PowerPoint ® Lecture Slides prepared by Betsy C. Brantley Valencia College C H A P T E R © 2013...
123
PowerPoint ® Lecture Slides prepared by Betsy C. Brantley Valencia College C H A P T E R © 2013 Pearson Education, Inc. The Lymphatic System and Immunity 13
-
Upload
gary-walden -
Category
Documents
-
view
227 -
download
4
Transcript of PowerPoint ® Lecture Slides prepared by Betsy C. Brantley Valencia College C H A P T E R © 2013...

PowerPoint® Lecture Slidesprepared byBetsy C. BrantleyValencia College
C H A P T E R
© 2013 Pearson Education, Inc.
The Lymphatic System and Immunity
13

© 2013 Pearson Education, Inc.
Chapter 13 Learning Outcomes
• Section 1: Anatomy of the Lymphatic System
• 13.1 • Describe the structure and function of important lymphatic
vessels, their relationship to blood vessels, and how lymph flows in the body.
• 13.2 • Describe the lymph collecting vessels, identify the structures
returning lymph to the venous system, and explain lymphedema.
• 13.3• Define lymphopoiesis, and discuss the classes of lymphocytes,
their importance, and their distribution in the body.• 13.4
• Identify and describe lymphoid tissues and lymphoid organs, and trace the pathway of lymph flow through a lymph node.

© 2013 Pearson Education, Inc.
Chapter 13 Learning Outcomes
• Section 2: Nonspecific Immunity
• 13.5• Explain how physical barriers and phagocytes play a role in
nonspecific defenses. • 13.6
• Explain the significance of inflammation and fever as mechanisms of nonspecific defenses, and summarize nonspecific defenses.
• Section 3: Specific Immunity
• 13.7• Explain how antigens trigger specific defenses and the immune
response.

© 2013 Pearson Education, Inc.
Chapter 13 Learning Outcomes
• 13.8• Discuss the structure of an antibody and the types of antibodies in
body fluids, and explain the primary and secondary responses to antigen exposure.
• 13.9• Explain the mechanisms used by antibodies to destroy target
antigens.• 13.10
• CLINICAL MODULE Define allergies and anaphylaxis and describe the role of antibodies in causing allergic and anaphylactic responses.
• 13.11• CLINICAL MODULE Describe autoimmune disorders, graft rejection,
allergies, immunodeficiency diseases, and age-related changes with respect to excessive or misdirected immune responses or inadequate immune responses.

© 2013 Pearson Education, Inc.
The Lymphatic System (Section 1)
• Includes cells, tissues, and organs that defend the
body against environmental hazards and internal
threats
• Cells are lymphocytes
• Vessels are lymphatic vessels (or lymphatics)
• Lymphoid tissues and organs are scattered
throughout the body

© 2013 Pearson Education, Inc.
The Lymphatic System (Section 1)
• Lymphocytes• Primary cells of lymphatic system that respond to:
• Invading pathogens
• Abnormal body cells
• Foreign proteins
• Most produced and stored within lymphoid tissues and organs
• Also produced in red bone marrow
• Surrounded by lymph
• Liquid that resembles interstitial fluid

© 2013 Pearson Education, Inc.
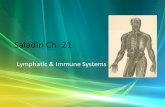
An overview of the lymphatic system
Figure 13 Section 1-2 2
Lymphatic Vessels and Lymph Nodes
Lymphoid Tissues and Organs
ThymusSpleenMucosa-associated lymphoid tissue(MALT) in digestive, respiratory,urinary, and reproductive tracts
Appendix
Tonsil
Cervical lymph nodesThoracic duct
Right lymphatic ductAxillary lymph
nodesCisterna chyli
Inguinal lymph nodes

© 2013 Pearson Education, Inc.
Fluid Flow (13.1)
• Lymphatic vessels
• Carry lymph from peripheral tissues to venous system
• Begin with lymphatic capillaries
• Found in almost every tissue and organ
• Closely associated with blood capillaries
• Interstitial fluid flows into lymphatic capillaries
• Fluid inside lymphatic capillaries is called lymph

© 2013 Pearson Education, Inc.
Arteriole
Endothelial cells
Lymphaticcapillary
Blood capillaries
Looseconnective
tissue
Lymphflow
Interstitialfluid
Venule
Lymphatic capillaries
Figure 13.1 1 1

© 2013 Pearson Education, Inc.
Lymphatic Capillaries (13.1)
• Lined by endothelial cells
• Incomplete or missing basement membrane
• Differ from blood capillaries
1. Originate as pockets instead of forming continuous
tubes
2. Have larger diameters
3. Have thinner walls
4. Look flattened or irregular in sectional view

© 2013 Pearson Education, Inc.
One-Way Flow (13.1)
• Overlapping endothelial cells in lymphatic
capillaries
• Act as one-way valve
• Permit entry of fluids and solutes
• Prevent return to intercellular spaces

© 2013 Pearson Education, Inc.
Sectional view of lymphatic and blood capillaries
Figure 13.1 2 2
Although lymphaticcapillaries are lined byendothelial cells, thebasement membrane isincomplete or missingentirely.
Overlapping endothelialcells act as one-way valve
Lymphflow
Lymphocyte
To largerlymphatics
Looseconnective
tissue
Interstitialfluid
Interstitialfluid
Looseconnective
tissueLymphaticcapillary
Bloodcapillary
Sectional view

© 2013 Pearson Education, Inc.
Lymphatic Flow (13.1)
• Lymph flows from lymphatic capillaries
• Into larger lymphatic vessels
• Toward body's trunk
• Larger lymphatic vessels contain valves
• Valves close together
• Vessels bulge at each valve
• Series of bulges make vessels resemble string of beads
• Low pressure in lymphatic vessels
• Valves prevent backflow

© 2013 Pearson Education, Inc.
Lymphatic vessels and valves
Figure 13.1 3 - 4 3 4–
Artery
Vein
Lymphaticvessel
To larger lymphatic vesselsthat deliver lymph to the venous system
From lymphaticcapillaries
Lymphatic valveLymphatic vessel
ArteryVein
Lymphatic valve
Lymphatic vessel
Valve in lymphatic vessel LM x 65

© 2013 Pearson Education, Inc.
Lymphatic Capillary Locations (13.1)
• Areas without blood supply have no lymphatic
capillaries
• Cornea of eye
• Other areas without lymphatic capillaries
• Red bone marrow
• Central nervous system

© 2013 Pearson Education, Inc.
Module 13.1 Review
a. What is the function of lymphatic vessels?
b. What is lymph?
c. What is the function of overlapping endothelial
cells in lymphatic capillaries?

© 2013 Pearson Education, Inc.
Extracellular Fluid Circulation (13.2)
• Blood confined to vessels of cardiovascular
system
• Water and solutes move from plasma into surrounding
interstitial fluid
• Lymph contained in lymphatic vessels
• Forms as interstitial fluid drains into lymphatic vessels

© 2013 Pearson Education, Inc.
Fluid Homeostasis (13.2)
• Continuous recirculation of interstitial fluid
1. Helps eliminate local differences in levels of nutrients,
wastes, and toxins
2. Maintains blood volume
3. Alerts immune system to infections in peripheral
tissues

© 2013 Pearson Education, Inc.
The circulation of extracellular fluid
Figure 13.2 1 1
The Circulation of Extracellular Fluid
StartArteries carry bloodaway from the heartand into the tissuesof the body.
Veins carry bloodfrom capillary beds tothe heart.
Capillaries are the smallest and mostdelicate blood vessels. All exchangebetween the blood and interstitialfluid occurs at capillaries.
At capillary networks, bloodpressure forces water and smallsolutes out of the bloodstream and into the surroundinginterstitial fluid.
Lymph forms as interstitialfluid enters lymphatic vessels.
Lymphatic vessels form anetwork that returns lymph tolarge subclavian veins nearthe heart.
1
2
Heart
Water andsolutes frombloodstream
3
4
56

© 2013 Pearson Education, Inc.
Lymphatic Drainage (13.2)
• Superficial and deep lymphatics converge to form:• Larger vessels, lymphatic trunks, which empty into:
• Collecting vessels
• Thoracic duct
• Right lymphatic duct
• Cisterna chyli is expanded chamber at base of thoracic duct• Receives lymph from inferior part of abdomen, pelvis,
lower limbs via:
• Right and left lumbar trunks
• Intestinal trunk

© 2013 Pearson Education, Inc.
Pattern of lymphatic fluid drainage in the body
Figure 13.2 2 2
Drainage ofthoracic duct
Drainage of rightlymphatic duct

© 2013 Pearson Education, Inc.
Lymphatic Ducts (13.2)
• Thoracic duct
• Collects lymph from:
• Body inferior to diaphragm
• Left side of body superior to diaphragm
• Empties into the left subclavian vein
• Right lymphatic duct
• Collects lymph from:
• Right side of body superior to diaphragm
• Empties into right subclavian vein

© 2013 Pearson Education, Inc.
Relationship between lymphatic ducts and the venous system
Figure 13.2 3 3
Right Lymphatic Duct
Right subclavianvein
Superior vena cava (cut)
Rib (cut)
Azygos vein
Intestinal trunk
Inferior vena cava (cut)
Right lumbar trunkLeft lumbar trunk
Cisterna chyli
Diaphragm
Parietalpleura (cut)
Thoraciclymph nodes
Thoracic duct
Thoracic Duct
Left jugular trunkLeft subclavian trunkThoracic duct enteringleft subclavian veinLeft bronchomediastinaltrunk
Right internaljugular vein
Brachiocephalicveins
Left internaljugular vein

© 2013 Pearson Education, Inc.
Lymphedema (13.2)
• Caused by blocked lymphatic drainage
• Interstitial fluid accumulates
• Causes swollen and distended areas
• Usually affects limbs; can affect other areas
• Swelling may become permanent
• Connective tissue loses elasticity
• Stagnant interstitial fluids may accumulate toxins and
pathogens
• Local immune defenses overwhelmed

© 2013 Pearson Education, Inc.
Lymphedema
Figure 13.2 4 4

© 2013 Pearson Education, Inc.
Module 13.2 Review
a. Name the two large lymphatic ducts into which
the lymphatic trunks empty.
b. Describe the drainage of the right lymphatic duct
and the thoracic duct.
c. Explain lymphedema.

© 2013 Pearson Education, Inc.
Lymphocytes (13.3)
• Account for 20–40 percent of circulating
leukocytes
• Circulating lymphocytes are a small fraction of
total lymphocyte population
• Three classes of lymphocytes
1. T cells
2. B cells
3. NK cells

© 2013 Pearson Education, Inc.
Antigens (13.3)
• All classes of lymphocytes are sensitive to
antigens
• Pathogens, parts or products of pathogens, or other
foreign substances
• Most are proteins
• Some are lipids, polysaccharides, and nucleic acids
• Stimulate an immune response

© 2013 Pearson Education, Inc.
T Cells (13.3)
• 80 percent of circulating lymphocytes
• Three major categories of T cells1. Cytotoxic T cells
• Attack foreign cells or body cells infected by viruses
• Primary cells involved in cell-mediated immunity
2. Helper T cells
• Stimulate activation and function of T cells and B cells
3. Suppressor T cells
• Inhibit activation and function of T cells and B cells
• With helper T cells, involved in sensitivity of immune response

© 2013 Pearson Education, Inc.
B Cells (13.3)
• 10–15 percent of circulating lymphocytes
• Differentiate into plasma cells when stimulated
• Produce and secrete antibodies
• Responsible for antibody-mediated immunity
• Some B cells become memory B cells instead of
plasma cells
• Remain in reserve to fight subsequent infections by
same antigen

© 2013 Pearson Education, Inc.
NK Cells (13.3)
• NK (natural killer) cells
• 5–10 percent of circulating lymphocytes
• Attack
• Foreign cells
• Body cells infected with viruses
• Cancer cells in normal tissues
• Continuously monitor peripheral tissues
• Immunological surveillance

© 2013 Pearson Education, Inc.
Classes of lymphocytes
Figure 13.3 1 1
Classes of Lymphocytes
T Cells B Cells NK Cells
CytotoxicT Cells
HelperT Cells
Suppressor T Cells
Plasma Cells
Cytotoxic T cell
Foreign or infected cell

© 2013 Pearson Education, Inc.
Lymphopoiesis (13.3)
• Lymphocyte production
• Involves:
• Red bone marrow
• Thymus
• Peripheral lymphoid tissues
• Red bone marrow primary in maintaining normal
lymphocyte population

© 2013 Pearson Education, Inc.
Lymphopoiesis in Red Bone Marrow (13.3)
• Hemocytoblasts generate lymphoid stem cells
• One group of lymphoid stem cells migrates to thymus
• Second group stays in red bone marrow and divides to
produce:
• B cells
• Mature and move into lymph nodes, spleen, other
lymphoid tissue
• NK cells
• Mature and migrate throughout body, patrolling
peripheral tissues

© 2013 Pearson Education, Inc.
Lymphopoiesis in Thymus (13.3)
• Blood-thymus barrier• Isolates stem cells from general circulation
• Thymic hormones• Stimulate lymphoid stem cells to divide, producing T
cells
• T cells • Produced and differentiate in thymus
• Reenter bloodstream when near mature and travel to:
• Red bone marrow
• Peripheral tissues

© 2013 Pearson Education, Inc.
The derivation and distribution of lymphocytes
Red Bone Marrow
Lymphoid stem cells
Lymphoid stem cells divide,producing various kinds of Tcells
Thymus
Migrates tothymus
Stays in red bone marrowand divides
Production anddifferentiationof immatureT cells Mature T cell B cells NK cells
As they mature, Bcells and NK cellsenter the bloodstreamand migrate toperipheral tissues.
Peripheral Tissues
When they arealmost mature,T cells reenterthe bloodstreamand either returnto the red bonemarrow or travelto peripherallymphoid tissuesand organs.
Cell-mediatedimmunity
Antibody-mediatedimmunity
Immunologicalsurveillance
Figure 13.3 2 2

© 2013 Pearson Education, Inc.
Lymphocyte Reproduction (13.3)
• Stem cells in red bone marrow
• Migrated B cells and T cells maintain ability to
divide
• Produce daughter cells of same type
• Crucial to success of immune response

© 2013 Pearson Education, Inc.
Module 13.3 Review
a. Identify the three main classes of lymphocytes.
b. Which cells are responsible for antibody-
mediated immunity?
c. Which tissues are involved in lymphopoiesis?

© 2013 Pearson Education, Inc.
Lymphoid Tissue (13.4)
• Connective tissue dominated by lymphocytes
• Lymphoid nodules
• Spherical masses of lymphoid tissue
• Lymphoid organs
• Lymph nodes, thymus, spleen
• Separated from surrounding tissues by fibrous
connective tissue

© 2013 Pearson Education, Inc.
Lymphoid Nodules (13.4)
• Clusters of lymphoid tissues
• Found in tracts opening to exterior environment
• Deep to epithelia lining passages
• As a group, called mucosa-associated lymphoid
tissue (MALT)

© 2013 Pearson Education, Inc.
The Tonsils (13.4)
• Three locations of large lymphoid nodules in walls of pharynx
1. Pharyngeal tonsil (or adenoid)
• Located on posterior, superior wall of nasopharynx
2. Palatine tonsils
• Located in posterior, inferior margin of oral cavity along boundary of pharynx
3. Lingual tonsils
• Deep to epithelium covering base of tongue
• Tonsillitis• Swollen tonsils from infection

© 2013 Pearson Education, Inc.
Lymphoid tissue in the body
Figure 13.4 1 - 2 1 2–
MALT in large intestine
Pharyngeal tonsil
Hard palatePalatine tonsilLingual tonsil

© 2013 Pearson Education, Inc.
Lymph Nodes (13.4)
• Small, lymphoid organs shaped like a kidney bean
• Function like a water filter
• Purifies lymph before reaching venous circulation
• Removes 99 percent of antigens from lymph
• Immune response stimulated as needed
• Afferent lymphatics bring lymph into lymph node
• Lymph flows through network of fibers and dendritic cells
• Involved in initiation of immune response
• Regions in lymph nodes contain B cells and plasma cells
• Efferent lymphatics carry lymph out of node toward veins

© 2013 Pearson Education, Inc.
Lymph node structure
Figure 13.4 3 3
Lymph node
Lymphatic vessel
Lymph nodesAfferent lymphatics
Dendritic cells
Regions containingB cells and plasmacells
Efferent lymphatics
Lymph node artery and vein

© 2013 Pearson Education, Inc.
The Thymus (13.4)
• Produces hormones important to development of
functional T cells
• Several complementary hormones known as
thymosins
• Size and secretory abilities decline with age
• Correlated with increased susceptibility to disease

© 2013 Pearson Education, Inc.
The thymus
Figure 13.4 4 4
Thyroid glandTrachea
Thymus
Heart
Diaphragm
Rightlung
Leftlung

© 2013 Pearson Education, Inc.
The Spleen (13.4)
• Contains largest mass of lymphoid tissue in body
• Same function for blood that lymph nodes
perform for lymph
1. Removes abnormal red blood cells by phagocytosis
2. Stores iron recycled from red blood cells
3. Initiates immune response by B cells and T cells

© 2013 Pearson Education, Inc.
The spleen
Figure 13.4 5 5
Diaphragm
Gastrosplenic ligament
Hilum
Gastric area
Renal area
Lateral surfaceof the spleen
Kidneys
Aorta
Spleen
SpleenSpleen
Pancreas
Rib
Stomach
Lateral surface of spleen
LiverLiver
Inferiorvena cava

© 2013 Pearson Education, Inc.
Module 13.4 Review
a. Name the lymphoid tissue that protects epithelia
lining the digestive, respiratory, urinary, and
reproductive tracts.
b. Define tonsils, and name the three types of
tonsils.
c. Describe the functions of the spleen.

© 2013 Pearson Education, Inc.
Immunity (Section 2)
• Ability to resist infection and disease
• Two forms that work independently and together
1. Nonspecific (innate) immunity
• Does not distinguish one type of pathogen from another
• Response is the same regardless of invading agent
• Present at birth (innate)
• Provide nonspecific resistance
2. Specific (adaptive) immunity

© 2013 Pearson Education, Inc.
Nonspecific Defenses (Section 2)
• Physical barriers
• Phagocytes
• Immunological surveillance
• Interferons
• Complement system
• Inflammatory response
• Fever

© 2013 Pearson Education, Inc.
Specific Defenses (Section 2)
• Protect against particular pathogen
• Depend on activities of specific lymphocytes
• Produce state of protection known as specific
resistance

© 2013 Pearson Education, Inc.
Overview of immunity
Figure 13 Section 2
Immunity
Nonspecific (Innate) Defenses Specific (Adaptive) Defenses Physical barriers
Phagocytes
Immunological surveillance
Interferons
The complement system
The inflammatory response
Fever
Destructionof abnormal
cells
Inflammation

© 2013 Pearson Education, Inc.
The Integumentary System (13.5)
• Provides major physical barrier to invasion by pathogens• Glands
• Sebaceous and sweat gland secretions flush surface• Wash away microorganisms and chemical agents• May contain bactericidal chemicals, destructive enzymes, and
antibodies
• Hair• Protects against mechanical abrasion• Often prevents hazardous material or insects from contact with skin
• Epithelial covering• Multiple layers• Keratinized cells in outer layers• Network of desmosomes locks adjacent cells together

© 2013 Pearson Education, Inc.
Integumentary system as a physical barrier to the external environment
Figure 13.5 1 1
Duct ofsweat gland
Hair Secretion
Epithelium
Sebaceousgland
KeratinizedcellsDesmosomes

© 2013 Pearson Education, Inc.
Epithelial Barriers (13.5)
• Line "tracts" (digestive, respiratory, urinary, and reproductive)
• Provide physical barrier
• Secretions contain enzymes, antibodies, or acid• Acid in stomach destroys many pathogens
• Mucus in respiratory tract traps pathogens
• Urine flushes urinary passageways
• Glandular secretions in reproductive tract flush tract
• MALT provides nonspecific defense

© 2013 Pearson Education, Inc.
Mucous membranes as a nonspecific defense barrier
Figure 13.5 2 2
Mucus
Mucouscell
Tight junctions
Basementmembrane
Epithelial cell
Epithelial cellstied together bytight junctions

© 2013 Pearson Education, Inc.
Phagocytes (13.5)
• "First line of cellular defense"
• Found in peripheral tissues
• Remove cellular debris
• Respond to invasion by foreign compounds or pathogens
• Can attack and remove microorganisms before lymphocytes detect presence
• Different types target different threats
• All function in same basic way

© 2013 Pearson Education, Inc.
Micrograph of phagocyte engulfing bacteria
Figure 13.5 4 4
Phagocyte (yellow)engulfing bacteria (orange)
SEM x 2900

© 2013 Pearson Education, Inc.
Types of Phagocytes (13.5)
• Neutrophils
• Abundant, mobile, fast-acting
• Phagocytize cellular debris or invading bacteria
• Eosinophils
• Less abundant than neutrophils
• Phagocytize foreign compounds or pathogens that have been
coated with antibodies
• Monocyte–macrophage system
• Macrophages derived from monocytes
• Fixed macrophages scattered among connective tissue
• Free macrophages travel throughout body

© 2013 Pearson Education, Inc.
Types of phagocytes
Figure 13.5 3 3
Types of Phagocytes
12 µm 8–10 µm Monocyte–macrophage system
Neutrophils Eosinophils
Fixed macrophages Free macrophages

© 2013 Pearson Education, Inc.
Functional Characteristics of Phagocytes (13.5)
• Can leave capillaries by squeezing between adjacent endothelial cells• Process called diapedesis
• May be attracted to or repelled by chemicals in surrounding fluids• Phenomenon called chemotaxis• Particularly sensitive to chemicals released by body cells or
pathogens
• Receptors on plasma membrane of phagocyte bind to surface of target• First step in phagocytosis
• After attaching, phagocyte either destroys target itself or promotes its destruction by activating specific defenses

© 2013 Pearson Education, Inc.
Module 13.5 Review
a. How does the integumentary system protect the
body?
b. Identify the types of phagocytes in the body, and
differentiate between fixed macrophages and
free macrophages.
c. Define chemotaxis.

© 2013 Pearson Education, Inc.
Inflammation (13.6)
• Localized tissue response to injury
• Produces swelling, redness, heat, and pain
• Caused by various stimuli that kill cells, damage connective tissue fibers, or injure tissue
• Result is altered chemical composition of interstitial fluid• Prostaglandins, proteins, potassium ions released
• Foreign proteins or pathogens introduced
• Changes trigger inflammation process

Chemical changein interstitial fluid
TissueDamage
© 2013 Pearson Education, Inc.
Inflammation and the steps in tissue repair
Figure 13.6 1 1
Slide 1

Chemical changein interstitial fluid
Mast cellsreleasehistamine andheparin
Mast Cell Activation
TissueDamage
© 2013 Pearson Education, Inc.
Inflammation and the steps in tissue repair
Figure 13.6 1 1
Slide 2

Chemical changein interstitial fluid
Phagocytes,especiallyneutrophils, areattracted to area
Blood vesselsdilate, bloodflow increas-es, vessel be-comes morepermeable
Clot forms(temporaryrepair)
Mast cellsreleasehistamine andheparin
Mast Cell Activation
Phagocyte Attraction
TissueDamage
Redness, Swelling, Heat, and Pain
© 2013 Pearson Education, Inc.
Inflammation and the steps in tissue repair
Figure 13.6 1 1
Slide 3

Chemical changein interstitial fluid
Release of cytokines(chemical messengers
affecting immunedefenses)
Neutrophils andmacrophagesremove debris;fibroblasts arestimulated
Specificdefensesareactivated
Clot forms(temporaryrepair)
Mast cellsreleasehistamine andheparin
Blood vesselsdilate, bloodflow increas-es, vessel be-comes morepermeable
Phagocytes,especiallyneutrophils, areattracted to area
Mast Cell Activation
Phagocyte Attraction
TissueDamage
Redness, Swelling, Heat, and Pain
© 2013 Pearson Education, Inc.
Inflammation and the steps in tissue repair
Figure 13.6 1 1
Slide 4

Chemical changein interstitial fluid
Mast Cell Activation
Phagocyte Attraction
Pathogensare removed,clot erodes,scar tissueforms
Tissue Repair
Clot forms(temporaryrepair)
Mast cellsreleasehistamine andheparin
Blood vesselsdilate, bloodflow increas-es, vessel be-comes morepermeable
Phagocytes,especiallyneutrophils, areattracted to area
Release of cytokines(chemical messengers
affecting immunedefenses)
Neutrophils andmacrophagesremove debris;fibroblasts arestimulated
Specificdefensesareactivated
TissueDamage
Redness, Swelling, Heat, and Pain
© 2013 Pearson Education, Inc.
Inflammation and the steps in tissue repair
Figure 13.6 1 1
Slide 5

© 2013 Pearson Education, Inc.
Fever (13.6)
• Rise in body core temperature above 37.2ºC
• Pyrogens (circulating proteins) reset temperature
thermostat in hypothalamus
• Can be beneficial within limits
• Inhibits some viruses and bacteria
• Increases body metabolism
• Quicker mobilization of tissue defenses
• Accelerated repair process

© 2013 Pearson Education, Inc.
Summary of Nonspecific Defenses (13.6)
• Physical barriers• Keep hazardous organisms and materials outside body
• Phagocytes• Engulf pathogens and cellular debris
• Immune surveillance by NK cells• Monitor peripheral tissues
• Release perforins that destroy abnormal cell's membrane
• Interferons• Released by lymphocytes, macrophages, or virus-infected cells
• Trigger production of antiviral proteins
• Stimulate macrophages and NK cells

© 2013 Pearson Education, Inc.
Summary of Nonspecific Defenses (13.6)
• Complement system
• Group of circulating proteins that help antibodies
destroy pathogens
• Inflammation (inflammatory response)
• Localized, tissue-level response to limit spread of injury
or infection
• Fever
• Accelerates body metabolism and defense activity

© 2013 Pearson Education, Inc.
Summary of Nonspecific Immunity
Figure 13.6 3 3
Physical Barriers
Prevent approach ofand deny access topathogens
Duct ofsweat gland
Secretions
Epithelium
Hair
Phagocytes
Remove debrisand pathogens
Neutrophil Eosinophil MonocyteFree
macrophageFixed
macrophage
Immune Surveillance by NK cells
Continuously monitornormal tissues anddestroy abnormal cells Natural killer cell Lysed abnormal cell
Interferons
Increase resistance ofcells to viral infection;slow the spread ofdisease
Complement System
When activated, attacks and breaksdown the surfaces of cells, bacteria,and viruses; attracts phagocytes;stimulates inflammation Complement
Lysedpathogen
Inflammation (Inflammatory Response)
Multiple effects makenonspecific and specificdefenses more effective
• Blood flow increased• Phagocytes activated• Damaged area isolated by clotting reaction• Capillary permeability increased• Complement activated• Regional temperature increased• Specific defenses activated
Fever
Mobilizes defenses;accelerates repairs;inhibits pathogens
Body temperature rises above 37.2°C inresponse to pyrogens
Mast cell
100
80
60
40
20
0

© 2013 Pearson Education, Inc.
Module 13.6 Review
a. What is the result of mast cell activation?
b. Summarize the body's nonspecific defenses.
c. A rise in the level of interferons in the body
suggests what kind of infection?

© 2013 Pearson Education, Inc.
Specific Immunity (Section 3)
• Protects against specific pathogens
• Coordinated activity of T cells and B cells provides
specific defenses
• T cells primarily responsible for cell-mediated
immunity
• Defends against abnormal cells and pathogens inside
cells
• B cells provide antibody-mediated immunity
• Defends against antigens and pathogens in body fluids

© 2013 Pearson Education, Inc.
Types of Specific Immunity (Section 3)
• Active immunity
• When body develops antibodies in response to antigen
• Passive immunity
• When receive antibodies from another source
• Both can be naturally acquired or artificially
acquired

© 2013 Pearson Education, Inc.
Forms of immunity
Figure 13 Section 3-1 1
Immunity
The ability to resistinfection and disease
Specific immunity is not present at birth;you acquire immunity to a specific antigenonly when you have been exposed to thatantigen or receiveantibodies fromanother source.
Specific (Adaptive) Immunity Nonspecific(Innate) Immunity
Present at birth—anatomical andother defensemechanisms
Active Immunity Passive Immunity
Produced by trans-ferring antibodiesfrom another source
Develops inresponse toantigen exposure
Naturally acquiredactive immunity
Artificially inducedactive immunity
Naturally acquiredpassive immunity
Artificially inducedpassive immunity
Conferred by admin-istering antibodies tocombat infection
Conferred bytransferringmaternal antibod-ies acrossplacenta or inbreast milk
Develops afteradministeringan antigen toprevent disease(as in a vaccine)
Develops afterexposure toantigens inenvironment

© 2013 Pearson Education, Inc.
Specific Properties of Specific Immunity (13.7)
• Specificity
• Each T cell or B cell has receptors that bind to one specific antigen,
but ignore all others
• Response of activated T cell or B cell specific only to that antigen
• Versatility
• Millions of different lymphocyte populations, each sensitive to
different antigen
• When activated, appropriate lymphocyte divides, producing more of
same lymphocyte type
• All cells produced by the division of activated lymphocyte
constitute a clone

© 2013 Pearson Education, Inc.
Specific Properties of Specific Immunity (13.7)
• Immunological memory
• Activated lymphocytes produce two groups of cells
• Group that attacks invader immediately
• Group that remains inactive unless exposed to same antigen later
• Memory cells that enable immune system to "remember" antigens
and launch faster, stronger, longer-lasting counterattack when
exposed again
• Tolerance
• Immune response ignores "self" but targets abnormal and foreign
("non-self")
• Can develop over time in response to chronic exposure to antigen

© 2013 Pearson Education, Inc.
Specific Defenses – Triggers (13.7)
• Exposure to antigen activates phagocytes, which
stimulate:
1. Cell-mediated defenses involving attacks by T cells
2. Antibody-mediated defenses
• First step is antigen presentation

© 2013 Pearson Education, Inc.
Overview of the immune response
Figure 13.7 1 1
Cell-MediatedImmunity
Specific Defenses
Antigen presenta-tion triggers spe-cific defenses, or animmune response.
Communicationand feedback
Phagocytesactivated
T cellsactivated
Direct Physical andChemical Attack
Activated T cellsfind the pathogensand attack themthrough phagocy-tosis or therelease of chemi-cal toxins.
Attack by CirculatingAntibodies
Antibody-MediatedImmunity
Activated Bcells giverise to cellsthat pro-duce anti-bodies.
Destroyantigens
Bacterium
Virus
1
2

© 2013 Pearson Education, Inc.
Antigen-Presenting Cells (13.7)
• Specialized cells
• Monocytes, macrophages, and dendritic cells
• Engulf a pathogen
• Digest pathogen to produce antigenic fragments
• Bind those fragments to proteins
• Display antigenic fragments on plasma membrane

© 2013 Pearson Education, Inc.
Antigen-presenting cells
Figure 13.7 2 2
Plasmamembrane
Phagocytic APCsengulf an extracel-lular pathogen.
Lysosomal actionproduces antigenicfragments.
Antigenicfragments arebound to theseproteins.
Antigenic fragmentsare displayed on theplasma membrane.
The rough endoplasmicreticulum producesproteins that will be incorporated into the phagocyticcell’s plasmamembrane.
Endoplasmicreticulum
NucleusNucleusLysosome
Phagocytic cell
1
2
3
4
5

© 2013 Pearson Education, Inc.
Defenses against Pathogens (13.7)
• Defenses against bacterial pathogens
• Usually initiated by active macrophages
• Followed by antigen presentation by macrophage
• Defenses against viruses involve:
• Direct contact with virus-infected cells
• Antigen presentation by antigen-presenting cells
(APCs)
• Release of interferons

© 2013 Pearson Education, Inc.
Defenses against bacterial and viral pathogens
Figure 13.7 3 - 4 3 4–
BACTERIA
Macrophageactivation
Antigenpresentation
Contact with activeAPCs activatescytotoxic T cells.Activated T cells divideto produce morecytotoxic T cells andinactive memory TC
cells.
Contact with thesurface of an activeAPC activates helperT cells. These cellsdivide to produceadditional activatedhelper T cells andmemory TH cells.
Contact with activatedhelper T cells activatesB cells. ActivatedB cells divide toproduce active plasmacells and inactivememory B cells.
Destroy bacteria by celllysis or phagocytosis
Plasma cells produceantibodies
VIRUSES
Infection of or uptakeby APCs
Infection oftissue cells
Release ofinterferons
Appearance of antigenin plasma membrane Antigen presentation
Contact with thesurface of an activeAPC activates helper T cells. These cellsdivide to produceadditional activatedhelper T cells andmemory TH cells.
ActivationofcytotoxicT cells
Contact withsurfaces ofinfected cellsstimulates NKcells.
Increasedresistance to viral infectionand spread
Destroyinfected cells
Contact with activatedhelper T cells activatesB cells. ActivatedB cells divide toproduce active plasmacells and inactivememory B cells.
Destroy viruses orprevent viruses fromentering into cells
Plasma cells produceantibodies

© 2013 Pearson Education, Inc.
Memory Cells (13.7)
• No role in initial infection
• Dramatically reduce response time for
subsequent infection by same pathogen
• Upon secondary exposure, differentiate into:
1. Cytotoxic T cells (memory TC cells)
2. Helper T cells (memory TH cells)
3. Plasma cells (memory B cells)
• Rapid and effective response

© 2013 Pearson Education, Inc.
Module 13.7 Review
a. Describe antigen presentation.
b. Which cells can be activated by direct contact
with virus-infected cells?
c. Which cells produce antibodies?

© 2013 Pearson Education, Inc.
Antibodies (13.8)
• Antibody molecule composed of:
• Two parallel pairs of polypeptide chains
• One pair heavy chains
• One pair light chains
• Each chain has:
• Constant segments
• Variable segments
• Constant segments of heavy chains form base of
molecule

© 2013 Pearson Education, Inc.
Antigen Binding Sites (13.8)
• Free tips of two variable segments
• Can interact with antigen similar to enzyme
interaction with substrate
• Differences in variable segment structure affect
shape of binding site
• Antibodies specific for different antigens
• Variation occurs during production, division, and
differentiation of B cells

© 2013 Pearson Education, Inc.
Antibody structure
Figure 13.8 1 1
Antigenbinding
site
Heavy chain
Disulfidebond
Variablesegment
Constantsegments
of lightand heavy
chains
Antigen binding sites
Light chain
Binding sites that can activate the complementsystem are covered when the antibody is secretedbut become exposed when the antibody binds toan antigen.
Binding sites may also be present that attach the secreted antibody to the surfaces of macrophages, basophils, or mast cells.

© 2013 Pearson Education, Inc.
Antigenic Determinant Sites (13.8)
• Antibody binds to antigen to form antigen-antibody
complex
• Binding between antibody and antigenic determinant
sites
• Specific portions of exposed antigen surface
• Bacteria may contain millions of antigenic determinant
sites

© 2013 Pearson Education, Inc.
Types of Antigens (13.8)
• Complete antigen• At least two antigenic determinant sites
• Partial antigen (or hapten)• Does not ordinarily activate B cells
• Can attach to carrier molecules and function as complete antigen
• Antibodies will attack hapten and carrier molecule
• If carrier molecule is normally found in tissues:
• Antibodies may attack normal cells
• Basis for drug reactions like allergy to penicillin

© 2013 Pearson Education, Inc.
Formation of antigen-antibody complex
Figure 13.8 2 2
Antigenic determinant sites
Antibody
Antigen-antibodycomplex
Complete antigen
Carriermolecule
Partial antigen(hapten)
Antibody
Partial antigen32
1

© 2013 Pearson Education, Inc.
Antigen
Antigenicdeterminant sites Antibodies
Antibodies bind to antigenic determinant sites
Figure 13.8 3 3

© 2013 Pearson Education, Inc.
Classes of Antibodies (13.8)
• Five classes of antibodies or immunoglobulins (Igs)
• Determined by differences in structure of heavy-chain
constant segments
1. IgG
2. IgE
3. IgD
4. IgM
5. IgA

© 2013 Pearson Education, Inc. Figure 13.8 4 4
IgG antibodies are responsible for resis-tance against many viruses, bacteria, and bacterial toxins. They account for 80 percent of all antibodies.
IgE attaches to basophils and mast cells, releasing histamine and speeding up inflammation.
IgD is an individual molecule on the surfaces of B cells, where it can bind antigens in the extra-cellular fluid. This binding can play a role in sensitizing the B cell.
IgM is the first class of antibody secreted after an antigen is encountered. IgM concentration declines as IgG production accelerates. The anti-A and anti-B antibodies responsible for the agglutination of incom-patible blood types are IgM antibodies.
IgA is found primarily in glandular secretions such as mucus, tears, saliva, and semen. These antibodies attack patho-gens before they gain access to internal tissues.

© 2013 Pearson Education, Inc.
Primary Response to Antigen Exposure (13.8)
• Primary response is initial response to exposure
• Takes time to develop
• Antigen activates B cells
• Differentiate into plasma cells
• Secrete antibodies
• Antibody titer (concentration) peaks one to two weeks
after exposure then declines if no longer exposed to
antigen

© 2013 Pearson Education, Inc.
Secondary Response to Antigen Exposure (13.8)
• Secondary response triggered when antigen
encountered again
• More extensive and lasts longer than primary
• Antibody titer increases rapidly and to much higher
levels
• Result of immediate response by memory B cells
• Appears even if second exposure is years after first
• Memory cells survive 20 years or more

© 2013 Pearson Education, Inc.
The primary and secondary responses in antibody-mediated immunity
Figure 13.8 5 - 65 6–
Primary response
IgMIgG
Time (weeks)
An
tib
od
y ti
ter
in p
las
ma
1 2 3 4 1 2 3 4Time (weeks)
IgG
IgM
Secondaryresponse

© 2013 Pearson Education, Inc.
Module 13.8 Review
a. Define antigenic determinant site.
b. Describe the structure of an antibody.
c. Name the five classes of immunoglobulins and
cite a function of each.

© 2013 Pearson Education, Inc.
Antibody Mechanisms (13.9)
• Seven different mechanisms for eliminating
antigens
1. Neutralization
2. Prevention of pathogen adhesion
3. Activation of complement
4. Opsonization
5. Attraction of phagocytes
6. Stimulation of inflammation
7. Agglutination

© 2013 Pearson Education, Inc.
Antibody Mechanisms (13.9)
1. Neutralization
• Bacteria and viruses must bind to plasma membrane of body cells
before they can enter cells
• Antibodies attach to binding sites on bacteria or toxins
• Neutralizes binding ability of bacteria and toxins
• No binding sites available now for attachment to body cells
2. Prevention of pathogen adhesion
• Antibodies part of saliva, mucus, tears, and perspiration
• Coating of antibodies creates barrier
• Difficult for pathogens to adhere to body surfaces

© 2013 Pearson Education, Inc.
Antibody Mechanisms (13.9)
3. Activation of complement
• Binding to antigen changes antibody molecule shape
• Exposed area binds to complement proteins, activating
complement system
4. Opsonization
• Coating of antibodies and complement makes surfaces of
bacteria less slick
• Phagocytes can bind more easily
5. Attraction of phagocytes
• Neutrophils, eosinophils, and macrophages attracted to antigens
coated with antibodies

© 2013 Pearson Education, Inc.
Antibody Mechanisms (13.9)
6. Stimulation of inflammation
• Antibodies stimulate release of heparin and histamine from
basophils and mast cells
• Promotes inflammatory response
7. Agglutination
• Antibodies can bind to antigenic determinant sites on adjacent
antigens
• Large numbers of antigens together create immune complex
• Formation of immune complex from surface antigens called
agglutination
• For example, clumping of erythrocytes in transfusion reaction

© 2013 Pearson Education, Inc.
Mechanisms antibodies use to destroy target antigens
Figure 13.9
Neutralization Prevention of Pathogen Adhesion Activation of Complement
Opsonization
Agglutination
ImmuneComplex
Antigenicdeterminant
sites
Stimulation of Inflammation
Attraction ofPhagocytes

© 2013 Pearson Education, Inc.
Module 13.9 Review
a. Describe the ways that antigen-antibody
complexes can destroy target antigens.
b. Define opsonization.
c. Which cells are involved in inflammation?

© 2013 Pearson Education, Inc.
Antibody Overreactions (13.10)
• Allergies
• Inappropriate or excessive immune responses to
antigens
• Sudden increase in cellular activity and antibody titers
• Neutrophils or cytotoxic T cells may destroy normal cells
in addition to antigen
• Antigen-antibody complex may trigger inflammation
• Antigens triggering allergic reactions called allergens

© 2013 Pearson Education, Inc.
Allergic Responses (13.10)
• Initial exposure to allergen
• Causes sensitization
• Production of large quantities IgE
• Immediate hypersensitivity
• Rapid, severe response to antigen
• Example is allergic rhinitis (includes hay fever)
• Inflammation of nasal membrane
• Hypersensitivity reaction
• May be limited to body surface or can be systemic

© 2013 Pearson Education, Inc.
Seasonal allergies
Figure 13.10

© 2013 Pearson Education, Inc.
Anaphylactic Shock (13.10)
• Allergen can trigger systemic response
• Anaphylaxis
• Circulating allergen stimulates histamine release from
mast cells throughout body
• Can cause extensive peripheral vasodilation
• Extreme drop in blood pressure leading to circulatory
collapse
• Anaphylactic shock

© 2013 Pearson Education, Inc.
Mechanism of anaphylaxis
Figure 13.10
First ExposureAllergen fragment
AllergensMacrophage TH cell activation
B cell sensitizationand activation
Plasma cell
IgE antibodies
SubsequentExposure
AllergenIgE
Granules
Massivestimulation of mast cellsand basophils
Sensitization ofmast cells andbasophils
Release of histaminesand other chemicals that
cause pain and inflammation
Localized Allergic Reactions Systemic Allergic Reactions
If the allergen is at the body surface: localized inflamma-tion, pain, and itchingExample: allergic rhinitis
If the allergen is in the bloodstream: itching, swelling, and difficulty breathing (due to constricted airway)Example: anaphylaxis

© 2013 Pearson Education, Inc.
Module 13.10 Review
a. Define allergy and allergen.
b. What is anaphylaxis?
c. Which chemicals do mast cells and basophils
release when stimulated in an allergic reaction?

© 2013 Pearson Education, Inc.
Immune Disorders (13.11)
• Can be excessive or misdirected immune
response
• Autoimmune disorders
• Graft rejection
• Allergies
• Can be inadequate immune response
• Immunodeficiency diseases
• Age-related reductions in immune activity

© 2013 Pearson Education, Inc.
Autoimmune Disorder Process (13.11)
• Immune system attacks body's own tissue
• Malfunction of "self" antigen recognition system produces
autoantibodies
• Affects about 5 percent of adults in North America and
Europe
• Many caused by similarities in proteins
• Protein associated with measles, Epstein–Barr, influenza, and
other viruses has the same amino acid sequence as myelin
proteins
• Antibodies targeting these pathogens may also attack myelin
sheaths
• Likely mechanism responsible for multiple sclerosis

© 2013 Pearson Education, Inc.
Autoimmune Disorders (13.11)
• Thyroiditis
• Inflammation from release of autoantibodies against
thyroglobulin
• Rheumatoid arthritis
• Autoantibodies attack connective tissue in joints
• Cause inflammation and destruction of joints
• Type I diabetes
• Autoantibodies attack insulin-producing cells in
pancreatic islets

© 2013 Pearson Education, Inc.
Autoimmune disorders
Figure 13.11

© 2013 Pearson Education, Inc.
Graft Rejection (13.11)
• Occurs after organ transplant
• Recipient's T cells activated by donated tissue
attack and destroy foreign cells
• Transplant success improved by
immunosuppression
• Reducing sensitivity of immune system
• Cyclosporin A (CsA)
• Suppresses immune response by inhibiting helper T cells
while not affecting suppressor T cells

© 2013 Pearson Education, Inc.
Inadequate Immune Response (13.11)
• Immunodeficiency diseases
• Result from:
1. Embryological development problems with lymphoid
organs and tissues
2. Infection with virus that depresses immune function
3. Treatment with or exposure to immunosuppressive
agents
• Age-related reductions in immune activity

© 2013 Pearson Education, Inc.
Immunodeficiency Diseases (13.11)
• Acquired immune deficiency syndrome (AIDS) • Most common immunodeficiency disease
• Caused by human immunodeficiency virus (HIV)
• Virus binds to CD4 proteins and infects helper T cells
• Infected cells synthesize and release new viral proteins
• Infected helper T cells destroyed by virus or immune defenses
• Impairs cell-mediated and antibody-mediated responses
• Suppressor T cells not affected by virus
• Body vulnerable to microbial invaders, opportunistic infections, cancer
• Spread by contact with body fluids (blood, semen, vaginal secretions)
• Infects 33 million people worldwide with 2 million deaths each year

© 2013 Pearson Education, Inc.
Immunodeficiency diseases
Figure 13.11
HIV (green) budding from an infected TH cell SEM x 40,000

© 2013 Pearson Education, Inc.
Age-Related Reductions in Immune Activity (13.11)• Immune system is less effective with age
• Thymus shrinks and thymic hormones decrease
• Increased susceptibility to viral and bacterial infections• T cells less responsive to antigens
• Fewer cytotoxic T cells respond to infection
• Number of helper T cells reduced
• B cells less responsive
• Antibody levels slower to rise after antigen exposure
• Vaccinations (flu, pneumonia) strongly recommended
• Increased incidence of cancer• Declining immune surveillance and elimination of tumor cells

© 2013 Pearson Education, Inc.
Age-related reductions in immune activity
Figure 13.11

© 2013 Pearson Education, Inc.
Module 13.11 Review
a. Define autoimmune disorders.
b. Describe immunosuppression.
c. Provide a plausible explanation for the increased
incidence of cancer in the elderly.