Pneumonia Still the “Old man’s friend?” -Bacterial, Viral, Chemical, Aspiration, Nosocomial,...
25
Pneumonia Still the “Old man’s friend?” -Bacterial, Viral, Chemical, Aspiration, Nosocomial, Community Acquired, “Walking,” Bronchopneumonia, Necrotizing, Ventilator Associated…
-
Upload
malcolm-ferguson -
Category
Documents
-
view
221 -
download
0
Transcript of Pneumonia Still the “Old man’s friend?” -Bacterial, Viral, Chemical, Aspiration, Nosocomial,...

PneumoniaStill the “Old man’s friend?”
-Bacterial, Viral, Chemical, Aspiration, Nosocomial, Community Acquired,
“Walking,” Bronchopneumonia, Necrotizing, Ventilator Associated…

True story (and disclaimer)
• A Family Practice doc is at the nurse’s station and asks the Respiratory Therapist standing next to him (who’s charting on a different patient), “What antibiotic do you think I should prescribe for this guy?”
• The RT replies, “Don’t ask me, I’m just the plumber.”

Diagnosis?
• A pulmonogist with 25+ years experience guesses he is only correct 60% of the time when diagnosing pneumonia before seeing the CXR. A little better than a coin-toss.

Guidelines
• CXR is considered the Gold Standard• Leukocytosis with leftward shift common• Tachypnea, fever, sputum production, and
abnormal lung sounds are helpful, but not definitive.
• Blood cultures- controversial, recommended for sickest patients.
• Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. AUMandell LA; Wunderink RG; Anzueto A; Bartlett JG; Campbell GD; Dean NC; Dowell SF; File TM Jr; Musher DM; Niederman MS; Torres A; Whitney CG SOClin Infect Dis. 2007 Mar 1;44 Suppl 2:S27-72.

CXR dilemma
• It looks like pneumonia, talks like it, walks like it, but the CXR is inconclusive. Sometimes the diagnosis will still be made.
• There’s a theory that a dehydrated, sick patient won’t have the infiltrate “appear” on their CXR until their volume is increased. This might be a fact in 7% of patients with all the other symptoms, but negative initial CXR. 1
• A CT Scan is not recommended if only looking for pneumonia, due to cost, and lack of outcome data.
• Patients admitted to hospital with suspected pneumonia and normal chest radiographs: epidemiology, microbiology, and outcomes. AUBasi SK; Marrie TJ; Huang JQ; Majumdar SR SOAm J Med 2004 Sep 1;117(5):305-11.

Sputum Cultures
• The 2007 IDSA/ATS consensus guidelines for which patient to obtain a culture from:
• Intensive care unit admission
• Failure of outpatient antibiotic therapy
• Cavitary lesions
• Active alcohol abuse
• Severe obstructive or structural lung disease
• Positive urine antigen test for pneumococcus
• Positive urine antigen test for legionella (special culture needed)
• Pleural effusion

Sputum continued….
• The specimen should be a deep cough specimen obtained prior to antibiotics.
• Cultures should be performed rapidly after collection, preferably within two hours; the alternative for rapid plating of the sample is to retain the specimen at 4ºC if the delay is two to 24 hours
• A "good" sputum sample is one with polymorphonuclear leukocytes (PMNs) but a low or absent number of squamous epithelial cells (SECs) on Gram stain.

Ways to Obtain Sample• Good, deep cough. (These are the best, but the patient has to
be strong enough to cough well, and the sputum well hydrated. Tough to find in the sickest patients.)
• Naso-Tracheal suctioning- very uncomfortable for patient, but sometimes the most effective way.
• BAL Cath (Broncho-Alveolar-Lavage) catheter is manufactured to allow samples to be obtained with minimal contamination.
• Bronchoscopy- most direct method, but expensive and resource consuming.
• Hypertonic Saline via Nebulizer and CPT…

Chest Physical Therapy
• Not always effective- needs the right kind of “phlegm” and patient cooperation.
• Pneumonia can be thought of as peanut butter, stuck in a jar. You can’t really tip the jar upside down and whack the peanut butter out of it.
• CPT needs mobile, well-hydrated phlegm, and can aid it’s drainage.
• Very helpful if patient has fairly effective cough to assist clearance.
• Limited by patient tolerance for being in Trendelenburg, surgical wounds, sore ribs from coughing or previous CPT.


Nebulizers/Bronchodilators
• Not really effective with pneumonia, unless wheezing/bronchospasm are present.
• Patients who have a history of lung dz and are more prone to pneumonia, may need an increase of their bronchodilators during the illness.
• Mucolytics can be helpful with mucous plugging; administered before CPT.

Data for Best Practice
• A multicenter controlled trial using cluster randomization in 1743 patients with CAP who presented to the Emergency Department in 19 hospitals; the trial compared conventional care to the use of a critical pathway algorithm for hospitalization and treatment [1].
• The care pathway included therapy with intravenous and oral levofloxacin; in comparison, levofloxacin was not available to physicians in the conventional treatment hospitals.
• 1. A controlled trial of a critical pathway for treatment of community-acquired pneumonia. CAPITAL Study Investigators. Community-Acquired Pneumonia Intervention Trial Assessing Levofloxacin. AUMarrie TJ; Lau CY; Wheeler SL; Wong CJ; Vandervoort MK; Feagan BG SOJAMA 2000 Feb 9;283(6):749-55.

It Works
• Patients treated according to the algorithm had significant reductions in the number of bed days per patient admitted (4.4 versus 6.1 days) and in the proportion of low-risk patients who were admitted (31 versus 49 percent).
• Although inpatients at critical pathway hospitals had more severe disease, they required significantly fewer days of intravenous therapy and were more likely to be treated with a single class of antibiotic.
• These reductions in the use of hospital resources were not associated with any adverse clinical effects, as complications, readmission, mortality, and quality of life were not different between the two groups.

General Ward Abx guidelines
• Beta-lactam (ceftriaxone, cefotaxime, ampicillin/sulbactam, ertapenem) plus macrolide (can use doxycycline if macrolide not tolerated)
• OR• Antipneumococcal fluoroquinolone alone
• 1. Clin Infect Dis. 2007.
(ATS/IDSA; 2007)

Severe/ICU Patient
• Beta-lactam (ceftriaxone, cefotaxime, ampicillin/sulbactam) plus IV azithromycin or IV fluoroquinolone
• If concern for Pseudomonas (eg, presence of structural lung disease such as bronchiectasis): antipseudomonal agent (piperacillin/tazobactam, imipenem, meropenem, or cefepime) plus antipseudomonal fluoroquinolone (ciprofloxacin or high dose levofloxacin);
• If concern for MRSA: add vancomycin or linezolid
• 1. Clin Infect Dis. 2007.(ATS/IDSA; 2007)

Causes of community-acquired pneumonia in hospitalized patients (non-ICU)
Table from UpToDate:1. Arch Intern Med 1997; 157:1709.2. Ir J Med Sci 1989; 158:230.3. Lancet 1982; 2:255.4. Thorax 1991; 46:508.5. Infection 1987; 15:328.

www.meddean.luc.edu


http://www.cdc.gov/ncidod/eid/vol6no1/scrimgeourG2.htm

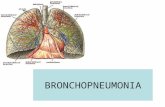
Why the Right Side with aspiration?
• When looking down the trachea, the RLL is a “direct shot” for anything aspirated.
• http://math.lbl.gov/~deschamp/html/gallery.html

The Sickest Patients• Mechanical Ventilation-
– As the pneumonia takes over healthy space in the lung, patients may not be able to compensate, or have the energy to keep up with the increased work of breathing.
– An endotracheal tube can be placed and the ventilator can now assist with respiration.
– Air provided to the patient is humidified to 100%, and warmed to 37 degrees, helping to thin secretions.
– In-line suction catheters allow for easy removal of retained secretions.
– PEEP (Positive End Expiratory Pressure) can be used to possibly recruit collapsed air sacs and improve oxygenation.


VAP and Prevention (What works for us)
• Wash hands (of course)• Subglottic Suction Tube (Hi Lo Evac)• HOB at 30 degrees• Orogastric Tube as opposed to Nasogastric • Mouth Care• Heated wire vent circuit • Don’t “break” the circuit if at all possible!• Gastric acid suppression may increase risk of VAP.
Care should be taken to avoid proton pump inhibitors or H2 blockers if pt is low risk for stress ulcers.
• (Strategies to prevent ventilator-associated pneumonia in acute care hospitals. AUCoffin SE; Klompas M; Classen D; Arias KM; Podgorny K; Anderson DJ; Burstin H; Calfee DP; Dubberke ER; Fraser V; Gerding DN; Griffin FA; Gross P; Kaye KS; Lo E; Marschall J; Mermel LA; Nicolle L; Pegues DA; Perl TM; Saint S; Salgado CD; Weinstein RA; Wise R; Yokoe DS SOInfect Control Hosp Epidemiol. 2008 Oct;29 Suppl 1:S31-40.

• The use of an endotracheal or tracheostomy tube with aspiration of subglottic secretions seems to decrease the incidence of VAP and should be recommended in patients expected to require more than 72 h of mechanical ventilation. The decontamination of subglottic space remains an attractive idea that needs further confirmation.
• Anesthesiology: Pneumatikos, Ioannis A. M.D., Ph.D., F.C.C.P.; Dragoumanis, Christos K. M.D., Ph.D.; Bouros, Demosthenes E. M.D., Ph.D., F.C.C.P.
• March 2009 - Volume 110 - Issue 3 - pp 673-680