Pleural bupivacaine placement for optimal postthoracotomy pulmonary function: A prospective,...
4
Pleural Bupivacaine Placement for Optimal Postthoracotomy Pulmonary Function: A Prospective, Randomized Study Jonathan Richardson, MD, MRCP, FRCA, Sabaratnam Sabanathan, MD, FRCS, Rajesh D. Shah, MS, FRCS, Brian J, Clarke, MSC, PhD, Surrindar Cheema, FRCA, and Alan J. Mearns, FRCS Objective: To determine dependent chest tube losses of bupivacaine with paravertebral versus interpleural adminis- tration, thereby helping to explain the significant differences in pulmonary function that exist between these two techniques. Design: A prospective, randomized study. Setting: A single hospital. Participants: Twelve adult patients undergoing posterolat- eral thoracotomies. Interventions: Paravertebral or interpleural administration of bupivacaine. Measurements and Main Results: Analgesia, as assessed by visual analog pain scores and patient-controlled mor- phine requirements, was similar in both groups. Postopera- tive spirometric values were significantly better at most times with the paravertebral route of administration. Dependent chest tube bupivacaine losses were approxi- mately four times higher in the interpleural group. Conclusion: Local anesthetic on the diaphragm might actively impair respiratory function through diaphragmatic and abdominal muscle weakness, while failing to contribute to pain relief. Copyright © 1998 by W.B. Saunders Company KEY WORDS: postoperative pain, thoracotomy surgery, bupi- vacaine nerve block, paravertebral block, interpleural analgesia I NSTILLATION OF local anesthetic posterior to the parietal pleura but anterior to the superior costotransverse ligament produces a paravertebral (extrapleural) block. Placed between the parietal and visceral pleurae, it can induce an interpleural block. In terms of preservation of postthoracotomy pulmonary function with a low side-effect profile, paravertebral administra- tion has recently been shown to be the superior option.a Because of the highly significant difference in pulmonary function between the two groups in that study, this prospective, random- ized assessment of chest tube loss of bupivacaine was initiated. The postulate was that interpleural administration might lead to higher dependent chest tube losses of local anesthetic because gravity markedly affects the distribution of solutions instilled into this space. 2 The dependent chest tube does not completely remove all the dependent chest fluid, and the presence of a high concentration of local anesthetic in the sump of fluid on the diaphragm could probably lead to active impairment of pulmo- nary function through diaphragmatic weakness. This might explain the significantly worse pulmonary function with inter- pleural analgesia compared with paravertebral analgesia found in a previous study.a METHODS With local institution ethics committee approval, 12 consecutive consenting adults aged between 17 and 70 years undergoing an elective posterolateral thoracotomy were studied. Exclusion criteria were sepsis in the chest cavity (empyema), bullous emphysema, previous or planned pleurectomy, known allergy to amide-type local anesthetics or nonsteroidal anti-inflammatory drugs (NSAIDs), contraindications to NSAIDs, psychiatric disease, or poor command of the English lan- guage. After an explanation of the use of the hand-held spirometer (Respira- dyne; Cheeseborough-Ponds Inc; Chicago, IL), 3 preoperative baseline From the Departments of Anesthetics and Thoracic Surgery, Brad- ford Royal lnfirmal?;, and the Department of Pharmaceutical Chemistry, University of Bradford, Bradford, England. Address reprint requests to Jonathan Richardson, MD, MRCP, FRCA, Department of Anesthetics, Bradford Royal Infirmary, Bradford BD9 6RJ, England. Copyright © 1998 by W.B. Saunders Company 1053-0770/98/1202-000858.00/0 pulmonary function test (PFT) measurements were obtained. These consisted of forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC). Linear visual analog pain scores, using a 10-cm line with 0 at one end representing no pain and 10 cm at the other representing the worst pain imaginable were explained, as was the use of the patient-controlled analgesia machine (PCA; Baxter, Newbury, Berkshire, England, UK). Premedication for all patients was morphine, 10 mg intramuscularly, and diclofenac, 100 mg rectally, 1 hour preoperatively. Randomization in the anesthetic room was by sequential allocation to computer-generated random numbers. Anesthesia was induced with propofol, fentanyl, and vecuronium and maintenance was with isoflurane in oxygen-enriched air in sufficient concentration to obtund cardiovascular responses. Patients in the paravertebral group had a preoperative percntaneous paravertebral injection using the method described by Kappis in reference 4. In patients in the interpleural group, the space was identified in the midscapular line by gradual advancement of a Tuohy needle until a "click" and free loss of resistance to saline was appreciated. In both groups, the dermatomal level of the injection T5 to T8 corresponded with the planned level of the incision and 20 mL of plain 0.5% bupivacaine was injected at least 10 minutes before the skin incision. A standard single posterolateral thoracotomy incision was performed between T5 and T8. Before chest closure, an epidural side-holed catheter was placed under direct vision either in the paravertebral space (in patients who had previously received a paravertebral block), using the method described by Richardson and Sabanathan, 4 or in the interplettral space alongside the vertebral column, with its tip at the intercostal level of the incision. During chest closure, another 20 mL of 0.25% bupivacaine was given. Apical and basal underwater-seal chest drains were inserted and left unclamped. All patients had an infusion of 0.5% plain bupivacaine at 0.1 mL/kg/hr, which was started approximately 1 hour after the end of surgery. As well as continuous oral or rectal diclofenac, 150 rag/day, patients had continuous access to PCA using morphine, l-rag bolus, with a 5-minute lockout period and no background infusion rate. The study period lasted for 48 hours postoperatively and data collection was performed by the ward nursing staff, who were unaware of the randomization group. Dependent chest tube bupivacaine losses were assessed at 24 and 48 hours by taking a sample from the mixed and measured pleurat fluid loss. Four-hourly pain scores were recorded at rest, as were opiate requirements, t2-hourly PFTs, and any untoward effects or complications. Pleural fluid bupivacaine losses were analyzed by liquid-liquid extraction and reversed-phase chromatography.5 Statistical analysis of pain and opiate usage was by Mann-Whitney U 166 Journal of Cardiothoracic and Vascular Anesthesia, Vo112, No 2 (April), 1998: pp 166-169
-
Upload
jonathan-richardson -
Category
Documents
-
view
219 -
download
0
Transcript of Pleural bupivacaine placement for optimal postthoracotomy pulmonary function: A prospective,...

Pleural Bupivacaine Placement for Optimal Postthoracotomy Pulmonary Function: A Prospective, Randomized Study
Jonathan Richardson, MD, MRCP, FRCA, Sabaratnam Sabanathan, MD, FRCS, Rajesh D. Shah, MS, FRCS, Brian J, Clarke, MSC, PhD, Surrindar Cheema, FRCA, and Alan J. Mearns, FRCS
Objective: To determine dependent chest tube losses of bupivacaine with paravertebral versus interpleural adminis- tration, thereby helping to explain the significant differences in pulmonary function that exist between these two techniques.
Design: A prospective, randomized study. Setting: A single hospital. Participants: Twelve adult patients undergoing posterolat-
eral thoracotomies. Interventions: Paravertebral or interpleural administration
of bupivacaine. Measurements and Main Results: Analgesia, as assessed
by visual analog pain scores and patient-controlled mor- phine requirements, was similar in both groups. Postopera-
tive spirometric values were significantly better at most times with the paravertebral route of administration. Dependent chest tube bupivacaine losses were approxi- mately four times higher in the interpleural group.
Conclusion: Local anesthetic on the diaphragm might actively impair respiratory function through diaphragmatic and abdominal muscle weakness, while failing to contribute to pain relief. Copyright © 1998 by W.B. Saunders Company
KEY WORDS: postoperative pain, thoracotomy surgery, bupi- vacaine nerve block, paravertebral block, interpleural analgesia
I NSTILLATION OF local anesthetic posterior to the parietal pleura but anterior to the superior costotransverse l igament
produces a paravertebral (extrapleural) block. Placed between
the parietal and visceral pleurae, it can induce an interpleural
block. In terms of preservation of post thoracotomy pulmonary function with a low side-effect profile, paravertebral administra-
tion has recently been shown to be the superior option.a Because
of the highly significant difference in pulmonary function be tween the two groups in that study, this prospective, random- ized assessment of chest tube loss of bupivacaine was initiated. The postulate was that interpleural administration might lead to higher dependent chest tube losses of local anesthetic because gravity markedly affects the distribution of solutions instilled into this space. 2 The dependent chest tube does not completely
remove all the dependent chest fluid, and the presence of a high concentration of local anesthetic in the sump of fluid on the
diaphragm could probably lead to active impairment of pulmo- nary function through diaphragmatic weakness. This might
explain the significantly worse pulmonary function with inter- pleural analgesia compared with paravertebral analgesia found
in a previous study.a
METHODS
With local institution ethics committee approval, 12 consecutive consenting adults aged between 17 and 70 years undergoing an elective posterolateral thoracotomy were studied. Exclusion criteria were sepsis in the chest cavity (empyema), bullous emphysema, previous or planned pleurectomy, known allergy to amide-type local anesthetics or nonsteroidal anti-inflammatory drugs (NSAIDs), contraindications to NSAIDs, psychiatric disease, or poor command of the English lan- guage.
After an explanation of the use of the hand-held spirometer (Respira- dyne; Cheeseborough-Ponds Inc; Chicago, IL), 3 preoperative baseline
From the Departments of Anesthetics and Thoracic Surgery, Brad- ford Royal lnfirmal?;, and the Department of Pharmaceutical Chemistry, University of Bradford, Bradford, England.
Address reprint requests to Jonathan Richardson, MD, MRCP, FRCA, Department of Anesthetics, Bradford Royal Infirmary, Bradford BD9 6R J, England.
Copyright © 1998 by W.B. Saunders Company 1053-0770/98/1202-000858.00/0
pulmonary function test (PFT) measurements were obtained. These consisted of forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC). Linear visual analog pain scores, using a 10-cm line with 0 at one end representing no pain and 10 cm at the other representing the worst pain imaginable were explained, as was the use of the patient-controlled analgesia machine (PCA; Baxter, Newbury, Berkshire, England, UK). Premedication for all patients was morphine, 10 mg intramuscularly, and diclofenac, 100 mg rectally, 1 hour preoperatively. Randomization in the anesthetic room was by sequential allocation to computer-generated random numbers.
Anesthesia was induced with propofol, fentanyl, and vecuronium and maintenance was with isoflurane in oxygen-enriched air in sufficient concentration to obtund cardiovascular responses. Patients in the paravertebral group had a preoperative percntaneous paravertebral injection using the method described by Kappis in reference 4. In patients in the interpleural group, the space was identified in the midscapular line by gradual advancement of a Tuohy needle until a "click" and free loss of resistance to saline was appreciated. In both groups, the dermatomal level of the injection T5 to T8 corresponded with the planned level of the incision and 20 mL of plain 0.5% bupivacaine was injected at least 10 minutes before the skin incision.
A standard single posterolateral thoracotomy incision was performed between T5 and T8. Before chest closure, an epidural side-holed catheter was placed under direct vision either in the paravertebral space (in patients who had previously received a paravertebral block), using the method described by Richardson and Sabanathan, 4 or in the interplettral space alongside the vertebral column, with its tip at the intercostal level of the incision. During chest closure, another 20 mL of 0.25% bupivacaine was given. Apical and basal underwater-seal chest drains were inserted and left unclamped.
All patients had an infusion of 0.5% plain bupivacaine at 0.1 mL/kg/hr, which was started approximately 1 hour after the end of surgery. As well as continuous oral or rectal diclofenac, 150 rag/day, patients had continuous access to PCA using morphine, l-rag bolus, with a 5-minute lockout period and no background infusion rate.
The study period lasted for 48 hours postoperatively and data collection was performed by the ward nursing staff, who were unaware of the randomization group. Dependent chest tube bupivacaine losses were assessed at 24 and 48 hours by taking a sample from the mixed and measured pleurat fluid loss. Four-hourly pain scores were recorded at rest, as were opiate requirements, t2-hourly PFTs, and any untoward effects or complications.
Pleural fluid bupivacaine losses were analyzed by liquid-liquid extraction and reversed-phase chromatography. 5
Statistical analysis of pain and opiate usage was by Mann-Whitney U
166 Journal of Cardiothoracic and Vascular Anesthesia, Vo112, No 2 (April), 1998: pp 166-169

PLEURAL BUPIVACAINE PLACEMENT FOR OPTIMAL POSTTHORACOTOMY PULMONARY FUNCTION 167
tests. PFT data analysis was by two-tailed independent t-tests for unequal variances.
RESULTS
Demographic details are listed in Table 1. There were no statistical differences in age, sex, weight, or type of surgery. One patient in the paravertebral group was withdrawn because of the postoperative omission of NSAID. Pain scores were similar in both groups of patients (Fig 1). Morphine require- ments were similar in both groups. In the first 24 hours, the interpleural group used a median of 41 mg (range, 29-150 mg) versus a paravertebral-group median of 48 mg (range, 16-56 mg). In the second 24 hours, the interpleural group used a median of 21 mg (range, 5-48 mg) versus a paravertebral-group median of 24 mg (range, 10-34 mg). PFTs, as a function of their preoperative value, were better in the paravertebral group than in the interpleural group, most differences being significant (Figs 2 and 3). Dependent chest tube fluid loss volumes were higher in the interpleural group, but this difference was not significant (Table 2). Almost the same amount of bupivacaine was bolused and infused in both groups of patients, but the pleural fluid bupivacaine loss was approximately four times higher in the interpleural group compared with the paravertebral group (Table 2). One patient in the interpleural group had a lobar collapse requiring intensive physiotherapy and one was temporarily confused.
DISCUSSION
After thoracotomy, a sump of fluid consisting of exudate and blood collects in the interpleural space dependent to the lower chest drain. With interpleural analgesia, the concentration of local anesthetic in this pool of fluid is much higher than with paravertebral administration, and this may be crucial in explain- ing the significantly worse PFTs using interpleural analgesia.
Interpleural instillation is known to result in marked gravita- tional pooling of injectate, even in the closed chest situation, ie, with an intact negative intrathoracic pressure. 2 After thora- cotomy, with an ensuing wide separation of the two layers of pleurae because of elimination of the negative intrathoracic pressure and a reduction in functional residual capacity of the operated lung, 6 it must be expected that gravitational pooling would be almost complete. Because these postoperative patients were routinely nursed in the sitting position, diaphragmatic function could have been actively impaired by bupivacaine, which is known to be avidly taken up by this muscle after
Table 1. Demographic and Surgical Data
Interpleural Paravertebral
Age (yr)
Mean 67 59
Range 62-74 45-76
Sex, M/F 5:1 4:1
Weight (kg) 67 71
SEM 4.3 6.8
Esophagogastrectomy 2 1
Antireflux procedure 2 2
Lobectomy 2 2
NOTE. All nonsignificant.
2.0
0 0
t- 1.5 0 .
O~ ..~ ~3 0 -~ 1.0
• ~ 0.5
0 . 0 ~ ,
4 8 12 16 20 24 28 32 36 40 44 48
H o u r s af ter s u r g e r y
Fig1. Mean pain scores at rest on a scale of 0 to 10 cm. The shaded boxes represent the paravertebral group and the open boxes repre- sent the interpleural group. There were no significant differences between the two groups (error bars have been omitted in the interests of visual clarity).
interpleural administration. 7 Blockade of the lower intercostal nerves leading to abdominal wall weakness may have occurred because of a similar mechanism. Bupivacaine in the dependent chest over the diaphragm cannot be expected to make any useful contribution to analgesia (skin incisions ranged from T5 to T8).
Containment of this fluid by intermittent clamping of the dependent chest tubes would not therefore be expected to improve analgesia or pulmonary function, and this has been found in previous studies, a,9 In this study, the chest tubes were left unclamped.
In many studies of interpleural analgesia, patients are kept supine for up to 20 minutes after a bolus of local anesthetic to facilitate its diffusion through the parietal pleura and innermost intercostal muscle or its membrane into the intercostal nerves. 2,s42 The authors used a postoperative continuous infu- sion regimen, which has been recommended in the interests of efficacy, 10,12-14 but which probably would require continuous
110
>= 100
go
80
~" 70
g 60 "fi 50
40 & 30
20- U
1 0 -
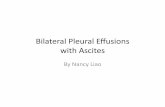
Post-operative FVC as a percentage of the pre-operative control
~> p<0 05
• Paravertebral [] Inter-pleural
i i i i
12 24 36 4 8
H o u r s a f t e r s u r g e r y
Fig 2. FVC as a percentage of the preoperative level for that patient. The shaded boxes represent the paravertebral group and the open boxes represent the interpleural group. Error bars represent two standard error of the mean (SEM); p < 0.05 at 12 and 36 hours.

168 RICHARDSON ET AL
120
.~ 110
100
o 90 & 80
70 g 60
== 50 40 30 20 ,,>, 10
0
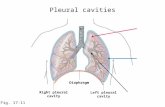
P o s t o p e r a t i v e F E V 1 a s a p e r c e n t a g e of the p r e o p e r a t i v e c o n t r o l
T ~. ~'~ two tailed
independent t test
• Paravertebral [] Inter-pleural
i i r i
0 12 24 36 48
H o u r s a f t e r s u r g e r y
Fig 3. FEV1 as a percentage of the preoperative level for that patient. The shaded boxes represent the paravertebral group and the open boxes represent the interpleural group. Error bars represent two standard error of the mean (SEM}; p < 0.05 at all time points.
assumption of the supine posture for the optimal analgesic effect. Because of the expectation of markedly impaired pulmo- nary mechanics with this maneuver, 6 its consideration was rejected.
Two patients in the interpleural group had complications related to their analgesic regimen. One patient had an episode of confusion that was resolved by temporary cessation of the infusion and was possibly because of bupivacaine toxicity. Another patient had a lobar collapse resulting from and contributing to poor pulmonary function. Because of the small numbers of patients in this study, statistical analysis was not attempted, but similar complications were found in the authors' previously published study.1
Paravertebral administration is very much less gravity depen- dent because solutions are contained by the overlying parietal pleura. They remain confined but well distributed within adjacent paravettebral spaces, in direct proximity to the intercos- tal nerve roots, their posterior primary rami, and the sympa- thetic chain. 4
It is possible that phrenic nerve impairment may also help to explain the differences in PFTs. Interpleural local anesthetics
Table 2. Bupivacaine Kinetics
Interpleural Paravertebral (n = 6) (n = 5)
Fluid loss in f irst 24 hr (mL) 625 +- 109" 416 -+ 73*
Fluid loss in second 24 hr (mL) 683 -+ 101" 466 ± 201"
Bupivacaine bolused and infused in
f irst 24 hr (mg) 293 ± 25.7* 299.6 _+ 34.2*
Bupivacaine infused in second 24 hr
(mg) 160 ± 10.6" 169 _+ 16.6"
Loss of bupivacaine in f irst 24 hr
(mg) 48 + 9f 10 -+ 4.91- Loss of bupivacaine in second 24 hr
(mg) 44 -- 4.55 9 ± 45
NOTE. All values are expressed as mean _+ SEM.
*Not significant.
t p = 0.017.
5p - 0.03.
have been found to attenuate or obliterate the phrenic nerve electromyogram in seven of nine dogs studied, 15 and at least one case report of phrenic nerve paralysis in humans has been reported. 16 This complication is not known with paravertebral analgesia. 4
It is not believed that differences in pulmonary function were because of losses of bupivacaine to analgesia through higher chest tube losses in the interpleural group because pain scores were similar in both groups.
It is concluded that interpleural analgesia leads to higher concentrations of local anesthetic in the dependent interpleural space than with paravertebral analgesia. Local anesthetic on the diaphragm can make no useful contribution ot postthoracotomy analgesia and might actively impair respiratory function through diaphragmatic and abdominal muscle weakness. Although the number of patients in this study was small, these results confirmed the findings of our previous study and helped to explain the significant differences in postoperative pulmonary function between these two techniques.
A C K N O W L E D G M E N T
The authors thank Consultant Anaesthetists Jane Bembridge, Carolyn Evans, Mark Fairbrass, and John Keeler for their kind cooperation, and Sister Bennett and ward 21 nursing staff for their data collection.
REFERENCES
1. Richardson J, Sabanathan S, Mearns AJ, et al: A prospective, randomised comparison of intrapleural and paravertebral analgesia in thoracic surgery. Br J Anaesth 75:405-408, 1995
2. Strcmskag KE, Hange O, Steen PA: Distribution of local anaesthet- ics injected into the interpleural space, studied by computerized tomography. Acta Anaesthesiol Scand 34:323-326, 1990
3. Jenkins SC, Barnes NC, Moxiham J: Evaluation of a hand-held spirometer, the Respiradyne, for the measurement of forced expiratory volume in the first second (FEV1), forced vital capacity (FVC) and peak expiratory flow rates (PEFR). Br J Chest Dis 49:70-75, 1988
4. Richardson J, Sabanathan S: Thoracic paravertebrai analgesia. A review. Acta Anaesthesiol Scand 39:1005-1015, 1995
5. Clark B J, Hamdi A, Berrisford RG, et al: Reversed-phase and high-performance liquid chromatographic assay of bupivacaine and its enantiomers after continuous extrapleural infusion. J Chromatog 553: 383-390, 1991
6. Sabanathan S, Eng J, Mearns AJ: Alterations in respiratory mechanics following thoracotomy. J R Col Surg Edinb 35:144-150, 1990
7. StrCmskag KE, Minor BG, Post C: Distribution of bupivacaine after interpleural injection in rats. Reg Anesth 16:43-47, 1991
8. Mann LJ, Young GR, Williams JK, et al: Intrapleural bupivacaine in the control of postthoracotomy pain. Ann Thorac Surg 53:449-454, 1992
9. Ferrante FM, Chart VWS, Arthur GR, et aI: Interpleural analgesia after thoracotomy. Anesth Analg 72:105-109, 1991
10. Raffin L, Fletcher D, Sperandio M, et al: Interpleural infusion of 2% lidocaine with 1:200,000 epinephrine for postthoracotomy analge- sia. AnesthAnalg 79:328-334, 1994
11. Kambam JR, Hammon J, Parris WCV, et al: Intrapleural analgesia for postthoracotomy pain and blood levels of bupivacaine following intrapleural injection. Can J Anaesth 36:106-109, 1989

PLEURAL BUPIVACAINE PLACEMENT FOR OPTIMAL POSTTHORACOTOMY PULMONARY FUNCTION 169
12. McIlvane WB, Knox RF, Fennessey PV, et al: Continuous infusion of bupivacaine via intrapleural catheter for analgesia after thoracotomy in children. Anesthesiology 69:261-264, 1988
13. Rosenberg PH, Scheinin BM-A, Lep~intalo MJA, et al: Continu- ous intrapleural infusion of bupivacalne for analgesia after thoracotomy. Anesthesiology 67:811-813, 1987
14. Brockmeier V, Moen H, Karlsson BR, et al: Interpteural or
thoracic epidural analgesia for pain after thoracotomy. A double-blind study. Acta Anesthesioi Scand 38:317-321, 1993
15. Kowalski SE, Bradley BD, Greengrass RA, et al: Effects of interpleural bupivacaine (0.5%) on canine diaphragmatic function. Anesth Analg 75:400-404, 1992
16. Lander GR: Interpleural analgesia and phrenic nerve paralysis. Anaesthesia 48:315-316, 1993