Plaque stabilization: A mechanism for the beneficial effect of lipid-lowering therapies in...
14
Progress in Cardiovascular Diseases VOL XXXVII, NO 3 NOVEMBER/DECEMBER 1994 Plaque Stabilization: A Mechanism for the Beneficial Effect of Lipid-Lowering Therapies in Angiography Studies David Waters E XCESSIVELY high levels of serum choles- terol, especially the low-density lipopro- tein (LDL) fraction, have been shown conclu- sively to be a primary risk factor for atherosclerotic vascular disease. The relation- ship between cholesterol and atherosclerotic coronary heart disease (CHD) is regarded as causal and, in the opinion of some authorities, is decisive? Moreover, there is evidence that asser- tive intervention to reduce serum total and LDL cholesterol, ideally in association with an in- crease in the high-density lipoprotein (HDL) fraction, is associated with a very substantial reduction in morbidity, is attributable to CHD, and may reduce mortality in specific circum- stances. This conclusion is a centerpiece of various national and supranational initiatives to reduce the numbers of people killed per annum by atherosclerotic disease. 2-4 Early clinical trials of lipid-lowering interven- tions dealt with the effect on clinical outcomes. In more recent years, however, there has been a movement toward studies based on quantitative angiography. Various pragmatic reasons have been identified for this trend, 5,6 including the ability to generate statistically robust data from relatively small numbers of patients in a relatively short period of time.7 The rationale underlying these studies may be summarized as follows: (1) raised cholesterol causes atheroscle- rosis; (2) progression of atherosclerosis causes clinical CHD events now and increases the risk for such events in the future; (3) halting progres- sion of atherosclerosis is a surrogate for prevent- ing CHD events; and (4) if elevated serum cholesterol causes CHD by promoting the growth of atheromatous plaques, it ought to be possible to show that lowering serum choles- terol levels halts the growth of plaques and may lead to a reduction in their size, so-called regres- sion. Implicit in this hypothesis is the belief that the likelihood of a plaque giving rise to clinical CHD is proportional to the size of the plaque. Recent developments in histology, micros- copy, and pathology have initiated a reappraisal of the relationship between plaque size, vessel occlusion, and CHD and, in doing so, have permitted a reinterpretation of the results of angiography studies. This reappraisal has con- firmed and strengthened the link between high levels of cholesterol and CHD and has shown more of the mechanisms by which lipid-lower- ing therapies may exert their beneficial effects. As a result, emphasis has shifted away from the original notion of regression, perceived as an improvement of luminal narrowing caused by a plaque, towards the concept of stabilization, which is envisaged as the consolidation of a subgroup of small- or medium-sized lipid-rich plaques that act as loci for the occlusive athero- thrombotic events of clinical CHD. ANGIOGRAPHY STUDIES Numerous angiography studies have been conducted, not all of which satisfy the criteria relevant to a discussion of plaque stabilization. These criteria are that (1) the coronary vascula- ture should be the object of the study; (2) serial From the Division of Cardiology, Hartford Hospital and the University of Connecticut School of Medicine, Hartford, CT. Address reprint requests to David Waters, MD, Director of Cardiology, Division of Cardiology, Hartford Hospital, 70 Seymour St, Hartford, CT 06102. Copyright 1994 by W.B. Saunders Company 0033-0620/94/3703-000155.00/0 Progress in Cardiovascular Diseases, Vol XXXVlI, No 3 (November/December), 1994: pp 107-120 107
-
Upload
david-waters -
Category
Documents
-
view
212 -
download
0
Transcript of Plaque stabilization: A mechanism for the beneficial effect of lipid-lowering therapies in...

Progress in
Cardiovascular Diseases VOL XXXVII, NO 3 NOVEMBER/DECEMBER 1994
Plaque Stabilization: A Mechanism for the Beneficial Effect of Lipid-Lowering Therapies in Angiography Studies
David Waters
E XCESSIVELY high levels of serum choles- terol, especially the low-density lipopro-
tein (LDL) fraction, have been shown conclu- sively to be a primary risk factor for atherosclerotic vascular disease. The relation- ship between cholesterol and atherosclerotic coronary heart disease (CHD) is regarded as causal and, in the opinion of some authorities, is decisive? Moreover, there is evidence that asser- tive intervention to reduce serum total and LDL cholesterol, ideally in association with an in- crease in the high-density lipoprotein (HDL) fraction, is associated with a very substantial reduction in morbidity, is attributable to CHD, and may reduce mortality in specific circum- stances. This conclusion is a centerpiece of various national and supranational initiatives to reduce the numbers of people killed per annum by atherosclerotic disease. 2-4
Early clinical trials of lipid-lowering interven- tions dealt with the effect on clinical outcomes. In more recent years, however, there has been a movement toward studies based on quantitative angiography. Various pragmatic reasons have been identified for this trend, 5,6 including the ability to generate statistically robust data from relatively small numbers of patients in a relatively short period of time. 7 The rationale underlying these studies may be summarized as follows: (1) raised cholesterol causes atheroscle- rosis; (2) progression of atherosclerosis causes clinical CHD events now and increases the risk for such events in the future; (3) halting progres- sion of atherosclerosis is a surrogate for prevent- ing CHD events; and (4) if elevated serum cholesterol causes CHD by promoting the growth of atheromatous plaques, it ought to be possible to show that lowering serum choles-
terol levels halts the growth of plaques and may lead to a reduction in their size, so-called regres- sion. Implicit in this hypothesis is the belief that the likelihood of a plaque giving rise to clinical CHD is proportional to the size of the plaque.
Recent developments in histology, micros- copy, and pathology have initiated a reappraisal of the relationship between plaque size, vessel occlusion, and CHD and, in doing so, have permitted a reinterpretation of the results of angiography studies. This reappraisal has con- firmed and strengthened the link between high levels of cholesterol and CHD and has shown more of the mechanisms by which lipid-lower- ing therapies may exert their beneficial effects. As a result, emphasis has shifted away from the original notion of regression, perceived as an improvement of luminal narrowing caused by a plaque, towards the concept of stabilization, which is envisaged as the consolidation of a subgroup of small- or medium-sized lipid-rich plaques that act as loci for the occlusive athero- thrombotic events of clinical CHD.
ANGIOGRAPHY STUDIES
Numerous angiography studies have been conducted, not all of which satisfy the criteria relevant to a discussion of plaque stabilization. These criteria are that (1) the coronary vascula- ture should be the object of the study; (2) serial
From the Division of Cardiology, Hartford Hospital and the University of Connecticut School of Medicine, Hartford, CT.
Address reprint requests to David Waters, MD, Director of Cardiology, Division of Cardiology, Hartford Hospital, 70 Seymour St, Hartford, CT 06102.
Copyright �9 1994 by W.B. Saunders Company 0033-0620/94/3703-000155.00/0
Progress in Cardiovascular Diseases, Vol XXXVlI, No 3 (November/December), 1994: pp 107-120 107

108 DAVID WATERS
Table 1. Entry Requirements, Treatment Regimens, and Lipid Responses to Treatment in Nine Angiography Studies
Eligibility Treatment LDL Response HDL Response Follow-Up Study Criteria Regimen (%)* (%) (yr)
NHLBI 8 CAD, LDL E + R -31 +8 5 CLAS 19 CAB D + R + N -43 +37 2 CLAS II 1~ CAB D + P + N -40 +37 4 POSCH ~ MI, CHOL >5.7 mmol/L D + PIB + R -42 +5 9.71" FATS (N + C) s CAD, Apo B D + R + N -32 +43 2.5 FATS (L + C) s CAD, Apo B D + R + L -46 +15 2.5 SCOR 12 FH D + R + N -+ L -39 +25 2 STARS (D only) 13 CAD, CHOL > 6 mmol/L D -16 0 3 STARS (D + R) ~3 CAD, CHOL > 6 mmol/L D + R 36 - 4 3 Ornish et al TM CAD V + M + E -37 - 3 1 SCRIP TM CAD D + (R/N/L/F) + E, BP -21 +13 4 Heidelberg~ CAD D + E - 8 +3 1 MARS ~7 CAD D + L -38 +8.5 2.2 CCAIT TM CAD, CHOL 5.7-7,8 mmol/L D + L -29 +7.3 2
Abbreviations: CAB, coronary artery bypass graft; CHOL, serum total cholesterol; LDL, LDL cholesterol greater than the 90th percentile; Apo B, apolipoprotein B greater than 125 mg/dL; FH, familial hypercholesterolemia; D, diet; V, vegetarian diet; R, bile acid sequestrant (resin); L, Iovastatin; N, nicotinic acid; F, fibrate-type drugs; PIB, partial ileal bypass; M, mediation techniques; E, exercise program; BP, blood pressure therapy.
*Mean LDL response to control therapy was -7%. tFollow-up has been extended beyond the formal conclusion of this study. Modified and reprinted with permission. 2~ @ Copyright 1993 American Heart Association.
angiography should be used; (3) the study must incorporate a suitable control group; and (4) the lipid-modifying therapy must effect a favor- able alteration in the serum lipid profile (princi- pally, a reduction in LDL cholesterol accompa- nied, ideally, by a decrease in triglyceride and an increase in HDL cholesterol).
Eleven studies meet these requirements: the National Heart, Lung, and Blood Institute type II trial (NHLBI); s the Cholesterol-Lowering Atherosclerosis Study (CLAS; including the extended follow-up designated CLAS-II); 9,t~ the Program on the Surgical Control of the Hyper- lipidemias (POSCH); 1] the Familial Atheroscle- rosis Treatment Study (FATS); 4 the San Fran- cisco Arteriosclerosis Specialized Center of Research (SCOR) study; ]2 the St. Thomas' Atherosclerosis Regression Study (STARS); ~3 the Lifestyle Heart Trial; 14 the Stanford Coro- nary Risk Intervention Project (SCRIP); 15 the Heidelberg study; 16 the Monitored Atheroscle- rosis Regression Study (MARS); 17 and the Ca- nadian Coronary Atherosclerosis Intervention Trial (CCAIT). is It is instructive to review these trials briefly (see Tables I and 2).
The NHLBI study involved 143 men with coronary artery disease (CAD) and LDL choles- terol in the uppermost 10% of the populationdis- tribution. Five years of therapy with a lipid- lowering diet plus the bile acid sequestrant,
cholestyramine (target dose, 24 g/d), was associ- ated with a 28% reduction in LDL cholesterol (P < .001 v placebo-treated controls). Definite plus probable CAD progressed in 49% of pa-
Table 2. Angiographic and Clinical Outcomes in Nine Angiography Studies
Study
Control Patients Treated Patients Event
Progres- Regres- Progrea- Regres- Reduction sion (%) sion (%) sion (%) sion(%) (%)*
NHLBI 8 49 7 32 7 33 CLASP 61 2 39 16 25 CLAS II l~ 83 6 30 18 43 POSCH 11 65 6 37 14 351" FATS (N + C) 5 46 11 25 39 80$ FATS (L + C) 5 22 32 70 SCOR 12 41 13 20 33 1 v 05 STARS
(D only) 13 15 38 691" 46 4
STARS (D + R) 13 12 33 89
Ornish et al TM 32 32 14 41 0 v I t SCRIP rs NA 10 NA 21 50 Heidelberg TM 42 4 20 30 27 MARS 17 41 12 29 23 24 CCAIT TM 50 7 33 1 O 25
*The nature of the clinical events recorded varies from study to study (see original reports for details).
tStudies in which the reduction in clinical events was statisti- cally significant by the criteria adopted for that study.
:~Results expressed as number of events rather than as a percentage because the total number of events was very small. Data are presented in the order "control group v treated group."
Modified and reprinted with permission. 21 �9 Copyright 1993 American Heart Association.

LIPID LOWERING AND PLAQUE STABILIZATION 109
tients in the placebo group and in 32% of the treated patients (P < .05). Increases in HDL cholesterol during therapy also correlated with a reduced progression of coronary atheroma.
CLAS studied 162 nonsmoking men (aged 40 to 59 years) who had undergone coronary artery bypass grafting. After baseline angiographic assessment by an expert panel, patients were randomized to diet therapy plus placebo or to diet plus colestipol and nicotinic acid for 2 years. Repeat angiograms were undertaken at the conclusion of the study. Lipid-lowering therapy was associated with a 26% reduction in plasma total cholesterol, a 43% reduction in LDL cholesterol, and a 37% increase in HDL cholesterol. These changes in lipid profile were accompanied by angiographic evidence of slowed progression of established disease in both native and grafted vessels. A small degree of regres- sion of atheroma was recorded in 16.2% of treated patients compared with 3.6% of pa- tients in the placebo group (P < .007). Four- year follow-up data on 113 patients involved in CLAS have subsequently been published (CLAS-II). These data confirm that the lipid response to drug therapy is sustained over the longer term and is associated with continued favorable effects on coronary atherosclerosis.
POSCH is the most extensive angiographic study of nonpharmacologic intervention against serum lipids. Nearly 900 survivors of a first myocardial infarction (MI) were randomized to either partial ileal bypass surgery or diet therapy. At the 5-year follow-up, serum total cholesterol in the surgery group was 23.3% lower than that in the control group (P < .0001), and LDL cholesterol was 37.7% lower (P < .001). A small, but significant (4.7%, P < .02), increase in HDL cholesterol was also observed. Compari- son of baseline angiograms with those taken at 3, 5, 7, and 10 years of follow-up confirmed that surgery was consistently associated with re- duced progression of coronary atheroma (P < .001). In addition, lipid-lowering surgery was associated with a statistically significant reduc- tion in the combined clinical end points of death caused by CHD and of confirmed nonfatal MI (125 events v 82 events; P < .001) and was also associated with a large reduction in the number of coronary bypass procedures (52 v 137; P < .0001). The POSCH investigators also reported reductions in overall mortality and deaths from
CHD in the surgery group. These reductions were not statistically significant at that time; however, patient follow-up and analysis are continuing, and the difference between the two groups of patients is now approaching signifi- cance at the 5% level.
In FATS, angiographically measured changes in coronary artery stenosis were related to clinical events. A total of 146 men with estab- lished CAD, familial history of coronary dis- ease, and serum apolipoprotein B in excess of 125 mg/dL were enrolled in this study and randomized to diet therapy plus placebo (or low-dose colestipol, for ethical reasons), to colestipol (30 g three times per day) and the reductase inhibitor lovastatin (20 to 40 mg, twice per day), or to colestipol (30 g three times per day) and nicotinic acid (4 g four times per day). Quantitative angiography conducted be- fore and at the conclusion of the 2.5-year trial established that both treatment regimens re- tarded the progression of atheromatous lesions; the overall change was in the direction of regression, with minimum lumen diameter in- creasing in both treatment groups but decreas- ing in the placebo group (P < .01). These favorable angiographic findings were accompa- nied by reductions in the number of clinical coronary events in both treatment groups.
STARS evaluated the impact of a lipid- lowering diet, alone or in combination with cholestyramine (8 g twice per day), on coronary atherosclerosis in 90 men with established CHD. Patients were assigned to usual therapy (U), diet therapy (D), or diet plus cholestyramine (D+C). Seventy-four patients completed the study (U, 24; D, 26; D+C, 24). Baseline lipid and lipoprotein parameters were very similar in all three groups. In the U group, little variation in lipids or lipoproteins occurred during the trial; net progression of atherosclerosis was recorded in this group.
In patients assigned to diet therapy, total cholesterol decreased by 14.2% and LDL choles- terol by 16.2% (bothP < .001). The correspond- ing reductions in the D+C group were 25.3% and 35.7%, respectively, (also both P < .001). Substantial reductions in the LDL:HDL ratio were recorded in both treatment groups (D, 17.6% and D+C, 34.6%; bothP < .001). These changes in lipid and lipoprotein profiles were accompanied by angiographic evidence of over-

110 DAVID WATERS
all regression of coronary disease in both treat- ment groups.
Women are underrepresented in angio- graphic studies, as is the case with clinical trials in general. The SCOR trial is an exception to this rule; 41 of the 72 patients involved were women. All participants had heterozygous famil- ial hypercholesterolemia and angiographic evi- dence of coronary atherosclerosis. Over the course of 2 years, lipid-lowering therapy consist- ing of a recommended diet plus colestipol, nicotinic acid, and (in some cases) lovastatin resulted in highly statistically significant reduc- tions in total and LDL cholesterol (both P < .01) and in significant increments in HDL cho- lesterol (P < .01). These changes were associ- ated with a mean change of -1.53 in the percentage of area stenosis; the mean change in percentage of area stenosis among controls was +0.80 (P < .039; two-tailed test). A separate analysis of the results for women showed that the mean percentage of change in area stenosis was -2.06 (P < .05).
Ornish et a114 have reported success in the use of lifestyle changes to reverse CAD in patients with existing atheromatous plaques. Over the course of 1 year, intensive efforts at smoking cessation, regular structured exercise protocols, strict lipid-lowering diets, and stress manage- ment resulted in regression of existing lesions in 18 of 22 patients.
In SCRIP, a 4-year program of risk reduction directed at hyperlipidemia, hypertension, ciga- rette smoking, and obesity was associated with favorable alterations in serum lipid profile, retardation of atherosclerosis progression, and a reduction in the number of cardiac events in 145 patients aged 75 years or less.
The Heidelberg study (n = 113) has reported retardation of atherosclerosis progression in response to rigorous dietary control plus a program of regular physical exercise.
MARS, one of the most recent of these angiography studies to be completed, examined the impact of monotherapy with the hepatic hydroxymethyl glutaryl coenzyme A reductase inhibitor, lovastatin (40 mg twice a day), on coronary atherosclerosis in patients with angio- graphic evidence of disease in at least two segments including at least one segment with a minimum 50% diameter stenosis. A total of 270
patients aged less than 70 years were enrolled in the 2-year, placebo-controlled trial; two-thirds of patients had total cholesterol less than 240 mg/dL (6.2 mmol/L).
The overall change in percent diameter steno- sis, measured by quantitative coronary angiogra- phy, was similar in both groups (lovastatin, +1.6% _+ 6.7%; placebo, +2.2% -+ 6.8%; P > .20), but lovastatin was associated with a reduc- tion in percent diameter stenosis in lesions greater than 50% at baseline (-4.1% _+ 11.0%). This reduction was statistically significant com- pared with the increase of +0.9% _+ 11.0% observed in the placebo group (P < .01). Lovastatin therapy was also accompanied by increased minimum lumen diameter (+0.13 mm _+ 0.35 mm) in lesions greater than 50% at baseline, whereas progressive reduction in lu- men occurred this category of lesions in the placebo group (-0.04 mm + 0.36 mm; P < .01). Comparison of the secondary end point of global changes score provided evidence of signifi- cantly less progression of CAD in patients treated with lovastatin (+0.41 _+ 1.14 v +0.88 _+ 1.12 in placebo group; P < .01). These angio- graphic responses to lovastatin therapy were accompanied by the expected large reductions in total cholesterol (-32%), LDL cholesterol (-45%), and apolipoprotein B (-26%) and by a modest increase in HDL cholesterol (+8.5%).
kovastatin monotherapy (in conjunction with diet) was also the intervention used in the latest of these 11 studies, CCAIT. The 331 enrolled patients, aged 21 to 70 years, were selected on the basis of diffuse but not necessarily severe coronary atherosclerosis accompanied by serum total cholesterol in the range 220 to 300 mg/dL (5.7 to 7.8 mmol/L).A total of 165 patients was assigned to diet plus lovastatin, and 166 patients were allocated to diet plus placebo. Lovastatin dosage was titrated against LDL cholesterol during the first 16 weeks of the trial with the objective of achieving LDL cholesterol less than 130 mg/dL (3.4. mmol/L).
The primary angiographic end point in CCAIT was a coronary change score (expressed in millimeters) that represented the net difference between minimum lumen diameter at baseline and after 2 years. Secondary end points in- cluded proportion of patients showing progres- sion only, regression only, and appearance of

LIPID LOWERING AND PLAQUE STABILIZATION 111
new lesions. Progression and regression were defined as widening or narrowing of at least 0.4 mm, and a new lesion was defined as one that was not apparent at baseline or that caused no more than 25% diameter stenosis, which nar- rowed by at least 0.4 mm during the study.
Mean lovastatin dosage during the trial was 36 rag/d; this was associated with a mean reduction of 29% _+ 11% in LDL cholesterol (P < .001). Owing to the dose titration protocol adopted for CCAIT, the mean dose consumed by patients with baseline LDL cholesterol greater than the group median of 176 mg/dL (4.6 mmol/L) was greater than that taken by patients with baseline LDL cholesterol less than the median (43 mg/d v 28 mg/d).
Mean coronary change score in the Iovastatin group was -0.05 mm _+ 0.13 mm, compared with -0.09 mm + 0.16 mm in the placebo group (P < .01). Subgroup analysis showed that this overall benefit was attributable to a reduced rate of progression among lesions causing steno- sis of less than 50% at baseline (-0.06 mm _+ 0.14 mm v -0.11 mm _+ 0.18 mm; P < .014). No significant difference in coronary change scores was registered in lesions causing more than 50% stenosis at baseline.
Progression only was a significantly less fre- quent outcome in patients treated with lova- statin (33% v 50%; P < .03), but the proportion of patients showing regression only was similar in both groups (lovastatin ,10%; placebo, 7%; no significant difference). One or more new lesions developed in 23 of 146 patients treated with lovastatin compared with 49 of 153 patients in the placebo group (P = .001). New total occlusions were recorded in 10% of patients in the lovastatin group and in 12% of patients assigned to placebo (difference not significant).
Multiple variable regression analysis estab- lished that better coronary change scores were associated with higher baseline LDL choles- terol level, wider baseline minimum lumen diam- eters, lovastatin therapy, greater numbers of lesions causing more than 25% stenosis at baseline, and hypertension. Cigarette smoking emerged as a major determinant of a worse coronary change score.
Two patients in each group of the CCAIT died during the study; both deaths in the lova- statin group and 1 death in the placebo group
were classified as cardiac deaths (the fourth patient died in an air accident). In addition, there were five episodes of M] in the lovastatin group and 8 episodes of unstable angina. A total of 6 episodes of MI and 13 episodes of unstable angina occurred in the placebo group. The differences in event rates were not statistically significant.
In the CCAIT, most lesions examined caused less than 50% diameter stenosis at baseline, and most instances of progression occurred in le- sions of these modest baseline dimensions (pro- gression was shown in only 14 of 339 lesions rated as causing more than 50% stenosis at baseline). Even among the smaller lesions, the overall rate of progression was low; 59 of 865 lesions progressed in the lovastatin group (6.8%), and 108 of 965 lesions progressed in the placebo group (11.2%; P = .005 between groups). Prescription of alternate-day aspirin (325 rag) to all patients enrolled in CCAIT has been nominated as a possible explanation for the lack of progression among larger lesions. 18 The natural history of atherosclerosis as shown in this study (ie, the apparent dormancy of many atherosclerotic lesions with substantial alter- ations [either progression of regression] occur- ring in only a small proportion of lesions, the concentration of progression among lesions of small to intermediate size, and the postulated involvement of platelets in progression of some lesions) is pertinent to the debate about plaque stabilization and will be considered in greater detail later in this review.
A NEW PERSPECTIVE ON ANGIOGRAPHY
Formal meta-analysis of these trials is hin- dered by differences in methodology and defini- tion of outcome. Moreover, as critics have noted, 19,2~ angiography is not without its deficien- cies and should be regarded as the best avail- able technique for evaluating coronary athero- sclerosis, not the best per se. (Proposals have been made that, if adopted generally, would help optimize the reliability, reproducibility, and variability of angiographic data. 7) However, what these studies may lack in homogeneity, they make up for in consistency. Regardless of the intervention used, lipid lowering was associ- ated with a lesser degree of progression of atherosclerosis and a greater propensity to

112 D A V I D W A T E R S
plaque shrinkage. Moreover, this trend was associated with statistically significant reduc- tions in the number of clinical CHD events (howsoever defined) in several trials in which elevated cholesterol or lipoprotein cholesterol was an entry criterion (FATS, POSCH, and STARS).
Therefore, in the aggregate, the results of these trials support the proposition that lipid- lowering therapy will prevent, delay, or even reverse (partially) the development of athero- sclerotic lesions. However, as Brown et a121 have pointed out, the clinical impact of lipid-lower- ing therapies in some of these trials has been out of all proportion to the effect on plaque size. In FATS, for instance, only 12% of lesions were deemed to have undergone regression in re- sponse to therapy, and the average difference in lumen diameter between actively treated pa- tients and controls was less than 0.1 ram. These trifling changes were nevertheless associated with a 70% to 80% reduction in cardiovascular events.5,21 In seeking to explain this apparent paradox, stress needs to be laid on the average- ness of the angiographic changes reported. The greater majority of plaques, probably in the region of 90%, do not change in response to lipid-lowering therapy. However, those that do change change quite a lot, probably enough to explain the reduction in clinical events.
Two additional observations from FATS are informative. First, aggressive lipid-lowering therapy had little influence on the progression of severely stenotic lesions (ie, those causing 70% to 90% stenosis at baseline), but decreased several-fold the likelihood of progression of smaller lesions (Fig 1). Second, 8 of 9 clinical events to occur in the control group of FATS were related to the progression of lesions desig- nated mild or moderate in extent at baseline (Fig 2). Conversely, only I of 4 clinical events in the actively treated groups was associated with such a lesion (Fig 2). These data are supple- mented by findings from another angiographic study in which it was reported that severely stenotic lesions were more likely than smaller plaques to progress to complete occlusion of the vessel but less likely to cause MI. 22 Taeymans et al, 23 in a small retrospective study, have con- firmed that lesions at high risk for occlusion are relatively modest proportions (causing approxi-
25%-
% of 20%- Lesions that 15O/o - Progress (_> 10%S) 10%-
5%-
Progression
:-,#i CONV N N I L+C I I N+C
NI 10-40%' 40-70% ' 70-98% (785) (312) (52)
Regression
% of Lesions that Regress (< -10%S
(785) (312) (100)
Baseline Stenosis Severity (% Stenosis)
Fig 1. The effect of lipid-lowering therapy in the FATS trial on progression and regression of lesions is shown according to percent baseline stenosis. Intensive lipid-lowering therapy substantially reduces the likelihood of progression of mild or moderate lesions but has little effect on the progression of lesions classified as severe at baseline. * P < .05; +P < .02;
** P < .005; ++P < .001 (versus conventional [CONV] group); see text for further details. (Adapted and reprinted with permissionY 1 [Circulation.] Copyright 1993 American Heart Association.)
mately 50% stenosis at the last pre-event angio- gram). These researchers also reported that lesions that progressed to occlusion were more likely to be located at sites of flow division and to be steeply angled, 23 findings that reaffirm the influence of high shear stresses in plaque rup- ture and thrombotic occlusion.
PLAQUE RUPTURE AND THROMBOSIS
These observations are compatible with the linked hypotheses that unstable angina, acute MI, and ischemic sudden death are the result of abrupt progression of small or moderately sized

LIPID LOWERING AND PLAQUE STABILIZATION 113
CAD Progression to Events
Fig 2. Clinical events in FATS are shown according to baseline status of causal lesions. Eight of the nine clinical events recorded in the control group (n = 46) were associated with progres- sion of lesions that caused mild or moderate stenosis at base- line. Only one of four events in the two treatment groups (n = 59) was attributable to progres- sion of such a lesion. Numbers in lower left corner of each box indicate the total number of le- sions of each type at baseline. Abbreviations: d, death; m, MI; p, progressive angina; u, un- stable angina; N+C, nicotinic acid plus colestipol; N+L, nico- tinic acid plus Iovastatin; CONV, conventional therapy (control group); %S, percent diameter stenosis. See text for further de- tails. (Adapted and reprinted with permissionY 1 [Circulation.] Copy- right 1993 American Heart Asso- ciation.)
N + C
L + C
CONV
n=27
32
Mild Moderate Severe
235 103 18 , , , , ,
2 3 7 108 18 e - ' (
i --4 . [ ] ni- ,-pa
hi---,, . O]
53 313 101 ~ 16
10 40 70 100 Stenosis Severity
(Baseline-- Event)(%S)
m .
B-
plaques, and that the value of lipid-lowering therapy as shown in angiographic trials lies in its ability to stabilize a subpopulation of lipid-rich plaques which have a propensity to rupture and which, once ruptured, become sites for the propagation of thrombi that create critical steno- sis or total occlusion of the affected vessel.
Plaque rupture with subsequent thrombosis as a critical factor in the genesis of acute coronary syndromes is a well-established con- cept. Results of recent studies indicate that rapidly evolving atherothrombotic lesions are the rule rather than the exception in patients who suffer fatal coronary events and have pro- vided more detailed information on the factors that dispose towards plaque rupture. 21,24,25
CHARACTERISTICS OF CRITICAL CORONARY PLAQUES
Atherothrombotic occlusion of a coronary vessel is most frequently the result of deep tears in the fibrous cap of the atherosclerotic plaque 26 and of the resultant exposure of platelets to proaggregatory factors such as collagen, ne- crotic debris, yon Willebrand factor, and throm-
boxanes. Small- to medium-sized plaques with the potential for such abrupt, deep fissuring are characterized by21.27-29: (1) a core of extracellu- lar lipid, perhaps including crystalline choles- terol, that occupies more than 40% of the plaque volume; (2) a relative paucity of connec- tive tissue in the fibrous cap overlying the lipid pool; (3) a relative paucity of smooth muscle cells in the fibrous cap overlying the centre of the lipid pool and an excess of lipid-filled macrophages in the same region; and (4) an eccentric position around the lumen of the vessel.
The physical frailties of such a plaque are evident. The substantial lipid pool, which is believed to be semiliquid at body temperature, is highly susceptible to deforming pressures that the weak fibrous cap is ill-suited to resist. The points of insertion of the fibrous cap into the surrounding normal intima are regions of high stress, 3~ at which rupture occurs frequently. Circumferential shear stresses in the fibrous cap are high in plaques with a large lipid pool. Loss from the cap of smooth muscle cells, some which have been transformed from the contrac-
114 DAVID WATERS
tile to the synthetic state, 27 may also contribute to the weakness of the fibrous cap by diminish- ing the capacity to manufacture connective tissue.
The ingress of lipid-filled macrophages to the weakest regions of the cap, first reported by Constantinides, 32 has been confirmed in several studies, but it is not clear if these cells contrib- ute to the creation of an unstable plaque or are merely markers for such a lesion. It is known, however, that macrophages release proteases capable of degrading the connective tissue ma- trix of the fibrous cap, and that they elaborate several thrombogenic factors. Therefore, they have the potential to contribute to plaque rup- ture and thrombosis.
The distribution of types of atheromatous plaques in individuals is heterogeneous, and lipid-rich plaques often represent only a small proportion. In one series of patients with stable angina, lipid-rich, eccentric plaques occupying more than 50% of coronary artery diameter accounted for only 12% of all plaques of this size. 33 Others have asserted that this subpopula- tion of atherosclerotic plaques represents only 10% to 20% of the total plaque population but accounts for 80% to 90% of acute coronary atherosclerotic events. 21 By contrast, Waller 34 has reported that eccentric plaques represent a much larger proportion of the total plaque population.
CONSEQUENCES OF PLAQUE RUPTURE
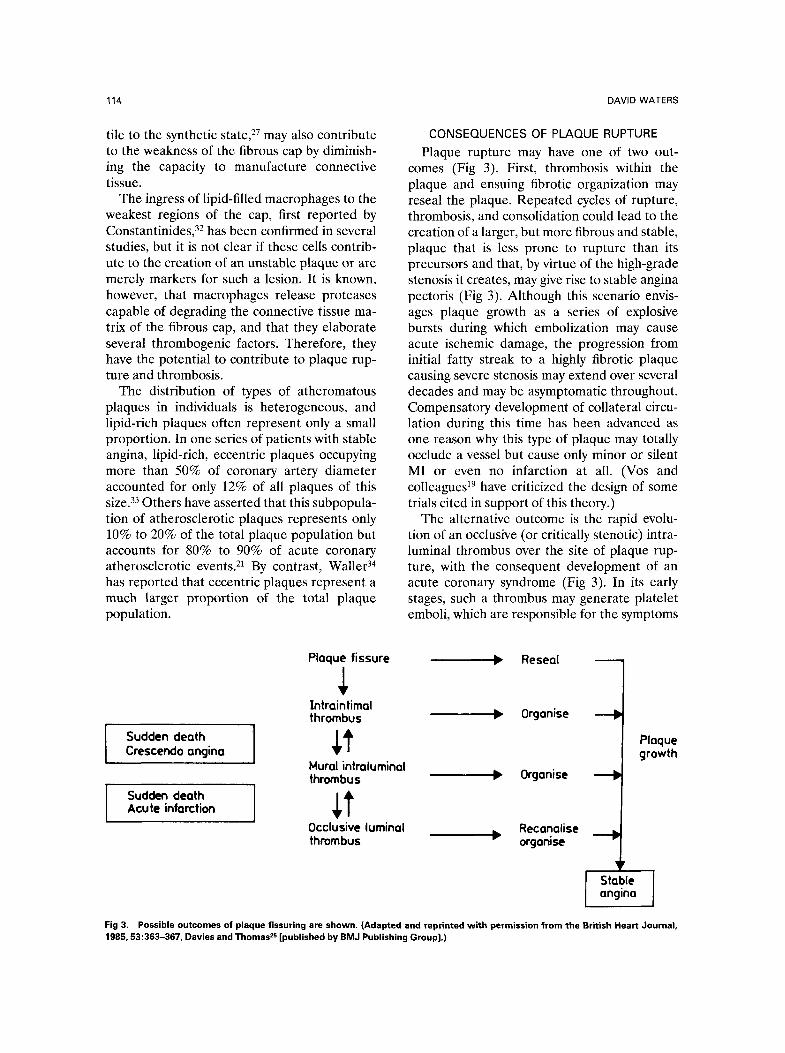
Plaque rupture may have one of two out- comes (Fig 3). First, thrombosis within the plaque and ensuing fibrotic organization may reseal the plaque. Repeated cycles of rupture, thrombosis, and consolidation could lead to the creation of a larger, but more fibrous and stable, plaque that is less prone to rupture than its precursors and that, by virtue of the high-grade stenosis it creates, may give rise to stable angina pectoris (Fig 3). Although this scenario envis- ages plaque growth as a series of explosive bursts during which embolization may cause acute ischemic damage, the progression from initial fatty streak to a highly fibrotic plaque causing severe stenosis may extend over several decades and may be asymptomatic throughout. Compensatory development of collateral circu- lation during this time has been advanced as one reason why this type of plaque may totally occlude a vessel but cause only minor or silent MI or even no infarction at all. (Vos and colleagues 19 have criticized the design of some trials cited in support of this theory.)
The alternative outcome is the rapid evolu- tion of an occlusive (or critically stenotic) intra- luminal thrombus over the site of plaque rup- ture, with the consequent development of an acute coronary syndrome (Fig 3). In its early stages, such a thrombus may generate platelet emboli, which are responsible for the symptoms
Sudden death ] Crescendo angina
Sudden death Acute infarction
Plaque fissure
Intraintimal thrombus
Reseal
0rganise
Mural intraluminal thrombus ~ 0rganise
Occlusive luminal Recanalise thrombus ~ organise ---'e
Stable 1 angina
Plaque growth
Fig 3. Possible outcomes of plaque fissuring are shown. (Adapted and reprinted with permission from the British Heart Journal, 1985, 53:363-367, Davies and Thomas 2s [published by BMJ Publishing Group].)

LIPID LOWERING AND PLAQUE STABILIZATION 115
of unstable angina and for sudden ischemic death in susceptible patients; lipid emboli re- leased from the ruptured plaque may also contribute to this process. Maturation of the thrombus into a fibrin-rich mass containing large numbers of red blood ceils creates a persisting occlusion and causes MI.
IMPACT OF LIPID LOWERING ON CRITICAL PLAQUES
Depletion of the lipid pool of critical athero- sclerotic plaques is perhaps one of the most important effect of sustained lipid-lowering therapy. Reference to Fig 2 shows that therapy with a bile acid sequestrant plus either lova- statin or nicotinic acid almost entirely pre- vented catastrophic progression of medium- sized lesions in FATS. Of 683 lesions designated as causing mild-to-moderate stenosis at the start of the study, only 1 was subsequently linked to a clinical event (P < .005 per patient and P < .02 per lesion). By contrast, 8 of 414 such lesions were associated with clinical events in the control group. This difference in out- comes has been ascribed to removal of lipid from the plaque secondary to the correction of an atherogenic serum lipid profile.
This explanation represents the atheroscle- rotic plaque as a sort of intravascular boil, with removal of the lipid content relieving the me- chanical forces that dispose to rupture. How- ever, lipid-lowering therapy may well have addi- tional favorable effects on these critical plaques, some of which are outlined below.
OXIDIZED LDL AND ENDOTHELIAL DYSFUNCTION
Oxidation, or similar modification, of LDL has been proposed as a key step in atherogen- esis. 35-37 In the context of the critical atheroscle- rotic plaque, a decrease of the native LDL substrate by lipid-lowering therapy may have several potentially favorable effects. Specifi- cally, oxidized LDL is chemotactic for monocyte/ macrophages; it also inhibits the motility of resident macrophages. In addition, oxidized LDL is preferentially phagocytosed by macro- phages (via the acetyl-LDL receptor) and, thereby, promotes the development of foam cells. As noted earlier, the amassing of macro- phages in the fibrous cap is one of the hallmarks
of a critical atherosclerotic lesion. Oxidized LDL may play a crucial role in this process.
In addition, oxidized LDL is cytotoxic and stimulates the release of growth factors and cytokines. These actions also may contribute to the weakening of the fibrous cap in critical lesions. Cholesterol-lowering therapies have been associated with a reduction in the numbers of lipid-laden intimal macrophages in atheroscle- rotic plaques. A reduction in the amount of substrate LDL available for oxidation may be partly responsible for this.
The possibility of supplementing lipid-lower- ing measures with antioxidant therapy has at- tracted much attention, and two recent studies in the United States have provided strong evi- dence of an epidemiologic association between a high intake of vitamin E and a lower incidence of CHD in both men and women. 38,39 It is premature to consider antioxidant therapy as having a confirmed role in the prevention of CHD, but interim data are encouraging.
Oxidized LDL particles may also be impli- cated in a second pathologic process, namely vascular endothelial dysfunction. Extensive data have been amassed which indicate that hyper- cholesterolemia is associated with dysfunction of the vascular endothelium, and that this dys- function leads to the development of a proaggre- gatory state. In addition, the response to vaso- constrictor stimuli is enhanced, whereas that to vasodilators is attenuated or transformed into a paradoxical vasoconstriction. 4~
Alterations of vascular sensitivity are detect- able before there is visible evidence of atheroma- tous lesions. There are persuasive reasons to regard endothelial dysfunction as the first mani- festation of diffuse atherosclerotic vascular dis- ease. It has been reported recently that early signs of endothelial dysfunction are evident at branch points in the human coronary vascula- ture43; these are recognized as sites especially prone to the development of atherosclerosis. Taeymans and colleagues 23 have concluded that plaques located at such sites are at particular risk for progressing to occlusion. The same group has reported a correlation between para- doxical vasoconstriction to acetylcholine and the presence of known risk factors, including serum total cholesterol.
There is ample evidence that the principal

116 DAVID WATERS
cause of the tendency toward vasoconstriction in hypercholesterolemia is impaired synthesis or release of endothelium-derived relaxant factor. The vasodilator response observed when endo- thelium-dependent (ie, receptor-dependent) va- sodilators such as acetylcholine or serotonin are applied to normal endothelium is attenuated, abolished, or reversed when these compounds are applied to the blood vessels of hypercholes- terolemic animals or humans, whereas the re- sponse to sodium nitroprusside (a nonendothe- lium-dependent vasodilator) is preserved. Treatment with lovastatin or lipid-lowering di- ets is associated with a substantial restitution of normal vasodilator responsiveness in hypercho- lesterolemic rabbits, suggesting a causal relation- ship between high serum lipid levels and endo- thelial dysfunction. 47 Lovastatin therapy has also been shown to reduce the extent of isch- emic damage in a model of M! in hypercholes- terolemic rabbits, 48 an effect attributed to im- proved vasodilator responsiveness.
Recent studies at two US centers have ex- tended these findings to humans. Treasure et a149 have reported improvement of endothelial dysfunction in patients with established CAD treated with lovastatin (40 mg twice per day) for 6 months. Anderson et aP ~ have reported simi- lar findings in patients with established coro- nary disease and elevated cholesterol (mean baseline total cholesterol, 220 _+ 33 mg/dL [5.7 -+ 0.85 mmol/L]). These patients were assigned to lipid-lowering therapy with diet only or diet plus lovastatin plus cholestyramine or probucol for 1 year. At the end of this time, paradoxical vasoconstriction induced by acetyl- choline was significantly attenuated in patients treated with diet plus drugs compared with those treated with diet alone (P < .05), and the improvement in endothelial function correlated with the extent of the reduction in serum cholesterol (P = .03). 5~
As well as producing endothelium-derived relaxant factor, functioning endothelium pro- duces prostacyclin and tissue plasminogen acti- vator, which prevent platelet aggregation and thrombus formation. Endothelial cells are also the loci of action of thrombomodulin and hepa- ran sulphate, which inhibit the powerful platelet agonists, thrombin and adenosine diphosphate. The equilibrium between these influences may
be disturbed in hypercholesterolemia-induced endothelial dysfunction, leading to the creation of a proaggregatory state.
CLINICAL CONSEQUENCES OF ENDOTHELIAL DYSFUNCTION
The clinical correlates of altered vascular sensitivity and a proaggregant condition are spasm and thrombosis, respectively. It is un- likely that spasm plays a significant role in the development of fatal acute coronary syndromes in patients with no visible obstruction of coro- nary vessels. However, it may have a contribu- tory role in the development of exercise- induced angina in patients with fixed obstruction and may increase the susceptibility of some patients to MI or sudden ischemic death. The characteristics of the critical coronary plaque (notably those of eccentric situation and a deformable, lipid-rich core) are compatible with vasoconstriction in the functioning, nonathero- sclerotic region of the blood vessel media. 33 Serotonin released from aggregating platelets may also contribute to coronary spasm at foci of endothelial dysfunction. Therefore, plausible mechanisms exist whereby vasospasm may con- tribute to the development of a critical coronary obstruction.
The possible contribution of platelet-rich thrombi to acute ischemic episodes in patients with no angiographic evidence of atherosclero- sis is hard to determine. However, the evidence, now incontrovertible, that antiplatelet therapy is capable of preventing a large number of cardiovascular events in patients with CHD 51 is supportive of a pathologic role for platelet-rich thrombi at sites of organic stenosis. Platelet emboli lodged in coronary microvessels down- stream from a ruptured coronary plaque may play a role in unstable angina or ischemic sudden death in a proportion of patients, 52 and interactions between aggregating platelets and areas of endothelial dysfunction have been implicated in the development of angiographi- cally visible plaques.
Endothelial dysfunction may also have impli- cations for the development of clinical investiga- tive techniques. Angiography might be ex- tended to evaluating the function of vascular endothelium in patients at high risk for the development of overt atherosclerosis. This would

LIPID LOWERING AND PLAQUE STABILIZATION 117
enable appropriate therapy to be initiated at an early stage in the development of the disease. Intravascular ultrasound may also have applica- tions in the detection of atheromatous changes.53,54
CRITICAL PLAQUES AND CORONARY EVENTS
The relationship of endothelial dysfunction and atherosclerotic plaques to coronary events has been summarized by Vos et al (Fig 4). 19 Acute coronary events may arise from plaque fissure, thrombosis, and occlusion at any stage in the development of atherosclerosis, including (albeit probably only rarely) the angiographi- cally undetectable phase of endothelial dysfunc- tion. The extent of thrombosis associated with plaque rupture is not always directly propor- tional to the magnitude of the exposure of lipid in the plaque; therefore, thrombosis at a diffuse,
early-stage lesion may explain the phenomenon of acute coronary events in patients with anglo- graphically normal vessels. However, a majority of events may be explained in terms of rupture, thrombosis, and occlusion at unstable, lipid-rich lesions of intermediate size.
IMPLICATIONS OF ATHEROTHROMBOSIS
So far as is known, the rupture of plaques is a random or arbitrary event. However, it may reasonably be assumed that the rules of probabil- ity apply and that the more unstable plaques a patient possesses, the more likely one is to fissure and give rise to a clinical event. There- fore, a case may be advanced for the use of all reasonable measures to improve the serum lipid profile to minimize the number of critical plaques that develop. These measures (ie, lipid- lowering diet, other lifestyle modifications, and
diameter stenosla
100%
80%
60%
40%
20%
40% 0%
0% plaque
area
t - O Q
0 0 0 A
Q
0 .D
E e
i
, (
n <
1 �9 o e = / = = . / = =
/ / ,V-,m,alred,,o. = ~ / intraluminal
i plaque
~ gra.phlcally de tectab le extraluminal
p l a q u e I: endothel ia l dysfunot lon
I: not d iseased t ime -)
Fig 4. The relationship between progression of atherosclerotic plaque, plaque rupture and thrombosis, and the development of a clinical coronary event is shown. The diagonal line represents the (presumed) linear growth of a plaque. Rupture of the plaque fol lowed by thrombosis and the development of a clinical coronary event may occur at any point along the line from the development of endothelial dysfunction onwards. The horizontal line represents the lower limit of detection by angiography and indicates that endothelial dysfunction (less than 40% of internal elastic lamina occupied by atheroma) does not cause angiographically detectable stenosis of the affected vessel. See text for further details, (Adapted and reprinted with permission. TM)

118 DAVID WATERS
appropriate drug therapy) are not guaranteed to eliminate the risk to individuals; a patient with only one such lesion may still be unlucky enough to have that plaque rupture. Applied consistently, however, such measures should reduce the risk of acute coronary events in a population.
The studies described earlier involved pa- tients with angiographic evidence of coronary atherosclerosis. Elevated cholesterol is a power- ful and often neglected risk factor in the second- ary prevention of CHD. 55,56 The concept of plaque rupture and its prevention by lipid- lowering interventions provides a mechanism to explain the discrepancy between the angio- graphic changes observed in these trials and the clinical outcomes. In doing so, this mechanism provides a rationale for more decisive action in lowering elevated cholesterol in patients with established heart disease. 1 Recent reports that abnormal vasoconstriction is a predictor of coro- nary artery restenosis are consistent with the reported connection between endothelial dys- function and atherosclerosis and reinforce the importance of vigorous intervention against es- tablished risk factors in patients who undergo coronary artery bypass and other revasculariza- tion procedures.
Similar considerations apply to primary pre- vention of CHD. That lipid lowering reduces clinical CHD events has been shown in large-
scale trials. Although angiographic data are not available from those trials, there is no reason to believe that the pathophysiologic processes of atherosclerosis in patients with no history of CHD differ from those in patients who have already experienced a clinical event. Indeed, the phenomenon of endothelial dysfunction in patients with no overt atherosclerosis suggests that patients free of CHD but with hypercholes- terolemia and abnormal vasomotor responses represent a distinct patient population in which early and assertive measures to correct the lipid profile may be highly beneficial.
The traditional definition of regression is closely circumscribed. Angiography data sug- gest that probably the greatest single contribu- tion of intensive lipid lowering is to reduce the likelihood of rupture among lipid-rich lesions of small to moderate dimensions by depleting these high-risk lesions of part of their lipid content. Rupture of these lesions with ensuing thrombosis is perceived increasingly as the prin- cipal cause of overt CHD events. Therefore, in clinical terms, stabilization of critical plaques is a more important goal than reduction of the size of large atherosclerotic lesions. Indeed, it may be that, in terms of hard end points such as death and disability, regression, in the original sense of the term, is neither realistic nor rel- evant, whereas stabilization is both.
REFERENCES
1. Roberts WC: Lipid-lowering therapy after an athero- sclerotic event. Am J Cardiol 64:693-695, 1989
2. Expert Panel on Detection, Evaluation, and Treat- ment of High Blood Cholesterol in Adults: Summary of the Second Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). JAMA 269:3015-3023, 1993
3. International Task Force for Prevention of Coronary Heart Disease on behalf of the European Atherosclerosis Society: Prevention of coronary heart disease: Scientific background and new clinical guidelines. Nutr Metab Cardio- vasc Dis 2:113-156, 1992
4. Beneridge DJ, Dodson PM, Durrington PN, et ah Management of hyperlipidaemia: Guidelines of the British Hyperlipidaemia Association. Postgrad Med J 69:359-369, 1993
5. Brown G, Albers JJ, Fisher DL, et al: Regression of coronary artery disease as a result of intensive lipid- lowering therapy in men with high levels of apolipoprotein B. N Engl J Med 323:1289-1298, 1990
6. Waters D, Craven TE, Lesperance J: Prognostic signifi-
cance of progression of coronary atherosclerosis. Circula- tion 87:1067-1075, 1993
7. Waters D, Lesperance J, Craven TE, et al: Advantages and limitations of serial coronary arteriography for the assessment of coronary atherosclerosis. Implications for clinical trials. Circulation 87:II-38-II-47, 1993 (suppl II)
8. Brensike JF, Levy RI, Kelsey SF, et al: Effects of therapy with cholestyramine on progression of coronary atherosclerosis: Results of the NHLBI Type II coronary intervention study. Circulation 69:313-324, 1984
9. Blankenhorn DH, Nessim SA, Johnson RL, et al: Beneficial effects of combined colestipol-niacin therapy on coronary atherosclerosis and coronary venous bypass grafts. JAMA 257:3233-3240, 1987
10. Cashin-Hemphill L, Mack WJ, Pogoda JM, et al: Benefits of colestipol-niacin on coronary atherosclerosis: A 4-year follow-up. JAMA 264:3013-3017, 1990
11. Buchwald H, Varco RL, Matts JP, et al: Effect of partial ileal bypass on mortality and morbidity from coro- nary heart disease in patients with hypercholesterolemia: Report of the Program on the Surgical Control of the

LIPID LOWERING AND PLAQUE STABILIZATION 119
Hyperlipidemias (POSCH). N Engl J Med 323:946-955, 1990
12. Kane JP, Malloy MJ, Ports TA, et al: Regression of coronary atherosclerosis during treatment of familial hyper- cholesterolemia with combined drug regimens. JAMA 264: 3007-3012, 1990
13. Watts GF, Lewis B, Brunt JNH, et al: Effects on coronary artery disease of lipid-lowering diet, or diet plus cholestyramine, in the St Thomas' Atherosclerosis Regres- sion Study (STARS). Lancet 339:563-569, 1992
14. Ornish D, Brown SE, Scherwitz LW, et al: Can lifestyle changes reverse coronary heart disease? Lancet 336:129-133, 1990
15. Haskell WL, Alderman EL, Fair JM, et al: The effects of intensive multiple risk factor reduction on coro- nary atherosclerosis and clinical cardiac events in men and women with coronary artery disease: The Stanford Coro- nary Risk Intervention Project (SCRIP). Circulation 89:975- 990, 1994
16. Schuler G, Hambrecht R, Schlierf G, et al: Regular physical exercise and low-fat diet: Effects on progression of coronary artery disease. Circulation 86:1-11, 1992
17. Blankenhorn DH, Azen SP, Kramsch DM, et al: The monitored atherosclerosis regression study (MARS): Coro- nary angiographic changes with lovastatin therapy. Ann Intern Med 119:969-976, 1993
18. Waters D, Higginson L, Gladstone P, et al: Effect of monotherapy with an HMG CoA reductase inhibitor upon the progression of coronary atherosclerosis as assessed by serial quantitative arteriography: The Canadian Atheroscle- rosis Intervention Trial (CCAIT). Circulation 89:959-968, 1994
19. Vos J, de Feyter PJ, Simoons ML, et al: Retardation and arrest of progression or regression of coronary artery disease: A review. Prog Cardiovasc Dis 35:435-454, 1993
20. Stone PH, Gibson CM, Pasternak RC, et al: Natural history of coronary atherosclerosis using quantitative angiog- raphy in men, and implications for clinical trials of coronary regression. Am J Cardio171:766-772, 1993
21. Brown BG, Zhao X-Q, Sacco DE, et al: Lipid lowering and plaque regression: New insights into preven- tion of plaque disruption and clinical events in coronary disease. Circulation 87:1781-1791, 1993
22. Webster MWI, Chesebro JH, Smith HC, et al: Myo- cardial infarction and coronary artery occlusion: A prospec- tive 5-year angiographic study. J AJn Coil Cardiol 15:218A, 1990 (suppl A, abstr)
23. Taeymans Y, Theroux P, Lesperance J, et al: Quanti- tative angiographic morphology of the coronary artery lesions at risk of thrombotic occlusion. Circulation 85:78-85, 1992
24. Fuster V, Badimon L, Badimon J J, et al: The patho- genesis of coronary artery disease and the acute coronary syndromes. N Engl J Med 326:242-250, 1992
25. Davies M J, Thomas AC: Plaque fissuring--the cause of acute myocardial infarction, sudden ischaemic death, and crescendo angina. Br Heart J 53:363-367, 1985
26. Davies MJ: A macro and micro view of coronary vascular insult in ischemic heart disease. Circulation 82:11- 38-11-46, 1990 (suppl II)
27. Waller BF: The eccentric coronary atherosclerotic
plaque: Morphologic observations and clinical relevance. Clin Cardiol 12:14-20, 1989
28. Woolf N: The atherosclerotic arterial wall. Can J Cardiol 9:3C-5C, 1993 (suppl C)
29. Bocan TA, Schifani TA, Guyton JR: Ultrastructure of the human aortic fibrolipid lesion: Formation of the atherosclerotic lipid-rich core. Am J Pathol 123:413-424, 1986
30. Richardson PD, Davies M J, Born GVR: Influence of plaque configuration and stress distribution on fissuring of coronary atherosclerotic lesions. Lancet 3:941-944, 1989
31. Lendon CL, Davies MJ, Born GVR, et al: Atheroscle- rotic plaque caps are locally weakened when macrophage density is increased. Atherosclerosis 87:87-90, 1991
32. Constantinides P: Plaque fissures in human coronary thrombosis. J Athcroscler Res 61:1-17, 1966
33. Hangartner JRW, Charleston AJ, Davies M J, et al: Morphological characteristics of clinically significant coro- nary artery stenosis in stable angina. Br Heart J 56:501-508, 1986
34. Waller BF: The eccentric coronary atherosclerotic plaque: Morphologic observations and clinical relevance. Clin Cardiol 12:14-20, 1989
35. Schwartz CJ, Valente A J, Sprague EA: A modern view of atherogenesis. Am J Cardiol 71:9B-14B, 1993 (suppl B)
36. Steinberg D: Antioxidants and atherosclerosis. Circu- lation 84:1422-1425, 1991
37. Steinberg D, Parthasarathy S, Carew TE, et al: Beyond cholesterol: Modifications of low-density lipopro- tein that increase its atherogenicity. 320:915-924, 1989
38. Stampfer MJ, Hennekens CH, Manson JE, et al: Vitamin E consumption and the risk of coronary disease in women. N Engl J Med 328:1444-1449, 1993
39. Rimm EB, Stampfer MJ, Ascherio A, et al: Vitamin E consumption and the risk of coronary heart disease in men. N Engl J Med 328:1450-1456, 1993
40. Vita JA, Treasure CB, Ganz P, et al: Control of shear stress in the epicardial coronary arteries of humans: Impair- ment by atherosclerosis. J Am Coil Cardiol 14:1193-1199, 1989
41. Chesebro JH, Fuster V, Webster MWI: Endothelial injury coronary vasomotion. J Am Coil Cardiol 14:1991- 1992, 1989 (editorial)
42. Vita JA, Treasure CB, Nabel EG, et al: Coronary vasomotor response to acetylcholine relates to risk factors for coronary artery disease. Circulation 81:491-497, 1990
43. McLenachan JM, Vita JA, Fish RD, et al: Early evidence of endothelial dysfunction at coronary branch points. Circulation 82:1169-1179, 1990
44. Henry PD: Hyperlipidemic arterial dysfunction. Cir- culation 81:697-699, 1990
45. Zeiher AM, Drexler H, Wollschl~iger H, et al: Modu- lation of coronary vasomotor tone in humans: Progressive endothelial dysfunction with different early stages of coro- nary atherosclerosis. Circulation 83:391-401, 1991
46. Vita JA, Treasure CB, Yeung AC, ct al: Patients with evidence of coronary endothelial dysfunction as assessed by acetylcholine infusion demonstrate marked increase in sensitivity to constrictor effects of catecholamines. Circula- tion 85:1390-1397, 1992

120 DAVID WATERS
47. Siegfried MR, Lefer AM: Amelioration of coronary vascular endothelial dysfunction in hypercholesterolemic rabbits by the HMG-CoA reductase inhibitor lovastatin. Coronary Artery Dis 2:621-627, 1991
48. Osborne JA, Lento PH, Siegfreid MR, et al: Cardio- vascular effects of acute hypercholesterolemia in rabbits: Reversal with lovastatin treatment. J Clin Invest 83:465-473, 1989
49. Treasure CB, TaUey JD, Stillabower ME, et al: Coronary endothelial responses are improved with aggres- sive lipid lowering therapy in patients with atherosclerosis. Circulation 88:1-368, 1993 (suppl I, abstr)
50. Anderson TJ, Meredith IT, Yeung AC, et al: Choles- terol lowering therapy improves endothelial function in patients with coronary atherosclerosis. Circulation 88:1-368, 1993 (suppl I, abstr)
51. Antiplatelet Trialists' Collaboration: Collaborative overview of randomised trials of antiplatelet therapy--I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Br Med J 308:81-106, 1994
52. Davies MJ, Thomas AC, Knapman PA, et al: Intra- myocardial platelet aggregation in patients with unstable angina suffering sudden ischemic cardiac death. Circulation 73:418-427, 1986
53. Nishimura R_A, Edwards WD, Warnes CA, et al: Intravascular ultrasound imaging: In vitro validation and pathologic correlation. J Am Coll Cardiol 16:145-154, 1990
54. St Goar FG, Pinto FJ, Alderman EL, et al: Intracoro- nary ultrasound evaluation in cardiac transplant recipients: In vivo evaluation of angiographically silent intimal thicken- ing. J Am Coil Cardiol 17:102A, 1991 (suppl A)
55. Pekkanen J, Linn S, Heiss G, et al: Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N Engl J Med 322:1700-1707, 1990
56. Cohen MV, Byrne M-J, Levine B, et al: Low rate of treatment of hypercholesterolemia by cardiologists in pa- tients with suspected and proven coronary artery disease. Circulation 83:1294-1304, 1991