
PLACENTAL TRANSFER OF FATTY ACIDS AND FETAL … · FATP, FAT Lipase LPL TG TG TG LPL, Lipoprotein...
25
PLACENTAL TRANSFER OF FATTY ACIDS AND FETAL IMPLICATIONS Dr. Elvira Larqué [email protected] Department of Physiology Unversity of Murcia (Spain) Note: for non-commercial purposes only
Transcript of PLACENTAL TRANSFER OF FATTY ACIDS AND FETAL … · FATP, FAT Lipase LPL TG TG TG LPL, Lipoprotein...

PLACENTAL TRANSFER OF FATTY ACIDS AND FETAL IMPLICATIONS
Dr. Elvira Larqué[email protected]
Department of PhysiologyUnversity of Murcia (Spain)
Note: for non-commercial purposes only

FETAL PROGRAMMING
BRAIN60% FAT (dry matter)
~ 40% LONG CHAIN POLYUNSATURATED FATTY ACIDS (LC-PUFA):
- 15% DOCOSAHEΧAENOIC ACID (DHA,22:6 n-3 ): Neuronal development
- 10% ARACHIDONIC ACID (AA, 20:4 n-6 ) : Infantile Growth

Polyunsaturated FA Synthesis
22:6ωωωω-3docosahexaenoic
18:2ωωωω-6 18:3ωωωω-3αααα-linolenic
18:3ωωωω-6γγγγ-linolenic
20:4ωωωω-6arachidonic
20:5ωωωω-3eicosapentaenoic
∆∆∆∆6-desaturase
elongase & ∆∆∆∆5−−−−desaturase & elongase
PROSTA-GLANDINS
MEMBRANES
linoleic
EFA and LC-PUFA PROVIDED BY PLACENTAL TRANSFER
EFA:
LC-PUFA:

FFA
FFA
PasiveDiffusion
Facilitated
Transport
Maternal circulation
Trofoblast cytosol FFA FFA
membrane
FFA
Lipoprotein
R
?
PLA2 Lipases
AGL
Lipase
EL
PL
EL, Endothelial lipase
Fatty Acid Placental Uptake
FABPpmFATP, FAT
Lipase
LPL
TG TG
TG
LPL, Lipoprotein lipase

• Placental transfer of fatty acids is a complex processthat includes theirbinding to membraneand cytosolic proteincarriers
Fatty Acid PlacentalTransfer
p-FABPpm (placental plasma fatty acid binding protein) not sequenced??.
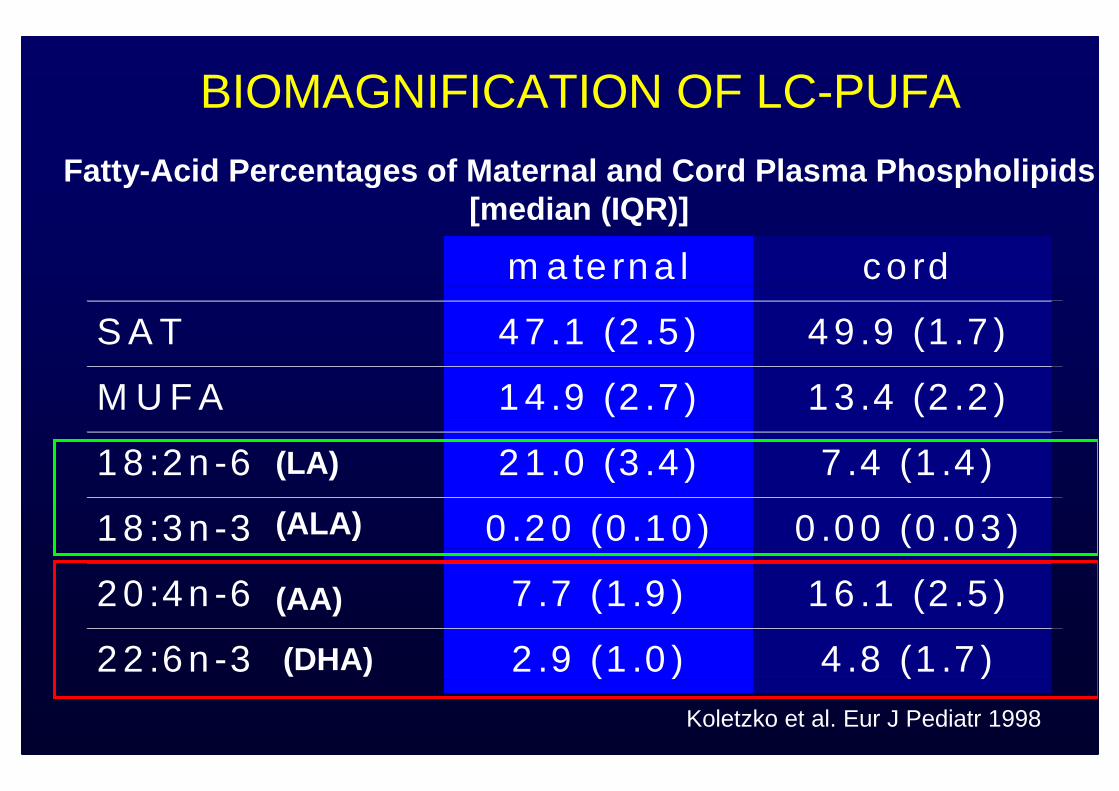
m a te rn a l co rd
S A T 4 7 .1 (2 .5 ) 4 9 .9 (1 .7 )
M U F A 1 4 .9 (2 .7 ) 1 3 .4 (2 .2 )
1 8 :2 n -6 2 1 .0 (3 .4 ) 7 .4 (1 .4 )
1 8 :3 n -3 0 .2 0 (0 .1 0 ) 0 .0 0 (0 .0 3 )
2 0 :4 n -6 7 .7 (1 .9 ) 1 6 .1 (2 .5 )
2 2 :6 n -3 2 .9 (1 .0 ) 4 .8 (1 .7 )
Fatty- Acid Percentages of Maternal and Cord Plasma Phosph olipids [median (IQR)]
Koletzko et al. Eur J Pediatr 1998
BIOMAGNIFICATION OF LC-PUFA
(LA)
(ALA)
(AA)
(DHA)

PERILIP PROJECT (FP6 EU)
Material y methods
Single oral dose of stable isotope tracer in a sugar cube:- 13C-PA (Palmitic acid: saturated FA): 0.5 mg/Kg- 13C-OA (Oleic acid: monounsaturated FA): 0.5 mg/Kg- 13C-LA (Linoleic acid: essential FA): 0.5 mg/kg
- 13C-DHA (Docosahexaenoic acid, LC-PUFA): 0.1 mg/kg
� Study 4 hours before cesarean section (n=4)
� Study 12 hours before cesarean section (n=11)
In vivo evaluation of the placental transfer of fatty acid slabeled with stable isotopes in humans
Aim
Stable Isotope Study on FA Placental Transfer

4h FA Tracer Study
-4 -3 -2 -1 0 10,0
0,2
0,4
0,6
0,8
1,0
DHA
LA
OA
PA
13C
-AP
E (
%)
time (h)
-4 -3 -2 -1 0 10,0
0,2
0,4
0,6
0,8
1,0
13C
-AP
E (
%)
time (h)
-4 -3 -2 -1 0 10,00
0,01
0,02
0,03
0,04
13C
-AP
E (
%)
time (h)
Appearance of 13C-FA enrichment in maternal plasma Maternal Plasma TG Maternal Plasma FFA
Maternal Plasma PLNo enrichment in Maternal CholesterolEsters
N=4 (Larqué et al. J. Lipid Res., 2003)
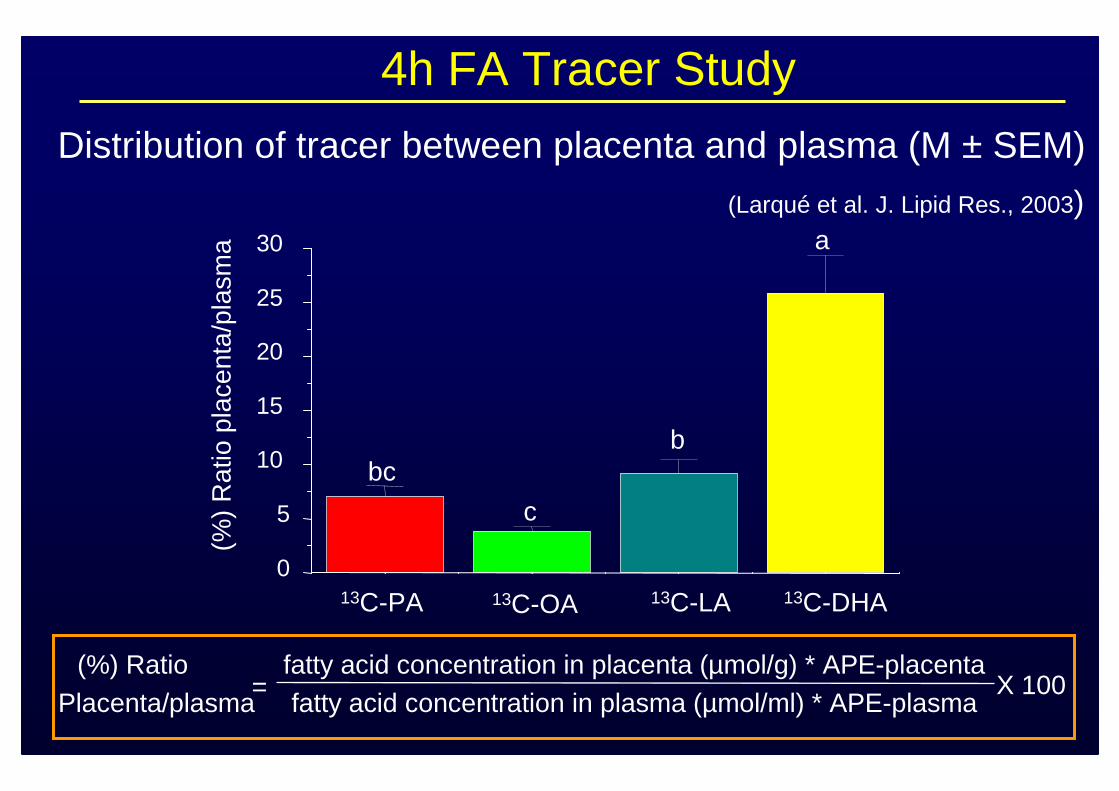
Placenta/plasma fatty acid concentration in plasma (µmol/ml) * APE-plasma(%) Ratio fatty acid concentration in placenta (µmol/g) * APE-placenta
X 100
Distribution of tracer between placenta and plasma (M ± SEM)
13C-PA 13C-OA 13C-LA 13C-DHA0
5
10
15
20
25
30(%
) R
atio
pla
cent
a/pl
asm
a
bc
c
b
a
=
4h FA Tracer Study
(Larqué et al. J. Lipid Res., 2003)

Design of 12h FA tracer StudySubjects: 11 pregnant women, elective caesarian section
weight: 78 ± 8 kg height: 161± 6 cmage: 33 ± 4 years gestation: 39.8 ± 1 wk
Oral application of stable isotope tracer in a sugar cube:• palmitic acid (13C-PA): 0.5 mg/kg • oleic acid (13C-OA): 0.5 mg/kg• linoleic acid (13C-LA): 0.5 mg/kg• docosahexaenoic acid (13C-DHA): 0.1 mg/kg
- Maternal blood: 0h, 9h, 10,11h, 12h (c-section), 13h - Placenta collection and venous cord blood
13C-enrichment of FA by gas chromatography combustion isotope ratio mass spectrometry (GC-C-IRMS)
Tracer administration (12h before caesarean section )

basal 9 10 11 12
0
2
4
6
8
10
12
14
(h)
basal 9 10 11 12
0
0,2
0,4
0,6
0,8
1
(h)
basal 9 10 11 12
0
2
4
6
8
10
12
14
16
(h)
basal 9 10 11 12
0
2
4
6
8
10
12
14
(h)
TGPL
FFACE
C-L
A(µ
mol
/l)13 C
-DH
A(µ
mol
/l)13
C-P
A(µ
mol
/l)13
C-O
A(µ
mol
/l)13
SATURATED FA MONOUNSATURATED FA
ESSENTIAL FA
a a
b bb
bcbc
aa
a
ab
bb
bb
LC-PUFA
P < 0.05
13C-FA CONCENTRATION IN MATERNAL PLASMA12
h F
A tr
acer
stud
y

0
2
4
6
8
10
12
14
16
PL
NEFA
TG
EC
13C-FA enrichment in placental TG and NEFA tended to be h igh
Phospholipids constituted about 80-90% of FA in placent a
13C-FA Concentration in Placenta
12h
a
a
a
ab
bb
bb b bcbbcc
C-F
A (
µm
ol/l)
13
13C-OA 13C-LA 13C-DHA13C-PA
Mean ± SD, P < 0.05
12h
FA
trac
erst
udy

12h FA tracer study
(%)
Rat
io p
lace
nta/
mat
erna
l pla
sma
0
50
100
150
200
250
300
350
400
450
500
4h
α=40,17 (DHA)
α=6,71( LA)α=4,75 (PA)α=4,18 (OA)
*
12h
* P<0,05
*
α = slope
(Gil-Sánchez, Larqué et al. Am. J. Clin. Nutr., 2010)
Distribution placenta/maternal plasma (M ± SEM)
0
10
20
30
40
50
(%)
Rat
io p
lace
nta/
mat
erna
l pla
sma
a
bb
b
Different letters: P<0,05
Placenta
13C-PA 13C-OA 13C-LA 13C-DHA
Comparison 4h vs 12h

Cord/plasma AUC FA concentration in plasma (µmol/ml) * APE-mat. plasma
(%) Ratio FA concentration in cord (µmol/g) * APE-cord plasmaX 100
Distribution Cord/Maternal Plasma
13C-PA 13C-OA 13C-LA 13C-DHA
(%)
Rat
io c
ord/
plas
ma
AU
C
a
bb b
Mean ± SD, P < 0.05
=
0
0,5
1
1,5
2
12h
12h
FA
trac
erst
udy

0
520
21
22
23
01234567
%-w
t/wt
Control 400µg MTHF 0.5mgDHA DHA+MTHF
PROYECTO NUHEAL: Placental PL
a a
b b
DHA AA
• Supplementation of 136 Spanish pregnant women from wk 20 to delivery
No significant changes in placental mRNA expression of FATP-1, FATP-4, FATP-6, FAT, FABPpm, H-FABP, B-FABP, A-FABP among the groups

NUHEAL: Correlations placental carriers-Placental PL
0
50
100
150
200
250
0 2 4 6 8 10
0102030405060708090
100
0 2 4 6 8 10
FA
TP
-1 (
AU
)
R = + 0.364; P = 0.001 R = + 0.387; P = 0.0007
FA
TP
-4 (
AU
)DHA (%) DHA (%)
DHA (%) IN MATERNAL PLASMA PL CORRELATES WITH PLACENTAL PROTEINS FATP-1 (r=0.32, p=0.001) AND FATP-4 (r=0.23, p=0.012)
(Larqué et al. Am J Clin Nutr. 2006)

FA
TP
-4 p
lace
nta
(AU
)
DHA(%) cord blood PL
r = + 0.20; P = 0.032*
(Larqué et al. Am J Clin Nutr. 2006)
0102030405060708090
100
0 5 10 15 20
NUHEAL: Correlations placental FA carriers-CordPlasma PL

Normal plasma LC-PUFA in women with gestational diabetes mellitus, but low erytrocyte PL LC-PUFA in their babies (Wijendran et al. 2000)
Pregestational or gestational diabetes mellitus was found toadversely affect attention span and motor functions of offspring at
school age (Ornoy et al. 2001)
GESTATIONAL DIABETES MELLITUS
Delayed brain maturity in these newborns compared to controls?
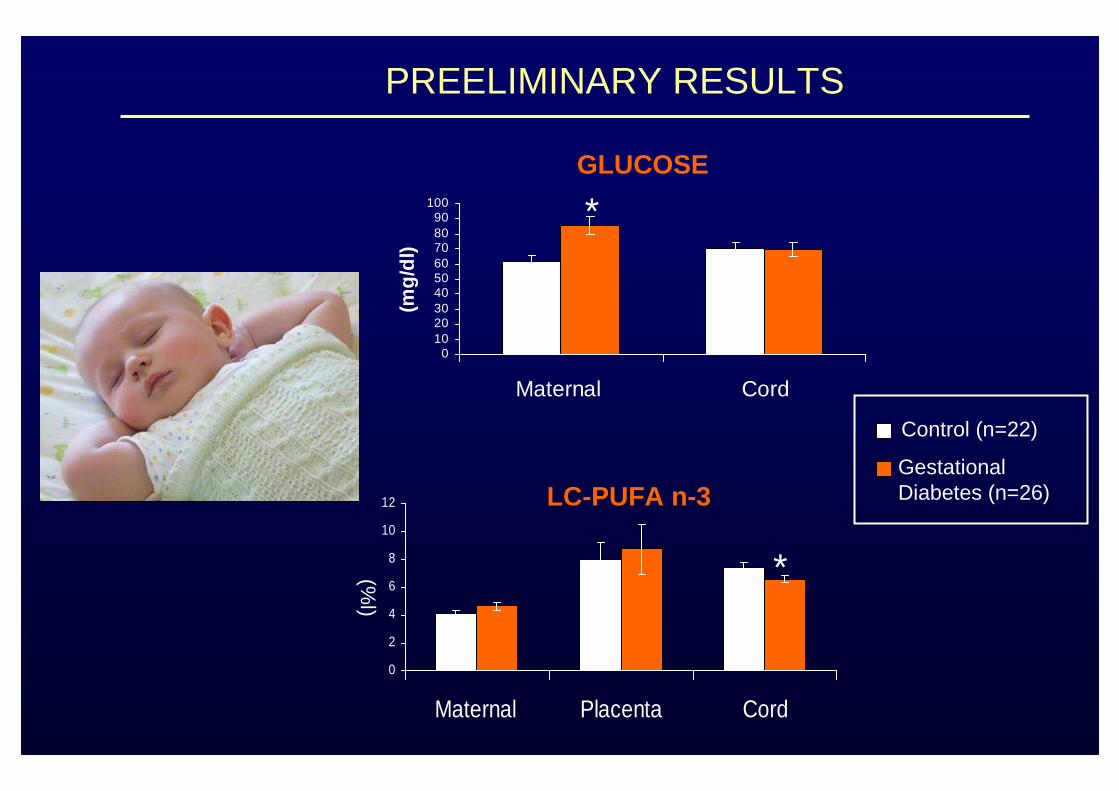
PREELIMINARY RESULTS
0102030405060708090
100
Maternal Cord(m
g/dl
)Control (n=22)
GestationalDiabetes (n=26)
*GLUCOSE
LC-PUFA n-3
*(%l)
0
2
4
6
8
10
12
Maternal Placenta Cord

**
DHA P =0.062
PREELIMINARY RESULTS
VENOUS CORD BLOOD
Control (n=22)
Gestational diabetes (n=26)
(%)
*
**
(%)
SATURATED (SFA)
EFA, LC-PUFA n-3
0
5
10
15
20
25
30
EFA LC-PUFA LC-PUFA n-3 DHA
0
5
10
15
20
25
30
35
40
45
SFA MUFA PUFA
PLACENTAL TRANSFER OF LABELED FA IN GESTATIONAL DIABETES ON GOING

NEURONAL DEVELOPMENT IN BABIES FROM GESTATIONAL
DIABETES MOTHERS DURING THE 1º YEAR OF LIFE
•Bayleys test (6 months and 12 months)
• Sleep/wake cycles by actigraphy methods
• Evaluation of circadian rhythms of temperatureusing temperature sensors.

Ondas medias de temperatura de la piel
32,00
32,50
33,00
33,50
34,00
34,50
35,00
35,50
36,00
9:00
10:2
0
11:4
0
13:0
0
14:2
0
15:4
0
17:0
0
18:2
0
19:4
0
21:0
0
22:2
0
23:4
0
1:00
2:20
3:40
5:00
6:20
7:40
Hora del día (hh:mm)
Tem
pera
tura
(ºC
)
15 días
30 días
90 días
Actimeter
EVOLUTION OF CHRONOBIOLOGICAL RHYTHMS
Temperaturesensor

32,0
32,5
33,0
33,5
34,0
34,5
35,0
35,5
15 days 30 days 3 months 12 years 20 years
Te
mp
era
ture
ºC
Age
Mesor
Different letters indicate significant differences by repeated measures ANOVA (for 15 days, 30 days and 3 months comparisons). Different numbers indicate significant differences when comparing babies (3 months) with child and adult groups.
EVOLUTION OF CORE BODY TEMPERATURE
ab a
b1
22
0,0
0,5
1,0
1,5
2,0
2,5
15 days 30 days 3 months 12 years 20 years
Te
mp
era
tu
re º
C
Age
M5-L10 Values
a
b1
1
2
ab
PREELIMINAR RESULTS
MEAN OF TEMPERATURE AMPLITUD OF TEMPERATURE
Sarabia et al. 2009. Acta Physiologica, 195 (667):101

Financial support by Alexander von Humboldt Foundation, HERO S.L. and by the Commission of the European Communities, within the FP 6 (PERILIP PROJECT and NUHEAL PROJECT).
This presentation does not necessarily reflect the views of the Commission and in no way anticipates its future policy in this area. Elvira Larqué is a recipient of the ESPGHAN Award for Young Investigators. Budapest. 2009.
Thank you for your kind attention!!!!

University of Murcia (SPAIN)Ana Pagán
María SabaterJ.A. Madrid
Salvador Zamora
UniversityUniversity ofof Murcia Murcia (SPAIN)(SPAIN)
Ana PagánMaría SabaterJ.A. Madrid
Salvador Zamora
Pediatric ServiceArrixaca Hospital
Murcia (Spain)Matilde ZornozaSilvia FuentesVicente Bosch
Manuel Sánchez-Solís
PediatricPediatric ServiceServiceArrixacaArrixaca HospitalHospital
Murcia (Murcia (SpainSpain))Matilde ZornozaSilvia FuentesVicente Bosch
Manuel Sánchez-Solís
Gynecology ServiceArrixaca Hospital
Murcia (SPAIN)Alfonso Gil-SánchezMaría Teresa PriteoJosé Eliseo BlancoJuan José Parrilla
GynecologyGynecology ServiceServiceArrixacaArrixaca Hospital Hospital
Murcia (SPAIN)Murcia (SPAIN)Alfonso Gil-SánchezMaría Teresa PriteoJosé Eliseo BlancoJuan José Parrilla
LMU Munich(GERMANY)Berthold Koletzko
Hans DemmelmairFabianne Hanebut
All staff
LMU MunichLMU Munich(GERMANY)(GERMANY)
Berthold KoletzkoHans DemmelmairFabianne Hanebut
All staff
THANK YOU !


















