Plain Chest X Ray
154
Click here to load reader
-
Upload
samuel-gamadey -
Category
Documents
-
view
175 -
download
8
description
The basics of chest radiographs.
Transcript of Plain Chest X Ray

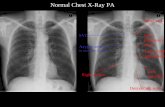
Chest RadiographsChest Radiographs
SAMUEL M. Y. GAMADEYSAMUEL M. Y. GAMADEY
1616THTH SEPTEMBER,2010 SEPTEMBER,2010

CHEST X RAYCHEST X RAY
A Chest X-ray (CXR) is normally taken erect and PA A Chest X-ray (CXR) is normally taken erect and PA (posterior anterior) at a distance of 5 or 6 feet (150 or (posterior anterior) at a distance of 5 or 6 feet (150 or 200cm).200cm).

PA VIEW LATERAL VIEW
PA RADIOGRAPH LATERAL RADIOGRAPH

LATERAL DECUBITUS
LATERAL DECUBITUS RADIOGRAPH AP LORDOTIC RADIOG.
LORDOTIC POSITION

Chest Radiography : Basics Chest Radiography : Basics PrinciplesPrinciples
A Structure is rendered visible on a radiograph by the A Structure is rendered visible on a radiograph by the juxtaposition two different densities juxtaposition two different densities

Silhouette SignSilhouette Sign
Loss of expected interface normally Loss of expected interface normally created by the juxtaposition of two created by the juxtaposition of two structures of different densitiesstructures of different densities
No boundary can be seen between two No boundary can be seen between two structures of similar densities.structures of similar densities.

ERECT FILMSERECT FILMS Erect position is the most ideal technique for chest x Erect position is the most ideal technique for chest x
ray becauseray becauseIt reproduces the normal state of the lungs & It reproduces the normal state of the lungs & mediastinum. mediastinum.
Air rises to the apical region, making it easy to Air rises to the apical region, making it easy to recognise a pneumothorax. recognise a pneumothorax.
Fluid runs downwards, producing a level at the Fluid runs downwards, producing a level at the base with a curved line (meniscus). base with a curved line (meniscus).
The diaphragms are lower showing more of the The diaphragms are lower showing more of the lung bases and the heart size can be accurately lung bases and the heart size can be accurately assessed.assessed.

POSTERIOR – ANTERIOR VIEWPOSTERIOR – ANTERIOR VIEW
The film is taken PA because:The film is taken PA because:
It is easier to clear the scapulae from the lung fields by It is easier to clear the scapulae from the lung fields by moving the shoulders forwardmoving the shoulders forward
There is less magnification of the heart because the heart There is less magnification of the heart because the heart is lying adjacent to the filmis lying adjacent to the film
When the patient is too sick to stand unaided or unable to When the patient is too sick to stand unaided or unable to keep still the X-ray is taken supine. keep still the X-ray is taken supine.

PA VIEW AP VIEWPA VIEW AP VIEW

EXPIRATORY FILM:EXPIRATORY FILM:
This is taken when the patient has breathed out.This is taken when the patient has breathed out.
This may help to show bronchial obstruction with air trapping This may help to show bronchial obstruction with air trapping (e.g. inhaled foreign body in a child):(e.g. inhaled foreign body in a child):
LATERAL FILM:LATERAL FILM:
A lateral film should never be part of a standard chest A lateral film should never be part of a standard chest examination especially for medical purposes or for follow up examination especially for medical purposes or for follow up of a known lesion. The PA film should be examined. If there of a known lesion. The PA film should be examined. If there is an abnormality, a lateral film may then be useful for further is an abnormality, a lateral film may then be useful for further assessment & localisation of abnormalities seen or assessment & localisation of abnormalities seen or suspected on the PA film.suspected on the PA film.

OBLIQUE VIEWS:OBLIQUE VIEWS:
These are helpful in assessing rib lesions & some These are helpful in assessing rib lesions & some pneumothoraces.pneumothoraces.
LORDOTIC VIEWSLORDOTIC VIEWS
They can be obtained to better visualize structures in the They can be obtained to better visualize structures in the thoracic apex obscured by overlying bony structures.thoracic apex obscured by overlying bony structures.
DECUBITUS VIEWDECUBITUS VIEW
The decubitus view can be done to locate fluid in the chest The decubitus view can be done to locate fluid in the chest cavity. The patient will have to lie on either the right or left cavity. The patient will have to lie on either the right or left side for two minutes and a shoot through x-ray is taken. side for two minutes and a shoot through x-ray is taken.

Poor Quality Poor Quality CXRCXR
Supine positionSupine position– Decreases lung volume, increased heart sizeDecreases lung volume, increased heart size– Basilar infiltrates & interstitial spaces accentuatedBasilar infiltrates & interstitial spaces accentuated– Increases venous return to the heartIncreases venous return to the heart
Semi-upright positionSemi-upright position– Enlarges normal structuresEnlarges normal structures– Changes air-fluid levelsChanges air-fluid levels
Failure to hold breathFailure to hold breath– Lung structures & diaphragm blurredLung structures & diaphragm blurred
Expiration filmExpiration film– Basilar infiltrates & interstitial spaces accentuatedBasilar infiltrates & interstitial spaces accentuated– Increased heart sizeIncreased heart size

Why order a Why order a CXR?CXR?
SYMPTOMSSYMPTOMS::
Bad or persistent Bad or persistent coughcough
Chest painChest pain
Chest injuryChest injury
Coughing up bloodCoughing up blood
FeverFever
Shortness of breathShortness of breath

Why order a Why order a CXR?CXR?
Pleural effusionPleural effusion
PneumothoraxPneumothorax
HemothoraxHemothorax
Pulmonary Pulmonary embolusembolus
TraumaTrauma
Monitoring chest Monitoring chest drainagedrainage
TBTB
Lung cancerLung cancer
Chest pain Chest pain (MI?)(MI?)
HypertensionHypertension
ScreeningScreening
PneumoniaPneumonia
COPDCOPD
AsthmaAsthma

The 12-Step ProgramThe 12-Step Program
11: : NameName22: : DateDate33: Anatomical markings: Anatomical markings44: What type of : What type of view(s)view(s)55: Penetration: Penetration66: Inspiration: Inspiration77: Rotation: Rotation88: Angulation: Angulation99: Soft tissues / bony structures: Soft tissues / bony structures1010: Mediastinum: Mediastinum1111: Diaphragms: Diaphragms1212: Lung Fields: Lung Fields
Quality Control
Findings
}}
Pre-read}

Quality ControlQuality Control
55. . PenetrationPenetration– Should faintly see ribs Should faintly see ribs
through the heartthrough the heart
– Barely see the spine Barely see the spine through the heart through the heart so so that lesions behind or that lesions behind or in front of the heart will in front of the heart will not be missed.not be missed.
– Should see pulmonary Should see pulmonary vessels nearly to the vessels nearly to the edges of the lungsedges of the lungs

Overpenetrated Film
• Lung fields darker than normal—may obscure subtle pathologies
• See spine well beyond the diaphragms
• Inadequate lung detail

Underpenetrated Film•Hemidiaphragms are obscured
•Pulmonary markings more prominent than they actually are

A body section view may be done in addition to a routine A body section view may be done in addition to a routine PA chest to outline the lower regions of the chest in very PA chest to outline the lower regions of the chest in very obsessed patients.obsessed patients.

Quality ControlQuality Control
66. . InspirationInspiration
– Should be able to Should be able to count 9-10 posterior count 9-10 posterior ribsribs
– Heart shadow should Heart shadow should not be hidden by the not be hidden by the diaphragmdiaphragm
1
2
3
4
5
6
7
8
9
10

9-10 posterior ribs are showing
9
About 8 posterior ribs are showing
8
Poor inspiration can crowd Poor inspiration can crowd lung markings producing lung markings producing pseudo-airspace diseasepseudo-airspace disease
With better inspiration, the “disease process” at the lung bases has cleared

Quality ControlQuality Control
77. . RotationRotation
– Medial ends of Medial ends of bilateral clavicles are bilateral clavicles are equidistant from the equidistant from the midline or vertebral midline or vertebral bodiesbodies


If spinous process appears closer to the right clavicle (red arrow), the patient is rotated toward their own left side
If spinous process appears closer to the left clavicle (red arrow), the patient is rotated toward their own right side

Quality ControlQuality Control
8.8. AngulationAngulation
– Clavicle should lay Clavicle should lay over 3over 3rdrd rib rib
1
2
3

Pitfall Due to AngulationPitfall Due to Angulation
A film which is apical lordotic (beam is angled up toward A film which is apical lordotic (beam is angled up toward head) will have an unusually shaped heart and the usually head) will have an unusually shaped heart and the usually
sharp border of the left hemidiaphragm will be absentsharp border of the left hemidiaphragm will be absent
Apical lordotic Same patient, not lordotic

FindingsFindings
99. . Soft tissue and bony Soft tissue and bony structuresstructures– Check for Check for
SymmetrySymmetry
DeformitiesDeformities
FracturesFractures
MassesMasses
CalcificationsCalcifications
Lytic lesionsLytic lesions

FindingsFindings
1010. . MediastinumMediastinum– Check for Check for
CardiomegalyCardiomegaly
Mediastinal and Mediastinal and Hilar contours for Hilar contours for increase densities increase densities or deformitiesor deformities

Measurement of the cardiothoracic ratio.

Maximum transverse diameter of the heart on Maximum transverse diameter of the heart on a normal PA film is not more than 15.5cm in a normal PA film is not more than 15.5cm in adult males and 14.5cm in adult females.adult males and 14.5cm in adult females.
When the cardiothoracic ratio is used it When the cardiothoracic ratio is used it should not exceed 50%. should not exceed 50%.
A+B = the transverse diameter of the heart. A+B = the transverse diameter of the heart.
C= the transverse diameter of the thorax C= the transverse diameter of the thorax which is measured at the level of the which is measured at the level of the diaphragms from the inner ribsdiaphragms from the inner ribs
A+B divided by C = the cardiothoracic ratio A+B divided by C = the cardiothoracic ratio (CTR)(CTR)

FindingsFindings
1111. . DiaphragmsDiaphragms
– Check sharpness of Check sharpness of bordersborders
– Right is normally Right is normally higher than lefthigher than left
– Check for free air, Check for free air, gastric bubble, pleural gastric bubble, pleural effusionseffusions



FindingsFindings
1212. . The Lung Fields!The Lung Fields!– To help you determine To help you determine
abnormalities and their abnormalities and their location…location…
Use silhouettes of Use silhouettes of other thoracic other thoracic structuresstructures
Use fissuresUse fissures
L

Lung AnatomyLung Anatomy
Right LungRight Lung– Superior lobeSuperior lobe– Middle lobeMiddle lobe– Inferior lobeInferior lobe
Left LungLeft Lung– Superior lobeSuperior lobe– Inferior lobeInferior lobe

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
The right upper lobe The right upper lobe (RUL) occupies the (RUL) occupies the upper 1/3 of the right upper 1/3 of the right lung. lung.
Posteriorly, the RUL is Posteriorly, the RUL is adjacent to the first adjacent to the first three to five ribs. three to five ribs.
Anteriorly, the RUL Anteriorly, the RUL extends inferiorly as far extends inferiorly as far as the 4th right anterior as the 4th right anterior ribrib

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
The right middle The right middle lobe is typically the lobe is typically the smallest of the smallest of the three, and appears three, and appears triangular in shape, triangular in shape, being narrowest being narrowest near the hilumnear the hilum

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
The right lower lobe is the The right lower lobe is the largest of all three lobes, largest of all three lobes, separated from the others separated from the others by the major fissure.by the major fissure.Posteriorly, the RLL Posteriorly, the RLL extend as far superiorly as extend as far superiorly as the 6th thoracic vertebral the 6th thoracic vertebral body, and extends body, and extends inferiorly to the diaphragm. inferiorly to the diaphragm. Review of the lateral plain Review of the lateral plain film surprisingly shows the film surprisingly shows the superior extent of the RLL.superior extent of the RLL.

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
These lobes can be These lobes can be separated from one another separated from one another by two fissures.by two fissures.The minor fissure separates The minor fissure separates the RUL from the RML, and the RUL from the RML, and thus represents the visceral thus represents the visceral pleural surfaces of both of pleural surfaces of both of these lobes.these lobes.Oriented obliquely, the major Oriented obliquely, the major fissure extends posteriorly fissure extends posteriorly and superiorly approximately and superiorly approximately to the level of the fourth to the level of the fourth vertebral body. vertebral body.

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
The lobar architecture The lobar architecture of the left lung is of the left lung is slightly different than slightly different than the right.the right.
Because there is no Because there is no defined left minor defined left minor fissure, there are only fissure, there are only two lobes on the left; two lobes on the left; the left upper the left upper

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
Left lower lobesLeft lower lobes

Lung Anatomy on Chest X-rayLung Anatomy on Chest X-ray
These two lobes are These two lobes are separated by a major separated by a major fissure, identical to that fissure, identical to that seen on the right side, seen on the right side, although often slightly although often slightly more inferior in location.more inferior in location.The portion of the left The portion of the left lung that corresponds lung that corresponds anatomically to the right anatomically to the right middle lobe is middle lobe is incorporated into the left incorporated into the left upper lobe.upper lobe.

Chest Radiographic Patterns of Chest Radiographic Patterns of DiseasesDiseases
Air Space OpacityAir Space Opacity
Interstitial OpacityInterstitial Opacity
Nodules and MassesNodules and Masses
LymphadenopathyLymphadenopathy
Cysts and CavitiesCysts and Cavities
Lung VolumesLung Volumes
Pleural DiseasesPleural Diseases

AIR SPACE OPACITY /AIR SPACE OPACITY /ALVEOLAR ALVEOLAR
SHADOWINGSHADOWING The alveoli are filled with fluid or solid tissue The alveoli are filled with fluid or solid tissue
and appear as small separate rounded and appear as small separate rounded 6mm opacities in the early stages. 6mm opacities in the early stages.
The vessels are obscured and there may be The vessels are obscured and there may be an air bronchogram and silhouette sign.an air bronchogram and silhouette sign.
When the alveoli fill with fluid or other When the alveoli fill with fluid or other substances, it is called substances, it is called consolidationconsolidation

ComponentsComponents
Air bronchogram : air – filled bronchus Air bronchogram : air – filled bronchus sorrounded by airless lung.sorrounded by airless lung.
Confluent opacity extending to pleural Confluent opacity extending to pleural surfaces.surfaces.
Segmental distributionSegmental distribution
Blood (hemorrhage)Blood (hemorrhage)

Water (edema) i.e. hydrostatic or non – Water (edema) i.e. hydrostatic or non – cardiogeniccardiogenic
Cells (tumor)Cells (tumor)
Protein/fat: alveolar proteinosis and lipoid Protein/fat: alveolar proteinosis and lipoid pneumoniapneumonia
Pus (pneumonia)Pus (pneumonia)

Air bronchograms. The bronchi in the upper lobes are visible as dark lines because the surrounding alveoli are filled with exudate due to pneumonia.

LUL PNEUMONIALUL PNEUMONIA

Interstitial opacityInterstitial opacityThis is due to a disease in the This is due to a disease in the
interstitium .i.e. the tissue in which interstitium .i.e. the tissue in which the blood vessels and bronchi lie the blood vessels and bronchi lie within the lungs. This leads to a non within the lungs. This leads to a non homogenous pattern of shadowing homogenous pattern of shadowing which may take many forms.which may take many forms.
The normally visualised blood vessels The normally visualised blood vessels become ill defined or obscured and may become ill defined or obscured and may be diffuse or localisedbe diffuse or localised..

HallmarksHallmarks : :
Small, well – defined nodulesSmall, well – defined nodules
Lines i.e. interlobular septal thickening or Lines i.e. interlobular septal thickening or fibrosisfibrosis
Reticulation . Reticulation .
Idiopathic interstitial pneumoniasIdiopathic interstitial pneumonias
Infections ( TB , Viruses)Infections ( TB , Viruses)

EdemaEdema
HemorrhageHemorrhage
Non – infectious inflammatory lesions e.g. Non – infectious inflammatory lesions e.g. scarcoidosisscarcoidosis
TumorTumor
Normal interstitiumNormal interstitium Interstitial diseaseInterstitial disease Reticulo nodular patternReticulo nodular pattern

Close up of interstitial shadowing in a patient with fibrosing alveolitis. Close up of interstitial shadowing in a patient with fibrosing alveolitis.
There is a nodular pattern super-imposed on a fine network of lines. There is a nodular pattern super-imposed on a fine network of lines.
Loss of vessels.Loss of vessels.

Nodules and MassesNodules and Masses
Nodule: any pulmonary lesion represented Nodule: any pulmonary lesion represented in a radiograph by a sharply defined, in a radiograph by a sharply defined, discrete nearly circular opacity 2 – 30 mm discrete nearly circular opacity 2 – 30 mm in diameterin diameter
Mass: larger than 3cmMass: larger than 3cm

Qualifies :Qualifies :
Single or multipleSingle or multiple
SizeSize
Border definitionBorder definition
Presence or absence of calcificationPresence or absence of calcification
LocationLocation

Well DefinedWell Defined
Ill DefinedIll Defined
CalcificationsCalcifications
MassMass

The solitary noduleThe solitary nodule

LymphadenopathyLymphadenopathy
Chronic abnormal enlargement of the lymph nodes Chronic abnormal enlargement of the lymph nodes
Non – specific presentationsNon – specific presentations
1.1. Mediastinal wideningMediastinal widening
2.2. Hilar prominenceHilar prominence
Specific patterns :Specific patterns :
1.1. Particular station enlargementParticular station enlargement

Right paratrachealRight paratracheal
lymphadenopathylymphadenopathy

Left Hilar LymphadenopathyLeft Hilar Lymphadenopathy

Cysts and CavitiesCysts and Cavities
Cyst:Cyst: abnormal pulmonary parenchymal abnormal pulmonary parenchymal space, not containing lung tissues but space, not containing lung tissues but filled with air and/or fluid, congenital or filled with air and/or fluid, congenital or acquired , with a wall thickness greater acquired , with a wall thickness greater than 1mmthan 1mm
Epithelial lining often presentEpithelial lining often present

CavityCavity: abnormal pulmonary parenchymal : abnormal pulmonary parenchymal space , not containing lung but filled with space , not containing lung but filled with air and / or fluid .air and / or fluid .
It is caused by tissue necrosis, with a It is caused by tissue necrosis, with a definitive wall greater than 1mm in definitive wall greater than 1mm in thickness and comprised of inflammatory thickness and comprised of inflammatory and / or neoplastic elements.and / or neoplastic elements.

Cysts and cavitiesCysts and cavities
Characterize:Characterize:
1.1. Wall thickness at the thickest portionWall thickness at the thickest portion
2.2. Inner liningInner lining
3.3. Presence/ absence of air/fluid levelPresence/ absence of air/fluid level
4.4. Number and locationNumber and location

Benign Lung Cyst :PCP PneumatoceleBenign Lung Cyst :PCP Pneumatocele
Uniform Wall ThicknessUniform Wall Thickness1mm1mmSmooth Inner liningSmooth Inner lining

Malignant Cavities: Squamous Cell CavitiesMalignant Cavities: Squamous Cell Cavities
Maximum Wall Thickness 16mmMaximum Wall Thickness 16mm
Irregular Inner LiningIrregular Inner Lining

Pleural EffusionPleural Effusion

Right Right Side Side
Pleural Pleural EffusioEffusio
nn

Fracture of posterior rib Fracture of posterior rib ##

cavitationcavitationFibrosisFibrosis
CalcificationsCalcifications
GranulomaGranuloma
((TuberculomaTuberculoma))
Pericardial EffusionPericardial Effusion
PleuralPleural
effusioneffusion
Hilar LymphadenopathyHilar Lymphadenopathy
ConsolidationConsolidation
Miliary ShadowingMiliary Shadowing
Manifestation of pulmonary tuberculosisManifestation of pulmonary tuberculosis

Pericardial effusionPericardial effusion

AtelectasisAtelectasis - - Collapse/ incomplete expansion.Collapse/ incomplete expansion.
Endobronchial– mucus plug/ tumor.Endobronchial– mucus plug/ tumor.Extrinsic compression– mass/ effusion/ ascites.Extrinsic compression– mass/ effusion/ ascites.Scarring-- post TB/ Radiation/ inflammation.Scarring-- post TB/ Radiation/ inflammation.Linear/curved/wedge(apex-hilum) density with hilar/tracheal/media-Linear/curved/wedge(apex-hilum) density with hilar/tracheal/media-stinal/diaphragm deviation with volume loss +/- compensatory stinal/diaphragm deviation with volume loss +/- compensatory hyper- inflation.hyper- inflation.

Right upper and lower lobe Right upper and lower lobe atelectasisatelectasis

Right middle lobe pneumoniaRight middle lobe pneumonia

Type of pneumoniaType of pneumoniaLobar - Lobar - entire lobe consolidated and air bronchograms entire lobe consolidated and air bronchograms commoncommon
Lobular - Lobular - multifocal, patchy.multifocal, patchy.
Interstitial - Interstitial - starts perihilar ,can become confluent starts perihilar ,can become confluent and/or patchy as disease progresses, no air and/or patchy as disease progresses, no air bronchogramsbronchograms
Aspiration pneumoniaAspiration pneumonia
Diffuse pulmonary infections - Diffuse pulmonary infections - nosocomial nosocomial (Pseudomonas, debilitated, mechanical vent, high (Pseudomonas, debilitated, mechanical vent, high mortality rate, patchy opacities, cavitation, immuno-mortality rate, patchy opacities, cavitation, immuno-compromised host(bacterial, fungal, Pneumocystic compromised host(bacterial, fungal, Pneumocystic Carinii PneumoniaCarinii Pneumonia))

Major differentiating factors between atelectasis and Major differentiating factors between atelectasis and pneumoniapneumonia
Atelectasis Atelectasis PneumoniaPneumonia
Volume LossVolume Loss normal or increased volume normal or increased volume
Associated Ipsilateral Shift no shift/ contralateral shiftAssociated Ipsilateral Shift no shift/ contralateral shift
Linear, Wedge-Shaped air space processLinear, Wedge-Shaped air space process
Apex at HilumApex at Hilum not centered at hilum not centered at hilum
Air bronchograms can occur in both.Air bronchograms can occur in both.

DextrocardiaDextrocardia

Aortic AneurysmAortic Aneurysm

Putting It Into PracticePutting It Into Practice

Case 1Case 1


A single, 3cm relatively thin-walled cavity is noted in the left A single, 3cm relatively thin-walled cavity is noted in the left midlung. This finding is most typical of squamous cell midlung. This finding is most typical of squamous cell carcinoma (SCC). One-third of SCC masses show cavitationcarcinoma (SCC). One-third of SCC masses show cavitation

Case 2Case 2


LUL Atelectasis: Loss of heart borders/silhouetting. LUL Atelectasis: Loss of heart borders/silhouetting. Notice over inflation on unaffected lungNotice over inflation on unaffected lung

Case 3Case 3


Right Middle and Left Upper Lobe PneumoniaRight Middle and Left Upper Lobe Pneumonia

Case 4Case 4


Cavitation:cystic changes in the area of consolidation due to Cavitation:cystic changes in the area of consolidation due to the bacterial destruction of lung tissue. Notice air fluid level.the bacterial destruction of lung tissue. Notice air fluid level.

CavitationCavitation

Case 5Case 5


TuberculosisTuberculosis

Case 6Case 6


COPD: increase in heart diameter, flattening of the COPD: increase in heart diameter, flattening of the diaphragm, and increase in the size of the retrosternal air diaphragm, and increase in the size of the retrosternal air space. In addition the upper lobes will become hyperlucent space. In addition the upper lobes will become hyperlucent due to destruction of the lung tissue.due to destruction of the lung tissue.

Chronic emphysema effect on the lungsChronic emphysema effect on the lungs

Case 7Case 7


Pseudotumor: fluid has filled the minor fissure creating a Pseudotumor: fluid has filled the minor fissure creating a density that resembles a tumor (arrow). Recall that fluid and soft density that resembles a tumor (arrow). Recall that fluid and soft tissue are indistinguishable on plain film. Further analysis, tissue are indistinguishable on plain film. Further analysis, however, reveals a classic pleural effusion in the right pleura. however, reveals a classic pleural effusion in the right pleura. Note the right lateral gutter is blunted and the right diaphram is Note the right lateral gutter is blunted and the right diaphram is obscurred.obscurred.

Case 8Case 8


Pneumonia:a large pneumonia consolidation in the right Pneumonia:a large pneumonia consolidation in the right lower lobe. Knowledge of lobar and segmental anatomy is lower lobe. Knowledge of lobar and segmental anatomy is important in identifying the location of the infectionimportant in identifying the location of the infection

Case 9Case 9


CHF:a great deal of accentuated interstitial CHF:a great deal of accentuated interstitial markings, Curly lines, and an enlarged heart. markings, Curly lines, and an enlarged heart. Normally indistinct upper lobe vessels are Normally indistinct upper lobe vessels are prominent but are also masked by interstitial prominent but are also masked by interstitial edema.edema.

24 hours after diuretic therapy24 hours after diuretic therapy

Case 10Case 10


Chest wall lesion: arising off the chest wall and not the lungChest wall lesion: arising off the chest wall and not the lung

Case 11Case 11


Pleural effusion: Note loss of left hemidiaphragm. Fluid Pleural effusion: Note loss of left hemidiaphragm. Fluid drained via thoracentesisdrained via thoracentesis

Case 12Case 12


Lung MassLung Mass

Case 13Case 13


Small Pneumothorax: LULSmall Pneumothorax: LUL

Case 15Case 15


Right Middle Lobe Pneumothorax: complete lobar collapseRight Middle Lobe Pneumothorax: complete lobar collapse

Post chest tube insertion and re-expansionPost chest tube insertion and re-expansion

Case 16Case 16


Metastatic Lung Cancer: multiple nodules seenMetastatic Lung Cancer: multiple nodules seen

Case 17Case 17


Right upper lower lobe pulmonary noduleRight upper lower lobe pulmonary nodule

Case 18Case 18


TuberculosisTuberculosis

Case 19Case 19


Perihilar mass: Hodgkin’s diseasePerihilar mass: Hodgkin’s disease

Case 20Case 20


Widened Mediastinum: Aortic Dissection Widened Mediastinum: Aortic Dissection

Case 21Case 21


Pulmonary artery stenosis with cardiomegally Pulmonary artery stenosis with cardiomegally likely secondary to stenosis.likely secondary to stenosis.

PA view: RML consolidation and loss of right heart silhouette
Lateral View: RML wedge shaped consolidation
RML pneumonia

RUL infiltrate / consolidation, bordered by minor fissure inferiorly
Patchy LLL infiltrate that obscures the left hemidiaphragm; right and left heart borders obscured
RUL and LLL pneumonia

Multiple bilateral cavitary lesions with air-fluid levels c/w pulmonary abscesses
Tuberculosis

RML consolidation that appears wedge shaped on lateral view
RML pneumonia

RLL infiltrate / consolidation
RLL pneumonia

Patient BIBA to ER s/p airplane crash.
Widened mediastinum
Concern for aortic injury

Obscuring of the right and left heart borders; infiltrate at the bases
Bilateral aspiration pneumonia

Diffuse bilateral fluffy interstitial infiltrates
Pneumocystis carinii pneumonia

LUL pneumonia

Left lung opacity
Later diagnosed as lung cancer

Cardiomegaly, increased pulmonary vascular markings, fluid in the horizontal fissure
CHF

Kerley B linesKerley B lines

The EndThe End
Thank youThank you