Poisoning/Overdose General Management Poisoning is Exposure to substance that is toxic in any...
64
Poisoning/Overdose General Management Poisoning is Exposure to substance that is toxic in any amount
-
Upload
georgia-johns -
Category
Documents
-
view
218 -
download
0
Transcript of Poisoning/Overdose General Management Poisoning is Exposure to substance that is toxic in any...

Poisoning/Overdose
General Management
Poisoning is Exposure to substance that is toxic in any amount
Overdose
Exposure to substance in excess amount
resulting in toxic effects
1998 TESS* Data1998 TESS* Data
• 2,241,082 reported human exposures
• 97.9 % at home
• Peak volume 4pm-10pm
• 91% of calls 8pm-midnight
*The Toxic Exposure Surveillance System (US based)

Exposures by Age
• < 6 years old 52.7%
• < 3 years old 39.6%
• 775 fatalities
• 0.03% of total exposures
• ages 20 - 49 years = 56%
• >6 years = 2.1%
Fatalities
Number of Substances
• 92.8% of all cases--one substance
• 44.7% of fatal cases-->2 substances
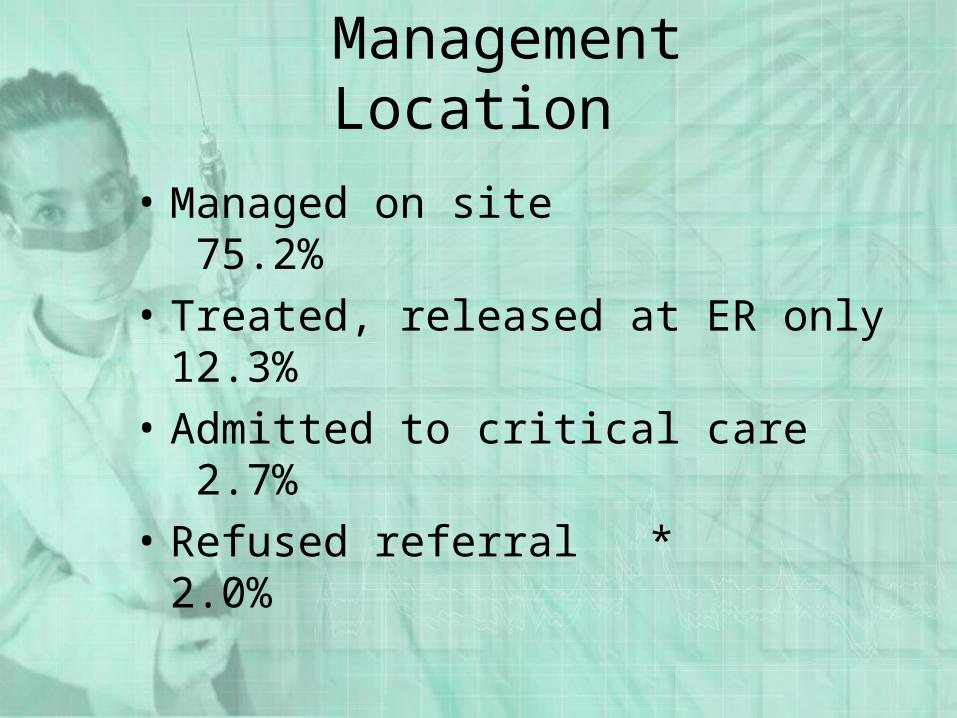
Management Location
• Managed on site 75.2%
• Treated, released at ER only 12.3%
• Admitted to critical care 2.7%
• Refused referral * 2.0%
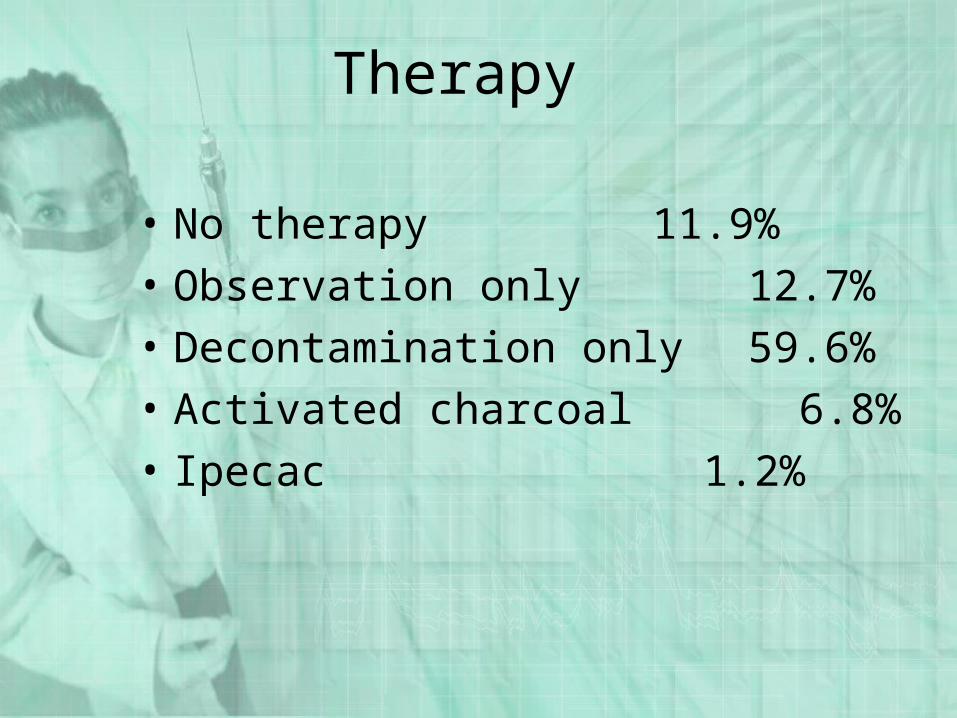
Therapy
• No therapy 11.9%
• Observation only 12.7%
• Decontamination only 59.6%
• Activated charcoal 6.8%
• Ipecac 1.2%
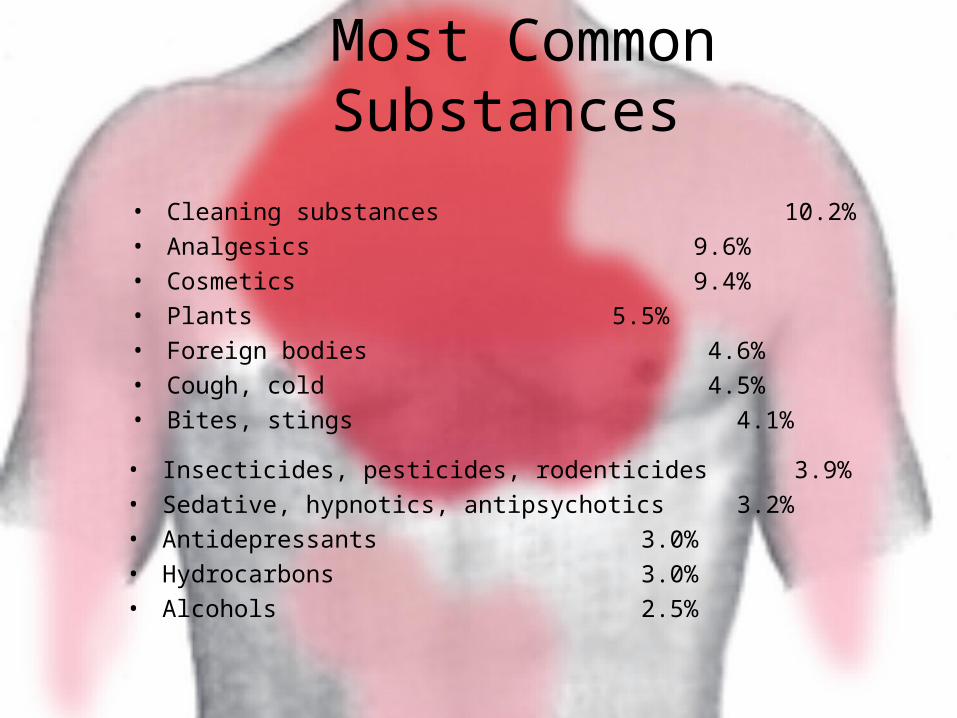
Most Common Substances
• Cleaning substances 10.2%
• Analgesics 9.6%
• Cosmetics 9.4%
• Plants 5.5%
• Foreign bodies 4.6%
• Cough, cold 4.5%
• Bites, stings 4.1%
• Insecticides, pesticides, rodenticides 3.9%
• Sedative, hypnotics, antipsychotics 3.2%
• Antidepressants 3.0%
• Hydrocarbons 3.0%
• Alcohols 2.5%
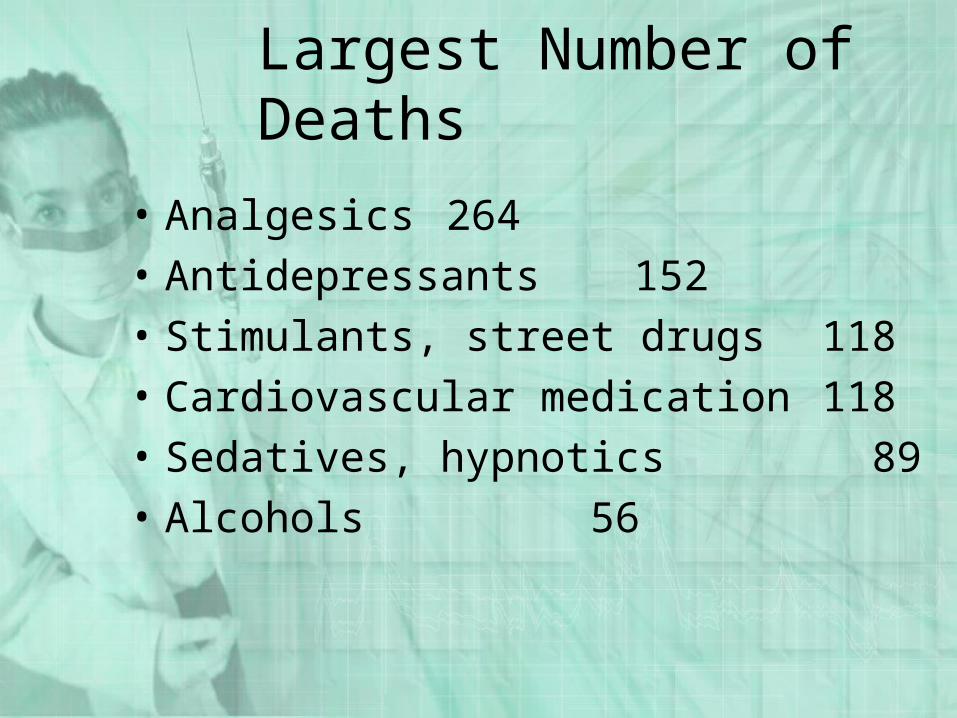
Largest Number of Deaths
• Analgesics 264
• Antidepressants 152
• Stimulants, street drugs 118
• Cardiovascular medication 118
• Sedatives, hypnotics 89
• Alcohols 56
Indicators
• Sudden onset of CNS signs:– Seizures– Coma– Decreased LOC– Bizarre behavior
• Sudden onset of:– Abdominal pain– Nausea– Vomiting

Indicators cont
• Sudden onset of unexplained illness
• Bizarre, incomplete, evasive history
• Trauma (>50% of adult trauma EtOH, drug-related)
• Pediatric patient with arrhythmias
History
• What?• How much?• How long?• Multiple substances?• Treatment attempted? How?
Whose advice?• Psychiatric history?• History of suicide?
Scene Survey
• Check out scene for :– 1– 2– 3– 4
• Where do you look for clues?
General Management
• Support ABC’s– Secure airway, secure with advanced airway
if needed– Ensure adequate oxygenation, ventilation– Maintain adequate circulation
• Monitor ECG• Obtain vascular access• Manage hypotension initially with volume• Use vasopressors cautiously
General Management
• Keep patient calm • Maintain normal body temperature• Evaluate nature/toxicity of poison
– Check container, package insert, poison center information
– Treat the patient, not the poison
General Management
• Rule out (differential diagnosis)– Trauma– Neurological disease– Metabolic disease
• Base general management on route of poison entry
Poison Entry
• Ingestion
• Slow movement from injection site throughout body
• Remove from skin surface
• Remove from exposure; Support oxygenation, ventilation
• Prevent absorption from GI tract
• Inhalation
• Absorption
• Injection

Ingested Poisons
Objective
Remove from GI tract before absorption occurs
Ipecac
• RARELY used anymore
• If used, has to have been initiated within few minutes after ingestion
• Vomiting in 20-30 minutes
• Only removes about 32% of contaminate
• Many contraindications
Ipecac
• Dose– 15 cc if 12 months to 12 years old– 30 cc if >12 years old
• Follow with 2-3 glasses of water
• Keep patient ambulatory if possible
Ipecac
• If no vomiting after 20 minutes, repeat
• When emesis occurs, keep head down
• Collect, save vomitus for analysis
Ipecac
• Contraindications– Comatose or no gag reflex– Seizing or has seized– Caustic (acid or alkali) ingestion– Low viscosity hydrocarbon ingestion– Late term pregnancy
Ipecac
• Contraindications– Severe hypertension, cardiovascular
insufficiency, possible AMI– Ingestion of:
• Strychnine• Phenothiazines (Thorazine, Stellazine, Compazine)• Tricyclic antidepressants• Iodides• Silver Nitrate
Lavage
• Commonly used in ED’s• Removes about 31% of substance• Helps get activated charcoal in
patient, especially if patient is unconscious
• Not helpful for sustained release tablets
• Will not remove large tablets
Activated Charcoal
• Adsorbs compounds, prevents movement from GI tract
• Very effective at adsorbing substances
• Binds about 62% of toxin
• Dose– 5 - 10X estimated weight of ingested
chemical
Activated Charcoal
• Inactivates Ipecac
• Do not give until vomiting stops
• Do not give with – Cyanide– Methanol– Tylenol (+)
• Containers must be kept airtight
• Can be given PO via slurry or by NG
Inhaled Poisons
Objective: Move to fresh air; optimize ventilation and protect
personnel from exposure
Absorbed Poisons
Objective: Remove poison from skin
Liquid: Wash with copious amounts of water
Powder: Brush off as much as possible, then wash with copious
amounts of water
Protect personnel from exposure

Dilute / Irrigate / Wash
• Use soap, shampoo for hydrocarbons
• No need for chemical neutralization - heat produced by reaction could be harmful

Eye Irrigation
• Wash for 15 minutes
• Use only water or balanced salt solutions
• Remove contact lenses
• Wash from medial to lateral
Examples of Specific Toxins
Acids
• Examples– Toilet bowl cleaner– Rust remover– Phenol (carbolic acid)– Hydrochloric acid
• Severe burning of stomach
• Absorption, systemic acidemia
Acids
• Loss of airway = most immediate threat
• Secure airway against edema
• IV with RL, NS for volume loss
• Emesis, gastric lavage contraindicated
• Dilution with water, milk NOT recommended
Alkalis
• Examples– Drain cleaner– Washing soda– Ammonia– Lye (sodium hydroxide)– Bleach (sodium hypochlorite)
• Severe burning of esophagus, stricture formation
Alkalis
• Loss of airway = most immediate threat
• Secure airway against edema
• IV with LR, NS for volume loss
• Emesis, gastric lavage contraindicated
• Dilution with water, milk NOT recommended

Hydrocarbons
• Examples– Kerosene– Gasoline– Lighter fluid– Turpentine– Furniture polish
Hydrocarbons
• Signs/Symptoms– Choking, coughing, gagging– Vomiting, diarrhea, severe
abdominal pain– Chemical pneumonitis, pulmonary
edemaIf the patient is coughing, aspiration has occurred
Methanol
methyl alcohol
wood alcohol
wood naphtha
Methanol
• Sources– Industry– Household solvents– Paint remover– Fuel, gasoline additives– Canned heat– Windshield washer antifreeze
Methanol
• Toxic dose– Fatal oral: 30-240ml– Minimum: 100 mg/kg– Example
• Windshield washer fluid 10% Methanol• 10 kg child needs only 10 cc to be toxic
Methanol
• Mechanism of toxicity– Methanol slowly metabolized to
formaldehyde– Formaldheyde rapidly metabolized
to formic acid• Acidosis• Ocular toxicity
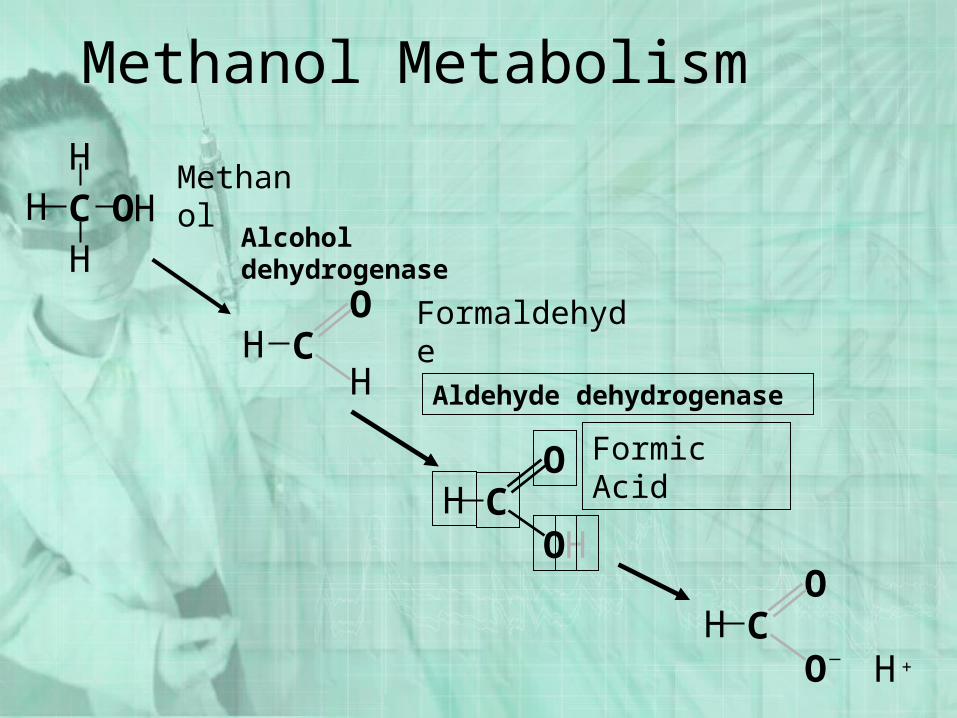
Methanol Metabolism
OC
OH
H+_
HOC
OH
Formic Acid
CH
OH
Formaldehyde
HOHH
HC
Methanol
Alcohol dehydrogenase
Aldehyde dehydrogenase

Cyanide
But first…• A little review of
biochemistry and biophysics
Staying alive requires energy...
• The natural tendency of the universe is for things to become more disorderly.
• This trend toward disorder is called entropy.
• Complex systems (including us) don’t tend to last long, unless…
• They have a constant supply of energy to combat entropy.
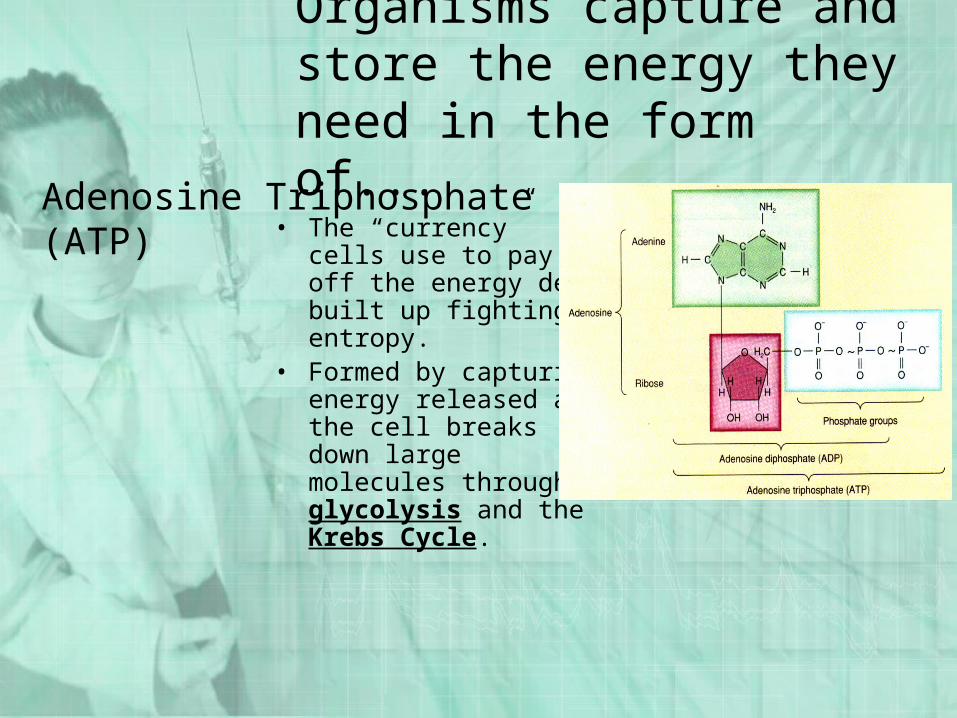
Organisms capture and store the energy they need in the form of...
• The “currency” cells use to pay off the energy debt built up fighting entropy.
• Formed by capturing energy released as the cell breaks down large molecules through glycolysis and the Krebs Cycle.
Adenosine Triphosphate (ATP)
Putting It All Together• Cells have to have energy to stay alive.• Cells get energy by breaking down glucose in two phases: glycolysis and
the Krebs Cycle.• Glycolysis yields 2 ATP and pyruvate.• Pyruvate is changed to acetate (acetyl-CoA) and sent to the Krebs Cycle.• The Krebs Cycle strips hydrogen and electrons off acetate and feeds them
into the electron transport chain.• Movement of electrons down the transport chain releases energy which is
trapped as ATP.
• At the end of the chain, the electrons combine with hydrogen and oxygen to
form water.
• CN messes with this !
Cyanide
• Chemical, plastic industries• Metallurgy, jewelry making• Blast furnace gases• Fumigants, pesticides• Present in various plants
– apples, pears, apricots, peaches, bitter almonds
• Remember there is CN gas released by BURNT plastics (e.g fire!!)
Cyanide Antidote Kit
• Amyl nitrite, sodium nitrite – Only be used in serious cyanide poisonings– Can induce life-threatening tissue hypoxia
secondary to methemoglobinemia
• Sodium thiosulfate – Can be used by itself– Is relatively benign

Salicylates
Salicylates
• Examples– Aspirin– Oil of wintergreen
• Uses– Analgesics– Antipyretics– Anti-inflammatories– Platelet function inhibitors
Salicylates
• Mechanism of Toxicity– Direct stimulation of respiratory center,
causing respiratory alkalosis– Irritation of gastrointestinal tract, causing
decreased motility, pylorospasm, nausea, vomiting, hemorrhagic gastritis
– Decreased prothrombin levels/platelet dysfunction, causing prolonged clotting times
– Uncoupling of oxidative phosphorylation
Results of Oxidative Phosphorylation Uncoupling
• ATP production decreases, resulting in CNS and cardiovascular failure.
• Cells attempt to compensate by increasing the rate they process glucose anaerobically through glycolysis.
• Lactic and pyruvic acids accumulate, leading to metabolic acidosis.
• Hypoglycemia results as liver sugar stores are depleted.• In absence of sugar cells begin to metabolize lipids, ketone
bodies are produced, acidosis worsens.• Energy normally trapped as ATP is wasted as heat, causing
a rise in body temperature.• The rise in body temperature accelerates metabolism,
increasing tissue oxygen demand and worsening acidosis.
Salicylates
– Vomiting– Lethargy– Hyperpnea– Respiratory
alkalosis– Metabolic
acidosis
– Coma– Seizures– Hypoglycemia– Hyperthermia– Pulmonary
edema
Clinical Presentation: Acute Toxicity
Salicylates
• Clinical Presentation: Chronic Toxicity– Usually young children, confused
elderly– Confusion, dehydration, metabolic
acidosis– Higher morbidity, mortality than acute
overdose– Cerebral, pulmonary edema more
common
Salicylates
• Acute Toxicity Management– Oxygen, monitor, IV– GI tract decontamination– Activated charcoal– Replace fluid losses, but do NOT
overload– Control hyperthermia
Salicylates
• Acute Toxicity Management– Bicarbonate for metabolic acidosis– D50W for hypoglycemia– Diazepam for seizures

Acetaminophen
Acetamophen
• Examples– Tylenol– Tempra– Many drugs contain this also
• Uses– Analgesic– Antipyretic
Acetaminophen
• Mechanism of toxicity– N-acetyl p-benzoquinonimine,
normal product of acetaminophen metabolism, is hepatotoxic
– Normally is detoxified by glutathione in liver
– In overdose, toxic metabolite exceeds glutathione capacity, causes liver damage
Acetaminophen
• Management– Induce emesis– Do NOT give activated charcoal in
general– Give specific acetaminophen
antidote
Acetaminophen
• The specific antidote for acetaminophen toxicity.
Mucomyst
• N-acetylcysteine Another sulfur-containing amino acid Substitutes for glutathione. Allows continued detoxification of NAPBQI. 140mg/kg initially followed by 70mg/kg every 4 hours
17 times. Tastes, smells like rotten eggs Mix with chilled fruit juice to decrease odor, taste
More to come
• Review – Cocaine OD– TCA OD– Opoid OD– MDMA - E– GHB