Pphn management
29
Diagnosis and Management of PPHN Dr Boopathi Sellappan Fellow Paediatric Cardiology, Bristol Childrens Hospital, Bristol, United Kingdom.
-
Upload
boopathi-sellappan -
Category
Healthcare
-
view
247 -
download
0
Transcript of Pphn management
Diagnosis and Management of PPHNDr Boopathi SellappanFellow Paediatric Cardiology, Bristol Childrens Hospital, Bristol, United Kingdom.
Persistent pulmonary hypertension(or persistent fetal circulation)
Characterised by sustained elevation in pulmonary vascuar resistance (PVR) rather than the decrease in PVR which normally happens after birth
Causes severe hypoxemia secondary to right-to-left shunting of blood through fetal circulatory pathways
Often preceded by severe fetal hypoxemia, prolonged stress, remodelling and abnormal vascularisation of pulmonary arteries
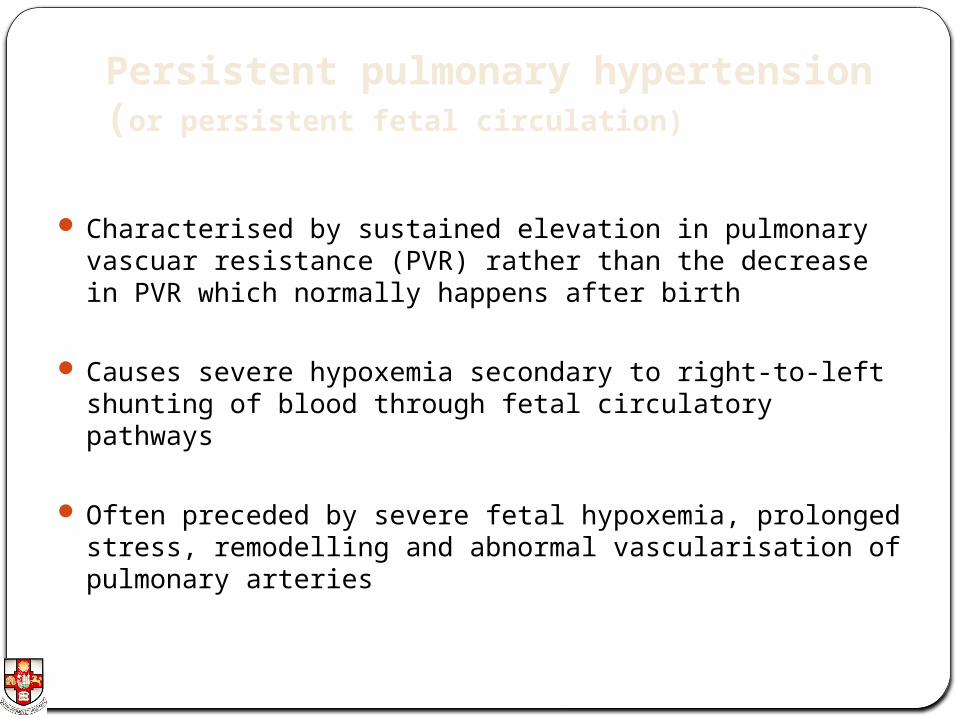
Fetal circulation.Aortic arch
Ductal arch

PPHN 2 to 6 per 1000 Live births 10-30% mortality Full term>preterm
Risk factors Meconium stained liqour Congenital pneumonia, surfactant deficiency Abnormal lung development-Pulmonary hypoplasia eg., potters sequele,
CDH etc., Polycythemia Preterm with prolonged rupure of membranes Maternal problems- Sepsis, Anaemia, Diabetis, SSRI intake, NSAID
Intake, Caesarean birth Myocardial dysfunction, myocarditis, Congenital heart disease, Lt to Rt
shunt ?Familial/ genetic predisposition.
Pediatrics. Aug 2007
Types of PPHN
Idiopathic PPHN Due to remodelling of pulmonary vessels
lung parenchymal diseases Meconium aspiration syndrome, Congenital pneumonia, Respiratory
distress etc
Hypoplastic lungs/ Vasculature eg.,Congenital diaphragmatic hernia

Endothelin pathwayNitric oxide pathway
Prostacyclin pathway
Vascular endothelial cell lining pulmonary arteryPreproendothelin
Proendothelin
Endothelin
L Arginine L Citrulline
Nitric Oxide
NO Synthase
Arachidonic acid
Prostaglandin I2
Prostacyclin(PG I2) CAMP
Smooth muscle cells in pulmonary artery
Regulation Of PA pressures
Vasoconstriction and proliferation
Cyclic GMP
Vasodilation and antiproliferation
The Lancet, Vol. 358, 2001

Clinical presentation of PPHN Respiratory distress
Cyanosis- Differential
Poor cardiac output and perfusion
Prominent precordial impulse
Single or narrow split, Loud S2, SM(TR)
>10% difference in pre and postductal saturation Beware of shunting at foramen ovale

Differential diagnosis Congenital heart disease
Primary pulmonary parenchymal diseasesCongenital pneumoniaCCAM, RDS/SDLDPulmonary sequestrationPulmonary hypoplasia etc.,
Sepsis
Alveolar capillary dysplasia
Investigations Septic screen, FBC, Renal and liver functions, Ca, Po4,
Magnesium,
Chest X ray- Normal or e/o pulmonary parenchymal disease
Transthoracic echocardiography (Urgent)
Arterial Blood gas
ECG- RV predominance, Myocardial ischemia or infarction
Cranial USS Scan

Oxygenation Index MAP x100 x FiO2
PaO2 (mmHg)
>25- Consider iNO>40 – Consider ECMO
Transthoracic ECHO in PPHN• Confirm Diagnosis
• Access ventricular function
• Exclude congenital heart defects
• Monitor progress
Findings
• Right to left shunting at level of PDA/foramen ovale(Beware of TAPVC)
• Flat septum/ pushed to the left
• Tricuspid regurtitation
• Pulmonary presure >=Systemic pressure(4*r2)
Skinner J Echocardiography for the neonatologist. Churchill Livingstone 2000

PPHN - Rt to Lt Shunt across PDA
Skinner J Echocardiography for the neonatologist. Churchill Livingstone 2000

Flat Septum/D Shaped Lt Ventricle
LV
RV
RV
LV
IVS IVS

Significant TR
RV
RA
LV
LA
Management Goals
• Pulmonary Vasodilation
• Systemic perfusion
• Oxygenation
• Minimal Iatrogenic trauma

Management In Tertiary NICU/PICU/CICU
Ongoing care and real time monitoring
Synchronised Ventilation/Oscillation, Pulmonary vasodilatos, Ionotropes
Correct hypothermia, acidosis, hypoglycemia, hypocalcaemia or hypomagnesaemia
Minimal handling
Exclude and treat other differentials

Ventilation• Minimimize Barotrauma
– HFOV useful in parenchymal lung disease– Oxygenation and ventilation with minimal tidal volume
• Sedation- Almost always• Paralysis- May be
• ? Increased risk of death and disbility
Blood Gases• PH- High normal• PCo2- > 35 mm Hg• PO2- >50 mm Hg
• Consider early surfactant – Useful in parenchymal disease

Haemodynamics Aim for high normal blood pressures to minimise Rt to Lt shunting
Ionotropes Dopamine, Noradrenaline, adrenaline, Dobutamine, Milrinone (To enhance myocardial contractility)
Real time monitoring of BP, saturations, pre and postductal saturations
4-6 hourly blood gases, Lactate
Crystalloids or colloids for filling
UAC/Peripheral arterial lines, UVC, Spare Jugulars for ECMO
Pulmonary Vasodilators Oxygen – Start with 100% FiO2
Nitric Oxide- Start at 20 PPM
Phosphodiestase inhibitors(Sildenafil PDE5, Milrinone PDE3)
Endothelin receptor antagonists- Bosentan
Prostacyclin I2 - Epoprostenol
Others- Sodium nitroprusside, Adenosine, Magnesium Sulphate
Exclude left to right shunt Pediatric Clin N Am 2012

Nitric Oxide (iNO)Advantages Superior speed of action, Targeted pulmonary effects, lack of reliance on gastric absorption Easy titrability
Disadvantages Cost Rebound PHT 30-40% unresponsive to iNO Rx Methaemoglobinemia
Cochrane Database of Systematic Reviews 2000

Sildenafil in PPHN Phosphodiesterase type 5 (PDE5) inhibitor Oral or IV, T1/2- 4hours Enteral route- 40% Peak bioavailability in 30-90 mins Multiple case reports and case series, few trials with small number Sildenafil in the treatment of PPHN-has significant potential especially in
resource limited settings. However, a large scale randomised trial comparing sildenafil with the currently used vasodilator, inhaled nitric oxide, is needed to assess efficacy and safety.Cochrane database syst 2011 Aug 10
Minimal and reversible side effects with short term use Enteral and IV preperations available

Alternatives Bosentan- Endothelin receptor antagonist
Few case reports and ongoing clinical trialsHepatotoxicity, teratogenicity, male infertility
Inhaled/IV Prostacyclin- Small studies have shown improvement in oxygenation
Short T1/2,Ventilation perfusion mismatch , systemic hypotension, unstable at neutral/acid PH, room temperature,rebound PHT
Adenosine infusions in small trials improved oxygenation
Magnesium sulphate, Sodium nitroprusside
Pediatric Clin N Am 2012

Endothelin pathwayNitric oxide pathway
Prostacyclin pathwayVascular endothelial cell lining pulmonary
artery
Preproendothelin
Proendothelin
Endothelin
L Arginine L Citrulline
NO Synthase
Arachidonic acid
Prostaglandin H2
Prostacyclin(PG I2)
Smooth muscle cells in pulmonary artery
Synergistic action of iNO
Vasoconstriction and proliferation
Cyclic GMPVasodilation and antiproliferation
Bosentan
Exogenous iNO
Epoprostenol
Sildenafil (PDE5
inhibitor)
Nitric Oxide

Beware of Systemic Hypotension with pulmonary vasodilators
Special Situations
PPHN in preterm
PPHN and Therapeutic hypothermia

Prematurity and PPHN Premature infants with PPROM and presumed severe
hypoxemic respiratory failure because of hypoplastic lungs often have significant PPHN and may show improvement in oxygenation after treatment with HFOV and INO
Early functional ECHO results in earlier identification and treatment of infants with PPHN in this high-risk group.
J Paediatr Child Health. 2011
PPHN and therapeutic hypothermia
Therapeutic hypothermia is not a risk factor for PPHN
Can be safely done in infants wih PPHN
Ela Chakkarapani, Perinatology 2010; 3:20-29

• Confirm diagnosis• Exclude/treat differential
• Ongoing Care(ABC) in a tertiary centre• Ventilation,Oxygenation, Normal BP• Sedation , ± paralysis, • Secure access- UAC,UVC• Exclude CHD• Correct hypothermia, hypoglycemia,
hypocalcaemia, hypomagnesaemia, Polycythemia
Oxygnation Index• > 25- Consider INO• >40 - Consider ECMO
Specific Rx- Pulmonary VasodilatorsO2Nitric OxideSildenafil- Oral/IV(± INO)Milrinone,Prostoglandins, Bosentan etc
Consider ECMO if no response
Sum
mar
y of
ca
re

Don’t forget the Parents
Thank you


















