PowerPoint Presentation - Allegheny Health Network · PDF file•TREVO –FDA 510(k)...
16
11/05/2015 1 Page 1 Endovascular Therapy REEMS Out Stroke Crystal Wong, MD Vascular Neurology November 13, 2015 Page 2 Acute Stroke Intervention • IV tPA has been the standard of care since 1995 (NINDS trial) – Can only be administered within 3 hours of stroke onset (or last known well) – Used off label in select circumstances up to 4.5 hours after stroke onset • Limitations to IV tPA – Time window – Eligibility criteria (mostly related to bleed risk) Page 3 Acute Stroke Intervention Endovascular thrombectomy used off label for many years Used in extended time window – usually up to 6 to 8 hours, in some cases longer Low risk of systemic bleeding Rescue therapy – higher rates of recanalization with large vessel occlusions Examples of devices – MERCI, Penumbra, retrievable stents (“stentrievers”)
Transcript of PowerPoint Presentation - Allegheny Health Network · PDF file•TREVO –FDA 510(k)...

11/05/2015
1
Page 1
Endovascular Therapy REEMS Out Stroke
Crystal Wong, MD
Vascular Neurology
November 13, 2015
Page 2
Acute Stroke Intervention
• IV tPA has been the standard of care since 1995 (NINDS trial) – Can only be administered within 3 hours of stroke onset
(or last known well) – Used off label in select circumstances up to 4.5 hours
after stroke onset
• Limitations to IV tPA – Time window – Eligibility criteria (mostly related to bleed risk)
Page 3
Acute Stroke Intervention
Endovascular thrombectomy used off label for many years Used in extended time window – usually up to 6 to 8 hours,
in some cases longer
Low risk of systemic bleeding
Rescue therapy – higher rates of recanalization with large vessel occlusions
Examples of devices – MERCI, Penumbra, retrievable stents (“stentrievers”)
11/05/2015
2
Page 4
Acute Stroke Intervention
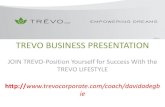
• Why consider endovascular therapy for acute ischemic stroke? – IV tPA is not always effective
• Poor recanalization rates for large vessel occlusion
• Pts who do not recanalize tend to have poor outcomes
– Many pts have contraindications to IV tPA
• TIME – present outside time window
• Recent procedure, GI bleed, etc
Page 5
Acute Stroke Intervention
31%
8%
24%
35% 40%
0%
5%
10%
15%
20%
25%
30%
35%
40%
All ICA MCA StemMCA Divsn MCA
Branch
Del Zoppo et al., Ann Neurol 1993
IV t-PA recanalization at one hour
(angiographic data)
Page 6
Middle cerebral artery branches (M2, M3)
Proximal middle cerebral artery (M1)
Internal carotid artery terminus
11/05/2015
3
Page 7
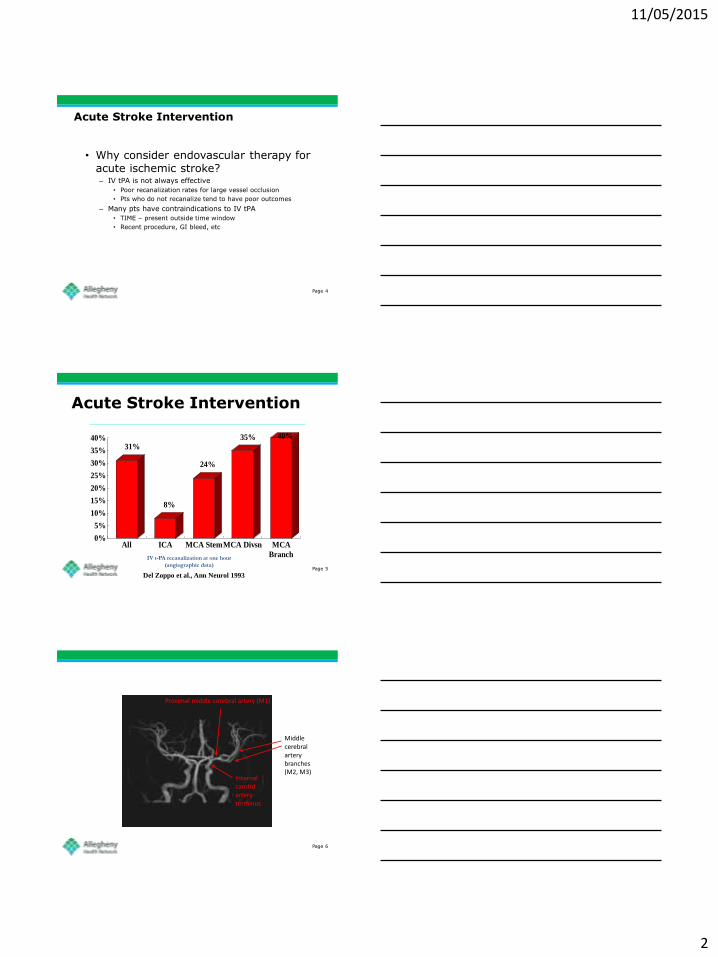
Acute Stroke Intervention
Riedel et al. Stroke, 2011
Page 8
Acute Stroke Intervention
Functional Independence
Dependent or bed-bound
Page 9
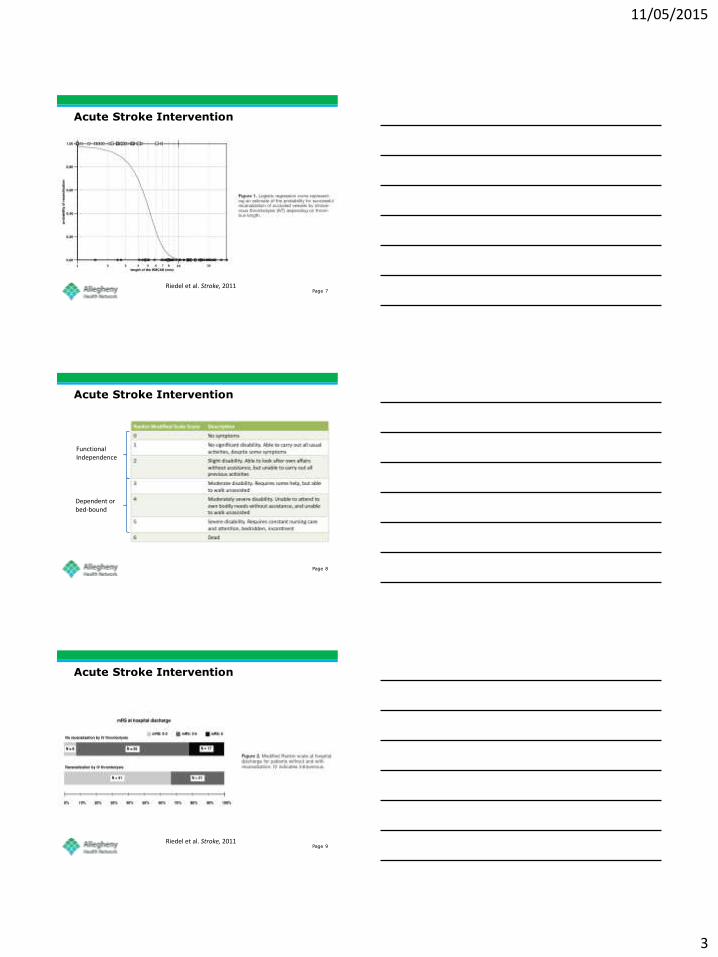
Acute Stroke Intervention
Riedel et al. Stroke, 2011

11/05/2015
4
Page 10
Acute Stroke Intervention
• Intra-arterial thrombolysis – 1999 - PROACT II – IA pro-urokinase
• MCA occlusions
• Within 6h of stroke onset
• 40% of treatment group showed improved outcome (mRS ≤ 2) compared to 25% of control group
• Increased intracranial bleeding rate in rx group (10% vs 3%)
• No difference in mortality
• Pro-urokinase not approved by FDA for endovascular treatment of acute ischemic stroke
Page 11
Acute Stroke Intervention
• 2004 – Interventional Management of Stroke (IMS) trial – IV tPA vs. IV tPA + IA tPA
– Open-label, non-randomized safety trial • No difference in mortality, ICH rates, or outcome scores
between groups
• IV tPA as bridging therapy to intra-arterial tPA is safe
• 2007 – IMS II – IV tPA + IA tPA vs. NINDS pts (IV tPA and placebo)
– Feasibility trial, non-randomized, single-arm
– Better functional outcome compared to both NINDS groups!
– No difference in safety endpoints (ICH, mortality)
Page 12
Acute Stroke Intervention
• Endovascular trials for device approval – Single arm, used historical data from prior
trials for comparison • MERCI/Multi-MERCI
• Penumbra
• SWIFT (Solitaire)
• TREVO
– FDA 510(k) medical device clearance • Easier to obtain than PMA (Pre-marketing approval),
which is much more stringent
• Does the device open up occluded cerebral arteries? Yes/No
• Endovascular devices are used “off-label” to open arteries when treating acute ischemic stroke

11/05/2015
5
Page 13
Acute Stroke Intervention
• 2013 – Three randomized, controlled endovascular acute stroke trials
– IMS III (2006-2012) • IV tPA vs. IV tPA + endovascular rx
– SYNTHESIS (2008-2012) • IV tPA vs. endovascular rx alone
– MR RESCUE (2004-2011) • Standard medical care (may include IV tPA) vs. Standard care +
endovascular rx
– No trial showed a benefit in favor of endovascular rx of acute ischemic stroke over the control group
Page 14
Acute Stroke Intervention
• Several drawbacks:
• Patient selection – Need to establish large vessel occlusion at presentation
• CTA/MRA not widely available at the time IMS III, SYNTHESIS were initiated
• Time is brain – Long times to treatment with IA therapy (4 to 5.5 hours from
onset) – Use of newer devices with faster, better recanalization
• Recruitment issues – More effective and speedy recruitment = larger sample size
and greater statistical power – Competing trials for same patient population – Lack of clinical equipoise – desire to use endovascular rx often
trumps enrollment into clinical trials
Page 15
• Endovascular Therapy “REEMS” Out Stroke
– REVASCAT
• June 2015
– ESCAPE
• February 2015
– EXTEND-IA
• February 2015
– MR CLEAN
• December 2014
– SWIFT-PRIME
• June 2015
11/05/2015
6
Page 16
MR CLEAN
Page 17
MR CLEAN
• Dutch study
• Randomized, controlled, open-label treatment with blinded endpoint assessments
• December 2010 – March 2014
• 16 medical centers (included all stroke centers)
• 500 patients – “usual care” (typically IV tPA alone) vs. “usual care” +
endovascular rx
• Selection – ≥ 18 yo; no upper age limit – Proof of anterior circulation artery occlusion on CTA/MRA – Ability to initiate IA within 6h of onset – NIHSS ≥ 2
• Treatment – Endovascular included IA thrombolysis, mechanical thrombectomy, or both
Page 18
MR CLEAN
RCT of IAT plus usual care vs. usual
care.
Similar pre-treatment characteristics
Proximal AOL in the anterior
circulation confirmed by CTA < 6
hours from onset
Outcome mRS ≤2 at 3 months
260 minutes - average time from
start of stroke symptoms to arterial
puncture for IAT:
11/05/2015
7
Page 19
ASPECTS
• Alberta Stroke Program Early CT Score
Page 20
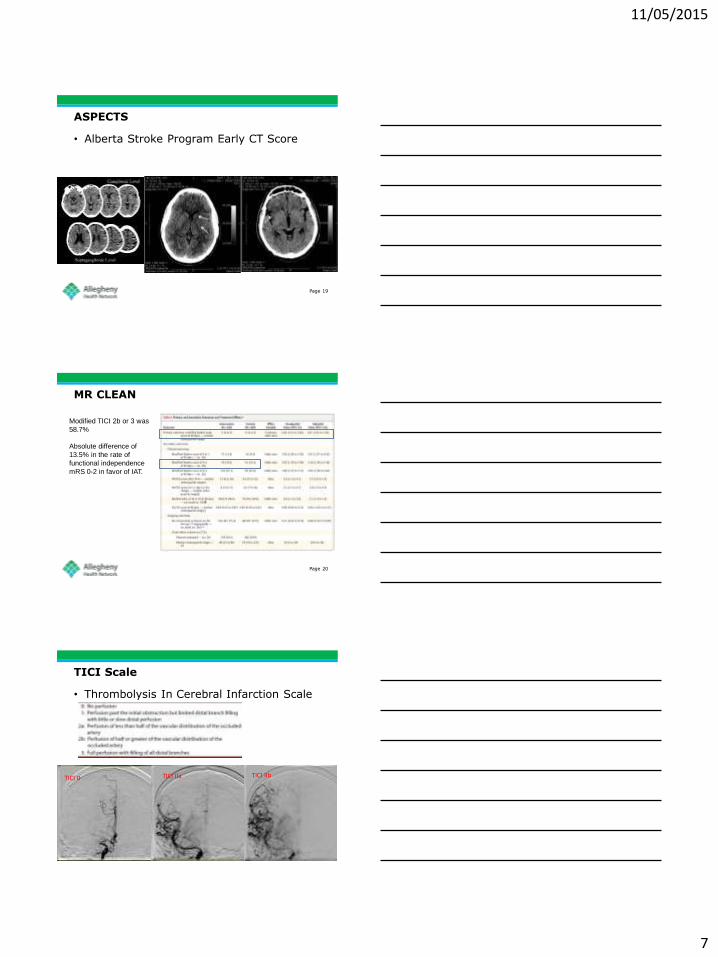
MR CLEAN
Modified TICI 2b or 3 was
58.7%
Absolute difference of
13.5% in the rate of
functional independence
mRS 0-2 in favor of IAT.
Page 21
TICI Scale
• Thrombolysis In Cerebral Infarction Scale
TICI 0 TICI IIb TICI IIa

11/05/2015
8
Page 22
MR CLEAN
No significant difference in SICH or
death.
Page 23
ESCAPE
Page 24
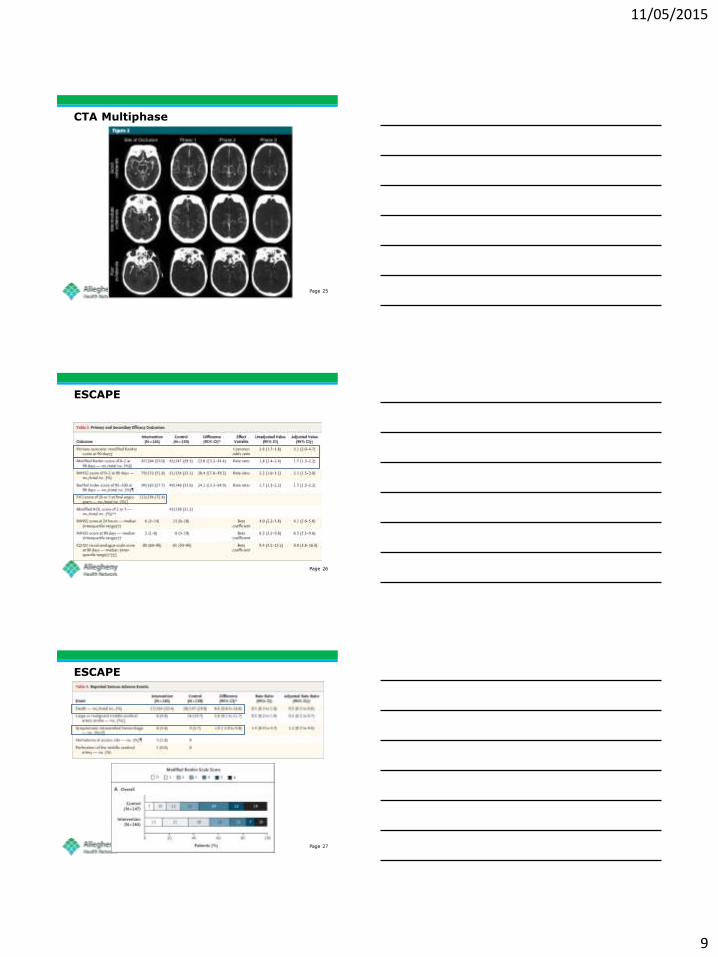
ESCAPE
Hypothesis – IAT vs standard care in patients with: 1. small core infarct 2. proximal AOL and 3. moderate-to-good collateral circulation – CTA
multiphase
Stopped for efficacy
11/05/2015
9
Page 25
CTA Multiphase
Page 26
ESCAPE
Page 27
ESCAPE

11/05/2015
10
Page 28
EXTEND IA
Page 29
EXTEND IA
IAT (Solitaire FR) vs usual care 1. Proximal AOL (ICAT, M1 M2) 2. Ischemic core <70 cc by CTP (Rapid Software)
Australia, New Zealand, 10 centers Stopped early after 70 patients randomized
Page 30
EXTEND IA
Reperfusion is % reduction of perfusion lesion volume at 24 hours. Early neurological improvement
is NIHSS decrease of 8 or 0-1 at day 3.
11/05/2015
11
Page 31
Page 32
SWIFT PRIME
Page 33
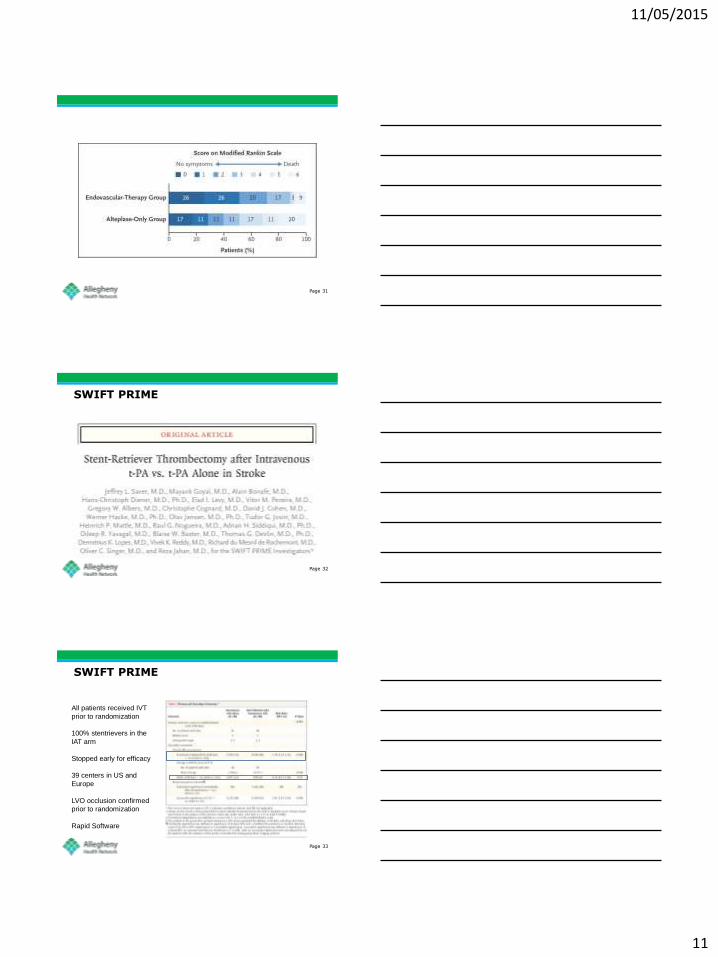
SWIFT PRIME
All patients received IVT
prior to randomization
100% stentrievers in the
IAT arm
Stopped early for efficacy
39 centers in US and
Europe
LVO occlusion confirmed
prior to randomization
Rapid Software
11/05/2015
12
Page 34
Page 35
REVASCAT
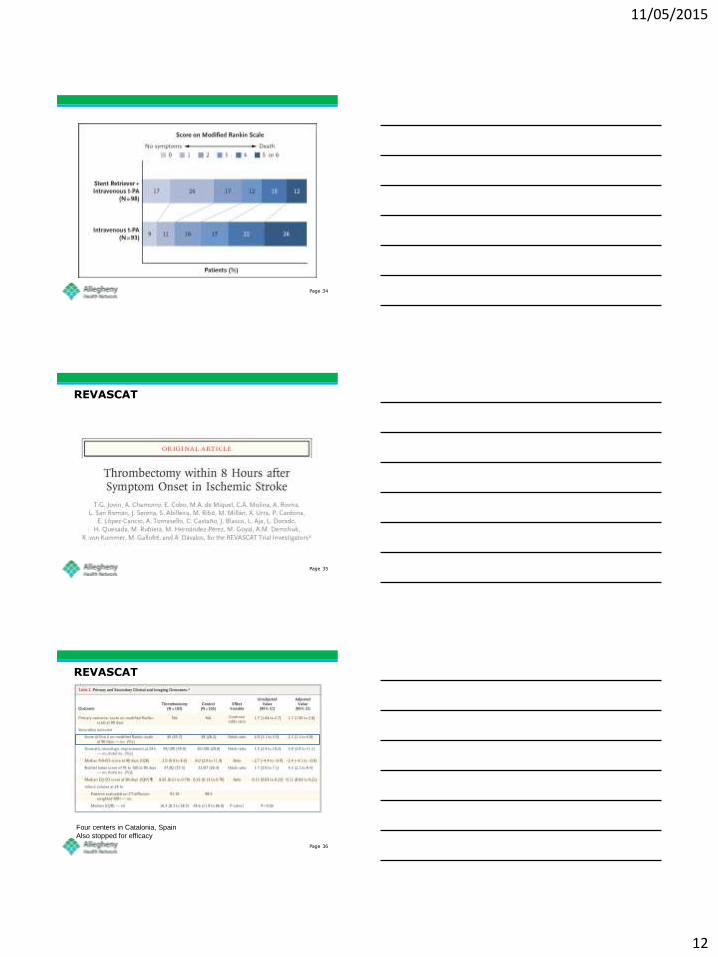
Page 36
REVASCAT
Four centers in Catalonia, Spain
Also stopped for efficacy
11/05/2015
13
Page 37
Page 38
Summary
Age NIHSS ASPECTS IVT Time to IAT IAT TICI ≥2b
Death SICH
mRS 0-2 favoring
IAT vs control
NNT for mRS 0-2
MR CLEAN
(n=233 IAT, n=267)
66 17 9 85% Onset to
GP 260 min
58.7% 18.9% IAT
vs 19% 6% IAT
13.5% increase
7
ESCAPE (n=165 IAT, n=150)
71 16 9 72%
Onset to first
reperfusion 241 min
72% 10.4% IAT
vs 19% 3.6% IAT
23% increase
4
EXTEND-IA (n=35 IAT, n=35) 68 17 -
100%
Onset to GP
210 min 86%
9% IAT Vs 20%
0% IAT 31%
increase 3
SWIFT PRIME (n=98 IAT, n=97)
61 17 9 100%
Onset to
GP 224 min
P2P 57 min
88% 9% IAT vs 12% (NS)
4% IAT 25%
increase 4
REVASCAT (n=103 IAT, n=103) 65 17 7 68%
Onset to GP
269 min 66%
15% IAT vs 18% (NS)
2.9% IAT
15% increase
6
Page 39
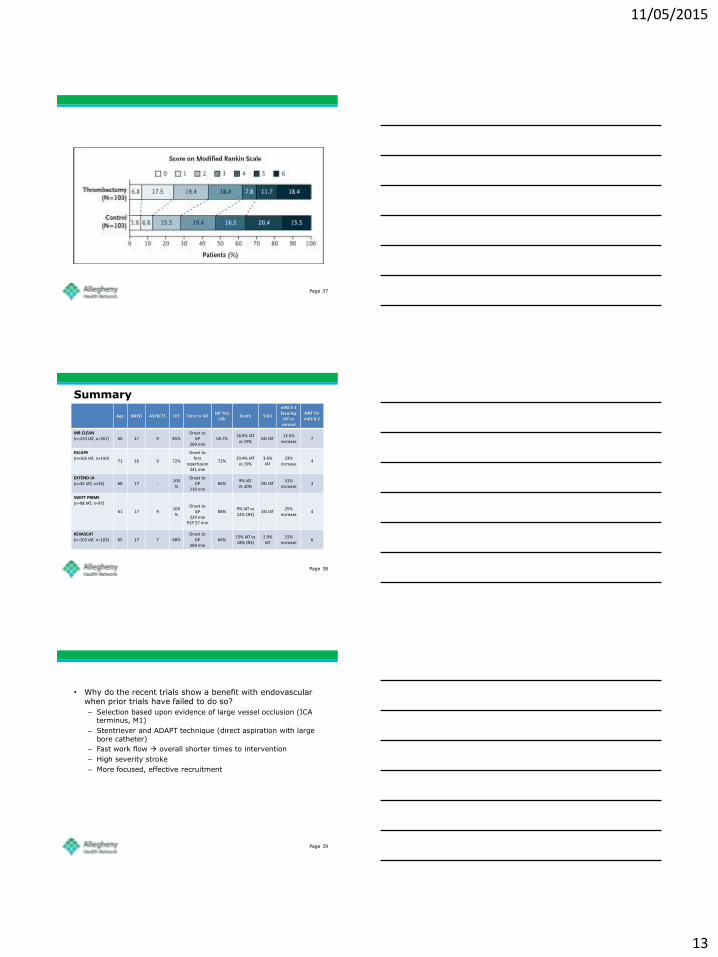
• Why do the recent trials show a benefit with endovascular when prior trials have failed to do so?
– Selection based upon evidence of large vessel occlusion (ICA terminus, M1)
– Stentriever and ADAPT technique (direct aspiration with large bore catheter)
– Fast work flow overall shorter times to intervention
– High severity stroke
– More focused, effective recruitment
11/05/2015
14
Page 40
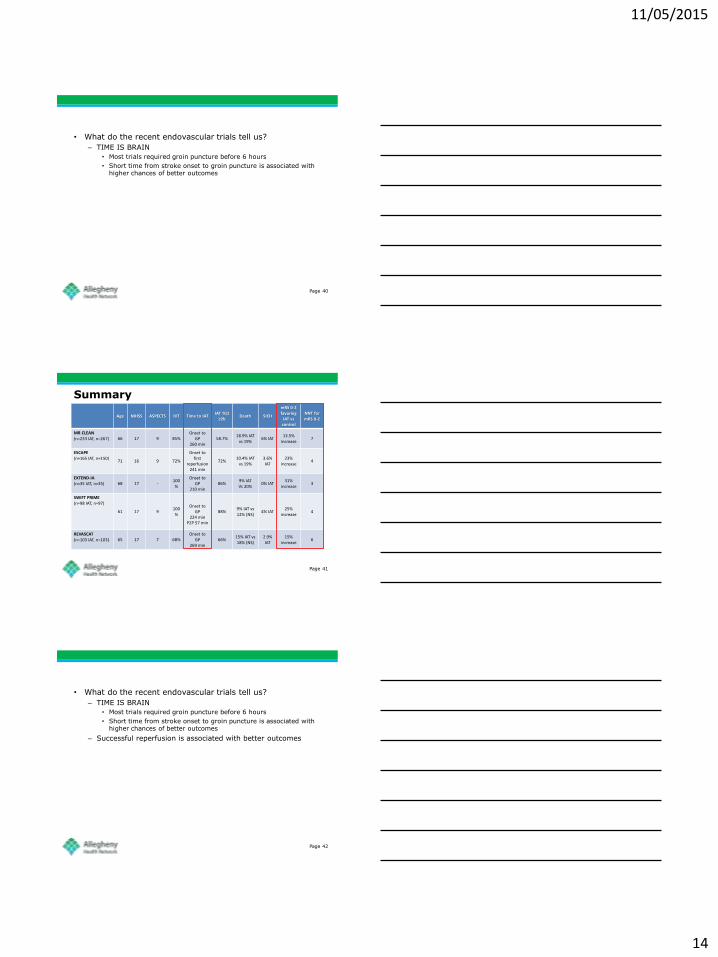
• What do the recent endovascular trials tell us?
– TIME IS BRAIN
• Most trials required groin puncture before 6 hours
• Short time from stroke onset to groin puncture is associated with higher chances of better outcomes
Page 41
Summary
Age NIHSS ASPECTS IVT Time to IAT IAT TICI ≥2b
Death SICH
mRS 0-2 favoring
IAT vs control
NNT for mRS 0-2
MR CLEAN
(n=233 IAT, n=267)
66 17 9 85% Onset to
GP 260 min
58.7% 18.9% IAT
vs 19% 6% IAT
13.5% increase
7
ESCAPE (n=165 IAT, n=150)
71 16 9 72%
Onset to first
reperfusion 241 min
72% 10.4% IAT
vs 19% 3.6% IAT
23% increase
4
EXTEND-IA (n=35 IAT, n=35) 68 17 -
100%
Onset to GP
210 min 86%
9% IAT Vs 20%
0% IAT 31%
increase 3
SWIFT PRIME (n=98 IAT, n=97)
61 17 9 100%
Onset to
GP 224 min
P2P 57 min
88% 9% IAT vs 12% (NS)
4% IAT 25%
increase 4
REVASCAT (n=103 IAT, n=103) 65 17 7 68%
Onset to GP
269 min 66%
15% IAT vs 18% (NS)
2.9% IAT
15% increase
6
Page 42
• What do the recent endovascular trials tell us?
– TIME IS BRAIN
• Most trials required groin puncture before 6 hours
• Short time from stroke onset to groin puncture is associated with higher chances of better outcomes
– Successful reperfusion is associated with better outcomes
11/05/2015
15
Page 43
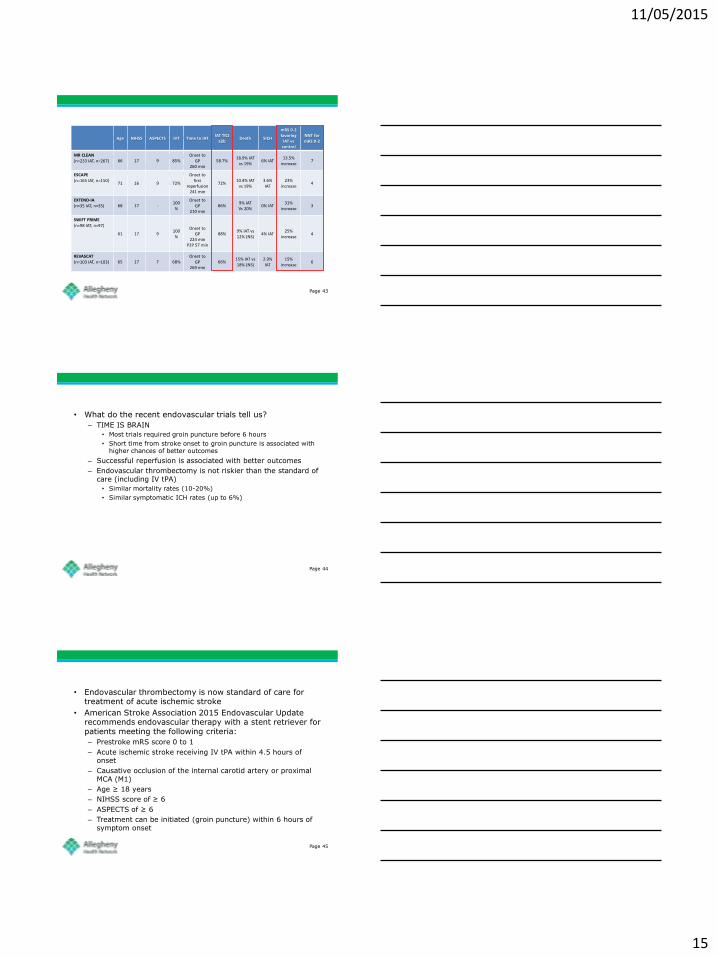
• What do the recent endovascular trials tell us?
– TIME IS BRAIN
• Most trials required groin puncture before 6 hours
• Short time from stroke onset to groin puncture is associated with higher chances of better outcomes
– Reperfusion is associated with better outcomes
Age NIHSS ASPECTS IVT Time to IAT IAT TICI ≥2b
Death SICH
mRS 0-2 favoring
IAT vs control
NNT for mRS 0-2
MR CLEAN (n=233 IAT, n=267)
66 17 9 85% Onset to
GP 260 min
58.7% 18.9% IAT
vs 19% 6% IAT
13.5% increase
7
ESCAPE (n=165 IAT, n=150)
71 16 9 72%
Onset to first
reperfusion 241 min
72% 10.4% IAT
vs 19% 3.6% IAT
23% increase
4
EXTEND-IA (n=35 IAT, n=35) 68 17 -
100%
Onset to GP
210 min 86%
9% IAT Vs 20%
0% IAT 31%
increase 3
SWIFT PRIME (n=98 IAT, n=97)
61 17 9 100%
Onset to
GP 224 min
P2P 57 min
88% 9% IAT vs 12% (NS)
4% IAT 25%
increase 4
REVASCAT (n=103 IAT, n=103) 65 17 7 68%
Onset to GP
269 min 66%
15% IAT vs 18% (NS)
2.9% IAT
15% increase
6
Page 44
• What do the recent endovascular trials tell us?
– TIME IS BRAIN
• Most trials required groin puncture before 6 hours
• Short time from stroke onset to groin puncture is associated with higher chances of better outcomes
– Successful reperfusion is associated with better outcomes
– Endovascular thrombectomy is not riskier than the standard of care (including IV tPA)
• Similar mortality rates (10-20%)
• Similar symptomatic ICH rates (up to 6%)
Page 45
• Endovascular thrombectomy is now standard of care for treatment of acute ischemic stroke
• American Stroke Association 2015 Endovascular Update recommends endovascular therapy with a stent retriever for patients meeting the following criteria:
– Prestroke mRS score 0 to 1
– Acute ischemic stroke receiving IV tPA within 4.5 hours of onset
– Causative occlusion of the internal carotid artery or proximal MCA (M1)
– Age ≥ 18 years
– NIHSS score of ≥ 6
– ASPECTS of ≥ 6
– Treatment can be initiated (groin puncture) within 6 hours of symptom onset

11/05/2015
16
Page 46
• Patients who have unfavorable advanced neuroimaging (perfusion, collateral grade) may not benefit from endovascular rx
• The new guideline recommendations are inclusion criteria (not exclusions) because they don’t address:
– Patients who are not eligible for IV tPA
– Patients with a prestroke mRS > 1
– Patients with “extended” time windows – those who physiologically have minimal infarct even after 6 hours
– Patients with occlusions of M2 branches, ACA, PCA, basilar or vertebral arteries
• These are smaller subpopulations that may still benefit from endovascular therapy on a case by case basis, and require further study
– Thus they should still be considered as potential candidates, and should be discussed with a vascular neurologist
Page 47
• Evaluation and administration of IV tPA should not be delayed in potential endovascular patients!!!
– Non-contrast head CT
– CTA/MRA head and neck (should not delay giving IV tPA)
– Advanced neuroimaging???
• Potential endovascular patients should be transferred to a Comprehensive Stroke Center
– Discussion with vascular neurologist
– 24/7 access to vascular neurology, neurosurgery, neurointensivists, neuroradiology, neurointerventionalists
– Transfer should occur as soon as possible
• Defer CTA/MRA and further imaging if performing them would delay transfer
Page 48
Questions?