
Post transplant infections and its management. Introduction Recognizing the presentation of...
54
Post transplant infections and its management
-
Upload
baldric-lang -
Category
Documents
-
view
215 -
download
0
Transcript of Post transplant infections and its management. Introduction Recognizing the presentation of...

Post transplant infections and its management
Introduction
Recognizing the presentation of infections in transplanted patients is paramount
However, immuno-suppressed patients often present atypically, and with far advanced stages of infection
Fever is a non-specific finding, which can be attributed to medications and acute rejection
Invasive testing is often required to make an accurate and timely diagnosis

PATHOGENESIS
DISEASE DETERMINANTS
MicrobeMicrobe HostHost
Inoculum or Inoculum or OrganismsOrganisms
VirulenceVirulence
LatencyLatency
DefenseDefenseMechanismsMechanisms

HOST DEFENSE MECHANISMS
Intact skin and mucous membranes Disrupted due to trauma, burns, ulceration, IV
catheters, surgery Types of infection
Wound infections, burn sepsis, diabetic foot infection, line sepsis
Usual organisms Bacteria – environmental, endogenous Fungi – environmental, nosocomial
HOST DEFENSE MECHANISMS
Physical removal / clearance of micro-organisms Respiratory muco-ciliary clearance Peristalsis and dynamics of hollow viscus (gut, bile
ducts, ureter, fallopian tube) Maybe abnormal due to underlying disease, surgery,
smoking etc. Intact sphincters/valves Types of infection
Pneumonia, urosepsis, biliary sepsis Usual organisms
Bacteria – environmental, endogenous
HOST DEFENSE MECHANISMS
Endogenous microflora Oropharyngeal, gut, skin, vagina Important for preventing colonization with
disease causing organisms (competitive) Antibiotics remove natural flora E.g. C. difficile colitis
Chemical antimicrobial agents Gastric acidity, cutaneous fatty acids

HOST DEFENSE MECHANISMS
Inflammatory response Number (mass) and function of circulating and
tissue phagocytic cells Neutrophils, monocytes, macrophages, spleen
Humoral Mediators Complement, fibronectin
HOST DEFENSE MECHANISMS
Specific Immune response T-lymphocytes
CD4+, CD*+ (helper, cytotoxic) Number, function
B-lymphocytes Make antibodies IgG, IgA

Common problems
Host Defect:Inflammatory response
Common microbes
Neutropenia (<0.5)
Splenectomy
Gram negative bacilli, Staph, Candida, Aspergillus
S. Pneumonia, H. influenza, N. Meningitis

Common problems
Host Defect:Complement
Common microbes
Early (C3, C5)
Late (C6,7,8)
S. Aureus, S. Pneumonia, gram negative bacilli
Neisseria species
Common problems
Host Defect:Immune response
Common microbes
T- Lymphocytee.g. HIV, organ transplant
B-Lymphocyte
Numerous microbes
S. Pneumonia, H. influenza, Giardia
INFECTION: BASIC PRINCIPLES
Inflammatory response attenuated by immunosuppressants
may abolish typical signs/symptoms decreased sensitivity of serological,
radiological tests Effects of established infection may be
devastating Treatment may have more toxicities
Rifampin - decrease CsA Erythromycin, azoles increase CsA Synergistic nephrotoxicity - aminoglycosides,
AmB, septra, cipro, vancomycin, pentamidine

INFECTIONS IN TRANSPLANTATION
Three main determinants of the risk of infectionin transplant recipients
• Infections related to technical / surgical problems

TECHNICAL COMPLICATIONS
Liver - biliary tree - leaks, strictures Lung - bronchial anastomosis necrosis,
dehiscence ; mediastinal fluid collection Kidney - uroterocystostomy - leak,
urinoma Pancreas - duodenum-bladder;
duodenum-bowel: anastomotic leaks, abscess

INFECTIONS IN TRANSPLANTATION
Major determinants of the risk of infection
The net state of The net state of ImmunosuppressionImmunosuppression
EpidemiologicalEpidemiologicalexposuresexposures

NET STATE OF IMMUNOSUPPRESSION
Immunosuppressive therapy: dose, duration, temporal sequence - ‘area under the curve’
Underlying immune deficiency Mucocutaneous barrier integrity: intubation,
drains, catheters, central lines Devitalized tissue, fluid collection Neutropenia, lymphopenia
NET STATE OF IMMUNOSUPPRESSION
Metabolic conditions Uremia Malnutrition Diabetes
Viral infection: Immune modulation Cytomegalovirus Epstein-Barr virus Hepatitis B, C, HIV

Epidemiology
The risk, rate, and type of infection vary over time from transplantation
Currently, there are no assays to measure risk/susceptibility to infection
Risk of infection is an interplay between Exposure history (of donor and recipient) Intensity and quality of immunosuppression Use of prophylactic medications

Classification of Infections
Donor-derived
Recipient-derived
Nosocomial
Community-acquired

Donor-derived Infection Most are latent
CMV, TB, T.cruzi
Rarely can be acute Bacteremia/viremia at time of procurement West Nile, rabies, HIV, hepatitis, LCV
The majority of these are sub-clinical in healthy patients, but can be catastrophic when transplanted into an immuno-suppressed patient
At present, routine evaluations of donors for infectious diseases relies upon serologic antibody testing, and thus sensitivity is not 100% for those that may not have had time to seroconvert

Donor-derived
Transplantation of organs from deceased donors with viral syndromes is controversial
Livers with known Chagas or Hep B infection may be used as there are effective treatments for these infections
Hep C infected organs are sometimes transplanted into Hep C(+) donors

Fishman J. N Engl J Med 2007;357:2601-2614

Recipient-derived Infections
Infections that can be treated or controlled do not necessarily preclude transplantation
Most commonly screened for: TB syphilis Viral: CMV, EBV, VZV, HSV, HIV, HBV, HCV
Other things to think of T.cruzi, strongyloides, cryptococcus Endemic fungi: histoplasma, coccidioides,
paracoccidioides, aspergillus, blastomycosis

Polyoma Viruses
2 major clinical manifestations are known BK virus JC virus both of these are members of the papovaviridae family
JC virus is primarily associated with progressive multifocal leukoencephalopathy in AIDS pt’s
BK virus is primarily associated with nephropathy and ureteral obstruction
Both are asymptomatic infections acquired in childhood that remain latent

BK virus
First recognized in 1971, not truly appreciated until mid 1990’s when recognized as a cause for renal allograft loss (~5% incidence)
Has a tropism for the uro-genital tract, tends to affect “diseased” kidneys
Clinical manifestations asymptomatic hematuria hemorrhagic cystitis ureteral stenosis interstitial nephritis (nephropathy)

BK virus
Viruria can be detected in many populations, but the most clinically important is renal transplant recipients
Exact pathogenesis of the infection is poorly understood
Diagnosis must be made histologically (biopsy) Special stains and PCR can help solidify the diagnosis
BK virus
Treatment Only effective therapy is immune reconstitution (i.e.
reduction of immunno-suppressant therapy) Cedofivir and leflunomide are effective in reducing viral
load, but do very little to change the course of disease, and are both nephrotoxic
One must effectively walk the tightrope between progressive renal destruction secondary to infection, and acute rejection causing graft loss

BK virus
Several case reports exist for BK nephropathy in non-renal transplant recipients Bone marrow Heart Lung
However, these are rare, and are at level of case report

Fishman J. N Engl J Med 2007;357:2601-2614

Immunizations Pt’s should be current on the following
vaccines MMR HBV Influenza Strep pneumoniae Tetanus Diphtheria Pertussis Polio VZV – if never infected
Consideration should be given to boosters for any of the above prior to transplantation as live vaccines are generally contraindicated post-transplant, and immunologic memory will become impaired

Peri-operative Prophylaxis
Liver Skin, enterococcus, anaerobes, enterobacteriaceae Most common site of invasive fungal infection
Lung GNR, molds, endemic fungi MRSA and VRE according to antiobiogram prevalence Second most common site of invasive fungal infection

Nosocomial Infections
MRSA VRE fluconazole-resistant Candida species
associated with surgical site and indwelling catheters
C.diff Resistant gram-negative bacilli,
Pseudomonas, Aspergillus

Community Infections
Aspergillus Nocardia Cryptococcus neoformans (birds) Respiratory viruses Community acquired pneumonia pathogen HIV, hepatitis viruses Environmental fungi Secondary bacterial superinfection
Enteric bacterial pathogens (salmonella) TB, zoonosis,

Monitoring Immunosuppression
There are no specific tests currently available to determine the overall susceptibility of patients to infection…
…but they are on the horizon
Currently, the known determinants contributing to the overall risk of infection are the dose, duration, and sequence of immunosuppressive therapies

Fishman J. N Engl J Med 2007;357:2601-2614
Dynamic Assessment of the Risk of Infection after Transplantation
Fishman J. N Engl J Med 2007;357:2601-2614
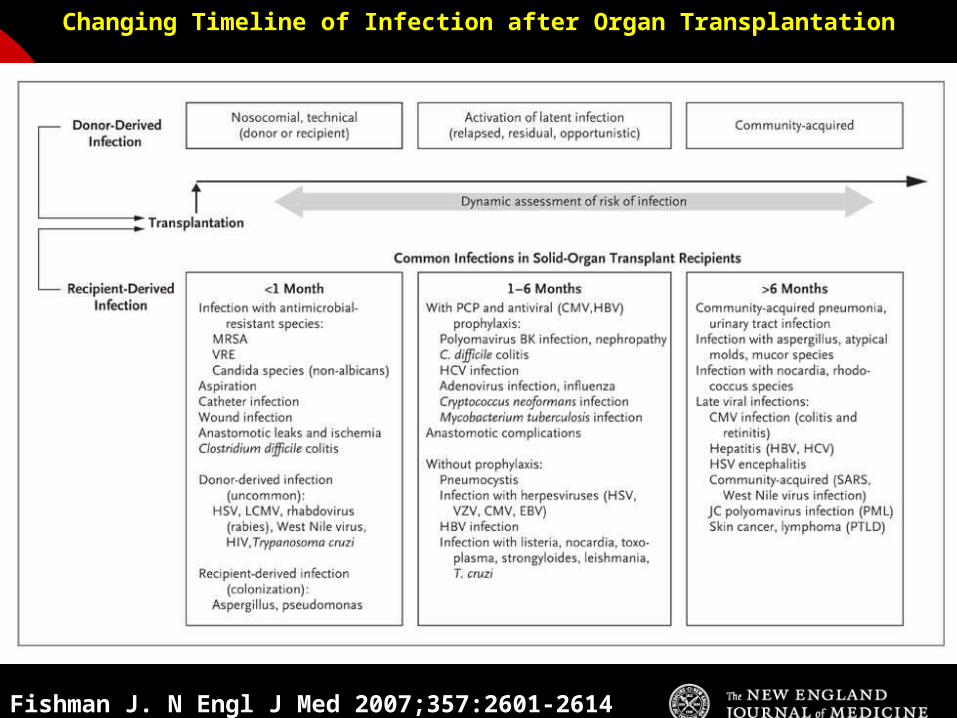
Changing Timeline of Infection after Organ Transplantation

Early post-transplant period (30d)
Opportunistic infections are rare in the first month post-transplant
>1 month of medical therapy is required to effectively deplete cell-mediated therapy
One exception is large, prolonged doses of corticosteroids
Infections are generally donor-derived or associated with complications from the surgery itself


TIMETABLE: 0-1 MONTH
Infections usual to post-op patients nosocomial pneumonia, wound, line sepsis, UTI
Key factors: nature of the operation, technical skill
Lung, heart, liver at highest risk longer intubation, ICU stay, lines, catheters
Most OI’s (eg. PCP) absent in the first month Exceptions – HSV, HHV6, Candida, Aspergillus
TIMETABLE: 0-1 MONTH
Also may see Infection transmitted with the allograft: eg.
lung transplant with pneumonia or a donor bacteremia which seeds the vascular anastamosis
Pre-existing infection within the recipient made worse by the transplant

Intermediate period (1-6mos) Viral infections and allograft rejection account for
the majority of febrile episodes
Adherence to Cotrimoxazole and antiviral prophylaxis renders infections such as PCP, UTI’s, listeria, toxoplasmosis, and herpes very unlikely
Fungi, cryptococcus, T.cruzi, strongyloides can surface
Other: polyoma virus (BK and JC), recurrent HCV


TIMETABLE OF INFECTION
One to 6 months post-Tx Maximal period of immunosuppression Effect of sustained immunosuppression or
‘area under the curve’ Opportunistic infections in the absence of
excessive epidemiological hazard

TIMETABLE - 1 TO 6 MONTHS
VIRAL CMV, EBV, VZV, HHV-6, Adenovirus, Influenza, RSV
BACTERIAL Nocardia, Legionella, Listeria, TB
FUNGAL PCP, Aspergillus, Cryptococcus, endemic mycosis
PARASITIC Toxoplasma, Strongyloides

Late post-transplant period (>6mos)
Risk wanes as immunosuppressive therapy is tapered
Risk profile however, is “reset” with each episode of acute rejection
Chronic viral infections can cause allograft injury HCV cirrhosis BOOP in lungs CMV coronary vasculopathy PTLD Skin/anogenital cancers
Fungi/molds, viruses and “typical” bugs still remain on radar


TIMETABLE - > 6 MONTHS
GROUP 1: Good graft function, minimal immunosuppression Community acquired pneumonia, UTI, OI based
on intense exposure
GROUP 2: Recurrent or chronic rejection, high level immunosuppression, chronic viral replication Continued risk of opportunistic infections

Long-term Prophylaxis
Co-trimoxazole for at least 3 months, sometimes for life
CMV and HSV prophylaxis is not standardized, and varies according to immunno-suppressive regimen and institution
Rarely chronic suppressive antifungal Rx for pt’s with history of significant disease

CMV PREVENTION
Universal prophylaxis: anti-viral therapy to all ‘at-risk’ patients
Pre-emptive therapy: anti-viral therapy to subgroups of ‘at-risk’ patients usually based on further diagnostic tests aimed at identifying early viral reactivation
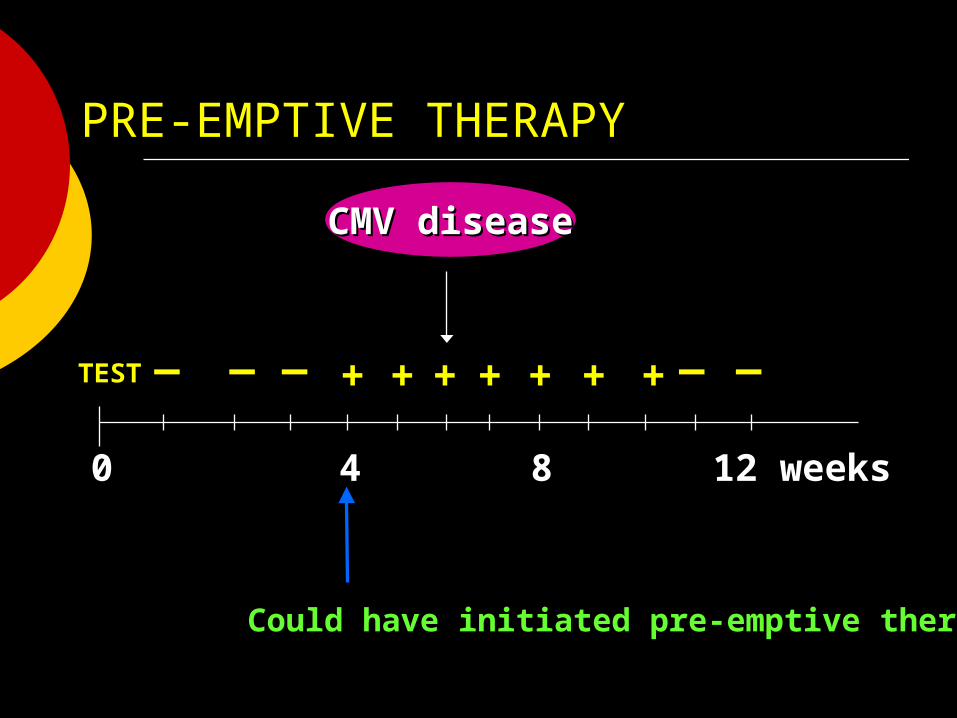
PRE-EMPTIVE THERAPY
++__
++ ++ ++ ++______
++ ++__
00 44 88 12 weeks12 weeks
Could have initiated pre-emptive therapyCould have initiated pre-emptive therapy
CMV diseaseCMV disease
TESTTEST

CMV IN LIVER TRANSPLANT RECIPIENTS
PRE-TRANSPLANT: Donor and recipient CMV serology
POST-TRANSPLANT: D+/R+, D-/R+
Week 2-12: Every clinic visit: CMV antigenemia CMV quantitative PCR
D+/R-: Ganciclovir prophylaxis 12 weeks
Bloodwork at week 12, 14, 16, 18. CMV antigenemia and quantitative PCR testing

General Lifestyle Recommendations
Avoid sick contacts, esp respiratory Avoid dusty sites (i.e. construction sites) Avoid ingestion of well and lake water Avoid undercooked meats Avoid soft cheeses and unpasteurized dairy
products Avoid unwashed fruits/veggies

Summary
Be aware of the time frame from transplant leading you to the most likely type of infection
<30d think nosocomial or donor-derived
1-6mos, reactivation of viruses and atypical infections “classic” for transplant pt’s
>6mos, think of “typical” or community-acquired bugs as their risk returns to somewhat normal
Fishman J. N Engl J Med 2007;357:2601-2614
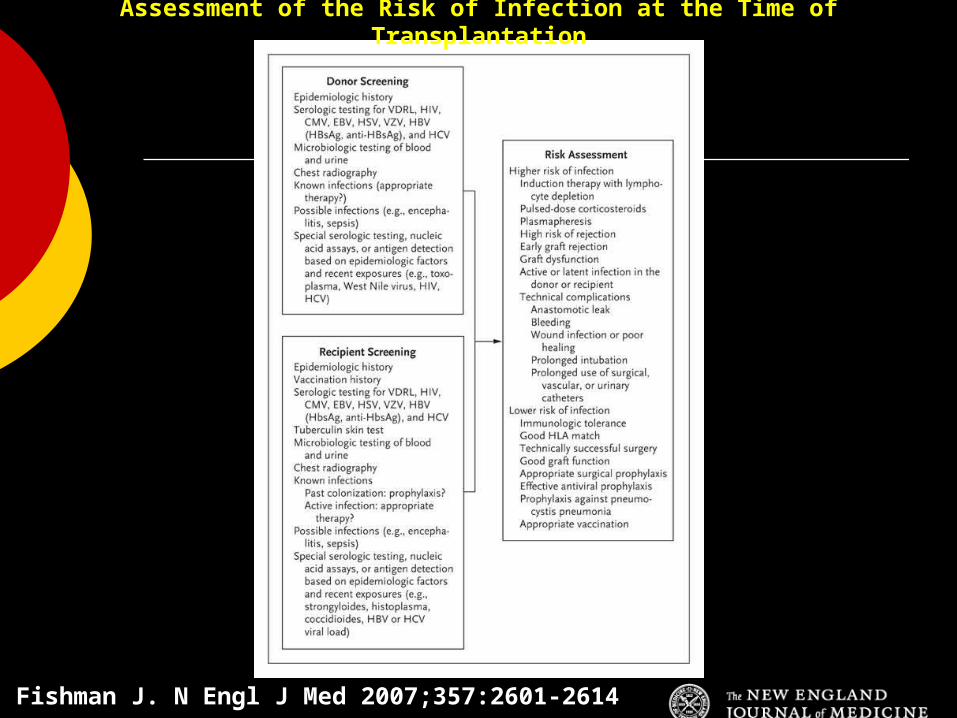
Assessment of the Risk of Infection at the Time of Transplantation

















