Posttraumatic spinal cord herniation
5
Posttraumatic spinal cord herniation David Francis, Peter Batchelor, Peter Gates * Neuroscience Department, Barwon Health, P.O. Box 281, Geelong Victoria 3220, Australia Received 6 April 2005; accepted 26 July 2005 Abstract We report a 28-year-old woman who presented with a partial Brown-Sequard syndrome 18 months after a fall from a horse. Inves- tigation revealed the cause of her symptoms to be a spinal cord herniation at the level of T6. A review of previously reported cases of posttraumatic spinal cord herniation was undertaken. Six of the cases reported have clear evidence of injury at the site of subsequent herniation; the remaining five cases may be related to trauma or may be spontaneous spinal cord herniation, with an unrelated history of trauma. Ó 2006 Elsevier Ltd. All rights reserved. 1. Introduction Posttraumatic spinal cord herniation is a rare cause of spinal cord dysfunction. The following case describes a 28-year-old woman who developed a Brown-Sequard syn- drome secondary to thoracic cord herniation at the T6 le- vel; this followed trauma to her thoracic spine. Other causes of spinal cord herniation are more common; these include idiopathic and spontaneous cases. Ten previous re- ports of spinal cord herniation attributed to trauma are reviewed. 2. Case report A 28-year-old woman, JM, riding a horse that reared up, striking its head on hers. She was knocked unconscious and fell from the horse, the horse then fell on top of her. She remained unconscious for 24 h. She suffered general- ised soft tissue injuries associated with pain, in particular in the lower thoracic region. There was no plain X-ray evi- dence of bony injury; CT scan revealed a mild central disc protrusion at the level of L4-L5. Immediately after the accident she experienced stiffness and cramping pain in her left leg. She complained of in- creased stiffness and progressive weakness in the same leg over the next 18 months. There was no sphincter disturbance. The examination findings were consistent with a partial Brown-Sequard syndrome. The tone was increased in the left leg with sustained ankle clonus and there was weakness of eversion and dorsiflexion of the left foot. The reflexes were abnormally brisk in the left leg with an up-going left plantar response. Proprioception and vibration were unaf- fected. There was diminished pain and temperature sensa- tion affecting the right side of the body from the level of T8 down. Magnetic resonance imaging revealed a dural herniation at the level of T6, postcontrast and CSF flow studies showed distortion of the cord at the T6 level, with the cord being anteriorly displaced to the left and mildly flattened (Figs. 1 and 2). The appearance of endplate irregularity of the T5 and T6 vertebral bodies was consistent with trauma. * Corresponding author. Tel.: +61 3 5226 7950; fax: +61 3 5226 7375. E-mail address: [email protected] (P. Gates). Fig. 1. Sagittal T1 gadolinium-enhanced MRI of thoracic spine and spinal cord demonstrating spinal cord herniation at T6 (arrow) and minor end plate changes at T5 and T6. 582 Case reports / Journal of Clinical Neuroscience 13 (2006) 582–586
-
Upload
david-francis -
Category
Documents
-
view
213 -
download
2
Transcript of Posttraumatic spinal cord herniation

Posttraumatic spinal cord herniation
David Francis, Peter Batchelor, Peter Gates *
Neuroscience Department, Barwon Health, P.O. Box 281, Geelong Victoria 3220, Australia
Received 6 April 2005; accepted 26 July 2005
Abstract
We report a 28-year-old woman who presented with a partial Brown-Sequard syndrome 18 months after a fall from a horse. Inves-tigation revealed the cause of her symptoms to be a spinal cord herniation at the level of T6. A review of previously reported cases ofposttraumatic spinal cord herniation was undertaken. Six of the cases reported have clear evidence of injury at the site of subsequentherniation; the remaining five cases may be related to trauma or may be spontaneous spinal cord herniation, with an unrelated historyof trauma.� 2006 Elsevier Ltd. All rights reserved.
1. Introduction
Posttraumatic spinal cord herniation is a rare cause ofspinal cord dysfunction. The following case describes a28-year-old woman who developed a Brown-Sequard syn-drome secondary to thoracic cord herniation at the T6 le-vel; this followed trauma to her thoracic spine. Othercauses of spinal cord herniation are more common; theseinclude idiopathic and spontaneous cases. Ten previous re-ports of spinal cord herniation attributed to trauma arereviewed.
2. Case report
A 28-year-old woman, JM, riding a horse that rearedup, striking its head on hers. She was knocked unconsciousand fell from the horse, the horse then fell on top of her.She remained unconscious for 24 h. She suffered general-ised soft tissue injuries associated with pain, in particularin the lower thoracic region. There was no plain X-ray evi-dence of bony injury; CT scan revealed a mild central discprotrusion at the level of L4-L5.
Immediately after the accident she experienced stiffnessand cramping pain in her left leg. She complained of in-creased stiffness and progressive weakness in the same legover the next 18 months. There was no sphincterdisturbance.
The examination findings were consistent with a partialBrown-Sequard syndrome. The tone was increased in theleft leg with sustained ankle clonus and there was weaknessof eversion and dorsiflexion of the left foot. The reflexeswere abnormally brisk in the left leg with an up-going leftplantar response. Proprioception and vibration were unaf-
fected. There was diminished pain and temperature sensa-tion affecting the right side of the body from the level ofT8 down.
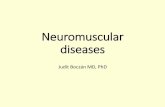
Magnetic resonance imaging revealed a dural herniationat the level of T6, postcontrast and CSF flow studiesshowed distortion of the cord at the T6 level, with the cordbeing anteriorly displaced to the left and mildly flattened(Figs. 1 and 2). The appearance of endplate irregularityof the T5 and T6 vertebral bodies was consistent withtrauma.
* Corresponding author. Tel.: +61 3 5226 7950; fax: +61 3 5226 7375.E-mail address: [email protected] (P. Gates).
Fig. 1. Sagittal T1 gadolinium-enhanced MRI of thoracic spine and spinalcord demonstrating spinal cord herniation at T6 (arrow) and minor endplate changes at T5 and T6.
582 Case reports / Journal of Clinical Neuroscience 13 (2006) 582–586

She underwent surgery 24 months after her initial injury.Laminectomy was performed, showing spinal cord hernia-tion through a ventral dural defect. There was a markedconstriction ring around the spinal cord at this point.The cord was reduced by incision of this ‘hernial ring’,and the duplicated dural fold was excised. The dura andwound were closed. There were no postoperative complica-tions and since surgery there has been marked improve-ment in the patient’s neurological function, and asignificant decrease in her pain. Follow-up MRI revealedthat the anterior deviation of the spinal cord at the T6 levelwas no longer apparent.
3. Discussion
A literature search revealed a total of 10 cases of spinalcord herniation attributed to trauma. There were manymore reports of spontaneous and idiopathic herniation1,2
and several reports of iatrogenic meningeal and cord herni-ation.3,4 The surgical findings are similar for all cord herni-ations, being a deficit in the ventral (or ventrolateral) duramater with attachment and tethering of the cord to thedura and/or posterior aspect of the adjacent vertebrae.
Table 1 summarises this case and the relevant previouslyreported cases.
This series of cases shows a great diversity in mechanismof injury and the interval between trauma and developmentof spinal herniation. In some reported cases there is insuf-ficient data about the suggested causative trauma to confi-dently attribute this to the subsequent development of thespinal cord herniation.
The key features of previously reported cases, which al-lows for confidence in attributing the trauma to the herni-ation, is a clear history of trauma to the spine andradiologic evidence of vertebral injury at the level wherethe subsequent herniation develops.
The cases reported by Marquardt et al. and Lees et al.illustrate a rapid progression of symptoms from the causa-
tive injury, less than 1 day and 16 days respectively.3,5 Bothdescribe trauma at the site of the subsequent herniationand had radiological evidence of vertebral injury.
Watters’ et al. third reported case, of a 46-year-old manfalling from a wall, is also indicative of posttraumatic her-niation.8 Identification of the cord herniation in this casetook 10 months, while in the current case identificationtook 18 months. In both cases the MRI at the time of diag-nosis showed evidence of bony injury at the site of the cordherniation. Both patients suffered several months of slowlyprogressive symptoms before investigation revealed spinalcord herniation. In Watters’ et al. case, evidence of bonyinjury was apparent at the time of the trauma, whereas inour case it was only identified following MRI 18 monthsafter the initial trauma.
The remaining two cases, where trauma to the spine canbe related to subsequent herniation, are these of Sachdevet al. and Baurs et al.10,11 Interestingly, with these twocases, the subjects had long symptom-free intervals, 9 and38 years respectively. Both patients had suffered crush frac-ture of vertebrae, where later cavitation occurred, intowhich the spinal cord herniated. This progression differsfrom the current case and may explain the long interval be-tween trauma and symptoms.
All six cases were treated surgically, halting the progres-sion of neurological symptoms in all cases. Some resolutionof symptoms was also evident in three of these cases at 6-month follow-up. The subject of this current case report,underwent surgery approximately 24 months after the ini-tial injury and follow-up revealed a significant neurologicalimprovement in 1 month.
Table 1 includes five other cases of spinal cord hernia-tion reported to be traumatic in origin. Of these cases, fourhave symptom-free intervals of greater than 17 years. Theinformation regarding the location of back injury in rela-tion to the subsequent herniation, and lack of radiologicevidence of bony injury at the site of diagnosed herniation,are insufficient to confidently regard these as true posttrau-matic spinal cord herniations. It is equally likely that thesecases of spinal cord herniation may be spontaneous or idi-opathic in origin. However, given the unclear pathophysi-ology of spontaneous spinal cord herniation, we areunable to rule out trauma as having some role in its even-tual development.
The pathophysiology of spinal cord herniation is clearerwhere there is evidence of trauma, or a history of surgery,at the site of subsequent herniation. It is likely that overtime, CSF pulsations, from respiration and heart beat,push the cord through the dural defect. Marquardt et al.hypothesise that at the time of injury a fracture in the ver-tebrae lacerated the dura and tethered the right side of thecauda into this fracture line; left-sided symptoms were ex-plained by the stretching of the left side of the cord dueto tethering.3 Lee et al. divided cord herniations into twogroups, those with large dural defects (from trauma or sur-gery) and those with smaller (1–2 cm) defects.5 The mech-anism hypothesised in the first group involved the spinal
Fig. 2. Gadolinium-enhanced axial MRI showing spinal cord herniation.
Case reports / Journal of Clinical Neuroscience 13 (2006) 582–586 583

Table 1Previously reported cases of traumatic spinal cord herniation
Author Age atdiagnosis
Sex Site of trauma Mechanism of injury Signs Site ofherniation
Interval untildiagnosis
Radiological Findings
Francis et al.(present study)
28 Female T6 Fall from horse, with horselanding on top of patient
Left lower leg weakness,hypertonicity and hyper-reflexia.Right leg loss of temperature andpin-prick sensation
T6 18 months Initial plain films showed no bonyinjury. CT revealed disc bulge atL4. MRI at time of diagnosisshowed vertebral endplateirregularity at T5 and T6, spinalcord herniation at T6
Marquardt et al.3 53 Male L1 Fall from fourth floor balcony,L1 fracture, left femur fracture,cerebral contusion of left frontallobe and facial and skullfractures
Right leg flaccid paralysis andareflexia. Left leg weakness andloss of sensation. Urinaryincontinence
L1 16 days Plain films – L1 fracture, nodislocation or instability.Myelography and CTmyelography – shift and tetheringof the cord into the L1 fractureline. Displacement of the conusmedullaris and cauda equina to theright
Lee et al.5 19 Male T11 Stab injury to back, lateral tomidline at the T11 level
Right leg flaccid paralysis. Leftleg loss of pin-prick andproprioception. Later, bilateralloss of sensation and urinary andfaecal incontinence
T11 <1 day Plain film – no bony fragment orforeign body. MRI - spinal cordhernitaed through dural defect atT11, posterior displacement, localleakage of CSF
Urbach et al.6 44 Male Not recorded Blunt trauma with no fracturebut temporary paraperisis at agesix
Dissociated sensory loss belowT6, no weakness. Urinaryincontinence and impotence
T6 38 years MRI – marked ventraldisplacement at T5-6, nosubarachnoid space ventral to thecord. Myelography and CTmyelogram excluded arachnoidcyst
Borges et al.7 68 Male Not recorded Shrapnel injury from grenadeexplosion. No neurologicaldeficit and after wounds healedno disability. No mention ofinjury to patients back
Left leg weakness andhypertonicity. Right leg loss oftemperature and pin-pricksensation
T3 >40 years 1989: CT myelogram normal.1992: MRI – ventral displacementof the spinal cord indicatingherniation at the T3 level
Watters et al.8 46 Male Lumbar spine Whiplash injury –torsohyperextension thentorsoflexion
Left leg weakness, hypertonicityand hyper-reflexia
T6 3 years CT myelogram and MRI –Scalloping of the dorsal vertebralbody of T6, with focal ventral corddisplacement at this level mostprominent on the left side, L4-5disc bulging
Watters et al.8 35 Male Thoracic spine Remote history of trauma to thethoracic spine, no further detailsgiven
Slowly progressive spasticparaparesis
T3 17 years MRI – extensive syrinx formationcavitation from C2 to T8 anddorsal cord herniation at T3
Watters et al.8 46 Male L1 Fall from 8 m wall, L1 burstfracture, pt underwent L1anterior vertebrectomy withstabilisation 6 weeks aftersustaining injury
Right leg weakness and areflexia.Neurogenic bowel and bladderdisturbances
L1 10 months MRI – herniation of the dura andcord dorsally and to the right ofthe lamina of L1. Myelography –dilated CSF space anterior todorsally displaced conusmedullaris at L1
584C
ase
repo
rts/
Jo
urn
al
of
Clin
ical
Neu
roscien
ce1
3(
20
06
)5
82
–5
86

cord adhering to scar tissue with CSF pulsation eventuallypushing the cord through the dural defect. They hypothes-ised that the second group herniate, secondary to CSF pul-sations, with cord ischaemia developing from stretchingand tethering. It is postulated that this second group donot develop adhesions between the cord and the duraand the onset of symptoms is within a few days from theonset of the injury.
The pathophysiology of spontaneous spinal cord hernia-tion is not well understood. Tekkok critically analyse severaltheories on how spontaneous spinal cord herniations arise,including repetitive minor trauma, pressure erosion due tointradural arachnoid cyst, and the possibility of congenitaldefects.1 They conclude however, that there are strong argu-ments against each of these theories. Miyake et al. postulatethat the initial event in spontaneous herniation of the spinalcord, is the herniation of the arachnoid membrane throughthe dura with subsequent adherence to the spinal cord.2 Ofthe reported spontaneous herniations, no dural or arach-noid abnormalities have been consistently reported.1
Magnetic resonance imaging and CT myelography havebeen the imaging modalities of choice to identify the leveland direction of cord herniation. MRI cine is useful to ex-clude pressure from an arachnoid cyst as the cause of corddisplacement.
4. Conclusion
Posttraumatic spinal cord herniation is a rare cause ofprogressive neurological deficit after significant injury tothe spine. In our opinion a clear history of trauma to thevertebrae at the site of herniation is required before attrib-uting causality to the injury. In all the cases reported todate, where there is a clear history of trauma at the levelof herniation, there has been radiological evidence of verte-bral injury to support this. MRI of the spine assists withidentification of both cord herniation and bony injury.Where MRI is not possible, CT and CT myelography isuseful. MRI cine is useful to exclude arachnoid cyst.
References
1. Tekkok IH. Spontaneous spinal cord herniation: case report andreview of the literature. Neurosurgery 2000;46:485–90.
2. Miyake S, Tamaki N, Nagashima T, Kurata H, Eguchi T, Kimura H.Idiopathic spinal cord herniation. J Neurosurg 1998;88:331–5.
3. Marquardt G, Weidauer S, Zannela FE, Seifert V. Acute posttrau-matic spinal cord herniation. J Neurosurg 2001;94:316–28.
4. Cobb C, Ehni G. Herniation of the spinal cord into an iatrogenicmeningocele. J Neurosurg 1973;39:533–6.
5. Lee ST, Lui TN, Jeng CM. Spinal cord herniation after stabbinginjury. Br J Neurosurg 1997;11:84–6.
6. Urbach H, Kaden B, Pechstein U, Solymosi L. Herniation of thespinal cord 38 years after childhood trauma. Neuroradiology
1996;38:157–8.7. Borges LF, Zervas NT, Lehrich JR. Idiopathic spinal cord herniation:
a treatable cause of the Brown-Sequard Syndrome – case report.Neurosurgery 1995;36:1028–32.W
ort
zman
etal
.963
Mal
eP
elvi
sF
ract
ure
dp
elvi
san
dse
vera
lm
ino
rb
ack
inju
ries
–n
ofu
rth
erd
etai
lsgi
ven
Lef
tle
gw
eak
nes
s,h
yper
ton
icit
yan
dh
yper
-refl
exia
.R
igh
tle
gar
eflex
ia.B
ilat
eral
hyp
alge
sia
and
ther
man
alge
sia
T7
36ye
ars
Mye
logr
aph
y–
alm
ost
com
ple
teo
bst
ruct
ion
of
con
tras
to
pp
osi
teth
eb
od
yo
fT
7.C
T–
cort
icat
edb
on
yd
efec
tsu
gges
tin
ga
ben
ign
lesi
on
ind
ors
alas
pec
to
fT
7S
ach
dev
etal
.10
44F
emal
eL
1M
oto
rca
rac
cid
ent,
thro
wn
fro
mca
ran
dla
nd
edo
nri
ght
glu
teal
regi
on
.L
1ve
rtra
lco
mp
ress
ion
.O
ne
year
afte
rin
jury
pat
ien
tu
nd
erw
ent
L1
lam
inec
tom
y
Rig
ht
leg
wea
kn
ess
and
all
sen
sory
mo
dal
itie
sd
imin
ish
edo
nth
issi
de
L1
9ye
ars
Pla
infi
lm–
scal
lop
ing
and
cavi
tati
on
of
L1.
CT
–sc
lero
tic
L1
mar
gin
san
der
osi
veca
vity
con
tin
uo
us
wit
hsp
inal
can
alin
the
po
ster
ior
asp
ect
of
L1.
Mye
logr
am–
con
us
med
ull
aris
dev
iate
dto
war
ds
the
nec
ko
fth
eca
vity
,n
erve
roo
tsen
teri
ng
and
emer
gin
gfr
om
the
cavi
tyar
ese
enB
aur
etal
.11
59M
ale
L4
Mo
torc
ycle
acci
den
t–
com
pre
ssio
nfr
actu
reo
fL
4tr
eate
dco
nse
rvat
ivel
yin
itia
lly,
app
rox
9ye
ars
late
rn
ucl
eoto
my
per
form
edfo
rd
isc
her
nia
tio
nat
L4/
5
Lef
tle
gw
eak
nes
s,ar
eflex
iaan
dse
nso
ryd
efici
tsL
438
year
sM
RI
–L
eft
roo
tso
fca
ud
ad
isto
rted
into
L4
cavi
tyw
hic
hw
asco
mm
un
icat
ing
wit
hsu
bar
ach
no
idsp
ace.
Mye
logr
am–
con
tras
tm
ater
ial
inb
on
yca
vity
inp
ost
erio
rp
ort
ion
of
L4.
Po
stm
yelo
gram
CT
–se
vera
ln
erve
roo
tsad
her
ent
toed
geo
fb
on
yle
sio
n
Case reports / Journal of Clinical Neuroscience 13 (2006) 582–586 585

8. Watters MR, Stears JC, Osborn AG, et al. Transdural spinal cordherniation: imaging and clinical spectra. AJNR Am J Neuroradiol
1998;19:1337–44.9. Wortzman G, Tasker RR, Rewcastle B, Richardson JC, Pearson FG.
Spontaneous incarcerated herniation of the spinal cord into a vertebralbody: a unique cause of paraplegia. J Neurosurg 1974;41:631–5.
10. Sachdev VP, Huang YP, Shah CP, Mallis LI. Posttraumatic pseud-omeningiocoele (enlarging fracture?) in a vertebral body. J Neurosurg
1981;54:545–59.11. Baur A, Stabler A, Psenner K, Hamburger C, Resiser M. Imaging
findings in patients with ventral dural defects and herniation of neuraltissue. Eur Radiol 1997;7:1259–63.
doi:10.1016/j.jocn.2005.07.013
Post-cranial irradiation syndrome with migraine-like headaches,prolonged and reversible neurological deficits and seizures
Dennis J. Cordato a,*, Peter Brimage b, Lynette T. Masters c, Patrick Butler d
a Department of Neurology, Bankstown-Lidcombe Hospital, Eldridge Road, Bankstown 2200, New South Wales, Australiab Miranda Neurology, Miranda, New South Wales, Australia
c Mayne Health Radiology, Kogarah, New South Wales, Australiad Department of Nuclear Medicine, St George Hospital, Kogarah, New South Wales, Australia
Received 27 October 2004; accepted 4 April 2005
Abstract
Two adult patients with a background history of astrocytomas treated with resection and cranial irradiation, 18 and 16 years previ-ously, presented with acute onset of headache associated with prolonged neurological deficits, including dysphasia and right hemiparesis.The first patient also developed seizures while in hospital. In both patients, magnetic resonance imaging brain scans failed to show evi-dence of acute ischaemia or tumour recurrence and symptoms reversed completely after 1 month and 7 days, respectively. A single pho-ton emission computed tomography scan, performed on the first patient at day 8 post-admission, showed hyperperfusion in the leftparieto-occipital region (in the same region as his previous tumour). The clinical histories and outcomes are consistent with the diagnosisof post-cranial irradiation syndrome with migraine-like headaches and prolonged and reversible neurological deficits. Recognition of thisdisorder is useful in providing reassurance of a favourable prognosis and may also help avoid invasive investigations.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Post-cranial irradiation; Migraine; Neurological deficits; Seizures
1. Introduction
Patients with migraine have an increased prevalence ofseizures and, conversely, patients with epilepsy have an in-creased prevalence of migraines.1,2 Headaches associatedwith epileptic seizures are also very common, occurringin up to 50% of epilepsy patients.3–5 Prolonged andreversible neurological deficits, lasting days to weeks andassociated with migraine-type headaches and seizures,have been rarely reported in children and adult patientswith a past history of cranial irradiation.6–8 Electroen-cephalography (EEG) in such patients fails to show epi-
leptiform activity and may even be normal. Magneticresonance imaging (MRI) shows abnormalities consistentwith patients’ previous radiation therapy without evidenceof tumour recurrence. Perfusion- or diffusion-weightedMRI abnormalities have not been reported, although, intwo patients, reversible cortical gadolinium enhancementof the posterior cerebral gyri was found.8 To the best ofour knowledge, there have been seven cases (five children,two adults)6–8 described previously in the literature. Apostulated mechanism is cerebral ischaemia secondary tovasospasm. A cerebral perfusion single photon emissiontomography (SPECT) scan may be helpful in distinguish-ing ischaemia from seizure activity, but we are not awareof any previous reports of cerebral perfusion SPECTscans in this clinical setting. Herein, we report on twoadult patients with a past history of cranial irradiationwho developed prolonged and reversible neurological def-
* Corresponding author. Present address: Suite 7E, Level 5, St GeorgePrivate Hospital, 1 South Street, Kogarah, New South Wales, 2217,Australia. Tel.: +61 2 9553 7444; fax: +61 2 9553 7455.
E-mail address: [email protected] (D.J. Cordato).
586 Case reports / Journal of Clinical Neuroscience 13 (2006) 586–590


















