Postmortem CT (PMCT)
45
Postmortem CT in Trauma Rathachai Kaewlai, MD
-
Upload
rathachai-kaewlai -
Category
Health & Medicine
-
view
989 -
download
0
Transcript of Postmortem CT (PMCT)
Postmortem CT in Trauma Rathachai Kaewlai, MD
BG Gil Brogdon, MD
It is believed that forensic scientists in other disciplines would find radiologists in their area interested in cooperative efforts
Sharing of interdisciplinary skills and knowledge would
• Improve the economy and effectiveness of investigative efforts
• Prevent some false starts and/or reinventions of well-worn wheels, and most important,
• Expand scientific horizons
Gil Brogdon, MD Father of Forensic Radiology
1929-2014
Outline
Postmortem imaging techniques
Role of PMCT in trauma Normal PMCT findings Traumatic pathologies on PMCT
Current status at Ramathibodi Q & A
Death Investigation
Situation peaceful No injuries
Medical history and ID cleared
Liberation for funeral
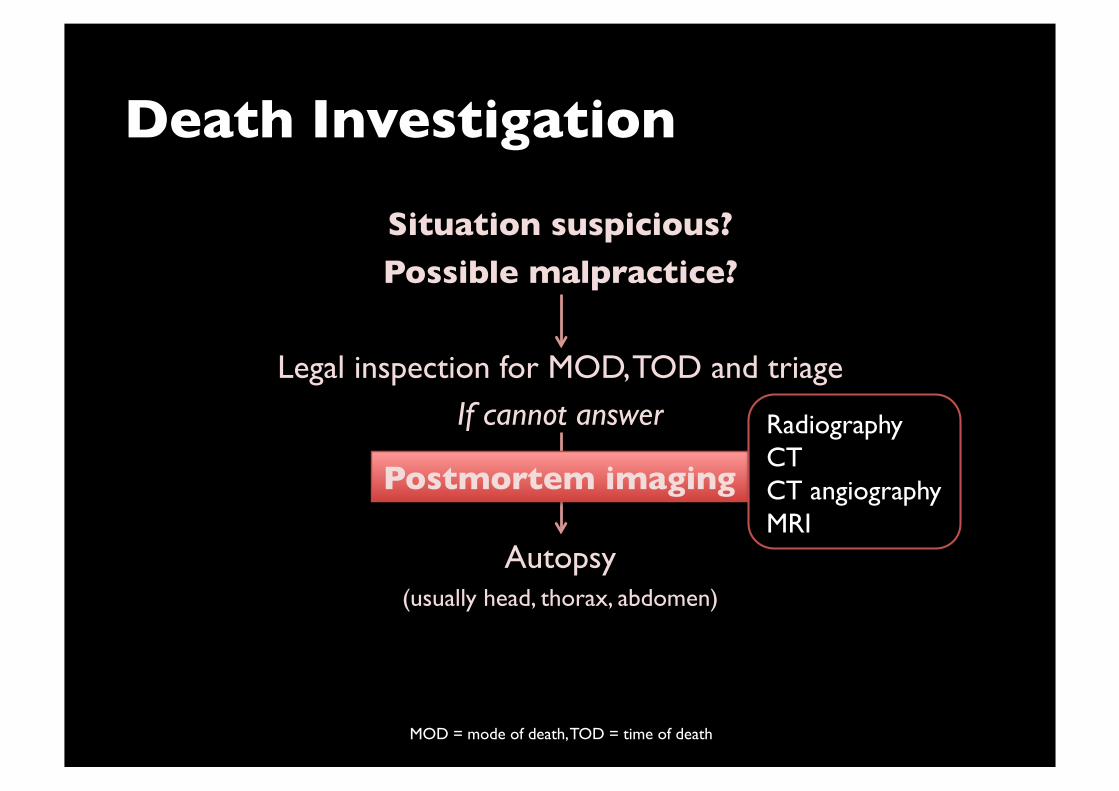
Death Investigation
Situation suspicious? Possible malpractice?
Legal inspection for MOD, TOD and triage If cannot answer
Autopsy
(usually head, thorax, abdomen)
Postmortem imaging Radiography CT CT angiography MRI
MOD = mode of death, TOD = time of death

“Virtopsy”
Virtual autopsy
Began in Germany, now settled in Switzerland What it covers: PMCT, PMCTA, PMMR
Biopsy Surface scanning Virtual reconstruction of trauma events
Virtopsy.com
PM Imaging: Filling the Void of Traditional Autopsy Traditional autopsy = reference standard
But Invasive Certain body parts difficult to dissect
Require permission from relatives of trauma victims Religious issue
Focusing on Trauma and PMCT
Very common Every 5s, a person in the world dies from trauma
Major cause of death worldwide 2nd in Thailand 1st in age group of 1-45 years in developing countries
Proven usefulness of PMCT New technology allows fast imaging in seconds 3D reconstruction for visualization
PMCT to Answer ���Key Forensic Questions Identity
Time of death Injuries: Self inflicted or 3rd party, priority, vitality, survival time
Type, severity, instrument, direction Concomitant injuries Reconstruction of events
PMCT: Advantages
To physicians Analysis of organs in situ Info added to autopsy
Less time consuming in certain body parts than autopsy (neck, spine, pelvis)
Stored images for years Trauma care evaluation Education Research
To victims’ relatives Less invasive Less rejection No religious issue
PMCT: Techniques
Coverage
Head/neck Body to knees or lower
No IV contrast
Arms on side High dose for image quality 2D reformations
3D imaging
PMCT: Supporting Evidence
Systematic review in Forensic Science International
Jalalzadeh H, et al. (2015) from The Netherlands 26 studies, 563 trauma victims
“PMCT demonstrated moderate to high-grade injuries and COD accurately”
“PMCT more sensitive than conventional autopsy in detecting skeletal injuries”
Normal PM Changes Seen on CT
Livor mortis
Rigor mortis Algor mortis Decomposition
Putrefaction
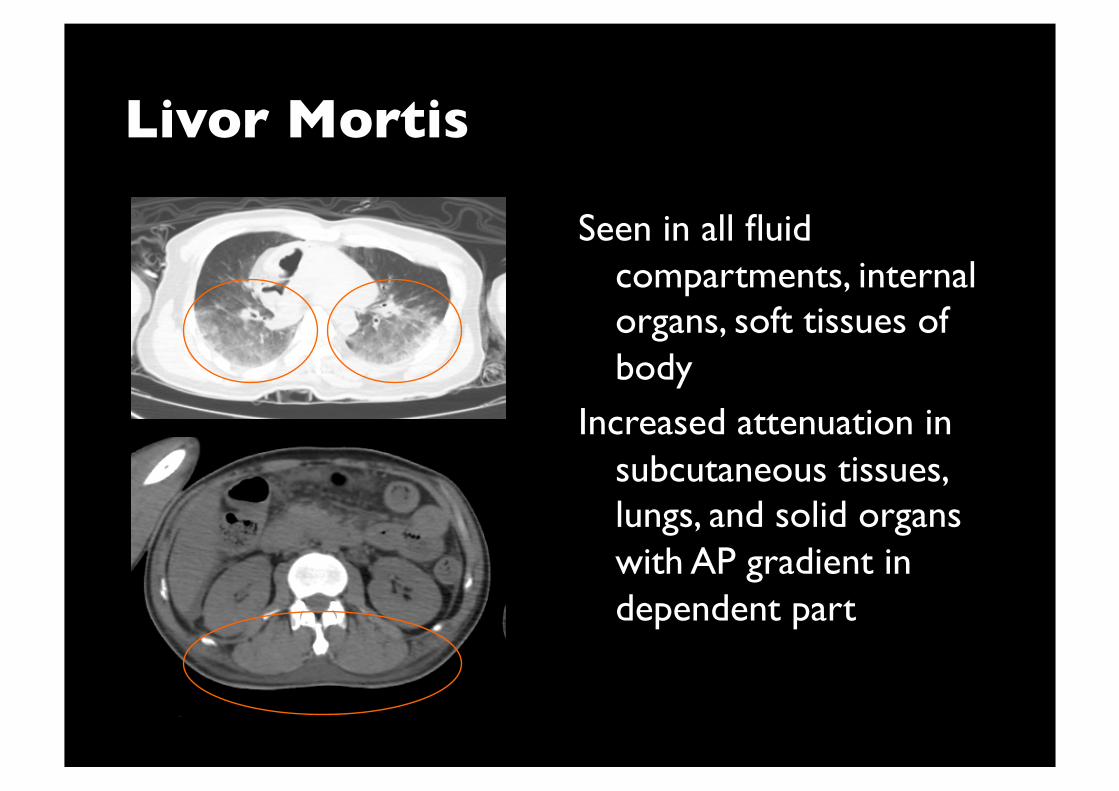
Livor Mortis
Seen in all fluid compartments, internal organs, soft tissues of body
Increased attenuation in subcutaneous tissues, lungs, and solid organs with AP gradient in dependent part
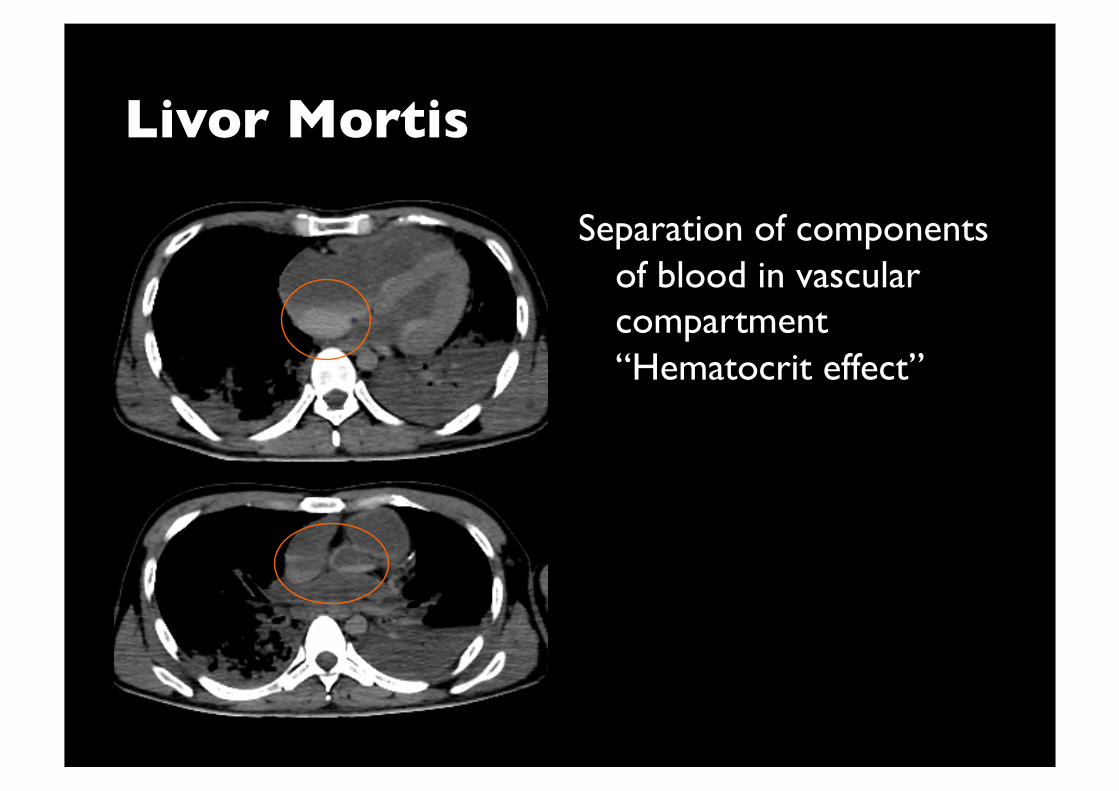
Livor Mortis
Separation of components of blood in vascular compartment “Hematocrit effect”
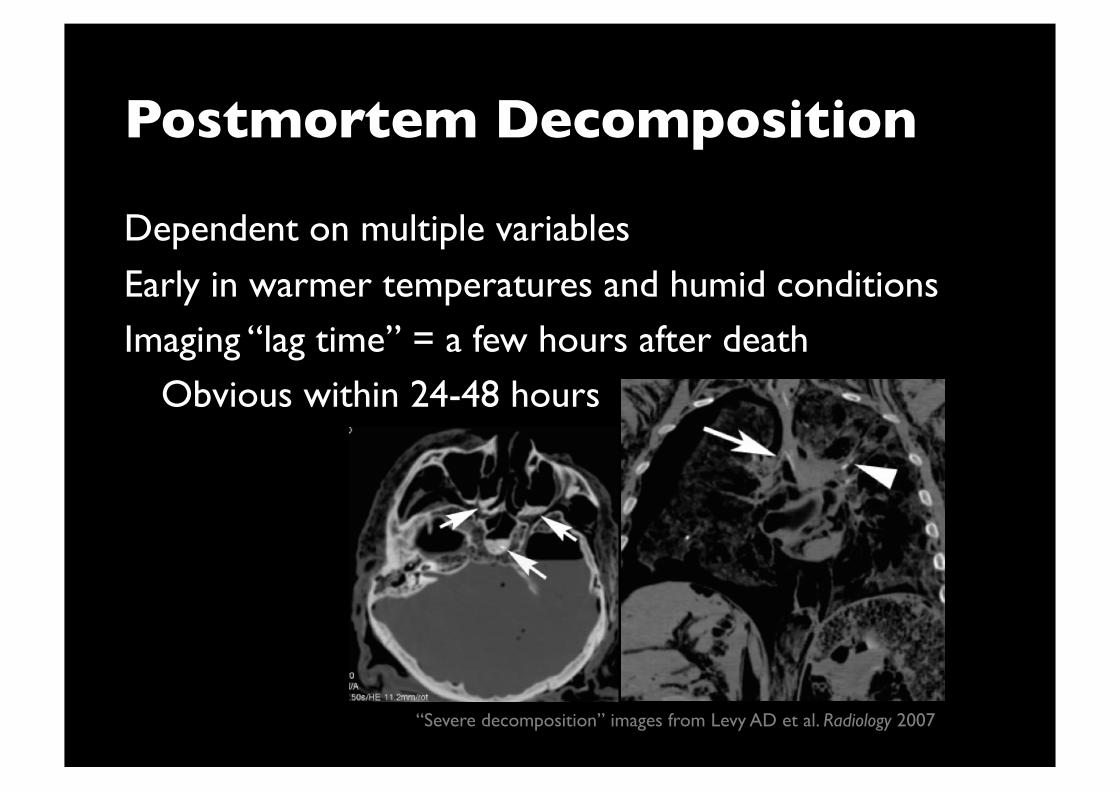
Postmortem Decomposition
Dependent on multiple variables
Early in warmer temperatures and humid conditions Imaging “lag time” = a few hours after death Obvious within 24-48 hours
“Severe decomposition” images from Levy AD et al. Radiology 2007
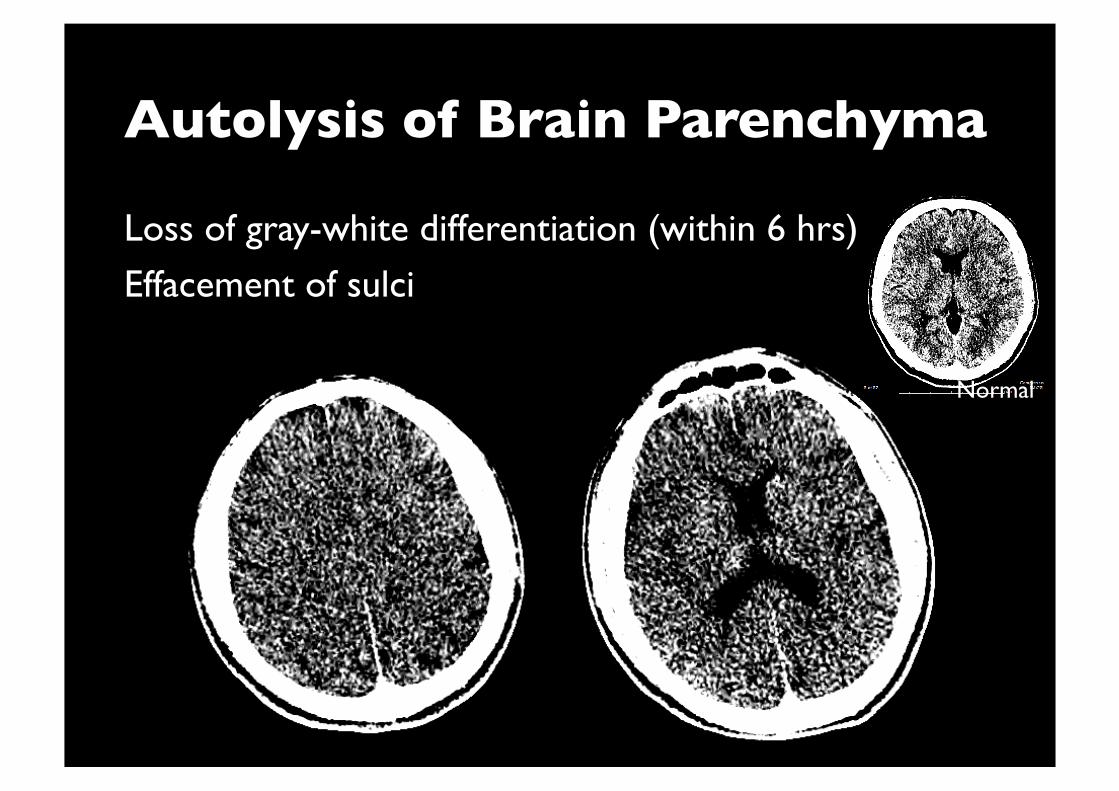
Autolysis of Brain Parenchyma
Loss of gray-white differentiation (within 6 hrs)
Effacement of sulci
Normal
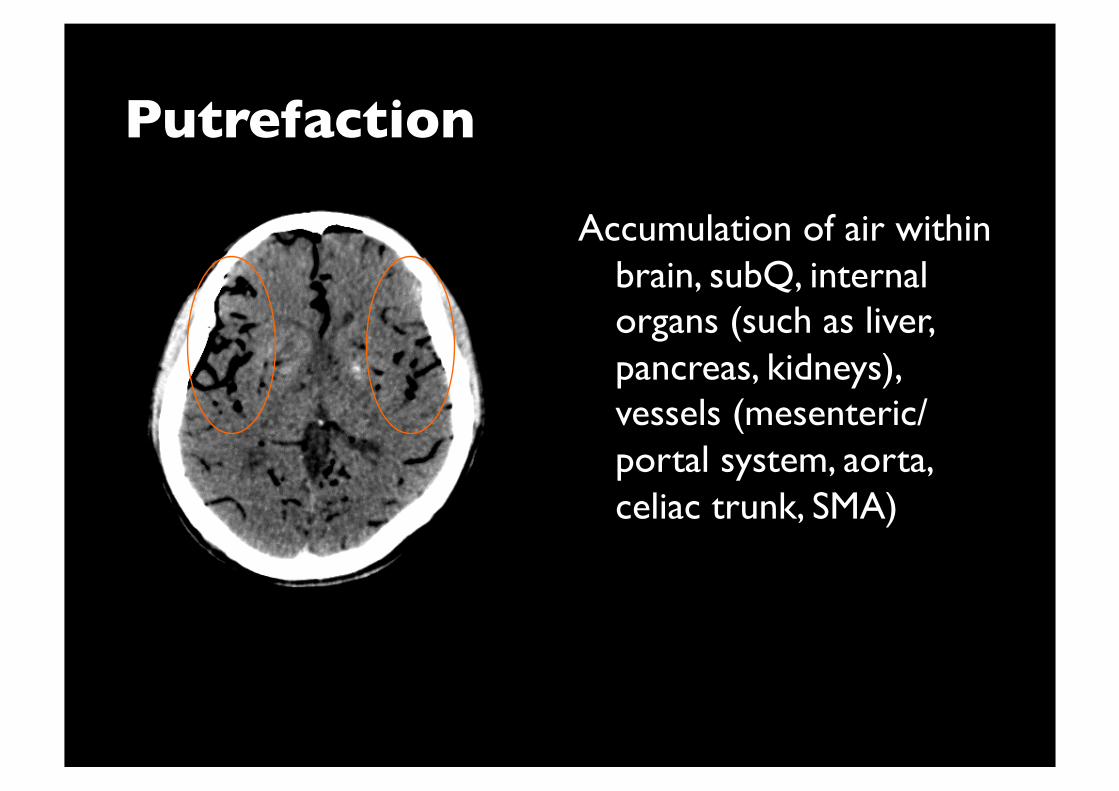
Putrefaction
Accumulation of air within brain, subQ, internal organs (such as liver, pancreas, kidneys), vessels (mesenteric/portal system, aorta, celiac trunk, SMA)
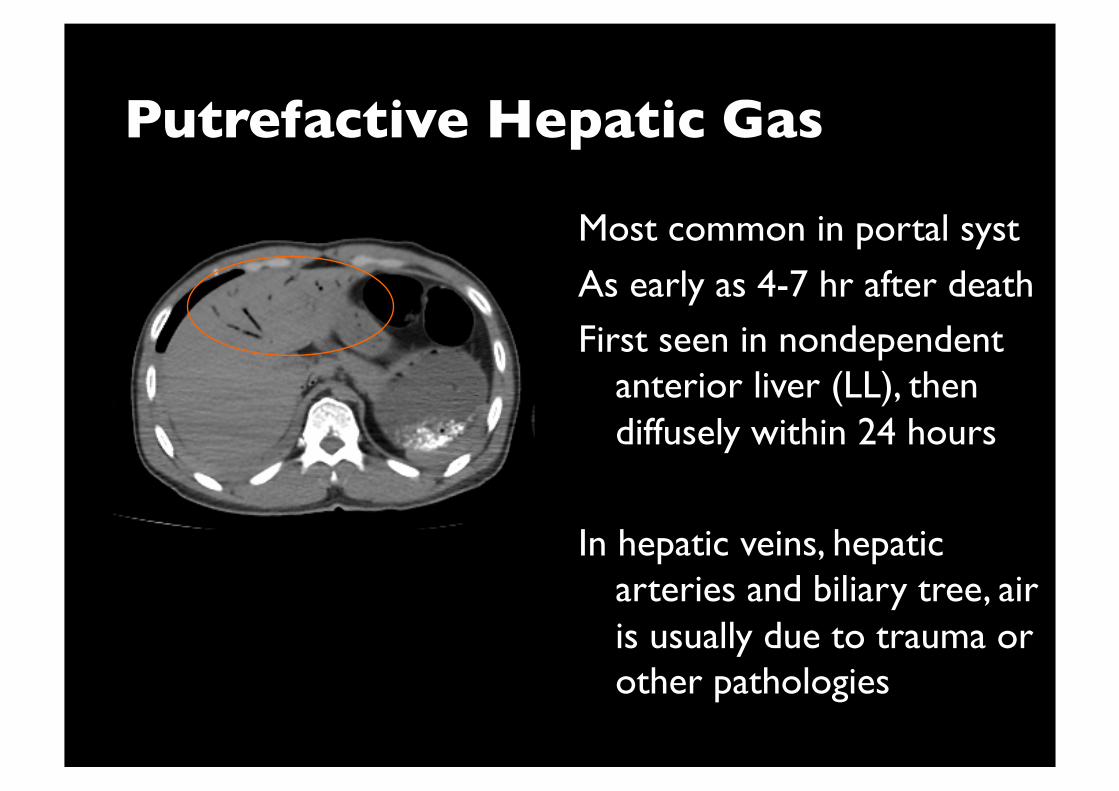
Putrefactive Hepatic Gas
Most common in portal syst
As early as 4-7 hr after death First seen in nondependent
anterior liver (LL), then diffusely within 24 hours
In hepatic veins, hepatic arteries and biliary tree, air is usually due to trauma or other pathologies
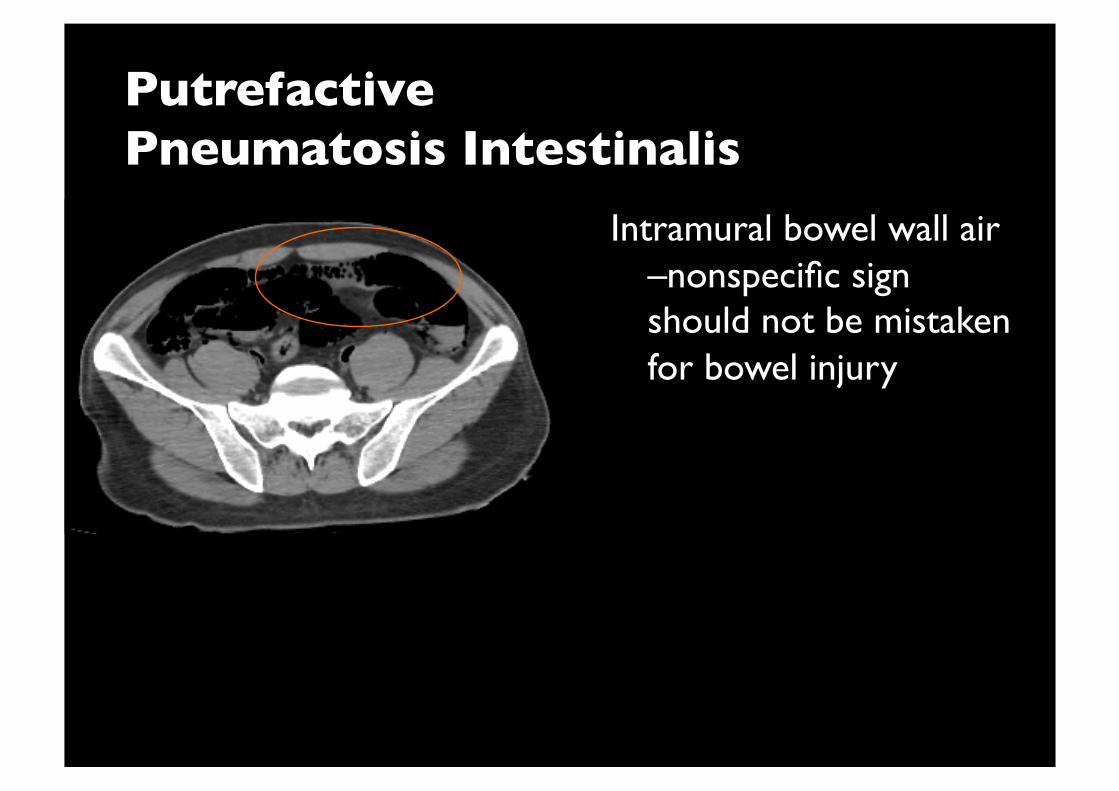
Putrefactive ���Pneumatosis Intestinalis
Intramural bowel wall air –nonspecific sign should not be mistaken for bowel injury
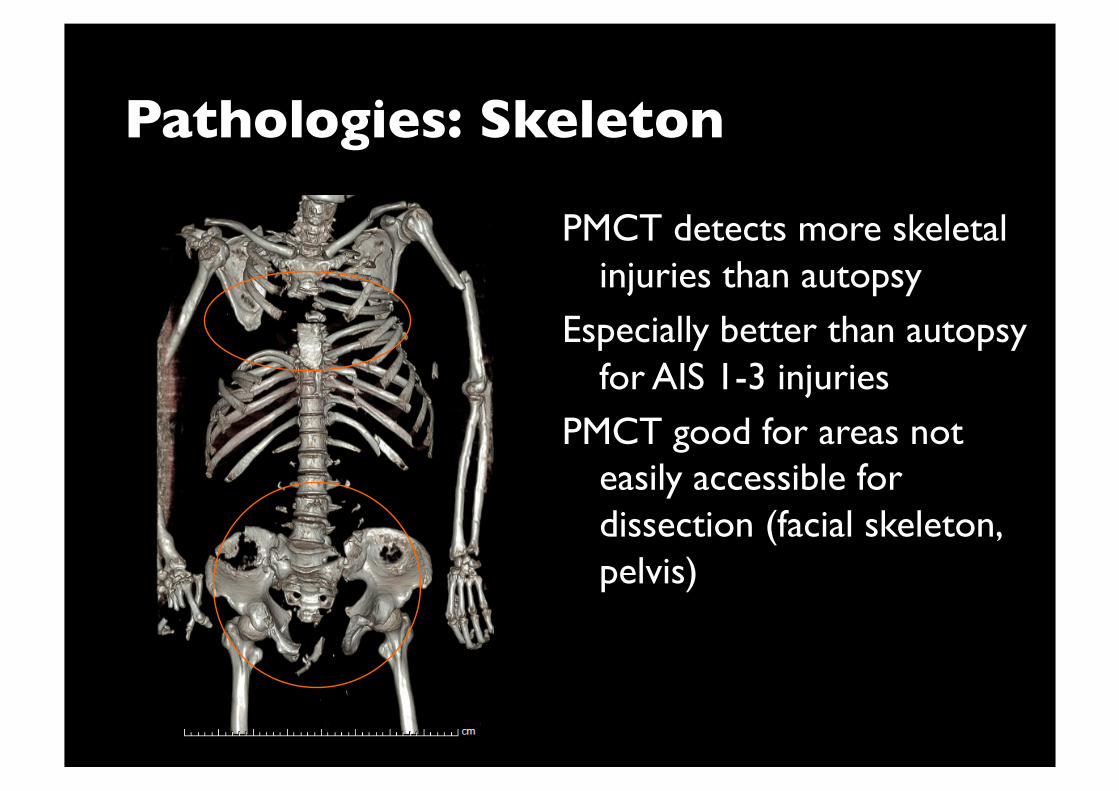
Pathologies: Skeleton
PMCT detects more skeletal injuries than autopsy
Especially better than autopsy for AIS 1-3 injuries
PMCT good for areas not easily accessible for dissection (facial skeleton, pelvis)
Soft Tissues
Hematomas often overlook with PMCT
Autopsy superior to PMCT For soft tissue and vascular injuries Even with AIS 3+ injuries
Exception is abnormal gas collections PMCT far better than autopsy even with under water technique
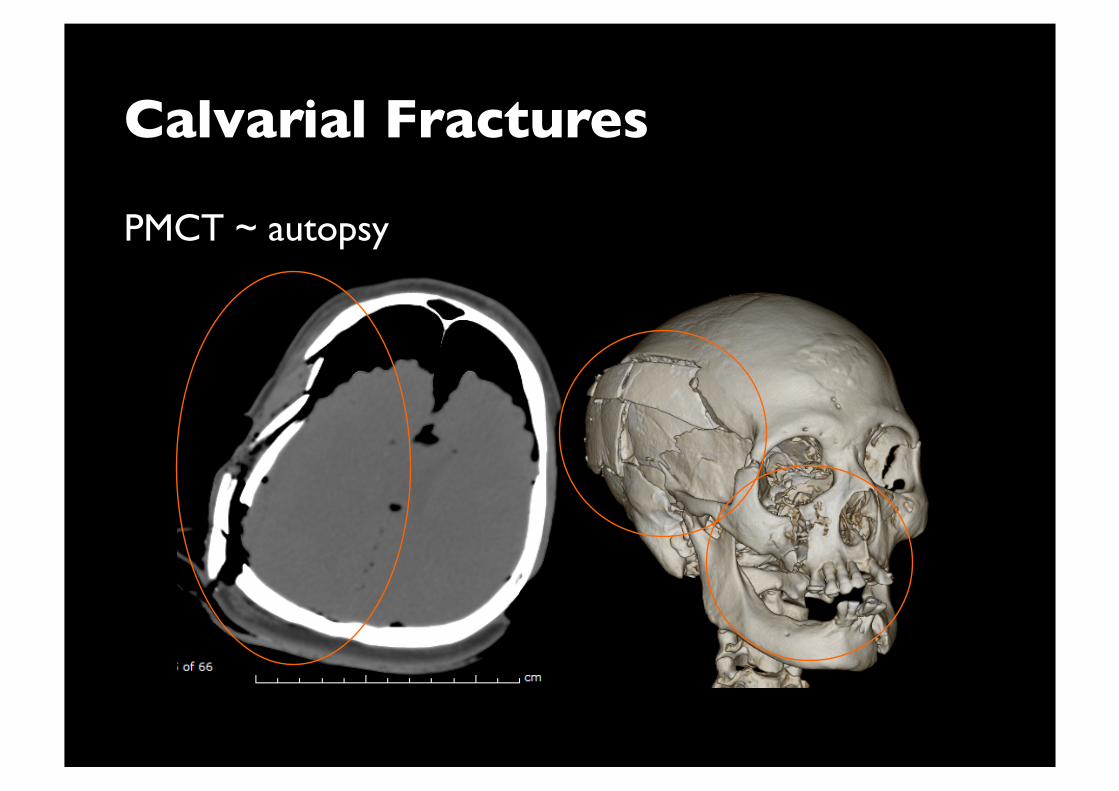
Calvarial Fractures
PMCT ~ autopsy
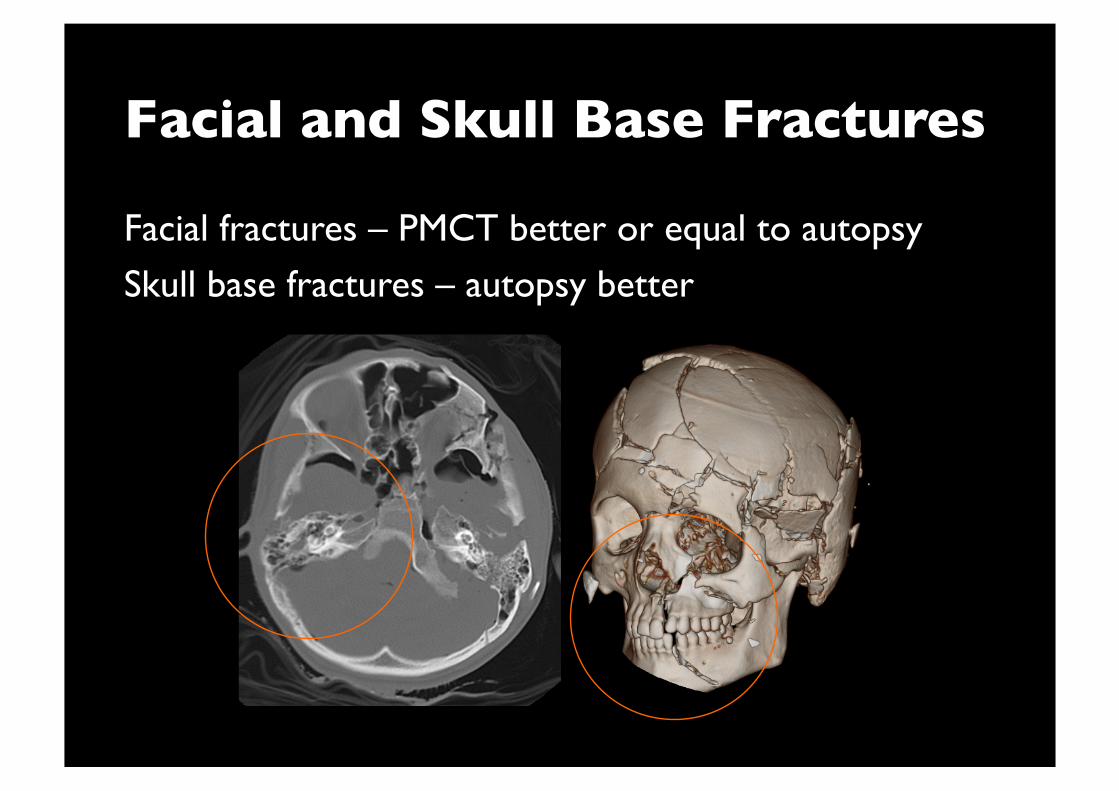
Facial and Skull Base Fractures
Facial fractures – PMCT better or equal to autopsy
Skull base fractures – autopsy better
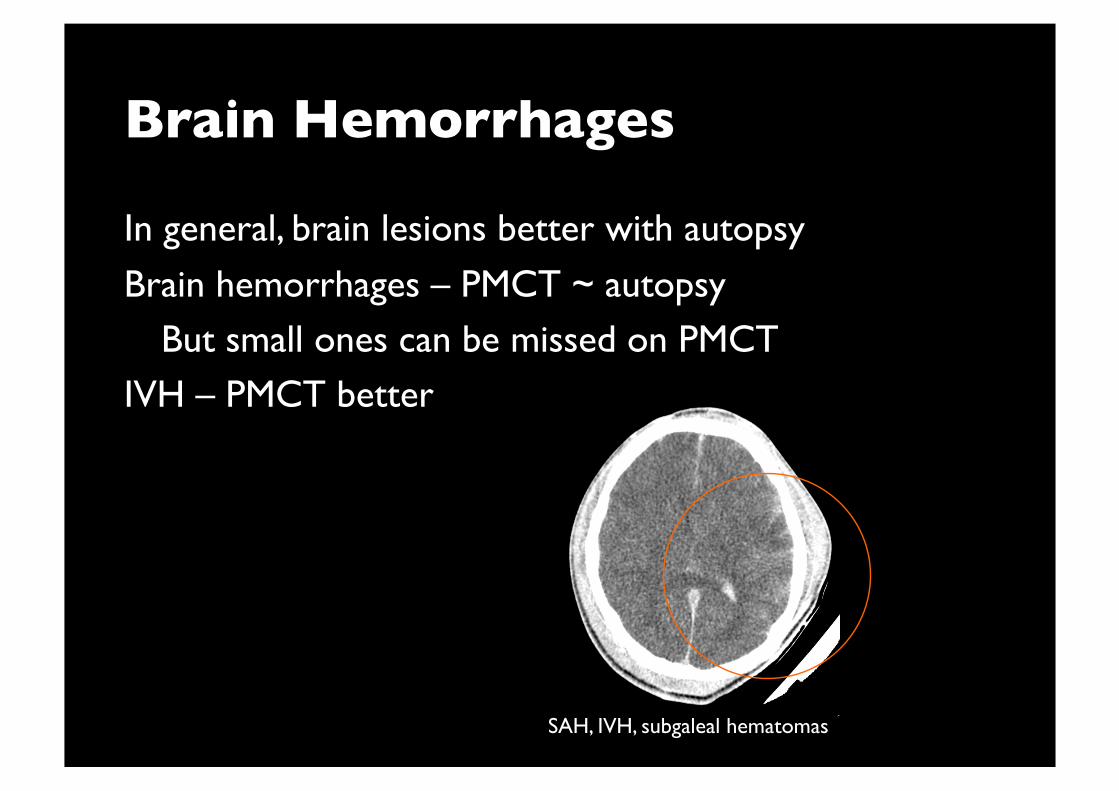
Brain Hemorrhages
In general, brain lesions better with autopsy
Brain hemorrhages – PMCT ~ autopsy But small ones can be missed on PMCT
IVH – PMCT better
SAH, IVH, subgaleal hematomas
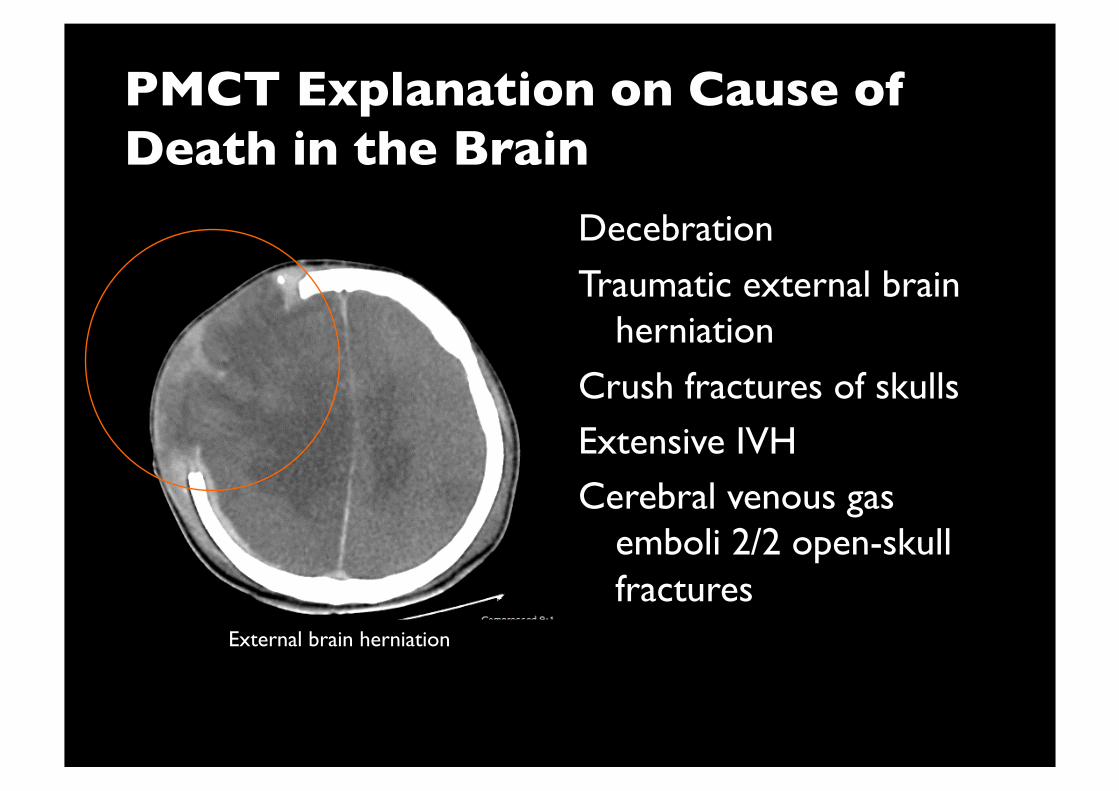
PMCT Explanation on Cause of Death in the Brain
Decebration
Traumatic external brain herniation
Crush fractures of skulls Extensive IVH Cerebral venous gas
emboli 2/2 open-skull fractures
External brain herniation
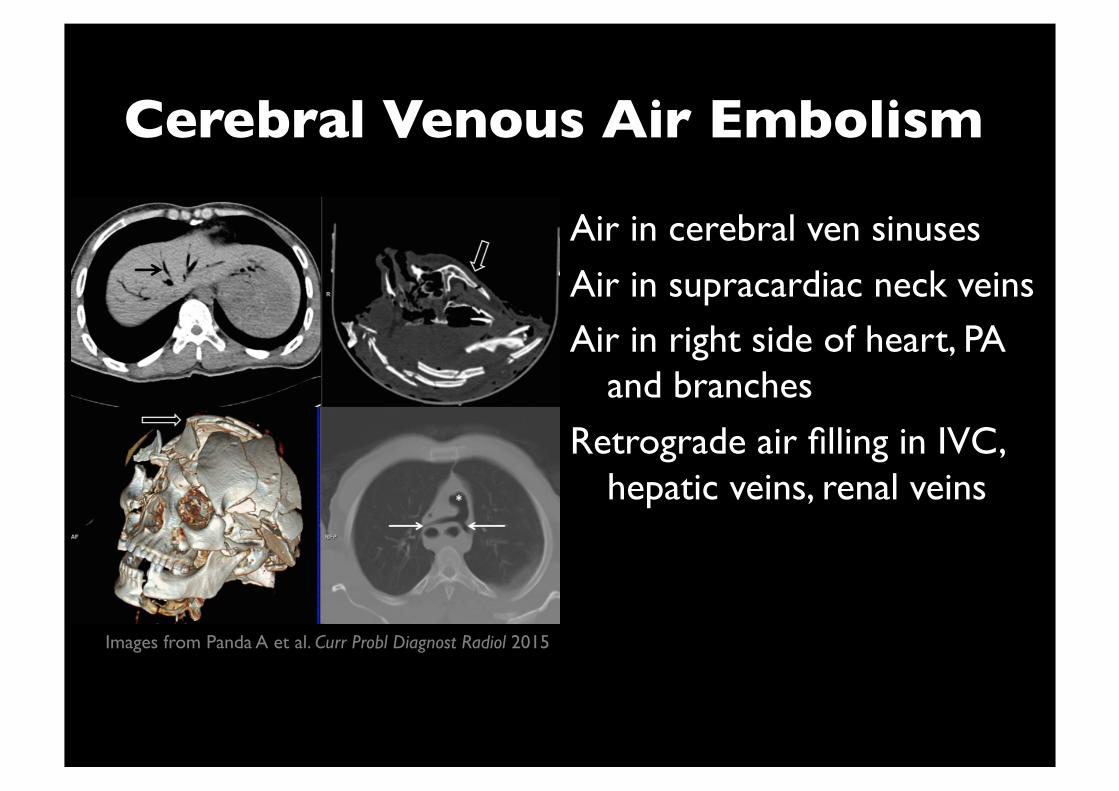
Cerebral Venous Air Embolism
Air in cerebral ven sinuses
Air in supracardiac neck veins Air in right side of heart, PA
and branches
Retrograde air filling in IVC, hepatic veins, renal veins
Images from Panda A et al. Curr Probl Diagnost Radiol 2015
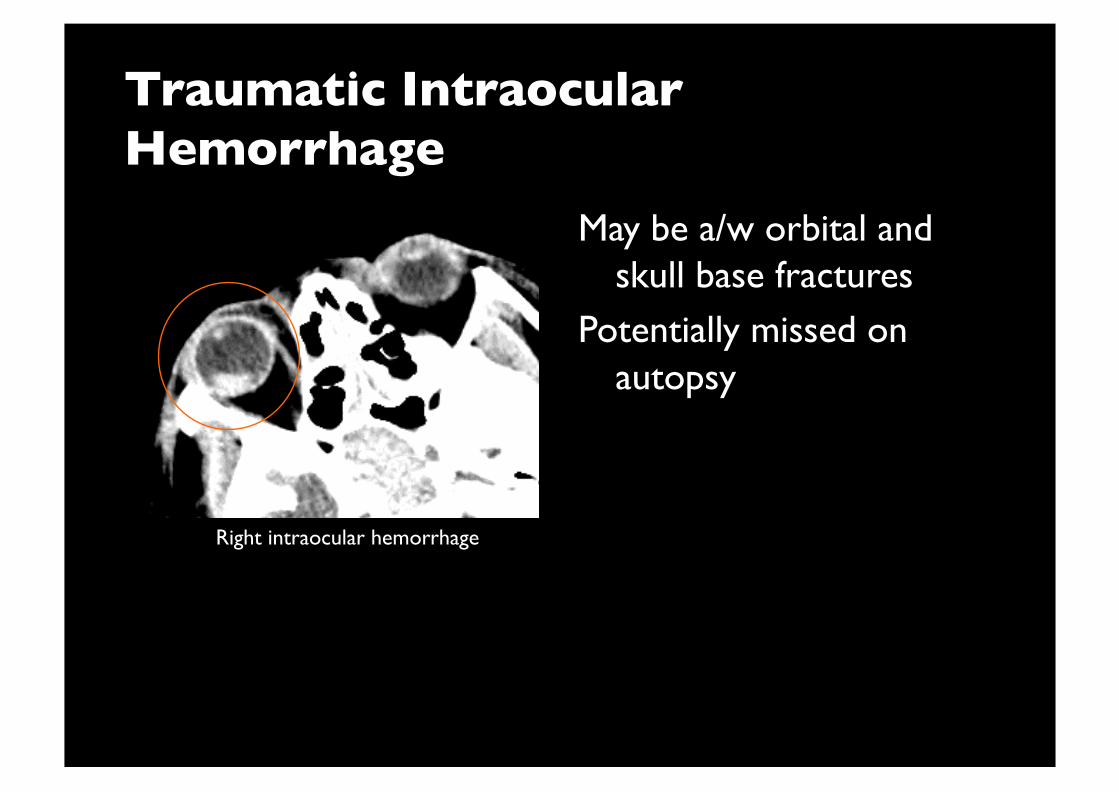
Traumatic Intraocular Hemorrhage
May be a/w orbital and skull base fractures
Potentially missed on autopsy
Right intraocular hemorrhage
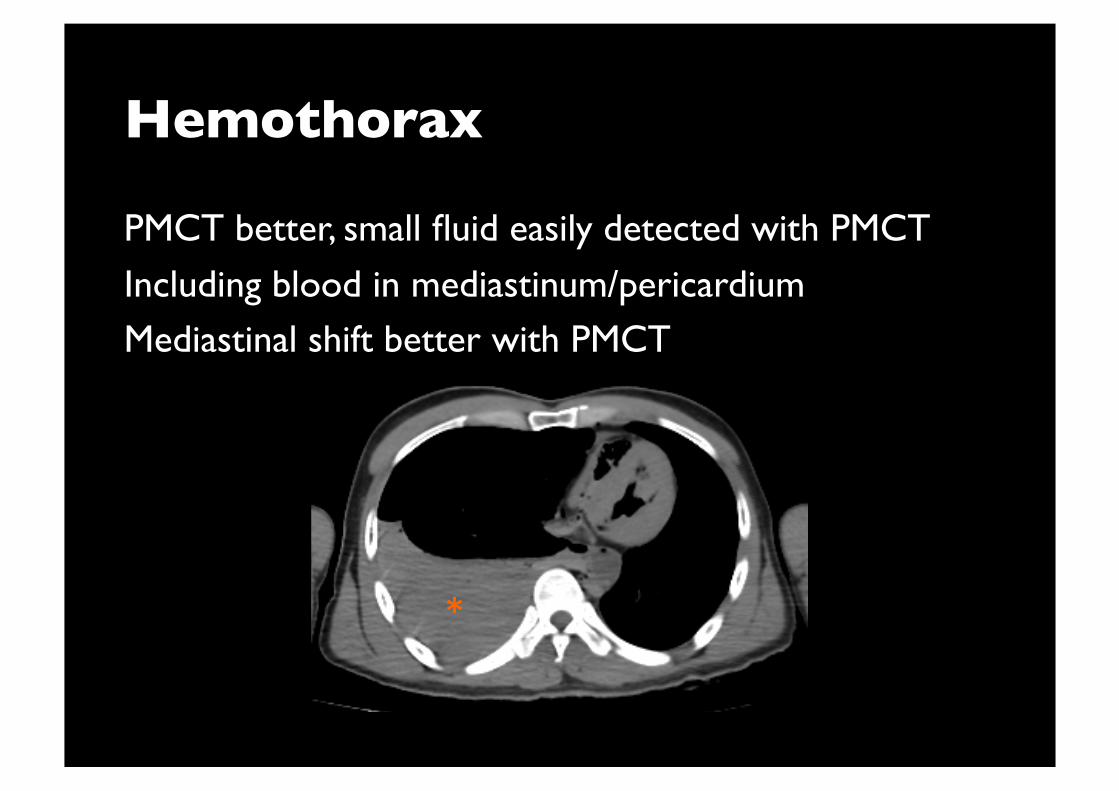
Hemothorax
PMCT better, small fluid easily detected with PMCT
Including blood in mediastinum/pericardium Mediastinal shift better with PMCT
*
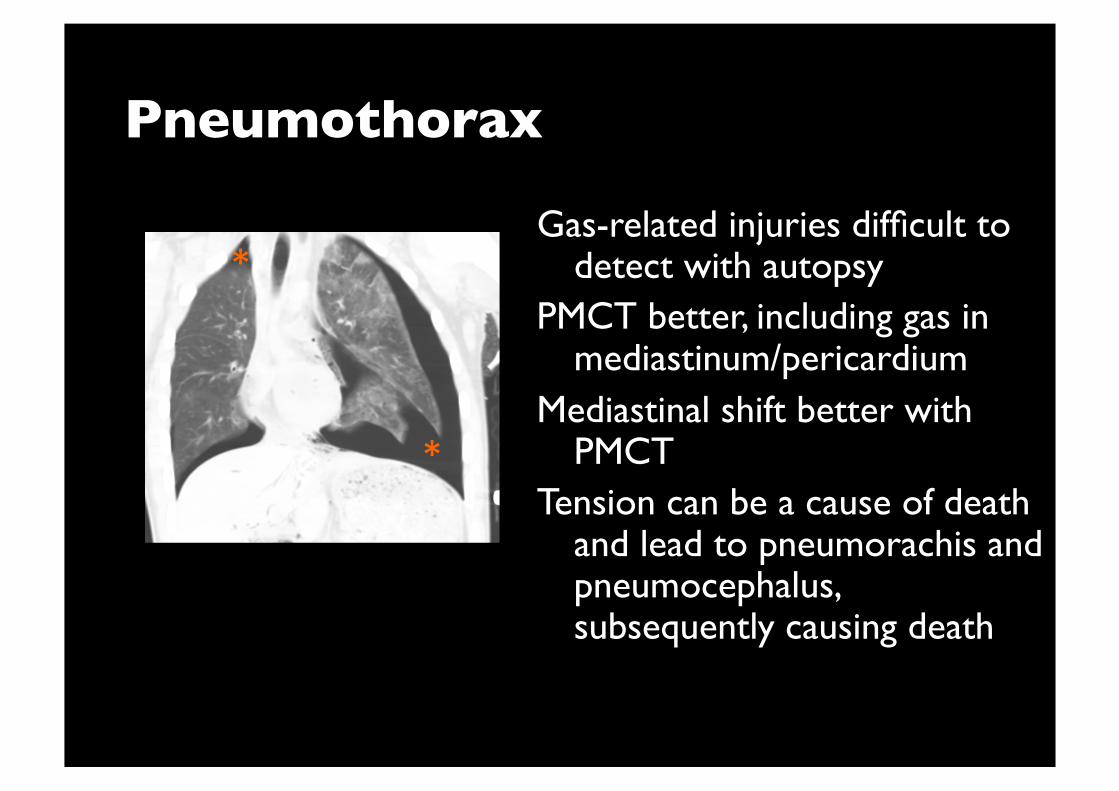
Pneumothorax
Gas-related injuries difficult to detect with autopsy
PMCT better, including gas in mediastinum/pericardium
Mediastinal shift better with PMCT
Tension can be a cause of death and lead to pneumorachis and pneumocephalus, subsequently causing death
*
*
Lung Lesions (in general)
Autopsy better
PMCT problem Hypostasis (normal PM change) Trauma: contusions, lacerations
Non-trauma: aspiration, infective pneumonia, edema Need correlation with time and mechanism of injury
Pulmonary Injuries
Large lacerations may be COD
Pulmonary alveolo-venous fistula formation Systemic arterial gas emboli
Open chest wall injury + lacerations +
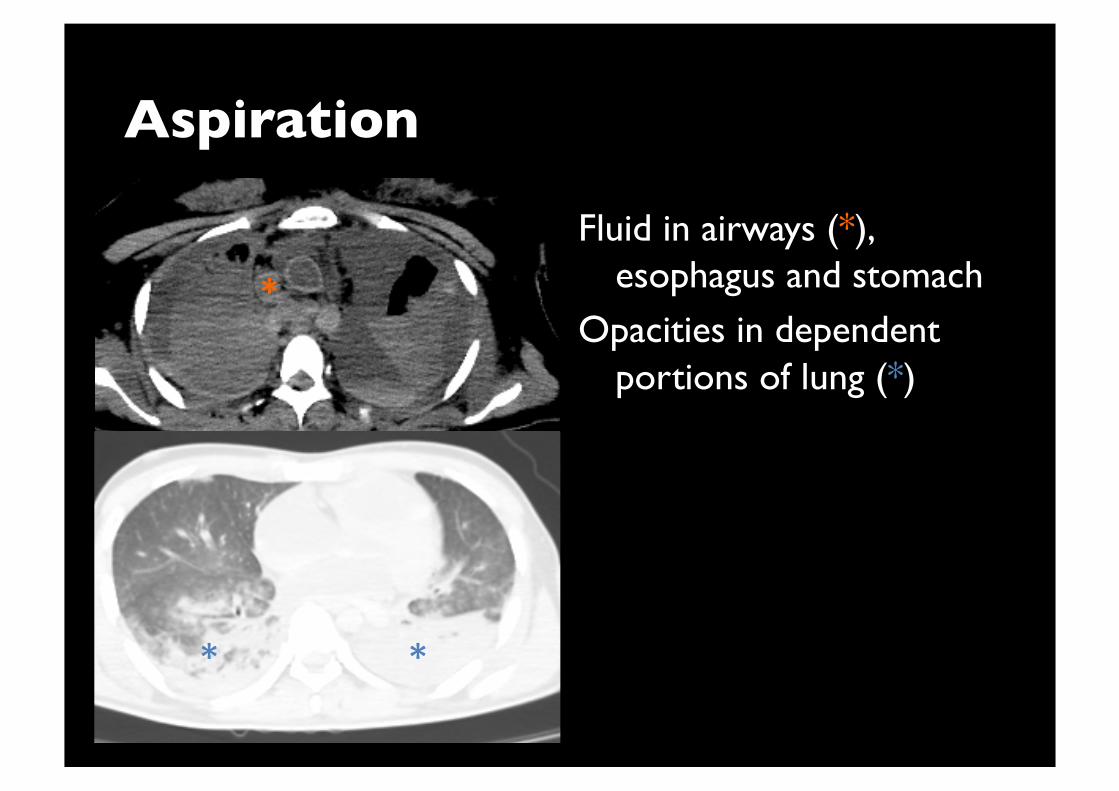
Aspiration
Fluid in airways (*), esophagus and stomach
Opacities in dependent portions of lung (*)
*
* *
Heart and Mediastinum Lesions
In general, autopsy better
Only large lesions can be seen on PMCT Pneumopericardium – PMCT better Hemopericardium – PMCT ~ autopsy
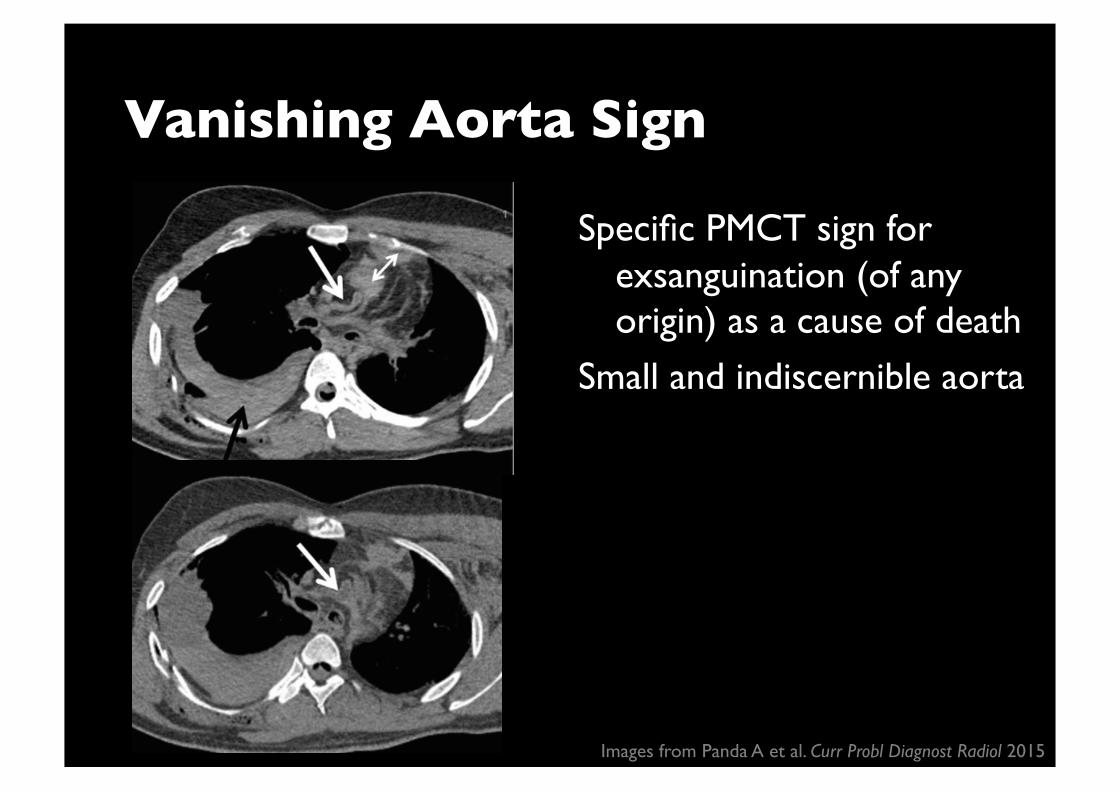
Vanishing Aorta Sign
Specific PMCT sign for exsanguination (of any origin) as a cause of death
Small and indiscernible aorta
Images from Panda A et al. Curr Probl Diagnost Radiol 2015
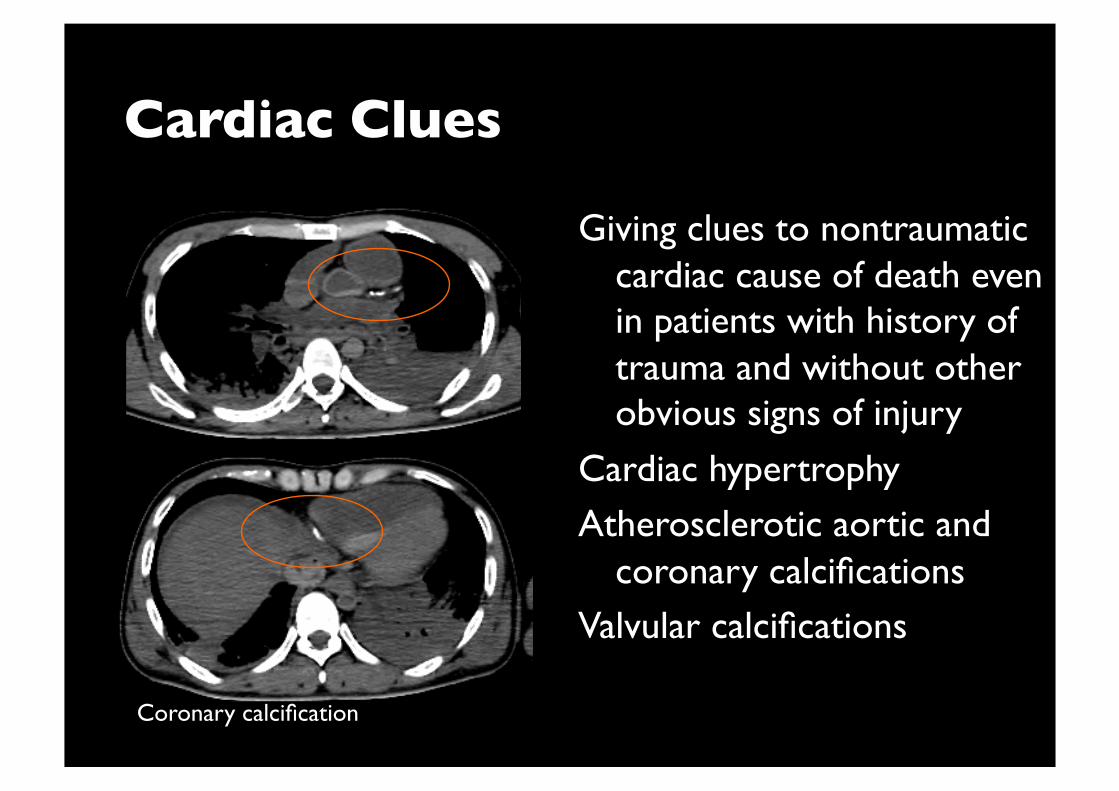
Cardiac Clues
Giving clues to nontraumatic cardiac cause of death even in patients with history of trauma and without other obvious signs of injury
Cardiac hypertrophy Atherosclerotic aortic and
coronary calcifications Valvular calcifications
Coronary calcification
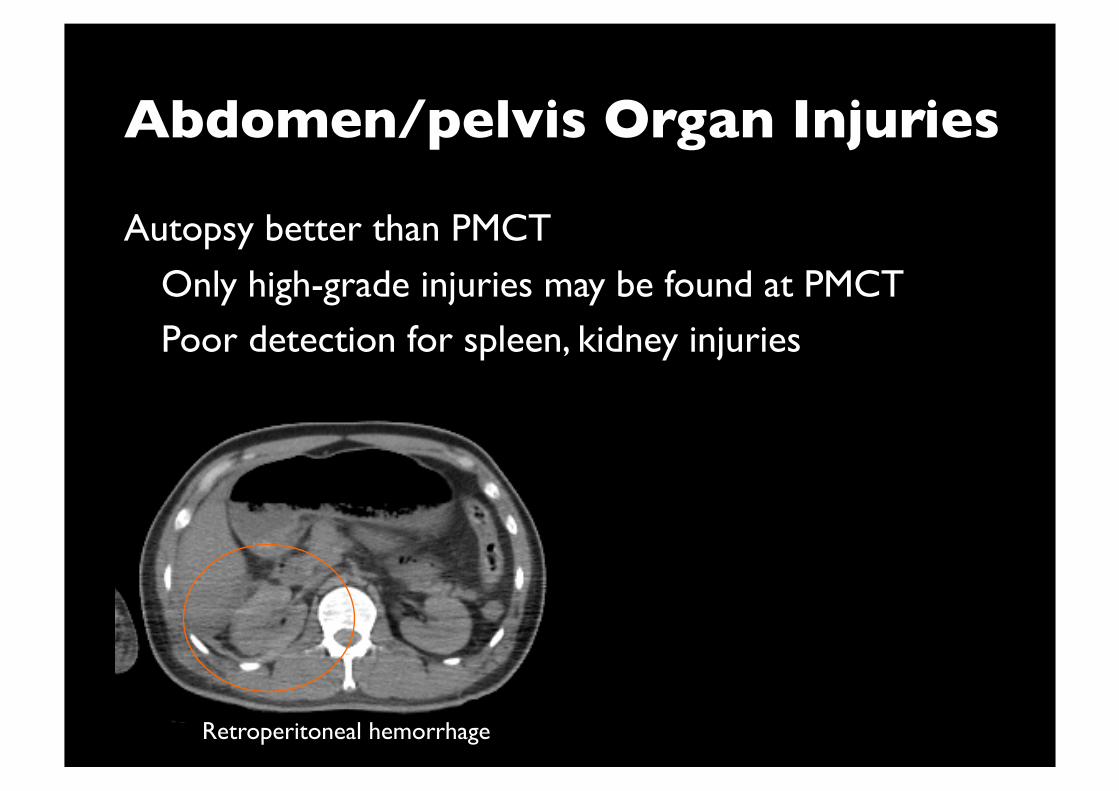
Abdomen/pelvis Organ Injuries
Autopsy better than PMCT
Only high-grade injuries may be found at PMCT Poor detection for spleen, kidney injuries
Retroperitoneal hemorrhage
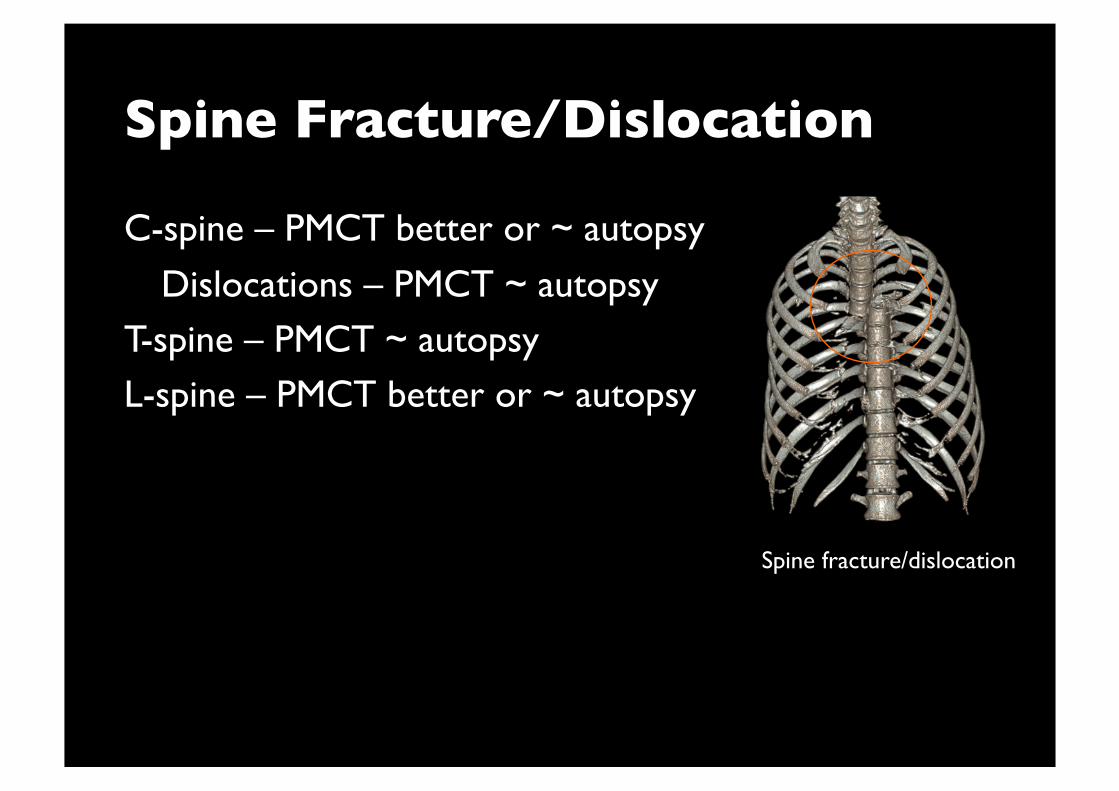
C-spine – PMCT better or ~ autopsy
Dislocations – PMCT ~ autopsy T-spine – PMCT ~ autopsy L-spine – PMCT better or ~ autopsy
Spine Fracture/Dislocation
Spine fracture/dislocation
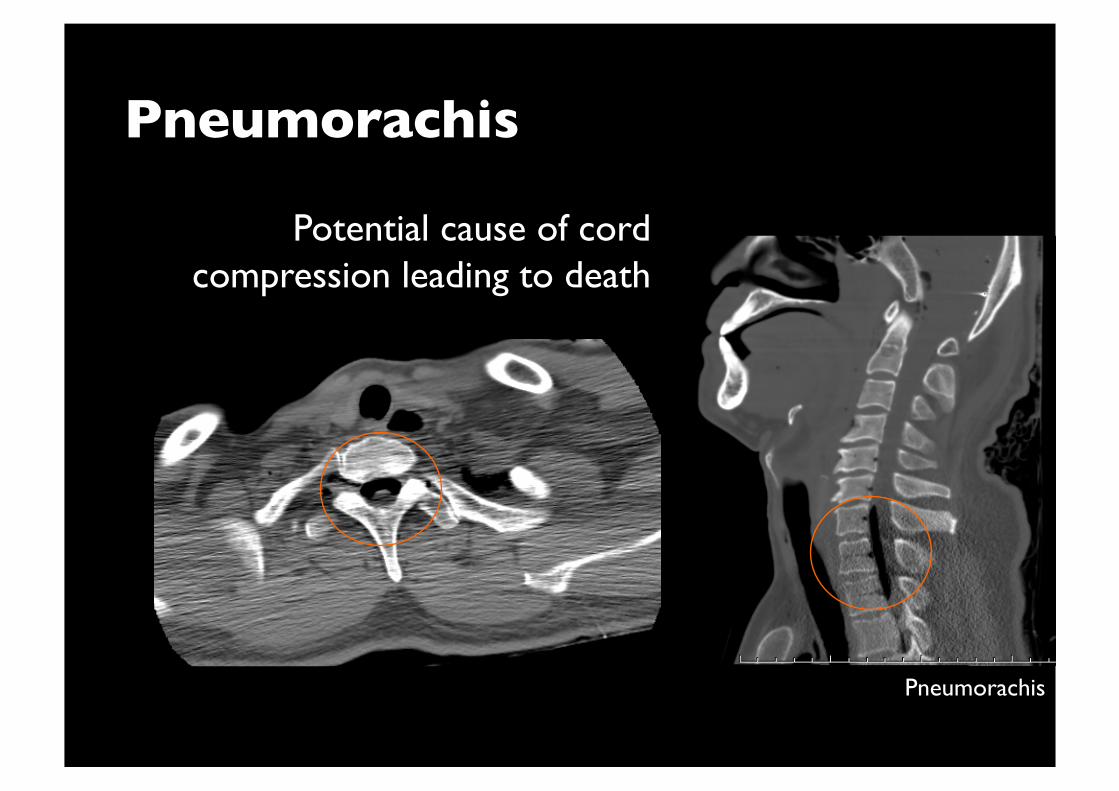
Pneumorachis
Potential cause of cord compression leading to death
Pneumorachis
Strangulation
Pneumomediastinum and cervical emphysema with abrupt cutoff at level of strangulation
Suggestive of antemortem hanging
Hyoid bone fractures Autopsy better
Cervical soft tissue injuries
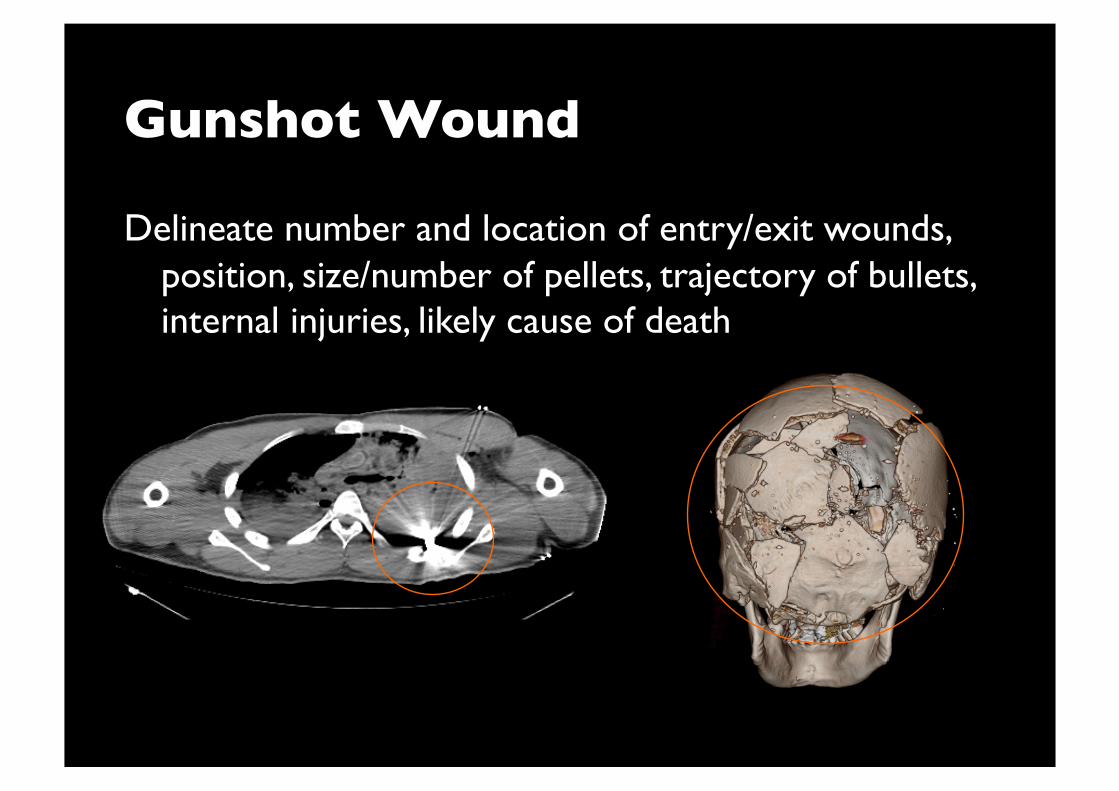
Gunshot Wound
Delineate number and location of entry/exit wounds, position, size/number of pellets, trajectory of bullets, internal injuries, likely cause of death
Cause of Death
Few PMCT studies investigated cause of trauma deaths
Exsanguination Central respiratory paralysis Hemopericardium
Concurrent gas embolisms Reports of limited no. of cases – most COD given by
PMCT were correct
Pitfalls
Common in soft tissues, heart, mediastinum, vessels and abdomen (missed diagnosis)
Unable to differentiate causes of pulmonary opacities
Setting up PMCT: Prerequisites
Curiosity
Cooperation between imaging and forensic teams Both physicians and non-physicians Role understanding
Readiness to learn Availability of scanner A little knowledge on forensic pathology, imaging
technique, interpretation and limitations
Summary
PMCT in trauma can detect wide spectrum of injuries
Most useful in detecting craniofacial, cerebral, thoracic and osseous injuries
Complementary to autopsy Can obviate need for autopsy in specific situations Limitations include inability to obtain toxologic samples,
hypothermia/burn as COD, pulmonary and fat emboli, myocardial infarctions, other natural COD