
Planned Caesarean Section (CS) Care Pathway protocols and... · - Anterior placenta praevia -...
24
© RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 1 of 24 Planned Caesarean Section (CS) Care Pathway Including Enhanced Recovery Likes to be known as Consultant Planned date of CS Named Midwife Date of admission Ward Known Allergies CODE Midwives responsibility White Pre op clerking and clinic visits Yellow Admission and pre op phase TX Doctors responsibility Pink Surgery Green Post op PAMS responsibility Version 7.4 November 2018 Review before: April 2020 Approval Group Date Maternity Clinical Governance 6 th April 2018 & 2 nd November 2018 Change History Version Date Author(s), Job title Reason Version 7.2 December 2015 Consultant Obstetrician Antenatal Services Manager Addition of PICO dressing for BMI >35 Version 7.3 February 2018 Acting Screening MW & Consultant Obstetrician Reviewed Version 7.4 Nov 2018 Dept. Lead Maternity Theatres Pg 5 - Live change to replace PN VTE risk assessment Pg 9 - Personalised CS question added Pg 13 - TEDs removed from criteria Pg 14 - Codeine changed to Dihydrocodeine Pg 17, 19 & 20 - minor changes
Transcript of Planned Caesarean Section (CS) Care Pathway protocols and... · - Anterior placenta praevia -...

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 1 of 24
Planned Caesarean Section (CS) Care Pathway Including Enhanced Recovery
Likes to be known as
Consultant
Planned date of CS
Named Midwife
Date of admission
Ward
Known Allergies
CODE
Midwives responsibility White Pre op clerking and clinic visits
Yellow Admission and pre op phase
TX Doctors responsibility Pink Surgery
Green Post op
PAMS responsibility
Version 7.4 November 2018 Review before: April 2020
Approval Group Date
Maternity Clinical Governance 6th April 2018 & 2nd November 2018
Change History
Version Date Author(s), Job title Reason
Version 7.2 December 2015 Consultant Obstetrician Antenatal Services Manager
Addition of PICO dressing for BMI >35
Version 7.3 February 2018 Acting Screening MW & Consultant Obstetrician
Reviewed
Version 7.4 Nov 2018 Dept. Lead Maternity Theatres
Pg 5 - Live change to replace PN VTE risk assessment Pg 9 - Personalised CS question added Pg 13 - TEDs removed from criteria Pg 14 - Codeine changed to Dihydrocodeine Pg 17, 19 & 20 - minor changes

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 2 of 24
All members of staff who are using this Pathway use black ink and fill in this section. You can then use initials when recording care
Print Name Designation Signature Initials

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 3 of 24
How to use an Integrated Care Pathway (ICP)
Firstly, if you are going to write in the ICP you need to state your Name, Job Title and give a sample signature and initials on the front of the ICP cover
If you are recording an event which is predicted by the ICP, then you just sign against that predicted intervention in the column provided.
If your intervention is not in line with the pathway, you must record this as a variance in the variance column with the action you will take to try to bring the patient back onto the pathway.
Care given by health care assistants and student nurses must be countersigned by a registered nurse.
There are many ‘NOTES’ pages for you to write free text about the care given to the patient by you. These notes should always be dated and timed.
The ICP has been colour coded to make it easier to document your aspect of care. Black background relates to Doctors, Clear background relates to nurses and grey background relates to PAMS but check the key prior to writing.
All ICPs are chronological so you should be able track the care given very easily
Abbreviations BO Bowels open NBM Nil by mouth
BP Blood pressure NOK Next of kin
FBC Full blood count N/A Not applicable
HB Haemoglobin PU’d Passed urine
I.M Intramuscular ROS Removal of sutures
IV Intravenous SB Stillborn
IVAB Intra venous anti biotic TPR Temperature, Pulse ,Respiration
LOS Length of stay TTOs Tablets to take out
U& E’s Urea and Electrolytes
Pre-operative blood tests and investigations Blood test Patient group
FBC All patients
Group & save All patients
Cross match For those women with the following;
Known major placenta praevia (2 units if additional risk factor: - Major praevia - Low haemoglobin - Anterior placenta praevia - Placenta accreta – suspected or diagnosed - Multiple fibriods - Surgical or anaesthetic decision)
Known bleeding disorder
Haemoglobin <8g/dl
Difficulty cross matching due to known antibodies

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 4 of 24

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 5 of 24

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 6 of 24
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 7 of 24
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 8 of 24
This page is intentionally
left blank

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 9 of 24
Antenatal Clinic visit (To be commenced when decision made to book caesarean section)
This section to be filled by medical staff booking the C/section
Name................................................................... Date.................... Name of the Doctor ............................................................Grade............................. (Doctor booking the C/section)
Reason for caesarean section.........................................................Gestation .................wks
Sterilisation Y N any other procedure (specify) .........................................
Specific medical / obstetric problems
Placental site ………………………………………
Allergy (including latex) ............................................................................................................ Medications...................................................................................................................................
Anaesthetic alert? Y N If yes, Anaesthetic referral/bleep 149 Y N
Consented Y N If No, please explain reason(s)
........................................................................................................................................................
This section to be filled by Midwife/MCA in Antenatal Clinic
Information giving Initial Reason for variance and action taken
Woman booked in CS diary
Pre op assessment arranged and date given as…………………………….
Explanation of operation and post op treatment discussed with patient ‘’elective c-section booking pack’’ given including anaesthetic information are highlighted to ensure women anticipating regional anaesthetic?
CS date given as……………
Date for CS documented in hand held notes
Enhanced recovery discussed Y N
Personalised CS discussed Y N
Anticipated date of discharge (24 hours if no contraindication) discussed? Date.....................
MRSA swabs taken Y (date ...................)
N
If latex allergy, Alert sticker Y N

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 10 of 24
Pre-operative assessment at Antenatal Clinic Date:
Planned date for caesarean section
Blood results from 34/40 check Date taken
Hb WBC Platelets
If Hb < 10.5, any treatment? Y N , Feso4 Ferrinject Blood transfusion If Platelets <100 – Anaesthetic review Y N MRSA (+) Y N If Yes, treatment given Y N
Pathology card request given for FBC Group and save Cross match (see cross
match protocol) Date bloods to be taken……………………..(to be taken within 72 hours of operation)
Maternal observations (noted from last appointment if no medical concerns) BP
Pulse
Temp Weight BMI Urinalysis Glucose Protein
TEDs Size………….
If weight greater than 130kg, theatres informed Bariatric equip arranged N/A
Current medication
Initials Reason for variance and action taken
If latex allergy, Alert sticker
Y N

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 11 of 24
Pre-operative assessment (continued) Date:
Pre-Assessment Clinic Initials Reason for variance and action taken.
Has patient read and understood anaesthetic
leaflet? Y N
Any concerns regarding spinal anaesthesia?
Y Bleep anaesthetist (149)
N
Has patient read and understood C/section
leaflet? Y N
Has patient sign consent form?
Y N
Any concerns regarding consent form?
Y Bleep Obstetrics SHO
N
Anaesthetist alert Y N Inform anaesthetist – Bleep 149 if notes with alert sticker have not been reviewed prior to clinic or any concerns from past medical history at booking or from anaesthetic questions –see below.
Information regarding Skin to skin contact Specify areas of body piercing
Information regarding baby feeding and hand expression
Consent gained for newborn Vitamin K Oral IM Documented in baby notes
Neonatal BCG discussed
Blood results within normal range Y N
Has the woman any body piercing Y N If yes, is she willing to have it removed prior to C section? Y N
Consent taken and checked with patient and form in notes Y N
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 12 of 24
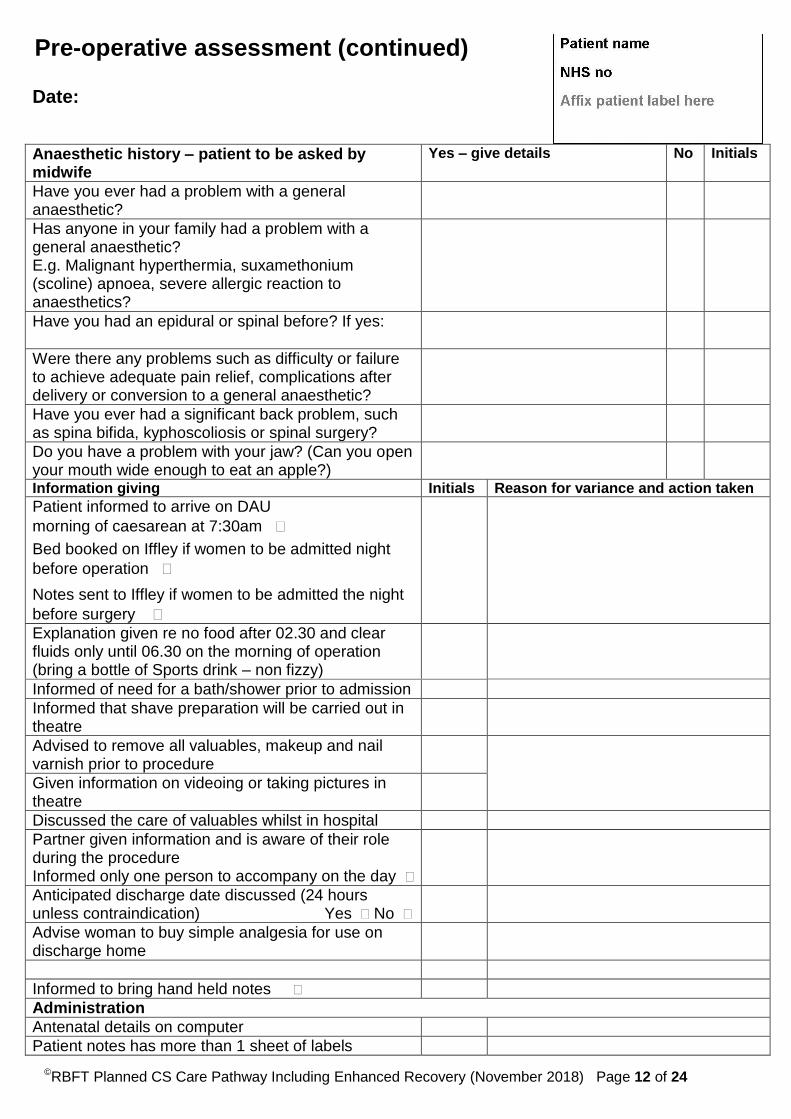
Pre-operative assessment (continued) Date:
Anaesthetic history – patient to be asked by midwife
Yes – give details No Initials
Have you ever had a problem with a general anaesthetic?
Has anyone in your family had a problem with a general anaesthetic? E.g. Malignant hyperthermia, suxamethonium (scoline) apnoea, severe allergic reaction to anaesthetics?
Have you had an epidural or spinal before? If yes:
Were there any problems such as difficulty or failure to achieve adequate pain relief, complications after delivery or conversion to a general anaesthetic?
Have you ever had a significant back problem, such as spina bifida, kyphoscoliosis or spinal surgery?
Do you have a problem with your jaw? (Can you open your mouth wide enough to eat an apple?)
Information giving Initials Reason for variance and action taken
Patient informed to arrive on DAU
morning of caesarean at 7:30am
Bed booked on Iffley if women to be admitted night
before operation
Notes sent to Iffley if women to be admitted the night
before surgery
Explanation given re no food after 02.30 and clear fluids only until 06.30 on the morning of operation (bring a bottle of Sports drink – non fizzy)
Informed of need for a bath/shower prior to admission
Informed that shave preparation will be carried out in theatre
Advised to remove all valuables, makeup and nail varnish prior to procedure
Given information on videoing or taking pictures in theatre
Discussed the care of valuables whilst in hospital
Partner given information and is aware of their role during the procedure Informed only one person to accompany on the day
Anticipated discharge date discussed (24 hours unless contraindication) Yes No
Advise woman to buy simple analgesia for use on discharge home
Informed to bring hand held notes
Administration
Antenatal details on computer
Patient notes has more than 1 sheet of labels

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 13 of 24
Pre-operative assessment (continued) Date:
Antibiotic prophylaxis at caesarean section See Obstetric antibiotic guidelines (GL787) Based on booking weight: 1st choice: BMI < 35 IV co-amoxiclav 1.2g single dose BMI ≥35 (IV co-amoxiclav 1.2g + IV amoxicillin 1g) single dose If true penicillin allergy: IV gentamicin 5 mg/kg STAT (*Use booking weight for BMI <50. If BMI ≥ 50, use corrected dosing weight to calculate gentamicin dose) + IV clindamycin 1.2 g single dose If ‘Known MRSA’ or ‘High risk for MRSA’: IV teicoplanin 10 mg/kg single dose + IV gentamicin 5 mg/kg STAT (*Use booking weight for BMI < 50. If BMI ≥ 50, use corrected dosing weight to calculate gentamicin and teicoplanin dose)
Other drugs at caesarean section
Diclofenac suppository +/- 100mgs PR at end of procedure
Paracetamol suppository 1g
Post op prescription Morphine 10-15mg 3-4 hourly for the 1st 24 hours Ibuprofen 400mg Four times a day (not for mod-severe asthmatics &
pre eclampsia) First dose should not be given prior to 12 hours post procedure
Dihydrocodeine phosphate & Paracetamol
60mg 1g
Six hourly as required in combination
Senna 1-2 tablets At night
For patient who CANNOT have NSAIDs
Tramadol 100mg 6 hourly orally
Medication Initial Reasons for variance and action
Outpatient prescription for Ranitidine 150mg (evening and morning before surgery) Dihydrocodeine phosphate 30-60mgs QDS for 7 days. Senna 1-2 tablets daily
Advice
Advice sought from surgeon Y N Not required
Name: Result
Advice sought from anaesthetist Y N Not required
Name: Result
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 14 of 24
This page is intentionally
left blank

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 15 of 24
Day of operation - Pre-operative check list Date:
Maternal Observations
Blood results
BP Blood group =
Pulse Hb WBC Platelets
Temp
Resp MRSA Swab Result
Fetal Observations Blood sugar
FH Time Blood sugar Action
Time of last fluid (Clear energy drink) intake
......................
Additional information
Initial Reason for variance and action taken
Patient admitted on computer
Theatre prepared for latex allergy Y N/A
Partner to be present in theatre Y N
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 16 of 24
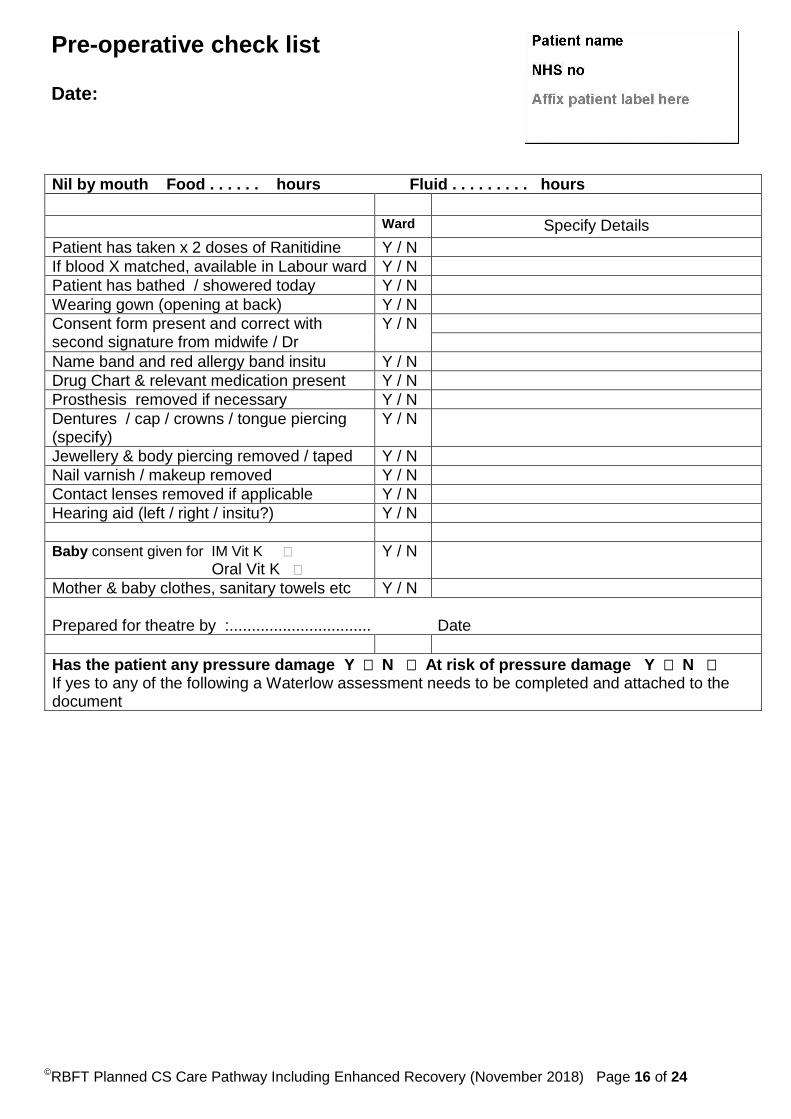
Pre-operative check list Date:
Nil by mouth Food . . . . . . hours Fluid . . . . . . . . . hours
Ward Specify Details
Patient has taken x 2 doses of Ranitidine Y / N
If blood X matched, available in Labour ward Y / N
Patient has bathed / showered today Y / N
Wearing gown (opening at back) Y / N
Consent form present and correct with second signature from midwife / Dr
Y / N
Name band and red allergy band insitu Y / N
Drug Chart & relevant medication present Y / N
Prosthesis removed if necessary Y / N
Dentures / cap / crowns / tongue piercing (specify)
Y / N
Jewellery & body piercing removed / taped Y / N
Nail varnish / makeup removed Y / N
Contact lenses removed if applicable Y / N
Hearing aid (left / right / insitu?) Y / N
Baby consent given for IM Vit K
Oral Vit K Y / N
Mother & baby clothes, sanitary towels etc Y / N
Prepared for theatre by :................................ Date
Has the patient any pressure damage Y N At risk of pressure damage Y N If yes to any of the following a Waterlow assessment needs to be completed and attached to the document

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 17 of 24

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 18 of 24
Theatre (To be completed by theatre team)
Date:
Time into theatre:………………hrs Time out of theatre……………. THEATRE (No:.................) Initial Reason for variance and action taken
Resuscitaire checked
Neonatologist present if required
Additional equipment Cell salvage Ultrasound scanner CTG machine Other ……………………….
WHO checklist
IV sited ………………………time……………..
VIP chart commenced
Spinal procedure commenced at…………..hrs
Urinary catheter inserted Size 12 (10mls water)
SPACE FOR CATHETER STICKER
Presentation/ Lie confirmed (please circle) Cephalic, Breech, Transverse
Fetal heart beat auscultated Y N
Patient position Supine with wedge Right arm Left arm By side By side Extended on board Extended on board Flexion onto chest Flexion onto chest
Pressure areas protected
Head Elbows Sacrum Leg rest
Flowtron leggings used Y N
Diathermy plate applied Thigh right left
Skin preparation used
Swab and suture count for operative procedure
Abdo Large Small Other Sutures Needles Blades
Swab and instrument count correct post procedure
Sutures; insoluble
Nylon Prolene & beads Clips Silk Other..................... Soluble
Monocryl Vicryl other............
Interrupted Continuous
Date to be removed……………
Drain insitu Y N Date to be removed……………

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 19 of 24
Operation performed Elective LSCS
Other procedure performed
Dressings applied;
Mepilex Steristrips Pressure dressing If Booking BMI>35 for PICO Dressing Other (please specify)……………………………………………………….
Diathermy plate site clear
Date:
Third stage details Method of delivery Placenta check
Spontaneous Complete Incomplete
Cord traction Sent to pathology Y N
Manual removal Membranes Complete Incomplete
Blood loss…………….mls 3 cord vessels present Y N ………………..
Obstetrician informed if placenta or membranes appear incomplete Y N
Medication Carbetocin
Oxytocin
Ergometrine
PR Diclofenac
Other procedures: …………………………………………………………………………………….
Blood taken Maternal Y N Reason Kleihauer
Cord Y N Electrophoresis
PH cord Other
Infant details Infant Birth date /
Time Weight Sex Maturity Alive / SB Apgar score
@ 1 min……… @ 5mins………
Initial
ID bands x2 to baby
Baby transferred to Ward NNICU Reason………………………………………….
Birth trauma or abnormalities
Further information Cord Blood Gases Arterial Venous
PH PH
PCo2 PCo2
PO2 PO2
HCO3 HCO3
Base Excess Base Excess
Machine no. Machine no.
Date Date
Time Time
Delivered by Status Midwife in charge (please print name)

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 20 of 24
Recovery observations Name:
Hospital No:
Date: Maternity Unit MOWS Chart
Date >
0o C Time >
220
39o C
200
38o C
180
37o C
160
36o C
140
35o C
120
Temp 100
FHR 80
x
Pulse 60
BP 40
Resp Rate
O2 L/min
O2 Saturation
Lochia
Fundus
Urine Output
Conscious Level
Signature
Score – Resp
Pulse
Systolic
Diastolic
Consciousness
Urine Output
Total MOWS
3 2 1 0 1 2 3
Resp rate < 8 8 9-18 19-25 26-30 >30
Pulse rate < 40 40-50 51-100 101-110 111-129
>129
BP Systolic
< =70 71-80 81-100 101-159 160–199 200 >200
BP Diastolic
< 95 95-109 >= 110
Urine 0ml/hr OR 0ml/24hrs
<=30ml/hr OR <=720ml/24hrs
<=45ml/hr OR <=1000ml/24hrs
>=45ml/hr OR >=1000ml/24hrs
Conscious level
Unresponsive
Responds to pain
Responds to voice Alert Irritated V6.4 Feb 17
Action to be taken
0
1
2
3
4 or more
Repeat observations when appropriate for clinical scenario – at least daily
Minimum of 4 hourly observations as there is potential for deterioration.
Inform midwife in charge, obstetric registrar. Minimum 1 hourly observations
Inform senior midwife, obstetric and anaesthetic staff. Minimum ½ hourly observations
As above but the consultant obstetrician and consultant anaesthetist should be informed. Minimum 30 minute observations. If no one is available to review the patient, inform the Outreach Team
©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 21 of 24
Recovery Record Date:
Fluid balance Time Fluid intake Fluid output
IV Oral Urine Vomit Lochia

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 22 of 24
Transfer Date:
Criteria for safe transfer to ward : Initial Reason for variance and action taken
MOWs less than 1
Medication prescribed: Post -op analgesia anti-emetics
Anticoagulants LMWH FLOTRONS
None IV fluids stopped Y N Time stopped............................
Haemodynamically stable
Pain score (page 5) <5 or acceptable to patient
Wound drain in situ Y N No signs of bleeding from drain site If yes, drain remains vacuumed
'Sensation/mobility returning to lower limbs' Y N If No please refer to Anaesthetist
Nausea & vomiting under control
Baby’s labels present and correct
Computer details completed
Birth register completed
LSCS letter
Blood group Kleihauer required Y N
Handover to ward staff completed using SBAR tool (to include review of post-op instructions)
Note, if Diamorphine has been given via spinal, Ward midwife made aware that further analgesia within 24hours to be discussed with an Anaesthetist Bleep 142
Time transferred................................hrs
Recovery midwife signature
Received by midwife signature
SBAR - To be completed in postnatal record book and sign over transfer of care.

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 23 of 24
Caesarean Section – Operation Record Date …………………………………………………..
Location ……………………………………………...
Time of Decision ……………………………………………
Consultant informed …………………Initials
Time of Incision ……………………………………………
Time of Delivery ……………………………………………
Time of Conclusion ………………………………………
Indication for delivery: ……………………………………………………………
Classification of Urgency: RCOG/RCA Category: 1 2 3 4
Written consent obtained: Yes No If not, reason …………………………………………………………..
Type of Anaesthesia: Epidural Spinal CSE GA
Pre-operative discussion:
Urinary Catheter: Foley Other Findings e.g. fetal position/tubes/ovaries/adhesions Procedure:
Drain: Yes / No Removal : ……
Skin closure: Monocryl Prolene Other....…….
Pressure dressing Yes Removal Instructions……….…... PICO Dressing 7 Days
Estimated blood loss………..If EBL > 2L MOH: Controlled / Uncontrolled Call
Swabs checked Needles checked Instruments checked
Paired cord gasses taken Yes No Vaginal Toilet Post-operative instructions:
Suggestion for next confinement VBAC ELCS
Surgeon (PRINT)………………………….. Signature…………………Grade
Assistant ……………………………….. Anaesthetist……………… Scrub nurse……………
C/S letter for GP signed Y N

©RBFT Planned CS Care Pathway Including Enhanced Recovery (November 2018) Page 24 of 24
This page is intentionally left blank


















