31) 0.002
Aspirin 0.26 0.77 (0.730.82) 0.001 0.32 0.72 (0.680.77) 0.001
Statin 0.08 0.93 (0.870.98) 0.009 0.12 0.89 (0.810.97) 0.010
-Blocker 0.06 1.07 (1.011.13) 0.032 0.12 0.88 (0.810.96) 0.003
ACE inhibitor 0.08 0.92 (0.870.97) 0.002 0.05 1.05 (0.991.12) 0.120Diabetes medication 0.06 1.06 (0.981.16) 0.184 0.01 1.01 (0.911.12) 0.90
ACE angiotensin-converting enzyme; PCI percutaneous coronary intervention; PPI proton-pump inhibitor.* Reference was no PPI therapy.
Appendix Table 4. Summary Data for Propensity ScoreMatched Case Patients and Control Participants
Parameter Patients Not Receiving Clopidogrel (n 8437) Patients Receiving Clopidogrel (n 6556)
Patients NotReceiving a PPI
PatientsReceiving a PPI
Difference Patients NotReceiving a PPI
PatientsReceiving a PPI
Difference
Mean 30.703 30.707 0.019 30.372 30.371 0.019
Minimum 10.518 10.320 0.000 11.486 11.486 0.000
10th percentile 18.101 18.101 0.000 18.118 18.119 0.000
25th percentile 22.754 22.753 0.001 21.796 21.796 0.000
75th percentile 36.380 36.378 0.002 37.203 37.204 0.003
90th percentile 43.768 43.771 0.010 45.091 45.081 0.011
Maximum 95.385 96.674 1.988 92.969 92.785 1.969
Total propensity score forall patients in group
259 042.1 259 078.3 161.736 199 109.6 199 121.8 127.047
PPI proton-pump inhibitor.
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 W-127
-
8/8/2019 Ppi Original
13/16
Appendix Figure 2. Distribution of probabilities of treatment with PPIs in propensity scorematched analysis.
PatientsReceiving
ClopidogrelandPPIs,%
Estimated Probability
0.90.840.780.720.660.60.540.480.420.360.30.240.180.12
0
2
4
6
8
10
12
14
PatientsReceiving
ClopidogrelbutNotPPIs,%
0
2
4
6
8
10
12
14
PatientsNotReceiving
ClopidogrelbutReceivingPPIs,%
Estimated Probability
0.9450.825 0.8850.7650.7050.6450.5850.5250.4650.4050.3450.2850.2250.1650.105
0
2
4
6
8
10
12
14
0
2
4
6
8
10
12
14
PatientsNotReceiving
Clopidogre
lorPPIs,%
PPI proton-pump inhibitor.
W-128 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 www.annals.org
-
8/8/2019 Ppi Original
14/16
Appendix Figure 5. Required size for an unmeasured
confounder.
20% prevalence in the cohort
30% prevalence in the cohort
OR
EC
RRCD
1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5
0
1
2
3
4
Size needed to account for the elevation of risk from 1 to 1.29. OREC
association between drug use category and confounder; RRCD associ-
ation between confounder and disease outcome.
Appendix Figure 3. Propensity scorematched KaplanMeier
estimates of cardiovascular death, myocardial infarction, or
stroke for subtypes of PPIs.
RiskinPatientsNotReceivingClopidogre
l,%
Time, dNo PPI
Omeprazole
Lansoprazole
Pantoprazole
Esomeprazole
30 90 150 210 270 330
60
70
80
90
100
RiskinPatientsReceivingClopidogrel,%
Time, d
30 90 150 210 270 330
60
70
80
90
100
PPI proton-pump inhibitor.
Appendix Figure 4. Risk for cardiovascular death, myocardial
infarction, or stroke for subtypes of PPIs.
Pantoprazole
Clopidogrel
+ Clopidogrel
Omeprazole
Clopidogrel
+ Clopidogrel
Lansoprazole
Clopidogrel
+ Clopidogrel
Esomeprazole
Clopidogrel
+ Clopidogrel
H2-antagonist
Clopidogrel+ Clopidogrel
Any PPI
Clopidogrel
+ Clopidogrel
No PPI*
Hazard Ratio (95% CI)
0.8 1.0 1.5 2.0
Time-dependent, propensity scorematched Cox proportional hazardsanalysis. PPI proton-pump inhibitor.* Used as reference.
www.annals.org 21 September 2010 Annals of Internal Medicine Volume 153 Number 6 W-129
-
8/8/2019 Ppi Original
15/16
-
8/8/2019 Ppi Original
16/16
Appendix Figure 6. Hazard ratio for cardiovascular death,
myocardial infarction, or stroke in subgroups treated with
PPIs.
Aged >70 y
Aged 70 y
Male
Female
Diabetes
Yes
No
Heart failure
Yes
No
PCI
YesNo
Any PPI
No PPI*
Hazard Ratio (95% CI)
Patients Not Receiving Clopidogrel
0.8 1 1.4 1.8
Aged >70 y
Aged 70 y
Male
Female
Diabetes
Yes
No
Heart failure
Yes
No
PCI
Yes
No
Any PPI
No PPI*
Hazard Ratio (95% CI)
Patients Receiving Clopidogrel
1 1.4 1.8