PowerPoint Presentation Challenges Health... · • at the core of the SPHCM curriculum; ......
81
FIMDP 2013 DEPT OF COMMUNITY MEDICINE SRM MEDICAL COLLEGE ,SRM UNIVERSITY & UNSW AUSTRALIA 9 TH & 10 TH JAN 2013
Transcript of PowerPoint Presentation Challenges Health... · • at the core of the SPHCM curriculum; ......

FIMDP 2013
DEPT OF COMMUNITY MEDICINE
SRM MEDICAL COLLEGE ,SRM UNIVERSITY
&
UNSW AUSTRALIA
9TH & 10TH JAN 2013

School of Public Health and Community Medicine
Seminar on Health Care Management
9th and 10th of January, 2013
Department of Community Medicine
SRM Medical College Hospital &
Research Centre
SRM University
Principle challenges of health
management
By way of introduction

University of New South Wales
• Established in 1949
• Ranked among the top 60 universities
in the world
• Founding member of Group of Eight
and of the Universitas 21
• More than 50 000 students from over
120 countries
• Eight faculties - Arts and Social
Science, Built Environment,
Engineering, Law, Medicine, Science,
Business and Fine Arts

School of Public Health and Community
Medicine (SPHCM)
• A leader in public health, community medicine, health management and system strengthening
• An extensive alumni network in Australia, the Asia-Pacific region and beyond

Faculty and students
> 90 academic, general and research staff> 200 conjoint or adjunct staff in clinical and research units
6 associated research centres
>$32 million in research funding > 400 published peer-reviewed papers a year
> 100 enrolled PhD candidates> 500 postgraduate coursework students.

Research strengths
• Infectious diseases
• Primary health care
• Health services management and research
• Global Health
• Indigenous health
• Ageing and aged care
• Social research


SPHCM Masters level programs
• at the core of the SPHCM curriculum;
• local and international reputations for:
– their relevance to work practice; and
– strong emphasis on adult education approaches to
learning.
• career-defining qualifications
Master of Public Health (MPH)
Master of International Public Health (MIPH)
Master of Health Management (MHM)
Dual degrees:
MPH/MIPH
MPH/MHM
MIPH/MHM

Enrolments in 2012
• Public Health 219
• Health Management 155
• International Public Health 83
• MPH/MHM 108
• MIPH/MHM 38
• MIPH/MPH 40
• PhD 113
Our students
• Currently over 500 students
• 25% international - from Asia, Africa, India, the Middle
East, Pacific, Europe, North and South America
• Medical, nursing and allied health backgrounds
• Minimum entry requirements for Masters coursework
programs
– Health or health related degree
– At least 2 years’ health or health related work experience
– English level minimum of IELTS 6.5 (TOEFL 100)
o Good English writing skills are essential for success
o Support for Academic Skills available at UNSW.

Master of Health Management (MHM)
• Oldest health management program in Australia (30 years)
• Internationally recognised
• Accredited by the Australian College of Health Service Executives
• Alumni hold senior health management positions globally, particularly in Asia/Pacific
• MHM program designed to
• meet the needs of health managers (Australia and other countries)
• set the benchmark for health services management training
• MHM program equips graduates to
• be leaders in their field
• develop skills & knowledge to manage health services effectively
• produce and evaluate health policy and related research
• effectively deal with workforce and finance issues.

MHM program structure
Core courses Units of
Credit
Semester*
Foundations in Public Health and Health Care Systems 6 1
Strategy, policy and change 6 1
Healthcare economics and financial management 6 1
Health leadership 6 2
Clinical governance and risk 6 2
Evidence informed decision making 6 2
The program comprises 48 units of credit (UOC) consisting of 36 UOC of core
courses and 12 UOC of elective courses. Each course contributes 6 UOC.

Core courses Electives
Health Promotion and
Social Perspectives of
Health*~
Community
Development
Economic Evaluation in
Health Care
Principles and Practice
of Primary Health Care
Services in the
Community
Management of
Laboratory Services
Foundations In Public
Health and Health Care
Systems *+~
Advanced Health
Economics and
Financial Management
Comparative Health
Care Systems
HIV Aids: Australian and
International Responses
Managing Human
Resources for Health
Epidemiology and
Statistics For Public
Health*
Program Design and
Evaluation
Advanced Biostatistics
and Statistical
Computing
The Global HIV
Epidemic: Social
Aspects and Impacts
Outbreak Investigation
Strategy Policy and
Change+
Qualitative Research
Methods
Advanced Epidemiology Inequalities and Health Public Mental Health in
Australia
Healthcare Economics
and Financial
Management+
Prevention and
Management Of Chronic
Disease
Tobacco, Alcohol and
Illicit Drugs
Health Impact
Assessment
Current Challenges In
Infectious Disease
Health Leadership and
Workforce
Management+
Applied Research
Methods For Public
Health
Reproductive, Maternal
and Children's Health
Public Health
Perspectives of
Indigenous Health
Communicable
Diseases in
Humanitarian
Emergencies and
Disasters
Clinical Governance and
Risk Management+
Ethics and Law In
Public Health
Rehabilitation and
Restorative Care
Indigenous Health and
Wellbeing Across The
Lifespan
Tropical Disease Control
Evidence-informed
Decision-making+
Policy Studies Management of Aged
Care Programs and
Services
Case Studies in
Aboriginal and Torres
Strait Islander Health
Mathematical Modeling
of Infectious Disease
International Health~ Environmental Health Health Aspects of
Crises, Emergencies
and Disasters
Social and Cultural
Aspects of Contagion
Communication in
Public Health
*Core course in MPH
+Core course MHM
~Core course in MIPH

Managing health services:Perspectives and challenges

‘Modern’ approaches to management
• The 20th Century has been called the ‘management’
century
• Roots of current management theory in engineering and
predominantly in the USA
• Three ages of management:
• The age of scientific management (productivity) from
early 1900s until WWI
• The age of modern management (human relations
and strategic thinking) until the 1980s
• The age of change (‘nervous’ globalism, GFC and its
causes, focus on transformational leadership)

From management to health management
• What makes managing health services different to
managing other types of public and private services?
– All the same areas of practice +++++
– Health systems are complex, and prone to wicked
problems

Productivity Commission 2010, Strengthening Evidence Based Policy in the Australian Federation, Volume 1: Proceedings, Roundtable Proceedings,
Productivity Commission, Canberra. http://www.pc.gov.au/research/confproc/strengthening-evidence 18

• Planning and goal setting
• Strategy development and
implementation
• Decision making
• Innovation and change
• Human resources and diversity
• Organisational behaviour
• Leadership
• Motivation
• Communication
• Productivity and quality
• Marketing
• Finance and accounting
• Project management
• Operations management
• Occupational health and safety
• Location and resources
• Legal and regulatory requirements
• Training and development
• Work based learning
• Finance
• Teamwork
• Policy and guideline development
• Compensation and payment
• Development of adaptive ‘learning’
organisations
• Recruitment and retention
• Job analysis
• Career development
• Performance management
• Employee well being
• Work life balance
• Organisational communication
• Corporate culture, climate and
environment
• Information technology
What does management involve?

• Health insurance
• Public and private financing
• Health system organization
• Overall health care spending
• Hospital spending and utilization
• Health care access
• Chronic care management
• Disease prevention
• Capacity for quality improvement
• Public views and loss of trust
• Ethics (professional, public)
• Innovations
• Performance indicators
• Efficiency and integration of
services
• Care coordination
• Use of health information
technology
• Use of evidence-based practice
• Translational research
• Cost containment
• Accreditation, regulation
• Reforms
• Health disparities
• Quality of care
• Patient safety
In addition healthcare managers are
concerned with:

Research
Inputs
Processes
Socio-cultural, political, economic and legal context
Outputs
and
outcomes
Equity
Quality and
safety
Acceptability
Efficiency
Workforce
Finance
Governance
Consumers
population,
groups,
individuals
Public
health
Primary
healthcare
Hospitals
Specialist
services
and
providers
Pharma-
ceuticals
Aged care
and
disability
services
Research
CommunitiesEnvironments
Consumer
Numbers
Education
of health professionals
Assistive
technology
Community
health

Structural
Political
Cultural
Educational
Emotional
Physical and technological
Specific challenges in achieving and sustaining
healthcare quality
Bate, Mendel and Robert (2008)

So what makes healthcare settings different?
• The stakes are very high
• The level of stress can be intense
• The demands are multiple and ongoing
• Staff have to deal with errors and adverse events as well as
patients/families (Yu’s ‘second victim’)
• Staff’s identities are tied up with their jobs/roles
• There is a culture of commitment (good and bad)
• Staff are exposed to risks far beyond those of the general population
• High and increasing levels of media, government and public scrutiny
• It’s rarely just a ‘job’
• Multiple professions, disciplines, approaches, attitudes, experiences
• Emerging roles, professions and practices, including those of
administrative and ancillary staff

Key challenges in health
management

Is high quality, high safety healthcare possible?
• Given the chaos of current world events?
• Given the turbulence of health care systems?
• Given the types and range of illnesses, diseases and
injuries treated?
• Given the history, power and embedded structures of
professions and services?
• Given the limitations of the knowledge and practice
of quality improvement strategies and systems?
• Given the complexity of clinician-patient
interactions?
• Given … [your own personal concerns] …?

Some key challenges
1. What are the current and future issues healthcare services?
2. How do we manage change and the pressure to change?
3. How do we improve communication and teamwork?
4. How do we look at the healthcare system in a new way?
5. How can we act as both managers and leaders?
6. How can we address inequities at all levels of the health system?
7. How can we make a difference?

Challenge 1: current and future
issues affecting healthcare
Scanning the horizon

Challenge 1: Issues affecting healthcare globally
and global healthcare
1. Demography
2. Healthy behaviours
3. Disease and disability
4. Workforce
5. Public attitudes and expectations
6. Broader determinants of health
7. Medical advances
8. Information technologies
9. Sustainable services
10.Economic pressures
The King’s Fund

Challenge 2: managing change
Managing the inevitable

Change
• Continuous or intermittent/sequential or
spasmodic/sudden/disruptive
• Managed/unmanaged
• Proactive/reactive
• The act or fact of changing; substitution of one thing for
another; succession of one thing in place of another;
substitution of other conditions or circumstances, variety.
(OED)

Patient safety strategies fall into eight categories
Change the awareness level of the individual
Change the skill of the individual
Change the practice
Change the environment
Change the task
Change the team
Change the organisation
(service, hospital)
Change the system
Challenge 3: How do we manage change?
Questions [we often fail] to ask about change:
1. What is the (perceived) relative advantage of the innovation/change?
2. How compatible is the innovation to the people who are meant to implement it?
3. How complex is the innovation?
4. Can we pilot it first?
5. Will everyone be able to see the outcomes?
6. How will we know that it is successful?
Modified from Professor John Øvretveit
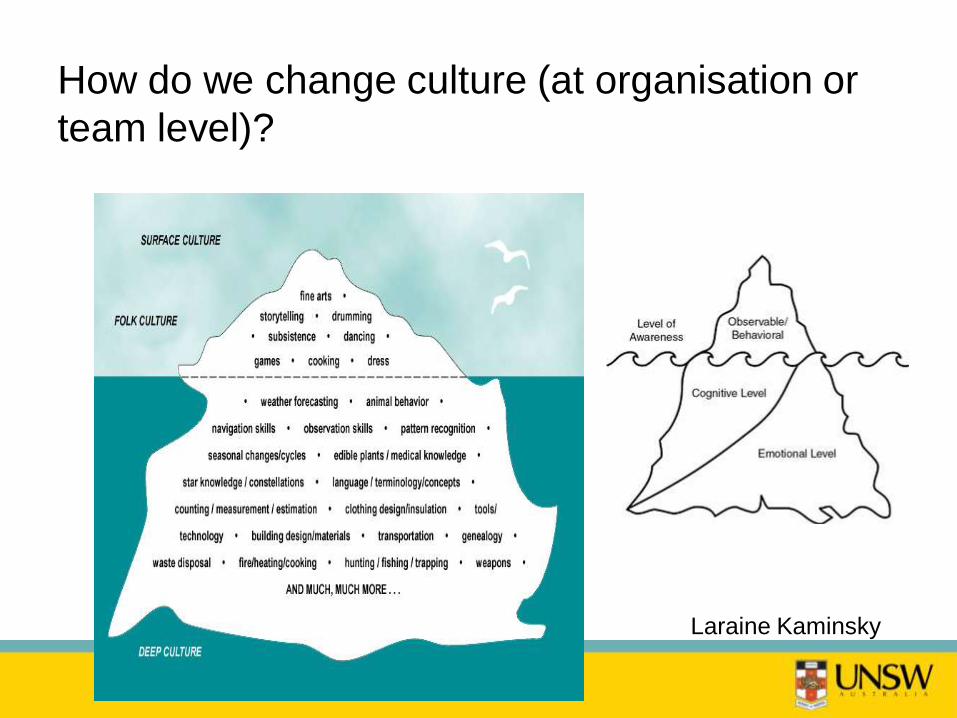
How do we change culture (at organisation or
team level)?
Laraine Kaminsky

Elements of culture
Raymond Williams

How does culture affect safety?
• Lack of integration of health care systems and services
• Resource shortfalls, competing priorities and inadequate
staffing and work overload
• Financial incentives to conceal errors
• Acceptance of poor, expectation of good quality services and
techniques
• e.g. written and oral communication
• Teams and services that are fragmented
• Professional and organisational culture clashes (including
definitions of errors)
• Lack of senior leadership involvement in safety strategies
Hindle, Braithwaite, Iedema (2005)
Hindle, Braithwaite, Travaglia (2006)

How does culture affect safety?
• Lack of clinician engagement
• Blame and shame, the ‘eating of young’
• The catching and or concealment or errors and near misses by
colleagues
• Treatment of whistleblowers and other system critics
• Involvement of consumers and carers
• Resistance to change
• Rate of change and innovation
• Level(s) of commitment to organisational learning and
improvement
• Integration of safety programs and the use of data
Hindle, Braithwaite, Iedema (2005)
Hindle, Braithwaite, Travaglia (2006)

What does safety culture look like?
Safety culture has been be defined as ‘… the product of
individual and group values, attitudes, perceptions,
competencies,and patterns of behavior that determine the
commitment to, and the style and proficiency of, an
organization's health and safety management.’
Organising for Safety: Third Report of the ACSNI (Advisory Committee on the Safety of Nuclear Installations) Study
Group on Human Factors. Health and Safety Commission (of Great Britain). Sudbury, England: HSE Books, 1993.
Sexton JB, L Helmreich RL, Neilands TB, Rowan K, Vella K,
Boyden J, Roberts PR, Thomas EJ. (2003) The Safety Attitudes
Questionnaire: psychometric properties,benchmarking data, and
emerging research. BMC Health Services Research, 6(44),
doi:10.1186/1472-6963-6-44

• No perceived benefit to those
implementing the change and their
patients
• High levels of insecurity (based on fear
or reality)
• May diminish their current
power/authority/status/wages (status
quo)
• Fear that the change might disrupt
their social and or professional
relationships
• Self-interest
• Feel a responsibility for the quality of
care
• Desire to uphold tradition
• Different goals and perspectives to
their managers
• Lack of trust of management
• High levels of existing or generated
uncertainty
• Unclear, misleading or conflicting
communication
• Lack of understanding of the change
and its purpose
• Mismatch between new innovation and
approach and skill set of staff
• Short implementation timeframes
• No consultation
• No leadership as opposed to
management
• Change burn-out
So why do people resist change?

Health staff are concerned about …
• Systems issues, including:
– Increases in ageing and disabled population(s) with
multiple co-morbidities
– Increase in chronic and complex illnesses
– These changes in population were seen as adding to
the complexities of care and potential for error
• Organisational issues, including:
– Inadequate resource management
– Heavy workloads
– Staff shortages
– Increased demands on staff for shiftwork
– Dependence on the use of causal staff

Health staff are concerned about …
• Teamwork issues, including:
– Poor communication
– Professional culture clashes
– Poor teamwork
– Pressure from inexperienced staff
• Individual issues, including:
– Emotional anxiety about witnessing or being involved in errors
– Personal and colleagues’ accountability for errors
– Increased patient aggression
– Burnout, tiredness
– Fear of litigation

Why is this important?
Staff under stress are likely to take up positions where they:
• Strong defence of current positions and tactics;
• Resort to familiar behaviour, irrespective of whether that
behaviour contributed to the error/disaster;
• Repeat of past solutions, irrespective of their applicability
to the current situation.
(Roberts, Madsen, & Desai, 2007, Weick 1990)
41

Again, why do people resist change?
They may not be ‘resisting’ change:
• Resisting ‘bad’ managerial decisions
• Not resisting at all, but confused as to how
to process and proceed

What can healthcare managers do? …
• Health workers are motivated to perform well when their organization
and managers:
• provide a clear sense of vision and mission;
• make people feel recognized and valued whatever their job;
• listen to staff and increase their participation in decisions;
• encourage teamwork, mentoring and coaching;
• encourage innovation and appropriate independence;
• create a culture of benchmarking and comparison;
• provide career structures, and transparent and fair opportunities for
promotion;
• give feedback on, and reward, good performance – even with token benefits
• use available sanctions for poor performance that are fair and consistent.
Source: WHO (2006). The World Health Report 2006 – Working Together for Health. Geneva, World Health
Organization

Improving our processes and our people
Challenge 3: How do we
improve communication and
teamwork?

Challenge 4: How do we improve
communication and teamwork?
The last half century has brought a sea change in the
provision of medical care, with massively increase complexity
… huge numbers of new medications and procedures, and
overwhelming evidence that the quality of teamwork often
determines whether patients receive appropriate care
promptly and safely … the outcomes of trauma care,
obstetrical care, care of the patient with an acute myocardial
infarction or stroke, and the care of the immunocompromised
patient are likely to hinge more on the quality of teamwork
than the brilliance of the supervising physician..
Watcher (2008) Understanding patient safety. p.100

Highly
ineffectiveAverage
performanceHighly effective
Hete
rogeneous
team
s
Hom
ogenous team
s
He
tero
ge
ne
ou
s te
am
s

Interprofessional factors affecting patient safety
• Communication and teamwork (Lyndon, 2006, Chacko et al, 2007), Manser, 2009)
• Peri-operative briefings (Lingard, et al 2008)
• Handovers (Nagpal et al 2010a; Nagpal, et al 2010b, Botti, 2009, Smith, 2008)
• Interdepartmental and inter-organisational relationships (Waring
et al, 2006, Fin et al 2006)
• Patient empowerment and involvement (Walton et al 2010; Howe: 2006)
• The importance of non-technical skills in surgery (Flin, et al 2008)
• Interprofessional conflict (Baldwin, Daugherty: 2008)
• Disaster management (Attack et al2009)

Interprofessional factors affecting patient safety
• Structures
• Processes and systems
• Roles and responsibilities
• Legal requirements
• Space and place
• Decision/sense making methods and models
• Group and interpersonal dynamics
• Patient/family involvement
Braithwaite, Travaglia (2005)
Hindle, Braithwaite, Iedema (2005)
Travaglia, Nugus, Braithwaite (2006)
Travaglia, Braithwaite (2010)
Nugus, Greenfield, Travaglia, Braithwaite (2010)

• The logic of assessment
• The focus of efforts
• The locus of responsibility
• The pace of action
• The focus of attention
• Interprofessional stereotypes
• Decision making expectations
• Beliefs about professional independence
Conceptual and practice differences (Qualls and Czirr,
1988)

Visualising professional
differences

Administrative staff’s view on safety and quality

Nurses’ views on safety and quality
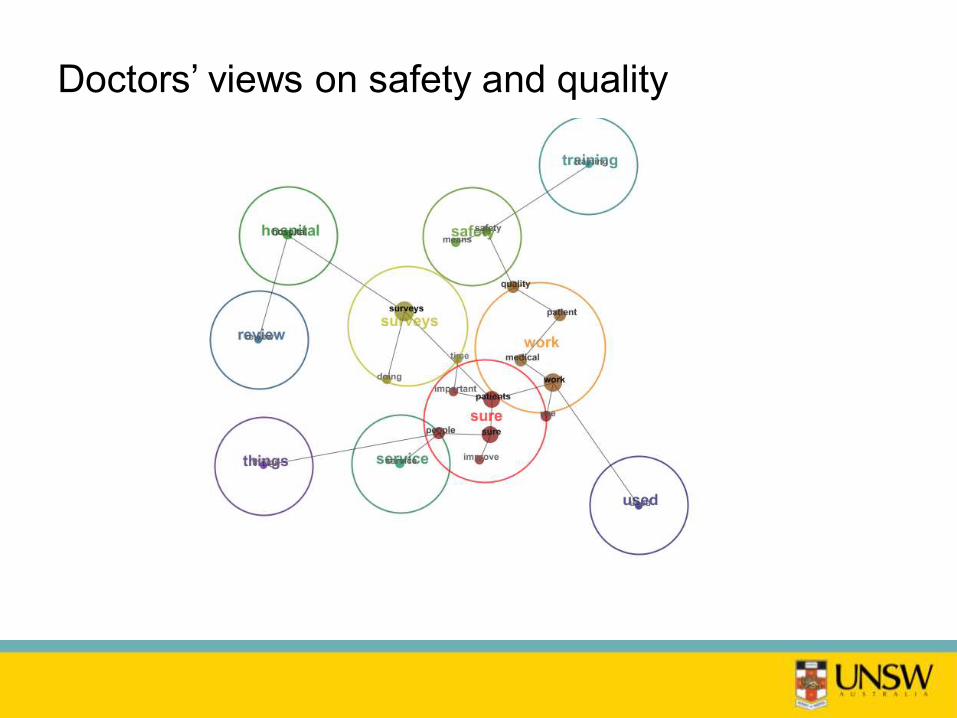
Doctors’ views on safety and quality

Allied Health’s views on safety and quality

Managers’ views on quality and safety

Providing a new vision for others to follow
Challenge 4: How do we look
at the healthcare system in a
new way?

Challenge 4: How do we look at the
healthcare system in a new way?
• Wellness versus illness systems
• Rocks versus birds
• Professional/patient/person/relationship centred
care?
• Who are our patients?

Paul Plsek, from Richard Dawkins; Douglas Eby
A rock or a bird?
Inanimate object or complex system
Is providing health care like
throwing …

SouthCentral Foundation Alaska

Patient centred approach to service delivery
It is more important to know what kind of a
patient has an [iatrogenic] disease than to
know what disease a patient has.
William Osler

Premise
• The patient safety movement has utilised systems theory and
risk perspectives to help identify and address the
organisational, team and clinical dynamics contributing to
errors and adverse events
• Interactions in healthcare are as influenced by the social-
cultural, and economic contexts of the patients as they are by
organisational, technical and workforce factors
• There is significant evidence on how social, situational an
structural vulnerability impacts on groups’ ability to access,
utilise and benefit from healthcare
• But less is known about how social, situational, structural and
system vulnerabilities affect the safety of healthcare

Sharing the load
Challenge 5: How can we act
as both managers and
leaders?

Challenge 5: How can we act as both managers
and leaders?Old management paradigm New management paradigm
Organisation discipline Organisation learning [lifelong]
Vicious circles Virtuous circles
Inflexible organisations Flexible organisations [Proactive]
Administrators Leaders
Distorted communication
(Information as power)
Open communication [information overload]
Hierarchies Markets [communities, networks]
Products driven by SBUs Products driven by core competencies
Apex strategic learning Widespread strategic learning
Theory x (most employees are not trustworthy) Theory y [+ + +]
(most employees are trustworthy)
Most employees are disempowered Empowerment [including patients]
Managerial prerogative must control local
knowledge of employees
Employee knowledge
(critical to success and creativity, creates on
prerogative)

Creating a healthcare system of leaders
• Beyond individual leaders - because of all the previous challenges,
healthcare systems need:
• Shared leadership versus individual leadership
• No heros – UK NHS – idea of servant and distributed leadership
• Importance of followership as well as leadership
• Increased focus on interactions and relationships
• Creation and support of networks and communities of practice
• Creation and support of learning organisations (Senge: systems
thinking, personal mastery, mental models, shared vision, team
learning)
• Focus on values (principles as the compass that point us in the
right direction) Covey

Peter Drucker
Managers do things right,
Leaders do the right thing.

Sharing the load
Challenge 6: How can we address
inequities?
Challenge 6: Dealing with inequities
How can we ensure that healthcare services are
safe, effective, patient-centred, timely, efficient and
equitable for all people
(Crossing the Quality Chasm)
• Equal access
• Equal utilization
• Equal quality of care
• Equal outcomes

Who is at risk in healthcare?
• The elderly
• Indigenous people
• People from CALD and refugees
• People with disabilities, especially cognitive impairments
• Children and youth
• Patients with literacy and communication problems
• People from lower SES
• Geographically isolated individuals
• Socially isolated individuals
• The homeless
• The frail and malnourished
• Patients with co-morbidities and chronic illness
• Patients with high acuity

Four factors every healthcare manager will deal
with ...
Complexity Diversity
Differentiation Context

Challenge 7: Can we make a
difference as managers?

Good news: good healthcare management
practice does make a difference
• Healthcare management practice (measured by operations,
performance and ‘talent’ management) was strongly related to
• Clinical outcomes (e.g. heart attack mortality rates)
• Patient satisfaction
• Hospital financial performance
• Healthcare management practices undertaken in the UK had resulted
in:
• Good UK average score vs other countries survey but
• Wide intra-country variations in practice (irrespective of
funding or physical size of country)
• No direct correlation between health expenditure and
management practices (and outcomes … the opposite in fact)

72

Good news: good healthcare management
practice does make a difference
• Five factors associated with better healthcare management practice
were:
• Share of clinically trained managers (more clinician managers,
better overall outcomes, particularly if those clinicians have
management training)
• Degree of competition (tougher competition better outcomes)
• Hospital size (larger hospitals have better outcomes)
• Managerial autonomy
• Hospital ownership (private have slightly higher scores)

Professor John Øvretveit
But they can also contribute to latent failures in
healthcare ...
Actions or inactions by managers/supervisors that cancontribute to the probability of errors:
• Heavy workloads of staff
• Poor communication between managers, clinicians and staff
• Lack of maintenance of buildings and equipment
• Lack of knowledge or experience of the manager
• Inadequate supervision of clinicians and staff
• Stressful environment
• Rapid organisational change
• Conflicting goals between managers and clinicians

So what is required of health services managers?
• Knowledge of the field; values; culture (Lawson & Rotem: 2004)
• Leadership; organisational planning; external relations; monitoring and
evaluation (Liang and Brown: 2008)
• Technical skills; industry knowledge; analytical and conceptual reasoning;
interpersonal and emotional intelligence (Robbins et al: 2001)
• Personal skills; interpersonal skills, group skills, communication skills (Carlopio
and Andrewartha: 2008)
• Leadership; communication; lifelong learning; consumer/community
responsiveness and public relations; political and health environment
awareness; conceptual skills; results oriented management; resources
management; compliance with standards, ethics and laws (CCHSE: 2005)
• Local knowledge; basic skills of working with people; basic skills of working
with data; library of theory; toolbox of technical knowledges and methods;
repertoire of different managerial personae; judgement or self knowledge,
ethical practice (Smyth et al, in Harris 2006)
• Wisdom (Rooney, Mintzberg, Reason, various)
Repertoire of Management Personae
• as teacher (high level knowledge and technical skills, role modeling, individual relationships with staff)
• as bureaucrat (guardian of roles, rules and relationships)
• as general (staff obedience, organisational flexibility and excellent intelligence about environment)
• as accountant (control of assets and expenditure)
• as engineer (production process as machine)
• as people person (relationships)
• as leader (create conditions for good decision-making and to project reassurance and confidence
(Legge & Stanton, 2002)

The final challenge

Final challenge: how can we see what we do
and who we are in a different light?
• Communication as the core of all healthcare
• The need for integration – co-ordination – collaboration
• The absolute necessity of multidisciplinary,
multiprofessional and multiperspective teams
• The balance of accountability and professional autonomy
• The role of the person in healthcare

Healthcare managers can contribute by ...
• Changing culture
• Engaging clinicians and staff
• Actively listening to and involving patients and
their families and communities
• Stop thinking rocks, start thinking birds
• Stop being the hero at the front, and start being
the leader at the heart

A little parable…

THANK YOU