POLYMORPHISM OF UDP-GLUCURONOSYLTRANSFERASE AND … · Figun 11. Figure 12. Page Gene Structure of...
116
GENETIC POLYMORPHISM OF UDP-GLUCURONOSYLTRANSFERASE UGT2B7 AND IN VIVO GLUCURONIDATION OF OXAZEPAM: A GENOTYPE-PHENOTYPE COMPARATIVE STUDY Peter Somphone Kard A thesis submitted in conformity with the requirements for the Master of Science Gnduate Department of Pharmacology University of Toronto 8 Copyright by Peter Somphoae Kard 1999.
Transcript of POLYMORPHISM OF UDP-GLUCURONOSYLTRANSFERASE AND … · Figun 11. Figure 12. Page Gene Structure of...

GENETIC POLYMORPHISM OF UDP-GLUCURONOSYLTRANSFERASE UGT2B7 AND IN VIVO GLUCURONIDATION OF OXAZEPAM:
A GENOTYPE-PHENOTYPE COMPARATIVE STUDY
Peter Somphone Kard
A thesis submitted in conformity with the requirements for the Master of Science Gnduate Department of Pharmacology
University of Toronto
8 Copyright by Peter Somphoae Kard 1999.

National Library !al of Canada Bibliothhque nationale du Canada
Acquisitions and Acquisitions et Bibliographie SeMces services bibliographiques
395 Wellington Street 395, rue Wellington OttewaON K I A O N 4 W w a O N K1AON4 Canada Canada
The author has granted a non- exclusive licence allowing the National Library of Canada to reproduce, loan, distribute or sel1 copies of this thesis in microform, paper or electronic formats.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la foxme de microfiche/film, de reproduction sur papier ou sur format électronique.
The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts fiom it Ni la thèse ni des extraits substantiels may be printed or othenMse de celle-ci ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation.

Genetic polymorphism of WDP-glucuronsyltransfenw UGT2B7 and in vivo
glucuronidation of oxazepam: A genotype-phenotype comparative study. M. Sc. 1 999.
Peter Somphone Kard. Department of Pharmacology. University of Toronto.
In this study, oxazepam was used as a probe dnig to study a genetic
polymorphism in UDP-glucuronsyltransferase UGTZB7. The SR oxazeparn glucuronide
ratio (SR ratio) of 203 subjects afier an oral dose of (RS) oxazepam was bimodally
distnbuted, with approximately 18% of the population possessing S/R ratios below an
antirnode of 1.66. An allele specific amplification assay that has the ability to distinguish
between the wildtype and variant alleles of UGT7B7 was established in this study.
Genotyping of 1 14 individuals demonstrated that the allelic frequency of the variant and
wildtype alleles within the population is 0.474 and 0.526, respectively. The genotype of
8 individuals who had previously been phenotyped demonarated that a homozygous
variant genotype is associated to an atypical phenotye, whereas, heterozygotes as well as
homozygotes for the wildtype allele are phenotypically normal in regard to the S/R ratio.
This is the first study that has demonstrated an association between a genetic
polymorphism in the UGT2B family and variations in the in vivo giucuronidation of a
drug .

1 would like to thank Dr. B.K. Tang, Dr. W. Kalow, and Dr. D.M. Grant for their guidance and support. 1 would also like to thank J. Wong, V. Ozdemir and G. Gwdfellow for technical assistance. Without the involvement of these individuals, this work could not have been possible.

Table of Contents
1. Introduction
Page
UDP-Glucuronosyltransferases The UGT Multigene Family UGTl Family Genetic Polymorphism in the UGT 1 Family
Gilbert's Syndrome Cng ler-Nad ar Syndromes
UGT2 Family UGT2 Gene Str~cture Genetic Polymorphisms in the UGT2B subfamily UGT2B7 UGT287 versus UGTZB7
Glucuronidation of Dmgs Variability in Glucuronidation
Oxazepam Factors that Influence the Metabolism of Oxazepam Enantioselective Glucuronidation Rationale Hypot hesis Objectives
II Methods and Materials
In vivo Glucuronidation of Oxazepam Subjects Chromatographic Anal ysis Data Analysis
Molecular Work DNA Extraction fiorn Tissue PCR of UGT2B7 fiorn Genomic DNA RNA Extraction fiom Tissue First-Strand Synthesis of cDNA PCR of Actin cDNA RT-PCR of UGT2B7 cDNA Gel Extraction of PCR products Subcloning and Transformation Miniprep of Plasmid DNA Sequencing Reaction
Allele S pecific Amplification Mouthwash Method for Obtaîning Genornic DNA

III Rcsults
In vivo Oxazepam Metabolkm Interindividual Variability in the S R ratio 5 1 Factors that Influence the S/R ratio 51 S- and R- Oxazepam Glucuranides vs. SIR ratio 56 Factors that Intluence the Glucuronidation of S- and R- Oxazepam 58
Molecular Work Genornic Sequence of UGT2B7 Sequence of UGT2B7 Triinscripts Allele Specific Amplification Genotyping Results Genotype-Phenotype Cornparison
IV Discussion
Distribution of the S/R Ratio S R Ratio vs. S- and R- glucuronides Factors that Influence Glucuronidation of S- and R- Oxazepam and the S/R Ratio Genotype within a population Genotype-Phenotype Cornparison Conclusion Future Studies
v References
VI Appendices Appendix 1. Appendix 2. Appendix 3. Appendix 4.
Appendix 5 . Appendix 6.
Individual Phenotypes Results Obtained in this Study Individual P henotypes Results nom Appana (1 995) Individual Genotype Results Sequence Cornparisons b e ~ n UGT2B7 and other UGT2B Isozymes Sequence of UGT2B4 Characteristics of the 8 individuals used in the genotype- phenotype comparative study

List of Figures
Figure 1.
Figure 2.
F i p n 3.
Figun 4.
Figun 5.
Figure 6.
Figure 7.
Figure 8.
Figure 9.
Figure 10.
Figun 11.
Figure 12.
Page
Gene Structure o f UGTs 4
Schematic of RT-PCR Amplification of UGT2B7 39
Vector Map of [email protected] 42
Schematic of Allele Specific Amplification 47
Distribution of SIR Ratio in a Population 53
Correlation Analyses of the S/R Ratio vs. S- and R- Glucuronides 57
Genomic Sequence of UGT2B7 62
Automated Sequence of UGT2B7 Transcript 65
Variant and Wildtype Sequences of UGT2B7 66
Allele Specific Amplification 68
Phenotype-Genotype Cornparison 71
A Plot of SIR Ratio vs. UGT2B7 Genotype 72

List of Tables Page
Table 1. Genetic Mutations Associated with CN and Gilbertk Syndromes 6
Table 2. Factors that Affect Oxazepam Metabolkm 18
Table 3. Characteristics of Subjects 3 1
Table 4. Summary Table for SR Ratios 54
Table 5. Correlation of Various Factors vs. S/R ratio, S-, and .R- Glucuronides
Table 6. Cornparison of S- and R- Glucuronides between sexes, ethnic groups, and OC users vs. Non-OC users 60
Table 7. Summary of UGT2B7 Genotypes 69

List of Abbrcviations
ASA
cDNA
CN
FISH
HDCA
HPLC
Km
MuLV
NAT
NS AID
mv
OC
PCR
RFLV
rGc
S/R ratio
UDPGA
UGT
YAC
Allele Specific Amplification
Complementary deoxyribonucleic acid
Crigler-Nad ar Syndrome
Fluorescent in situ hybridization
Hyodeoxycholic acid
High pressure liquid chromatography
Michaelis constant
Murine Leukemia Virus
N-acetyltransferase
Non-stenodal anti-inflammatory dmg
Norrnality test variable
Oral contraceptive
Polymerase chah reaction
Restriction fragment length variation
Genetic component value
SIR oxazepam glucuronide ratio
Uridine-diphospho-D-glucuronic acid
Uridine-disphospho-g~ucuronosy ltransferase
Yeast artificial chromosome


UDP-GLUCURONOSYLTRANSFERASES
UDP-glucuronosyltransfetases (UGTs) are a superfamily of dmg metabolizing
enzymes. UGTs caîaiyze the transfer of the glucuronic acid moiety of UDP glucuronic
acid (UDPGA) to a wide variety of substrates. In humans, glucuronidation represents a
major detoxification pathway for many xenobiotics as well as endogenous substrates
(Bock, 199 1; Burchell et al., 1995; Dutton. 1980). Phamaceutical agents, plant
constituents, environmental pollutants, and carcinogens are al1 substrates for UGTs.
Endogenous compounds for glucuronyhransferases include; bilimbin, steroid hormones,
fat-soluble vitamins, bile acids, thyroxine. and biogenic amines.
The UGT Multigene Family
To date, 48 distinct mamrnal ian cDNAs of the UGT multigene famil y have been
characterized (Mackenzie et al., 1997). Of these 48, there are 18 human isoforms, 17 rat
forrns, 4 mouse fons, 6 rabbit forms, 2 monkey forms, and one bovine isofonn.
The human UGTs are separated into two families, UGTl and UGT2. This
separation is based upon the similarity of the amino acid sequences. Members of the
UGTl family have a p a t e r than 50% sequence homology to each other but less than a
50% homoiogy to the members of the UGTZ family (Burchell et al., 1991).

UGTl Famiiy
Al1 the human members of the UGTl family are produas of a single gene. The
UGTl gene complex is located on chromosome 2q37 and consists of 16 exons spanning
500 Kb (Harding et al., IWO). Each isofom is comprised of one of the 12 unique
promoterffirst exons and common exans 2 to 5 (Ritter et al., 1992a). The isozymes of the
UGTl family therefore share a comrnon carboxyl tail, while possessing a unique amino
terminal region (see Figure 1 .).
The substrate preferences of six UGT l isofoms (UGT 1 A 1, 1 A3, 1 A4, 1 A6, 1 A8.
and 1A9) have been detemiined. When the full-length cDNAs of these isofoms were
transiently expressed in COS cells or aably expressed in V79, or HEK 293 fibroblasts,
they glucuronidated a wide range of substrates (Burchell et al., 1995; Cheng et al., 1998;
Ebner and Burchell, 1993; Green et al., 1998; Visser et al., 1993). Endogenous substrates
include bilirubin, thyroid hormone. and some foms of steroids. Some of the exogenous
substrates include small planar phenols, halogenated and bulky alkyl phenols, aromatic
carboxylic acids, coumarins, and amines. UGTI Al is thought to be the major isoform
responsible for the glucuronidation of bilirubin, while the phenols are specific substrates
for UGTlA6 and UGTlA9. The substrate specificity for UGTIM, 1A7, 1A8, 1 Al0 have
not been elucidated since the cDNAs fiom these isofoms have not been isolated. It is
believed that UGTl AZ, UGTl Al 1, UGTlA12 isozymes are pseudogenes since the first
exons of these isoforms contain non-sense mutations within their predicted amino acid
sequences.

Figure 1. The gene structure for the UGTl farnily and the UGT2B subfamily (l,2). UGTl isozymes are encoded frorn a single gene locateci on chromosome 2. Whereas, the UGT2B isoforms are transcribed fkom independent genes located on chromosome 4. The diagrams are not drawn to d e .
Unique promot edexon 1 Common exons 2-5

Genetic Polymorhisms in the UGTl Famüy
Much of the knowledge about genetic variations in UGTs have been gained from
the study of Gilbert's and Crigler-Naüar (CN) syndromes (see Table 1 .). Unconjugated
hyperbilimbinemia is a characteristic of both of these disorders. Before the discovery
that the isofoms of the UGTl family were encoded by a single gene complex,
researchers studying Gilbert's and CN were pualed by the findings that some patients
with Gilbert's or CN also had an inability to glucuronidate phenols while other patients
with the same disorders exhibited normal phenol metabolism. It is now known that
mutations in the unique promoter/exon 1 region of UGTl Al will give rise to a phenotype
of hyperbilimbinemia. Whereas, mutations in the cornmon exons 2-5 will not only affect
the bilimbin-metabolizing enzyme but also dl of the other isoforms encoded by the
UGT 1 gene complex including the phenol-metabolizing enzymes.

Table 1. Human UGTl A l aileles in patients with Gilbert's or Crigler-Najar di- (CN). The human wild-type UGT 1 A 1 allele, encoding the functional enzyme is regardcd as UGT 1 A 10 1.
Namt
Gilûert's Syndrome
UGTlA1*3 UGTlAlfS UGTlA1*10 UGT1AlS16 UGTlAl*17 UGTlA1*18 UGTlAl*19 UGTlA1*20 UGTlAl*21 UGT 1 A 1 *22 UGTlA1*23 UGTlA1*24 UGTlAl*25
-
Nudeotidt change
Effect on Protein
teduccd expression
S375F deletion of exon2
R341X Q35fR S381R A401P W33 JX A368T
Frameshdt A292V KS26E K437X C280X
Bosma et al. 1995/Monaghan et al. 1996lBeuîier et al. 1998 Aono et al. 1993 Aono et al. 1993Koiwai et al. 1995 Aono et al. 1995Koiwai et al. 1995 Aono et al. 1995Koiwai et al. 1995
Bosma et al. 1992 B o s m et al. L 992 Moghrabi et ai. 1993 Labrune et ai. 1994 Labrune et al. 1994 Labrune et al. 1994 Labrune et al. 1994 Labrune et al. 1994 Labrune et al. 1994 Labrune et al. 1994 Labrune et al. 1991 Labrune et al. 1994 Aono et al. 1994
Aono et al. 1993 Aono et al. 1993 Bosma et al. 1993lSeppen et al. 1994 Seppen et al. 1994
v - heteroqgous genotypes have Gilbert's syndrome, while homozygous genotypes have the CN2 phenotype -X represents non-sense mutations - adapted from Mackenzie et al. 1997

Gilbert's Syndrome
Gilbert's syndrome is a mild fonn of unconjugated hyperbilirubinemia. This
disorder is found in 2019% of the population (Bosma et al., 1995a). tt is believed that this
disorder results fkom genetic abnonnalities in the UGT responsible for the
glucuronidation of bilirubin, namel y UGTl Al. Recently, a polymorphism in the
promoter region of the UGTl Al gene was reported to be linked with most of the clinical
cases of Gilbert's syndrome (Aono et al., 1995; Bosma et al., 1995b). Patients with
Gilbert's syndrome were genotyped as being homozygous for 7 TA repeats in the
(TA),,TAA box of the promoter region. The usual number of TA repeats is six.
Recently, the nomenclature for this polymorphisrn was assigned as UGT I A 1 *28
(Mackenzie et al., 1997).
A population study conducted in Scotland demonstrated that (TA)d(TA)7
individuals possessed significantly higher biiirubin concentrations than individuals with
either the (TA)o/(TA), or (TA)o/(TA)6 genotypes (Monaghan et al., 1996). They also
reported that among the Scottish population 10-13% of individuals within the population
are homozygous for the UGT 1 Al *28 mutation.
Interesting 1 y, interethnic di fferences of the (TAhTAA box repeats were observed
between Asians. AFncans, and Caucasians (Beutler et al., 1998). Africans had the highest
gene fiequency for the (TA17 allele (0.43), followed by Caucasians (0.39), while Asians
had the lowest (TA)7 gene frequency (0.16). Furthemore, arnong the Afncan population
there were individuals with 5 and 8 (TA) repeats. In comrast, both the 5 and 8 (TA)
repeats were not observed in either the Asian or Caucasian populations.

Mutations in the coding region of UGTlAl gene have aiso been shown to be
sssociated with Gilbert's syndrome (Aono et al., 1995; Koiwai et al., 1995).
Heteroqgosity of the one of following missense mutations is linked to Gilbert's
syndrome: exon 1 (G7 1 R or P229Q). exon 4 (R3 67G), or exon 5 (Y486D). Interestingly,
homozygosity of either the G71R or the Y486D results in Crigler-Najjar syndrome type
II (Aono et al., 1993).
Crigkr-Najjar Syndrome
Cngler-Najar (CNl and CN2) syndromes are a potentially lethal form of
unconjugated hyperbilinibinemia resulting from the complete absence or severely
reduced ability to glucuronidate bilinibin (Crigler and Najjar, 1952). Based upon the
plasma levels of unconjugated bil irubin and the response to barbiturate therapy, Crigler-
Najar syndrome is categorized into two types; CXl and CN2 (Arias et ai., 1969). CN1
patients have unconjugated plasma bilinibin levels in excess of 340 pM, whereas the
bilinibin levels of CN2 patients are below 340 W. Furthemore, when both patient
groups are prescribed phenobarbital, only the CN2 patients show a decrease in
unconjugated bilirubin plasma levels.
The molecular basis for Crigler-Najjar syndrome has been extensively studied
(see Table 1 .). Like Gilbert's syndrome, both types of Crigler-Najjar syndrome are linked
to genetic variations in the UGTl gene locus.
Inactivating substitutions as well as fiameshifi and non-sense mutations which
produces tmncated proteins are shown to be associated with Crigler-Nadar syndrome
type 1. Bosma et al. (1992) were arnong the first to demonstrate that genetic

abnonnalities in the UGTl gene were linlced to CNl. Sequence analysis of one CNl
patient showed a C+T substitution in exon 4 resulting in a change of a serine residue to a
phenylalanine (üGT 1 Al *3). Another CN 1 patient had a C+T substitution at position
99 1 (UGT 1 A l *5) of the coding region. This mutation resulted in the deletion of the
entire second exon. The rnRNAs of the UGTlA4, 1A6, and 1 A9 isofoms in both
patients also contained the respective mutations. Moreover, neither of these individuals
had the abiiity to glucuronidate phenol cornpounds (Bosma et al., 1992).
In a study of CN 1 children from various regions in Europe, 9 novel mutations
associated with Crigler-Najjar syndrome type 1 were discovered (Labrune et al., 1994).
Of the 9 new mutations discovered, 6 produced inactive proteins (UGT I A1 * 16, * 17, * 18,
*20, *22, and UGTlA1*23), 2 resulted in terminal codons (UGTI A1 * 19 and
UGT1A1*24), and one was a fiameshifi mutation that produced a truncated UGTl Al
protein (UGT1 Al *2 1).
A family study of one Japanese CN1 patient reported a novel mutation (Aono et
al., 1994). The patient was genotyped as being homozygous for a missense mutation at
position 840 of the coding region (UGTlA1*25). What was interesting about this case
was that both the parmts and a brother of this individual had normal phenotypes even
though they were heterozygotes for the mutant allele.
Recently, a novel molecular basis for the pathogenesis of CN1 was reported
(Gantla et al., 1998). Two separate mutations in the non-coding intronic sequences of the
UGTl Al gene were associated with CNI. One individual was hornozygous for a G+C
mutation at the exon lhntron junction. This mutation resulted in a cryptic splice site
which deleted 141 nucleotides in the mRNA of exon 1. The other patient was

heterozygous for a C+T mutation at the splice-donor site between exon 3 and exon 4.
This individual also possessed a non-sense mutation at position 145 of the coding region
on the other allele. Both of these mutations are thought to have contnbuted to the CNl
phenotype in this individual.
In contrast to CNl patients, CN2 patients have the ability to glucuronidate
bilinibin, albeit this ability is severely limited. In general, the mutations that are
associated with a CN2 phenotype reduce the activity of the UGTI Al enzyme. Whereas.
the mutations that are linked to the CNl phenotypes generally result in the complete
inactivation of the UGTl Al protein. Thus, CN2 patients can be homozygous for a
pmicular mutation and still exhibit some biiinibin glucuronidation. UGTIAI *6,
UGTI AI *7, and UGT1Alt8 are examples where the patients have a CN2 phenotype and
are homozygous for a particular mutation (Aono et al., 1993; Bosma et al., 1993).
However, CN2 phenotypes could also result from heterozygosity of a mutation
(UGTI Al * 12) that causes CNI (Seppen et al., 1994).
The UGT2 Family
The mammalian UGT2 family consists of 2 subfamilies, UGT2A and UGTZB.
The cDNAs of both rat and bovine UGT2A genes have been isolated, and were shown to
be olfactory-specific proteins that conjugate odorant molecules Gazard et al., 199 1). To
date, however, the isolation of a human UGT2A homologue has been unsuccessful.
UGT2B genes have been isolated in humans, rats, mice, and rabbits. In humans,
7 distinct UGTZB cDNA clones have been isolated thus fu. The substrate preferences for
UGT2B 10 and UGT2B 1 1 have yet to be daermined while UGT2B4,287,2B 1 5, and

UGT217 have been show to be specific for stemids and bile acids (Beaulieu et al., 1996;
Jackson et al., 1987; Ritter a ai.. 1990). However, like the members of the UGTl family,
these isoforms also have the ability to glucuronidate a broad range of substrates.
UGTZB Gene Structure
Sequence analysis of UGT2B transcnpts have show that among the UGT2B
subfamily members, sequence differences occur throughout the entire coding region, thus
indicating that the memben of the UGT2B sufamily are transcribed fkom independent
genes. Yeast artificial chromosome (YAC) technology as well as fluorescent in situ
hybridization (FISH) studies were used to localize UGT2B4, UGT2B 1 5, and UGTZB 17
genes to a "UGTZB gene cluster" on chromosome 4q13 (Beaulieu et al.. 1997; Monaghan
et al., 1997). Analysis of UGT2B4 and UGTlB 17 exodintron structures demonstrated
that the intron locations are conserved between the UGT2B isoforms (see Figure 1). This
conservation of the gene structure suggests that the UGT2B isoforms originated fiom a
cornmon ancestral gene. Furthemore, it is believed that the individual isozymes of the
UGT2B subfamiiy are derived fkom gene duplication events.
Genetic Poly morhisms in the UGT2B Famüy
In contrast to the UGTl family, knowledge about genetic polymorphism(s) in the
UGT2 family is limited. As yet. there have been no known genetic defect(s) in the UGT2
family that are linked to clinically important phenotypes.
Recently, Belanger's group at Laval University reported the characterizarion of
genetic polymorphisms in two UGT2B genes, UGT2B15 and UGT2B4 (Levesque et al.,

1998; Levesque et al., 1997). In their fint snidy, a novel UGTZB CDNA cione was
isolated âom human prostate and LNCaP ce11 cDNA libraries UGTZB 1 5(Y8'). There
was a single amino acid difference (aspartate to tyrosine at position 85) between
UGT~B 1 5(Ya5) and UGT~B 1 5(D8'), the previous published sequence ofUGT2B 15
(Green et al., 1994). Using PCR and direct sequencing techniques. 27 subjects were
genotyped for the mutation. Of the 27 individuals tested, 6 were homotygous for the
(Y8? allele, 5 were hornozygous for the (Dg') allele. while 16 subjects had both alleles.
Similar substrate specificities were obsewed for both alleles when they were expressed in
HK 293 cells. However, the Vmax values for UGTZB 15(y83 were 2 fold higher than
that for UGT2B 1 508').
In their other study, they reponed the isolation of a novel UGT2B4 cDNA clone,
UGTZB~(E"~) (Levesque et al., 1998). The difference between U G T ~ B ~ ( ~ ~ ~ ) and the
published sequence, U G T ~ B ~ @ ~ ' ~ ) , is a substitution of aspartic acid for glutamic acid at
position 458. Sequencing of genomic DNA from 26 Caucasian subjects demonstrated
that 8% of the population were hornozygous for the (E4j8) allele, 30% were homozygous
for the allele, while 62% had both alleies. When expressed in HK293 cells,
UGT~B~(E~. '~ ) was highly active towards hyodeoxychoiic acid (HDCA). In contrast,
UGTZB~@~*) did not glucuronidate HDCA The results suggest that this amino acid is
responsible for substrate specificity.
It has yet to be detemined whether or not the genetic polymorphisms seen in the
UGTZB4 gene as well as in that of UGTlB15 gene have any physiological importance.

UGT2B7
A UGTZB7 cDNA clone was fin isolated from a Xgtl 1 cDNA library by
hybridization to a mouse glucuronosyltransferase cDNA clone (Ritter et al., I W O ) . The
transcnpt of UGT2B7 encodes a 529 amino acid protein whose primary substrates are
3 +catechol estrogens and estriol. Using human liver Ncrosomes and di fferent
expression systems, UGT2B7 has been shown to be a very non-specific enzyme.
UGT2B7 is reported to be the major UGT isofonn that glucuronidates hyodeoxycholic
acid. oxazepam, NSAIDs, and hydroxylated derivatives of prototypical carcinogens such
as benzo[a]pyrene and 2-acetylaminofluorene as well as estrogen derivatives (Jin et al.,
1993a; Jin et ai., 1997; Jin et al., 1993b; Patel et al.. 199Sb; Ritter et al., 1990; Ritter et
al., 1992b). In contrast to earlier reports, recently, UGT2B7 has been shown to have the
ability to glucuronidate morphine, opioid agonists, antagonists, and partial agonists
(Cofhan et al., 1998; C o f i a n et al., 1997).
The fact that UGT2B7 is the major isoform that glucuronidates a diverse range of
clinically important compounds attests to the physioiogical imponance of this enzyme.
Therefore, any genetic variation(s) that alters the substrate specificity or changes the
activity of the UGTZB7 protein may result in clinically relevant alterations.
UGT~B~(H'U) venus UGTZB~(Y'U)
In 1993, Jin et al. isolated a novel UGT2B7 cDNA clone from a hgt 1 1 hurnan
liver cDNA library. This clone had a C+T substitution at position 802 of the coding
region. The base pair change resulted in an amino acid (histidine to tyrosine) change at
position 268. The UGT?B~(H'") was assigned as the wildtype allele since it was

discovered first, convenely, U G T ~ B ~ ( Y ~ ~ ' ) was assigneci as the variant form. In contrast
to the wildtype fonn, when the variant form was expressed in COS cells it had the ability
to glucuronidate menthol and androsterone (Jin et al., 1993a; Rina a al., 1990).
Therefore, by changing a tyrosine residue for a histidine residue at position 268, one
could alter the substrate specificity of UGT2B7.
In this laboratory, both U G T ~ B ~ ( H ~ ~ ' ) and UGT~B~(Y'~') were expreaed in
COS-1 cells (Patel 1998). Known substrates of UGT2B7 (oxazepam, ketoprofen, (S)-
naproxen, 2-OH-estriol, estriol, hyodeoxycholic acid) were then used to compare the
kinetic parameters of both the wildtype and variant forms. There were no differences in
the Km values of the various substrates tested. However, the wildtype form had
significantly higher Vmax values for oxazepam 2-OH-estriol, and estriol as compared to
the variant form. The wildtype form had a 2 fold higher efficiency for the glucuronidation
of both 2-OH-estriol, and estnol. More imponantly, however, was the fact that the
wildtype form was able to glucuronidate oxazepam 100 times more eficiently than the
variant form when expessed in COS-1 cells.
Recently, U G T ~ B ~ ( H ' ~ ~ ) and U G T ~ B ~ ( Y ' ~ ~ ) were stably expressed in HK 293
cells (Cofhan et al., 1998). The findings obtained by Coffman et al. (1998) have
contradiaed the findings of both Jin et al. (1993) and Patel(1998). The authors reported
that both U G T ~ B ~ ( H ' ~ ~ ) and UGT~B~(Y'") efficiently glucuronidated menthol and
androsterone. Furthemore, they were unable to fuid any significant differences in the
glucuronidation of oxazepam between the stably expressed and H ~ ~ ~ . They also
reported that both UGT2B7 alleles had the ability to glucuronidate either isomer (R or S)
of oxazepam. Moreover, they suggested that UGTZB7 might not be the major isozyme

responsible for the glucuronidation of oxrwpam. since oxazeparn was found to be a very
poor subarate for the stably expressed UGTZB7 enzymes. Differences in enzyme
concentration, substrate concentration, incubation conditions, as wcll as the use of
different expression systems could possibly explain the above discrepancies.
The authors however did report that the variant fonn had approximately 100-fold
higher activity towards nomorphine and naltriben as compared to the wildtype form of
UGT2B7. In addition, the variant also possessed a 10-fold higher efficiency towards the
glucuronidation of buprenorphine.
Glucuronidation of Drugs
Glucuronidation is a major rnetabolic pathway for the elimination of many drugs
in humans (Burchell and Coughtne, 1989; Miners and Mackenzie, 1991). Many drugs
are excreted in urine and bile as glucuronide conjugates. Ouazepam (Alvan et al., 1977),
morphine (Osborne et al.. 1990). chloramphenicol (Arnbrose, l984), and zomepirac
(OWeill et al., 1982) are examples in which glucuronidation is the predominate means by
which the compound is excreted from the body.
In the past, research in the metabolism of drugs and xenobiotics has been
primarily focused on the oxidative reactions catalyzed by the cytochromes P450.
Conversely, glucuronidation has received considerably l e s attention because the
metabolites of glucuronidation are generally considered to be pharmacologically inactive
(Mulder, 1992). Nevertheless, the phannacological significance of glucuronidation
should not be overlooked since glucuronidation has major effects on the disposition,
metabolism and excretion of many therapeutic agents.

Variability in Glucuroaidation
Large interindividual variations in glucuronidation have been observed in vivo
(Miners and Mackenzie. 199 1) and in vitro using hepatic microsornes (Burchell et al.
1989). Substantial variations in the pharmacoicinetics of a drug may suggest genetic
variations in dnig metabolizing enzyme(s) (Kalow, 1989). However, the variations seen
in glucuronidation may also be due to factors such as age. sex, diet, disease state, and
exposure to xenobiotics as wel! as genetic factors.
Due to the wide overlapping substrate specificity of UGTs, the invoivement of
other metaboiic pathways, and confounding pathophysiological and environmentai
factors, finding an adequate in vivo probe to snidy polymorphic variations in a pmicular
UGT isoform may seem to be a daunting task.
The candidate in vivo probe drug should be a safe therapeutic agent with minimal
side effects. Gtucuronidation should be its predominate means of elimination. The
particular isozyme(s) responsible for its metaboiism should be elucidated. Furthemore,
the population study itself should be large enou& as to account for any non-genetic
factors that may be influencing glucuronidation activity.
Ouzepam
Oxazepam is a 3-hydroxy- 1,4-benrodiazepine derivative. Oxazeparn is one of the
moa widely used dmgs in the world (Marks, 1980). It is mainly prescribed for its
anxiolytic properties, however it aiso possesses sedative, anticonvulsant, and muscle

relaxant effects. Oxazepam has a wide margin of d e t y ; the side effects associated with
its use results from a direct extension of its therapeutic property.
Oxazepam is the active metabolite of several 1.4-benzodiazepines including
diazepam, temazepam, chiorazepate. chlordiazepoxide, and medazeparn (Sisenwine et al.,
1982). These benzodiazepines undergo N-deaikylation and C3-hydroxylation via
microsomal cytochrome P450s to form oxazepam.
Oxazepam is completely absorbed fiom the G.I. tract after an oral dose (Alvan
and Odar-Cederlof, 1 978; Sonne et al., 1 988). Glucuronidation is the major metabolic
pathway for the elimination of oxazepam: greater than 85% of oxazeparn is excreted in
urine as a glucuronide conjugate (Alvan and Odar-Cederlof, 1978). Oxidative
metabolites of oxazepam have also been reponed (Grifin et al., 1995). The major
oxidative metabolite is 6-chloro4phenyl-2(l H)-quinazoline carboxylic acid (CPQ-
carboxylic acid). Only trace amounts of the original compound are excreted in urine.
Oxazepam is characterized as a low clearance dm& clearance values range from 0.42
ml/min/kg to 2.38 ml/min/kg (Alvan and Odar-Cederlof, 1978; Greenblatt and Shader,
1980). The elimination half-life of oxazepam ranges fiom 5 to 12 hours; this is relatively
short compared to the other benzodiazepines. Oxazepam is extensively bound to plasma
proteins. with greater than 90 % of it being bound to the protein.
Many pathophysiological and environmental factors are known to influence the
metabolism of oxazepam ( S o ~ e , 1993). The following is a review of some of these
factors (Table 2).

Table 2. The effect of pathophysiological and environmental factors on the glucuronidation of Oxazepam.
Factor
Liver Acute viral hcpatitis Compensateci alcoholic iivtr cirhosis Cornpexmed aicoholic liver cirrhosis Severe alcoholic iiver cirrhosis
CL uncbanged CL unchanged Eliminauon half-life unchangecl T O ~ a reduccd by 52% Unbound CL teducal by 84%
Shull et al. 1976 Shull et al. 1976 Seilers et al. 1979 SOM^ et al. 1990
7ïtyroid Hyperthyroidism Hypothyroidism Severe hypothyroidism
Incrcase in apparent oral CL CL unchangai CL n d u d
Scott et al. 1984 Scott et al. 1984 Sonne et al 1990b
CL unchanged Scott et al 1988
Abernethy et ai. 1986
CL unchangai CL negative trend Total CL uncbangtd unbound CL rcduccd by 55%
Greenblatt et al. 1980 Drerevfuss et al. 1986 Sonne et al. 199 1
Sex Greenblatt et al. 1980 Total & unbound CL > in men
Smoking Greenblatt et al. 1980 Ochs et al. 198 1
Very low in calories/Suaicient in protein Energy deficient Protein dcficient
Sonne et al. 1989 Hamôerg et al. 1990 Hamberg et al. 1990
Concomitant drug administration
Cimetidine Propranolol Labetalol Phenobaritailphcnytoin Oral contraceptive stcmids
Patwardhan et al. 1980 Sonne et al 1990C Sonne et al 1990c Scott et al. 1983 Patwardhan et al. 1983 Abernethy et al. 1983 Sellers et al. 1980 Sellers et al. 19ûû
CL unchangcd CL uncbanged CL inrreased CL inCrtascd CL uncbangcd CL unchangcd No dispositional changes
CL incmased SR ratio &mased dt(e to increase in R-giucuwnide
Seidenan et al. 198 1

Livtr Diseme
While oxidative functions are severely harnpered in liver disease, glucuronidation
processes seem to be preserved. The eiimination of oxazeparn is not significantly
different between patients with liver cirrhosis as compared to controls (Sellers et al.,
1979; Shull et al., 1976). Significant reductions in the glucuronidation of oxazepam have
been reported in patients with sevcre hepatic dysfunction (Sonne et al., 1990a). The
mechanism(s) of this apparent sparing of the glucuronidation of oxazepam is unknown.
One theory to explain this curious finding emphasizes the importance of extrahepatic
glucuronidation. In dogs, it has been observed that as hepatic functions decrease,
extrahepatic glucuronidation becomes more appreciable (Gerkens et al., 198 1; Jaqz et al.,
1986) or in fact increases parallel to the decreases in liver function (Patwardhan et al.,
198 1). Another theory suggeas that the deeper localization of UGTs within microsornes
may be a proteaive mechanisni against liver injuries (Gregus et al., 1982).
EIypothyroidismAyperthy roidism
The pharmacokinetic properties of oxazepam in patients with thyroid disease were
detedned (Scott a al., 1984). Patients with hypothyroidism exhibited normal
pharmacokinetics for the metabolism of oxazepam. Whereas, there was an increase in
the clearance and a decrease in the half-life of oxazepam in patients with hyperthyroidism
as compared to control subjects. Patients with severe hypothyroidism were reported to
have diminished oxazepam clearance (Sonne et al., 1990b). The above findings suggest
that the thyroid hormone may influence the regulation of the UGT(s) that metabolize
oxazepam.

Diabetes
When the elimination of oxazepam was compared in 6 patients with uncontrolled
diabetes with the values obtained two months later in these same individuals when the
disease was controlled, no signifiant differences were obsennd (Scott et al., 1988).
Obesity
Obese individuals were reported to have enhanced glucuronidation capacities
(Abemethy and Greenblatt, 1986). The total metabolic clearance of lorazepam.
oxazepam, and paracetamol were reported to be increased in individuals who were
considered to be obese (179% ideal body weight).
Age
Studies involving benzodiapines that undergo biotransforrnation via oxidation
have shown age-related declines in clearance (Allen et al., 1980; Greenblatt and Shader,
1980; Kloa et al., 1975). The effects o f aging on oxazepam pharmacokinetics on the
other hand are less defined. While some have reported that the biotransformation of
oxazepam were unaffected by age (Greenblatt a al., 1980; Ochs et ai., 198 l), a trend
towards reduced clearance was detected among five elderly patients (Dreyfuss et al.,
1986). More recently, it was observed that among the very elderly (mean age 88 years)
the unbound clearance of oxazepam was reduced by 55% (Sonne et al., 199 1). The
researchers demonsuated that the reduction in the unbound clearance of oxazepam was
attributed to low concentrations of plasma albumin. Since oxazepam is a highly bound
dm& it is believed that the significant changes in unbound drug that is observed in the

elderly, combined with a decrease in oxidative metabolism may explain the obsewation
that geriatric patients have increased sensitivity towards benzodiapines.
Scx
The metabolism of oxazepam was reponed to be different between males and
females (Greenblatt et al., 1980). The elimination half-life was longer in females (9.7
hours) than males (7.8 hours). Total clearance as well as unbound clearance was
significantly greater in males than in females.
Ditt
The effects of dietary energy, protein deficiency, nutritional ingredients and
malnutntional States may influence hepatic drus metabolism (Vesell, 1984). A change in
diet fiom a high protein-low carbohydrate to a low protein-high carbohydrate resulted in
an increase in the urinary recovery for oxazepam giucuronides. The effects of energy and
protein diets on the metabolism of oxazepam antipyrine and metronidazole were
investigated (Hamberg et al., 1990). Both the energy and protein deficient diets produced
a decline in the clearance rate and prolonged the half-life of oxazepam. The diets had no
appreciable effens on the oxidative pathways of diug metabolism as measured by
antipyrine and rnetronidazole. A diet low in calories and carbohydrates but suficient in
protein has been reported to produce a decrease in the clearance of oxazepam (Sonne et
al., 1989).

Dmgs
In clinical settings, benzodiazepines are oftcn prescribed with other medications.
As such, the possibility of dnig-dmg interactions exists. Concurrent administration of
dmgs may exert diserential effects on oxidative and conjugative drug metabolism.
Cimetidine, an anti peptic ulcer dmg has been shown ta be a strong inhibitor of p hase 1
drug metabolism (Desmond et al., 1980; Serlin et al., 1979). However, cimetidine has no
effect on the glucuronidation of oxazepam and lorazepam (Pawdhan et al., 1980). The
disposition and elimination of oxazepam and lorazepam did not differ in 4 subjects before
and after the treatment with cimetidine.
The effect of the P-adrenoceptor antagonists propranolol and labetalol on the
metabolism of oxazepam was investigated ( S o ~ e et al., 1990~). Both propranolol and
labetalol were reported not to influence the pharmacokinetics of oxazeparn. Interestingly
however, there was a pharrnacodynamic interaction between oxazepam and propranolol.
The glucuronidation of oxazepam in nine epiieptic patients who were being
treated with phenytoin alone or in combination with phenobarbitone was significantly
different as compared to nine healthy volunteers (Scott et al., 1983). The patients
exhibited an increase in the apparent oral clearance and a shoner half-life for the
elimination of oxazepam.
The studies regarding the influence of oral contraceptives on the metabolism of
oxazepam are confliaing. Women who were taking low-dose estrogen oral
contraceptives (50 pg or less ethinyl estradiol) for at least 3 months did not have
signi f icantl y di fferent total oxazepam clearances from dmg-free control w omen
(Abemethy et al.. 1983). On the other hand. women who had been taking oral

contraceptives (norethindrone acetate, h g ; ethinyl estradiol, 50 pg) for as Ieast 6 months
exhibited an increase in the plasma clearance of oxazepam as compared to m r o l s
(Patwardhan et al., 1983).
The effea of acute ethanol doses on the disposition of drugs in healthy subjects
was investigated (Sellers et al., 1980). The researchers reponed that ethanol inhibited the
N-desmethylation of diazepam but spared the glucuronidation of oxazepam. In the same
shidy, disulfiram, a drug used in the treatment of some forms of alcoholism was
administered to aicoholics and control subjects. Disulfiram was able to decrease the
plasma clearance of chlorazepoxide, a drus that is mainly eliminated by oxidation
reactions. Disulfram however had minimal effects on the elimination of oxazepam and
lorazepam, dnigs that mainly undergo glucuronidation.
Ethnicity
There are many examples of interethnic differences in drug metabolism (Kalow,
199 1). Aldehyde dehydrogenase, alcohol dehydrogenase, debrisoquine hydroxylase, and
N-acetyltransferase are some of the classical examples of interethnic differences in drug
metabolism. Interethnic differences in glucuronidation have been suggested but it has
not been conclusively proven.
The glucuronidation of paracetamol was reponed to be difierent benveen
Caucasians and Afncans (Critchley et al., 1986). The mean fractional recovery of the
glucuronides of paracetamol and its metabolites over a 24 hour penod was statistically
higher in Aûicans (58%) than in Caucasians (54%). Whether or not this represents a mie
ethnic difference in the glucuronidation of paracetamol has yet to be confïrmed.

The glucuronidation of codeine phosphate was investigated in t 49 Swedish
Caucasians and 133 Chinese (Yue et al., 1989). A greater proportion of codeine-6-
glucuronide was excreted in Caucasians (62%) than in Chinese subjects (44%) in an 8
hour period. The interpretation of interethnic differences in the glucuronidation of
codeine is difficult since codeine has many metabolites and these metabolites are from
multiple metabolic pathways.
The phannacokinetic and pharmacodynamic propenies of morphine were
compared between 8 Chinese and 8 Caucasians (Zhou et al., 1993). While the
metabolism of nomorphine was not significantly different between Caucasians and
Chinese subjects, the clearance of morphine was higher in Chinese individuals than in
Caucasians. The increase in the clearance of morphine was attributed to an increase in
glucuronidation activity. Pharmacodynamically, Caucasians displayed a greater
morphine-induced reduction in blood pressure as compared to Chinese subjects.
There have been no studies that investigated the interethnic differences in the
glucuronidation of oxazepam.
Enantioselective Glucuronidation
Many drugs are prescribed in racemic formulations. It is known that
stereochemical factors have important influences on both the disposition and therapeutic
effectiveness of a dmg (Caldwell et al., 1988; Drayer, 1988; Eichelbaum, 1988).
Oxazepam is clinically prescribed as a racemic mixture. The two enantiomers of
oxazeparn have been shown to be pharmacodynamically distinct molecules. The 3(S)
enantiomer is considered to be the pharmacologically active isomer because it has a

greater than 200-fold ability to displace the specific binding of '~-diaze~am as compared
to the 3(R) enantiomer (Corbella et al., 1973; Mohier et al., 1977). Conjugation with D-
glucuronic acid produces two diastereomeric conjugates which are both
pharrnacologically inactive (Greenblatt et al., 1983; Mascher et al., 1984; Ruelius et ai.,
1979).
In vivo and in vitro studies have demonstrated that enantioselective
glucuronidation occurs in humans. Benoxaprofen, ibuprofen, naproxen (El Mouelhi et
al., l987), E- 1 O-hydroxynortriptyline (Dahl-Puustinen et al., 1989a), mexiletine (Grech-
Belanger et al., 1986), and oxazepam (Patei et al.. 1995a; Seideman et al., 1981; Vree et
al., 1991) have al1 shown varying degrees of stereoselectivity. There seems to be no
preferential enantiomer configuration (R or S) in regards to the stereoselective nature of
glucuronidation. The degree of stereoselectivity ranges fiom 9.65 for mexiletine (Grech-
Belanger et al., 1986) to 1.14 for naproxen (El Mouelhi et al., 1987). There are species
differences in the stereoselective glucuronidation of oxazepam. In vivo, rhesus monkeys
had the lowest S R oxazepam glucuronide ratio (approximately 0.6) and man had the
highest ratio (approximately 3.5) (Sisenwine et al.. 1982).
Organ stereospecifictiy have also been observed in humans. Using microsornes
fiom the liver, only the (S) enantiomer of E-10-hydroxy nortryptiline was glucuronidated.
While, microsornai preparations fiom the duodenum only glucuronidated the (R)
enantiomer (Dahi-Puustinen et al., 1989b).

Rationait
A preliminary population study perfonned on 40 healthy volunteers demonstrated
that the S/R oxazepam glucuronide ratio (SR ratio) was bimodally distributed, with 10%
of the subjects possessing abnomialiy low S R ratios (Patel et ai., 1995a). Another study
involving 94 subjects confinned the bimodal distribution of the S/R ratio (Appanna,
1995). However, Appanna observed that 20% of the subjects had SR ratios below the
antirnode. One individual was discovered to have an S/R ratio below 1. It was believed
that this individual had an enhanced ability to glucuronidate the R- isomer of oxazepam.
Unfortunately, the urine volumes were not noted for any of the subjects. Thus, a
cornparison between the total amounts of R- and S- oxazeparn glucuronide excreted could
not be made.
A family study demonstrated that the SIR ratio was hentable (Appanna, 1995).
Furthemore, a cornpanson between the inter- and intra-individual variabiiity of the S/R
ratio resulted in an extremely high (rcc = 0.98) senetic component value (Kalow et al.,
1998). This high genetic component value alon3 with the fact that the ratio is heritable
suggests that the S/R ratio is under genetic control. The bimodal distribution of the S/R
ratio in the population in tum, is therefore indicative of a genetic variability in the
isozyme(s) that are responsible for the giucuronidation of the R- and S- enantiorners of
oxazepam.
In vitro studies conducted in this laboratory using human liver microsornes have
suggested that the glucuronidation of the S- and R- enantiomers are catalyzed by different
UGT isozymes (Patel et al., 1995b). Furthemore, an inhibition profile of S- oxazepam

glucuronidation implicated UGT2B7 as the isozyme responsible for the conjugation of
the S enantiomer.
A study of 37 human liver microsornes demonstrated that approximately 10% of
the livers displayed abnormally high Km values for the fonnation of (S) glucuronide
(Patel et al., 1995a). In contrast, the formation of (R) oxazepam glucuronide in the 37
livers tested was normally distributed. From the in vitro data, it was suggeaed that the
phenotypic variations seen in vivo is a reflection of a genetic defect of the isozyme
catalyzing S- oxazepam glucuronidation namely UGT2B7.
In 1993, Jin et al. isolated a novel UGT2B7 cDNA clone from a hgt 1 1 human
liver cDNA library. There was an amino acid difference between this clone and the
wildtype form of UGTZB7. When this variant fom of UGT2B7 was expressed in COS- 1
cells, it did not have the ability to glucuronidate oxazepam (Patel, 1998).
H ypo thesis
The observed phenotypic variations in SIR oxazepam glucuronide ratios are due
to a specific UGT2B7 gene alteration.

Objectives
Most of the studies to date have focused on the glucuronidation of oxazepam as a
whoie compound or as the S R ratio. Therefore, very little is known about the factor(s)
controlling the glucuronidation of the individual enantiomers of oxazepam. It has been
demonstrated that enzyme induction by pentobarbital may alter the stereoselectivity of
oxazepam glucuronidation (Seideman et ai., 198 1). Six healthy volunteers were given a
racemic dose of oxazepam prior and pon ten &y treatment with pentobarbital.
Following the treatment, oxazepam plasma clearance was increased by approximately
50% as compared to the clearance pnor to the pentobarbitol treatment. In addition, the
S/R ratio of oxazepam glucuronides was decreased. The decrease in the SIR ratio was
attributed to an increase in the glucuronidation of the R- enantiomer.
One of the objectives of this midy is to therefore determine if any environmental
andor pathophysiologicai factors such as age, sex, ethnicity, smoking, alcohol and oral
contraceptive use influences the glucuronidation of the individuai isomers of oxazepam,
and thereby affecting the SIR ratio.
The second objective of this midy is to develop a genomic genotyping assay that
has the ability to distinguish between the UGTZB7 wildtype and variant alleles. The
assay will then be used to determine the allelic fiequencies of the wildtype and variant
alleles within the population.
The third and last objective of this study is to detemine if there are any
associations between the SIR ratio and the particular genotypes ofUGTZB7.

METHODS AND MATERIALS

In Vivo Glucuronidation in Human Subiect~
Racemic oxazepam in an oral preparation (Sem@) was supplied by Wyeth
Phannaceuticals. Al1 other ingredients were of HPLC grade obtained fiom Caledon
Laboratories.
Subjects
Two hundred and three healthy volunteers between 15-69 years of age
participated in this study. Before participating in the study, each subject was required to
fil1 out a questionnaire as well as sign a consent fonn. Age, height, weight, race, sex,
alcohol, smoking, and drug taking histories were ascenained prior to the study (Table 3).
The subjects were asked to take 15 mg (R, S) oxazepam p.o. with a glass of water
pnor to sleeping. Ovemight unne (8 hours) sarnples were collected, and the total volume
of urine was noted. A 10 ml sample was stored for analysis at -20°C.
The urine sample was diluted (50 pl of urine to 1950 pl of diailled water). The
diluted sample was then injected (30 pl) using a WISP automated programmable injector
(Waters), the mobile phase was delivered via a Waters 650 Solvent Delivery System at
1 .O rnlhin, ont0 a 25 cm Cl 8 reverse-phase ODS column. The mobile phase consisted
of 19% acetonitnle, and 7.5% isopropyl aicohol in 0.3% phosphoric acid. Glucuronides
of 3(R)-and 3(S) oxazepam were detected using a Waters Programmable Multi-
wavelength Detector with the detection wavelength set at 230 m, and AUFS set at 0.01.
The extinction coefficient of oxazepam (in methanol) is 34.2 cm1-mM'- at 230 nm (Yang
et al. 1990). The detector was attached to a Shirnadzu C4 Chromatopac analyzer and the
recorder set ai an attenuation of 2 and a chart speed of 5 .O mm/min.

Table 3.
Characteristics of Subjects Mean
Total Subjects 203 Males 118 Fernales 85 Caucasians 133 Orientais 58 Birth Conrol Pill Users 24 Age (~eam) 15169 28.9 Alcohol (d rinkdweek) 0-25 3.28 Smoking (ciga rettesheek) 0-400 9.46 Coffeefïea (cupdday) 0-11 1.64 WeightRfeight (lbslich) 1.46-3.78 2.18

Data Analvsig
Statistical analyses were paformed witb the Statistical Package for Social
Sciences (SPSS), release 8.0. The dependent variables were S-oxazepamlR-oxazeparn
ratio, amount of S- or R-oxazeparn glucuronide in eight-hour urine. The staîistical
significance of potential CO-variates (age, alcohol and caffeine consurnption, body size,
ethnicity, gender, oral contraceptive use and smoking habits) was tested with use of non-
parametric tests including the Mann-Whitney Lr test, Kolmogorov and Smirnov test,
Wilcoxon rank sum test, Chi-square test, and Spearman tank order correlations. The
subjects with Chinese, Japanese and Korean erhnic background were grouped together
and entered as a single factor (CO-variate) in the analyses. The statistical significance
level accepted for al1 statistical analyses was a = 0.05. Al1 data were presented as mean k
SD, unless otherwise stated.

DNA Extraction fiom Tissue
Genomic DN A fkom human post-mofiern liver tissues was isolated according to
the Stratagene DNA Extraaion Kit.
A small portion of liver tissue samples fiom the -70°C fkeezer was cut out and
weighed. The samples were then homogenized in a solution containing 0.32 M sucrose,
10 rnM Tris-HC1 (pH 7.5). 5 m M MgCl?, 1% Triton X-100,0.02% sodium azide (1 5 ml
of the solution to 250 mg of tissue). The sarnples were homogenized using a Brinkman
Polytron homogenizer (setting 5) for 30 seconds. Pronase (1 mg/ml) was added to the
homogenate, and the solution was then incubated for 3 houn in a shaking water bath at
5S°C, then chilled on ice for 10 minutes. 6 M sanirated NaCl solution (5 ml) was added,
and the solution was mixed by inverting the tube several times. The sample was
incubated on ice for 5 minutes. Following a centrifugation at 12,000 x g in a Sorvall
RC2-B centrifuge for 15 minutes at 4"C, a protein pellet could be visualized. The
supernatant was transferred with a sterile large bore pipette to a sterile 50 ml conical tube
(Falcon). RNAase (GibcoIBRL) was added to the supematant to yield a final
concentration of 20 &ml. The solution was then incubated at 37°C for 15 minutes. 10
ml of saturated phenol (Sigma) was added, the sample was centnfùged at 12,000 x g for 5
minutes at 4OC. The upper aqueous layer was recovered. The DNA was precipitated
with the addition of 2 volumes of 100% ethanol to the supernatant. The sample was
cmtrifbged at 12,000 x g for 10 minutes at 4OC. ï h e supematant was decanted off, and
the DNA pellet was washed with 1 ml of 70% ice-cold ethanol. The soiution was spun at
12,000 x g for 5 minutes at 4OC. The ethanol was decanted off, and the pellet was air-

dried for 10 minutes. The DNA was resuspended in 500 pi of Tns-EDTA buffer (10 mM
Tris, 0.1 rnM EDTA) and stored at 4'C until needed.
PCR h~iif icat ion of UGT2B7 fiom Genomic DNA
Two oligonucleotide primers, Pr (5'-TGACATGAAGAAGTGGGATC-3') and P6
(5'-TCAACATTTGGTAAGAGTGG-3'1, which were complementary to bases -68 1 to
700, and 824 to 805 of the UGT2B7 coding region, nspectively were used to perfonn
PCR reactions on genornic DNA extracted from liver tissue samples.
The PCR reactions contained: 0.5 pM of P? and Ps primers, -1 pg of genomic
DNA 100 @î of each dNTPs, 1.5 rnM MgC12, 2.5 units of Platinum Taq DNA
polymerase (Gibco/BRL) in 1 X reaction buffer (20 mM Tns-HCI (pH 8.4), 50 rnM KCI).
The PCR conditions were: an initial denaturation of 94OC for 3 minutes, 25 cycles
of 1 minute denaturation at 94°C. 1 minute and 30 seconds annealing at 57OC, 1 minute
and 30 seconds extension at 72OC, and a fina1 extension of IO minutes at 72°C. The PCR
was perfonned on a Gene Amp PCR System 2400 Thermal Cycler (Perkin-Elmer). 10 pl
of the amplification product was loaded in a 1% standard agarose gel (GibcofBRL)
containing 0.0 1% ethydium bromide and electrophoresed for l hour at 90 volts. The PCR
fiagrnent was visualized using a LiV transillulimator.
RNA Extraction
Human liver total RNA was isolated âom post-mortem samples. The liver tissue
samples were obtained fiom renal transplant donors with the consent of the next-of-kin,
and stored at -70°C. RNA was isolated according to the TRhlB Reagent (GibcoIBRL)
protocol.

Liver samples were taken from the -70°C freezer, and a small portion was cut out
and weighed. The sample was then homogmized in l'Rh01 (100 mg of liver tissue per 1
ml of TRkol) using a Brinkman polytton homogenizer (setting 5) for 30 seconds. A 5
minute incubation at room temperature (15-30°C) following the homogenization
permitted the complete dissociation of the nucleoprotein complexes. Chlorofonn was
then added (0.2 ml of chloroform per 1 ml of m o l ) and the samples were shaken
vigorously for 15 seconds by hand. After incubating the samples at room temperature for
3 minutes, the samples were then centrifuged at 12,000 x g in a Sorvall RC2-B centrifuge
for 15 minutes at 4OC. Following centrifugation the mixture separated into a lower red,
phenol-chloroform phase, an interphase. and a colorless upper aqueous phase. The upper
aqueous layer, which contained the RNA was carefilly removed using a I ml eppendorf
pipettor, and transferred to a fresh tube.
The RNA was then precipitated with isopropyl alcohol (0.5 ml of isopropyl
alcohol per 1 ml of TIUzol Reagent). The samples were then incubated at room
temperature for 10 minutes and centrifuged at 12.000 x g for 10 minutes at 4OC. An
RNA gel-like pellet at the bottom of the tube was visualized after the centrifugation
process. The supernatant was carefully decanted off. and the RNA pellet was washed
with ice-cold 75% ethanol in DEPC-treated water (1 ml of 75% ethanol per t ml of
-01 reagent). The samples were then vonexed for 10 seconds using a Fisher Vortex
Genie 2 and subsequently centrifuged at 7,500 x 8 for 5 minutes at 4OC. The supematam
was then decanted off, and the RNA pellet was air-dried for 10 minutes. The pellet was
redissolved in DEPC-treated H20, and the optical density was measured at 260 and 280

nm on a Beckman Du@-7 Spectrophtometer to determine the extraction efficiency and
the total RNA concentration.
Gel electrophoresis was perfonned on 1% agarose gel with 1-2 pg of total RNA
to check integrity of the RNA through the assessrnent of the 18s and 28s ribosomal RNA
bands. The individual RNA samples were then aored at -70°C until needed.
First-Strand Svnthesis of cDN A
Fust-strand cDNA was synthesized from human liver total RNA using reverse-
transcriptase M-MuLV (Boehringer-Mannheim). In a PCR tube (Perkin-Elmer), total
RNA (1-2 pg) was diluted ia DEPC-treated RNase-fiee HtO to a final volume of 8 pl, and
incubated at 6S°C for 10 minutes followed by a 5 minute incubation at 4OC. 32 ~1 of a
"master-mix" was then added to the PCR tube. The final reverse-transcriptase mixture
contained the following components: 1-2 pg of RNA, 1 m M of each dNTP, 20 units
RNase inhibitor, 140 pmol pN6 (randorn hexamer) or 200 pmol Oligo-dT, and 20 units of
M-MuLV reverse-transcriptase in 1X RT buffer (50 rnM Tris-HC1 (pH 8.3), 50 rnM KCI,
4 mM MgC12, 10 pM DTT). The mixture was incubated at room temperature for 10
minutes, and then at 3 7 T for Lhour. Samples were then stored at -70°C.
PCR Am~l i f i~a t i~n of Actin cDNA
The RNA from post-mortem tissue is ofien highly degraded, and rnay not yield
fust-strand cDNA of sufficient quality for PCR. Amplification of a 300 bp segment o f
Actin, a protein with ubiquitous expression, was used to assess the success of fist-strand
synthesis described above.
The 100 @ PCR teaction mixiure contained the foilowing: 10 pi of the reverse-
transcriptase reaction, 1.0 pM each of the forward and backward actin-specific

oligonucleotide primers, 1.0 m M Mgch. 2.5 units of Taq DNA polymerase (GibcolBRL)
in 1 X reaction buffer (20 rnM Tris-HCl (pH 8.4), 50 m M KCl). The PCR conditions
were: an initial denaturation of 94°C for 3 minutes, 30 cycles of 45 seconds denaturation
at 94°C. 30 seconds annealing at 53OC. 1 minute extension at 72OC, and a final extension
of 10 minutes at 72OC. The PCR was pdonned on a Gene Amp PCR System 2400
Thermal Cycler (Perkin-Elmer). 10 pl of the amplification produa was loaded in a 1%
standard agarose gel (Gibco/BRL) containing 0.0 1% ethydium bromide and
electrophoresed for 1 hour at 90 volts. The PCR âagment was visualized using a W
transillulimator.
PCR am~lification of UGT2B7 cDNA
Due to the degradation of the RNA, amplification of the fill-length coding region
of UGT2B7 was unsuccessful. Therefore, 2 sets of primers which produced PCR
fragments overlapping by 144 bp were used to ampli@ the entire coding region (see
Figure 2.). The first fiagment was amplified using the fonvard primer Pa (5'-
TGCATTGCACCAGGATGTC-3') and the backward primer P h (5'-
TCAACATTTGGTAAGAGTGG'), which were complementary to bases -14 to 5, and
824 to 805 of the UGT2B7 coding region. respdvely. The second fiagment was
am pli fied using the foward primer Ps (5'-TGAC ATGAAGAAGTGGGATC-3') and the
backward primer Pq (5'-AACTGAAGTAGTCTCACC-3'), which were complementary to
bases 681 to 700, and 1642 to 1625, respectively. The overlapping fiagment was also
amplified using the forward P, and backward Ps pnmers. The primers were designed to
minimize cross-hybridization with the cDNA of homologous UGT isozymes.

Each PCR reaction was 100 pl and contained 10 @ of the reversetranscriptase
reaction, 1 .O pM each of the fonvard and backard UGT2B7-specific oligonucleotide
primers, 1 .O rnM MgCI1 2.5 units of Taq DNA polymerase (Gibco/BRL) in 1X reaction
buffer (20 rnM Tris-HCI (pH 8.4), 50 mM K I ) . This mixture was preheated at 94°C for
3 minutes, followed by 30 cycles of 45 seconds denaturation at 94"C, 30 seconds
anneahg at 53OC, 1 minute extension at 72OC. and a final extension of 10 minutes at
72OC. A 10 pl aliquot of each amplification was loaded onto a 1 .û% agarose gel
containing 0.01% ethydium bromide. The sizes of the fragments were then determined
by using either a 100 bp marker andor a 1 Kb marker (MBI Fermentas) as the standard
markers.

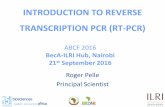
Figure 2. Schcmatic of RNA isolation, first-sûand sycthcsis. and subscqucnt PCR amplincation of UGT2B7 cDNA
RNA Isolation
5 ' * poly A tail UGT2B7 mRNA
7 9 - OR
Random Hexamer
I Reverse Transcription
cDNA of UGT2B7 -
PCR amplincation with UGT2B7-specific priniers

Gel Extraction of PCR Products
The QIAquick Gel Extraction Kit Protocol (QIAGEN) is designed to extract and
purifi DNA from agarose gels. 50 NI of the PCR product was loaded ont0 a 1% agarose
gel containing 0.01% ethydiurn bromide and electrophoresed for 2 hours at 60 Volts. The
DNA fragment was excised from the agarose gel with a clean, sharp scalpel. The gel
slice was placed in a 1.5 ml microfuge tube and weighed. Buffer QX1 was added (3
volumes of Buffer QX1 to 1 volume of gel). The sample was incubated at 50°C for 10
minutes. 1 gel volume of isopropyl alcohol was added to the sarnple, and the solution
was vortexed. A QIAquick spin column was placed in a provided 2 ml collection tube.
To bind the DNA to the column, the sample was applied to the QIAquick column,
and centrifuged at 10,000 x g for 1 minute. The flow-through was discarded. and 0.5 ml
of Buffer QX1 was added to the column and centrifuged at 10,000 x g for 1 minute. The
sample was washed with the addition of 0.75 ml of Buffer PE to the QIAquick column.
The column was centrifuged at 10.000 x p for lminute. The flow-through was discarded
and the column was centrifuged for an additional minute at 10,000 x g. The QIAquick
column was placed into a clean 1.5-ml microfuge tube.
The DNA was eluted by the addition of 50 pl of 10 rnM Tris-HCI (pH 8.5), and
centrifugation at 10,000 x g for 1 minute. The DNA sample was stored at -20°C until
needed.
Subclonin~ and Transformation of Gel Extraaed PCR Produas
The gel extracted PCR products were insened into the plasmid vector pCR02.1-
TOPO (Invitrogen). Taq DNA polymerase has a nontemplate-dependent terminal
transferase activity which adds a single deoxyaâenosine (A) to the 3' ends of the PCR

products. The linearized plamid vector pCR02.1 -TOPO has single, overhanging 3'
deoxythymidine (T) residues (Figure 3). The overhangs allow the PCR insen to be
ligated by topoisornerase to the linearized veaor.
Subcloning and transformation was perforrned according to the T O P O - C ~ O ~ ~ ~ ~ ~ ~
protocol (Invitrogen). In a 1.5-ml microfuge tube, 2 @ of the gel extracted PCR produa
was added to 2 @ of sterile water and 1 of pCRB2.1-TOPO vector. The solution was
gently mixed and then incubated at room temperature (-2S°C) for 5 minutes. The
mixture was briefly centrifùged and placed on ice.
A vial of One s hotTM cornpetent ceils (TOPO 10 strain of E. coli) was thawed on
ice. 2 pl of 0.5 M P-mercaptoethanol was added to the via1 of competent ceils and mixed
by gently stimng with the pipette tip. 2pl of the cloning reaction was added to the vial of
One shotm cells and mixed gently. The solution was incubated on ice for 30 minutes.
The cells were then heat shocked for 30 seconds at 42OC. The via1 was imrnediately
placed on ice and incubated for 2 minutes. 250 VI of room temperature SOC medium
was added to the vial. The tube was then capped tightly and placed in a G24
Enviromental Incubator Shaker (New Brunswick Scientific Co. hc.) and shaken at 225
rpm for 30 minutes at 37OC. The vial was then placed on ice. LB agar plates containing
50 Mm1 ampicillin (Sigma) were prewarmed at 37°C for 30 minutes. 40 pl of 40 mg/ml
X-gal (GibcoA3R.L) was spread on the plates. The transformation reaction (50 pl and 200
pl) was then spread on the LB agar plates and incubated ovemight at 37OC. The strain of
E. coli used in this protocol allowed for bludwhite screening without the addition of
PTG. M e t an ovemight incubation, there were hundreds of colonies. Individual white

colonies (16 colonies) were picked streaiced on LB plates containing 50 pi/rnl ampicillin.
and culnired overnight in 3 ml of LB medium containing 50 flml ampicillin.
Figure 3.
Vector map of plasniid pCR 932.1-TOPO
EcoRi
M 13 Reverse Primer l t
EcoRI
l t M 13 Fonvard Primer

Mini~rep of Plamid DNA
The bacteria were harvested by pouring 1.5 ml of the culture into a microfùge
tube and centrifuged in a Biofûge A centrifuge (Canlab) at 12,000 x g for 1 minute. The
remainder of the culture was stored at 4OC. The medium was removed by aspiration,
leaving the bacterial pellet as dry as possible.
The rniniprep protocol was obtained from Miniatias (1990). The bacterial pellet
was resuspended in 100 pl of icetold Solution I(50 m M glucose, 25 mM T r i s 4 (pH
&O), 10 rnM EDTA (pH 8.0)) by vigorous vortexing. 200 pl of Solution II ( 0.2 N
NaOH, 1% SDS) was added and the solution was mixed by inverting the tube rapidly five
times. 150 pi of ice-cold Solution ID ( 3 M potassium, 5 M acetate) was added, and the
solution was vortexed for 10 seconds. The solution was stored on ice for 5 minutes.
Mer a centrifugation at 12.000 x g for 5 minutes at 4OC, the supernatant was caretiilly
transferred to a fiesh tube.
The double-stranded DNA was precipitated with the addition of 2 volumes of
ethanol at room temperature. The tube was then vonexed, and centrifuged at 12,000 x g
for 5 minutes at 4OC. The supematant was carefully removed by aspiration. The DNA
pellet was rinsed with 1 ml of ice-cold 70% ethanol. The tube was then centrifuged at
12,000 x g for 5 min at 4OC. The supematant was removed and the pellet air-dried for 1 O
minutes. The DNA was redissolved in 50 pl of TE (pH 8.0) containing 10 pg/ml
RNAase (GibcoiSRL). The DNA was stored at -20°C.
Analvsis of Plasmid DNA bv Restriction Analvsis
To CO* tht the transformed cells contained the insert of interest, the DNA
isolated previously, were subjected to restriction analysis. The restriction reaction

contained: 5 pl of the isolated D N 4 5 units of EcoRI (Gibco/BRL), in 1 X REA& 3
Bufier. The restriction reaction (10 pl) was loaded in a 1 % agarose gel containing 0.01
% ethydium bromide and electrophoresed for 1 hour at 90 Volts.
Seauenci na Reaction
The sequencing protocol used is described in the m~equencingTM Kit (Phannacia
Biotech). 1.5-2.0 pg of miniprep DNA was diluted in Hz0 to a final volume of 32 pl.
The double-stranded template was denatured by the addition of 8 pl of 2 N NaOH. The
tube was vonexed gently, and centrifuged briefly, then incubated at room temperature for
10 minutes. 7 pl of 3 M sodium acetate (pH 4.8) and 4 pi of H20 was added. The DNA
was precipitated by the addition of 120 ~1 of 100% ethanol. The solution was mixed and
placed on dry ice for 15 minutes. The precipitated DNA was collected by centrifugation
at 12,000 x g for 15 minutes at 4°C. The supernatant was carefully removed and
discmded. The pellet was washed with 70% ethanol. The sample was recentrifuged for
10 minutes. After the ethanol was removed, the pellet was dried, and the DNA was
redissolved in 10 pi of dinilled water.
The annealing reaction consisted of 10 pl of template DN& 2 pl of 5 pM of
Primer; either P7 or SP6 (refer to the vector map) and 2 p1 ofthe annealing buffer (1 M
Tris-HCl (pH 7.6), lOOmM MgC12 and 160 mM DTT). The sample was vonexed,
centrifuged bnefly, and incubated at 65OC for 5 minutes. The tube was quickly
transferred to a 37OC water bath and incubated for minutes. The sample was placed at
room temperature for 5 minutes, then centrifuged briefly.
The labelling reaction immediately followed the annealing reaction. The reaction
consisted of the following: 14 pl of the annealecl templatdpnmer reaction, 3 pl of the

Labelling Mix A ( 1.38 each dCTP, dGTP. and d m and 333,5 rnM NaCl), 1 pl ( 10
pCu) of labelled dNTP ( [ 3sa~ ] dATPa fmm MNm Life Science Produas hc.) and 2
pl of diluted Ti DNA polymerase. The components were mixed, and then incubated at
room temperatun for 5 minutes.
Mer the labelling reaction, 4.5 pi of the reaction was transferred into each of the
four pre-wmed sequencing mixes ("A", "C", "G", and "T" Mix-Short). The reaction
was then incubated at 37OC for 5 minutes. Mer the 5 minute incubation, 5 pl of the stop
solution was added to each tube.
The samples were heated at 75-80°C for 2 minutes and then immediately loaded
into the appropriate well of a 6% sequencing gel. The temainder of the sample was
stored at -20°C.
The sequencing gel was run at 80 Watts on a Mode1 S2 Sequencer (GibcoBRL)
for 3 hours. The gel was fixed ont0 fiiter paper, then dried for 1 hour and 15 minutes
under vacuum in a Mode 583 Gel Dryer (Bio-Rad) set at 80°C.
The Gel was exposed to BIOMAX~~MR Xray film (Kodak) ovemight at room
temperature. The autoradiograph was developed. and the sequence of the DNA was read.
Several samples were also sent to be sequenced automatedly at the Sequencing
Center located at the Hospital for Sick Children (Toronto, Ontario, Canada).
Allek-S~ecific Amdification (ASA)
PCR is a method that utilizes oligonucleotide primers to ampli@ a segment of
DNA more than a million-fold. Allele-specific amplification (ASA) is an adaptation of
PCK which can rapidly detect single base pair changes in DNA ASA relies on a single
base pair substitution at the 3' end of a primer. The substitution causes a Msmatch

between the primer and template D N 4 preventing the efficient 3' elongation by Taq
polymerase. This mismatch between pnmer and template at the 3' causes poor or no
amplification of a PCR produa Thus, by designing an extension primer with a 3' end
Iocated on the mutation site, it is possible to distinguish one allele over another.
Two separate PCR reactions were used for the allele-specific proiocol (Figure 4.).
To eliminate false negatives, the amplification of a 422 bp segment of the Hurnan growth
hormone gene (HGH) was used as an intemal control. The first reaction (wild-type
reaction) contained: O. 5 ph4 forward HGH primer (5'-TTCCCAACCATTCCCTTA-31,
O. 5 pm backward primer (5'-GGATmCTGTTGTGTmC-3'), 0.5 phi P3 pnmer (5'-
TGACATGAAGAAGTGGGATC-3'), 0.5 pi%f Wild-type primer (5'-
ATTTGGTAAGAGTGGATG-3'), -1 pg of genomic DNA 100 pM of each dNTPs, 1.5
mM Mgch, 2.5 units of Platinum Taq DNA polyrnerase (Gibco/BRL) in LX reaction
buffer (20 rnM Tris-HC1 (pH 8.4), 50 mM K I ) . In a separate tube, the variant reaction
contained the above components, but. the Variant primer (5'-
ATTTGGTMGAGTGGATA-3') for the Wild-type primer.
The PCR conditions were: an initial denaturation of 94°C for 3 minutes, 25 cycles
of 1 minute denaturation at 94T, 1 minute and 30 seconds annealing at 57"C, 1 minute
and 30 seconds extension at 72"C, and a final extension of 10 minutes at 72°C. The PCR
was performeâ on a Gene Amp PCR Syaem 2400 Thermal Cycler (Perkin-Elmer). 10 pl
of the arnplification product was loaded in a 1% standard agarose gel (Gibco/BRL)
containing 0.01% ethydium bromide and electrophoresed for 1 hour at 90 volts. The PCR
âagment was visualized using a W transilluminator.


1 A Sim~le M o u t h w a s h A
8 subjects were chosm to condua phenotype-genotype correlation comparisons.
Of the 8 individuals chosen, 3 were phenotypeâ as having atypical SR ratios (< 1.66).
The remaining 5 subjects had normal phenomes. The characteristics of the 8 individuals
used in this study are in Appendix 6.
Genornic DNA from these individuals was collected using a recently developed
method (Lum and Merchand. 1998). The method involves using mouthwash (FreshBurst
Listerine) to collect the genornic DNA of buccal cells. 10 ml of undiluted Listerine was
given to the subjects approximately 1 hr after they brushed their teeth. The subjects were
told to swish the mouthwash vigomusly throughout the mouth for 1 min. The samples
were then collected and transferred to a 50-1111 conical tube for centrinigation at 2700 rpm
for 15 minutes. The supematant was decanted, and the pellet was washed in 25 ml of TE
bufier [10 mM Tris (pH 8.0), 10 rnM EDTA (pH 8.0)]. The suspension was centrifûged
at 2700 rpm for 15 minutes, and the supernatant was discarded. The pellet was
resuspended in 700 p1 of lysis buffer [10 mM Tris (pH 8.Q 10 m . EDTA (pH &O), 0.1
M NaCI, and 2% SDS] and transferred to a 2-ml microcentrifige tube containing 3 5 pl of
20 mg/rnl proteinase K. The samples were mixed and digeaed at 58 OC for 2 hours. The
DNA was then extracted f?om each sample with eqwl volumes of phenoCchloroform
(1 : 1) and with an equal volume of chloroform alone, each time vortexing for 10 seconds
and centrifùging at 14,000 rpm for 2 minutes. The DNA was removed from the
supematant with 3 M NaOAc (pH 6.0; 1/10 volume of supematant) and 2 volumes of
cold 100% ethano1 and precipitated at -20 O C for 2 hours. The DNA was pelleted at
10,000 rpm for 10 minutes, washed with 70Y0 ethanol, and air-dried for 10 minutes. The

pellet was resuspended in 100 pl of TE, and the concentration of the DNA was calculated
on a Bedonan Du@-7 Spectrophtometer. The DNA samples were then subjected to ASA
genotyping following the protocols described above.


Interindividual variabüity in SIR ouzepam giucuroiiide ratio (S/R ratio)
A histogram of the results demonstrates that the data is bimodally distributed
(Figure 5). Furt hermore. pro b it (Bli ss, 1 93 4) and NTV (Endrenyi and Patel. 1 99 1 )
analyses of the log-transformed ratios demonmated that approximately 18 % of the
popuiation have S/R ratios below an apparent antimode of 1.66. herestingl y, 2 out of
the 203 individuals had extremely low SR ratios.
Factors that influence the S/R ratio
The S/R ratio amonp 203 healthy volunteers varies from 0.45 to 9.07. The mean
S/R ratio was 3.06 with a standard deviation of 1.14 (Table 4). Note that the S / R ratios of
94 subjects were obtained from Appanna (1995).
The 133 Caucasians in this study seemed to possess a higher mean S R ratio
(3.10k1.62) than the 58 Orientais (2.9511.00). However, this difference was not
statistically significant (p>O.OS). The percentase of individuals below the population
antimode also differed between the two racial groups. Among the Caucasian population
21% of individuals had S/R ratios below 1.66, while only 14% of individuals in the
Oriental population had S/R ratios below the antimode. A chi-square test however
demonstrated that this difference was not statiaically significant (p= 0.28).
When the metabolism of oxazepam was cornpared between male (n= 118) and
female (n= 85) subjects, a statistical difference was observed (pC0.05). In general, male
subjects have higher S/R ratios (3.22k1.49) than females subjects (2.82I1.32).
Furthemore, the percentage of individuals with atypical phenotypes (S/R ratio below

1.66) in the male population (13%) was also statistically different f5om the female
population (26%).
When the female subjects were demarcated by oral contraceptive use, females
who were taking oral contraceptives had mon variation and higher S/R ratios (3.13f 1.46)
than women who were not taking oral contraceptives (2.72Il.22). This difference was
not statistically significant.
Speannan's rank correlations were perfomed between the S/R ratio and potential
co-variates; age, body sire, caffeine consumption, ethanol use, and smoking habits (Table
5). Of the above factors mentione4 body size was the only variable that was
significantly correlated to the S/R ratio (rs= 0.28. p<O.OO 1).

Figura 5. Distribution of log SIR oxazepam glucuronide ratio (SIR ratio) in 203 volunteers. The SIR ratios of 94 subjects were obtained from Appana (1 995). The arrows represent the location of the antimode as detemined by N l V analyses.
Log SIR Ratio

Table 4. Summary table for the SIR oxazepam glucuronide ratio (SIR ratio) in 203 healthy volunteeo.
Total Populrtioa
Caucuirn Oriental
Female P"" I Noa Oral Contraceptive users Oral Contnceptive uscn
I Caucasian Male Oriental Male
I Caucosian Femrile Oriental Female
Mann-Whitney U-test, p* 0.05 " Chi-Square test, p< 0.05
O/. BELOW ANTIMODE
18
2 1 12
9 25
./. BELOW POP. AlVTIMODE
-Note that the S/R ratios of 94 subjects were taken from Appana (1995)

Table S. Non-parametnc cornlation analyses for S/R oxazepam glucuronide ratio, amount of Ssxaxepam glucuronide. and amount of R-glucuronide versus age. body size, caffeine, ethanol, and smoking.
Ase
Body Size (IbTinc h)
Caffeine (CU pdday )
E thanol (glass/w k)
, Smoking (cighk)
S/R ratio
Spearman's pvalue
O. 10
Amouat of S-giuc. (n- 1
Spearman's r. pvalue
0.38
0.02
O. 74
0.07
0.83
Spearman's ra
-0.1 1

AmounLi of S and R-oxazepam glucuronida ucreteâ in 8 eight-hour urine samples and the S/R ratio
The S/R ratio was significantly correlated to the amounts of both S- and R-
oxazeparn glucuronide excreted (Figure 6 4 6B). A strong positive correlation with a
spearman's rank coefficient of 0.63 was observed between the amount of S- oxazepam
glucuronide excreted and the SIR ratio (p<O.OOI). In contrast, the amount of R-
oxazepam glucuronide excreted over an 8-hou period was negatively correlated (rs= - 0.29) to the S/R ratio (p<O.OS).
When the amount of S- oxazeparn glucuronide was plotted against the amount of
R- oxazepam glucuronide (Figure 6C), a statiaically significant correlation was observed

Figure 6. Correlation analysis between the log SIR ratio and the log amounts of S and R oxazepam glucuronide excreted in an 8 hour period (A,B). Correlation between log amount of S and R oxazepam glucuronide (C). (n= 11 5)
-0.50 0.00 0.30 1 .O0
Log SR Ratio
- .
0.00 0.30
Log S;R Ratio

Facton that influence the amount of R- oxazepam giucuronide escretcd
There was no difference in the amount of R- oxazepam glucuronide excreted in 8-
hour urine samples between 29 Oriental (1 46H2) and 79 Caucasian (1 57k68) subjects
(Table 6A).
The metabolisrn of R- oxazepam was also not statistically significant b e ~ e e n
male (n= 73) and female (n= 42) subjects. hterestingly, when oral contraceptive users
were removed from the female group, the amount of R-oxazepam glucuronide excreted
by males (156k65) was significantly higher (pc0.05) than by females who were not
taking oral contraceptives (1 24H2).
Oral contraceptive users excreted significantly (pC0.05) more R- oxazepam
glucuronide (198B4) than females who were not taking oral contraceptives (124k42).
Neither age, body size, caffeine, ethanol. or smoking had any significant effects
on the amount of R- oxazepam glucuronide excreted (Table 5).
Facton that influence the amount of S oxazcpiim glucuronide excreted
The glucuronidation of S-oxazepam was not different between Caucasians and
Orientals (p>O.OS). However, Caucasians tended to excrete more S-oxazepam
glucuronide (437G20) than Orientais (4 1 1flO3).
The glucuronidation of S-oxazepam was not different between the male and
female subjects of this snidy (Table 68). But, males generally excrete more S-oxazeparn
glucuronide (#8*l9 1) than females (399I246).
Similar to the results of R- oxazepam, the glucuronidation of S- oxazepam was
statistically different between non-oral contraceptive users and oral contraceptive users

(p<O.OS). Females who were taking oral contraceptives excreted much higher amounts of
S- oxazepam glucuronide (546B8 1) than women who were not taking oral
contraceptives (325k193).
Fwthemore, when oral contraceptive users were nmoved from the female
population, a statistical difference @<0.05) was observed between males (4481 19 1) and
female subjects who were not taking ord contraceptives (325k193) in regards to the
glucuronidation of S-oxazeparn.
Body size was significantly correlated (p<O. OS) with the rnetabolism of S-
oxazepam (rr= 0.23). In contras& age, caffeine. ethanol, or smoking was shown not to
influence the glucuronidation of S- oxazepam (Table5).

Table 6. Cornparison of the variation in the amount of R-,S -oxazepam glucuronides, and SIR ratio excreted in an 8 hour period (A,B,C).
A. Amount of (R)-axazepam glucumnidc @ea& keight~oîume cdfecteQ
1 1 MEAN 1 STDEV 1 CV% Oriental (n= 29)
Caucasian (n= 79)
Male (n= 73)
Female (n= 42)
Non OC Users (n=2%)
Orien ta1 (n= 29)
Caucasian (n= 79)
Male (n= 73)
Female (n= 42)
Non OC Users (n=28) OC Usem (1144)
Amount of (S)-epam glucuronidr @e& height *volume coüected)
STDEV
*, (-) Mann-Whitney U-test, p< 0.05
SR aazepam glucuronide rutb in an 8 hour urine sample.
1 MEAN 1 STDEV
Onen ta1 (n=29)
Caucasian (n-79)
Male (n=73)
Femde (n=42)
Non OC Usen (n= 28) 1 2.65 1 1.26

Genomic Sequeace of UGT2B7
Previous sequences of UGT~B~(H~'*) and UGT~B~(Y'~*) were obtained h m
either cDNA clones Grom human cDNA libraries or messenger RNA fiom human tissue
amples. Here, we report the f i s t genomic sequence of the variant UGTZB7 allele
(UGT~B 7 ( ~ 268)).
Two primen, P5 and P6 which amplie a 144 base pau fragment of the UGT2B7
coding region encompassing the 802 mutation site were used in a PCR reaction on
genomic DNA. The PCR amplification produced 2 produas (Figure 7B). The lengths of
the Fragments were approximately 1.4 Kb and 1.6 Kb, respectively. The 1.6 Kb Fragment
is believed to be UGT2B4. The difference in site of these produas amplified from
mRNA (144 bp) and h m genomic DNA (1.4 Kb) suggests the existence of an intron in
this portion of the coding region.
Sequence analyses of the 1.4 Kb fragment revealed an introdexon splice site 105
base pairs away fiom the 3' end of the PCR fiagment (Figure 7A). Furthermore, the
sequence of the fragment matched that of the UGTZB7 variant allele with 2 additional
mutations (a T+A mutation and a G+A mutation at positions 73 5 and 80 1 of the coding
region). The 2 new mutations were silent mutations since they did not result in a change
of the amino acid sequence of the UGT2B7 gene.

Figure 7. Sequence of genomic DNA. PCR was pe~ormed on genomic DNA isolated fiom human liver tissue using P5 and P6 pnmers. Using RT-PCR P5 and P6 primers amplifies a I w bp fragment. However. PCR amplification with P5 and P6 pnmers using yenomic DNr\ as a template produces two fragments (B). nie upper band is approximately 1.6 Kb. the lower band is approximately 1.4 Kb. The lower band was gel purified. subcloned. transformed and then sequenced. The sequence matched that of the UGT2B7 variant with two additional mutations (A). The sequence also contains a intron/exon splice-site. The 1.6 Kb fragment is believed to be UGT2B4. (* npresents mutated base pairs)

Squence o f UGT2B7 Triascript
A sequence cornparison of the various members of the human UGT2B subfamily
reveals that the region amplified by the PS-P6 primers is highly homologous. in this
region, UGTZB7 shares a pater than 85% homology with UGT2B4, 2B 10, and
UGT2B 15 (Appendix 4.). The high homology of the UGTZB isozymes in this region
originally caused conceni as to the identity of the 1.4 Kb fiagment. Although the
fiagment shares the highest homology to UGT2B7, the fiagment could also have been a
novel UGT isoform or a mutated fonn of one of the other UGTZB enzymes. Therefore,
we decided to txy and ampli@ the entire coding region of UGT2B7 to see whether or not
the 2 new mutations observed in the genomic sequence also existed in the transcripts of
UGT2B7.
Our initial attempts to ampli@ the entire coding region of UGT2B7 from 6 Iivers
(K- 16, K- 19, K-27, K-28, L- 19, and L- 16) were unsuccessful due to the degradation of
the messenger RNA frorn these liver samples. We then decided to use 2 sets of primers,
P3-P6 and P5-P4 that together ampli@ the entue coding region of UGT2B7 (see Figure
2). Mer several attempts, we were successful in ampliQing the P3-P6 and P5-P4
fragments tiom al1 6 liven.
When 3 clones containing the P3-P6 insen âom 3 different liver sampies (K- 19,
K-28, L-19) were squenced automatedly, 866 out of the 869 base pairs completely
matched the published sequence of UGT2B7 (Figure 8). The three differences were the
C+T, T+A, and G+A mutations at positions 802, 80 1, and 735 of the coding region,
respectively. 'ïherefore, the genomic sequence of the variant allele with the 2 additional

mutations was neither a sequencing artifact nor the sequence of another UGT isozyme. It
is the sequence of UGT2B7.
hterestingly, al1 six liver samples contained at least one clone that possessed the
variant UGT2B7 allele. Furthemore. in addition to the mutation at position 802, the
variant allele was always associated with the 735 and 801 mutations. Figure 9A and 9B
are sequencing gels fkom UGT2B7 wildtype and UGT2B7 variant sequences,
respectively .
While using PS and P6 pnmers to perfonn RT-PCR we discovered that the P5 - P6 pnmers were not specific for only the UGT2B7 gene, the pnmers also had the ability
to amplifi the UGT2B4 gene as well (Appendix 5.). Therefore, we believe that the 1.6
Kb @ment produced fkom using P5-P6 pnmers to PCR genomic DNA is UGT2B4,
while the 1.4 Kb produa is UGT2B7.

Figure 8. Squence Analysis. RT-PCR was perfomed on mRNA ervtracted from human liver tissue using P3-P6 primers. The 839 base pair m e n t wac subsequently gel purifieci, subcloned and then sequenced. Ml3 foward (A) and reverse (B) pnmers were used to sequence. The sequence matched the published sequence of the UGT2B7 variant allele with 2 additional mutations. (U represents mutated base pairs)

Figure 9. Sepuence analysis. RT-PCR was performed on RNA isolated from human liver tissue using P3 and P6 primers. The RT-PCR product was subsequently subcloned. transformed. and then sequenced. The sequence matches that of UGT2B7 wildtype (A) and UGT2B7 variant plus two additional mutations (B). (* represents mutated base pairs)
802 (C)
735 (G)
+$O1 (A)
"735 (A)
*802 (T)

Allele Specific Amplification Aasay (ASA)
The results h m 3 individuals who were genotyped using the ASA method are
shown in Figure 10. The 422 bp eagment represents the amplification of the intemal
conaol (the human growth hormone gene), the 1.4 Kb fragment is UGT2B7, while the
1.6 Kb fragment is UGT2B4.
Individual A is a heterozygote, individual B is homozygous wildtype, whereas
individual C is a homozygous variant.
Genotyping a population using ASA
Of the 114 subjects genotyped, 54 individuals were heterozygotes, 33 were
homozygous wildtypes. while 27 subjects were homozygous for the variant allele (Table
7). Therefore, the gene frequencies of the wildtype and variant alleles are 0.526 and
0.474, respectively .
No difference was observed when the genotypes 50 male and 6 1 female subjects
were compared. In males, the percentage of homozygous wildtype, heterozygous, and
homozygous variant genotypes were 32,44, and 24, respectively. While, in females
28%, 49%. and 23% were genotyped as homozygous wiidtype, heterozygous, and
homozygous variant, respectively.
Out of the 98 Caucasian subjects testeà, 30%- 46%, and 23% were genotyped as
homozygous wildtype, heterozygous. and homozygous variant, respectively.

Figure 10. Allele Specific Amplification (ASA). Results Born heterozygous (A). homozyçous wildtype (B). and homozygous variant ( C ) individuais. The lower band is an amplitication of the human growh hormone gene The rniddle band is UGT3B7. and the uppermosr band is believed to be CGT384

Table 7. Summary of results from ASA genotyping assoy of 114 subjects.
Heterozygous
Homozygous Wildtype
Homozygous Variant
Total
Number Observed
Number Ex~ected

Genotypepbenotype cornparisons
8 individuals who had been previously phenotyped were chosen to perfonn a
genotype-p henotype comparative study (Figure 1 1). 2 of the 3 individuals who had
atypical S/R ratios were homozygous for the variant allele, while the other abnomial
subject was a heterozygote. Looking at the arnounts of S and R-oxazepam glucuronide
exmted, the heterozygote excreted normal amowits of the S-oxazepam glucuronide,
however, he excreted an abnonnally high amount of R- oxazepam glucuronide. Of the 5
normal phenotypes, 4 were genotyped as heterozygotes, while the remaining subject was
a homozygote for the wildtype allele (Figure 12.).

Figure 11. Phenotype-Genotype Cornparisons. Summary of phenotype-genotype results from 8 individuals, 3 were classified as being atypical (S/R ratio below 1.66). while 5 had normal phenotypes (SR ratio above 1.66) (A). Genotyping results Born the 8 individuals dong with the appropriate controls (B). ûenomic DNA controls were collected fkom blood (1-3). whereas genomic DNA used for phenotype-genotype cornparisons was collected from mouthwash. ASA of atypical abjects (4-6) and individuals with S/R ratios above the antimode (7- 1 1).
A.
Atypi cal
Normal
-
- -Note Variant is UGT21 -NA: Not Available
S/R oxazepam gi~ctnnide
ratio
1.38 1.17 1.38
1.8 1 2.20 2.98 4.67 3 .O4
hount of S-oxazepam glucuronide excreted in
8hrs (peakheightivol)
422 202 240
Amount of R-oxazepam glucuronide excreted in
8hn (peakheight*vol)
305 172 173
V W V W V W v w V W V W V W V W V W V W V W

Figure 12. SIR ratio versus genotype of UGT2B7 in 8 subjects.
W N V N
Genotype for UGTZB7

DISCUSSION

Distribution of the SIR oxazepam giucuronide ratio
There is a p a t e r than 20 fold variation in the Sm-oxazepam glucuronide ratio
( S R ratio) among 203 healthy volunteers. A histogram as well as probit and NTV
analyses of the data reveals that the SIR ratio is bimodally distributed (Figure 5).
Furthermore, approximately 18% of the population possess S/R ratios below an apparent
antimode of 1.66.
A previous population study conducted in this laboratory had also demonstrated a
bimodal distribution in the SIR ratios of 77 subjects (30 students, 47 elderly patients).
However, in contrast to our data, Patel et al. (1995a) reported that approximately 10 % of
the population had S/R ratios below an apparent antimode of 1 .go. This discrepancy in
the antimode value as well as the percentage of atypical subjects within a population
between the 2 studies may have resuited nom the inclusion of 47 geriatric patients to the
earlier study. Differences in age, health status, and concomitant dmgs in the elderIy
patients may have produced the differences seen. In fact. Patel observed that the S R
ratio in the patient population displayed positive skewness. He also reponed that there
was prevalence for higher S- to R- ratios in the geriatric subjects as compared to the
student population.
Kinetic analysis of 11 subjects demonstrated that urinary S/R ratios were
significantly correlated (r,= 0.90, p<0.05) to the plasma clearance of oxazepam (Patel et
al., 1995a). in the same midy, the phannacolcinetic parameters of 2 atypical subjects who
had S/R ratios of 1.41 and 1.57, respectively were compared to 9 normal individuals
(Mean f SD: 3.52 k 0.60). The results demonstrated that the 2 atypical subjects possess a
2-fold increase in the half-life of oxazepam as well as a 50% reduction in the plasma

clearance of the dnig as compared to nomal subjects. Inferring from the above results,
Our data thenfore suggeas that approximately 20 % of the population exhibit abnormal
kinetics for the metabolism of oxazepam. However, more pharmacokinetic studies are
needed to confinn this hypothesis. Since owepam is one of the most prescribed drugs
in the worki, the findings from these studies may have major clinical implications.
S/R ratio versus amount of S and R glucuronide
A strong correlation (r,= 0.63, p<O.OO 1) was observed between the S/R ratio and
S- glucuronidation (Figure 6A). However, the S I R ratio was also significantly correlated
( r r -0.26, pC0.05) to the amount of R- glucuronide (Figure 6B). Thus, in general, in
vivo variations in the S/R ratio is mainly a reflenion of the variations in the
glucuronidation of S-oxazepam. However, the importance of variations in R-
glucuronidation to the variations in the SIR ratio can not be discounted.
Interestingly, the amount of S- glucuronide was also significantly correlated to the
amount of R- glucuronide (rr= 0.5 1, p<O.OO 1). Inhibition studies using human liver
microsornes demonstrated that the glucuronidation of the S- an R- isomers of oxazepam
are catalyzed by different UGT isozymes (Patel et al., 1995b). The correlation seen here
thus suggests that the different UGT isoforms that ghcuronidate the S- and R-
enantiomers of oxazepam are co-regulated.
Factors that influence the metaboiism of osazepam
As described in the introduction, many factors are known to influence the
glucuronidation of oxazepam. In this study, Eicton such as age, ethanol, smoking, and

caffeine were shown not to infiuence either the glucuronidation of the individual isomers
of oxazepam or the S/R ratio (Table 5). in con- body size and oral contraceptives
were shown to influence the glucuronidation of oxazepam.
Obesity
Obesity was shown to enhance the glucuronidation of S- oxazepam (r,= 0.23,
p<0.05) in 1 15 volunteers. Furthemore, among 203 subjects, body size was significantly
correlated to the S/R ratio (r,= 0.28, p<0.001). These results are in agreement with a
report that demonstrated that the clearance of oxazepam was increased in obese subjects
(Abemethy and Greenblatt, 1986). An increase in the Iiver size of obese subjects is
believed to be the reason why obese in4viduals have a higher capacity to glucuronidate
oxazepam. Interestingly, however, the glucuronidation of R- oxazepam was not
influenced by body size.
Oral contraceptivesi
A previous study demonstrated that oral contraceptive use increases the clearance
of oxazepam by 2-fold when compared to females who were non-oral contraceptive users
(Patwardhan et al., 1983). Whether this inductive effect is directly due to the progestin or
estrogen in the oral contraceptives or secondary hormonal changes resulting from oral
contraceptive use is still not known.
In this study. orai contraceptives were shown to significantly influence the
glucuronidation of both S- and R- isomen of oxazepam (Table 64B). The mean
amounts of the S- and R- oxazepam glucuronides excreted in oral contraceptive users

(546a8 1 and 198I 94, respectively) was significantly higher (p<0.05) than the mean
amounts of the S- and R- oxazepam glucuro~des excreted in females who were not
taking oral contraceptives (325I193 and 124k 42, respeaively).
Furthemore, oral contraceptives seem to induce the glucuronidation of S-
oxazepam to a greater extent than R- oxatepam. This was evidenced by the fact that the
S/R ratios in oral contraceptive users (n= 14, 3.13f 1.65) is higher than the SIR ratios in
women who were not taking oral contraceptives (n= 28, 2.6511.26).
The differential induction pattern seen in body-size and orai contraceptive use
suppons the hypothesis that the different isomen of oxazepam are catalyzed by different
UGT isoforms. However, the earlier suggestion that these isoforms are CO-regulated may
have been an overgeneralization.
The difference in the S/R ratio b e ~ e e n 1 18 males (3.22k1.49) and 85 females
(2.82f 1.32) was shown to be statistically significant (pC0.05). A sexual dimorphism was
also apparent when the percentages of atypical subjects ( S / ' ratio below 1.66) were
compared between the sexes. Twice as many females (26%) had S/R ratios below the
antimode as compared to males (13%). Furthemore, when oral contraceptives users
were removed h m the female population, the formation of both S- and R- glucuronides
were significantly less (p<0.05) in the female population (3252193 and 124k 42,
respectively) as compared to the male population (448k191 and 156k 65, respectively).
There is incnasing evidence that hormonal nicton are significant contributors the
glucuronidation of many drugs. In fa* sexual dimorphisms been demonstrated for the

glucuronidation of paracetamol, temazepam. and propranolol as well as oxazepam
(Greenblatt et al., 1980; Miners and Mackenzie, 1991). In al1 these cases, males have
shown a p a t e r capacity for glucuronidation than females.
Paracetamol is the only substrate thus fa that has been used to study the effects of
the menstrual cycle on dmg glucuronidation (Miners et al., 1983; Somaja and Thangam,
1987). The glucuronidation of paracetamol during the follicular and luteal phases were
shown not to be different in these studies.
Ethnicity
Studies involving morphine, codeine. and paracetamol have suggested that there
are interethic differences in the glucuronidation of these cornpounds (Critchley et al.,
1986; Yue et al., 1989; Zhou et ai., 1993). In this study, we observed that Caucasians
tended to metabolize oxazeparn more eniciently than Orientals, however, the differences
were not statistically significant. The SR ratio was higher in 133 Caucasian subjects
(3.10k1.62) as compared to 58 Oriental subjects (2.95c1.00). The percentage of atypical
subjects within the Caucasian population (2 1%) was aiso higher than that observed in the
Oriental population ( 14%).
The glucuronidation of the individuai enantiomers of oxazepam was also shown
not to be statistically different between the two racial groups. However, Caucasians
tended to excreted more S- and R- oxazepam glucuronides (437e20 and 157f 68,
respectively) than Orientais (4 1 1 e O 3 and 146= 72, respectively).

Genttics
Although fàctors such as sex, oral contraceptive use. and obesity have been
demonstrated to be contributors to the variability of the SIR ratio seen in vivo, these
factors do not completely explain why a large percentage of individuals within the
population have amical S R ratios.
A study involving microsomes from 37 human livers have demonstrated that the
distribution of both the SIR ratio as well as the Km values for the formation of S-
glucuronide display a distinct bimodality (Patel et al., 1995a). In vivo, we have observed
that the distribution of the S/R ratio among 203 volunteers is also bimodally distributed.
Furthermore, family studies have demonstrated that the atypical phenotype is heritable
(Appana, 1995). Moreover. cornparisons of the inter- and intra-individual variability of
the SR ratio demonstrated a high genetic component value (roc= 0.98) (Kalow et al.,
1998). These results therefore suggest that the SR ratio may also be influenced by
genetic as well as environmental factors.
In vitro studies onginating f?om this laboratory irnplicated UGTZB7 as the major
UGT isoform that catalyzes the glucuronidation of S-oxazepam (Patel et al., 1995b). In
1993, Jin et ai. isolated a variant clone of UGT2B7 fiom a Lgt 1 1 human liver cDNA
library (Jin et al., 1993). This clone had a C 4 ' substitution at position 802 of the coding
region. The base pair change resulted in an amino acid (histidine to tyrosine) change at
position 268 of the amino acid sequence.
When the wildtype (H~~') and variant sequences were expressed in COS4
cells (Patel. 1998), the wildtype form was shown to be able to giucuronidate oxazepam
100 times more efficiently than the variant fon.

A genotyping assay (RFLV) was developed to test for this particular mutation in
the mRNA of human liver tissue samples (Patel, 1998). RFLV consists of RT-PCR,
restriction analysis. followed by another PCR reaction. The genotyping of 4 atypical and
33 normal livers, demonstrated that a heterozygosity of the variant allele was associated
with an atypical phenotype, whereas, normal phenotypes were associated with
homozygosity of the wildtrpe allele. Thus, it was hypothesized that the variation in the
SIR ratio seen in vivo results âom a genetic mutation of the UGT2B7 gene.
Attempts to repeat the RFLV genotyping assay produced inconsistent results.
However, reanalysis of the data by the sequencing of RT-PCR products of 2
heterozygotes (K- 16, K 19) and 4 hornozygous wildtype livers (K-27, K-28, L 1 9, and L-
16) discovered that al1 6 samples contained the variant sequence. Thus suggesting that
the RFLV assay is not allele specific and that the hquency of the variant allele is higher
than previously thought.
Allele Specific Amplification of UGT2B7
In this study, we developed a new, rapid and simple genomic genotyping assay
that has the ability to discriminate between the UGT2B7 wildtype and variant alleles
(Figure 10). Allele specific amplification (ASA) is an approach that has been
successfblly used in the genotyping of mutations in N-acetyltransferase 2 (NATZ) as well
as mutations in Cytochromes P450 CYP LAI, 2A6, and 2D6 (Blum et al., 199 1; Daly et
al., 1994).
The genotyping of 1 14 individuals was conducted using ASA (Table 7). The
allelic fiequencies of the wildtype and variant gaies within the population were

determined to be 0.526 and 0.474, respectively. Chi-square analysis of the observed and
expected fiequencies demonstrates that the data is in agreement with the Hardy-Weinberg
principle (%'= 0.286, pi 0.87). The high prevalence of the variant allele (0.474) within
our population is in direct conflid to the earlier genotyping study (Patel. 1998) which
reported that the Eequency of the variant allele was 0.04.
Gilbert's syndrome is a mild form of unconjugated hyperbilirubinaemia. This
disorder is very common, affecting between 249% of the population (Bosma et al.,
1995). Gilbert's syndrome is clinically characterized by a consistent mildly raised non-
fasting total serum bilitubin concentration above 17 pmol/L. Most of the clinical cases of
Gilbert's syndrome are associated with a mutation in the promoter region of the bilirubin
glucuronsyltransferase, UGT 1 A 1 (Monaghan et al.. 1996). A homozygosity of the (TA),
mutation in the promoter region produces Gilbert's syndrome. Funhemore, it is believed
that the wildtype (TA)o allele exhibits dominance over the mutated (TA), allele, since,
both homozygosity or heterozygosity of the (T& allele produce normal phenotypes. In
the Sconish population, 10-13 percent ofthe population was reponed to be homotygous
for (TA), mutation (Monaghan et al., 1996).
The genotyping of 114 subjects for UGTZB7 aileies revealed that approximately
20% ofthe population were homozygotes for the variant allele. The phenotyping of 203
individuals demonstrated that approximately 20 % of the population exhibit abnorrnal
oxazeparn metabolism. The consistency between the genotyping and phenotyping results
suggested that a homozygosity of the variant allele might be associated with an atypical
phenotype. The data also suggests that the wildtype allele displays dominance over the

variant allele. This situation may be analogous to the situation of the (TAb mutation and
its association with Gilbert's syndrome.
Pbenotype-Genotype Coinparison
A phenotyps-genotype comparative study was conduaed to test the hypothesis
that atypical S/R ratios are associated with homozygous variant genotypes. The genomic
DNA from 8 subjects who had been previously phenotyped (5 normal, 3 atypical) was
obtained from mouthwash. ASA wâs then perfomed on these 8 samples (Figure 1 1B).
All five normal phenotypes had either a hornozygous wildtype (n= 1) or
heterozygous (n= 4) genotypes. whereas, 2 out of the 3 atypical subjects were
homozygotes for the variant allele. However. contrary to the hypothesis, the other
atypical individual possessed a heterozygous genotype. What was interesting about this
individual was that he exhibited a significantly enhanced ability to glucuronidate the R-
isomer of oxazepam (Figure 1 1 A). In contra% his ability to glucuronidate S-oxazepam
was normal. Therefore, in this panicular case, the atypical phenotype resulted from an
increase in the ability to glucuronidate R-oxazepam and not a genetic alteration in
UGTZB7.
The genotyping results fiom these 8 individuals supported the hypothesis that the
S/R ratio phenotypes and UGT2B7 genotypes are associated to one another. However,
due to the limited number of individuals in the study, we were not able to definitively
prove the hypothesis.
Nothing is known about the identity of the UGT isoform(s) that catalyzes the
formation of Rsxazepam glucuronide. Therefore, whether or not there are any genetic

alteration(s) in the enzyme(s) that influence the metabolism of oxazepam is still
unknown. Furthemore, we have previously demonstrated that environmental factors
have the ability to influence the S I R ratio. We can not, therefore, discount the tact that
the induction of R-oxazepam glucuronidation seen in this particular individual was
caused b y non-genet ic facto r(s).
Condusion
In summary, we were able to demonstrate that approximately 20% of the
population possess atypical S/R ratios. Funhennore. we also demonstrated that the
variation in the S I R ratio is rnainly a refiection of the variation in S-oxazepam
glucuronidation. Moreover, factors such as sex. body site. as well as oral contraceptive
use were shown to significantly influence the glucuronidation of oxazepam.
A genotype assay that is able to discriminate between the wildtype and variant
alleles of UGT2B7 was also established. The 6equencies of the wildtype and variant
alleles within a population were s h o w to be 0.526 and 0.474. respectively. And lady, a
phenotype-genotype comparative study revealed an association between the SIR ratio
phenotypes and UGT2B7 genotypes.
Future Studies
Patel(1995a) using 2 atypical and 9 normal subjects concluded that atypical S/R
ratios are related to abnormal oxazepam metabolism. in this study, we were able to show
an association between the S/R ratio and a specific genetic alteration in the UGT2B7
gene in 8 subjects. From these results, we suggest that a genetic aiteration in UGTZB7 is

relateâ to an atypical S/R ratio, which in tum causes abnonnal oxazepam metabolism. A
possible future study would be to combine genotype-phenotype -dies with
phannacokinetic analyses.
Family studies have demonstrated that the SR ratio is heritable (Apparia, 1 995).
Whether or not the UGT2B7 genotypes are inherited. and the mode of inhentance, is still
to be elucidated.


Abemethy, D. R., and Greenblatt, D. J.: Drug disposition in obese humans. An update. Clin Pharmacokinet 11: 199-213, 1986.
Abernethy, D. R., Greenblatt, D. J., Ochs. K R., Weyers, D., Divoll. M., Hmatz , J. S., and Shader, R. 1.: Lorazeparn and oxazepam kinetics in women on low-dose oral contraceptives. Clin Pharmacol Ther 33: 628-32, 1983.
Allen, M. D., Greenblatt, D. J., Hannatz, I. S., and Shader, R. 1.: Desmethyldiazepam kinetics in the elderly afler oral prazepam. Clin. Pharmacol. Ther. 28: 196-202, 1980.
Alvan, G., and Odar-Cederlof, 1.: The pharmacokinetic profile of oxazepam. Acta Psychiatr Scand Suppl 274: 47-55, 1978.
Alvan, G., Siwers, B., and Vessman, J. : Pharmacokinetics of oxazepam in healthy volunteers. Acta Phannac. Tox. 40 (Suppl. 1): 40-5 1, 1977.
Arnbrose, P. J. : Clinical p harmacokinetics of chloramp henicol and chlorarnp henicol succinate. Clin. Pharmacokinet. 9: 222-23 8, 1984.
Aono. S., Adachi, Y., Uyama, E.. Yamada Y.. Keino, H., Namo, T., Koiwai, O., and Sato, H: Analysis of genes for bilirubin UDP-glucuronosyltransferase in Gilbert's syndrome [see comments]. Lancet 345: 95 8-9, 1995.
Aono, S., Yamada, Y., Keino, H., Hanada, N., Nakagawa, T., Sasaoka, Y., Yazawa, T., Sato, K, and Koiwai, O.: Identification of defect in the genes for bilirubin UDP- glucuronosyl- transferase in a patient with Crigler-Najar syndrome type II. Biochem Biophys Res Commun 197: 1239-44, 1995.
Aono, S., Yamada, Y., Keino, H., Sasaoka, Y., Nakagawa, T., Onishi, S., Mirnura, S., Koiwai, O., and Sato, H.: A new type of defect in the gene for bilirubin uridine 5'- diphosphate- glucuronosyltransferase in a patient with Crigler-Najjar syndrome type 1. Pediatr Res 35: 629-32, 1994.
Appana, G.: Pharmacogenetic studies: in vitro biotransformation of bupranolol. In vivo glucuronidation of oxazepam. In Department of Phmacology, pp. 1 1 i , Unverstiy of Toronto, Toronto, 1995.
Arias, 1. M., Gartner, L., Cohen, M., Ben Esser. J., and Levi, A. J.: Chronic non- haemolytic unconjugated hyperbilirubinaemia with giucuronosyltransferase deficiency. Am. J. Med. 47: 395-409, 1969.
Beaulieu, M., Levesque, E., Hum, D. W., and Belanger, A: Isolation and characterization of a novel cDNA-encoding a human üDP-glucumnosyltransferase active on C-19 steriods. J. Biol. Chem. 271: 22855-22862, 1996.

Beaulieu, M., Levesque, E., Tchernof. A., Beatry, B. G., Belanger, A, and Hum, D. W.: Chromosomal localization, structure, and regulation of the UGTZB 17 gene, encoding a C 19 steroid metabolizing enzyme. DNA Ce11 Bi01 16: 1 143-54, 1997.
Beutler, E., Gdbart, T., and Demina, A.: Racial variability in the LJDP- glucuronosyltransferase 1 (UGT 1 A 1) promoter A balanced polymorp hism for regulation ofbilhbin metabolism? Proc. Natl. Acad. Sci. 95: 81704, 1998.
Bliss, A.: The method of probits-a correction. Science 79: 409-4 10, 1934.
Blum, M., Demierre, A., Grant, D. M., Heim, Y.. and Meyer, U. A: Molecular mechanism of slow acetylation of dmgs and carcinogens in humans. Proc. Natl. Acad. Sci. USA 88: 5237-5241, 199 1.
Bock, K. W.: Roles of UDP-glucuronosyltransferases in chernical carcinogenesis. Crit Rev Biochem Mol Bi01 26: 129-50, 1991.
Bosma, P., Chowdhury, J., and Jansen, P.: Genetic inheritance of Gilbert's syndrome. Lancet 346: 314-315, 1995a.
Bosma, P. J., Chowdhury, J. R., Bakker, C.. Gantla S., de Boer, A., and Oostra, B. A.: The genetic basis of the reduced expression of bilirubin UDP-glucuronosyltransferase I in Gilbert's syndrome. N. Engl. J. Med. 333: 1 171 -5, 199%.
Bosma, P. J., Chowdhury, J. R.. Huang, T. J., Lahiri. P., Elferink, R. P., Van Es, H. H., Lederstein, M., Whitington, P. F.. Jansen, P. L.. and Chowdhury, N. R.: Mechanisms of inherited deficiencies of multiple UDP- glucuronosyltransferase isofonns in two patients with Crigler-Najjar syndrome, type 1. Faseb J 6: 2859-63. 1992.
Bosma, P. J., Goldhoom, B.. Oude Elferink, R P.. Sinaasappel, M., Oostra. B. A., and Jansen, P. L.: A mutation in bilirubin uridine 5'-diphosphate-glucuronosyltransferase isoform 1 causing Crigler-Najjar syndrome type II [see comments]. Gastroenterology 105: 2 16-20, 1993.
Burcheil, B., Brierley, C. H., and Rance, D.: Specificity of human UDP- Glucuronosyltransferases and xenobiotic glucuronidation. Life Sciences 57: 18 19- 183 1, 1995.
Burchell, B., and Coughtrie, M. W. : UDP-glucuronosyltransferases. Phannacol Ther 43: 26 1-89, 1989.
Burchell, B., Nebert, D. W., Nelson, D. R.. Bock K. W., lyanagi, T., Jansen, P. L., Lancet, D., Mulder, G. J., Chowdhury, J. R, Siest. G., and et al.: The UDP glucuronosyltransferase gene superfamily: suggested nomenclature based on evolutionary divergence. DNA Cell Bi01 10: 487-94, 199 1.

Caldwell, J., Winter, S. M.. and Hutt, A J.: The pharmacologicai and toxicological significance of the stereochemistry of dnig disposition. Xenobiotica 18 (Suppl. 1): 59-70, 1988.
Cheng, Z., Radorninska-Pandya, A, and Tephly, T. R.: Cloning and expression of human UDP-glucuronosyitransferase (UGT) lA8. Arch Biochem Biophys 356: 30 1-5, 1998.
Coffman, B. L., King, C. D., Rios, G. R, and Tephly, T. R.: The glucuronidation of opioids, other xenobiotics, and androgens by human UGT2B7Y(268) and UGT2BîH(268). Dnig Metab Dispos 26: 73-7, 1998.
Coffman, B. L., Rios, G. R., King, C. D., and Tephly, T. R.: Human UGT2B7 catalyzes morphine glucuronidation. Dtug Metab Dispos 25: 1-4, 1997.
Corbella, A., Ganboboldi, P., Jommi, G., Forgione, A, Marcucci, F., Martelli, P.. Mussini, E., and Mauri, F.: Stereochemistry of the enzymatic 3-hydroxylation of 1.3dihydro-2H- 1.4-benzodiapin-2-ones. J. Chem. Soc. Chem. Comrn. 1973 : 72 1-722.
Crigler, J. F., and Najar, V. A.: Cogenital familial non-haemolytic jaudice with kemicterus. Paediatrics 10: 169- 180, 1952.
Critchley, J. A., Nimmo, G. R., Gregson, C. A., Woolhouse, N. M.. and Prescott, L. F.: Intersubject and ethnic differences in paracetamol metabolism. Br. J. Clin. Pharmac. 22: 649-657, 1986.
Dahl-Puustinen, M. J. , Peny, T. L., Dumont, E., von Bahr, C., Nordin, C., and Bertilsson, L.: Stereoselective disposition of racemic E- 10-hydroxynortnptyline in human beings. Clin. Pharmac. Ther. 45: 650-656, 1989a
Dahl-Puustinen, M. L., Dumont, E., and Bertillsson, L.: Glucuronidation of E- 10- hydroxynonriptyline in human liver, kidnay, and intestine: organ-specific differences in enantioselectivity. Dmg Metab. Dispos. 17: 422436, 1989b.
Daly, A, Cholenon, S., Armstrong, M., and Idle, J. R.: Genotying for polymorphisms in xenobiotic metabolism as a predictor of disease susceptibility. Envir. Health Perspect. 102 (Suppl(9): 55-61, 1994.
Desmond, P. V., Patwardhan, R V., Schenker, S.. and Speeg, K. V.: Cimetidine impairs the elimination of chlordiazepoxide in humans. h a i s of Intemal Medicine 93: 266-268. 1980.
Drayer, D. E.: Problems in the therapeutic dm8 monitoring: The dilemma of enantiomenc drugs in man. Ther. Dmg Monit. 10: 1-7, 1988.

Dreyfiss, D., Shader, R. I., Harrnatz, J. S., and Greenblatt, D. J.: Kinetics and dynamics of single doses of oxazepam in the elderly: implications of absorption rate. J Clin Psychiatry 47: 5 1 1 4 , 1986.
Dutton, G.: Glucuronidation of dnigs and other compounds, CRC Press, Boca Raton, FL. 1980.
Ebner, T., and Burchell, B.: Substrate specificities of two stably expressed human liver UDP- glucuronosyltransferases of the UGT1 gene farnily. Drug Metab Dispos 21: 50-5. 1993.
Eichelbaum, M.: Pharmacokinetics and pharmacodynamie consequences of stereoselective dnig metabolism in man. Biochem. Pharmac. 37: 93-96, 1988.
El Mouelhi, M., Ruelius, H. W., Feneslau, C., and Dulik, D. M.: Species dependent enantioselective glucuronidation of three 2-arylpropionic acids. Naproxen, ibuprofen, benoxaprofen. Dnig Metab. Dispos. 15: 767-772. 1987.
Endrenyi, L., and Patel, M.: A new. sensitive graphical method for detecting deviations from the normal distribution of drug responses: the NTV plot. Br. J. Clin. Pharmacol. 32: 159-166, 1991.
Gantla, S., Bakker, C. T., Deocharan, B.. Thurnmala, N. R., Zweiner. J., Sinaasappel, M., Roy Chowdhury, J., Bosma, P. J., and Roy Chowdhury, N.: Splice-site mutations: a novel genetic mechanism of Crigler-Najjar syndrome type 1. Am J Hum Genet 62: 585-92, 1 998.
Gerkens, J. K., Desmond, P. V., Schenker, S., and Branch, R. A.: Hepatic and extrahepatic glucuronidation of lorazepam in the dog. Hepatology 1 : 3 29-3 3 5, 198 1.
GrechoBelanger, O., Turgeon, J., and Gilbert, M.: Stereoselective disposition of mixiletine in man. Br. J. Clin. Pharmac. 21: 481487, 1986.
Green, M., Otum, E. M., and Tephly, T. R.: Stable expression of a human liver UDP- glucuronosyltransferase (UGT2B 15) with activity toward steroid and xenobiotic substrates. Dnig Metab. Disp. 22: 799-805, 1994.
Green, M. D., King, C. D., Mojarrabi, B., Mackenzie, P. I., and Tephiy, T. R.: Glucuronidation of amines and other xenobiotics catalyzed by expressed human UDP- glucuronosyltransferase 1 A3. Dnig Metab Dispos 25: 37- 12, 1998.
Greenbla~ D. J.. Divoll M.. Abemathy, D. R, Ochs, H. R., and Shader, R 1.: Clinical pharmacokinetics of the newer benzodiapines. Clin. Pharmacokinet. 8: 233-252, 1983.
Greenblaa D. J., Divoll, M.. Harmatz, J. S., and Shader, R. 1.: Oxazepam kinetics: effects of age and sex. J. Pharmac. Exp. 'fher. 215: 86-9 1, 1980.

Greenblatt, D. J., and S hader, R. 1. : Effects of age and other drugs on benzodiazepine kinetics. Armeirnittelforschung 30: 886-90. 1980.
Gngus, Z., Watkins, J. B., Thompson , T. N., and Naassen, C. D.: Resistance of some phase II biotransfomation pathways to hepatotoxins. J. Pharmacol. Exp. Ther. 222: 471- 479, 1982.
Hamberg, O., Ovesen, L., Dorfeldt, A, Loft, S., and Sonne, J.: The effect of dietary energy and protein deficiency on drug metabolism. Eur J Clin Phmacol 38: 567-70, 1990.
Harding, D., Jeremiah. S. J., Povey, S., and Burcheil, B.: Chromosornal mapping of a human p henol UDP-glucuronosyltransferase. Ann. Hum. Genet. 54: 17-2 1, 1990.
Jackson, M. R., Mccarthy, L. R., Harding, D.. Wilson, S., Coughtrie, M. W., and Burchell, B.: Cloning of a human liver microsoma1 UDP-glucuronosyltransferase cDNA. Biochem. J. 242: 581-588, 1987.
Jaqz, E., Ward, S., Johnson, R. F., Schenker, S.. Gerkens, J., and Branch R. A.: Extrahepatic glucuronidation of morphine in the dog. Drug Metab. Disp. 14: 627-630, 1986.
Jin, C., Miners, J. O., Lillywhite, K. J., and Mackenzie, P. 1.: Complementary deoxyribonucleic acid cloning and expression of a human livet uridine diphosphate- glucuronosyltransferase glucuronidating carboxylic acid-containing drugs. J Pharmacol Exp Ther 264: 475-9, 1993a
Jin, C. J., Mackenzie, P. 1.. and Miners, J. O.: The regio- and stereo-selectivity of C 19 and C2 1 hydroxysteroid glucuronidation by UGT2B7 and UGT2B 1 1. Arch Biochem Biophys 341: 207-1 1, 1997.
Jin, C. J., Miners, J. O., Burchell, B., and Mackenzie. P. 1.: The glucuronidation of hydroxylated metabolites of benzo[a]pyrene and 2- acetylaminofluorene by cDNA- expressed human UDP- glucuronosyltransferases. Carcinogenesis 14: 263 7-9, 1993 b.
Kalow, W.: Race and therapeutic drug response. New Engl. J. Med. 320: 588-590, 1989.
Kalow, W.: Interethic variation of dmg metabolism. TIPS 12: 102- 107, 199 1.
Kalow, W., Tang, B., and Endrenyi, L.: Hypothesis: Cornparisons of inter- and intra- individual variations can substitute for twin studies in drug research. Pharmacogenetics 8: 283-289, 1998.
Klotz, U., Avant, G. R., Hoyumpa, A., Schenker, S., and Wilkinson, G. R.: The effects of age and liver disease on the disposition and elimination of diazepam in adult man. I. Clin. Invest. 55: 347-359, 1975.

Koiwai, O., Nishizawa, M., Hasada, K., Aono, S., Adachi, Y., Marniya, N., and Sato, H.: Gilbert's syndrome is caused by a heterozygous missense mutation in the gene for bilirubin UDP-glucuronosyltransferase. Hum Mol Genet 4: 1 1836, 1995.
Labrune, P., Myara, A, Hadchouel, M., Ronchi. F., Bernard, O., Trivin, P., Chowdhury, N. R, Chowdhury, J. R., Munnich, A., and Odievre, M.: Genetic heterogeneity of Crigler-Najjar syndrome type 1: a snidy of 14 cases. Hum Genet 94: 693-7, 1994.
Lazard, D., Zupko, K., Poria, Y., Nef. P., Lazarovits, J., Hom S., Khen, M., and Lancet, D. : Odorant signal temination by olfactory üDP @ucuronosyl transferase. Nature 349: 790-3, 1991.
Levesque, E., Beauiieu, M., and Belanger, A: uGT2B4 @a): A üDP- glucuronosyltransferase encoded by a polymorphic gene with differential substrate specificity. Submitted for publication in Pharmacogenetics, 1998.
Levesque, E., Beaulieu, M., Green, M. D., Tephiy. T. R., Belanger. A.. and Hum. D. W. : Isolation and characterization of UGTZB 1 j(YS5): a UDP- ~lucuronosyltransferase encoded by a polymorphic gene. Pharmacogenetics 7: 5 17-25, 1997.
Lum, A, and Marchand, L. L.: A simple mouthwash method for obtaining genomic DNA in molecular epidemiological studies. Cancer Epidemiology, Biomarken & Prevention 7: 7 19-724, 1998.
Mackenzie, P. L, Owens, 1. S., Burchell. B., Bock K. W., Bairoch, A., Belanger, A., Foumel-Gigleux, S., Green, M., Hum, D. W., Iyanagi. T., Lancet, D., Louisot, P., Magdalou, J., Chowdhury, J. R., Ritter, J. K., Schachter, H., Tephly, T. R., Tipton, K. F., and Neben, D. W.: The UDP glycosyltransferase gene superfamily: recommended nomenclature update based on evolutionary divergence. Pharmacogenetics 7: 255-69, 1997.
Maniatis, T., Fritsch, E. F., and Sambrook J.: Molecular cloning: a laboratory manual., Cold Spring Harbor Laboratory, Cold Spring Harbor, NY, 1990.
Marks, J.: The benzodiazepines-Use and abuse. .Anneim-Forsch.30: 898-90 1, 1980.
Mascher, H., Nitsche, V., and Shutz, K: Separation. isolation, and identitication of optical isomers of 1.4-benzodiazepine glucuronides hom biological fluids by reversed phase high-perfomance liquid chromatography. J. Chromatogr. Biomed. Appl. 306: 23 1- 239, 1984.
Miners, J. O., Attwood, J., and Birkett, D. J.: hluence of sex and orai contraceptive neriods on paracetamoi metabolism. Br. J. Clin. Pharmac. 16: 503-509. 1983.
Miners, J. O., and Mackenzie, P. 1.: Drug giucuronidation in humans. Pharmacol Ther 5 1: 347-69, 199 1.

Mohler, H., Okadda, T., Heitz, P. H., and Ulrick J.: Biochemical identification of the site of action of benzodiapines in human brain by 3 ~ d i a z e ~ a m binding. Life Sci. 77: 985- 996, 1977.
Monaghan, G.. Burchell, B., and Boxer, M.: Structure of the human UGT2B4 gene encoding a bile acid UDP- glucuronosyitransferase. Marnm Genome 8: 692-4, 1997.
Monaghan, G., Ryan, M., Seddon, R., Hume, R., and Burchell, B.: Genetic variation in bilinibin UPD-glucuronosyltransferase gene promoter and Gilbeds syndrome [see comments]. Lancet 347: 578-8 1, 1996.
Mulder, G.: Glucuronidation and its role in regulation of biological activity of drugs. Annual Review of Pharmacology and Toxicology 32: 25-49, 1992.
Ochs, H. R., Greenblatt, D. J., and Otten, H.: Disposition of oxazepam in relation to age, sex and cigarette smoking. Klin. Wochenschr. 59: 899-903, 198 1.
O'Neill, P. J., Yorgey, K. A., Renzi, N. L., Williams, R. L., and Benet, L. 2.: Disposition of zomepirac sodium in man. J. Clin. Pharmac. 22: 470476, 1982.
Osborne, R., Joel, S., Trew, D., and Slevin. M.: Morphine and metabolite behavior after different routes of morphine adminstration: Demonstration of the importance of the active metabolite morphine 6-glucuronide. Clin. Pharmac. Ther. 47: 12- 19. 1990.
Patel, M.: Genetic variability of an Uridine-diphosphoglucuronosyltransferase: UGT2B7. In Department of Pharmacology, pp. 125, University of Toronto, Toronto, 1998.
Patel, M., Tang, B. K., Grant, D. M., and Kalow. W.: Interindividual variability in the glucuronidation of (S) oxazepam contrasted with that of (R) oxazepam. Pharmacogenetics 5: 287-97, 1995a.
Patel, M., Tang, B. K., and Kalow, W.: (S)oxazepam glucuronidation is inhibited by ketoprofen and other substrates of UGT2B7. Pharmacogenetics 5: 43-9, 1995b.
Patwardhan, R. V., Johnson, R. F., Hoyurnpa, A., Sheehan, A, Desmond, P. V., Wilkinson, G. R., and Branch, R. A.: Normal disposition of morphine in cirrhosis. Gastroenterology 81: 1001-1011, 1981.
Patwardhan, R. V., Mitchell, M. C., Johnson. R. F., and Schenker, S.: Differential effects of oral contraceptive steroids on the rnetabolism of benzodiazepines. Hepatology 3: 248- 53, 1983.
Patwardhan, R. V., Yarborough, G. W.. Desmond, P. V., Johnson, R. F., Schenker, S., and Speeg, K. V., Jr.: Cimetidine spares the glucuronidation of lorazepam and oxazepam. Gastroenterology 79: 912-6, 1980.

Ritter, J. K., Chen, F., and Sheen, Y. Y. : A novel complex locus UGTl encodes human bilimbin, phenol, and other UDP-glucuronosyltransferase family with identical carboxyl tennini. J. Biol. Chem. 267: 3257-6 1, 1992a
Ritter, J. K., Sheen, Y. Y., and Owens, 1. S.: Cloning and expression of human liver UDP-glucuronosyltransferase in COS- 1. 3,4-catechol estrogens and estnol as primary substrates. J. Biol. Chem. 265: 7900-7906, 1990.
Ritter, K., Chen, F., Sheen, Y. Y., Lubet, R. A, and Owens, 1. S.: Two human liver cDNAs encodes UDP-glucuronosyltransferases with 2 log differences in activity toward parallel substrates including hydeoxycholic acid and certain earogen denvatives. Biochemistry 31: 3409-34 14, 1 W2b.
Ruelius, H. W., Tio, C. O., Knowles, J. A., McHugh S. L., Schillings, R. T., and Sisenwine, S. F.: Diastereoisomeric glucuronides of oxazepam. Isolation and stereoselective enzymic hydrolysis. Dmg Metab Dispos 7: 40-3, 1979.
Scott, A. K., Cameron, G. A., Khir, A. S. M., McHardy, K. C., and Hawksworth, G. M.: Oxazepam elimination in patients with diabetes mellitus. Br. J. Clin. Pharmac. 26: 224, 1988.
Scott, A. K., Khir, A. S., Bewsher. P. D., and Hawksworth, G. M.: Oxazepam pharmacokinetics in thyroid disease. Br J Clin Pharmacol 17: 49-53, 1984.
Scott. A. K., Khir, A. S., Steeie, W. H., Hawkswonh G. M., and Petrie, J. C.: Oxazepam pharmacokinetics in patients with epilepsy treated long-term with phenytoin alone or in combination with phenobarbitone. Br J Clin Phmacol 16: 44 1-4, 1983.
Seideman, P., Ericsson, O., Groningsson, K., and von Bahr, C.: Effect of pentobarbital on the formation of diastereomeric oxazepam glucuronides in man: analysis by high performance liquid chromato.graphy. Acta Pharmacol Toxicol (Copenh) 49: 200-4, 198 1.
Sellers, E. M., Giles, H. G., Greenblatt, D. J., and Naranjo, C. A.: Differential effects of benzodiazepine disposition by disulfiram and erhanol. Armeirnittelforschung 30: 882-6, 1980.
Sellers, E. M., Greenblatt, D. J., Giles, H. G., Naranjo, C. A., Kaplan, K., and MacLeod, S. M.: Chlordiazepoxide and oxazepam disposition in cirrhosis. Clin Pharmacol Ther 26: 240-6, 1979.
Seppen, J., Bosma, P. J., Goldhoom, B. G., Bakker, C. T., Chowdhury, I. R., Chowdhury, N. R, Jansen, P. L., and Oude Elferink, R P.: Discrimination between Crigler-Najjar type 1 and II by expression of mutant bilirubin uridine diphosphate- glucuronosyltransFerase. J Clin Invest 94: 23 85-9 1, 1994.

Serlin, M. I., Sibeon, R. B., and Mossman, S.: Cirnetidine: interaction with oral anticoagulants in man. Lancet 2: 3 17-3 19. 1979.
Shull, H. J., Wilkinson, G. R., Johnson, R.. and Schenker, S.: Normal disposition of oxazepam in acute viral hepatitis and cirrhosis. ANI Intern Med 84: 420-5, 1976.
Sisenwine, S. F., Tio, C. O., Hadley, F. V., Liu, A. L., Kimmel, H. B., and Ruelius, H. W.: Species-related diReremes in the stereoselective glucuronidation of oxazepam. Dnig Metab Dispos 10: 605-8, 1982.
Somaja, L., and Thangam, J.: Salivary paracetamol elimination kinetics during the menstruai cycle. Br. J. Clin. Pharmac. 23: 348-350, 1987.
Sonne, J.: Factors and conditions atfecting the glucuronidation of oxazepam. Phmacol Toxicol73 (Suppl 1): 1-23, 1993.
Sonne, J., Andreasen, P. B., Loft. S ., Dossing, M., and Andreasen, F. : Glucuronidation of oxazepam is not spared in patients with hepatic encep halopathy . Hepatology 1 1 : 95 1-6, 1990a.
Sonne, J., Boesgaard, S., Poulsen, H. E., Loft. S., Hansen, J. M., Dossing, M.. and Andreasen, F.: Pharmacokinetics and pharmacodynarnics of oxazepam and metabolism of paracetamol in severe hypothyroidism. Br J Clin Phannacol 30: 737-42. 1990b.
Sonne, J., Dossing, M., Loft, S., Olesen, K. L., Voiimer-Larsen, A., Victor. M. A.. Hamberg, O., and Thyssen, H.: Single dose phannacokinetics and pharmacodynarnics of oral oxazepam during concomitant administration of propranolol and labetalol. Br J Clin Phannacol 29: 33-7, 1990c.
Sonne, J., Dragsted, J., LoR S., Dossing, hl., and Andreasen, F. : Influence of a very low calorie diet on the clearance of oxazeparn and antipyrine in man. Eur J Clin Pharmacol 36: 407-9, 1989.
Sonne, I., LoA. S., Dossing, M., Boesgaard, S., and Andreasen, F.: Single dose phannacokinetics and pharmacodynarnics of oral oxazepam in very elderly institutionalised subjects. Br. J. Clin. Pharmacol. 31: 719-722, 199 1.
Sonne, J., Loft, S., Dossing, M., Vollmer-Larsen, A. Olesen, K. L., Victor. M., Andreasen, F., and Andreasen, P. B.: Bioavailability and p harmacokinetics of oxazepam. Eur J Clin Pharmacol 35: 385-9, 1988.
Vesell, E.: Complex effects of diet on dnig metaboism. Clin Pharmacol Ther 36: 285- 296. 1984.

Visser? T. J., Kaptein, E., Gijzel, A L., de Herder, W. W., Ebner, T., and Burchell, B.: Glucuronidation of thyroid hormone by human bilirubin and p henol UDP- glucurony ltransferase isoenzymes. FEBS Lett 324: 3 58-60, 1 993.
Vree, T. B., Baars, k M., and Wuis, E. W.: Direct high pressure liquid chromatographie analysis and preliminary pharmacokinetics of enantiomen of oxazepam and temazepam with their corresponding glucuronide conjugates. Pharm Weekbl [Sci] 13: 83-90, 199 1.
Yue, Q. Y., Svensson, J. O., Alm, C., Sjoqvist, F.. and Sawe, J.: Interindividual and interethnic differences in the demethylation and glucuronidation of codeine. Br J Clin Pharmacol 28: 629-37, 1989.
Zhou, H. H., Sheller, J. R., Nu. H.. Wood, M., and Wood, A. J.: Ethnic diflerences in response to morphine. Clin Pharmacol Ther 54: 507-13, 1993.


SE?< AG€ iUCE
O M 25 CHINESE
1 F 24 CAUCASIAN
2 M 23 CHINESE
3 F 42 CAUCASIAN
4 M 24 CAUCASIAN
5 F 40 CHINESE
6 M 25 CAUCASIAN
7 F 24 C W S 1 A N 8 M 23 CHINESE
9 M 24 CAUCASIAN
10 M JO CHMESE
11 F 39 CAUC.4SIAN
12 M 26 CAUCXSUN
13 M 18 CAUCASIAN
14 hl 19 CAUCASIAN
15 .CI 18 CACCASlrLV
16 F 19 CAUCr\SlXN
17 hl 19 CAUCASIAN
18 .Cl 19 E.iND. 19 hl 19 CAUCSIZuV
20 M 19 E.MD. 21 M 19 CAUCASIAN
22 M 18 CAUCASIAN
23 M 18 CAUCASlAV
24 M 19 PHILOPiNO 25 M 22 CAUCASIAN
26 hl 20 CAUCASIAN
27 hl 23 CAUCASIAN
28 hf 25 CAUCASlAN
29 F 32 EMD. 31 hI 32 CAUCSUV
32 F 30 CAUCASIAN
33 F 27 CAUCASiAii
35 M 19 CAUCASIAPJ
36 .Li 18 CAUCASIAN
37 hi 19 CAUCASttV
38 M 41 C H M S E 39 F 39 CHINESE M X1 26 CAUCASIAN
JI 81 29 CAUCASWN
42 M 34 CAUCASiAN
43 19 CAUCASIAN
46 M 19 CAUCASUN
47 M 19 CHINESE
48 M 18 PiüLOPiNO 49 M 18 CHINESE 50 M 23 CAUCASM
OC
NO YEs NO NO NO NO NO
YES NO NO NO E S NO NO
NO Y 0
HO Y 0
NO NO NO NO
NO NO NO
NO NO NO NO YES NO NO
YES NO NO NO NO NO NO NO NO NO NO
NO NO NO NO
Vol (II) 0.3 85 0.460
0.525
0.300
0.335
0.630
0.460
0.265
0.330
1.020
0.365
0.700
0.365
0.240
0.475
0.235
0.085
0.200
0.500
0.230
0.425
0.095
0.385
0.225
0.470
0.400
0.265
0.270
0.230
0.070
0.235
0.565
0.365
0.430
0.305
0.385
0.320
0.455
0.300
O. 130
0.550
O. 105
0.720
0.480
0.150
0.245
0.500

SEX AGE RACE
19 CHINESE
23 K o m 20 CAUCASWrJ
22 CAUCASIAN
51 CAUCStAN
37 P?IILOP[NO
24 C A U C s h v
22 CAUCSMN
32 CAUCSWN
23 CHMESE
19 CAUCASMN
22 CHMESE
23 CAUCr\SUrJ
2s CAUCASIAN
22 CAUCA!%lR
22 CAUCASUN
19 CAL'CZ\Slu
19 CAUCASIAN
25 CAUCASWIV
22 CHINESE 24 CAUCASIAN
22 CAUCASIAN
20 CAuCsIrLV
22 C A U C S I r n
22 CAUCASIAN
22 CXUCASIrn
27 CAL'CSlrtV
29 CAUCA!WN
24 CHCESE
20 CAUCASWN
22 C m C A u C
22 CAUCfiIAN
22 CIUNESE
51 CAUCSLW
49 CAUCASIAN
21 CAUCASIAN
23 CHINESE
38 CAUCASIrLV
18 CHINESE 19 EiND. 2s CAUCIISIAÀ'J
24 CAUCASUN
21 CHINESE
19 EJND. 24 CAUCASWN
19 CAUCASWN
18 CAUCASUN
24 CHINESE 21 CAUCASUN
2.36 NO 3.00 NO
2.01 NO
2.46 NO
2 . 1 NO
1.n NO 2.0 t NO 2.11 NO
1.74 NO 2.32 NO
1.97 NO
2.78 NO 2.16 NO
1.86 YES 2.28 NO 2.04 NO 1.91 NO
2.01 YES 2.73 NO
1.76 NO
2.03 YES 1.83 YES 2.16 NO
1.88 NO
2.64 NO
1.67 NO
2.04 NO
2.3 1 YES 1.67 NO
3.20 Y 0
1.79 YES 1.97 NO
1.46 NO
2.65 NO 236 NO
243 NO
231 NO
3.62 .JO
2.29 NO
2.57 NO
2.06 NO
2.09 NO
1.48 NO
197 NO
1.97 NO
206 NO 1.63 NO
23s NO
3.07 NO

M E RACE 24 CAUW1AN 26 CAUCASIAN
22 CAUCASIAN
33 CAUCASIAN
26 CAUCASIAN
23 CHINESE 34 CAUCASIAN
34 CAUCASIAN 20 CAUCASIAN
20 CAUCASIAN 37 M. E S T 29 M. EAST
21 CAUCASIAN
21 CAUCASIAN 22 CAUCASIAN 47 CHINESE 43 CHMESE 17 CHMESE 16 CHXNESE
2.12 NO
2.28 NO 247 NO
2.67 NO
1.75 YES 1.83 NO 2.78 NO
2.09 NO
1.99 NO 1.72 YES
2.43 NO
2.44 NO
2.26 NO 2.06 YES
2.12 NO
2.17 NO
1.82 NO
2.08 NO
1.81 NO

Appendix 2.
Results from Appana (1 995) W/HT AL SMOKING COFFATA
SEX AGE RACE 37 CAUCASIAN 3s CAUCASIAH 39 CAUCASIAY 29 CAUCASIAN 44 CAUCASWN 31 CAUCASIAN 43 CAUCASIAN
20 CAUCASIAN 22 CAUCASIAN 34 CAUCASIAN 56 CAUCASMN
21 CAUCASIAN 23 CAUCASIAN 34 CAUCSfAN 27 CAUCASWN
23 CAUCASIAN 23 CAUCASIAN 42 CAUCMIiLV 23 CAUCASIAN 21 CAUCASIAN
28 CAUCASIAN 23 CAUCASUN 62 CHINESE 60 CHINESE
30 END 20 CHMESE 24 CHTNESE 27 CAUCASIAi
61 CAUCASIAN 47 CHmEsE 22 CHLNESE 21 CHINESE 32 CAUCASLW 18 CHDESE 24 CtiiNE!jE 19 CHINESE 23 CHINESE 27 CHINESE 32 CAUCASIAN 41 JAPANEsE 54 CHDIESE 23 CiiiNESE 24 CHINESE 21 CAUCASIAN 34 CAUCSWN 30 CAUCASWIV
2.73 YES 1.86 NO 2 3 NO
1.67 NO 220 NO 2.25 NO
2.5 1 NO 2.54 NO
2.64 NO 2.11 NO
2.13 Y 0 2.13 NO 2.63 NO 2.07 YES
2.03 NO
2.06 NO
2.55 NO 2.19 YES 2.18 YES 2.29 NO 2.24 NO 2.76 NO
1.88 NO
2.30 NO 2.17 NO
1.61 NO
2.39 NO 2.02 NO
2.55 YES 1.81 NO
8 NO
2.18 NO 2.67 NO
1.94 NO
210 N O
1.74 NO
2.06 NO
1.67 YES 2.63 NO
2-17 NO
2.87 NO 2.36 NO
2.28 NO
1.81 NO
1.83 YES 1.71 NO

SEX AGE RACE 63 CAUCAsL4N
35 CAUCASWN
64 CAUCASWN 29 LiND. 30 CAUCASLW 37 CAUCASIAN
21 CAUCMfAN
35 EIM). 35 Enm. 29 B MD. 26 CAUCASfAN 27 CAUCASIAii
26 CAUCASIAN 15 CHTNESE
63 CAUCAStAN
63 CAUCASIAN
69 CAUCASIAN 57 CAUCASLLY 64 CAUCASIAN
23 CHI?(ESE
22 CHINESE 26 CAUCASIAN
51 CHINESE 20 CHNESE 19 KORErlN
23 PHïtiPCNO 22 K 0 R E . W 26 CHINESE 45 CAUCASIAN
76 CWNE!X 31 C A K X S I M
20 CÂL'CASlrtV 52 CHMESE 27 CAUCSWN
22 CAUCAS1AN
31 CHINESE 37 CHINESE
25 CAUCSMN 34 CAUCASIAN
59 CÂUCrSSIrW 30 CAUCASWN
29 CAUCASIAN
31 CAUCA!3IAN
30 CAUCAStAN
62 CAUCSWN
60 CAUCASlAN
29 CAUCASIAN
31 CAUCASIAN
WTm (Iblbch) OC
2.27 NO 270 NO 2 . NO 2.17 NO 1.82 NO 2 3 4 NO 1.7 NO
2.27 NO
2.02 YES
1.97 NO 2.44
2.43 NO
2.52 NO 1.83 NO 2.46 NO
1.64 NO 2.21 NO
1.73 NO
2.36 YES
1.86 NO 1.65 NO
2.21 NO
2.34 NO 1.97 NO
2.37 NO
1.78 NO
2.21 NO 2.07 NO
1.95 NO
2.22 NO
1.83 YES
1.83 YES 2.36 NO
L.70 NO
2.00 YES
1.80 NO
1.88 NO
1-75 30 2.43 NO
2.42 NO 2.01 NO 1.67
2.25
2.03
237 NO
2.28 NO l.67
2.28

Appendix 3. Resuits of ASA genotyping assay. Gcnomic DNA uns loiDdly pmvidcd by Dr. Grant.
Subject
00 1NC 003CB OOJBP 007EV 013A.R OZOCB 029NJ 034AG 039TW 040SS 042DS 043PV OJIYA OJSSD 0~6m 047MC 048JG 049ED 052MS 053IR 054sv 055SJ 056RF 057AP 058KM 059MH O6 lDM 062KA 063DS 064LC 065BC 066ST 067TT 06SSH O7OB W 07 1BT 072MM 073K 071CB 075JL 076DM 077RS 082RW O83 CD 084CD
Race
C C C C C C M C C C C I C C O C
C C C
OC C C
C C C C C C C C C C I C C C C C C C C C C
Sex
F F M F F M F F F F M F F M F F
M F F F F F
M M F F F M M M M F F F F F M M M M F M F
Hctcrozygous Homozygous Homo ygous W iidtype Variant



Appendix 4.
Sequence cornparison between UGT2B7 and tlie otlier UGT2B subfamily niernbers in tlie 144 base pair stretcli amplified by P5 and P6. Note that the regions of the PS and P6 priniers are identical to the sequences of UGT2B7 and UGT2B4. Also note that ASA uses PS and either the variant or wildtype primers (PV, PW), and tliat the products produced by ASA is 5 base pairs shorter than the products produced by the P5 and P6 primers.
- + represents the 802 mutation site - * represents base pair difference from UGT2B7

Appendu 5. The sequence of the UGT2B4. P5 and P6 pnmers were used in a RT-PCR reaction on mRNA extfacted âom human liver tissue. The product was subcloned, transformecl, and then sequenced. The sequence matches the sequence of UGT2B4.
+ Position 723 on coding region
4-• Position 829 on coding region
C G T

Appendix 6.
Characteristics of the 8 individuals in the genotype-plienotype coniparative study.
S/R Ratio
1.38 1.17 1.38 1.81 2.20 2.98 4.67 3.05
Ami. of S-giuc.
42 1 172 240 587 235 N A 859 73 1
k1cc
Cliincse Caticasifin Caiicasian
Korcan Caiicasian Chinesc
Caucasian Caucasian
2.57 1.76 2.34 3 .O
2.24 2.36 1.92 2.28
LA-
Oral coiitraceplive
NO NO NO NO NO NO YES NO --
- NA: nd available