Policy & Procedures Manual for the Division of Infectious Diseases
119
Policy & Procedures Manual for the Division of Infectious Diseases University of Kansas School of Medicine Kansas City, Kansas Covering Policies and Procedures for Fellows In Training As a supplement to the House Staff Policy and Procedure Manual of the University of Kansas School of Medicine, Office of Graduate Medical Education And Program Manual for Residents in the Department of Medicine University of Kansas School of Medicine, Kansas City, Kansas Designed & Approved by the KUMC Infectious Diseases Education Committee (Committee of the Whole) Revised August 2011 Daniel Hinthorn, MD, Program Director Lisa Clough, MD, Associate Program Director Michael Luchi, MD, Associate Program Director Division of Infectious Diseases Department of Internal Medicine
Transcript of Policy & Procedures Manual for the Division of Infectious Diseases

Policy&ProceduresManualforthe
DivisionofInfectiousDiseasesUniversityofKansasSchoolofMedicine
KansasCity,Kansas
CoveringPoliciesandProceduresforFellowsInTraining
AsasupplementtotheHouseStaffPolicyandProcedureManualoftheUniversityofKansasSchoolofMedicine,
OfficeofGraduateMedicalEducationAnd
ProgramManualforResidentsintheDepartmentofMedicineUniversityofKansasSchoolofMedicine,KansasCity,Kansas
Designed&ApprovedbytheKUMCInfectiousDiseasesEducationCommittee
(CommitteeoftheWhole)
RevisedAugust2011
DanielHinthorn,MD,ProgramDirectorLisaClough,MD,AssociateProgramDirectorMichaelLuchi,MD,AssociateProgramDirector
DivisionofInfectiousDiseasesDepartmentofInternalMedicine
2
TABLEOFCONTENTS:
I. INTRODUCTION 4II. CONTACTINFORMATION 5III. INSTITUTIONALSUPERVISINGFACULTY 7IV. ACADEMIC
A. ProgramOverview 9B. MissionStatement 9C. DivisionGoals 9D. PerformanceExpectations 10E. Curriculum 14F. Conferences,LecturesandOtherEducationopportunities 22G. EvaluationofFellows 27H. Advancementtosucceedingtrainingyear 28I. EvaluationofFacultyandProgram 28J. DocumentationofTraining 29
V. POLICYANDPROCEDURES 30A. Prerequisites 30B. FellowshipSelectionProcess 30C. DurationofProgram 31D. Duties 31E. DutyhoursPolicyandFatigue 32F. CallSchedule 33G. LinesofCommunicationandResponsibilities 34H. MeetingAttendance 36I. VacationandLeaveTimePolicy 37J. Benefits 39K. Moonlighting 40L. Ethics 41M. UtilizationManagement 41N. QualityImprovement 41O. RiskManagement 42P. Professionalism 43Q. Impairment 44R. DisciplinaryActions,Probation,SuspensionandTermination 44S. GrievanceResolution 47
VI. APPENDIX…A. CoreCurriculumSchedule 49B. IDConferences 51C. ObjectivesbyCompetencies
1. YearOne 522. YearTwo 52
D. GoalsandObjectiveforRotations1. Inpatient 542. OutpatientClinics 58

3
3. Microbiology 654. Research 68
E. CoreCompetencyMatrix 71F. RequiredEvaluations 72G. Evaluations
1. FacultyofProgram 732. FacultyofFellow 763. FellowofFaculty 794. FellowofProgram 835. FellowofPeer 866. FellowSelfAssessment 897. PatientEvaluation 928. ResearchFacultyofFellow 939. SupportStaffofFellow 96
H. RecommendedReadingforFellows 98I. FellowHand‐OffPolicy 99J. GMECFatigue(Transportation/SwingRoom)Guidelines 100K. OnlineTrainingL. VanderbiltMatrix M. SupervisionTemplate
ThepurposeofthemanualistoconsolidateourrotationGoalsandObjectives,PoliciesandProceduresandCurriculumandtoprovideaguidetoformattingindividuallearningplansforourfellows.Additionalinformationwillbeaddedovertime.Versionnumbersanddatesreflectupdatestothemanual.

4
I.IntroductionWelcometotheInfectiousDiseasesDivisionattheUniversityofKansasSchoolofMedicine.WearepleasedthatyouhavechosenthisProgramtocontinueyourtraining.WebelievethatyouwillfindtheKUIDDivisiontobeanexcellentprogramwithatalentedanddedicatedfacultyeagertoprovideinstructionandguidancetoyouasyoucompleteyourtraining.Withinthisprogram,youwillencounterabroadarrayofinfectiousdiseasesthatwillallowyoutobecomeanexcellentconsultantinthediscipline.Additionally,webelievethatprofessionalism,ethicalstandardsandhumanisticqualitiesareparamounttothesuccessfulpracticeofmedicineandarefosteredwithinourprogram.Ourfacultysubscribestothe“leadbyexample”philosophy.Whenyoucompleteyourtraining,ourgoalandexpectationsarethatyouwillbeacompetent,compassionate,ethicalinfectiousdiseasesphysicianwhowillbealife‐longlearnerandadedicatedteacherforthenextgeneration,readytosolvenewproblemsanddisseminateinformationforotherstostudyandemulate.TheKUInfectiousDiseasesfacultyandIconsideritaprivilegetoworkwithyou,thephysiciansofthefuture,andwetakeourcontributionstoyoureducationseriously.Myexpectationsarethesameforyouaswellasforourfaculty:acommitmenttoexcellenceinclinicalcare,education,andresearch,coupledwithazestforlife‐longlearning.Welookforwardtoworkingwithyouandhaveeveryconfidencethatyouwillgraduateasacompetent,confident,compassionatephysician.Youhavemanyexcitingopportunitiesahead,andwewelcometheopportunitytosharethemwithyou.
DanielR.Hinthorn,M.D.,FACP,FIDSAProfessorofMedicine,Pediatrics,andFamilyMedicineDirector,DivisionofInfectiousDiseases

5
II.ContactInformationInfectiousDiseasesFacultyDivisionofInfectiousDiseases‐KUMCDanielHinthorn,M.D.–Director,ProfessorofMedicine,Pediatrics(hon.),andFamilyMedicine(hon.)MichaelLuchi,M.D.,AssociateProfessorChienLiu,M.D.(EmeritusProfessorofMedicineandPediatrics)AlbertEid,M.D.,AssociateProfessorStephenWaller,MD,AssistantProfessorLisaClough,M.D.,AssistantProfessorFernandoMerino,MD,AssistantProfessorKassemHammoud,MD,AssistantProfessorWissamElAtrouni,MD,AssistantProfessorNitaGanguly,MD,AssistantProfessorDanaHawkinson,MD,AssistantProfessorDivisionofInfectiousDiseases‐KCVAMCVinuthaKumar,M.D.,AssistantProfessorArundhatiDesai,MD,AssistantProfessorDivisionofInfectiousDiseases‐ResearchMedicalCenterDavidMcKinsey,M.D.,ClinicalProfessorJoelMcKinsey,MD,ClinicalProfessorPaulBrune,MD,ClinicalAssistantProfessorAssociatedFaculty:DivisionofPediatricInfectiousDiseases‐KUMCWilliamKeough,MD,AssistantProfessorDepartmentofPharmacyPractice‐InfectiousDiseaseSpecialistsAmberSawyer,Pharm.D.DepartmentsofClinicalMicrobiologyLaboratoryRebeccaHorvat,Ph.D.‐Director,ClinicalMicrobiologyLaboratoryDepartmentofPreventiveMedicineTomD.Y.Chin,M.D.,M.P.H.(EmeritusProfessor)StanleyEdlavitch,PhD,ProfessorofEpidemiologyandPreventiveMedicineHospitalInfectionControlandPreventionShawnMueller,RN,InfectionPreventionandControlmanagerSupportStaffoftheIDDivisionJudithSpeer,BBA,DivisionAdministratorKendraColburn,OfficeSecretary

6
JennyWest,RN,OPATCoordinatorAmyStewart,RN,OPATCoordinatorStacyMcCrea‐Robertson,MS,MT,ResearchCoordinatorMeaganMcDade,LPN,ClinicCoordinatorDianaZarco,RN,ClinicNurseKarenLane,PatientServicesRepresentative

7
III.InstitutionalSupervisingFacultyKUHospital(KUH)andKUMC:SponsoringInstitutionDirector&SiteDirector:DanielHinthorn,MD(20hrseachweek)Supervisoroffellowonconsultationservice:AttendingassignedtoprimaryserviceSupervisoroffellowonclinicrotation:AttendingassignedtocliniconsamedaySupervisoroffellowonresearchrotation:Director,LisaClough,MDKansasCityVeteransAdministrationMedicalCenter(KCVAMC)SiteDirector:VinuthaKumar,MDSupervisoroffellowonconsultationservice:AttendingassignedtoprimaryserviceSupervisoroffellowonclinicrotation:AttendingassignedtocliniconsamedayResearchMedicalCenter(RMC)SiteDirector:DavidMcKinsey,MDSupervisoroffellowonconsultationservice:AttendingassignedtoprimaryserviceSupervisoroffellowonclinicrotation:AttendingassignedtocliniconsamedayKeyClinicalFaculty,teachingfaculty(10hrseachweek)Requirements:broadknowledgeofandexperiencewithID,ABIMcertified,scholarlyactivity(definedasSectionV.E.)DanielHinthorn,MD,DivisionDirector,FellowshipDirector,ViceChairofMedicineMichaelLuchi,MD,AssociateFellowshipDirectorLisaClough,MD,AssociateFellowshipDirectorWissamElAtrouni,MDKassemHammoud,MDNitaGanguly,MDFernandoMerino,MDStephenWaller,MDAlbertEid,MDDanaHawkinson,MDArundhatiDesai,MDVinuthaKumar,MDDavidMcKinsey,MDJoelMcKinsey,MDPaulBrune,MDKeyClinicalFacultyClinicalInvestigators(10hrseachweek)Requirements:publicationsinpeerreviewedclinicaljournals,&responsibleforplanning,implementing,monitoringandevaluationoffellow’sclinicalandresearchtraining.KUHospital(KUH)andKUMCLisaClough,MDAlbertEid,MDWissamElAtrouni,MD

8
NitaGanguly,MDKassemHammoud,MDDanaHawkinson,MDDanielHinthorn,MDMichaelLuchi,MDFernandoMerino,MDStephenWaller,MDKansasCityVeteransAdministrationMedicalCenter(KCVAMC)ArundhatiDesai,MDVinuthaKumar,MDResearchMedicalCenter(RMC)DavidMcKinsey,MDJoelMcKinsey,MDPaulBrune,MD

9
IV.AcademicA.ProgramOverview:TheInfectiousDiseasesFellowshipTrainingProgramattheUniversityofKansasisatwo‐yearprogramdesignedtotrainoutstandingcliniciansininfectiousdiseaseswhowillhavetheskillsandknowledgetosucceedineithertheacademicorprivatehealthcaresectors.Athirdyearoftrainingismadeavailableinexceptionalcasesinwhichthefellowistraininginresearchtechniquesinpreparationtoacceptafacultyposition.Thetrainingprogramutilizesthreetrainingsites:TheUniversityofKansasMedicalCenter,KansasCityVeteran’sAdministrationMedicalCenterandResearchMedicalCenter.Theeducationalrationaleforpresenceateachtrainingsiteiscarefullyconsidered.ClinicalexperienceattheUniversityofKansasHospitalprovidesopportunitiesforfellowstolearnunderthementorshipofbothclinicalinvestigatorsandmedicaleducators,whilecaringforapatientpopulationwhichincludestertiarycarereferralsfromphysiciansthroughouttheregion,aswellaslocal,culturallydiversepopulations.OureducationalaffiliationwiththeKansasCityVAMedicalCenterisdesignedspecificallytoexposefellowstoapracticesettingwithincreasedautonomy,yetadequatefacultysupervision,andapatientpopulationwithadifferentspectrumofdiseasethanouruniversityhospital.ExperienceatResearchMedicalCenteremphasizescarewithininalargemetropolitanhospitalbasedprivateInfectiousDiseasespractice.Thissettingisdesignedtoexposefellowstoapracticeenvironmentthatisrepresentativeofhealthcaresystemsinmanycities.B.MissionStatementThemission of the Division of Infectious Diseases at the University of Kansas School ofMedicine aligns closely with the overall mission of the Department of Medicine. Ourprimarymissionistoprovideaneducationalenvironmentconducivetopreparationforalifetimeofstudy,problemsolving,andcriticaldecisionmakinginthepracticeofInfectiousDiseases. The fulfillmentofoureducationalmissionrequires theprovisionofexemplaryclinicalservices.ThemissionoftheInfectiousDiseasesFellowshipProgramistodevelopandfosterexcellenceinpostgraduatetraininginInfectiousDiseasesbyeducatingfellowstobeoutstandingpractitioners,lifelonglearners,criticalthinkers,andpatientadvocates.TothisaimtheProgramseeksto:1.FostermaximumdevelopmentofeachfellowinthecorecompetenciesofinternalmedicinewhichincludePatientCare,MedicalKnowledge,Practice‐BasedLearningandImprovement,InterpersonalSkillsandCommunication,Professionalism,andSystems‐BasedPracticeastheyapplytoInfectiousDiseases;2.Developmeasuresdesignedtoimprovedeficienciesandassessprogressiontowardmasteryineachofthesixdefinedcorecompetences;3.Fosteracommitmenttoacademicachievementbyemphasizingtheimportanceofresearchandinvestigationbothasacareerchoiceandasameansofincorporating

10
principalsofcriticalthinkingintoeachfellow’sclinicalpractice,continuingeducationandprofessionaldevelopment.C.DivisionalGoalsGoalsforFellowscompletingtheKUInfectiousDiseasesFellowshipprograminclude:
1. To obtain clinical competence by experiencing comprehensive training in both inpatient and outpatient setting of the clinical features, diagnosis, natural history, prevention and treatment of a broad range of infectious diseases.
2. To acquire a knowledge base and cognitive skills to be an effective independent consultant and practitioner of the discipline of Infectious Diseases.
3. To acquire,andmaintaintheprofessionalism,ethicalstandardsandhumanisticqualitiesrequiredtobeaneffective,respectedphysician.
4. Toprovideeducationtoothers,includingpatients,otherhealth‐careworkers,andphysicians,andtodosowithhumilityandcompassion.
5. To develop personal life-long learning skills,includingsystemizedassessmentofpatientcarepracticesandimprovementinpracticebasedonscientificevidenceasappliedtotheassessment.
6. Tohaveabasicknowledgeofqualityassurance,qualityimprovementandeconomicsinreferencetoone’sindividualpracticeofinfectiousdiseasesaswellasthehealthcaresystem.
7. Toobtainabasicunderstandingofcriticalreviewofmedicalliterature,researchdesign,informedconsent,ethicsinresearchandcommunicationofresearchresults.
8. Tobecome a graduate who is competent, compassionate, and is successful in becoming a board eligible and board certified physician in Infectious Diseases.
D.PerformanceExpectations
TheAccreditationCouncilforGraduateMedicalEducation(ACGME)hasidentifiedsixareasofcompetencytobetaughtandevaluatedbyfellowsoverthecourseoftheirtraining.TheprogramprovidesaunifiedexperiencethatallowsfellowstodevelopexcellenceinthecompetenciesspecifiedbytheACGMEastheyapplytothespecialtyofInfectiousDiseases.Thiscurriculumpresentstheobjectives,educationalactivities,evaluationtoolsandclinicalrotationswithintheframeworkofthesesixcompetencies.
1. PatientCareFellowsareexpectedtoprovidecarethatiscompassionate,appropriate,andeffectiveforthepromotionofhealth,preventionofillness,treatmentofdisease,andcareattheendoflifetopatientsofeachgenderfromadolescencetooldage.Specifically,thisrequiresthatafellowbecompetentinthefollowingareas:
a. Gatheraccurate,essentialinformationfromallsources,includingmedicalinterviews,physicalexamination,records,anddiagnostic/therapeuticprocedures.
b. Makeinformedrecommendationsaboutpreventive,diagnostic,andtherapeuticoptionsandinterventionsthatarebasedonclinicaljudgment,scientificevidence,andpatientpreferences.

11
c. Develop,negotiate,andimplementpatient‐focusedmanagementplansemphasizingtheappropriateuseofantimicrobialagents.
d. Performcompetentlythediagnosticproceduresconsideredessentialtothepracticeofinfectiousdiseases.
EducationalActivitiesExposuretotheentirerangeofcasesininfectiousdiseasesincludingregularlyencounteredinpatientandoutpatientinfectionsandspecialsituationincludingHIV/AIDS,impairedhosts,nosocomialinfections,sexuallytransmittedinfections,illnessesoftravelersandtheepidemiologyofinfectiousdiseaseswillbeprovided.Avarietyofpatientcenteredexperiencesinclude:InpatientConsultation,OutpatientClinic,CaseConference,CurriculumConference,ClinicalMicrobiologyConference,AntibioticCommittee,InfectionControlCommitteeandJournalClub.
EvaluationtoolsDailydirectobservationbyattendingphysician,360‐degreeevaluation,chart‐stimulatedrecall,periodicobservationtoolssuchasmini‐clinicalevaluation(mini‐CEX),andsimulationoftherapeuticdecisionmaking.
2. MedicalKnowledge
Fellowsareexpectedtodemonstrateknowledgeofestablishedandevolvingbiomedical,clinical,andsocialsciences,anddemonstratetheapplicationoftheirknowledgetopatientcareandeducationofothers.Specifically,thisrequiresthatafellowbecompetentto:
a. Applyanopen‐mindedandanalyticalapproachtoacquiringnewknowledge.b. Developclinicallyapplicableknowledgeofthebasicandclinicalsciencesthat
underliethepracticeofInfectiousDiseases.c. Applythisknowledgeindevelopingcriticalthinking,clinicalproblem‐
solving,andevidence‐basedclinicaldecision‐makingtothedifferentialdiagnosisandcomplexmanagementofpatientswithinfectiousdiseases,includingthosewithregularlyencounteredinpatientandoutpatientinfections,andspecialsituationssuchasHIV/AIDS,impairedhosts,nosocomialinfections,antibiotic‐resistanceinfectionsandthoseinfectedwithneworemergingpathogens.
d. Accessandcriticallyevaluatecurrentmedicalinformationandscientificevidenceandmodifyknowledgebaseaccordingly.
e. UnderstandpatientconfidentialityandHIPPAregulations. EducationalActivities Directpatientcareinavarietyofsettingswillincludethefollowing:Inpatient
consultation,OutpatientClinic,CaseConferences,JournalClub,ResearchConference,ClinicalMicrobiologyRounds,InfectionControlCommittee,AntibioticCommittee.AppropriateuseofthemedicalliteraturethroughEMRandlibrarylinkedresources.
Evaluationtools:In‐servicetrainingexamination,chartstimulatedrecall,directobservationbyattendingphysician,conferenceattendanceandpresentation.

12
3. Practice‐BasedLearningandImprovement:Fellowsareexpectedtobeabletousescientificmethodsandevidencetoinvestigate,evaluate,andimprovetheirpatientcarepractices.Specifically,thisrequiresthatafellowbecompetentasfollows:
a. Identifyareasforimprovementandimplementstrategiestoimprovetheirknowledge,skills,attitudes,andprocessesofcare.
b. Analyzeandevaluatetheirpracticeexperiences,setlearningandimprovementgoalsandimplementstrategiestocontinuallyimprovetheirqualityofpatientpractice.
c. Developandmaintainawillingnesstolearnfromerrorsanduseerrorstoimprovethesystemorprocessesofcare.
d. Useinformationtechnologyorotheravailablemethodologiestoaccessandmanageinformationandsupportpatientcaredecisionsandtheirowneducation.
e. Facilitatethelearningofpatients,families,studentsandotherhealthcareprofessionals.
EducationalActivitiesCriticalevaluationofpracticeexperienceandperformancewilloccurthroughInpatientConsultationrounds,Outpatientclinics,CaseConference,CurriculumConference,JournalClub,ResearchConference,In‐servicetrainingexamination,OPATprogram,libraryandlinkedresourcesof“bestpractices”anduseoftheEMR.
Evaluationtools360degreeevaluation,continuityclinicQIprojects,IDCaseConferenceandDepartmentofMedicinePatientSafetyConferenceparticipationutilizingtheVanderbiltPatientHealthcareMatrix,directobservationandEMR.
4. InterpersonalSkillsandCommunication:
Fellowsareexpectedtodemonstrateinterpersonalandcommunicationskillsthatenablethemtoestablishandmaintainprofessionalrelationshipswithpatients,familiesandothermembersofhealthcareteams.Specifically,thisrequiresthataresidentbecompetentto:
a. Provideeffectiveandprofessionalconsultationtootherphysiciansandhealthcareprofessionals.
b. Interactwithconsultantsinarespectfulandappropriatefashion.c. Sustainethicallysoundprofessionalrelationshipswithpatients,their
families,andcolleagues.d. Useeffectivelistening,nonverbal,questioning,andnarrativeskillsto
communicatewithpatientsandfamiliesacrossabroadrangeofsocioeconomicandculturalbackgrounds.
e. Maintaincomprehensive,timely,andlegiblemedicalrecords.
EducationalActivities
13
Throughexperienceininpatientandoutpatientsettingsincludingrounds,clinics,OPATprogram,fellowswilllearnandpracticecommunicationsskillswithpatients,familiesandprofessionals.ThroughpresentationsinavarietyofconferencesincludingResearchConference,CaseConference,CurriculumConference,JournalClubfellowswilldevelopwrittenandoralcommunicationskills.
EvaluationTools360‐degreeevaluations,observedclinicalevaluationskills(OCES)withfacultyfeedback,mini‐CEX,mentoredself‐reflectionduringsemi‐annualevaluations,chartreview.
5. Professionalism:
Fellowsareexpectedtodemonstratebehaviorsthatreflectacommitmenttocontinuousprofessionaldevelopment,ethicalpractice,anunderstandingandsensitivitytodiversityandaresponsibleattitudetowardtheirpatients,theirprofessionandsociety.Specifically,thisrequiresthataresidentbecompetentinthefollowingways:
a. Demonstraterespect,compassion,integrity,andaltruismintheirrelationshipswithpatients,families,andcolleagues.
b. Demonstratesensitivityandresponsivenesstopatientsandcolleagues,includingbutnotlimitedtodiversityingender,age,culture,religion,sexualorientation,socioeconomicstatus,beliefs,behaviors,anddisabilities.
c. Adheretoprinciplesofconfidentiality,scientific/academicintegrity,andinformedconsent.
d. Recognizeandidentifydeficienciesinpeerperformance.e. Bepersonallyawareoflimitations,excessivestress,fatigue,burn‐out,or
depressionandknowwhenandfromwhomtoseekguidance.EducationalActivitiesAllacademicandclinicvenueswillprovideexperiencetopracticeprofessionalism.Clinicalvenueswillprovideanopportunitytodealwithpatientsofmanyages,ethnicitiesandvaryingdegreesofimpairment.Intellectualintegrityisemphasizedinallsettings,includingtheclinic,theconferenceroomandresearchopportunities.
EvaluationTools360‐degreeevaluations,presentationskillsevaluationandfeedback,mentoredself‐reflection,conferenceattendancetracking,medicalrecordcompliance.
6. Systems‐BasedPractice:
Fellowsareexpectedtodemonstrateanunderstandingofthecontextsandsystemsinwhichhealthcareisprovided,anddemonstratetheabilitytocalleffectivelyonotherresourcesinthesystemtoimproveandoptimizehealthcare.Specifically,thisrequiresthataresidentbecompetenttodothefollowing:
a. Understand,access,andutilizetheresourcesandprovidersnecessarytoprovideoptimalcare.
14
b. Understandthelimitationsandopportunitiesinherentinvariouspracticetypesanddeliverysystems,anddevelopstrategiestooptimizecarefortheindividualpatient.
c. Incorporatecost‐awarenessandriskbenefitanalysistopresentation,diagnosis,anddiseasemanagement.
d. Advocateforqualitypatientcareandoptimalpatientcaresystemse. Workininter‐professionalteamstoenhancepatientsafetyandimprove
patientcarequalityincludingtransitionofcarebetweensettings
EducationalActivitiesOpportunitiestodevelopanawarenessandresponsivenesstothehealthcaresystemwillbeavailableinallsettingsincluding:InpatientConsultation,OPATprogram,InfectionControlandPreventionandOutpatientclinic,inparticularthefellow’sHIV/AIDSclinic.Thesesettingswillserveasvenueswheretheywillcoordinateinterdisciplinarycarebyarangeofmedicalandnon‐medicalspecialists.Theywillutilizecomponentsofthelocalandnationalhealthcaresystemsandoptimizecoordinationofpatientcarebothwithinone’sownpracticeandwithinthehealthcaresystem.
EvaluationTools360evaluations,QIprojects,chartstimulatedrecall,IDCaseConferenceandInternalMedicinePatientSafetyConferenceparticipationutilizingtheVanderbiltpatientHealthcareMatrix,semi‐annualcontinuityclinic,QIproject.
E.CurriculumTheDivisionhasestablishedrotationalgoalsandobjectivesforallaspectsofitsfellowshipeducationandtrainingwhichisavailabletothefellowsandfacultyforreviewonourwebsite.Thecurriculumcontainsalistofobjectivesforeachleveloftraining.Theselearningobjectivesaremeanttobetheminimumachievedwhileoneachservice.Asummarytableofrotationalgoalsandobjectivesisprovidedintheappendix.YearOneFellowshipInfectiousDiseaseConsultationServicesTrainingSites:KansasUniversityHospital(KUH),KansasCityVeteransAdministrationMedicalCenter(KCVAMC),ResearchMedicalCenter(RMC).
FirstyearfellowsparticipateintheInfectiousDiseaseConsultationServicefor12rotationsofonemontheach.Atthediscretionofthefellowshipdirector,2weeksfromaclinicalrotationmaybegrantedduringofthefirstyeartoorganizeandsubmitaclinicalresearchprojecttotheInstitutionalReviewBoard.FellowsrotatebetweenKUH,KCVAMCandResearchMedicalCenterproviding6monthsconsultserviceKUHand3monthseachconsultserviceatKCVAMCandRMC.WhileatKUH,fellowsrotateonamonthlybasisamongfourgeneralIDconsultativeservices.WhileatKCVAMCandRMCfellowsareassignedtothegeneralIDconsultativeservice.

15
Ateachparticipatingtrainingsite,thefellowisresponsibleforallactivitiesoftheinpatientconsultservice.Theyevaluateanddiscusseachpatientwiththeprimaryservice,viewradiographicstudieselectronically,reviewthelaboratorystudiesandmicrobiologyandimmunologyresults.Oftenthiswillinvolveconsultationwiththemicrobiologylaboratory.ThefellowprepareseithertheconsultationreportordailyprogressnoteandpresentsthepatientandfindingstotheIDconsultantattending.Togethertheyinterviewandexaminethepatient,reviewanddiscussthelaboratoryandmicrobiologyresults.Thefellowpresentshisorherassessmentofproblemsanddiagnosesandmanagement,whichtheattendingreviews,critiques,andmodifies.Eachpatientisseendailyonattendingrounds.Bedsideteachingbytheattendingisintegraltodailyrounds.Theattendingandfellowseeallconsultationsonthesamedayaswhentheconsultationisordered.TheDivisiondiscouragescurbsideconsultsandrequestsformalreviewbythefacultyandfellow.
Fellowsarerequiredtocontacttheattendingoftheirserviceforanyareaofdiagnosticortherapeuticuncertainty,andbeforetheymakeevenpreliminaryrecommendationsinsuchcases.Ifquestionsariseafterhours,onefacultypersonisoncallforsuchtelephonecalls24hourseveryday.FellowsareencouragedtocalltheDirectoratanytimeifadditionalquestionsarise.
Fellowsarealsoresponsiblefortheorganizationanddirectorshipofotherlearners,includingInternalMedicineresidentsandmedicalstudentsthatmayberotatingontheconsultativeservice.Fellowsshouldmeetwiththelearnerspriortoformalrounds,reviewwork‐upandpresentationsandofferinstructionasappropriate.Fellowsarealsoexpectedtoprovidebriefformallecturescoveringbasicinfectiousdiseaseprinciplesonaroutinebasis.Facultyshouldbeavailabletocontributetotheseteachingsessions.
IDconsultationsatKUHarefromallmedicalandsurgicalservicesincluding:generalmedicineandeachofthemedicalandsurgicalsub‐specialists,familyandcommunitymedicine,ICUs,Level1traumaforgeneral,neurologicalandorthopedicservices,hematology&oncology,burn,stemcellandsolidorgantransplant,obstetricsandgynecology,emergencymedicine,pediatrics,geriatrics,palliativeandrehabilitationmedicine.
ConsultationsatRMCandKCVAMCarefromallmedicalandsurgicalservicesincludingICU.KCVAMCofferstheadditionalopportunitytoseepatientswithmilitaryexperiencewhomaybereturningfrominternationalconflicts,andtheuniqueinfectionsassociatedwiththeseexperiences.
EachfellowisassessedastohowwelltheydemonstrateknowledgeofIDliterature,obtainacompletehistory,performappropriateexaminationandmakecogentassessments.Thefellowisevaluatedaswhetherheorshehascollectedclinicalinformationinarespectful,thorough,andcompletemannerandwhetherheorshehasbeenabletogivealogicalpresentationwithappropriateassessmentandrecommendations.Theactivitiesofthefellowareevaluatedforethicalandprofessionalconduct.Fellowevaluationsareinformallymadeverballyonanongoingbasisthroughouttheclinicalrotationandformallyinwrittenandverbalformatatthecompletionoftherotationasdescribedbelow.
Theprogramdirectorandchieffellowmakeupthecallschedulewithattentiontogivingeachfellowatleastonedayoffeverysevendays.Onserviceswherethereisonlyonefellow,atRMCandKCVAMC,fellowsarealwaysgivenonedayoff(includingbeepercall)eachsevendaysaveragedoveronemonth.
16
ObjectivesfortheFirst‐yearFellowonInpatientConsultativeServices
a. Demonstrateabilitytogatherdata,orderdiagnostictests,interpretdata,makediagnosticandtherapeuticdecisions.
b. DemonstrateabilitytoperformandinterpretGramstains.c. Demonstrateabilitytomanagepatienttherapiesemphasizingappropriateuseof
antimicrobials.d. Workwithotherstoprovidepatient‐focusedcare.e. Demonstratecompetenceinthediagnosisandmanagementofinfectiousdisease
areasincluding:Bacterialinfections,Fungalinfections,Viralinfections,HIV/AIDS,Parasiticinfections,Sepsissyndromes,Infectionsinpatientswithimpairedhostdefenses,Infectionsinpatientsinintensivecareunits,Infectionsinsurgicalpatients,Healthcare‐associatedinfections,Infectedtravelers,Sexuallytransmittedinfections,Prostheticdeviceinfections.
f. Demonstrateknowledgeofinfectioncontrolandhospitalepidemiology.g. Understandtheprinciplesofprophylaxistoenhanceresistancetoinfections.h. RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS.i. ManagecommonandcomplexIDproblemsinthefaceofantibioticresistance.j. Understandthefundamentalsofhostdefenseandmechanismsofmicroorganism
pathogenesis.k. Understandthecharacteristics,useandcomplicationsofantiretroviralagents,
mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents.l. Demonstratecomprehensiveknowledgeofindications,contraindications,
limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
m. Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents.
n. Demonstrateknowledgeofantimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds.
o. Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsinthehospitalandnonacutecareunits.
p. Developskillstoappraisethecurrentmedicalliteraturetosupportdecision‐making.q. Developcommunicationskillstofacilitatethelearningofothers.r. Useeffectivelistening,narrative,andnon‐verbalskillsandwritelegibleand
comprehensivenotes.s. Beresponsivetopatientsandsocietyneedssupersedingself‐interest.t. Demonstrateintegrity,honesty,reliability,cooperative,andacceptresponsibility.u. Workwithhealthcareprofessionalstoprovidepatientfocusedcare;advocatefor
qualitypatientcare.v. Workininter‐professionalteamstoenhancepatientsafetyandimprovepatient
qualityofcare.w. Demonstrateahighstandardofethicalbehavior,includingabilitytomaintain
professionalrelationshipswithotherphysiciansandabilitytoavoidconflictsofinterest.
x. Participateinscholarlyactivitiesincludingpresentationatjournalclub,case

17
conferences,IDcorelectures.
EducationalActivitiesInadditiontodirectpatientcare,educationalobjectivesaremetthroughaseriesofcase‐based,smallgroupinteractivediscussion,problem‐orientedreading,role‐modelingbyexperiencedfacultyandhealthsystempersonnel,interactionwithotherhousestaffandfacultyandself‐directedstudy.InfectiousDiseasesClinicsTrainingsites:KUH,KCVAMC
FirstyearfellowsparticipateintheInfectiousDiseases/HIVClinicatKansasUniversityHospital.Fellowsarerequiredtohaveone½daycontinuitycliniceachweekatKUH.Thisclinicprovidesanopportunitytoseeavarietyofoutpatientambulatoryinfectiousdiseasesconsults,hospitalfollow‐up,OPATandpatientswithHIV.Fellowsareexpectedtocontinuouslyfollowaminimumof20HIVpatientsinthisclinic.Duringtheclinic,thefellowinitiallyevaluateseachpatient,andpresentsthecasetotheattendingphysicianwhoconfirmsthehistoryandthephysicalfindingsandwiththefellowdevelopsaplanofmanagement.Underthedirectionofafacultymember,eachfellowdealswithissuesofcomplexantibioticmanagement,antimicrobialresistance,antiretroviraltherapy,analysisofgenotypesofHIV,prophylaxisandmanagementofopportunisticinfectionsandthesocialandfinancialaspectsofcasemanagement.Inaddition,fellowslearntoworkwiththehealthcareteamincludingnurses,pharmacists,andsocialservicecasemanagers
WhenrotatingattheKCVAMC,thefellowsattendtwoHIVclinicseachweek.ThisprovidesfellowswithanopportunitytoexperienceabroaderrangeofHIVinfectedpatientsandexposuretothevariousmanifestationsandcomplicationsofthisdisease.
Fellowsareassessedonhowtheyperforminclinicusingthecorecompetencycomputerbasede*valueevaluationonamonthlybasis.
ObjectivesfortheFirst‐yearFellowinOutpatientClinicsa. Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;make
diagnosticandtherapeuticdecisions.b. Managemedicalandpsychosocialaspectsofcommonandcomplexoutpatient
infectiousdiseases.c. Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
including:Bacterialinfections,Fungalinfections,Viralinfections,HIV/AIDS,Parasiticinfections,Infectionsinpatientswithimpairedhostdefenses,Infectionsinsurgicalpatients,Healthcare‐associatedinfections,Infectedtravelers,Sexuallytransmittedinfections,Prostheticdeviceinfections.
d. Developskillintheuseofantimicrobialandprophylacticagents.e. DemonstrateunderstandingofHIVinfectionincludingantiretroviraltherapy,genotype
resistanceprofiles,prophylaxisandmanagementofopportunisticinfections,andnon‐medicalofcasemanagementandfinancialandpsychosocialissues.

18
f. Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
g. Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents,antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds.
h. Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsintheoutpatientclinicsetting.
i. Appraisethemedicalliteratureregardingoutpatientcaretosupportdecisionmakingj. Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleand
comprehensivenotes.k. Beresponsivetoneedsofpatientsandsocietysupersedingself‐interest.l. Demonstraterespect,compassion,andintegrity;behonest,reliable,cooperative,and
acceptresponsibility.m. Workwithhealthcareprofessionalseffectivelytoprovidepatientfocusedcareand
advocateforqualitypatientcare.n. Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientquality
ofcare.ClinicalMicrobiologyLaboratoryTrainingSites:KUH,KCVAMC,RMC
ThemicrobiologylabsatKUH,KCVAMCandRMCarefully‐equipped,stateoftheartclinicalmicrobiologylabswhichuseup‐to‐datediagnosticequipmentfortheidentificationofbacteriaanddeterminationoftheirantimicrobialsusceptibility.Thelaboratoriesalsomaintainequipmentnecessaryforthepurposeofculturing,detecting,identifyingandcharacterizingbacteria,fungi,virusesandmycobacterium.TheKUHlaboratoryisequippedwithaSmartCyclerforPCRandBiosafetylevel2and3workareas.
FellowsattendClinicalMicrobiologyRoundstwodaysperweekatKUH.Roundsareattendedbyfellows,residents,andstudentsrotatingonIDservice,IDfaculty,clinicalmicrobiologydirectorandlaboratorytechnologists.Topicsofinstructionincludebasictechniquesinculturing,identificationandsusceptibilitytesting,presentationofroutinecases,aswellasdiscussionofunusual,butimportantpathogensthathavebeenidentifiedinthelaboratory.
ClinicalMicrobiologyRoundspromotetraininginbasicandadvancedclinicalbacteriology,mycology,virology,parasitology,antimicrobialsusceptibilitytesting,immunology,mycobacteriology,advancemoleculardiagnosticsandmedicalgenetics.Communicationandprofessionalismskillsareemphasizedbyprovidinginteractionswithotherhealthsystemproviders.
Patientsimulationinvolvesapplicationofspecimenspresentedtohypotheticalpatientswiththispathogeninfectinganyanatomicsite.Fellowsareexpectedtodiscusshowdiagnosisandmanagementwouldbemodifiedbyalternatefactors
ObjectivesfortheFirst‐yearFellowinClinicalMicrobiologyLaboratory

19
a. Becomefamiliarwiththetechnicalaspectsofpathogenisolation,sensitivitytestingandmolecularmethods.
b. Developcommunicationskillstofacilitatethelearningofothers.c. Communicateclearlywiththemicrobiologystaff.d. Workwithmicrobiologystaffandclinicalservicestoprovideamultidisciplinary
approachtothediagnosisandtreatmentofinfections.e. Demonstratehonesty,integrityandreliability.f. Appraisethemedicalliteraturetosupportdecisionmaking.g. Workwiththemicrobiologystaffandclinicalserviceteamstoenhancepatient
safetyandimprovepatientqualityofcare.ResearchTrainingsite:KUH
Firstyearfellowsareexpectedtoidentifyafacultymentorandresearchprojectearlyintheirfirstyear.Thisallowsthemtheopportunitytoadequatelyplanstudyobjectives,methods,datacollectionandbiostatisticalanalysis.FellowswillpresenttheirproposedresearchprojectatthemonthlyIDResearchmeetingduringtheirfirstyear.Thismeetingisattendedbyfellows,faculty,andinterdepartmentalcontributorsandprovidesavenueforcriticalappraisaloftheproject.Fellowswillsubmittheirprojectforinstitutionalreviewboard(IRB)reviewwhenappropriateandapprovalduringtheirfirstyear.
Duringthisyear,fellowsareencouragedtocompletetheweb‐basedversionoftheSchoolofMedicineIntroductiontoClinicalResearchCourse.Coursematerialcanbeaccessedathttps://www.kumc.edu/som/facdev/researchers.html.Thisisa16‐sessioncoursedesignedtoprovideabasicandbroadoverviewtoclinicalresearch.FellowsarerequiredtocompletetrainingandcertificationinHumanSubjectProtectionandHIPPA(HealthInsurancePortabilityandAccountabilityAct)andhavetheopportunitytoparticipateassub‐investigatorsonthedivisionssponsoredclinicalresearch.FellowsattendthemonthlyIDResearchConference.Thisconferenceprovidesavenueforfacultyandfellowstopresenttheirongoingresearchprojectsandgenerateideasforfutureresearch.Attendancefromcollaborativepartnersoutsidethedivisionisstronglyencouraged.ObjectivesfortheFirst‐yearFellowonResearch
a. Learnthebasicprinciplesofresearchincluding:studydesign,outcomemeasures,appropriatestatisticalmodeling.
b. Demonstratecompetenceinformulatingatestablehypothesis.c. Provideawrittendescriptionoftheirproposedprojects.d. LearnabouttheIRBapprovalprocessandwhatapprovalsarenecessaryforspecific
projecttypes.e. SuccessfullygainIRBapprovalforallprojectsinvolvinghumansubjects.f. SuccessfullygainIACUCapprovalforallprojectsinvolvinganimals.g. Understandtheissuessurroundingappropriatetreatmentofresearchsubjects.h. Demonstratecompetenceinsummarizingdatainabstractsforpresentationat
regionalandnationalmeetings.

20
i. Demonstratecompetenceinposterororalpresentationpreparationforanationalmeeting.
j. Learntheconstructionofstudieswhichadequatelystresstheethicsofclinicalresearch,protectionofhumansubjectsandobtainingeffectiveinformedconsent
k. Communicateinterimresultstofaculty.l. Demonstratecompetenceinevaluatingrelevantliteraturerelatedtoaspecific
researchquestion,includingtypeofresearchmodelandevaluationoftheappropriateuseofstatistics.
m. Learntorecognizeandmakecontingencyplansforpotentialproblemsinaresearchplan.
n. Demonstratetheabilitytounderstandhowclinicalandbasicscienceresearchresultsinfluenceclinicalpractice.
o. Developcommunicationskillstofacilitatethelearningofothers.
YearTwoFellowshipInfectiousDiseaseConsultationServicesTrainingSites:KUH,KCVAMCSecondyearfellowsparticipateintheInfectiousDiseaseConsultationServiceforninerotationsofonemontheach.WithapprovaloftheFellowshipDirector,DivisionDirector,&DivisionalResearchDirector,sixtoninemonthsofclinicalconsultationservicemaybecompletedinordertoprovideadditionalmonthsofresearchtraining. Inadditiontotheobjectivesandresponsibilitiesdescribedforthefirstyearfellowsontheconsultationservice,thesecondyearfellowthathasmadesatisfactoryprogressisgivenmorefreedomtomakeinitialrecommendations.Thisisencouragedifheorsheiscomfortableandconfidentintherecommendation.Inthesecondyear,thefellow’srecommendationmaybereviewedinitiallywiththeattendingbyphoneandmadedirectlytotheprimaryservice,buttheattendingphysicianwillseethepatientthesamedayastheconsultisrequested.Fellowsshouldcontacttheattendinganytimedayornightifheorshehasdoubtaboutanyassessmentorrecommendation.Asduringthefirstyearoffellowship,theweekendcoverageisarrangedtoensurethatfellowshaveonedayoffeverysevendays,averagedoverfourweeks,andonthatday,theywillbefreeofdirectpatientcaredutiesandfreeofbeepercall..Inadditiontoyear1objectives,theyear2fellowwilldothefollowing:
a. Participateinanddirectconsultationrounds.b. Accuratelyapplyclinicalinformationtoensurepositivepatientoutcomes.c. Assumemoreresponsibilitymakingclinicaldecisions.d. Havespecialized,detailedknowledgeofimportantareasinID.e. Regularlyusemedicalliteraturetosupportdecisionmaking.f. Demonstrateknowledgeandleadershipinguidingotherhealthcarememberson appropriateantibioticutilizationandrestrictionpolicies.g. Effectivelydiscussendoflifecarewithpatientsandfamilies.h. Displayinitiativeandleadership.i. Appropriatelydelegateresponsibilitytoothers.

21
j. Showcommitmenttoprofessionaldevelopment.k. Usesystematicapproachestoreduceerrors.l. Partnerwithproviderstoimprovepatientcare.m. Providecosteffectivecare.n. Understandqualityofcareprinciplesandapplytheseatthebedside.o. Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐
benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients.
InfectiousDiseasesClinicTrainingSite:KUH,KCVAMCSecondyearfellowscontinuetospend½dayeachweekinthecontinuityambulatoryclinicforinfectiousdiseasesatKUH.DuringclinicalrotationsatKCVAMC,fellowswillspendanadditionaltwo½daysperweekinambulatoryclinic.Theresponsibilitiesandobjectivesdescribedforfirstyearfellowscontinue,butinadditioneachfellowisgivenmoreindependentauthoritytomakemanagementdecisionsontheirownpanelofHIV‐infectedpatients.Thiscontinuestobedoneunderthedirectionoftheirattendingphysicianwhoalsoseeseachpatientwiththefellow.Thisincludesbutisnotlimitedtoselectionandmodificationantiretroviraltherapy,immunizations,managementofpreventionandtherapyofopportunisticinfections,andsocialandfinancialaspectsofcomplexHIVcases.
Inadditiontoyear1objectives,theyear2fellowwilladdthefollowing:
a. EstablishtheirownpanelofHIV‐positivepatientstounderstandmanagementissues,includingfinancialandpsychosocial,relatedtoantiretroviraltherapy,prophylaxisandmanagementofopportunisticinfections,andnon‐medicalofcasemanagement.
b. Understandmanagementissuesassociatedwithoutpatientadministrationofantibiotics.
c. Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
d. Continuetodevelopandimproveconsultativeskillsintheoutpatientsetting.e. Effectivelydiscussendoflifecarewithpatientsandtheirfamilies.f. Displayinitiativeandleadershipininitiatingandmaintainingeffective
communication.g. Showacommitmenttoprofessionaldevelopment.h. Partnerwithotherproviderstoimprovepatientcare.i. Regularlyusemedicalliteraturetosupportdecisionmaking.j. Regularlyapplynewcontributionstothemanagementandcareofinfectiousdisease
patientsinoutpatientsettings.k. Continuetodevelopandimproveconsultativeskillsintheoutpatientsettings.l. Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐
benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients.m. Usesystematicapproachestoreduceerrorsinoutpatientsettings.
ResearchTrainingsite:KUH

22
Secondyearfellowsareencouragedtospendthreemonthsdirectlyineitherclinicalorbasicresearch.Thistimemaybeshortenedorlengthenedatthediscretionoftheprogramdirectorbaseduponproposedresearchproject.Inadditiontotheobjectivesandresponsibilitiesforfirstyearfellows,secondyearfellowsareencouragedtoprepareandpresentoralandwrittenpapersforpeerreviewandpublicationinappropriatejournalsandatregionalandnationalmeetings.Academicprofessionalismisstressedduringthisresearchprocess.Inadditiontoyear1objectives,theyear2fellowwilladdthefollowing:
a. Becomeadeptatobtainingandanalyzingtherelevantresearchliterature.b. Demonstratecompetenceinmanuscriptpublicationinapeer‐reviewedjournal,
includingpreparationoffigures.c. Learntoacceptandutilizecriticalevaluationofone’swork.d. Displayinitiativeandleadershipininitiatingandmaintainingeffective
communicationregardingresearchideasandformaldisseminationandpresentationofresearchfindings.
e. Showacommitmenttoprofessionaldevelopment.f. Prepareresearchforpublicationand/orpresentationatanationalmeetingor
conference.g. Demonstratecompetenceindatacollectionandorganizationforsubsequent
evaluation.h. Demonstrateunderstandingofstatisticalanalysisofdatacollected.i. Learntoevaluateresultsforagivenprojectinthecontextofotherworkinthe
researcharea.j. Competenceinproposingfutureexperimentstoaugmentresultsfromagiven
project.PediatricInfectiousDiseasesTrainingsite:KUH
IDfellowsseepediatricpatientsinconjunctionwiththeirattendingwhenconsulted
onthispatientpopulation.ThepediatricIDfacultymemberattendstheadultIDmeetingsandpresentscasesandleadsdiscussiononuniquetopicsinpediatrics.Pediatricinfectionsareintegratedintotheusualrotationsforfellows.PediatricinfectionsarealsoaddressedinJournalClubs,caseconferences,andinlecturesinthecorecurriculumgivenbythepediatricIDconsultant.YearThreeofInfectiousDiseasesFellowshipGoalsforthethirdyearoftrainingAthirdyearoftrainingismadeavailableinexceptionalcases.Thepurposeofthe3rdyearofFellowshipinInfectiousDiseasesistopreparethetraineeforacareerinacademicmedicine.FellowswhodesirethistrackwillplantheirspecificrotationswiththeFellowshipProgramDirectorandwillhaveaspecificresearchprogramplannedaswellasadesignatedfacultymentor.Suchafellowwillhaveworkedonthespecificorarelatedproblemearlierduringtheirtrainingprogram.

23
The3rdyearoffellowshipmayincludecourseworkinstatistics,molecularbiology,andbiochemistry,ifpertinent.OthersmayelecttoparticipateintheMasterofPublicHealthdegreeprogram.Suchfellowswillbecompletingongoingprojects,andpreparetoenteranacademiccareerbysubmittingagrantapplication.F.Conferences,LecturesandOtherEducationOpportunitiesAttendanceatIDcaseconferences,CoreConference,ResearchConferenceandJournalClubismandatory.Fellowsareexpectedtowillinglytakepartintheseconferenceopportunities.Attendanceistakenateachconference.Itistheexpectationthatfellowswillattendallconferencesexceptintheinstancesofillnessorvacation.InfectiousDiseasesClinicalCaseConferenceClinicalcaseconferenceisheldweekly.Casesareselectedbytheattendingphysicianindiscussionwiththefellowandgenerallyinvolveunusualandcomplexcases.Fellowsareaskedtoframethepresentationaroundoneortwoimportantclinicalquestions.Casepresentationsinvolvereviewofclinicalinformation,radiographicstudies,gramstainandothermicrobiologicdiagnosticsandpathologystudies.Followingcasepresentation,afellownotpreviouslyinvolvedinthecaseisaskedtodevelopanapproachtothecaseandtodiscussinterpretationsofclinicaldata,differentialdiagnosisandmanagement.Followingthisdiscussion,thepresentingfellowprovidesanevidence‐baseddiscussionoftheclinicalquestionsandmanagementissuesrelevanttothecase.Attheconclusionoftheconference,anevaluationofthefellowpresentationisconductedbyoneofthefaculty.Inaddition,relevantsupplementalarticlesandupdatesareprovidedtothefacultyandfellows.
CompetenciesEmphasized1. PatientCare:Specificelementsofthecareofeachcasearedescribedindetailand
arecriticallyaddressedbythefaculty.Discussionemphasizesthediagnosticandtherapeuticapproachtotheproblem(s)manifestedbythepatient.Fellowsactivelyparticipateindiscussingallaspectsofcare.Themanagementofaclinicalproblemservesasthebasisforanactivediscussionofproblemsolvingandliteraturereview.
2. MedicalKnowledge:Thediscussionreviewscurrentandrelevantmedicalliterature.3. Practice‐BasedLearning:fellowsidentifystrengths,deficienciesandlimitsintheir
knowledgeandexpertise.4. InterpersonalandcommunicationSkills:Clarityandorganizationarekeyelements
oftheconference.Fellowsinteractwithotherfacultyandfellows,5. Professionalism:Academicprofessionalismandintegrityareemphasized.6. System‐BasedPractice:Discussioninvolvesconsiderationofmultipledisciplines.
CoreCurriculumConferenceCoreConferenceisheldweeklyandattendedbyfellowsandfaculty.Conferencesaremadeavailabletofellowsoffsitethroughweb‐basedprogram.Theconferenceseriesisa2‐yearcurriculumoflectures.LecturescoverallmajortopicsofInfectiousDiseasesmodeledaftercontentsofPrincipleandPracticesofInfectiousDiseases(seeAppendixforconferenceschedule).Duringthefirst4weeksofeachacademicyear,conferencesareheldtwice

24
weekly.ThegoalsofthisacceleratedconferenceseriesistoexposenewfellowstocoreIDtopicsearlyintheirtraining(HIVinfection,boneandjointinfections,endocarditis).InadditiontomajorIDtopics,supplementallecturesincludingmoleculardiagnostics,specialpopulationssuchasCysticfibrosisandtransplantation,billingcompliance,Qualityimprovementarealsoincludedwithinthe2‐yearcurriculum.Conferencesarepresentedasdidacticteachingsessionsledbyfellowsandfacultyandassignedonayearlybasis.Fellowsareassignedafacultymentorwhocontributestothefellow’spreparationandpresentation.
CompetenciesEmphasized1. PatientCare:Thefellowsapplyinformationtotheirownpatients,2. MedicalKnowledge:Discussionsreviewcurrentconceptsininfectiousdiseases.3. Practice‐BasedLearning:Fellowsidentifystrengths,deficiencies,andlimitsintheir
knowledgeandexpertisecanandcansetlearninggoals.4. InterpersonalandCommunicationSkills:Theclarityandorganizationofthe
discussionarekeyelementstotheconference.5. Professionalism:Fellowsareresponsibleforassignedreadingandpresentation6. System‐BasedLearning:Discussionoftopicsofteninvolveconsiderationofmultiple
disciplinessuchasothermedicalandnon‐medicalspecialties,infectionprevention,quality,billingandpublichealth.
ResearchConferenceResearchConferencetakesplacemonthly.Firstyearfellowsareaskedtopresenttheirproposedresearchproject,whichisopentocriticaldiscussionbytheattendees.Inthesecondyear,fellowsareaskedtopresentthefindingsoftheirresearchproject.Inadditionthisconferenceisusedtoupdatefellowsonfacultyresearchandtoserveasavenueforgeneratingnewprojectsandcollaborativeendeavors.
CompetenciesEmphasized1. PatientCare:Theapplicabilityoftheresearchtopatientcareisdiscussed.2. Medicalknowledge:Discussionincludesareviewoftheresearchtopicandits
importance.3. Practice‐BasedLearning:Fellowscanidentifystrengths,deficienciesandlimitsin
theirknowledgeandexpertise.4. InterpersonalandCommunicationSkills:Theclarityandorganizationofthe
presentationarekeyelementsintheconference.5. Professionalism:Ethicalissuesofresearcharediscussed.6. System‐BasedPractice:Asystemsbasedapproachtoresearchisemphasized.
JournalClub
TheJournalClubConferencehasbeenheldweeklysince1961,andisthesettingforreviewofawidearrayofclinicalandbasicsciencearticles.Thefellows,clinicalmicrobiologists,clinicalpharmacists,biostaticiansandepidemiologists,presentarticlesonarotatingbasis.Thediscussionfocusesoncriticalevaluationandinterpretationoftheinfectiousdiseaseliterature.CompetenciesEmphasized

25
1. PatientCare:Presentationsemphasizetheapplicabilityoffindingstopatientcare.2. MedicalKnowledge:Thediscussionincludesacriticalpresentationofthe proposedarticle,anddisseminationandreviewofemerginginfectiousdiseases literature.3. Practice‐BasedLearningandImprovement:Theliteratureiscriticallyappraisedby facultyandfellows.Thereisemphasisonsamplesize,potentialbiases, appropriatenessofstatisticaltestsandlegitimacyofconclusions.Conclusions derivedfromthereviewareappliedtoindividualpatientcarepracticeofthe fellows.4. Interpersonalskills:Theclarityandorganizationofthepresentationarekey elementsintheconference.5. Professionalism:Academicprofessionalismisemphasized.6. Systems‐BasedPractice:Emphasisisplacedonsystemsapproachtoresearch.
TheKansasCityInfectiousDiseasesSociety(KCIDS)KCIDSmeetingconsistsofcliniciansfromtheKansasCityareawhopresentinterestingandchallengingcasesfordiscussion.Presentationoccursonarotatingbasisfromcontributinginstitutions.FellowsarerequiredtopresentrepresentativecasesfromKUH,RMCandtheKCVAMC.ConferenceformatfollowstheKUHClinicalCaseconferenceprovidingcasepresentation,asegmentinwhichtheaudienceisaskedtodevelopanapproachtothecaseanddiscussinterpretationofdata,differentialdiagnosisandmanagement,pathophysiology,appropriateuseoftechnologyandprevention.Thepresenterthenprovidesanevidencebaseddiscussionofmanagementissues.
CompetenciesEmphasized1. PatientCare:Specificelementsofthecareofeachcasearedescribedindetailand
arecriticallyaddressedbytheaudience.Discussionemphasizesthediagnosticandtherapeuticapproachtotheproblem(s)manifestedbythepatient.Fellowsactivelyparticipateindiscussingallaspectsofcare.Themanagementofaclinicalproblemservesasthebasisforanactivediscussionofproblemsolvingandliteraturereview.
2. MedicalKnowledge:Thediscussionreviewscurrentandrelevantmedicalliterature.3. Practice‐BasedLearning:fellowsidentifystrengths,deficienciesandlimitsintheir
knowledgeandexpertise.4. InterpersonalandcommunicationSkills:Clarityandorganizationarekeyelements
oftheconference.FellowsinteractwithotherfacultyandcommunitybasedIDclinicians.
5. Professionalism:Academicprofessionalismandintegrityareemphasized.6. System‐BasedPractice:Discussioninvolvesconsiderationofmultipledisciplines.
AntibioticCommitteeThefocusofthecommitteeistomonitortheepidemiologyofinfectionandantimicrobialdruguseininpatients,providedirectionforcost‐effectiveandrationaldruguse,reviewdrugutilizationandpracticeguidelinesanddeterminehowtheseshouldbeusedtochangeindividualandsystempractice.ThecommitteeisdirectedjointlybyIDDirectorandIDPharmD.Committeemembersrepresentabroadrangeofhealthsystemexperts:

26
Pharmacy,InfectionPreventionandControl,Microbiology,CriticalCareMedicine,Trauma,andFamilyMedicine.
CompetenciesEmphasized1. PatientCare:Presentationsemphasizetheapplicabilityoffindingstopatientcare.2. MedicalKnowledge:Thediscussionincludesacriticalpresentationofthe guidelinesandarticlesimportanttosupportingsystem‐basedchanges.3. Practice‐BasedLearningandImprovement:Theliteratureiscriticallyappraisedby thecommittee.Conclusionsderivedfromthereviewareappliedtoindividual patientcarepracticeofthefellows.4. Interpersonalskills:Discussionamongamultidisciplinarygroupofhealthcare providersisrequired.Theclarityandorganizationofthepresentationarekey elementsintheconference.5. Professionalism:Academicprofessionalismisemphasizedstressingintegrity, honestyandrespect.6. Systems‐BasedPractice:Emphasisisplacedonsystemsapproachtoimproving antibioticadministrationanddevelopmentofinstitutionalguidelines.
InfectionPreventionandControlCommitteeInfectiousDiseasesfellowsattendthemonthlyinfectioncontrolmeetingatKUHandparticipateininfectioncontrolrelateddecisions.ThiscommitteeisdirectedbytheIDAssociateProgramDirectorandtheChiefInfectionPreventionPrecautionNurse.Participationinthiscommitteeprovidesfellowswithexperienceandexpertiseintheappropriateusesofinfectioncontrolinterventionsinahospitalsystem.Fellowswillhaveopportunitiestoassistwithdevelopmentandimplementationofinfectioncontrolpolicies,determiningappropriateinfectioncontrolmeasuresininpatientandoutpatientsettings,learnhospitalandpatientbenefitsofeffectivequalityassuranceandcostcontainment,OSHAregulations,riskmanagementandadministrativeresponsibilitiesoftheinfectionpreventionandcontrolcommittee.
CompetenciesEmphasized1. PatientCare:Discussionemphasizestheapplicabilityoffindingstopatientcare.2. MedicalKnowledge:ThediscussionincludesapresentationofNationalguidelinesandinstitutionalpoliciesapplicabletopatientcare.
3. Practice‐BasedLearningandImprovement:Fellowscanidentifystrengths,deficienciesandlimitsintheirknowledgeandexpertiseandapplyevidence‐basedchangestotheirpractice.
4. Interpersonalskills:Discussionamongamultidisciplinarygroupofhealthcareprovidersisrequired.Theclarityandorganizationofthepresentationarekeyelementsintheconference.
5. Professionalism:Academicprofessionalismandintegrityisemphasized6. Systems‐BasedPractice:Emphasisisplacedonsystemsapproachtoimprovinginfectionpreventionandcontrolanddevelopmentofinstitutionalguidelines
OutpatientAntibioticTherapy(OPAT)

27
Duetoearlydischargefromtheinpatientservices,outpatientparenteralantibiotictherapyhasbecomecommon.ThereforeappropriateinstructionregardingmanagementofoutpatientparenteraltherapyisvitaltoanIDtrainingprogram.Fellowslearnstrategiesfordeterminingappropriatenessofoutpatienttherapy,safety,monitoringanddeliveryofoutpatientantibiotics.TheyworkcloselywiththeIDantibioticnurseclinician,hospitaldischargeplanningcoordinatorandprimaryservices.Fellowsareinvolvedincommunicationwithhomehealthagencyandassistedlivingfacilitiesinvolvedinpatientcare.Fellowshavedirectfacultysupervision.AllOPATpatientsareassignedtoanattendingphysicianthatworkswiththefellowtodeliversafeandreliablecare.
CompetenciesEmphasized1. PatientCare:ThefellowlearnstodeliverOPATinsafeandappropriatemanner.2. MedicalKnowledge:Becomefamiliarwithselectionofappropriatepatients,antibioticchoicesandmonitoringofOPAT.
3. Practice‐BasedLearningandImprovement:Fellowscanidentifystrengths,deficienciesandlimitsintheirknowledgeandexpertiseandapplyevidence‐basedchangestotheirpractice.
4. Interpersonalskills:Workcloselywithamultidisciplinaryteamofnurses,casemanagers,pharmacist,homehealthagenciesandassistedlivingfacilityadministrators.
5. Professionalism:Emphasizeacademicprofessionalismandintegrity.6. Systems‐BasedPractice:EmphasisisplacedonsystemsapproachtoimprovingthedeliveryofOPAT.
DepartmentofMedicinePatientSafetyandClinicopathologicalConferenceFellowsattendthesetwoDepartmentalConferenceswhicheachmeetmonthly.ThePatientSafetyConferenceisdesignedtocriticallyreviewpatientmanagementacrossthespectrumofthehealthcaresystem.Fellowswillspecificallylearnhowtocreatea“cultureofsafety”,aligningtheinterestsofclinicianswiththegoalsoftheorganization,learnfromdefectsinpatientcare,incorporatehumanandenvironmentalfactorstoreduceerror,andempowercliniciansbyprovidingthemwithtoolstoeffectivelyimplementchange.TheVanderbiltMatrixisusedasakeytooltoevaluatingeachcase(Seeappendix)inthePatientSafetyConference.ThistoolfollowsthesixACGMEClinicalCompetenciesaswellasthesixIOMAims(safe,timely,effective,efficient,equitable,patientcentered).Thisisdevelopedingridlikeformattocovereachpatientallowingidentificationofanyareaofdeficiency.Attendeespresentrepresentallspecialtiesfromthemedicalcenterandalsoincludetheriskmanagement,attorneys,administration,nursing,qualitycontrol,andothers.TheClinicopathologicalConferenceisamultidisciplinaryconferencepresentedascase‐basedteachingfollowedbycorrelationofclinicalandpathologicalfindings.Thisconferenceprovidesavenueforfellowstoreviewbiopsyorautopsyresultsofcasesanddiscusstheimpactthesefindingshaveonpatientandsystemchangestoimprovehealthcaredelivery.Inaddition,theconferenceservestoconveyanunderstandingofproblem‐solvingskillsandtoprovideanin‐depthreviewofcomplexorunusualcases.

28
EthicsandSocietalImpactThetrainingprogramprovideseducationtailoredtoethicsofmedicalcareandbiomedicalresearch.Areasaddressedinclude:thesocialandeconomicimpactofmedicaldecisionsonpatientsandsociety,physicianaspatientadvocate,qualityassessmentandimprovement,riskmanagement,preventivemedicine,occupationalandenvironmentalhealth,medicalinformatics,painmanagement,endoflifecareandsubstanceusedisorders.Muchofthistrainingoccursatthebedsideandinconferencesandlectures.ProfessionalEthicalBehaviorThetrainingprogrammentorsstrivetomaintainandrolemodelaculturethatvaluesprofessionalismandethicalbehavior.Qualitiesemphasizedbyfacultyinclude:commitmenttoscholarship,excellenceinclinicalcare,humanisticqualitiesincludingrespect,compassiontowardpatientsandprofessionalandcollegialattitudetowardcolleagues.Fellowsareinstructedtorecognizeandinterveneifcolleaguessufferphysicalorpsychologicalimpairment,includingsubstanceabuse,alcoholism,sleepdeprivation,orexcessivestress.Opportunityistakeninconferences,bedsideroundsandinone‐on‐oneevaluationsessionwiththeprogramdirectorandfacultytodiscussandeducatethefellowsonbiomedicalethicsandtoallowthefellowstoparticipateinethicaldecisionsarisingfromthemanagementoftheirpatients.G.EvaluationofFellowsFellowsareevaluatedusingavarietyofassessments(seeappendix:RequiredEvaluationsforIDfellowsandprogram).Facultymembersevaluatefellowsoninpatient,outpatientandresearchrotations.Ontheconsultservices,fellowsareassessedmonthlybyafacultymemberwhohaddirectsupervisionduringtherotation.Theevaluationisconductedwithanelectronicform(e*value)subdividedintothesixcorecompetenciesofpatientcare,medicalknowledge,practice‐basedlearning,interpersonalskillandcommunication,professionalismandsystembasedpractice.Evaluatorsareaskedtochoosearatingscalethatmeasuresthestrengthofagreementwithaclearstatementaboutthehowwellthefellowsucceededineachcategory.Inaddition,inpatientchartsareauditeddailybytheattendingphysician,anddailycase‐basedfeedbackisprovidedtothefellow.ConcernsofthefacultyorfellowsareaddressedimmediatelybytheProgramDirector.Fellowsalsoreceivequarterly3600evaluationsfromclinicstaffandpatientwithassessmentsoftheircommunication,interpersonalandprofessionalismskills.Evaluationofresearchrotationsiscompetencybasedandassessesthefellow’scompetencyinresearchdesign,skillsinscientificwriting,knowledgeofIRBregulations,andaccomplishmentofstatedgoals.Evaluatorsareaskedtochoosearatingscalethatmeasuresthestrengthofagreementwithaclearstatementaboutthehowwellthefellowsucceededineachcategory.TheProgramDirectormeetswitheachfellowatleasttwiceperyearforareviewofhisorherperformancewithawrittenreportfiledinthetrainee’sevaluationfolder.Attheendofthetwo‐yeartraining,awrittensummaryofthetrainee’sperformancereviewedwiththe

29
fellowandplacedinhisorherfolderforapermanentrecordforfuturereference.H.AdvancementtoSucceedingTrainingYearTheKUIDPromotionCommitteemeetsyearlytorevieweachfellow’sperformanceandmakerecommendationsforadvancingtothenextyear.AdditionalmeetingmaybecalledatthediscretionoftheIDFellowshipProgramDirector.AllKUIDfacultyareappointedtothePromotionCommittee.Criteriausedtobaserecommendationsforpromotioninclude:qualityofmonthlyrotationalevaluationswithspecificemphasisonthefellows’performanceinthecoreACGMEcompetencies;participationinacademicconferences;scoringsatisfactorilyontheannualIDin‐trainingexamination(althoughanabsolutescoreontheexaminationisnotrequiredforpromotion);compliancewithallhospital,departmentalandfellowshiprecordkeeping,policyanddocumentationrequirements.AdditionalexpectationsareoutlinedinSectionV.Rbelow.Disciplinaryandremedialactionmaybeinitiatedwhentheprogramdirector,afterconsultingwithkeyclinicalfaculty,determinethatsuchactioniswarranted.IDDivisionalactionsfollowtheproceduresandappealsasoutlinedintheProgramManualfortheDepartmentofInternalMedicineandaredescribedbelowinSectionII.M.I.EvaluationofFacultyandProgramFellowsevaluatefacultyattheendofeachrotation.Theseevaluationsaresubmittedanonymously.TheyaresummarizedforindividualfacultyandfortheProgramDirectorandareusedtocounselfacultyandtoassignfacultytospecificteachingrotations.FellowsevaluatetheprogramonanannualbasisandtheseevaluationsareusedtodevelopprogrammaticchangesJ.DocumentationofTrainingTheprogrammaintainsafileoneachfellow,whichincludescopiesoftheirevaluations,copiesoftheirsummaries,lettersofrecommendation,andanyotherdocumentpertinenttotheirtrainingandperformance.Thefellowmayviewthisfolderatanytime.Thesefilesaremaintainedpermanentlytodocumentthelengthandcontentoftheirtrainingaswellastheirperformance.Theprogramisresponsibleforcompletionofformsdocumentingtrainingasresidentsapplyforhospitalcredentials,statemedicallicenses,etc.Fellowsshouldensurethattheprogramhasupdatedcontactinformation,includingbusinessaddress,e‐mail,andphonenumberssothatfuturecommunicationcanbemaintained.

30
V.POLICIESANDPROCEDURESTheInfectiousDiseasesProgramusesitsbestefforts,withinthelimitsofavailableresources,toprovideaneducationaltrainingprogramthatmeetstheACGME'saccreditationstandards.Inaddition,theprogramwillprovidethefellowwithadequateandappropriatesupportstaffandfacilitiesinaccordancewithfederal,state,local,andACGMErequirements.Thepolicyandproceduresinthismanualareinadditiontothepoliciesandproceduresmanualsinplaceatthedepartmentalandinstitutionallevel.FellowsshouldrefertotheGMEofficeHousestaffPolicyandProcedureManualandtheProgramManualDepartmentofInternalMedicineforacomprehensivereviewofHousestaffPolicyforfulldetails.Thesemanualsarereviewedatgeneralhousestafforientation.Copiesofthesematerialsareavailablefromtheprogramdirector,departmentadministration,orthedean'soffice.TheyarealsoavailableontheKUMCwebsites:http://gme.kumc.edu/policiesandprocedures.htmlandhttp://www2.kumc.edu/internalmedicine/residency/residency.html A.PrerequisitesFellowsmustholdaMDorDOdegreefromanaccreditedmedicalschoolmeetingoneofthefollowingcriteria:1.GraduationfromamedicalschoolintheUnitedStatesorCanadaaccreditedbytheLiaisonCommitteeonMedicalEducation(LCME)2.GraduationfromacollegeofosteopathicmedicineintheUnitedStatesaccreditedbytheAmericanOsteopathicAssociation(AOA)3.GraduationfromanacceptablemedicalschooloutsidetheUnitedStatesorCanadawithoneofthefollowing:
i.SuccessfulcompletionofaFifthPathwayprogramprovidedbyanLCMEaccreditedmedicalschool,
ii.Acurrent,validcertificatefromtheEducationalCommissionforForeignMedicalGraduates(ECFMG)priortoappointmentiii.AllCanadiancitizensandeligibleCanadianLandedImmigrantswhoareNOTgraduatesofaforeignmedicalschoolmustholdastatus,whichallowsemploymentasamedicalresident,andmaintainanappropriatestatusthroughoutthelengthofthegraduatemedicaltrainingprogram.Possessionofvalidimmigrationdocumentswhichverifythestatusmustbepresentediv.Afull,unrestrictedlicensetopracticemedicineintheStateofKansasandtheStateofMissouri,dependingonthetrainingprogram.DefinitionofacceptableMedicalschooloutsidetheUnitedStatesisfurtherdefinedintheGME office Housestaff Policy and Procedure Manual (Section 4.1)
FellowsmusthavesatisfactorilycompletedanACGMEaccreditedUSresidencyprograminInternalMedicine.Onrareoccasions,fellowsmaybeacceptedintransferfromanotheraccreditedInfectiousDiseasesTrainingprogram.TransferringfellowsmustmeetrequirementsandregulationsasoutlinedintheGMEofficeHousestaffPolicyandProcedureManual(Section4.2)B.FellowshipSelectionProcessTheIDdivisionparticipatesintheElectronicResidencyApplicationService(ERAS).We

31
alsoparticipateintheNationalResidencyMatchProgramforInternalMedicineSubspecialtyPrograms.PotentialfellowapplicantsmustsubmitanapplicationconsistingoftheERASform,anupdatedcurriculumvitae,threelettersofrecommendation,andapersonalstatementpriortoconsiderationforapersonalinterview.Afterreviewofthesubmittedmaterials,selectedapplicantsmaybeinvitedtopersonallyvisittheprogramandinterviewwithmembersofthefaculty.Everyattemptismadeforapplicantstomeetthemajorityofthefull‐timeKUMC‐basedkeyclinicalfaculty.Afterthepersonalinterviewwiththeprogramdirectorandfaculty,candidateevaluationformsaresubmittedtothedirector.Oncethecandidateisinterviewed,afellowshipselectioncommittee,consistingoftheprogramdirectorandKUMCfaculty,meettorankthecandidatesaccordingtointerviewevaluationratings.TheapplicantsselectedbythecommitteeareinformedoftheselectionbytheProgramDirector.Afterreceivingacontingentofferofappointment,thefellowmustcompleteappropriatedocumentationandrequirementsasdetailedintheGMEofficeHousestaffPolicyandProcedureManual(Section4.5).OfficialnotificationfromtheUniversityofKansasSchoolofMedicineisbycontractthatismailedinthespringpriortobeginningthefellowship.C.DurationofProgramTheprogramistwoyears(24months)withanemphasisontraininginclinicalinfectiousdiseases.Athirdyearoftrainingismadeavailableinexceptionalcasesinwhichthefellowisacceptedintoresearchstudiesinpreparationtoacceptanacademicposition.D.DutiesThefellowshipincludesbothclinicalandresearchresponsibilities.Itwillbethedutyofthefellowtocarryouttheclinicalresponsibilitiesoftheservicestowhichthefellowhasbeenassigned.Thisincludesnotonlyclinicallyevaluatingpatients,followingtheirprogressandimplementingtherapybutalsoteachingofmedicalstudentsandresidents.Fellowsshouldbeawareofthefellowandattendingon‐callscheduleaspostedontheDivisionalcalendar.Weeklyelectronicemailremindersofcallschedulewillbesent.Fellowsareexpectedtoutilizethedivisionalstructuredcheckoutprocedurewhenrotatingtoanewservice.Thisprovidesanopportunityforthefellowtolearntoworkinteamsandeffectivelytransmitnecessaryclinicalinformationtoensuresafeandpropercareofpatients.Specificdutiesforeachrotationareoutlinedandreviewedpriortothebeginningofeachrotation.Educationalexpectationsandguidelinesshouldbereviewedbythefellowanddiscussedbytheattendingstaffatthebeginningoftherotation.Theguidelinesareprovidedtoeachfellowatthebeginningofthefellowshipandremainavailablethroughdepartmentalwebsiteforreview.Intheareaofresearch,thefellowisexpectedtocarryoutaprojectundertheguidanceofafacultymentor.Thisprojectshouldculminateinbothpublicationinajournalandscientificpresentationataregionalornationalmeeting(ExamplesofthesemeetingsincludetheKansasACP,theIDSA,theASMortheICAACmeetings).LaboratoryresearchtrainingandexperiencemaybeacquiredinconjunctionwithInfectiousDiseases,InternalMedicinefacultyorthroughanotherdepartmentapprovedbytheProgramDirector.ExperiencewithInfectiousDiseasesClinicalTrialsisavailablewiththeInfectiousDiseasesresearchstaff.

32
Inadditiontotraininginthedisciplineofinfectiousdiseases,fellowsareexpectedtoparticipateintheeducationofInternalMedicineresidents,medicalstudents,pharmacystudents,nursepractitioners,inPracticeBasedLearning(PBL),FacultyStudentInteractionsessionsandinphysicaldiagnosiseducation.Itisthephilosophyoftheprogramthatfellowsshouldbehighlymotivatedanddeveloplifelonghabitsofself‐instruction.Thus,fellowsareexpectedtousethemedicalliteraturetosolveclinicalproblemsbeforethecasesarepresentedtothefaculty.AlthoughmostdisordersencounteredbyanIDconsultantwilleventuallybeseenandmanagedbythefellowduringthetwo‐yearfellowship,somedisorderswillnot.Thus,itisexpectedthatmostofthesewillbediscussedincorecurriculumconferences,caseconferencesorthatthefellowwillidentifysuchareasandobtainarticlesfromthemedicalliteraturesothattheyhaveaconceptualunderstandingofthesedisorders.Thefacultyareexpectedtobereadilyavailableforguidanceandsuggestions.E.DutyHoursPolicyandFatigueThefellowshipprogramstrictlyadherestotheACGMErequirementconcerningworkhoursasreflectedintheKUGMEPolicyandProcedureManual(Section15).Tothisend,fellowswillnotworkmorethan80hoursperweekaveragedoverafourweekperiod,inclusiveofallin‐housecallactivitiesduringanyrotation.Moonlightinghourswillbeincludedinthiscalculation.Fellowswillbeprovided1dayin7freefromalleducationalandclinicalresponsibilities,averagedovera4‐weekperiod,inclusiveofcall.Onedayisdefinedas1continuous24‐hourperiodfreefromallclinical,educational,andadministrativeduties.Adequatetimeforrestandpersonalactivitiesmustbeprovided.Theprogramdirectorcontinuouslymonitorsworkhoursbymonthlyrotationsurveysperformedbythefellowsandatthesemi‐annualevaluationconductedwitheachfellow.Inaddition,questionsaboutworkhourswillbeaddedtotheendofmonthrotationsurvey.TheGMEofficewillconductsemi‐annualsurveysofalltraineesatKUMC.Theusualtimeforfellowstobegintheworkdayvariesbyhospital,rotation,anddayoftheweek.Ingeneral,fellowsareexpectedtobeginclinicalserviceworkby7am.Oneto2daysperweek,fellowsareexpectedtoattenda7amconference.Theconclusionofthedayiswhenallclinicalresponsibilitiesaremetincludingevaluatingpatients,completingappropriatedocumentationandcoordinatingacareplanforthefollowingdaywiththeattending.Itismandatorythatsenior‐levelresidentshavetenhoursfreeofdutybetweenscheduleddutyperiods.Specificdutyhourandworkexpectationswillbeuniquetotheindividualsitethefellowisassigned.Expectationsareatthediscretionoftheattendingandwillbereviewedatthebeginningofeachclinicalrotation.EachIDfellowworkscloselywithoneIDfacultypersonatonetime.Thuswhenthefelloworthefacultysensethattheclinicalcareneedsoftheservicearelikelytobecomegreaterthanafellowshouldbeinvolvedintogivetheoptimaleducationalexperience,thefacultyassumestheprimarycareforpatients.FellowsareshieldedfromasignificantportionoftheclinicalresponsibilitiesoneachofthefiveKUinpatientservicesinordertoprovidethemwithanoptimalworkenvironment.

33
Allclinicalfacultyandfellowshavebeeninstructedontheworkhourpolicyandthedetectionoffatigueintraineesandupdatedoninstitutionalpoliciesannually.BothfacultyandfellowsarerequiredtosuccessfullycompletetheANGELFatiguemodule.Signsandsymptomsoffellowfatigueand/orstressmayincludebutarenotlimitedtothefollowing:inattentivenesstodetails,forgetfulness,emotionalstability,moodswings,increasedconflictswithothers,lackoforattentiontoproperattireorhygiene,difficultywithnoveltasksandmultitasking,awarenessisimpaired(fallbackonrotememory),lackofinsightintoimpairment.Supervisingfacultyconstantlymonitorfellowsforsignsoffatigueandreportthesefindingstotheprogramdirectorassoonaspossible.Theprogramencouragesresidentstousealertnessmanagementstrategiessuchasstrategicnapping,inthecontextofpatientcareresponsibilities.Fellowshaveaccesstosleepingquarters(KUHIMoncallrooms4461‐4464)tobeusedattheirdiscretion.Appropriateactionincludingreliefofdutiesforrest,modificationofdutiestoinsureadequaterest,cancellationofmoonlightingprivilegeswillbeinstitutedbytheprogramdirectorafterdiscussionwiththefellowandfacultyifsuchneedarises.AnoverviewoftheGMECFatigue(Transportation/SwingRoomGuidelinesareprovidedintheAppendix,pg100).F.CallScheduleFellowswillbeonat‐homecallwhenonaninpatientconsultationservices.AtKUH,arotatingcallscheduleamongeligiblefellowsismadebytheInfectiousDiseaseschieffellow.Thecallscheduleandscheduleofdutyassignmentsispublishedandmadeavailableforreviewbythefellowsonamonthlybasis.FellowcallatKCVAMCandRMCwillbemadeinagreementbetweentheattendingphysicianandfellowandmeetprogramrequirementsofworkhoursandtimeawayfromwork.At‐homecallwillnotbesofrequentastoprecluderestandreasonablepersonaltimeforeachresident.Residentstakingat‐homecallmustbeprovidedwithonedayinsevencompletelyfreefromalleducationalandclinicalresponsibilities,averagedoverafour‐weekperiod.Duringoncallduty,fellowswilltakefirstcallonclinicalcasesreferredtotheIDdivision.Theywilltakecallfromhomeintheeveningsandonweekends.Theywillbeexpectedtoseeanynewemergencyconsultinatimelymanner.Thismayinvolvecomingtothehospitalatanytimeofthedayorweekthattheyareassignedtobeonat‐homecall.Weexpecttheat‐homecallfellowtoreceive3to7telephonecallsatnightoronweekends.Ingeneral,fellowsarerequiredtoreturntothehospitaltoparticipateinpatientcarenomorefrequentlythanonceweekly.Thisgenerallyoccursduringweekendcall.Saturdaycallrequirementsincludetakingfirstcallonclinicalcases,completinginitialevaluationandrecommendationfornewconsultationsandprovidingfollow‐uprecommendationforselectongoingpatientsinconjunctionwiththeattendingphysician.Attendingphysiciansareexpectedtoseeanddiscussthesecaseswiththefellowoncallinatimelymanner.InhouserequirementsforSaturdayaregenerallycompletedbetween7amand5pm.AtKUH,afellowwilltakecallonSunday.InhouseSundayworkhoursaverage4‐6hours.Whenfellowsarecalledintothehospitalfromhome,thehoursthefellowspendsin‐housearecountedtowardthe80‐hourlimit.Fellowcallbackstothehospitalwhileonhome‐calldonotinitiateanewoff‐dutyperiod.FellowswillbefreefromcallonSundaysattheKCVAMCandRMC.Theprogramdirectorandthefacultywillmonitorthedemandsofat‐homecallintheirprograms,andmakeschedulingadjustmentsasnecessarytomitigateexcessiveservicedemandsandorfatigue.

34
G:LinesofCommunication,ResponsibilityandHand‐OffCommunicationCommunicationbetweenfacultyandfellowsisessentialregardingpatientcareaswellasothersareas.Fellowsareencouragedtousetextpaging,voicemail,EMRandGroupWiseelectroniccommunicationtoupdatefacultyofanyinteractionswithpatients.Telephonecallsbetweenpatientsandfacultyshouldbechartedastelephoneencounterintheelectronicmedicalrecordedandcopiedtothefacultyattendingphysicianinatimelymanner.Whencomplexdecisionsareaddressed,fellowsarerequiredtocontactfacultyatoncepersonallyorbyphone.Facultysupervisionoccurscontinuously.Duringthefirstyearoftraining,fellowsreviewallchangesintherapyorrecommendationsforinvasiveprocedureswiththefacultyattendingpriortomakingtherecommendationtoanotherphysician.Duringthesecondyear,ifthetraineehasmadesatisfactoryprogress,theyaregivenmoreresponsibilitytomakerecommendationsifhe/sheiscomfortableandconfidentintherecommendationandthenreviewwiththeIDattendingfollowingthecommunication.Traineerecommendationsmustbereviewedwithin24‐hours.TraineesareencouragedtocontacttheconsultingIDphysician,atanytimedayornightregardingtheirrecommendations.Suchsupervisionappliestoinpatientandoutpatientcare,homehealthcaremanagement,phonecallsfromoutsidephysiciansorfamilymembers.Supervisionbyattendingfacultymemberisexpectedforallprocedures.Duringaclinicalservicerotation,fellowsmayworkdirectlywithmedicalstudentsandInternalMedicineresidentsassignedtotheservice.StudentsshouldreportinitiallytoIMresidentsortoIDfellowsaccordingtotheservicetheyareassigned.TheIMresidentsreporttotheIDfellowwhomanagestheconsultationservices.AnyofthetraineesmaydirectlycontacttheIDconsultationattendingatanytimeforproblems,advice,ordirection.Whencommunicatingwithotherservices,studentsandresidentsmustbeclearthattheirrecommendationsaresuggestionsandmustbereviewedwiththeIDattendingpriortomakingaformalrecommendation.IDServiceHand‐OffFellowsareinstructedtofollowastandardhand‐offprocesswhenrotatingfromonemonthlyconsultativemonthtothenext(SeeAppendixpg).TheprocessisbasedontheANTICIpatemodel.Onthefinaldayofconsultrotation,thefellowisaskedtoEmailacheckoutlistofthepatientstheyareactivelyfollowingtothefellowtakingovertheirservice.Emailsshouldonlybesentusingthepasswordprotected/securedkumc.eduaddresswithtitle[SecuredPatientInformation].Theemailshouldinclude:1)AtKUH:allpatientsontheteam’sEMRlist(i.e.TeamAlist)2)AtResearchMedicalCenter:theICUpatientslikelytoremaininICUatthetimethenewfellowwilltakeovertheservice3)AtKCVAMC:allpatientsontheIDinpatientconsultservicelist.Fellowsshouldcopytheattendingphysicianonthischeckoutforreviewofcontent.Ifthefellowisroundingwitharesident/studenttheyaretocopythemaswell.Thecheckoutisahelpfulteachingtool.Fellowsshouldalsoencouragetheresidentworkingwiththemtosignouthis/herpatients

35
totheincomingresidentaswellforimprovedcontinuityofcare.SignoutnotesshouldincludetheelementsofANTICipate:Administrative,NewInformation,Task,Illness,andContingencyplans.Theemailshouldprovidethenewfellowtimetoreviewandcall/email/pagewithquestionsandshouldbecompletedassoonaspossiblethedayservicerotationsoccur.Thecheckoutshouldconcludewithacontactpiecee.g.pleasecallmycellat999‐999‐9999after8tofurtherdiscussthepatientsorifyouhaveadditionalquestions.Itmayhappenthatrelevantquestionsdonotariseuntilthefirstdaythenewfellowtakesovercareandfellowsshouldbepreparedtofieldquestionslatershouldtheycomeup.Inadditiontofellowhand‐off,attendingphysicianswillbeengaginginasignoffprocessastheyrotateonandoffserviceaswellasonweekendcoverage.Thiswilloccurthroughwrittenandverbalreport.Fellowsareexpectedtobecopiedonwrittenhand‐offreportsandavailablefordiscussionsthatmightoccur.Atallinstitutionstheactivepatientlistsintheelectronicrecordshouldbekeptupdatedwithservicedesignationandprovidername.ThisprovidesboththeIDserviceandotherpatientcareprovidersawarenessoftheassignedIDpatientandcontactinformationfortheconsultingteam.Non‐teachingPatientsAnoccasionalpatientisseenbythefacultyattendingphysicianandnotbytheIDfellow.Suchapatientisconsideredanon‐teachingpatient.Fellowsarenotexpectedtoprovideanytypeofroutineservicesforsuchpatients.Fellowsdonotroundonthem,donotwriteordersnormonitortheirlaboratorystudies.Ifthefellowshouldreceiveacalltoassistinthemanagementofsuchapatient,theyareexpectedtocontacttherespectiveIDconsultantattendingphysicianortheon‐callattendingstafftoconferandtoprovidemanagement..AtKUHthereare5IDconsultationservices.NotallIDservicesarecoveredbyanIDfellow.Duringregularworkhours,fellowsarenotexpectedtocoverorevaluatepatientswhoarenotontheirassignedservice,unlessthereareexceptionalcircumstances.Afterhourstheon‐callfellowmaybeaskedaboutclinicpatientsorinpatientswithwhomheorsheisnotfamiliar.Fellowsareexpectedtoreviewtherelevantrecordsasindicatedandtodeveloparesponsewhichmaybedelivereddirectlytothephysicianorpatientcalling.Insituationsinwhichthefellowisuncertainastowhichcourseofactionshouldbepursued,heorsheshouldcalleithertheattendingoncall,orthefacultymemberfollowingthepatient.Attendingsareopentoquestionsregardingtheirpatientsatalltimes,andfellowsshouldnothesitatetocall.ATRMCandtheKCVAMCIDconsultationpatientsareonasingleservice.Fellowsareexpectedtoevaluatenewconsultsontheseservicesandfollowthemdaily.Thereisnoafterhourscallforfellowsateitherlocation.Fellowsarenotaskedtocovernon‐teachingpatients.OrderWritingInfectiousDiseasesFellowsdonotwriteroutineordersonpatientsseeninconsultation.Exceptionstothisruleincludethefollowing:1)Whenrequestedbytheconsultingservice.2)Iftheclinicalconditionoftheindividualpatientrequiresatimelyorderandtheprimary

36
serviceisnotimmediatelyavailable.ItistheresponsibilityoftheIDfelloworattendingwhoiswritingtheordertonotifytheprimaryservicethattheorderwaswritten.Thismaybedonebyphone,textpageorEMRnotificationoftheprimaryservice.FellowsmustundergotheappropriateEMRtrainingpriortowritingorders.TheProgramrequiresthatallfellowsabidebythehospital’sorderguidelinesforlearner’s‐in‐trainingregardingallpoliciesincludingorderwritingpoliciesforphysiciansasoutlinedbythePharmacyDepartment.Ingeneral,itisthefellow’sresponsibilitytoensurethathis/herDEAlicenseisup‐to‐dateandthatthenumberisprovidedtothepharmacyDepartment.Whenconcernsaboutafellow’sorderwritingcompetencyareraised,afellowhashis/herorderwritingprivilegessuspendedandmusthaveallorderscosignedbeforetheybecomepartofthechartandarecarriedout.ThisdecisionisattheProgramDirector’sdiscretionandexplicitlyoutlinedtothefellowinquestionbeforeimplementation.LinesofresponsibilityTheIDDivisionDirectorreportsdirectlytotheChairoftheDepartmentofInternalMedicinewhoisresponsibletotheDeanoftheMedicalSchool.TheIDDivisionFellowshipdirectorreports,inthiscapacity,totheDepartmentofMedicineResidencyandFellowshipCommitteeandDirector.TheInternalMedicineResidencyandFellowshipDirectorreportstotheDIO. TheIDattendingreporttotheDirector,DivisionofInfectiousDiseases.TheIDfellowsareresponsibletotheIDattendingassignedtooverseeclinicalresponsibilitiesforpatientrelatededucationalmatters.FellowsaretoreporttotheIDDivisionDirectorortotheIDFellowshipDirectorforfellowshipconcerns.H.MeetingAttendanceFellowsareexpectedtoattend3weeklyconferencesandonemonthlyconference.
Monday7amCaseConference Tuesday12pmJournalClub Thursday12pmCoreCurriculumConference Wednesday12:30pm,monthlyResearchConference
TheMondayamCaseConferenceisconductedatKUMC.WhenafellowisassignedtoarotationoutsideKUMCtheyareexpectedtotraveltoKUMCforthisconferencesbutreturnpromptlytotheirtrainingsitetocompleterotationassignmentsinatimelymanner.JournalClub,CoreCurriculumandResearchConferencesareavailablethroughinteractivewebbasedpresentationanddonotrequirethatfellowstraveltoKUMC.FellowsareprovidedcomputerandofficespacetoparticipateinthesewebbasedconferenceswhenassignedtorotationsoutsideKUMC.Fellowsareexpectedtoaccuratelyrecordattendanceandtimingwiththeircentraladministration.Fellowsareexpectedtoattendallconferencesunlessillnessorvacationprecludes.Intheeventofamissedconference,PowerPointpresentationsareavailableonasecuredivisionalwebsite.Itistheexpectationthatfellows

37
willreviewthecontentofamissedconferencewithinareasonableperiodoftime.ItistheexpectationoftheprogramthatIDfacultywillroutinelyattendthesemeeting.TheDivisionregardsseveralinstitutionalmeetingsasanintegralpartoffellowshipeducation.Fellowsareexpectedtoparticipateinthefollowingmeetingsateacheducationalsite(KUH,KCVAMC,andRMC):infectionpreventionandcontrol,pharmacyandtherapeuticsantibioticsubcommittee,PatientSafetyConferences,ClinicalPathologicConference,InternalMedicineGrandRounds,InternalMedicineCoreConferencegivenbyIDfaculty.Inaddition,fellowsareexpectedtoparticipateinregionalmeetingsincludingKansasCityInfectiousDiseasesSociety(KCIDS)andKansasACP.I.VacationandLeaveTimeScheduledleave(sickleave,maternityandpaternityleave,personalandinterviewtime)mustberequestedinadvancebycompletingthe“DivisionofInfectiousDiseasesFellowLeaveRequest”form.ThisformmustbesignedbyboththeDivisionDirectorandtheIDattendingontheserviceatanysite(RMC,KCVAMC,KUH)influencedbytheleave.TheIDOfficeCoordinator,willmaintaintheformsandprovideofficialnotificationthatleavetimehasbeenapproved.TheIDDivisionrequiresthatIDfellowscompletetheLeaveRequestformatleast6weekspriortoplannedvacation,meeting,orothertimeawayfromanyrotation.VacationFellowsareentitledto3weeksvacationeachyear.Inaddition,fellowsmaytakeoneweekofCME/meetingactivityiftheyarepresentingapaperorposterataregionalornationalmeeting.Attendanceatmeetingswherethefellowdoesnothaveascheduledpresentationwillcounttowardvacationtime.Fellowsareexpectedtotakevacationin1‐weekblocksunlessaspecialexceptionhasbeengranted.VacationsgenerallystartonMondaysandfinishonSundays;howeversomeexceptionscanbemadebasedonthefellowsschedule.The3weeksmaynotbesplittomakemorethantheintended3weeks.Thethreeweek’svacationrefersto3x5workdaysexcludingweekends,not21dayssplittomean4+weeks.Vacationsshouldbeplannedsothatone‐weekistakenateachinstitution(RMC,KCVAMC,andKUMC).TheKUInfectiousDiseasesandInternalMedicineprogramsrequiresleavewithoutpayforfellowthatdoesnotreturnontimefromvacation–includingpersonsunabletoreturnontimeduetoimmigrationprocessreasons.ThisprogramalsoadvisesIDfellowsthattheprogramisnotresponsibleforproblemsthatimpedeascheduledinternationalreturn.Shouldanyfellowwishadviceonthismatter,theymayseekcounselfromtheKUMCofficethatspecializesinimmigrationmattersandimmigrationlaw.PersonalandInterviewLeaveFellowsreceiveuptothree(3)daysduringtheirtrainingtouseforinterviewingforpost‐fellowshippositions.Fellowsarealsoentitledto2personalleavedaysduringthefellowship.ApprovalforinterviewleavemustbeobtainedfromtheProgramDirector,andtheIDofficeadministrativestaff.Writtennotificationmustbeonfileinthefellowship

38
officeatleast6weekspriortotheleave.Notificationofapersonaldayleaveuseshouldbeprovidedtotheattendingandfellowshipofficeassoonasitisevidentthatthefellowwillrequiretimeoff. SickLeaveTheUniversitywillprovideupto10workdaysofsickleaveperyeartocoverpersonalillnessorillnessintheresident’simmediatefamily(spouseorchildren).Sickleavecannotbeaccumulatedfromyeartoyear.TheuseofsickleavemustbeapprovedbytheProgramDirectororDivisionChair.AtthediscretionoftheProgramDirectororChair,aphysician’sstatementmayberequiredasaconditionofapprovalofsickleaveorforreturntowork.Forshort‐termillnesses(colds,fluduringyourresidency)fellowsareaskedtosimplyinformtheappropriateIDattendingandDivisionAdministrativeCoordinator.Foranyillness,whichwillrequiretheresidenttotakealeaveofabsence,promptnotificationtotheProgramDirectormustbeobtainedinwriting.Shouldaleaveofabsenceexceedaccruedtime,stipendpaymentswillbeinterrupted.However,familyhealthinsurancebenefitswillcontinueaslongastheresidentpaystheindividualpremium.TheAmericanBoardofInternalMedicineallowsuptoonemonth,peryear,astimeawayfromtheprogram.TimeusedbeyondthisonemonthwillberequiredtobemadeuptomeettherequirementsforwritingtheBoards.TheABIMdoesnotdistinguishbetweenvacationtimeandleaveforillness,includingpregnancy‐relateddisabilities,andincludesthemastimeawayfromtheprogram.(SeeIMHouseStaffProgramManual,SectionL)FamilyLeavePolicyTheDivisionofInfectiousDiseasesfollowsthefamilyleavepolicydelineatedintheKUSchoolofMedicineGraduateMedicalEducationPolicyManual(Section5).Thisdocumentincludesdescriptionofleavepolicyforeachparent,andsupersedesanypolicyoftheIDDivision.Shouldtherebeextenuatingcircumstances,theDivisionDirectorwelcomesthefellowtobringanyunforeseenproblemstoattentionforconsideration.ItisimportanttoinformtheProgramDirectorpromptlyuponknowledgeofpregnancy.Thispermitsnecessaryadjustmentsintheschedule.Ingeneral,maternityleaveiscoveredbyunusedsickleave/vacationtime.Therefore5weeksincluding3weeksofvacationand2weeksofsicktimecanbeusedtocovermaternityleave.Oneweekofvacationorsickleavemaybetakenforpaternityleave.Shouldaleaveofabsenceexceedaccruedtime,stipendpaymentswillbeinterrupted.However,familyhealthinsurancebenefitswillcontinueaslongastheresidentpaystheindividualpremium.Inaddition,residentsarerequiredtomakeuptimeattheendofresidencyshouldtheyexceedtheiraccumulatedtimeforleave.ThisissubjecttoapprovalfromtheProgramDirectorastheDepartmentofMedicinebecomesfinanciallyresponsibleforaresident’ssalaryiftrainingiscompleted“offcycle,”orafterJune30ofthesecondyearoftraining.(SeeIMHousestaffProgramManual,SectionM)LateStart

39
TheIDprogramcannotallowalatestart(afterJuly1)totheusualtrainingperiodduetofinancialrestraintsattheUniversity.Thismeansthatanunscheduledandunforeseenabilitytoinitiateortocontinuetrainingontimemayresultintheinabilityoftheprogramtoacceptsuchafellow.J.BenefitsCompensationissetbytheDepartmentofMedicine.ThefirstyearfellowisconsideredatthePGY4levelandthesecondyearatthePGY5level.AdditionalbenefitsarethosedesignatedbytheDepartmentofMedicineforresidentsofthesamelevel.TheseareprovidedbytheDepartmentofMedicineandareoutlinedindetailintheDepartmentofMedicineProgramManual(Section5).BenefitquestionscanbefurtherdirectedtotheIDDivisionadministrator(588‐3891)ortheInternalMedicineBusinessoffice.(588‐6001).
A. PayFellowsgetpaideverytwoweeks,startingtwoweeksafterthefellowcompletesthefirstpayperiod.Aresidentcanchoosetohavethepaycheckmailedtohis/herhomeorhaveitdepositedelectronicallyintohis/heraccount.
B. MedicalinsuranceMedicalinsuranceispaidbytheUniversitybutfellowsdohaveachoiceregardingparticularplans.ThisisthesamechoiceofferedtoUniversityemployees.Detailedinformationonthevariouscoverageplanswillbemadeavailableduringthenewfellow’sorientation.
C. Lifeinsurance.TheDepartmentpurchasesagrouptermlifeinsurancepolicyforallofitsresidentsandfellowswithoutthenecessityofpriorexamination.Thisincludesaccidentaldeathanddismembermentprotectionintheamountof$50,000.Thispolicyisconvertibletopermanentlifeinsurancewithin31daysofleavingthegroup.Thisbenefitshouldbekeptfirmlyinmindasthetrainingprogramfinishes.
D. MalpracticeinsuranceWhilepracticingmedicineattheKUMedicalCenteranditsaffiliatedhospitaltrainingsites,fellowsarecoveredbyaself‐insuranceplanadministeredbytheStateofKansas.Thispolicyprovidesstandardcoverageforallactivitiestypicaltointernalmedicine.ThereistailcoverageforanysuitsfiledafterafellowshaslefttheDepartmentforaperiodof3years.ThispolicycoversfellowsonlywhilepracticingunderapprovedcircumstancesintheKUMCanditsaffiliatedhospitals.Ingeneral,thisisnotconfining.However,whenconsideringissuesrelatedtomoonlighting,theremaynotbecoverageprovidedfornon‐affiliatedhospitals.Itistheresident’sresponsibilitytoknowiftheyhavecoverageduringmoonlightingtime.
E. DisabilityinsuranceTheDepartmentinsuresresidentsshouldtheybecomedisabledandcannotwork.Thepolicypays$1000/monthinbenefitsbeginning181daysafterthedisability.Thispolicytakeseffectwithoutthenecessityofaqualifyingphysicalexamination.Thispolicymaybeconvertedtoprivateuse,againwithoutrequiringanexamination,ifonedecidestodosowithin31daysoftheterminationofwiththeDepartment.Thisispotentiallyaveryvaluablebenefitwhichshouldbeconsideredasoneapproachestheendoftraining.Therearemultiplesupplementalpolicieswhicharefurtherdefinedinoneoftheorientationlectures.

40
F. ParkingAKUparkingpassisprovidedbytheIDDivisionatthebeginningoftheacademicyear.ParkingattheKCVAMCandRMCisalsoprovidedfreeofcharge.
G. WhitecoatsTheIDDivisionprovideseachresidentwithtwowhitecoats.ResidentsshouldbeawarethatitisofficialmedicalschoolpolicythatwhitecoatswithnameandhospitalIDbewornatalltimes.Thissamepolicystatesthatnootherbuttons,stickers,pictures,appliqués,statements,politicalcommentsetc.adornthewhitecoats.
H. AccesstoMedicalLiteratureandBoardPreparationMaterialsTheArchieDykesLibraryfortheHealthSciencesislocatedacross39thStreetnorthofthehospital.Thelibrarystocksthevastmajorityofcommonlydesiredperiodicalsbytheclinicalandbasicsciencestaff.Booksandmanualsarealsoreadilyavailable.Accesstothelibrary’selectronicjournalsanddatabasesareavailableonlinethroughtheKUMCwebsite,bothonandoffcampus.TherearebooksandcomputersavailableintheIDFellowoffice(6065)andtheDivisionLibrary(Delp6070).AlltheUniversityandKCVAMCcomputershaveUpToDateonthemandinternetaccesstotheDykeslibraryisavailable.Inaddition,anumberofboardreviewresourcesareavailableforfellows’useintheIDFellowsoffice
I. WorkenvironmentTheIDProgramwillprovideasafeandadequateworkenvironmentasoutlinedintheGMEofficeHousestaffPolicyandProcedureManual(Section5.8.3).FoodandRestTheProgramwillprovideaccesstofoodserviceandsleepingquarterstothefellowwhileon‐callorotherwiseengagedinclinicalactivitiesrequiringthefellowstoremainintheMedicalCenterovernight.Sleepingquartersandquietroomsarealsoavailableforfellowsshouldtheyexperiencefatiguethatwouldmitigatealertnessmanagementstrategiessuchasstrategicnapping.ProtectiveEquipmentInaddition,personalprotectiveequipmentincludinggloves,face/mouth/eyeprotectionintheformofmasksandeyeshields,andgownswillbeavailable.TheOccupationalSafetyandHealthAdministration(OSHA)andtheCentersforDiseaseControl(CDC)assumethatalldirectcontactswithapatient’sbloodorotherbodysubstancesareinfectious.Therefore,theuseofprotectiveequipmenttopreventparenteral,mucousmembraneandnon‐intactskinexposurestoahealthcareproviderisstronglyrecommended.
K.MoonlightingPolicyProfessionalactivityoutsideofthescopeofthefellowshipprogram,whichincludesvolunteerworkorserviceinaclinicalsetting,oremploymentthatisnotrequiredbytheprogram(moonlighting)shallnotjeopardizeanytrainingprogramoftheUniversity,compromisethevalueofthetrainee'seducationexperienceorinterfereinanywaywiththeresponsibilities,dutiesandassignmentsofthefellowshipprogram.Itiswithinthesole

41
discretionoftheProgramDirectortodeterminewhetheroutsideactivitiesinterferewiththeresponsibilities,dutiesandassignmentsofthefellowshipprogram.BeforeengaginginactivityoutsidethescopeoftheFellowshipProgram,fellowsmustreceivethewrittenapprovaloftheDivisionDirectorand/orFellowshipProgramDirectorofthenature,durationandlocationoftheoutsideactivity.Furthermore,thefrequencyordurationofoutsideprofessionalactivitiesmustnotbesuchastoresultinphysicalandmentalfatigueleadingtoimpairmentoftraining.TheIDfellowmaynotscheduletimetoexceedthe80hoursmaximumdutytimeeachweekmandatedbytheGMEPolicyandProcedureManual.Fellowswhileengagedinprofessionalactivitiesoutsidethescopeofthefellowshiparenotprovidedprofessionalliability.AfellowprovidingservicesoutsidethescopeofthefellowshipprogramshallwarranttoUniversitythatthefellowisandwillremaininsuredduringthetermofanyoutsideprofessionalactivities.TheregulationsgoverningmoonlightingactivitiesandprofessionalliabilityinsurancerequirementsfortheseactivitiesarediscussedintheDepartmentofMedicineProgramManualPolicyandProceduresSectionV.OandtheKUGMEPolicyandProcedureManualSection16.ThedocumentsaremadeavailabletothefellowduringtheDepartmentofMedicineorientationandareavailableonline.L.EthicsWithincreasingmedicalsophistication,theethicalquestions,whichsurroundapatient’scareoftenoverwhelmthemedicaldecisions.Medicaland,evenmoreso,ethicalcomplexitiesarecommonplaceinthefieldofmedicine.Eveninthemostcomplicatedethicalsituation,thefirstandmostimportantstepistotalkwiththepatientand,ifpermittedbythepatient,thefamily.Onlythroughfullcommunicationwiththeappropriatedecisionmakercanthefellowaddresshonestly,thoroughlyandexpedientlytheissuesofconcern.Thehospitalethicscommittee,available24hoursadaybypager,consistsofbothmedicalandotherpersonnelwhoareavailabletoexploreandadviseonmajorethicalconcerns.Physiciansonthecommitteeareavailablefordiscussionandforconsultationatanytime.Inaddition,thereisamonthlyEthicsconferenceheldbytheEthicscommitteeinconjunctionwiththeGeneralMedicinedivision.Ethicaldilemmasarisingontheinpatientmedicalservicesarediscussedinaninformalsetting.M.UtilizationManagementItistheresponsibilityoftheIDFellowtoassurethatdocumentationintherecordcompletelydescribesthepatient'sseverityofillness,aswellastheintensityoftreatmentservicesprovidedtothepatient.Documentationoflevelofcare,complexityofthecase,recordsreviewed,diagnostictestsandradiographspersonallyreviewed,diagnoses,andrecommendedmanagementaretobeincludedoneverynoteinthepatient’schart.N.QualityImprovement

42
ContinuousQualityImprovement(CQI)isanongoing,flexible,integratedandcoordinatedhealthcareprogramthatstressesacommitmenttocontinuouslyimprovepatientcareandserviceandresolveidentifiedproblemsbyassessingandimprovingallaspectsthatmostaffectpatientoutcomes.Itistheresponsibilityofallemployees,includingfellows,toactivelyparticipateintheCQIactivities.ThegoaloftheCQIprogramistodevelopcollectiontools,analyzedata,formulatedatadrivenrecommendationsforimprovement,andcoordinateresolutionoftheidentifiedopportunitiesforimprovement.Inidentifyingopportunitiesforimprovement,theCQIprogramplacesemphasisoncost,quality,access,customerservice,desiredpatientoutcome.Itpursuesopportunitytoimprovecare/service,allowsforresolutionofidentifiedproblems,assuresasafeandhealthyenvironmentforpatients,patientfamiliesandemployees,andensuresappropriateandeffectiveutilizationofresources.ContinuousQualityImprovementActivitiesFacultyandfellowswillbeexpectedtoparticipateinthePatientSafetyConferenceoftheDepartmentofMedicine,whichispresentedmonthly.InthisconferencetheVanderbiltHealthcareMatrixisutilizedtoreviewthecase.ThistoolfollowsthesixACGMEClinicalCompetenciesaswellasthesixIOMAims(safe,timely,effective,efficient,equitable,patientcentered.Thetoolprovidesastructuredopportunityfortheparticipantstolookatanepisodeofcareanddeterminehowthequalityofcarewasaffectedbythecorecompetenciesandidentifypotentialareasofdeficienciesandopportunitiesforimprovement.Similarly,theVanderbiltHealthcareMatrixhasbeenincorporatedintotheweeklyIDCaseConference.HerefellowsandattendingsareprovidedtheopportunitytoexaminetheepisodeofcareinthesettingofthecorecompetenciesandIOMaimsandinstitutechangesdirectlytotheirpatientsandpractice.ThemonthlyDepartmentofMedicineCPCConferencealsoprovidesastructuredenvironmenttoexamineindividualandsystempracticesandopportunitiesforimprovement.LecturescoveringthetopicofqualityimprovementaresponsoredthroughouttheyearbytheDepartmentofMedicine.InfectiousDiseasesFellowsarerequiredtoattend.O.RiskManagementThissectionsupplementstheKUGMEandInternalMedicinePolicyandProcedureManuals.RiskManagementinvolvesboththeHospitalandTheUniversityofKansas.Italsoinvolvesthepreventionorhandlingofadverseeventsandthehandlingoflegalissues.AdverseEventsTheStateofKansasrequiresreportingofalladverseeventstoaconfidentialreportingsystem.Whenapatientsuffersanadverseevent,thefirstpriorityistoassurethepatient’ssafetythroughinterventionandfollow‐up,includingorderinganyadditionalmonitoringortests.Anexamplemightbeananaphylacticreactiontoaknownmedicationallergen.Prioritiesincludestabilizingthepatientandmakingsurestaffreporttheadversethroughthehospitalsadverseeventreportingsystem.

43
Ifanadverseeventoccursthathasthepotentialtoleaveapatientwithsevere,permanentdisabilityordeath,TheJointCommissionrequiresaRootCauseAnalysis(RCA)beconductedtodeterminecontributingfactorsandanactionplantopreventrecurrenceofsuchanevent.TheHospital’s1RiskManagerwillfacilitatetheRCAanditsfollow‐up.FellowsshouldalsocontacttheUniversityRiskManagerat913‐588‐7283,andinformtheUniversityRiskManagerofthesituation.Donotwriteanynotesaboutthesituation,otherthanobjectivechartinginthepatient’srecord,oradditionalnotesintheadversereportingsystemfortheHospitalorfacility.Ifanyoneasksyoutowriteasummaryofevents,contacttheUniversityRiskManager.OtherReasonstoContacttheUniversityRiskManagerInadditiontoseriousorfataladverseeventsinvolvingpatients,theUniversityRiskManagershouldbecontactedwheneverthefollowinghappens:
1. Aphonecallreceivedfromanyattorneyrequestingtomeetwithyou.Thesecanbeplaintiff’sattorneysinourorothersmalpracticecases,defenseattorneysinourorothersmalpracticecases,criminaldefenseattorneys,orcriminalprosecutingattorneys,usuallyaDistrictAttorney’soffice.
2. Asubpoenareceivedfromanysource.Asubpoenaisacourtdocumentdirectingyoutocourttotestifyoradepositiontoprovidesworntestimonypriortoacase,eithercivilorcriminal.AsubpoenamustbeproperlyservedbeforeitisenforceableandtheUniversityRiskManagerwillassistyouinproperlyrespondingtothesubpoenaandassuringyoudonotmissanytimedeadlinesthatmightputyouatriskofbeingheldincontempt.
3. Asummonsreceivedfromanysource.Thisisacourtdocumentthat“summons”youtocourttodefendyourselfinalawsuit.Youhavealimitedtime,20days,torespondtoasummonssocontacttheUniversityRiskManagerimmediately.Adefenseattorneywillbeassignedtoyoutorespondtothesummons.Incivilcases,thesummonsisaccompaniedbyapetitionorcomplaint.Inacriminalcase,thesummonsisaccompaniedbyanarrestwarrant.
4. Ifthereareanyquestionsaboutmedical‐legalsituations.Itisfareasierforeveryoneinvolvedtoanswerquestionsandtakepreventativemeasuresthantoundosomesituations.Examplesinclude:
a. Questionsaroundrequiredreportingofabuse,victimsofcrimes,etc.b. Questionsaroundhowtochartadverseeventsinthepatientchart.c. Questionsaroundlitigationprocess,contactingdefenseattorneys,etc.d. Wantingtoreviewacaseandevaluatepotentialrisksissues.
P.ProfessionalismItisimperativethatthefellowlearnappropriatebehaviorofaprofessionalduringtheirexperience.Itisrecognizedthathealthcareisbestdeliveredwhenphysiciansarecollegial,yetfrankwitheachotherandrespectfulandcaringoftheirpatients.Itisthusthe1ThiscouldbetheVeterans’AdministrationMedicalCenter,theUniversityofKansasHospital,orotherfacilitywherefellowactivitiesareperformed.

44
responsibilityofthefellowtobefit,readyforworkanddressedappropriately.Facultyshouldbenotifiediftheconductofthefellowsiseverconsideredlessthanprofessional.TheProgramDirectorwilldiscusssuchincidentswiththefellowinquestion.Theuseofillicitdrugswillnotbepermittedatanytimeandalcoholshallnotbeconsumedbyanyonewhoisoncalloronactiveduty.Anyonefoundinviolationoftheseruleswillbetreatedinaccordancewithdepartmentalandschoolpolicy.Sexualorgenderharassmentbyfellowsofanyonewillnotbetoleratedandwillbegroundsforreferraltothedepartment'sadministration.Atthesametime,nofellowshouldeverbethesubjectofsexual,gender,religious,ethnicorotherharassment.AnycomplaintofsuchbehaviorshouldbereportedtotheDivisionDirector,theprogramdirector,orthedepartmentchairman.Finally,theDivisionrecognizestheadvantagesofdiversityamongstitsmembersandsupportstheirrightstodifferentreligious,political,economic,andartisticbeliefs.Thus,anydiscriminationorharassmentofanyfellow,oranyothermemberoftheDivision,becauseofthesedifferencesshouldbereported.ThesepoliciesandproceduresareasupplementtothepoliciesandproceduresoutlinedfortheDepartmentofMedicineandtheKUSOMGraduateMedicalEducationOffice.ThesemanualsareprovidedatthebeginningofthefellowshipandavailableonthewebsitesofInternalMedicineortheGraduateMedicalEducationOffice.Q.ImpairmentSatisfactoryperformanceincludestheabsenceofsignificantimpairmentduetophysical,mental,oremotionalillness,personalitydisorder,orsubstanceabuse.Afellowthatshowsimpairedfunctiontoadegreeitiscausinglessthansatisfactoryperformance,and/ortheimpairedfunctionisnotcorrectedorisuncorrectable,islikelytoleadtofutureunsatisfactoryperformance.Everyeffortwillbemadetoreasonablyaccommodatethoseindividualswithconditionsorimpairmentsthatqualifyasadisabilityunderapplicablelaw,providedthattheaccommodationdoesnotpresentanunduehardshipfortheDepartment,theMedicalSchool,orvenuesoftraining.FellowswillneverthelessberequiredtosatisfactorilymeettheDepartment’sperformancecriteria,requirements,andexpectationsoftheInfectiousDiseasesFellowshipProgram.IftheDirectorhascausetosuspectthatafellow’sbehaviormaybealteredduetoaphysicalormentalimpairment,theuseofdrugs,narcotics,oralcohol,theDirectorwillconsultwiththeIMRRCofficetofollowthestandardproceduresoftheUniversityinthisregard.PleaserefertoKUGMEPolicyandProcedureManual(Section7)forthedetailsofinstitutionalpolicyregardingidentificationofimpairment,reintegrationintotraining,andongoingmonitoringofaffectedresidentsorfellows.R.DisciplinaryActions,Probation,SuspensionandTerminationTheFellowshipDirectorortheAssociateFellowshipDirectorisresponsiblefortheevaluationanddisciplineofeachIDfellowinthisprogram.Fellowsaremonitoredand

45
evaluatedbasedonthesixcorecompetenciesandstandardssetforthbytheDivisionandInstitutionandincludethefollowing:
1) Patientcarethatiscompassionate,appropriateandeffectiveforthetreatmentof healthproblemsandthepromotionofhealth.2) Medicalknowledgeincludingestablishedandevolvingbiomedical,basicscienceand
clinical,sciencesandtheapplicationofthesetopatientcare.3) Practice‐basedlearningandimprovementthatinvolvesinvestigationandevaluation
ofthefellow’sownprovisionsofpatientcare,appraisalandassimilationofscientificevidence,followedbyimprovementsindeliveryofpatientcare.
4) Interpersonalandcommunicationskillsthatresultineffectiveinformationexchangemakingprovisiontoteamwithpatients,families,andotherhealthprofessionals.
5) Professionalismasshownbyacommitmenttocarryingoutprofessionalactivitiesandresponsibilities,adherencetoethicalprinciples,andsensitivitytodiversepatienttypesandbackgrounds.
6) Systems‐basedpracticeshownbyactionsthatdemonstrateawarenessofandresponsivenesstothelargerhealthcaresystem,theabilitytoeffectivelyusesystemresourcestoprovideoptimalcare.
Inaddition,thefellowwillcomplywiththerulesandrequirementsofKUH,theKUMCGMEoffice,theDepartmentofMedicineInternalMedicineProgramManual.WhilerotatingattheKCVAMCorRMC,eachfellowwillcomplywiththeirspecificrules,guidelines,andrequirementsaswellasthosepromulgatedbytheBoardsofHealingArtsoftheStatesofKansasorMissouriasrequired.Otherspecificguidelinesrequirethateachfellowwill:
1) Developapersonalprogramoflearningforcontinuedprofessionalgrowthwithguidancefromtheteachingstaff.
2) Participateintheeducationalandscholarlyactivitiesoftheirprogramandteachorsuperviseotherresidents,students,orfellows.
3) Participateinappropriateinstitutionalcommitteesasappointedbythedivisiondirectororthedesignee.
4) Submitregularlyanelectronicanonymousconfidentialevaluationofthefacultyandoftheeducationalexperience.
5) Continueinactivescholarship.Thismayincludepublications,orpresentationsatlocal,regional,ornationalscientificsocietymeetingsandcouldinvolvecases,reportsorclinicalseries,ortranslationalresearch.
6) Beanactiveparticipantinclinicaldiscussions,rounds,journalclubs,andresearchconferencesinamannerthatpromotescollegiality,inquiryandscholarship.
PerformanceDeficienciesAftertheDirectorreceivesnotificationofsatisfactoryevaluationsandcompliancewiththestandardsoutlinedaboveandafterallothertermsoftheIDFellowshiptrainingPoliciesandProceduresaremet,eachfellowshouldexpecttocontinuetothenextleveloftrainingtocompletetheprogram.
46
Shouldafellowbefoundtobedeficientinanyofthecriteriaorparametersofperformanceandnotmeetadvancementorpromotionspecifics,he/shewillmeetwiththeProgramDirector,theAssociateDirectorortheirdesigneewherein:1.Theexpectationsanddeficiencieswillbestated.2.Whattheindividualcandotoimprovewillbeexploredandplanned.3.Anattemptwillbemadetodetermineifthereareoutsidefactorswhichmayexplainwhyaproblemhasdeveloped.AtthispointadeterminationwillbemadebytheprogramleadershipofwhetherthefellowisingoodstandingorisinaPerformanceWarningStatus(PWS).ThePWSwillinvolveaperiodof3months,wheretheperformanceofthefellowcanbemonitoredmoreclosely.PWSisdesignedtoidentifyweaknessesthat,ifnotremedied,mayleadtoprobationordismissal.TheProgramDirector,AssociateProgramDirector,ortheirdesigneewillberesponsiblefordeterminingtheprocessforremediation.Thismeetingwillbedocumented,giventothefellowforhis/heragreementofthemeetingcontent,andafinalcopywillgointothefellow’spersonalfile.Unlessotherwisestated,afellowinPWSisstillconsideredtobeingoodstandinganddoesnothavetoreportthisactiononfutureprofessionalapplications.Should,however,thefellowsbeplacedinPWSagainaftertheinitial3monthperiod,he/sheiseligibletobeplacedonprobation.Shouldtheresidentcontinuetobedeficientdespiteappropriatecounseling,professionalassessmentandinput(ifindicated),andfacultyefforts,aperiodofprobation(usually3months)isindicated.Beforebeingplacedonprobation,thefellowwillappearbeforetheResidencyEducationCommitteewhereinhis/hercasewillbediscussed.Thefellowinquestionwillhavetherighttorebuketheclaimsmadeagainsthim/her.Ifhis/herperformanceisdeemedtowarrantprobation,thentheinstitution’sGraduateMedicalEducationofficewillbenotifiedandallpoliciesdelineatedwithintheGMEPolicyManualwillbefollowed.Aformalwrittenletterofprobationwillbedrafted.Awrittenletterofprobationshould:1.Statedeficienciesthattheindividualhasbeencounseledforanddocumentthatinsufficientimprovementhasbeenmade.2.Stateexplicitlythatbecauseofthistheindividualisbeingputonprobation.3.Stateperiodofprobation,4.Statewhatisexpectedduringthisperiod.5.Statewhatwillbedonetoassisttheindividualinmeetingtheseexpectations.6.Statewhatthemechanism(s)willbetodetermineimprovement.7.Statewhattheconsequencesoroptionsaretobeifexpectationsarenotmet.Thedeficientfellowwillreceivethisletterandacopywillgointohis/herpersonalfile.Fellowsplacedonprobationmayhavedifficultywithlicensureinsomejurisdictions.TheprobationaryperiodisintendedtoemphasizetotheresidenttheimportanceofsatisfactorilymeetingthefellowshiptrainingrequirementsandexpectationsoftheDepartment.Thefellowshouldclearlyappreciatethemeaningofexpectedremediation,appreciatethedefinedtimeinwhichthismustbeaccomplished,andalerthis/herattendingfacultyduringthisperiodofprobationtotheimportanceofhelpingthefellow

47
withdefinedproblems.Thefacultyshouldprovideanhonestevaluation,andcomplywithrequestsbytheDepartmentforassessment,counseling,orassistance,shouldtherebeanypossibilityofpersonalproblems,learningdisability,oroutsidefactorsthatmaybecontributorytothefellow’sperformance.Fellowsonprobationmustachieveasatisfactoryevaluationfromtheirattendingfacultyonassignedclinicalservicerotationsduringtheirprobationaryperiod.Probationaryactionswillonlybesharedwiththoseneedingtoknow.Shouldthefellowfailtheaboveprobationaryperiod,thenatthediscretionoftheDepartment,aletterextendingtheprobationmaybeissued,oraletterdismissingthefellowfromtheprogramonadesignateddatewillbeissued,assumingthatdismissalwasaconsequenceofprobationaryfailureasstatedabove.Accompanyingthislettermustbeastatementofthefellow’srightofappeal.Afellowwhomayormaynothavebeenonprobation(andsuccessfullyaccomplishedremediationintheprobationaryperiod),butwhohasreceivedintermittentlowsatisfactoryorisolatedunsatisfactorymarksduringthe8to12monthsoftheacademicyear(andparticularlyfollowingaprobationaryperiod),maybeaskedtorepeattheyear.ThisisparticularlytrueiftheDepartmentwillinalllikelihoodbeunabletocertifytheresidenttositfortheABIMexaminationshouldtheresident’sperformancetrendcontinue.(PleaserefertotheGMEmanualforacomprehensivesectionondeficiencyandremediationpolicies.)S.GrievanceResolutionGrievablemattersarethoserelatingtotheinterpretationof,applicationof,orcompliancewiththeprovisionsoftheResidentAgreement,thepoliciesandproceduresgoverninggraduatemedicaleducation,andthegeneralpoliciesandproceduresoftheUniversityofKansasMedicalCenter.Questionsofcapricious,arbitrary,punitiveorretaliatoryactionsorinterpretationsofthepoliciesgoverninggraduatemedicaleducationonthepartofanyfacultymemberorofficeroftheInfectiousDiseasesFellowshipProgramaresubjecttothegrievanceprocess.Agrievanceprocedureisavailabletofellowsforresolutionofproblemsrelatingtotheirappointmentsorresponsibilities,includingdifferenceswiththeSchool,Program,oranyrepresentativethereof.TheSchoolensurestheavailabilityofproceduresforredressofgrievances,includingcomplaintsofdiscriminationandsexualharassment,inamannerconsistentwiththelawandwiththegeneralpoliciesandproceduresoftheUniversityofKansasandtheSchool.AcompletedescriptionofthegrievanceprocessisavailableintheIMandGMEProgrammanuals

48
VII. APPENDIX

49
IDCORECURRICULUMSCHEDULE
Itisexpectedthatbytheendofthetrainingperiod,thetraineewillhavehadextensivepersonalexperienceandwillhaveacquiredaknowledgebasefromdidacticteachingandreadingtodealcompetentlywithallofthefollowing:(Pleaseseedivisionalcalendarforeachspecificyearforthedatesoftheselecturesandpresenters)Year1and2BootCampCurriculum(Twiceweeklyfor5weeks)InfectioncontrolLine‐relatedinfectionsOsteomyelitis:(includingvertosteo/septicarthritis)ProstheticJointInfections/ForeignbodyInfections(CNSshunts;pacemakers,etc.)HIV:GeneraloverviewHIV:anti‐retroviralsHIV:opportunisticinfectionsAntibioticsI:B‐lactams/aminoglycosidesAntibioticsII:otherabxclassesMicrobiologyLab:basicoverview

50
Year1Curriculum(Weeklyconference)
Nocardia/actinomycesSTD’s:gonorrhea,Chlamydia,chancroid,etcDesigningaresearchprotocolSyphilisandotherspirochetalillnessesFungalInfectionsI:endemicfungi(histo/blasto/cocci,sporothrix)FungalInfectionsII:cryptococcus/candidaspp.FungalInfectionsIII:filamentousfungiHuman/animalbiteInfectionsinIVDU’sAntiviralagentsPK/PDFoodpoisoningBMToverviewStemcell/BMTInfectionsTropicalmedicinereview(otherthanmalaria)TravelmedicineZoonoses
Burns/WoundsHIV:relatedmalignanciesMono‐likesyndromes(DMV,EBV,Toxo,etc)Bacterialgenetics/mechanismsofresistanceStreptococcalinfectionsStaphylococcalinfections/virulencefactorsBasicsofbillingImmunosuppressionImmunizationsofadultsAntimicrobialProphylaxis:(surgical;bacterialendocarditis,HIVPEP,Hepatitis,Rabies,Varicella,etcAntifungalagents

51
Year2Curriculum(WeeklyConference)MoleculardiagnosticsSepsisFebrileneutropeniaCommunity‐acquiredpneumoniaHospital‐acquiredpneumoniaSOTInfections:ISOTInfections:IIHepB/HepCHepatitisA,D‐GCNSII:acutemeningitis/brainabscessesCNSIII:chronicmeningitis/prionsAntibiogramIntraabdominalinfectionsC.diff/InflammatoryEnteritidiesTuberculosisNon‐tuberculousmycobacteriumMicrobialpathogenesisHeadandneckinfectionsInfectionsoftheeyeFUOHSV/VZVRickettsialinfectionsTick‐borneIllnessesHIV:Coinfection(TB;HepB/HepC;pregnancy)UrinarytractinfectionsPost‐partuminfectionsBioterrorism

52
IDCONFERENCES
Conference Day Time Frequency IDCaseConference Monday 7am WeeklyIDJournalClub Tuesday 12pm WeeklyIDCoreConference Thursday 12pm WeeklyIDResearchMeeting 3rdWednesday 12:30pm MonthlyIMPatientSafety 2ndMonday 12pm MonthlyIMClinicalPathologicConference 4thTuesday 12pm MonthlyIMGrandRounds Friday 8am WeeklyInfectionControlandPrevention Friday 1pm MonthlyAntibioticP&TSubcommittee 2ndTuesday 7am MonthlyGMEcurriculumseries Tobeannounced 6:30am Quarterly

53
GMERESIDENTSUPERVISIONTEMPLATE
Per
Pro
gram
Spe
cific
RR
C R
equi
rem
ents
RRC APPROVED LICENSED INDEPENDENT PRACTITIONER SUPERVISOR (PR VI.D.1) VI.D.1. In the clinical learning environment, each patient must have an identifiable, appropriately-credentialed and privileged attending physician (or licensed independent practitioner as approved by each Review Committee) who is ultimately responsible for that patient’s care. Infectious Diseases does not utilize licensed independent practitioners. VI.D.1.a) This information should be available to residents, faculty members, and patients. VI.D.1.b) Residents and faculty members should inform patients of their respective roles in each patient’s care. OPTIMAL CLINICAL WORKLOAD (PR VI.E.) Clinical Responsibilities The clinical responsibilities for each resident must be based on PGY-level, patient safety, resident education, severity and complexity of patient illness/condition and available support services. The optimal clinical workload is not currently defined by RRC for Infectious Diseases. MEMBERS OF THE INTERPROFESSIONAL TEAM (PR VI.F.) VI.F. Teamwork Residents must care for patients in an environment that maximizes effective communication. This must include the opportunity to work as a member of effective interprofessional teams that are appropriate to the delivery of care in the specialty. Specific review committee elements have not been defined by RRC for Infectious Diseases. COMPETENCIES TO ALLOW PGY1 RESIDENTS TO PROGRESS TO INDIRECT SUPERVISION (PR VI.D.5.a).(1) ) Not applicable for Infectious Diseases DEFINING RESIDENT LEVELS “INTERMEDIATE LEVEL” & “FINAL YEARS OF TRAINING ” For establishing the minimum rest period between duty periods (PR VI.G.5.b&c) Not applicable for Infectious Diseases VI.G.5.c) Residents in the final years of education [as defined by the Review Committee] must be prepared to enter the unsupervised

54
practice of medicine and care for patients over irregular or extended periods. CIRCUMSTANANCES WHEN RESIDENTS IN THEIR FINAL YEARS OF EDUCATION MAY REMAIN OR RETURN IN < 8 HOURS (PR VI.G.5.c).(1)) The majority of RRCs defined these circumstances as “required continuity of care for a severely ill or unstable patient, or a complex patient with whom the resident has been involved; events of exceptional educational value; or, humanistic attention to the needs of a patient or family. As a consulting service, requirements for fellows to remain or return with less than 8 hours off does not occur. DEFINED MAXIMUM NUMBER OF CONSECUTIVE WEEKS AND MAXIMUM NUMBER OF MONTHS PER YEAR OF IN-HOUSE NIGHT FLOAT (PR VI.G.6.) VI.G.6. Maximum Frequency of In-House Night Float Fellows must not be scheduled for more than six consecutive nights of night float. Infectious Diseases fellows do not participate in night float.
Program-specific guidelines for circumstances and events in which residents must communicate with appropriate supervising faculty (PR VI.D.5)
1. Admission to Hospital 2. Consultation 3. Transfer of patient to a higher level of care 4. End-of-Life decisions
Source of specific criteria and/or specific national standards-based criteria
used to evaluate each resident’s abilities (PR VI.D.4.a) RRC has yet to define specify criteria or identify national standard based criteria to
be used for Infectious Diseases

55
Inpatientservice Outpatientclinic Research MicrobiologyFellowswill:‐gatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;performandinterpretGramstains;managepatienttherapies,emphasizingappropriateuseofantimicrobials;andworkwithotherstoprovidepatient‐focusedcare(PC,MK,P,CS,PB,SBL)‐managecommonandcomplexID;problemsnthefaceofantibioticresistance(PC,MK,PBL)‐developskillstoappraisethecurrentmedicalliteraturetosupportdecision‐making(PBL,MK‐developcommunicationskillstofacilitatethelearningofothers(PBL,SBL,CS,P)‐useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes(CS,P)‐beresponsivetopatientsandsociety,supersedingself‐interest(P)‐demonstrateintegrity,honesty,reliability,cooperative,andacceptresponsibility(P)‐workwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare(SBL,CS,P)
Fellowswill:‐managemedicalandpsychosocialaspectsofcommonandcomplexoutpatientinfectiousdiseases(PC,MK,CS,PBL,SBL,P)‐developskillintheuseofantibiotics,andprophylacticagents(PC,MK)‐appraisethemedicalliteratureregardingoutpatientcaretosupportdecisionmaking(PBL,MK,SBL,PC)‐Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes(CS,P)‐Beresponsivetoneedsofpatientsandsocietysupersedingself‐interest(P)‐demonstraterespect,compassion,andintegrity;behonest,reliable,cooperative,andacceptresponsibility(P)‐Workwithhealthcareprofessionalseffectivelytoprovidepatientfocusedcareadvocateforqualitypatientcare(SBL,CS,P)
Fellowswill:‐provideawrittendescriptionoftheirproposedprojectandseekIRBapproval(CS,P,SBL)‐gainskillsinthedesignofapproachesthatprotectsubjectsinresearchstudies(PC,MK,P,PBL,CS)‐learntheconstructionofstudieswhichadequatelystresstheethicsofclinicalresearch,appropriatestatisticalmodeling,obtainingeffectiveinformedconsent(PC,MK,P,PBL,SBL,CS)‐communicatinginterimresultstopatientsfaculty,andtheIRB(CS,P)
Fellowswill:‐becomefamiliarwiththetechnicalaspectsofpathogenisolation,sensitivitytesting,andmolecularmethods(MK,PC)‐communicateclearlywiththemicrobiologystaffandclinicalservice(SBL,CS,P)‐demonstratehonesty,integrity,reliability(P,CS)
OverviewoftheEducationalObjectiveswithReferenceToSixCoreCompetenciesYearOneFellowship
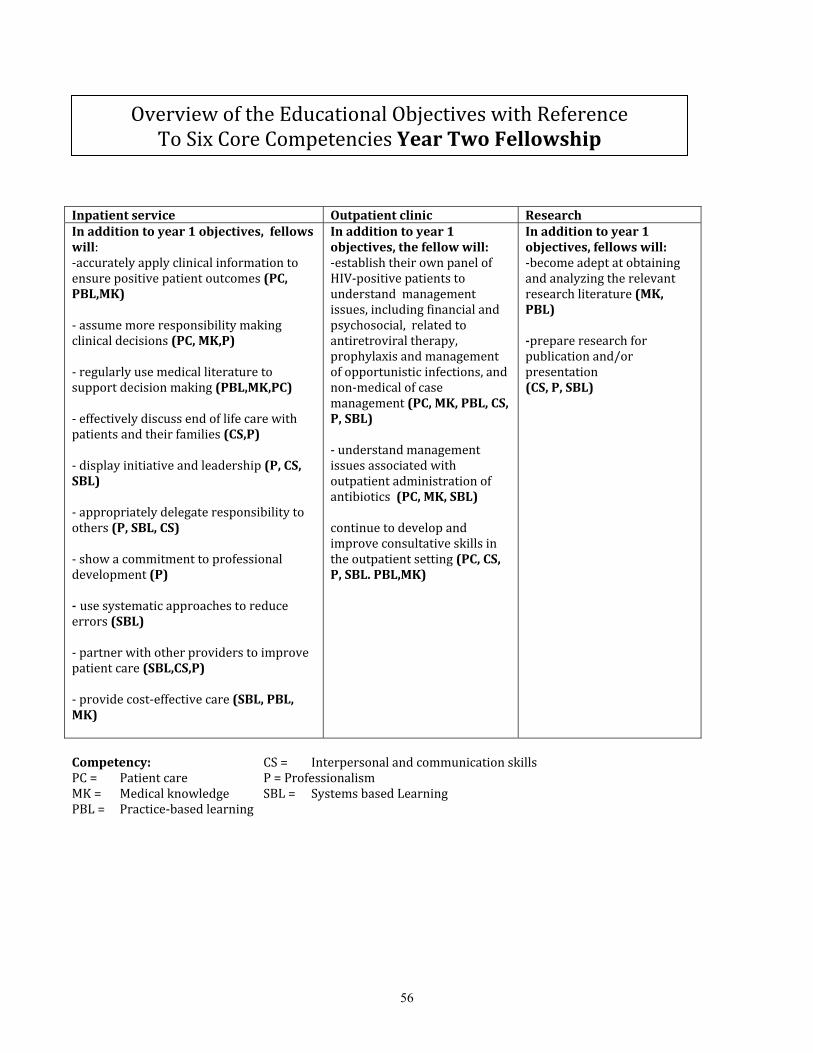
56
Inpatientservice Outpatientclinic ResearchInadditiontoyear1objectives,fellowswill:‐accuratelyapplyclinicalinformationtoensurepositivepatientoutcomes(PC,PBL,MK)‐assumemoreresponsibilitymakingclinicaldecisions(PC,MK,P)‐regularlyusemedicalliteraturetosupportdecisionmaking(PBL,MK,PC)‐effectivelydiscussendoflifecarewithpatientsandtheirfamilies(CS,P)‐displayinitiativeandleadership(P,CS,SBL)‐appropriatelydelegateresponsibilitytoothers(P,SBL,CS)‐showacommitmenttoprofessionaldevelopment(P)‐usesystematicapproachestoreduceerrors(SBL)‐partnerwithotherproviderstoimprovepatientcare(SBL,CS,P)‐providecost‐effectivecare(SBL,PBL,MK)
Inadditiontoyear1objectives,thefellowwill:‐establishtheirownpanelofHIV‐positivepatientstounderstandmanagementissues,includingfinancialandpsychosocial,relatedtoantiretroviraltherapy,prophylaxisandmanagementofopportunisticinfections,andnon‐medicalofcasemanagement(PC,MK,PBL,CS,P,SBL)‐understandmanagementissuesassociatedwithoutpatientadministrationofantibiotics(PC,MK,SBL)continuetodevelopandimproveconsultativeskillsintheoutpatientsetting(PC,CS,P,SBL.PBL,MK)
Inadditiontoyear1objectives,fellowswill:‐becomeadeptatobtainingandanalyzingtherelevantresearchliterature(MK,PBL)‐prepareresearchforpublicationand/orpresentation(CS,P,SBL)
Competency: CS= InterpersonalandcommunicationskillsPC= Patientcare P=ProfessionalismMK= Medicalknowledge SBL= SystemsbasedLearningPBL= Practice‐basedlearning
OverviewoftheEducationalObjectiveswithReferenceToSixCoreCompetenciesYearTwoFellowship

57
OVERVIEWOFGOALSANDOBJECTIVESFORROTATIONS
InfectiousDiseasesFellowship:KansasUniversityHospital(KUH)InpatientConsultation
Duration: 1styearFellowsareassignedtotheKUHinpatientconsultservicefor6months
2ndyearFellowsareassignedtotheKUHinpatientconsultservicefor9months.
Supervision(Interactionwithfaculty)
SupervisionofthefellowbyInfectiousDiseaseattendingatKUHforinpatientservice
RotationFacility UniversityofKansasHospital
RequiredDidactics/conferences:
IDCaseConference,IDJournalClub,IDCoreConference
InfectiousDiseasesFellowship:KUHInpatient
ConsultationRotation
FellowYear1&2
PATIENTCAREGoal:Demonstratecompetenceinthecontinuumofinpatientcareforinfectiousdiseasespatients
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;
DemonstrateabilitytoperformandinterpretGramstains;
Demonstrateabilitytomanagepatienttherapies,emphasizingappropriateuseofantimicrobials;
Workeffectivelywithotherstoprovidepatient‐focusedcare;
DemonstrateabilitytomanagecommonandcomplexIDproblemsinthefaceofantibioticresistance
2 Accuratelyapplyclinicalinformationtoensurepositivepatientoutcomes
Goal:Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Thiswillincludethefollowinginfectiousdiseasesareas:BacterialinfectionsFungalinfectionsViralinfections
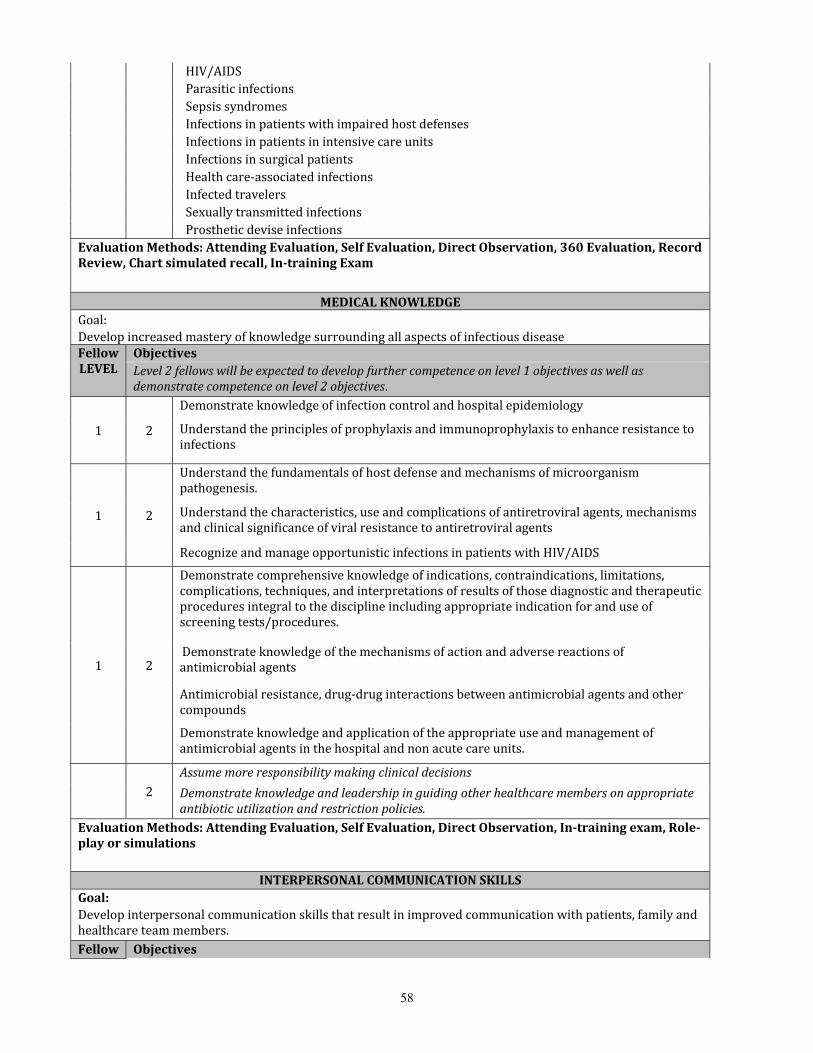
58
HIV/AIDSParasiticinfectionsSepsissyndromesInfectionsinpatientswithimpairedhostdefensesInfectionsinpatientsinintensivecareunitsInfectionsinsurgicalpatientsHealthcare‐associatedinfectionsInfectedtravelersSexuallytransmittedinfectionsProstheticdeviseinfections
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,RecordReview,Chartsimulatedrecall,In‐trainingExam
MEDICALKNOWLEDGEGoal: DevelopincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdiseaseFellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives.
1 2
Demonstrateknowledgeofinfectioncontrolandhospitalepidemiology
Understandtheprinciplesofprophylaxisandimmunoprophylaxistoenhanceresistancetoinfections
1 2
Understandthefundamentalsofhostdefenseandmechanismsofmicroorganismpathogenesis.
Understandthecharacteristics,useandcomplicationsofantiretroviralagents,mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents
RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS
1 2
Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents
Antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds
Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsinthehospitalandnonacutecareunits.
� 2Assumemoreresponsibilitymakingclinicaldecisions
Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,In‐trainingexam,Role‐playorsimulations
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultinimprovedcommunicationwithpatients,familyandhealthcareteammembers.Fellow Objectives

59
LEVEL Level2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developcommunicationskillstofacilitatethelearningofothers
Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes
� Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunication.EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,Patientsurvey
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicprinciplesinthecareofinfectiousdiseasepatients.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstratetheabilitytoberesponsivetopatientsandsociety,supersedingself‐interest
Demonstrateintegrity,honesty,reliability,cooperative,andacceptresponsibility
Demonstrateahighstandardofethicalbehavior,includingabilitytomaintainprofessionalrelationshipswithotherphysiciansandabilitytoavoidconflictsofinterest
Demonstrateacommitmenttolifelonglearning
� Showacommitmenttoprofessionaldevelopment
PartnerwithotherproviderstoimprovepatientcareEvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation
PRACTICEBASEDLEARNINGGoal:Demonstrateunderstandingandabilityforselfreflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1 objectivesaswellasdemonstratecompetenceonlevel2objectives
Developskillstoappraisethecurrentmedicalliteraturetosupportevidencebaseddecision‐making
� Regularlyusemedicalliteraturetosupportdecisionmaking
Regularlyapplynewcontributionstothemanagementandcareofinfectiousdiseasepatients.EvaluationMethods:AttendingEvaluation,SelfEvaluation
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL Objectives

60
Level2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstrateabilitytoworkwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare
Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientqualityofcare.
�
Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
Usesystematicapproachestoreduceerrors EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation

61
InfectiousDiseasesFellowship:KansasCityVeteransAdministrationMedicalCenter(KCVAMC)Inpatient
Consultation
Duration: 1styearFellowsareassignedtotheKCVAMC inpatientconsultservicefor3monthseach2ndyearFellowsareassignedtotheKCVAMC inpatientconsultservicefor1‐2monthseach
Supervision(Interactionwithfaculty)
SupervisionofthefellowbyInfectiousDiseaseattendingatKCVAMCforinpatientservice
RotationFacility KansasCityVeteransAdministrationCenter
RequiredDidactics/conferences:
IDCaseConference,IDJournalClub,IDCoreConference
InfectiousDiseasesFellowship:KCVAMCInpatient
ConsultationRotation
FellowYear1&2
PATIENTCAREGoal:Demonstratecompetenceinthecontinuumofinpatientcareforinfectiousdiseasespatients
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;
DemonstrateabilitytoperformandinterpretGramstains;
Demonstrateabilitytomanagepatienttherapies,emphasizingappropriateuseofantimicrobials;
Workeffectivelywithotherstoprovidepatient‐focusedcare;
DemonstrateabilitytomanagecommonandcomplexIDproblemsinthefaceofantibioticresistance
2 Accuratelyapplyclinicalinformationtoensurepositivepatientoutcomes
Goal:Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Thiswillincludethefollowinginfectiousdiseasesareas:BacterialinfectionsFungalinfectionsViralinfectionsHIV/AIDS

62
ParasiticinfectionsSepsissyndromesInfectionsinpatientswithimpairedhostdefensesInfectionsinpatientsinintensivecareunitsInfectionsinsurgicalpatientsHealthcare‐associatedinfectionsInfectedtravelersSexuallytransmittedinfectionsProstheticdeviseinfections
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,RecordReview,Chartsimulatedrecall,In‐trainingExam
MEDICALKNOWLEDGEGoal: DevelopincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdiseaseFellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives.
1 2
Demonstrateknowledgeofinfectioncontrolandhospitalepidemiology
Understandtheprinciplesofprophylaxisandimmunoprophylaxistoenhanceresistancetoinfections
1 2
Understandthefundamentalsofhostdefenseandmechanismsofmicroorganismpathogenesis.
Understandthecharacteristics,useandcomplicationsofantiretroviralagents,mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents
RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS
1 2
Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents
Antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds
Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsinthehospitalandnonacutecareunits.
2Assumemoreresponsibilitymakingclinicaldecisions
Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,In‐trainingexam,Role‐playorsimulations
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultinimprovedcommunicationwithpatients,familyandhealthcareteammembers.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives

63
Developcommunicationskillstofacilitatethelearningofothers
Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes
Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunication.EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,Patientsurvey
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicprinciplesinthecareofinfectiousdiseasepatients.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstratetheabilitytoberesponsivetopatientsandsociety,supersedingself‐interest
Demonstrateintegrity,honesty,reliability,cooperative,andacceptresponsibility
Demonstrateahighstandardofethicalbehavior,includingabilitytomaintainprofessionalrelationshipswithotherphysiciansandabilitytoavoidconflictsofinterest
Demonstrateacommitmenttolifelonglearning
Showacommitmenttoprofessionaldevelopment
PartnerwithotherproviderstoimprovepatientcareEvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation
PRACTICEBASEDLEARNINGGoal:Demonstrateunderstandingandabilityforselfreflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developskillstoappraisethecurrentmedicalliteraturetosupportevidencebaseddecision‐making
� Regularlyusemedicalliteraturetosupportdecisionmaking
Regularlyapplynewcontributionstothemanagementandcareofinfectiousdiseasepatients.EvaluationMethods:AttendingEvaluation,SelfEvaluation
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives

64
Demonstrateabilitytoworkwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare
Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientqualityofcare.
Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
Usesystematicapproachestoreduceerrors EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation
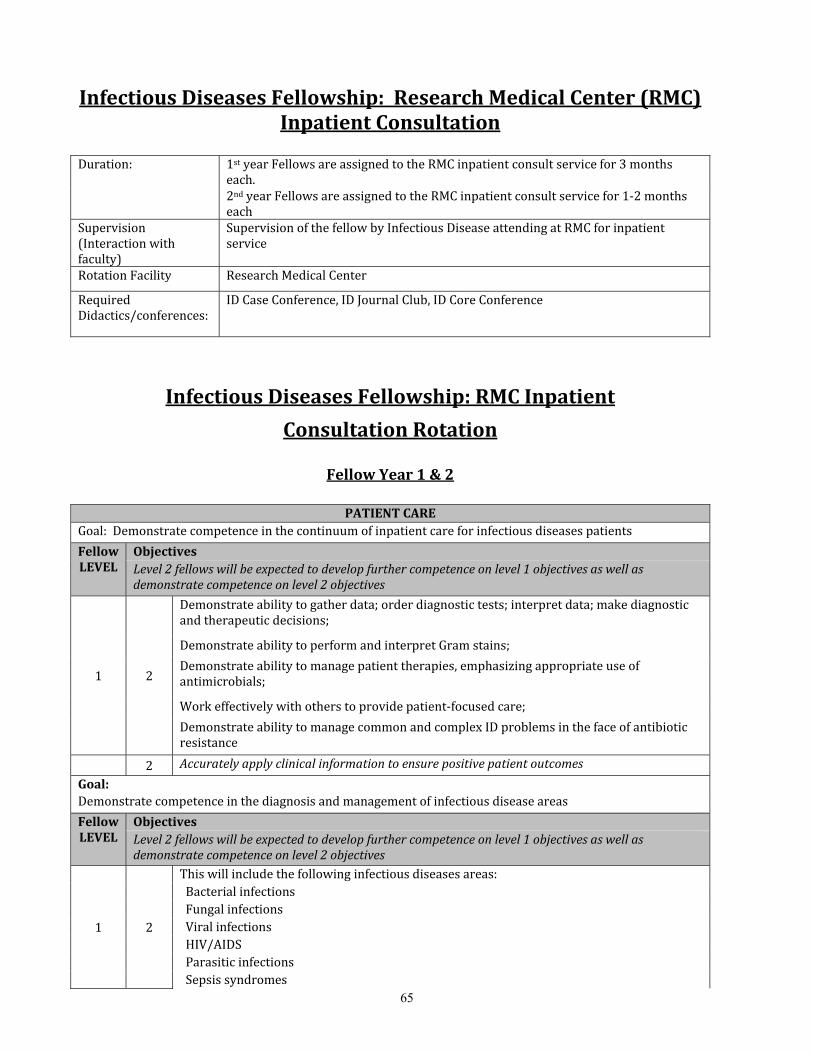
65
InfectiousDiseasesFellowship:ResearchMedicalCenter(RMC)InpatientConsultation
Duration: 1styearFellowsareassignedtotheRMCinpatientconsultservicefor3months
each.2ndyearFellowsareassignedtotheRMC inpatientconsultservicefor1‐2monthseach
Supervision(Interactionwithfaculty)
SupervisionofthefellowbyInfectiousDiseaseattendingatRMCforinpatientservice
RotationFacility ResearchMedicalCenter
RequiredDidactics/conferences:
IDCaseConference,IDJournalClub,IDCoreConference
InfectiousDiseasesFellowship:RMCInpatient
ConsultationRotation
FellowYear1&2
PATIENTCAREGoal:Demonstratecompetenceinthecontinuumofinpatientcareforinfectiousdiseasespatients
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;
DemonstrateabilitytoperformandinterpretGramstains;
Demonstrateabilitytomanagepatienttherapies,emphasizingappropriateuseofantimicrobials;
Workeffectivelywithotherstoprovidepatient‐focusedcare;
DemonstrateabilitytomanagecommonandcomplexIDproblemsinthefaceofantibioticresistance
2 Accuratelyapplyclinicalinformationtoensurepositivepatientoutcomes
Goal:Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Thiswillincludethefollowinginfectiousdiseasesareas:BacterialinfectionsFungalinfectionsViralinfectionsHIV/AIDSParasiticinfectionsSepsissyndromes
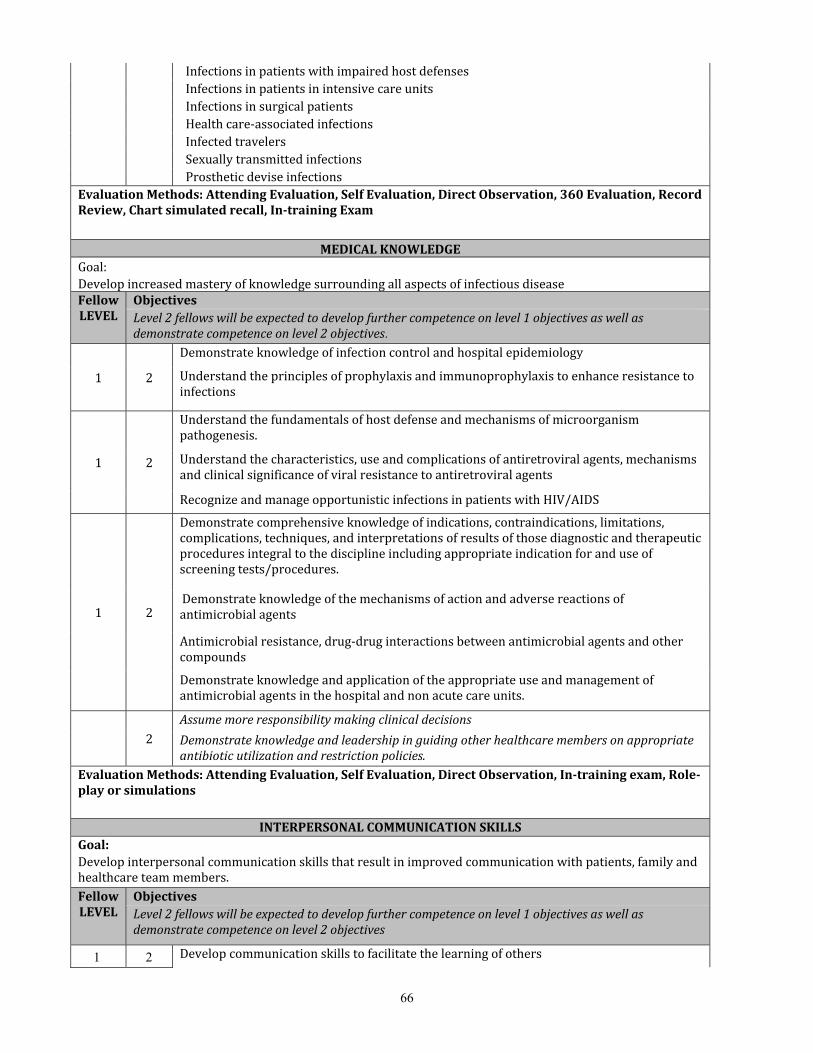
66
InfectionsinpatientswithimpairedhostdefensesInfectionsinpatientsinintensivecareunitsInfectionsinsurgicalpatientsHealthcare‐associatedinfectionsInfectedtravelersSexuallytransmittedinfectionsProstheticdeviseinfections
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,RecordReview,Chartsimulatedrecall,In‐trainingExam
MEDICALKNOWLEDGEGoal: DevelopincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdiseaseFellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives.
1 2
Demonstrateknowledgeofinfection controlandhospitalepidemiology
Understandtheprinciplesofprophylaxisandimmunoprophylaxistoenhanceresistancetoinfections
1 2
Understandthefundamentalsofhostdefenseandmechanismsofmicroorganismpathogenesis.
Understandthecharacteristics,useandcomplicationsofantiretroviralagents,mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents
RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS
1 2
Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents
Antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds
Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsinthehospitalandnonacutecareunits.
2Assumemoreresponsibilitymakingclinicaldecisions
Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,In‐trainingexam,Role‐playorsimulations
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultinimprovedcommunicationwithpatients,familyandhealthcareteammembers.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developcommunicationskillstofacilitatethelearningofothers

67
Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes
Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunication.EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation,Patientsurvey
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicprinciplesinthecareofinfectiousdiseasepatients.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstratetheabilitytoberesponsivetopatientsandsociety,supersedingself‐interest
Demonstrateintegrity,honesty,reliability,cooperative,andacceptresponsibility
Demonstrateahighstandardofethicalbehavior,includingabilitytomaintainprofessionalrelationshipswithotherphysiciansandabilitytoavoidconflictsofinterest
Demonstrateacommitmenttolifelonglearning
Showacommitmenttoprofessionaldevelopment
PartnerwithotherproviderstoimprovepatientcareEvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation,360Evaluation
PRACTICEBASEDLEARNINGGoal:Demonstrateunderstandingandabilityforselfreflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developskillstoappraisethecurrentmedicalliteraturetosupportevidencebaseddecision‐making
Regularlyusemedicalliteraturetosupportdecisionmaking
Regularlyapplynewcontributionstothemanagementandcareofinfectiousdiseasepatients.EvaluationMethods:AttendingEvaluation,SelfEvaluation
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives

68
Demonstrateabilitytoworkwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare
Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientqualityofcare.
Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
Usesystematicapproachestoreduceerrors EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectObservation
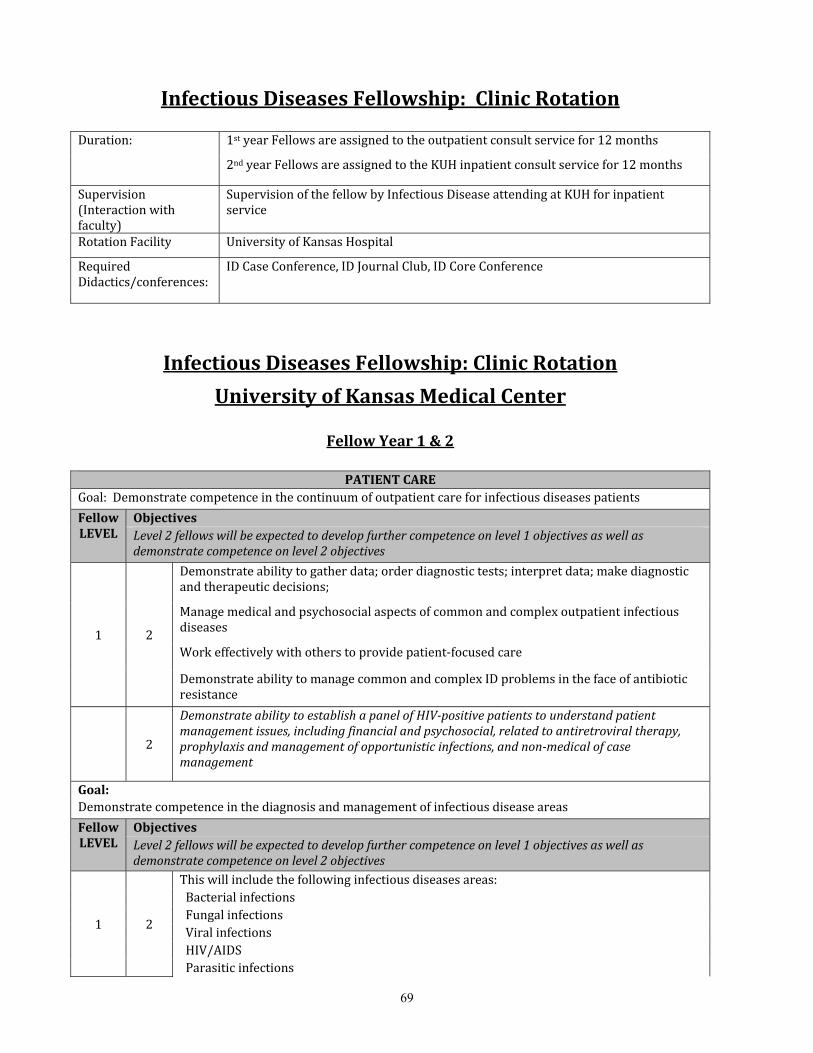
69
InfectiousDiseasesFellowship:ClinicRotation
Duration: 1styearFellowsareassignedtotheoutpatientconsultservicefor12months
2ndyearFellowsareassignedtotheKUHinpatientconsultservicefor12months
Supervision(Interactionwithfaculty)
SupervisionofthefellowbyInfectiousDiseaseattendingatKUHforinpatientservice
RotationFacility UniversityofKansasHospital
RequiredDidactics/conferences:
IDCaseConference,IDJournalClub,IDCoreConference
InfectiousDiseasesFellowship:ClinicRotation
UniversityofKansasMedicalCenter
FellowYear1&2
PATIENTCAREGoal:Demonstratecompetenceinthecontinuumofoutpatientcareforinfectiousdiseasespatients
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;
Managemedicalandpsychosocialaspectsofcommonandcomplexoutpatientinfectiousdiseases
Workeffectivelywithotherstoprovidepatient‐focusedcare
DemonstrateabilitytomanagecommonandcomplexIDproblemsinthefaceofantibioticresistance
2
DemonstrateabilitytoestablishapanelofHIV‐positivepatientstounderstandpatientmanagementissues,includingfinancialandpsychosocial,relatedtoantiretroviraltherapy,prophylaxisandmanagementofopportunisticinfections,andnon‐medicalofcasemanagement
Goal:Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Thiswillincludethefollowinginfectiousdiseasesareas:BacterialinfectionsFungalinfectionsViralinfectionsHIV/AIDSParasiticinfections

70
SepsissyndromesInfectionsinpatientswithimpairedhostdefensesInfectionsinpatientsinintensivecareunitsInfectionsinsurgicalpatientsHealthcare‐associatedinfectionsInfectedtravelersSexuallytransmittedinfectionsProstheticdeviseinfections
TeachingMethods:DirectPatientCare,IDCoreCurriculum,IDCaseConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation,360Evaluation
MEDICALKNOWLEDGEGoal: DevelopincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdiseaseFellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives.
1 2
Developskillintheuseofantibioticsandprophylacticagents
Understandtheprinciplesof prophylaxisandimmunoprophylaxistoenhanceresistancetoinfections
1 2
Understandthefundamentalsofhostdefenseandmechanismsofmicroorganismpathogenesis.
Understandthecharacteristics,useandcomplicationsofantiretroviralagents,mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents
RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS
1 2
Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents
Antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds
Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsintheoutpatientsetting.
2Understandmanagementissuesassociatedwithoutpatientadministrationfantibiotics
Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
TeachingMethods:DirectPatientCare,IDCoreCurriculum,IDCaseConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation,360Evaluation
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultin improvedcommunicationwithpatients,familyandhealthcareteammembers.

71
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developcommunicationskillstofacilitatethelearningofothers
Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes
Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunication.TeachingMethods:DirectPatientCare,IDCoreCurriculum,IDCaseConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation,360Evaluation
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicprinciplesinthecareofinfectiousdiseasepatients.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstratetheabilitytoberesponsivetopatientsandsociety,supersedingself‐interest
Beresponsivetoneedsofpatientsandsocietysupersedingself‐interest
Demonstraterespect,compassionandintegrity;behonest,reliable,cooperativeandacceptresponsibility
Demonstrateacommitmenttolifelonglearning
Showacommitmenttoprofessionaldevelopment
Partnerwithotherproviderstoimprovepatient careEvaluationMethods:AttendingEvaluation,SelfEvaluation,360Evaluation
PRACTICEBASEDLEARNINGGoal:Demonstrateunderstandingandabilityforself‐reflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developskillstoappraisethecurrentmedicalliteraturetosupportevidencebaseddecision‐making
Regularlyusemedicalliteraturetosupportdecisionmaking
Regularlyapplynewcontributionstothemanagementandcareofinfectiousdiseasepatientsinoutpatientsettings
Continuetodevelopandimproveconsultativeskillsintheoutpatientsetting.
TeachingMethods:DirectPatientCare,IDCoreCurriculum,IDCaseConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation

72
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstrateabilitytoworkwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare
Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientqualityofcare
Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
Usesystematicapproachestoreduceerrors TeachingMethods:DirectPatientCare,IDCoreCurriculum,IDCaseConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation,360Evaluation

73
InfectiousDiseasesFellowship:KansasCityVeteransAdministrationMedicalCenter(KCVAMC)ClinicRotation
Duration: 1styearFellowsareassignedtotheKCVAMCoutpatientclinicsfortwo1/2daysper
weekduringrotation
2ndyearFellowsareassignedtotheKCVAMCoutpatientclinicsfortwo1/2daysperweekduringrotation
Supervision(Interactionwithfaculty)
SupervisionofthefellowbyInfectiousDiseaseattendingatKCVAMCforinpatientservice
RotationFacility KansasCityVeteransAdministrationMedicalCenter
RequiredDidactics/conferences:
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
InfectiousDiseasesFellowship:ClinicRotation
KansasCityVeteransAdministrationMedicalCenter(KCVAMC)
FellowYear1&2
PATIENTCAREGoal:Demonstratecompetenceinthecontinuumofoutpatientcareforinfectiousdiseasespatients
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstrateabilitytogatherdata;orderdiagnostictests;interpretdata;makediagnosticandtherapeuticdecisions;
Managemedicalandpsychosocialaspectsofcommonandcomplexoutpatientinfectiousdiseases
Workeffectivelywithotherstoprovidepatient‐focusedcare
DemonstrateabilitytomanagecommonandcomplexIDproblemsinthefaceofantibioticresistance
2
DemonstrateabilitymanageHIV‐positivepatientstounderstandpatientmanagementissues,includingfinancialandpsychosocial,relatedtoantiretroviraltherapy,prophylaxisandmanagementofopportunisticinfections,andnon‐medicalcasemanagement
Goal:Demonstratecompetenceinthediagnosisandmanagementofinfectiousdiseaseareas
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2Thiswillincludethefollowinginfectiousdiseasesareas:Bacterialinfections

74
FungalinfectionsViralinfectionsHIV/AIDSParasiticinfectionsSepsissyndromesInfectionsinpatientswithimpairedhostdefensesInfectionsinpatientsinintensivecareunitsInfectionsinsurgicalpatientsHealthcare‐associatedinfectionsInfectedtravelersSexuallytransmittedinfectionsProstheticdeviseinfections
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
EvaluationMethods:AttendingEvaluation,SelfEvaluation
MEDICALKNOWLEDGEGoal: DevelopincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdiseaseFellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives.
1 2
Developskillintheuseofantibioticsandprophylacticagents
Understandtheprinciplesofprophylaxisandimmunoprophylaxistoenhanceresistancetoinfections
1 2
Understandthefundamentalsofhostdefenseandmechanismsofmicroorganismpathogenesis.Understandthecharacteristics,useandcomplicationsofantiretroviralagents,mechanismsandclinicalsignificanceofviralresistancetoantiretroviralagents
RecognizeandmanageopportunisticinfectionsinpatientswithHIV/AIDS
1 2
Demonstratecomprehensiveknowledgeofindications,contraindications,limitations,complications,techniques,andinterpretationsofresultsofthosediagnosticandtherapeuticproceduresintegraltothedisciplineincludingappropriateindicationforanduseofscreeningtests/procedures.
Demonstrateknowledgeofthemechanismsofactionandadversereactionsofantimicrobialagents
Antimicrobialresistance,drug‐druginteractionsbetweenantimicrobialagentsandothercompounds
Demonstrateknowledgeandapplicationoftheappropriateuseandmanagementofantimicrobialagentsintheoutpatientsetting.
2
Understandmanagementissuesassociatedwithoutpatientadministrationfantibiotics
Demonstrateknowledgeandleadershipinguidingotherhealthcaremembersonappropriateantibioticutilizationandrestrictionpolicies.
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect

75
EvaluationMethods:AttendingEvaluation,Self Evaluation
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultinimprovedcommunicationwithpatients,familyandhealthcareteammembers.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developcommunicationskillstofacilitatethelearningofothers
Useeffectivelistening,narrative,andnon‐verbalskills;writelegibleandcomprehensivenotes
Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunication.
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
EvaluationMethods:AttendingEvaluation,SelfEvaluation
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicprinciplesinthecareofinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstratetheabilitytoberesponsivetopatientsandsociety,supersedingself‐interest
Demonstraterespect,compassionandintegrity;behonest,reliable,cooperativeandacceptresponsibility
Demonstrateacommitmenttolifelonglearning
Showacommitmenttoprofessionaldevelopment
Partnerwithotherproviderstoimprovepatientcare
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
EvaluationMethods:AttendingEvaluation,SelfEvaluation
PRACTICEBASEDLEARNINGGoal:Demonstrateunderstandingandabilityforself‐reflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Developskillstoappraisethecurrentmedicalliteraturetosupportevidencebaseddecision‐

76
making
Regularlyusemedicalliteraturetosupportdecisionmaking
Regularlyapplynewcontributionstothemanagementandcareofinfectiousdiseasepatientsinoutpatientsettings
Continuetodevelopandimproveconsultativeskillsintheoutpatientsetting.
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
EvaluationMethods:AttendingEvaluation,SelfEvaluation
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
Demonstrateabilitytoworkwithhealthcareprofessionalstoprovidepatientfocusedcare;advocateforqualitypatientcare
Workininter‐professionalteamstoenhancepatientsafetyandimprovepatientqualityofcare
Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
Usesystematicapproachestoreduceerrors
TeachingMethods:DirectPatientCareandIDCoreCurriculum,IDCaseConferencebyAdobeconnect
EvaluationMethods:AttendingEvaluation,SelfEvaluation

77
InfectiousDiseasesFellowship:MicrobiologyRotation Duration: PGY4Fellowsareassignedtothemicrobiologylab30minutesfor2daysaweekfor6
months
PGY5fellowsareassignedtothemicrobiologylab30minutesfor2daysaweekfor9months
Supervision(Interactionwithfaculty):
SupervisionofthefellowbyfacultyMicrobiologists
RotationFacility: UniversityofKansasMedicalCenter
InfectiousDiseaseFellowship:MicrobiologyRotation
UniversityofKansas
Fellowyear1&2
PATIENTCAREGoal:Demonstratecompetenceaspectsofmicrobiologyasitappliestoinfectiousdiseases.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2Becomefamiliarwiththetechnicalaspectsofpathogenisolation,sensitivitytesting,andmolecularmethodsanddevelopknowledgeofhowtheyareappliedtothecontinuumofpatientcare
2
Begintoinstructtheyearonefellowsandaskclinicalquestionsofthemwhileviewingthepathogenwiththemicrobiologists
TeachingMethods:DirectPatientCare
EvaluationMethods:SelfEvaluation,360Evaluation
MEDICALKNOWLEDGEGoal:Developincreasedmasteryofknowledgesurroundingallaspectsofinfectiousdisease.FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2Becomefamiliarwiththetechnicalaspectsofpathogenisolation,sensitivitytesting,andmolecularmethods.
2Begintoinstructtheyearonefellowsandaskclinicalquestionsofthemwhileviewingthepathogenwiththemicrobiologists
TeachingMethods:DirectPatientCare,IDCaseConference,IDCoreConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation
INTERPERSONALCOMMUNICATIONSKILLSGoal:Developinterpersonalcommunicationskillsthatresultinimprovedcommunicationwithpatients,familyandhealthcareteammembers.Fellow Objectives

78
LEVEL Level2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Developcommunicationskillstofacilitatethelearningofothers
Communicateclearlywiththemicrobiologystaffandclinicalservice
Workwithmicrobiologystaffandclinicalservicestoprovideamultidisciplinaryapproachtothediagnosisandtreatmentofinfections
2
Effectivelydiscussendoflifecarewithpatientsandtheirfamilies
DisplayinitiativeandleadershipininitiatingandmaintainingeffectivecommunicationTeachingMethods:DirectPatientCare
EvaluationMethods:AttendingEvaluation,360Evaluation
PROFESSIONALISMGoal:Demonstrateabilityandcommitmenttocarryingoutprofessionalresponsibilitiesandadherencetoethicalprinciplesinthecareofinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpected todevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2 Demonstraterespect,compassion,andintegrity;behonest,reliable,cooperativeandacceptresponsibility
2Showacommitmenttoprofessionaldevelopment
Partnerwithotherproviderstoimprovepatientcare
TeachingMethods:DirectPatientCare
EvaluationMethods:AttendingEvaluation,360Evaluation
PRACTICEBASEDLEARNINGGoal:
Demonstrateunderstandingandabilityforself‐reflectionandlife‐longlearningthroughtheabilitytoinvestigateandevaluatepersonalcareofpatientsandappraiseandassimilatescientificevidencetocontinuallyimprovepatientcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2 Appraisethemedicalliteraturetosupportdecisionmaking. 2 Regularlyusemedicalliteraturetosupportdecisionmaking
TeachingMethods:IDCaseConference,IDCoreConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation
SYSTEMSBASEDPRACTICEGoal:Demonstrateunderstandingandresponsivenesstothelargercontextandsystemofhealthcareandabilitytoutilizeresourcesinthesystemtoestablishandmaintainoptimalhealthcareforinfectiousdiseasepatients.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives

79
1 2Workwiththemicrobiologystaffandclinicalserviceteamstoenhancepatientsafetyandimprovepatientqualityofcare.
2Advocateforqualitypatientcareincorporatingconsiderationofcostandrisk‐benefitanalysisasappropriateforequitablecareforallinfectiousdiseasepatients
UsesystematicapproachestoreduceerrorsTeachingMethods:DirectPatientCare
EvaluationMethods:AttendingEvaluation,360Evaluation

80
InfectiousDiseaseFellowshipResearchRotation Duration: PGY4Fellowsmaybeassignedtotheresearchrotationfor2weeks
PGY5fellowsareassignedtotheresearchrotationforupto3months
Supervision(Interactionwithfaculty):
SupervisionofthefellowbyInfectiousDiseasefacultymentor
RotationFacility: UniversityofKansasMedicalCenterRequiredDidactics/conferences: KUResearchConference;Regularlyscheduledmeetingwithresearchmentor
InfectiousDiseaseFellowshipResearchRotation
UniversityofKansas
Fellowyear1&2INTERPERSONALCOMMUNICATIONSKILLS
Goal:Developcompetenceinpresentationofresearchstudyfindings,includingpresentationsatnationalmeetingsaswellaspreparingamanuscriptforpublication..FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Developcommunicationskillstofacilitatethelearningofothers
Demonstratecompetenceinsummarizingdatainabstractsforpresentationatregionalandnationalmeetings
Demonstratecompetenceinposterororalpresentationpreparationforanationalmeeting
2
Demonstratecompetenceinmanuscriptpublicationinapeer‐reviewedjournal,includingpreparationoffiguresLearntoacceptandutilizecriticalevaluationofone’swork
Displayinitiativeandleadershipininitiatingandmaintainingeffectivecommunicationregardingresearchideasandformaldisseminationandpresentationofresearchfindings
TeachingMethods:FacultyMentoring
EvaluationMethods:AttendingEvaluation,SelfEvaluation
PROFESSIONALISMGoal:Become familiar with research regulations and ethics. FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
LearnabouttheIRBapprovalprocessandwhatapprovalsarenecessaryforspecificprojecttypes
Demonstratecompetencyinprivacyregulationsregardinguseofpatientdata
SuccessfullygainIRBapprovalforallprojectsinvolvinghumansubjects

81
SuccessfullygainIACUCapprovalforallprojectsinvolvinganimals
Understandtheissuessurroundingappropriatetreatmentofresearchsubjects
2Showacommitmenttoprofessionaldevelopment
Prepareresearchforpublicationand/orpresentationatanationalmeetingorconference
TeachingMethods:IDCaseConference,IDResearchConference
EvaluationMethods:AttendingEvaluation,SelfEvaluation,DirectedProject
PRACTICEBASEDLEARNINGGoal:Understand how to design a research project, including formulating a hypothesis and designing an experimental strategy to evaluate it.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
1 2
Demonstratecompetenceinevaluatingrelevantliteraturerelatedtoaspecificresearchquestion,includingtypeofresearchmodelandevaluationoftheappropriateuseofstatistics
Demonstratecompetenceinformulatingatestablehypothesis
Demonstratefamiliarizationwithappropriatestatisticalmethodstobeusedfordataanalysis
Learntorecognizeandmakecontingencyplansforpotentialproblemsinaresearchplan
Demonstratetheabilitytounderstandhowclinicalandbasicscienceresearchresultsinfluenceclinicalpractice
Goal:
Learn to execute a clinical and/or a basic science research project, including mastering the appropriate technical skills required for completion of the project.
FellowLEVEL
ObjectivesLevel2fellowswillbeexpectedtodevelopfurthercompetenceonlevel1objectivesaswellasdemonstratecompetenceonlevel2objectives
2
Demonstratecompetenceintheappropriatemethodsforexecutionofabasicscienceproject,includingtissueprocessing,physiologicalrecording,etc.
Demonstratecompetenceintroubleshootingtechnicalproblemsandevaluatingtheirimpactonprojects
Demonstratecompetenceindatacollectionandorganizationforsubsequentevaluation
Demonstrateunderstandingofstatisticalanalysisofdatacollected
Learntoevaluateresultsforagivenprojectinthecontextofotherworkintheresearcharea
Competenceinproposingfutureexperimentstoaugmentresultsfromagivenproject
TeachingMethods:FacultyMentoring,IDCoreCurriculum
EvaluationMethods:AttendingEvaluation

82
CORECOMPETENCYTEACHINGANDASSESSMENTMATRIXTEMPLATECoreCompetency TEACHINGMETHODS EVALUATIONMETHODS
Didactic Lecture
Group Discussion
Online Tool
Project
Role M
odeling
Simulations
Clinical Patient
Experience
Vanderbilt m
atrix
OTH
ER
Record Review
Chart Stim
ulated Recall
Global Rating
Assessm
ents (E*value)
Obj Structured Clinical
Exam
Simulations & M
odels
360° Assessm
ents
Written Examination
On‐Line Training
Vanderbilt M
atrix
Patient Survey
PRACTICE‐BASEDLEARNING&IMPROVEMENT PRACTICE‐BASEDLEARNING&IMPROVEMENTAnalyzeownpracticeforneededimprovements
X X X X X X X X X
Useofevidencefromscientificstudies X X X X X X X X X
Applicationofresearch&statisticalmethods
X X X X X
Useofinformationtechnology X X X X X
Facilitatelearningofothers X X X X X X X X X
INTERPERSONAL&COMMUNICATIONSKILLS INTERPERSONAL&COMMUNICATIONSKILLSCreationoftherapeuticrelationshipwithpatients
X X X X X X X X
Listeningskills X X X X X X X X
PROFESSIONALISM PROFESSIONALISM
Respectful,altruistic X X X X X X X X X X X
Ethicallysoundpractice X X X X X X X X X X
Sensitivetocultural,age,gender,disabilityissues
X X X X X X X X X X
SYSTEMS‐BASEDPRACTICE SYSTEMS‐BASEDPRACTICE
Understandinteractionoftheirpracticeswiththelargersystem
X X X X X X X X X X
Knowledgeofpracticeanddeliverysystems X X X X X X X X X X X X
Practicecost‐effectivecare X X X X X X X X X X
Advocateforpatientswithinthehealthsystem
X X X X X X X X X

83
RequiredEvaluationsforIDFellows&IDProgramEvaluations,required,andine‐value Format
1.Facultyoffellow/endrotation Electronic
2.Fellowoffaculty Electronic
3.Fellowofprogram Electronic
4.Facultyofprogram Electronic
5.FellowSemi‐annualevaluation Paper(Scannedin)
6.360ofresident(patient,RN,LPN) Electronic
7.Peerevaluation(chieffellow) Electronic
8.Selfevaluation Electronic
9.FellowFinalsummative Paper(Scannedin)
10.Programdirectoroffaculty Electronic
11.Annualprogramreview Electronic
12.Alumnisurvey Paper

84
FACULTY EVALUATION OF PROGRAM
Fellows model professional behavior in their interactions with patients and co-workers. (Question 1 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
There is an appropriate volume and variety of patients available to the program for educational purposes. (Question 2 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellows have adequate opportunities for clinical research. (Question 3 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellows are adequately supervised during patient care activities. (Question 4 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellowship program staff is responsive and helpful. (Question 5 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The program leadership is responsive to faculty questions and concerns. (Question 6 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The program communicates well with the faculty regarding educational goals and requirements. (Question 7 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellows are compliant with work hour limitations (avg. 80 hrs/wk, max 24 hr. continuous duty, avg. at least one day off per week). (Question 8 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellows completing the program are well-prepared for Infectious Diseases practice. (Question 9 of 21 - Mandatory)
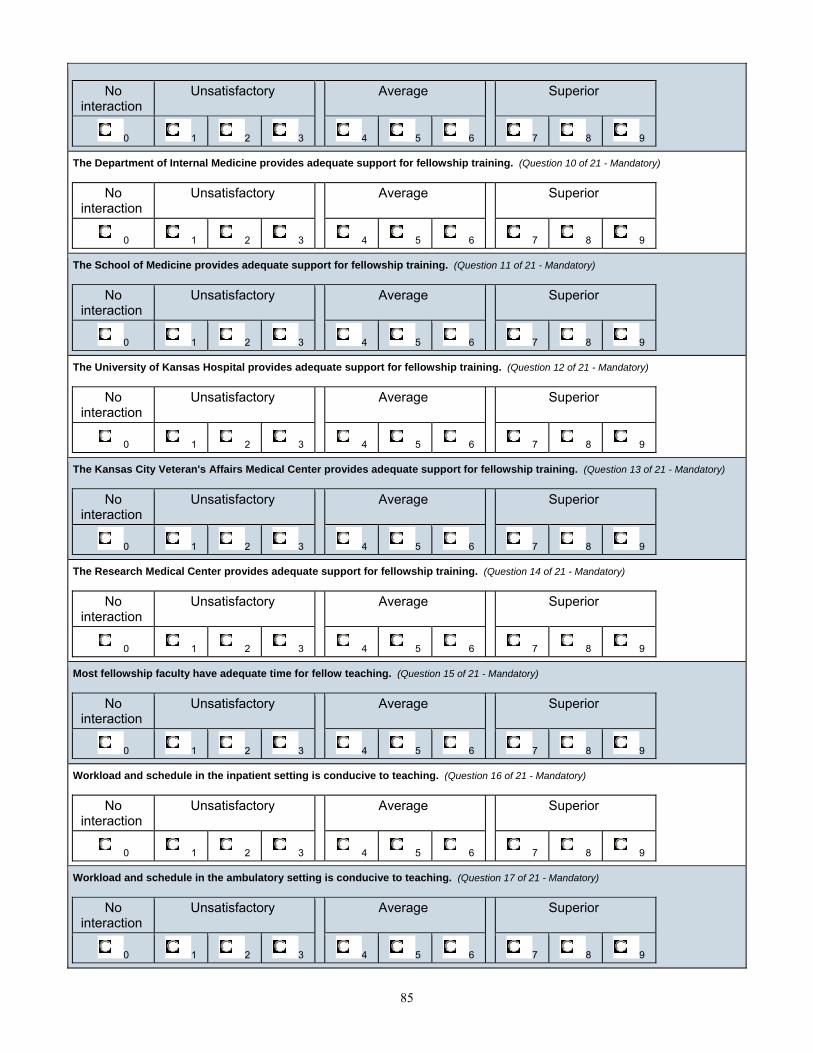
85
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The Department of Internal Medicine provides adequate support for fellowship training. (Question 10 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The School of Medicine provides adequate support for fellowship training. (Question 11 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The University of Kansas Hospital provides adequate support for fellowship training. (Question 12 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The Kansas City Veteran's Affairs Medical Center provides adequate support for fellowship training. (Question 13 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The Research Medical Center provides adequate support for fellowship training. (Question 14 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Most fellowship faculty have adequate time for fellow teaching. (Question 15 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Workload and schedule in the inpatient setting is conducive to teaching. (Question 16 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Workload and schedule in the ambulatory setting is conducive to teaching. (Question 17 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9

86
Fellows are well-prepared for rounds on their patients. (Question 18 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Faculty does a good job of providing feedback about fellow performance. (Question 19 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellows read appropriately and are prepared to discuss differential diagnosis and pathophysiology on their patients. (Question 20 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 21 of 21 - Mandatory) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

87
FACULTY OF FELLOW EVALUATION
Demonstrates understanding of clinical problems: (PC) (Question 1 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates appropriate physical exam skills: (PC) (Question 2 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates appropriate test selection: (PC) (Question 3 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Advocates for patients: (PC) (Question 4 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Reads specific knowledge: (MK) (Question 5 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Develops appropriate differential diagnoses: (MK) (Question 6 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Has appropriate knowledge base for level of training: (MK) (Question 7 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Note content is appropriate: (ICS) (Question 8 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Interpersonal skills with staff and patients are appropriate: (ICS) (Question 9 of 21 - Mandatory)
No Unsatisfactory Average Superior

88
interaction
0 1 2 3 4 5 6 7 8 9
Presents cases in clear, concise manner: (ICS) (Question 10 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Displays professional attitude: (P) (Question 11 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Completes work in a timely fashion and attends round on time: (P) (Question 12 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Responsible for their workload: (P) (Question 13 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Effectively utilizes hospital resources: (SBP) (Question 14 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Communicates effectively with consultants: (SBP) (Question 15 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Understands health care delivery appropriate for level of training: (SBP) (Question 16 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Advocates for quality patient care and assists patients in dealing with systems complexities: (SBP) (Question 17 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Identifies areas for improvement and applies it to practice: (PBLI) (Question 18 of 21 - Mandatory)
89
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Shows interest in learning from complex care issues: (PBLI) (Question 19 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Participates in educational activities including rounds and conferences: (PBLI) (Question 20 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 21 of 21) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.
c

90
FELLOW OF FACULTY EVALUATION
Placed the patient’s interest first: (P) (Question 1 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Displayed sensitive, caring, respectful attitude towards patients: (P) (Question 2 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Established rapport with team members: (P) (Question 3 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Established respect for physicians in other specialties/subspecialties and health care professionals: (P) (Question 4 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Served as a role model: (P) (Question 5 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Was enthusiastic and stimulating: (P) (Question 6 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrated gender sensitivity: (P) (Question 7 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Is usually prompt: (Question 8 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Respected the value of my time: (Question 9 of 24 - Mandatory)
No Unsatisfactory Average Superior

91
interaction
0 1 2 3 4 5 6 7 8 9
Kept interruptions to a minimum: (Question 10 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Spent enough time on rounds; was unhurried: (Question 11 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Kept discussions focused on case or topic: (Question 12 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Used bedside teaching to demonstrate history and physical skills: (Question 13 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Emphasized problem solving (thought processes leading to decisions): (Question 14 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Provided feedback regarding performance on rotations or evaluation period: (Question 15 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Showed an interest in teaching: (Question 16 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Discussed pathophysiological mechanism of the disease encountered: (Question 17 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrated cost effective use of laboratory and therapeutic modalities: (Question 18 of 24 - Mandatory)
92
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Provided instruction and adequate assistance in helping manage patients in the outpatient clinics: (Question 19 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Suggested references for further reading/studying: (Question 20 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Stimulated team members to read and review pertinent data: (Question 21 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Provided special help as needed: (Question 22 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Attending provides appropriate supervision during procedures: (Question 23 of 24 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 24 of 24) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

93
FELLOW OF PROGRAM EVALUATION
The diversity of diseases in this program gave me a broad experience in infectious diseases: (PC) (Question 1 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The ambulatory experience has allowed me to develop appropriate outpatient skills: (PC) (Question 2 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I understood what I should learn from each rotation: (MK) (Question 3 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I became more comfortable in selecting cases that provide good teaching concepts (Clinical Case Conference): (ICS) (Question 4 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Program leadership serves as my advocate: (ICS) (Question 5 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I had opportunity to work on or present an oral or written presentation: (ICS) (Question 6 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I was able to work with one or more HIV care coordinators: (ICS) (Question 7 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Faculty teach and supervise in ways that facilitate learning: (P) (Question 8 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The case conference was an appropriate learning experience: (P) (Question 9 of 15 - Mandatory)
No Unsatisfactory Average Superior

94
interaction
0 1 2 3 4 5 6 7 8 9
The information technologies (computers) available to me allowed me to obtain current medical information and scientific evidence: (SBP) (Question 10 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
These sessions helped me to read gram stains and understand them (Clinical Micro Conference): (SBP) (Question 11 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I was given sufficient responsibility for decision-making and patient care:(PBLI) (Question 12 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I was able to work on one or more research projects: (Question 13 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
My overall level of satisfaction with this fellowship program is such that I would recommend it to junior residents. (Question 14 of 15 -Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
95
Comments: (Question 15 of 15) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

96
FELLOW PEER EVALUATION
PATIENT CARE: Fellows must be able to provide patient care that is compassionate, appropriate and effective for the treatment of health problems and the promotion of health. (Question 1 of 15 - Mandatory) I am comfortable picking up cases this fellow has managed.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
I am comfortable having this fellow cover my patients. (Question 2 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
MEDICAL KNOWLEDGE: Fellows are expected to demonstrate knowledge of established and evolving biomedical, clinical and basic science principles and to apply them to the tasks at hand. (Question 3 of 15 - Mandatory) Fellow demonstrates an active pursuit of knowledge.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow is able to synthesize data effectively in formulating management plans. (Question 4 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
INTERPERSONAL AND COMMUNICATION SKILLS: Fellows are expected to be able to demonstrate interpersonal and communication skills that result in effective information exchange and teaming with co-workers, peers and professional associates. (Question 5 of 15 - Mandatory) Fellow objectively listens to information provided by other members of the health care team.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow records complete and accurate information in a manner that makes it easier for members of the health care team to care for the patients. (Question 6 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
PROFESSIONALISM: Fellows are expected to demonstrate a commitment to carrying out professional responsibilities, adherence to ethical principles and professional behavior. (Question 7 of 15 - Mandatory) Fellow demonstrates honesty and integrity.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9

97
Fellow respects other members of the health care system. (Question 8 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow is accountable for own actions. (Question 9 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
SYSTEMS BASED PRACTICE: Fellows must demonstrate an awareness of and responsiveness to the larger context and system of health care, as well as the ability to call effectively on other resources in the system to provide optimal health care. (Question 10 of 15 - Mandatory) I would want this fellow to join me in my practice after I graduate.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow effectively accesses and evaluates patients when receiving or referring a consult. (Question 11 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
PRACTICE BASED LEARNING AND IMPROVEMENT: Fellows are expected to be able to use scientific evidence and methods to investigate, evaluate and improve research practices. (Question 12 of 15 - Mandatory) This fellow identifies and analyzes own strengths and weaknesses.
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow satisfactorily conveys their knowledge to residents, students and other health care professionals. (Question 13 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
OVERALL RATING: Based on the above ratings of each component skill, please provide an overall rating of and comments about the fellow's clinical performance. (Question 14 of 15 - Mandatory) Overall rating:
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Overall comments: (Question 15 of 15 - Mandatory)

98
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

99
FELLOW SELF ASSESSMENT EVALUATION
OVERVIEW: The Fellow Self Evaluation is part of the Division of Infectious Diseases Multi Source Assessment, which will be useful in assessing the Fellowship Training Program. This evaluation will be done semi-annually. The goal of this form is to provide information from which the fellow and faculty, working together, can create goals and action plans.
Assess your delivery of patient care and whether or not it is compassionate, appropriate and effective for the treatment of health programs and the promotion of health. (PC) (Question 1 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 2 of 15 - Mandatory)
Assess your medical knowledge about established and evolving biomedical, clinical and cognitive sciences and how it has been applied to patient care? (MK) (Question 3 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 4 of 15 - Mandatory)
Assess your communication and interpersonal skills as manifested in your effective exchange of information and collaboration with patients, their families and other health professionals. (ICS) (Question 5 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 6 of 15 - Mandatory)

100
Assess your professionalism as manifested through your commitment to carrying out professional responsibilities, adherence to ethical principles and sensitivity to patients of diverse backgrounds. (P) (Question 7 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 8 of 15 - Mandatory)
How do you assess your system based practice as manifested by actions that demonstrate an awareness of and responsiveness to the large context and system of health care, as well as the ability to call effectively on other resources in the system to provide optimal health care? (SBP) (Question 9 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 10 of 15 - Mandatory)
Assess your practice based learning and improvement which involves the investigation and evaluation of care for patients, the appraisal and assimilation of scientific evidence and improvements in patient care. (PBLI) (Question 11 of 15 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
In what ways do you believe you can improve? (Question 12 of 15 - Mandatory)

101
After having completed this self-assessment, what would you identify as your strengths? Please list three. (Question 13 of 15 - Mandatory)
What would you identify as your areas for improvement? Please list three. (Question 14 of 15 - Mandatory)
Please list three specific learning objectives and goals to work on over the next six months. (Question 15 of 15 - Mandatory)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

102
NURSE EVALUATION OF FELLOW
The fellow provided excellent patient care consistent with his or her level of training: (PC) (Question 1 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow shared appropriate understanding and gave good responses when asked questions about the patient's disease states: (MK) (Question 2 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow was available to nursing staff within a reasonable time when assistance was needed: (ICS) (Question 3 of 10 -Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow communicated effectively and respectfully with the patient and their family: (ICS) (Question 4 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow communicated effectively and respectfully with nursing staff: (ICS) (Question 5 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow demonstrated respect and compassion for the patient and their family: (P) (Question 6 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow demonstrated respect for the role and opinions of nursing staff: (P) (Question 7 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow demonstrated respect for the roles and opinions of all team members: (P) (Question 8 of 10 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow participated effectively as a member of the multi-disciplinary team: (SBP) (Question 9 of 10 - Mandatory)

103
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 10 of 10) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.
104
PATIENT EVALUATION OF FELLOWS
Greeting you warmly: being friendly, never rude: (P) (Question 1 of 6 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Letting you tell your story and asking thoughtful questions: (ICS) (Question 2 of 6 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Letting you know, during the physical exam about what he/she is going to do; tell you what is found: (ICS) (Question 3 of 6 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Addressing your questions: (ICS) (Question 4 of 6 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Using words you can understand: (ICS) (Question 5 of 6 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 6 of 6) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

105
RESEARCH FACULTY OF FELLOW
Develops relevant research questions and objectives: (RP) (Question 1 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates appropriate understanding of research design implementation: (RP) (Question 2 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates appropriate understanding of data management and analysis: (RP) (Question 3 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates good understanding of Good Clinical Practice Guidelines including research subject rights and protection: (RP) (Question 4 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Reads specific ID literature relevant to research project: (MK) (Question 5 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Demonstrates understanding of research design: (MK) (Question 6 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Has appropriate understanding of research infrastructure for level of training: (MK) (Question 7 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Written research proposals are appropriate: (ICS) (Question 8 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Interpersonal skills with staff and patients are appropriate: (ICS) (Question 9 of 21 - Mandatory)
No Unsatisfactory Average Superior

106
interaction
0 1 2 3 4 5 6 7 8 9
Presents research ideas in a clear, concise manner: (ICS) (Question 10 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Displays a professional attitude: (P) (Question 11 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Completes work in a timely fashion and attends conferences on time: (P) (Question 12 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Responsible for their workload: (P) (Question 13 of 21 - Mandatory)
Not Applicable Strongly Disagree
Disagree Neutral Agree Strongly Agree
0 1 2 3 4 5
Effectively utilizes research resources: (SBP) (Question 14 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Communicates effectively with research team and consultants: (SBP) (Question 15 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Understands research system appropriate for level of training: (SBP) (Question 16 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Advocates for rights and protection of research subjects: (SBP) (Question 17 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Identifies areas for improvement and applies it to practice: (PBLI) (Question 18 of 21 - Mandatory)

107
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Shows interest in learning from complex care issues: (PBLI) (Question 19 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Participates in educational activities including rounds and conferences: (PBLI) (Question 20 of 21 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 21 of 21) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

108
Support Staff of Fellow Evaluation
The fellow is available within a reasonable time when assistance is needed (P) (Question 1 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow communicates effectively with Staff (P) (Question 2 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow completes GME paperwork in a timely manner (P) (Question 3 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Fellow is approachable (P) (Question 4 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow demonstrates accountability (P) (Question 5 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
The fellow takes responsibility for their education (P) (Question 6 of 7 - Mandatory)
No interaction
Unsatisfactory
Average
Superior
0 1 2 3 4 5 6 7 8 9
Comments: (Question 7 of 7) (Please write about Strengths, Weaknesses and Areas of Improvement)
Review your answers in this evaluation. If you are satisfied with the evaluation, click the SUBMIT button below. Once submitted, evaluations are no longer available for you to make further changes.

109
RECOMMENDEDREFERENCES
1. Mandel,Douglas,andBennett‐PrinciplesandPracticeofInfectiousDiseases,6thed.,Churchill‐Livingston,NewYork(CurrentEdition)
2. SanfordGuidetoAntimicrobialTherapy‐CurrentEdition3. Murray,Baron,Pfaller,et.al.,ManualofClinicalMicrobiology,CurrentEdition,,ASM
Press,Washington,DC4. JournalofInfectiousDiseases5. ClinicalInfectiousDiseases6. InfectiousDiseaseinClinicalPractice7. AntimicrobialAgentsandChemotherapy8. JournalofClinicalMicrobiology9. ClinicalMicrobiologyReviews10. Science11. Nature12. LancetInfectiousDiseases13. NewEnglandJournalofMedicine14. AmericanJournalofMedicine15. JournaloftheAmericanMedicalAssociation16. AnnalsofInternalMedicine,andACPJournalClub17. ArchivesofInternalMedicine18. MMWR19. MedicalLetter20. CherryandFeigen,PediatricInfectiousDiseases,currentedition21. Up‐to‐date‐online
Fulltextsareavailableon‐linethroughtheKUHwebsiteandtheDykesLibrary.Inaddition,mostoftheseresourcesareavailableintheDivisionLibrary(Delp6070).Traineesareexpectedtoreadextensivelyfromtheaboveresourcesthroughoutthetrainingperiod.
110
FELLOWHAND‐OFFPOLICY
ANTICipateAdministrative‐name,location,primaryteamNewInformation(clinicalupdate)Task‐pending,follow‐upresultsIllness‐ActivemedicalissuesContingencyplans‐if___then____
1) Email(usingthepasswordprotected/securedkumc.eduaddresswiththetitle:[SECUREPATIENTINFORMATION]acheckoutlistofthepatientsyouareactivelyfollowingtothefellowtakingoveryourservice.Include:
a. AtKU:allpatientsonyourteam’sEMRlist(i.e.onTeamAlist)b. AtResearchMedicalCenter:theICUpatientslikelytoremaininICUatthetime
thenewfellowwilltakeovertheservicec. AtKCVA:allpatientsontheIDinpatientconsultservicelistd. Atalllocationsencouragetheresidentyouareworkingwithtohand‐offhis/her
patientstotheincomingresidentaswellaspartofyouteachingservicesandforimprovedcontinuityofcare)
2) Copyyourattendingphysicianonthischeckoutforreviewofcontent.Ifyouareroundingwitharesident/studentpleasecopythemaswell.Thecheckoutisahelpfulteachingtool.
3) Hand‐offnoteshouldincludetheelementsofANTICipatenoteoutlinedabove.Hand‐offatKUwilldifferslightlyastheEMRprovidesmuchoftheAdministrativeinformationinthecheckout.Theemailshouldutilizepatientnamesbutcanskipto“N”whenrelayinginformationasitshouldbeusedinconjunctionwiththeEMRlisting.
4) Theemailshouldprovidethenewfellowtimetoreviewandcall/email/pagewithquestionsthusshouldbecompletedassoonaspossiblethedayyoufinishservice.Knowingthatinmanyinstancesthispass‐offmayoccuronaweekday,itshouldbenearlycompletedpriortothelastdayonserviceprovidingyoutimetoupdateitthedayyoufinish.
5) Thecheckoutshouldconcludewithacontactpiecei.e.pleasecallmycellat999‐999‐9999after8tofurtherdiscussthepatientsorifyouhaveadditionalquestions.Itmayhappenthatrelevantquestionsdonotariseuntilthefirstdaythenewfellowtakesovercareandyoushouldbepreparedtofieldquestionslatershouldtheycomeup.

111
GMECFatigue(Transportation/SwingRoom)Guidelines
•Ifyouarefatiguedandunabletoperformyourpatientcareduties,pleasecontactyoursupervisor(i.e.,chieffellow,facultysupervisor,programdirector,Chairand/orGMEOffice/DIO).Pleaseinformyoursupervisorofyoursituationsothattheycanarrangeforalternatecoveragetoensurecontinuityofpatientcare.•Programcallrooms(KUH4461‐4464)shouldbeutilizedforfatiguedresidents/fellowsforrestand/orpowernapping.•Ifyourprogramdoesnothaveacallroomorifyourassignedcallroomsareunavailableorinuse,youmayusetheswingcallroom–(HHroom2901(code1023*)•Ifadequaterestfacilitiesarenotavailable,thenyoumayusethevoucherfatiguetransportationservice•Theprogramleadershipandadministrationwillreceive2vouchersforevery10residents.(Attached)ThePCshouldkeepthisinaplacewellknowntotheresidentsforeasyaccessafterhours.•Foreachevent2voucherswillbeneeded(oneforhomeandthenoneforbacktoworkthefollowingmorning)•TheVoucherswillneedtobefilledinbytheresident/fellowandthetransportationservicedriver(designatedasKUMCResidentProgramTransportationvoucher).Pleaseprintyourname,Departmentandhomeaddressonthevoucher.•Whenyouarereadytoleave,pleasecall10/10TaxiService(913‐647‐0010)andtellthemyouareusingtheKUMCResidentProgramTransportationvoucherandyourdestination.TheywillpickyouupattheMainEntranceofthehospital.•ThetransportationservicewillcollecteachvoucherwhitecopyandsubmittotheGMEOffice.ItisimportantthatyoureturntheYELLOWcopyofthevouchertoyourprogramdirector.•ThetransportationserviceisallowedtopickyouupfromtheKUHHospitalMainEntranceanddropyouoffatyourhomeaddress,withoutanyintervalstops.Thisalsoappliesforthereturntripfromyourhometobacktothehospitalmainentrancethenextmorning.Youneedtousethesecondvoucherforthereturntrip.•TheresidentisresponsiblefordiscussingtheeventandfatigueissuewiththeirProgramLeadershipthefollowingday.Thismustbedocumentedbytheprogramleadershipinthe“Fatigue/TransportationIncidentReport”ThisisavailableinE*Value–Fatigue/TransportationIncidentReport(examplebelow).Again,pleasereturntheyellowvouchercopiestoyourprogramdirectoratthistimeaswell.Thepurposeofthisfileistotrackbothindividualandprogram‐wideepisodesoffatigueandadditionaldutyinordertomitigatefuturerecurrences.•TheGMEOfficewillmanagethecabvouchersandbillbackthedepartmentsastheyarebeingusedaswellasreplenishthevouchersupply.

112
FELLOWREQUIREDONLINETRAININGCOURSES
AngelTrainingCourses
Course Title Assessment Title RequirementGME: Required Curriculum
Professionalism Module: Post Test
One-Time
GME: Required Curriculum
Life Curriculum - Fatigue: Post Test
One-Time
GME: Required Curriculum
Life Curriculum - Substance Abuse: Post Test
One-Time
GME: Required Curriculum
Residents as Teachers: Post Test
One-Time
ChalkTrainingCourses
Training RequirementComputer Security Awareness Training
Ongoing
Counseling and Support Services One-Time
Duty Hour Reporting One-Time
Employee Health Overview One-Time
Equal Rights and Responsibilities One-Time
GME Policy and Procedure Manual One-Time
HIPAA Training for KUMC Providers Ongoing
Harassment Training Ongoing
KU Precautions and OSHA One-Time
KUMC Policies for New Employees One-Time
Safety Training Annual Update Ongoing
Violence in the Workplace Ongoing

113
2011COMMONPROGRAMREQUIREMENTUPDATES
RESIDENTS’ PARTICIPATION IN PATIENT SAFETY PROGRAMS (ANNUAL) (PR VI.A.3) Institutional:
Institutional quarterly Patient Safety Conference GME Core Competency Conferences Resident PGY‐1 orientation: Take Action course synopsis & Resident Handovers group sessions Resident education in patient safety & quality GMEC subcommittee PSN reporting mechanism Risk Management CHALK online modules Resident Council PSN education & reviews of quarterly reports
Program: Internal Medicine Departmental Patient Safety Conference Internal Medicine Departmental CPC conferences ID Program Handover education & process education ID Program Case Conferences with Vanderbilt Matrix tool Antibiotic Subcommittee review of patient safety concerns
RESIDENTS’ PARTICIPATION IN INTERDISCIPLINARY CLINICAL QUALITY IMPROVEMENT PROGRAMS (ANNUAL) (PR VI.A.3) Institutional:
Institutional quarterly Patient Safety Conference GME Core Competency Conferences Resident PGY‐1 orientation: Take Action course synopsis & Resident Handovers group sessions Resident education in patient safety & quality GMEC subcommittee PSN reporting mechanism Risk Management CHALK online modules Resident Council PSN education & reviews of quarterly reports TeamSTEPPS dissemination
Program:
InterdisciplinaryProgramPBLIprojects(usePBLItemplate)Internal Medicine Departmental Patient Safety Conference Internal Medicine Departmental CPC conferences
IDDepartmentQImonitoringIDCaseConferencewithVanderbiltMatrixtool
BACK UP SYSTEM WHEN CLINICAL CARE NEEDS EXCEED RESIDENTS’ ABILITY (PR VI.C.2) Institutional:
Institutional GME Manual Policy statement KUH Hospital Links online on‐call system‐
TeamupdatesofO2TeaminEpic Resident Orientation (Duty Hour & Supervision talk)

114
Program: IDDivisionCallSchedule‐postedonlineIDDivisionPolicyManualdescriptionofcontinuitycoverageforfatiguedresident
SCHEDULES THAT INFORM ALL TEAM MEMBERS OF ATTENDING/RESIDENTS CURRENTLY RESPONSIBLE FOR EACH PATIENT’S CARE (VI.B.4) & RESIDENTS & FACULTY INFORM PATIENTS OF THEIR ROLES IN CARE (VI.D.1.B) Institutional:
KUH admission Handout to patient with description of level of caregivers UKP clinic handout of caregiver definitions KUH Oncall system in Hospital links O2 “patient care team” accuracy Bedside whiteboard
Program:
RRC‐defineddesignationoflicensedindependentpractitionerinGMECResidentSupervisionTemplateattachedtoG&Oand/orhandbookProgramsupervisionpoliciesupdatedtoincludenewsupervisionrequirementsID Division on‐call schedule mechanisms education Picture roster (faculty with all residents listed) Business cards given to patients with names/titles
DESCRIBE HOW CLINICAL ASSIGNMENTS DESIGNED TO MINIMIZE PATIENT CARE TRANSITIONS (PR VI.B.1) Institutional:
Program:
AnnualIDProgramOutcomesAssessmentandActionPlanReportcheckboxMonthly Fellow rotation schedule Continuity clinic assigned to faculty clinic for 2 year duration
EDUCATION & IMPLEMENTATAION OF STRUCTURED HAND-OVER PROCESS(PR VI.B.2) Institutional:
Residents’ orientation video & small group sessions Residents’ SIGNOUT Template pocket card EPIC O2 Signout instrument Angel online module about handoffs/transitions of care
Program: ID Program specific education at orientation Written handoff process described in ID Division manual
FATIGUE, SLEEP DEPRIVATION AND MITIGATION EDUCATION (PR VI.A.5.e & VI.C.1.a), INCLUDING EDUCATION OF PREFESSIONAL RESPONSIBILITY TO APPEAR FOR DUTY RESTED/FIT (VI.A.1) Institutional:
GME ANGEL online Fatigue Education Module modification
115
Resident Orientation (Duty Hour & Supervision talk) Institutional Policy statement Add to IR and SV preparation process checklists
Program:
IDDivisionspecificfatigueeducation InternalMedicineDepartmentandIDDivisionPolicyManualStatements(inprofessionalismorDutyHourPolicy)
FATIGUE MITIGATION PROCESSES, CONTINUITY OF CARE IF UNABLE TO PERFORM DUTIES AND SLEEP/TRANSPORTATION FOR FATIGUED RESIDENTS (VI.C.1-3) Institutional:
Resident Orientation (Duty Hour & Supervision talk) Resident Council education GMEC education Department call rooms & Swing Call room Fatigue Transportation service (GME Manual guidelines section)
Program:
E*Value fatigue file (fatigue transportation incidents & explanation box for 24hr and 8hr rule violations‐ monitored by PD)
ID Division call schedule ID Division Policy Manual‐describe continuity process Team updates of O2 Team in Epic
MONITORING PATIENT CARE PERFORMANCE INDICATORS (VI.A.5.g) Institutional: Program:
Dept QI requirements/measures KUH QI report requirements/measures UKP QI report requirements/measures Internal Medicine Patient Safety and CPC conferences Infectious Diseases Case Conference Patient 360‐degree surveys/evaluations
FACILITIES (all available) □ Sleeping Rooms – segregated by Gender □ Shower/Bath □ Secure room or lockers

116
INDEX A
Advancement to Succeeding Training Year 28 Adverse Events 42
B Benefits 39 Access to Medical Literature 40 Board Preparation Materials 40 Disability Insurance 39 Life Insurance 39 Malpractice Insurance 39 Medical Insurance 39 Parking 40 Pay 39 White Coats 40 Work Environment 40
C Call Schedule 33 Common Program Requirement Updates 111 Communication 34 Conferences, Lectures and Other Education Opportunities 22 Antibiotic Committee 25 Clinicopathological Conference 27 Core Curriculum Conference 23 Infection Prevention and Control Committee 26 Infectious Diseases Clinical Case Conference 23 Journal Club 24 Kansas City Infectious Diseases Society (KCIDS) 25 Patient Safety Conference 27 Research Conference 24 Contact Information 5 Core Competency Teaching and Assessment Matrix 82 Core Curriculum Schedule 49 Curriculum 14 Year One Fellowship 14 Year Two Fellowship 20 Year Three Fellowship 22
D Disciplinary Actions 44 Divisional Goals 10 Documentation of Training 29 Duration of Program 31 Duties 31 Duty Hours Policy 32
E Educational Objectives 53 Ethics 28, 41

117
Evaluation of Faculty and Program 29 Evaluation of Fellows 28 Evaluations, Forms Faculty Evaluation of Program 84 Faculty of Fellow Evaluation 87 Fellow of Faculty Evaluation 90 Fellow of Program Evaluation 93 Fellow Peer Evaluation 96 Fellow Self Assessment Evaluation 99 Nurse Evaluation of Fellow 102 Patient Evaluation of Fellows 104 Research Faculty of Fellow 105 Support Staff of Fellow Evaluation 108 Evaluations, Required 83
F Family Leave 38 Fatigue 32 Fatigue Guidelines 111 Fellowship Selection Process 30
G GME Supervision Template 53 GMEC Fatigue (Transportation/Swing Room Guidelines 107 Goals, Divisional Grievance Resolution 47
H Hand Off Policy 110 Hand Off, Service 34
I ID Conferences 52 ID Service Hand Off 34 Impairment 44 Institutional Supervising Faculty 7 Interview Leave 37 Introduction 4
L Late Start 38 Leave Family 38 Interview 37 Personal 37 Vacation 37 Lines of Responsibility 36
M Meeting Attendance 36 Mission Statement 9 Moonlighting 40

118
N Non-teaching Patients 35
O Objectives First Year Inpatient Consultative Service 16 First Year Outpatient Clinics 17 First Year Clinical Microbiology Laboratory 18 First Year Research 19 Second Year Inpatient Consultation Service 20 Second Year Outpatient Clinics 21 Second Year Research 22 Online Training 112 Order Writing 35 Outpatient Antibiotic Therapy (OPAT) 26 Overview of the Educational Objective with Reference to Six Core Competencies Year One 55 Year Two 56 Overview of Goals and Objectives for Rotations University of Kansas Inpatient Consultation 57 Kansas City Veterans Administration Medical Center Inpatient Consultation 61 Research Medical Center Inpatient Consultation 65 University of Kansas Clinic Rotation 69 Kansas City Veterans Administration Medical Center Clinic Rotation 73 Microbiology Rotation 77 Research Rotation 80 Overview, Program 9
P Pediatric Infectious Diseases 22 Performance Deficiencies 45 Performance Expectations 10 Patient Care 10 Medical Knowledge 11 Practice-Based Learning 12 Interpersonal Skills and Communication 12 Professionalism 13 Systems-Based Practice 13 Personal Leave 37 Policies and Procedures 30 Prerequisites 30 Probation 44 Professional Ethical Behavior 28 Professionalism 43 Program Overview 9
Q Quality Improvement 41
R Recommended References 109

119
Required Evaluations, List 81 Required Online Training 112 Risk Management 42
S Sick Leave 38 Suspension 44
T Termination 44
U Utilization Management 41
V Vacation Leave 37
Y Year One Fellowship 14 Year Two Fellowship 20 Year Three Fellowship 22