
Physiotherapy in Pediatric Orthopedics III: School Age and Adolescence Kristy Brundage, B.Sc. P.T.,...
40
Physiotherapy in Pediatric Orthopedics III: School Age and Adolescence Kristy Brundage, B.Sc. P.T., M.Sc.
-
Upload
rosa-morrison -
Category
Documents
-
view
232 -
download
3
Transcript of Physiotherapy in Pediatric Orthopedics III: School Age and Adolescence Kristy Brundage, B.Sc. P.T.,...

Physiotherapy in Pediatric Orthopedics III: School Age and
Adolescence
Kristy Brundage, B.Sc. P.T., M.Sc.

• Skeletal Changes and Growth
• Disorders– Scoliosis– Disorders of the Hip– Disorders of the Knee– Other: Fractures, Trauma
• Sports and Recreation

Skeletal Changes and Growth
Continued longitudinal and appositional bone growth dependent on:– Hormones– Nutrition– Mechanical factors
• growth spurts• proportions change at puberty

Development
• Mature patterns of running, jumping, throwing
• Increased coordination, eye-hand coordination, balance, endurance, attention span
• Develop sense of competitiveness

Disorders
• Scoliosis
• Hip
• Knee
• Fractures and Trauma

Scoliosis


Scoliosis
• Etiology: idiopathic, congenital, neuromuscular
• Plane of deformity: coronal, sagittal
• Levels of spine involved: cervical, thoracic, lumbar

Scoliosis - etiological subtypes
• Congenital: secondary to bony abnormality
• Neuromuscular: secondary to muscular weakness, imbalance
• Idiopathic: most common type; precise etiology unknown

Adolescent idiopathic scoliosis
• Asymptomatic
• Most common age presentation (10+ years)
• Not associated with back pain
• May have positive (extended) family hx
• Forward bend test – screening important
• Careful neurological exam mandatory

AdolescentIdiopathic Scoliosis -forward bendtest

Adolescent idiopathic scoliosis
• Goal of treatment is to prevent progression of curve
• Risk of progression related to growth remaining and curve magnitude
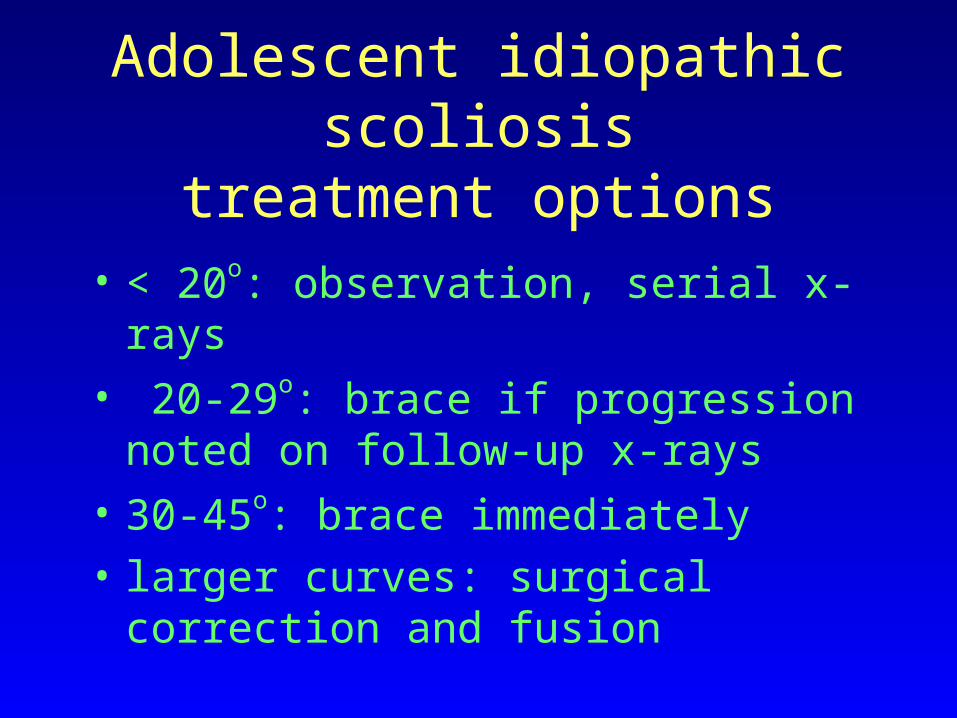
Adolescent idiopathic scoliosistreatment options
• < 20o: observation, serial x-rays
• 20-29o: brace if progression noted on follow-up x-rays
• 30-45o: brace immediately
• larger curves: surgical correction and fusion

Physiotherapy Treatment
• Historically
• Maintain mobility and strength in brace
• Post op

Disorders of the Hip
• Common
• Conditions unique to childhood
• Most have potential for early osteoarthritis
• Important to know what conditions are likely at various ages

Disorders of the HIP
• Legg Calve Perthes
• Slipped Capital Femoral Epiphysis

Legg-Perthes disease
• Initial presentation: pain, limp, normal x-rays (synovitis phase)
• More common (later) presentation: painless limp, abnormal x-rays
• Age 2-8 years• M>F

Legg-Perthes disease
• Etiology unknown
• Femoral head dies, resorbs, reforms over 18-24 months
• Treatment principle: maintain range, containment
• Observation, physio, bracing, surgery (osteotomy of femur or pelvis)



PT Management of LCP
• Crutch walking
• ROM: – With or without traction– all movements, BID– Passive, by parents– Within pain limits– Close monitoring

Slipped Capital Femoral Epiphysis
• Fracture through upper femoral growth plate
• Usually no identified trauma
• Pre-adolescent age group
Slipped Capital Femoral Epiphysis
• Usually obese
• Presentation: hip (groin) or knee pain (referred); acute or chronic
• Up to 40% are bilateral—monitor other hip

Slipped Capital Femoral Epiphysis: Treatment
• Surgical: Stabilize with insertion of screw across growth plate (encourage fusion of plate)
• Physio:– Post op care– Abductor strengthening

Disorders of the Knee
• Osgood Schlatter
• Patella femoral
• Discoid meniscus
• Osteochondritis dessicans

Osgood-Schlatter’s Disease
• Inflammation of the patellar tendon insertion (apophysitis) on the tibial tubercle
• ?from rapid growth of long bone, microavulsion, repetitive stress
• Presents as pain, swelling, prominence of tibial tubercle, occasionally limp

Osgood-Schlatter Disease: Treatment
• Analgesics/anti-inflammatories• Ice (massage)• Rest, activity modification (no jumping, squatting)• ?stretching and strengthening• ?ultrasound• **self limiting
ALSO: Sinding Larsen Johansson, Sever’s

Patella Femoral Syndrome
• Most common complaint of young athlete
• SPECTRUM
• Malalignment and maltracking
• Causes:– anatomical factors– acquired factors

PFS: Treatment
• PHYSIO:– Rest/activity modification– strengthening– Stretching– Other: orthotics, bracing, taping
• SURGICAL:– Lateral release– Patellar realignment

Discoid Lateral Meniscus
• Uncommon, but important diagnostically• Lateral meniscus undeveloped, remains
thick, disc shaped• Presents as joint line tenderness, decreased
ROM, swelling and snap on flexion-extension
• Rx is surgical removal with post op rehab (ROM, quads)

Osteochondritis Dessicans• Usually medial femoral condyle
• Necrosis of segment of articular bone and its overlying cartilage, often resulting in separation of fragment—intrarticular loose body.
• Presents as pain, swelling, giving way

Osteochondritis Dessicans: Treatment
• Rest +/- cast
• Surgical:– removal of loose fragment– resorbing pin
• Physio:– Post op– ROM, strengthening, retraining

Trauma and Fractures• Upper Extremity:
– Acromioclavicular
– Clavicle fracture
– # upper humerus
– Subluxation of G-H joint
– Elbow fractures: supracondylar
– Pulled elbow
– Wrists fractures: torus, both bones
– Hand: scaphoid, gamekeepers

Trauma and Fractures
• Lower Extremity:– Stress fractures– Snapping hip– #’s of femur, tibia– Ligamentous injury– Jumper’s knee– Growth plate #’s of distal tibia and fibula

Sports and Recreation
1. Team/competitive: school or community, coach +/-trainer, demanding, may involve contact,
2. Individual: recreational or training, with or without coach, protective equipment inconsistent
3. Family/community recreational: no trained supervision
*relate to types of injuries

Risk Factors for Injury
• Training
• Muscle tendon imbalance
• Anatomic malalignment
• Equipment, footwear and playing surface
• Associated disease states
• growth

Competition
• Young: learn to compete against other teams and individually
• Older: also learn to compete against themselves to better performance
• Injuries from: – Children– Parents– safety

Training
• Fitness statsTraining program:1. Energy: aerobic,anaerobic2. Muscle:
A. StrengthB. EnduranceC. FlexibilityD. Power
3. Speed
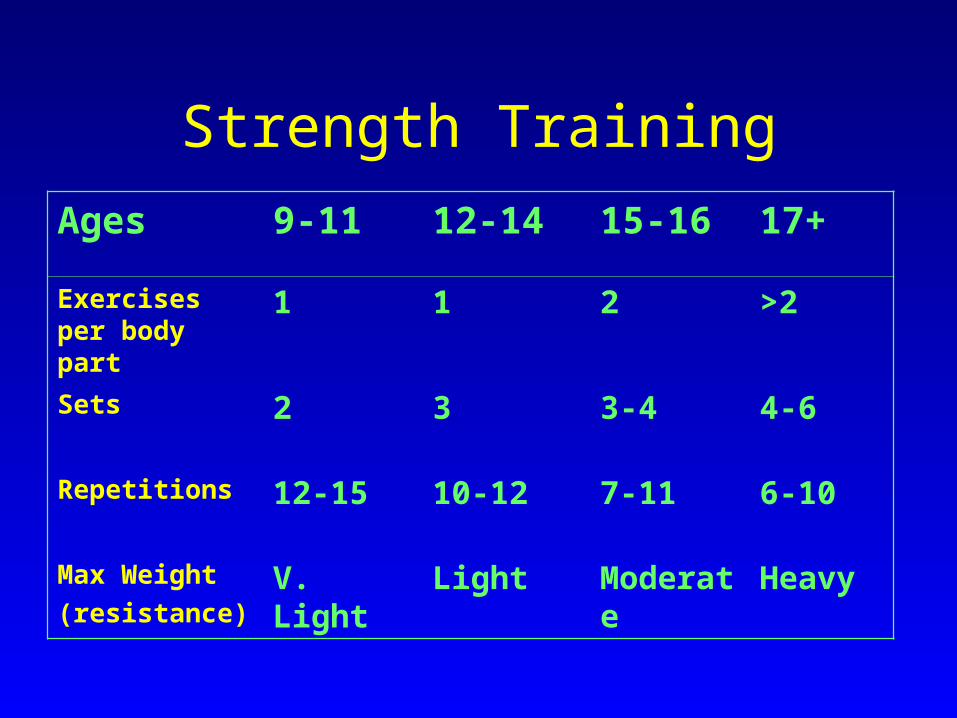
Strength Training
Ages 9-11 12-14 15-16 17+
Exercises per body part
1 1 2 >2
Sets 2 3 3-4 4-6
Repetitions 12-15 10-12 7-11 6-10
Max Weight
(resistance)V. Light Light Moderate Heavy

Return to Sport
• No swelling
• ROM: full, normal, pain free
• Strength: objective and functional testing
• Use of braces
• GRADUAL!












![[p.T] Well Test Procedures Manual](https://static.fdocuments.in/doc/165x107/5475c8f2b4af9fb40a8b5e0b/pt-well-test-procedures-manual.jpg)


![[p.T] Stratigraphy Geologic Time](https://static.fdocuments.in/doc/165x107/577d34871a28ab3a6b8e3c40/pt-stratigraphy-geologic-time.jpg)

![[p.T] Water Well Manual](https://static.fdocuments.in/doc/165x107/577d34871a28ab3a6b8e3c4c/pt-water-well-manual.jpg)