
PMDC Inspection for College
16
INSPECTION PROFORMA - B PAKISTAN MEDICAL & DENTAL COUNCIL PROFORMA FOR INSPECTION OF MEDICAL/DENTAL COLLEGES AND ATTACHED TEACHING HOSPITALS
-
Upload
asif-manzoor -
Category
Documents
-
view
418 -
download
17
Transcript of PMDC Inspection for College

INSPECTION
PROFORMA - B
PAKISTAN MEDICAL & DENTAL COUNCIL
PROFORMA
FOR
INSPECTION OF MEDICAL/DENTAL COLLEGES
AND
ATTACHED TEACHING HOSPITALS

Name of the Medical/Dental College
Tagged Area & Population Served Date of last inspection of the College Proposed date of inspection Present status of the College (Permanent, Temporary, Provisional/Recognition granted by the Pakistan Medical & Dental Council. Details of improvements made since last inspection).
Number of Yearly Admission/Passed for the last five- (5) years
Admission Passed percentage
19 19 2000 2001 2002
No. of Admissions at the time of last inspection.
Present Admission
Building Department-Wise

TEACHING STAFF Department
Designation Requirement of
PMDC Actual Teaching
Staff Deficiency
A- ESSENTIAL SUBJECT ANATOMY
Professor Associate Prof. Assistant Prof. Lecturer/ Demonstrator
PHYSIOLOGY
Professor Associate Prof. Assistant Prof. Lecturer/ Demonstrator
BIOCHEMISTRY
Professor Associate Prof. Assistant Prof. Lecturer
PHARMACOLOGY
Professor Associate Prof. Assistant Prof. Lecturer
PATHOLOGY AND BACTERIOLOGY
Professor Associate Prof. Assistant Prof. Lecturer
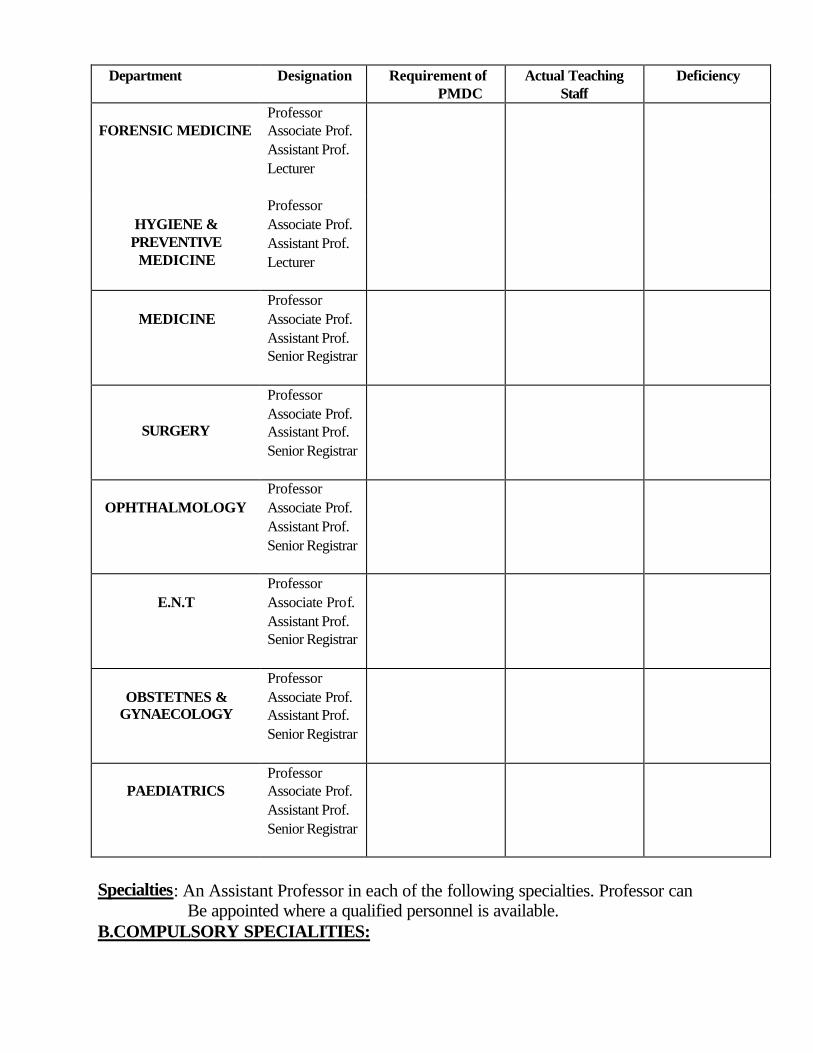
Department
Designation Requirement of
PMDC Actual Teaching
Staff Deficiency
FORENSIC MEDICINE Professor Associate Prof. Assistant Prof. Lecturer
HYGIENE &
PREVENTIVE MEDICINE
Professor Associate Prof. Assistant Prof. Lecturer
MEDICINE
Professor Associate Prof. Assistant Prof. Senior Registrar
SURGERY
Professor Associate Prof. Assistant Prof. Senior Registrar
OPHTHALMOLOGY
Professor Associate Prof. Assistant Prof. Senior Registrar
E.N.T
Professor Associate Prof. Assistant Prof. Senior Registrar
OBSTETNES &
GYNAECOLOGY
Professor Associate Prof. Assistant Prof. Senior Registrar
PAEDIATRICS
Professor Associate Prof. Assistant Prof. Senior Registrar
Specialties: An Assistant Professor in each of the following specialties. Professor can Be appointed where a qualified personnel is available. B.COMPULSORY SPECIALITIES:

Department
Designation Requirement of
PMDC Actual Teaching
Staff Deficiency
Psychiatry
Asstt:Professor
Radiology(diagnostic)
Asstt:Professor
Radiology(Therapeutics)
Asstt:Professor
Anesthesia
Dentistry
Orthopedics
Tuberculosis
Dermatology
C.OPTIONAL SPECIALITIES:
Department
Designation Requirement of PMDC
Actual Teaching Staff
Deficiency
Neurology
Cardiology
Urology
Dermatology &V.D.
Plastic Surgery
Neuro-Surgery
STATEMENT SHOWING THE QUALIFICATIONS & EXPERIENCES OF TEACHING STAFF OF________________________________________________ S no. Name Designation Qualification PMDC
Registration No.
Teaching Experience
REMARKS
Name of Attached Teaching Hospital _____________________Total bed strength_____________ Student/bed ratio_______________________
Department No. of beds No. of units Remarks 1. MAJOR SUBJETS Medicine
Surgery
Obstetrics & Gynaecology
Ophthalmology
E.N.T
Paediatrics
Orthopaedics
Casualty
Tuberculosis
Cardiology
Psychiatry
Maternity & Child Health
Radiology(Diagnostics)
Radio-Therapy
Medico-legal
Pathology
Anaesthesiology

Department No. of beds No. of units Remarks 2. COMPULSORY
SPECIALITIES
3. OPTIONAL SPECIALITIES
Total number of beds in hospital

STATEMENT SHOWING THE QUALIFICATIONS & EXPERIENCES OF DOCTORS/ SPECIALISTS OF TEACHING HOSPITAL ATTACHED TO THE
MEDICAL COLLEGE ____________________________________________
S.No Name of Doctors/
Specialist Designation Qualification PMDC
Registration No.
Teaching Experience
REMARKS
LIST OF EQUIPMENT (Department-wise)
S.No Department Name of Equipment
Model / Make Quantity Serviceable/ Unserviceable
Condition Of
Equipment
Remarks
Library Accommodation Adequate/inadequate No. Of Books subject-wise No. Of Magazines Museum Building Models Specimens

Prospectus of the College. (Copy should be attached) Syllabus of the College Examination System -- (Regulation of the University should be Supplied) Average Result of Last five years Year No. of Students appeared No. of Students
passed Percentage
19
19
2000
2001
2002

HOSTEL FACILITIES (For Boys)
HOSTEL FACILITIES (For Girls)
EXTRA CURRICULAR ACTIVITIES AVAILABLE IN THE COLLEGE
1. 2. 3. 4. 5.
Signature__________________________
Name______________________________
Principal Medical
__________________ College
Dental

GENERAL OBSERVATIONS OF THE INSPECTION TEAM
Recommendations of Inspection Team. Not Recommended for Recognition. Recommended for Provisional recognition for __________________Years.
Signature of Convenor___________________ NAME_______________________________
DESIGNATION_______________________ Signature of Members Name/Designation


















