PICTURE Study P lace of Reveal I n the C are pathway and T reatment of patients with U nexplained R...
18
PICTURE Study P lace of Reveal I n the C are pathway and T reatment of patients with U nexplained R ecurrent SyncopE
-
Upload
emily-phelps -
Category
Documents
-
view
217 -
download
1
Transcript of PICTURE Study P lace of Reveal I n the C are pathway and T reatment of patients with U nexplained R...

PICTURE Study
Place of Reveal In the Care pathway and Treatment
of patients with Unexplained Recurrent SyncopE

SYNCOPE – Background
• Syncope is common in the general population1
• Syncope accounts for 3-5% of Emergency Department (ED) visits and 1-3% of all hospital admissions2,3
• Cardiac syncope doubled the risk of death from any cause4

Challenges in Diagnosing Unexplained Syncope
• Occurrence of syncope tends to be unpredictable, observers are unlikely to have the opportunity to record ECGs at the time of an event5
• Gold standard of diagnosis: when a correlation between the symptoms and a documented arrhythmia is recorded6

What did PICTURE aim to do?
• The PICTURE registry aimed to collect information on the use of the Reveal® ICM in the patient care pathway and to investigate the effectiveness of the Reveal ICM in the diagnosis of unexplained recurrent syncope and pre-syncope in everyday clinical practice
• PICTURE was a prospective, multi-center, observational post-marketing study conducted from November 2006 until October 2009
• Data was gathered after the publication of the 2004 ESC guidelines and before the new 2009 version became available

• To evaluate the time to diagnosis in relation to the timing of the Reveal® ICM implant
PICTURE: Primary Objective
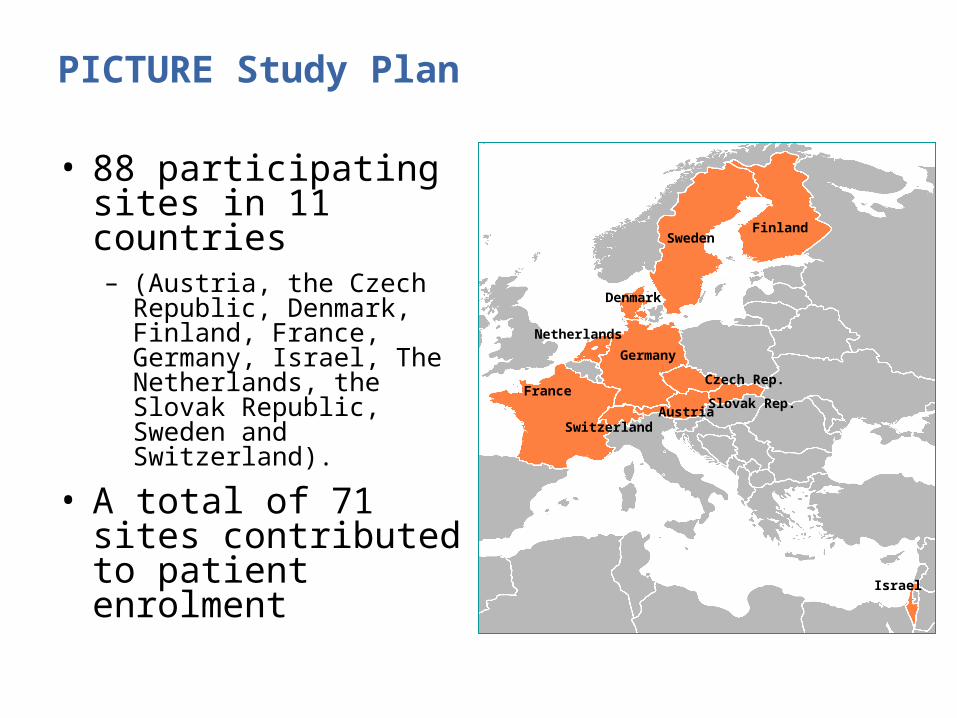
PICTURE Study Plan
• 88 participating sites in 11 countries – (Austria, the Czech
Republic, Denmark, Finland, France, Germany, Israel, The Netherlands, the Slovak Republic, Sweden and Switzerland).
• A total of 71 sites contributed to patient enrolment
Germany
SwedenFinland
Denmark
Netherlands
AustriaSlovak Rep.
Israel
FranceCzech Rep.
Switzerland

• Patients were eligible if they had recurrent unexplained syncope or pre-syncope
• Patients were followed up until the first recurrence of a syncopal event leading to a diagnosis or for at least 1 year
Study Methods

• 650 patients enrolled (2006-2008)
– 570 patients followed-up
• Average Follow-Up time: 10±6 months
Study Methods
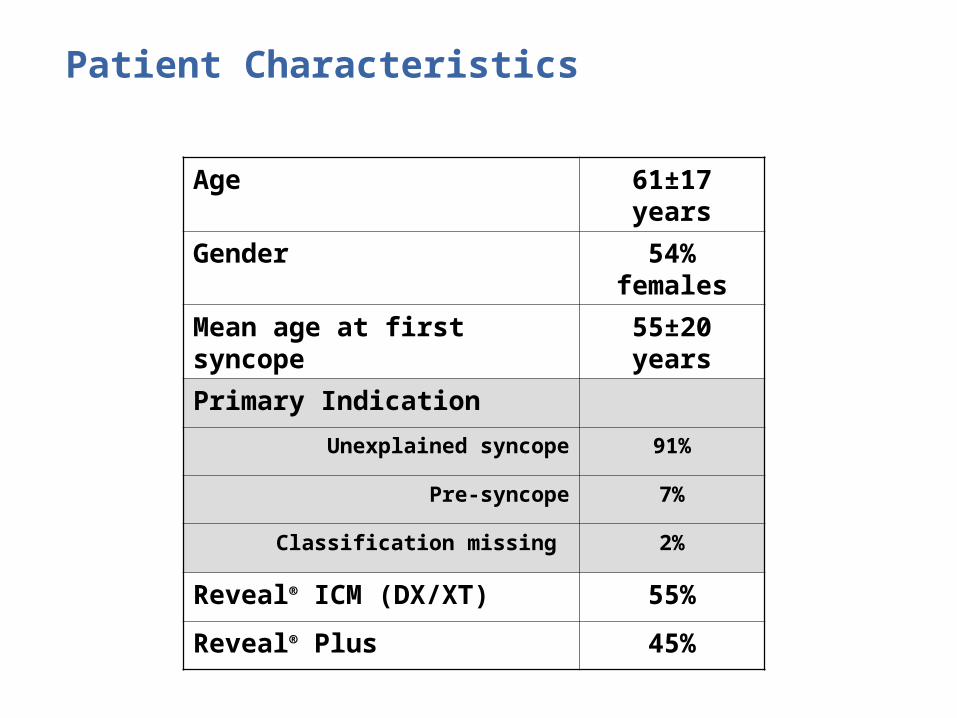
Patient Characteristics
Age 61±17 years
Gender 54% females
Mean age at first syncope
55±20 years
Primary IndicationUnexplained syncope 91%
Pre-syncope 7%
Classification missing 2%
Reveal® ICM (DX/XT) 55%
Reveal® Plus 45%

Physicians Consulted and Diagnostic Tests Performed (before Reveal® ICM
implant)5
• Overall, patients had seen an average of 3 different specialists for management of their syncope
• Most patients (70%) had been hospitalized at least once for syncope,
– one third (36%) of these patients had experienced significant trauma in association with a syncopal episode

Diagnostic Tests Performed Before Reveal® ICM implant5
Total recruitment 570 (100%)
Standard ECG 556 (98%)
Echocardiography 490 (86%)
Basic laboratory tests 488 (86%)
Ambulatory ECG monitoring 382 (67%)
In-hospital ECG monitoring 311 (55%)
Exercise testing 297 (52%)
Orthostatic blood pressure measurements
275 (48%)
MRI / CT scan 267 (47%)
Neurological or psychiatric evaluation
270 (47%)
EEG 222 (39%)
Carotid sinus massage 205 (36%)
Tilt test 201 (35%)
Electrophysiology testing 144 (25%)
Coronary angiography 133 (23%)
External loop recording 67 (12%)
ATP test 15 (3%)
Other tests 52 (9%)
No tests performed 1 (0%)
•The median number oftests performed per patient in the total study population was 13 (inter-quartile range 9 - 20)
”No studies evaluated the use of brain imaging for syncope.CT or MRI in uncomplicated syncope should be avoided.”6

Results5
• During follow-up,
– 218 patients (38%) had a recurrence of syncope within 12 months (shaded area)
• Reveal® ICMs guided the diagnosis in 170 (78%) patients with recurrent syncope, 75% of these patients had cardiac causes.
Blue Line: time to syncopal episode Red Line: time to syncopal episode where Reveal® ICMs played a role in the diagnosis
*Patients were followed for a maximum of 720 days
*

Treatment of Patients with Episodes5
Treatment decisions made in relation to syncope after diagnosis.

Treatment Statistics5
• Pacemaker implantations (86) 51%• Antiarrhythmic drug therapy 7%• ICD implantations 6%• Ablation therapy 5%• No specific treatment 18%

Conclusions
• PICTURE is the largest observational study to date to evaluate the usage and diagnostic effectiveness of ICMs in the everyday clinical work-up of patients with unexplained syncope5
• Reveal® ICMs contributed to establishing the mechanism of syncope in the vast majority of patients with a recurrence5
• The PICTURE study found a great diversity and number of physicians consulted, plus a large number of tests performed5
• The findings support the recommendation in the 2009 EXC/HRS Syncope Guidelines that the Reveal® ICMs should be implanted early rather than late in the evaluation of unexplained syncope6
References
1. Amer A, et al. Incidence and Mortality Rates of Syncope in the United States. The American Journal of Medicine (2009) 122, 181-188
2. Day SC. Et al. Evaluation and outcome of emergency room patients with transient loss of consciousness. Am J Med. 1982;73:15-23.
3. Silverstein MD et al. Patients with syncope admitted to medical intensive care units. JAMA. 1982;248:1185-1189.4.
4. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-885. [Framingham Study Population]
5. Edvardsson N, Frykman V, van Mechelin R, et al. Use of an implantable loop recorder to increase the diagnostic yield in unexplained syncope: results from the PICTURE registry. Europace. February 2011; 13(2):262-269.
6. Moya A. et al. Guidelines for the diagnosis and management of syncope (version 2009) The Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). European Heart Journal; 2009.

Indications9529 Reveal® XT and 9528 Reveal® DX Insertable Cardiac MonitorsThe Reveal® XT and Reveal® DX Insertable Cardiac Monitors are implantable patient-activated and automatically-activated monitoring systems that record subcutaneous ECG and are indicated in the following cases:-patients with clinical syndromes or situations at increased risk of cardiac arrhythmias-patients who experience transient symptoms such as dizziness, palpitation, syncope and chest pain, that may suggest a cardiac arrhythmia. 9539 Reveal® XT and 9538 Reveal® Patient AssistantsThe Reveal® XT and Reveal® Patient Assistants are intended for unsupervised patient use away from a hospital or clinic. The Patient Assistant activates one or more of the data management features in the Reveal® Insertable Cardiac Monitor:-To verify whether the implanted device has detected a suspected arrhythmia or device related event. (Model 9539 only)-To initiate recording of cardiac event data in the implanted device memory.
ContraindicationsThere are no known contraindications for the implant of the Reveal® XT or Reveal® DX Insertable Cardiac Monitors. However, the patient’s particular medical condition may dictate whether or not a subcutaneous, chronically implanted device can be tolerated.
Warnings/Precautions9529 Reveal® XT and 9528 Reveal® DX Insertable Cardiac MonitorsPatients with the Reveal® XT or Reveal® DX Insertable Cardiac Monitor should avoid sources of diathermy, high sources of radiation, electrosurgical cautery, external defibrillation, lithotripsy, therapeutic ultrasound and radiofrequency ablation to avoid electrical reset of the device, and/or inappropriate sensing. MRI scans should be performed only in a specified MR environment under specified conditions as described in the device manual. 9539 Reveal® XT and 9538 Reveal® Patient AssistantsOperation of the Model 9539 or 9538 Patient Assistant near sources of electromagnetic interference, such as cellular phones, computer monitors, etc., may adversely affect the performance of this device.
Potential ComplicationsPotential complications include, but are not limited to, device rejection phenomena (including local tissue reaction), device migration, infection, and erosion through the skin. See the device manual for detailed information regarding the implant procedure, indications, contraindications, warnings, precautions, and potential complications/adverse events. For further information, please call Medtronic at 1-800-328-2518 and/or consult Medtronic’s website at www.medtronic.com.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
Brief Statement

www.medtronic.com
World HeadquartersMedtronic, Inc.710 Medtronic parkwayMinneapolis, MN 55432-5604USATel: (763) 514-4000Fax: (763) 514-4879
Medtronic USA, Inc.Toll-free: 1 (800) 328-2518(24-hour technical support forphysicians and professionals)
© Medtronic, Inc. 2010Minneapolis, MNAll Rights Reserved02/2011