PHYSIOLOGY OF PAIN SENSATION
58
DR NILESH KATE MBBS,MD ASSOCIATE PROF ESIC MEDICAL COLLEGE, GULBARGA. DEPT. OF PHYSIOLOGY PHYSIOLOGY OF PAIN SENSATION.
-
Upload
nileshkate79 -
Category
Health & Medicine
-
view
786 -
download
0
Transcript of PHYSIOLOGY OF PAIN SENSATION

DR NILESH KATE
MBBS,MDASSOCIATE PROF
ESIC MEDICAL COLLEGE, GULBARGA. DEPT. OF PHYSIOLOGY
PHYSIOLOGY OF PAIN
SENSATION.

OBJECTIVES Definition of pain Types of pain Varieties of pain Pain pathway Pain inhibiting pathway Central analgesia Referred pain Applied physiology

Definition The sensation of pain is defined as the The sensation of pain is defined as the
physical adjunct of an imperative physical adjunct of an imperative protective reflex.protective reflex.
pain is an, unpleasant sensory and emotional experience associated with actual or potential tissue damage - The The International Association for the Study of International Association for the Study of Pain (IASP)Pain (IASP)

Types of pain Fast pain is due to activity of
myelinated A δ fibres and it is appreciated as sharp bright and localized sensation.
Slow pain is due to activity of unmyelinated C fibres and it is appreciated as dull aching and more diffuse. Slow pain follows fast pain.
PeripheralPeripheralNerveNerve
C-FiberC-Fiber
A-delta FiberA-delta Fiber

Fast pain & Slow pain Fast pain: is also described as
sharp pain, pricking pain, Acute pain, electric pain. it is elicited by mechanical and thermal type of stimuli.
Slow pain is also called as, slow burning pain, aching pain, throbbing pain, nauseous pain, chronic pain. slow pain can be elicited by mechanical, thermal and chemical stimuli.

Types of Pain
Fast painFast pain Slow painSlow painFelt within about 0.1 second after a painful stimulus.
Begins after 1 second or more and then increases slowly over many sec. or min.
“Bright," sharp, localized sensation
Dull, intense, diffuse, and unpleasant feeling
sharp pain, pricking pain, acute pain, and electric pain
slow burning pain, aching pain,throbbing pain, nauseous pain, and chronic pain
Felt mainly in skin. Not felt in most deeper tissues of the body
It can occur both in the skin and in almost any deep tissue or organ

Types of PainFast painFast pain Slow painSlow pain
Pin prick, cutting or Pin prick, cutting or burning of skinburning of skin
Associated with tissue Associated with tissue destruction.destruction.
Caused by mechanical or Caused by mechanical or thermal stimuli.thermal stimuli.
Caused mainly by Caused mainly by chemical stimulichemical stimuli
Transmitted by Aδ fibersTransmitted by Aδ fibers(velocity 6-30 m/sec)(velocity 6-30 m/sec)NT- GlutamateNT- Glutamate
Transmitted by C fibersTransmitted by C fibers(velocity 0.5-2 m/sec)(velocity 0.5-2 m/sec)NT- Substance PNT- Substance P
Neo-spinothalamic tractNeo-spinothalamic tract Paleo-spinothalamic tractPaleo-spinothalamic tract


TYPES OF PAIN
source of origin -- three types of pain. Superficial pain: pain arising from skin and
mucous membrane. Deep (somatic) pain: pain originating from
somatic structures deep to the skin are known as deep pain.
Visceral pain: pain arising from different internal organs or viscera

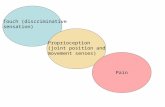
Where Does Pain Come From? Cutaneous Pain – sharp, bright, burning; can
have a fast or slow onset Deep Somatic Pain – stems from tendons,
muscles, joints, periosteum, & bl. Vessels Visceral Pain – originates from internal organs;
diffused @ 1st & later may be localized (i.e. appendicitis)
Psychogenic Pain – individual feels pain but cause is emotional rather than physical

VARIETIES OF PAIN
ACUTE PAIN CHRONIC PAIN CUTANEOUS PAIN DEEP SOMATIC PAIN VISCERAL PAIN REFERRED PAIN NEUROPATHIC PAIN PHANTOM PAIN
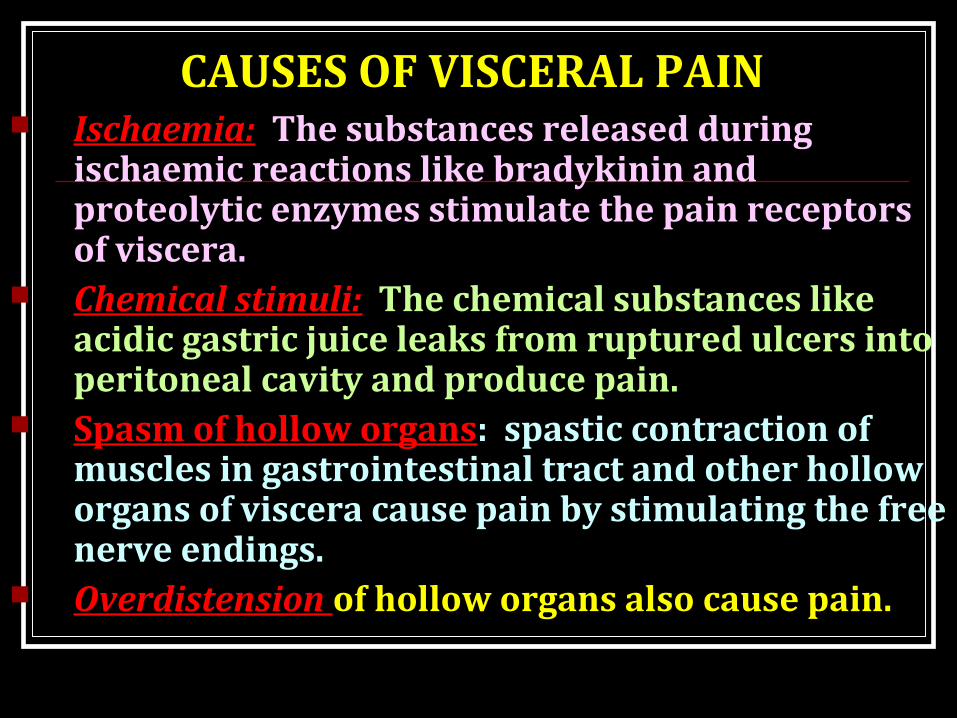
CAUSES OF VISCERAL PAIN Ischaemia: The substances released during
ischaemic reactions like bradykinin and proteolytic enzymes stimulate the pain receptors of viscera.
Chemical stimuli: The chemical substances like acidic gastric juice leaks from ruptured ulcers into peritoneal cavity and produce pain.
Spasm of hollow organs: spastic contraction of muscles in gastrointestinal tract and other hollow organs of viscera cause pain by stimulating the free nerve endings.
Overdistension of hollow organs also cause pain.
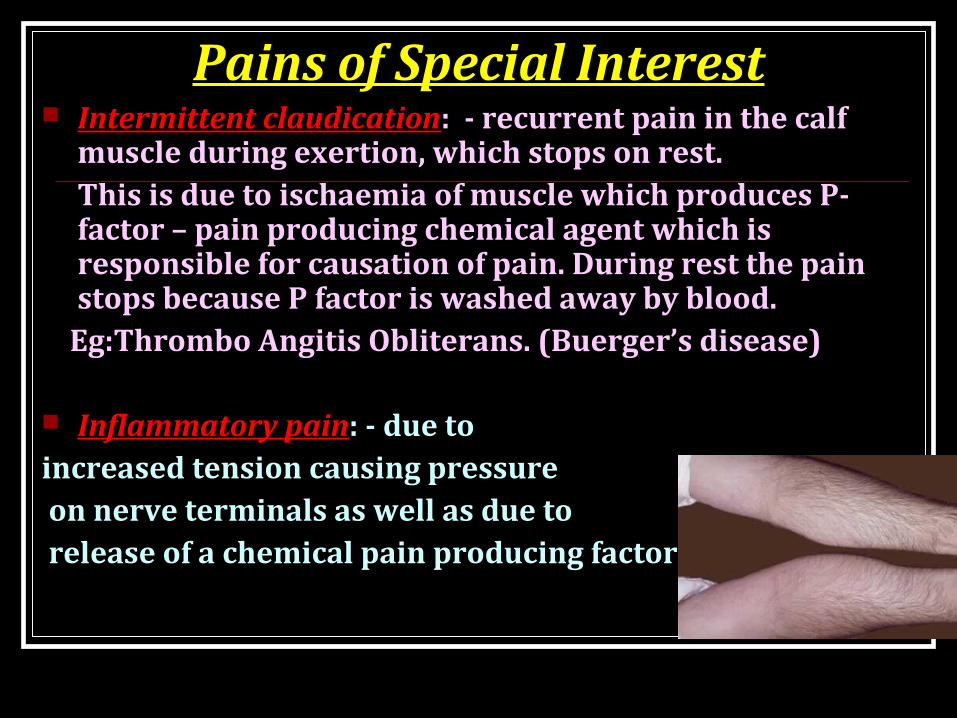
Pains of Special Interest Intermittent claudication: - recurrent pain in the calf
muscle during exertion, which stops on rest. This is due to ischaemia of muscle which produces P-factor – pain producing chemical agent which is responsible for causation of pain. During rest the pain stops because P factor is washed away by blood.
Eg:Thrombo Angitis Obliterans. (Buerger’s disease)
Inflammatory pain: - due to increased tension causing pressure on nerve terminals as well as due to release of a chemical pain producing factor.

PAINS OF SPECIAL INTEREST Coronary occlusion: In addition to P factor, there
is release of 5HT and plasma pain producing polypeptide.
Nerve pain: partial compression of nerve or a nerve root leads to irritability of the nerve or the nerves concerned and gives rise to the formation of areas of Hyperalgesia and pareaesthesia
Ischaemic Muscular pain: Due to release of P factor during active work, on accumulation cause pain. The P factor may be potassium or kinin. Repeated muscular contraction compress blood vessel.

REFERED PAIN
Definition: The pain sensation produced in some part of
the body is felt in other structures away from the place of development. This is called refered pain. The deep pain and some visceral pain are referred to other areas. But superficial pain is not referred.

REFERED PAIN1) Heart pain is referred to
the inner aspect of left arm.2) Diaphragmatic pain to the
tip of the shoulder3) Ureteric pain to the testes
in male and the inner aspect of the thigh in female.
4) Gall bladder pain referred to epigastric region.
5) Pain from the maxillary sinus referred to the nearby tooth.

Referred Pain

Referred Pain
Pain in organs is poorly localized
May be displaced if
Multiple 1° sensory neurons converge on single ascending tract

Mechanism of Referred Pain When the visceral pain fibers are stimulated
pain signals from the viscera are conducted through some of the neurons that conduct pain signals from the skin and the person has the feeling that,
the sensation originate in the skin itself.

Dermatomal Rule
Referred pain is always felt over a structure that developed from the same embryological segment or dermatome from which the organ which is the source of pain developed. This phenomenon of referred pain is called Dermatomal rule.

Dermatomal Rule
During Embryonic development, the diaghragm migrates from the neck region to its adult location between the chest and abdomen and takes its nerve supply, the phrenic nerve with it.
Similarly the heart and the arm have the same segmental origin.
Testicles have migrated with its nerve supply from the primitive urogenital ridge from which kidney and ureter has developed.

CONVERGENCE THEORY The number of peripheral pain afferent fibres
exceed the number of lateral spinothalamic tract. So, Both the somatic and visceral afferents converge upon the same spinothalamic neurons at the spinal cord level.
Hence when visceral pain impulses travel in the same pathway along which impulses from the skin travels, the individual gets the feeling that the pain originates in the skin itself.
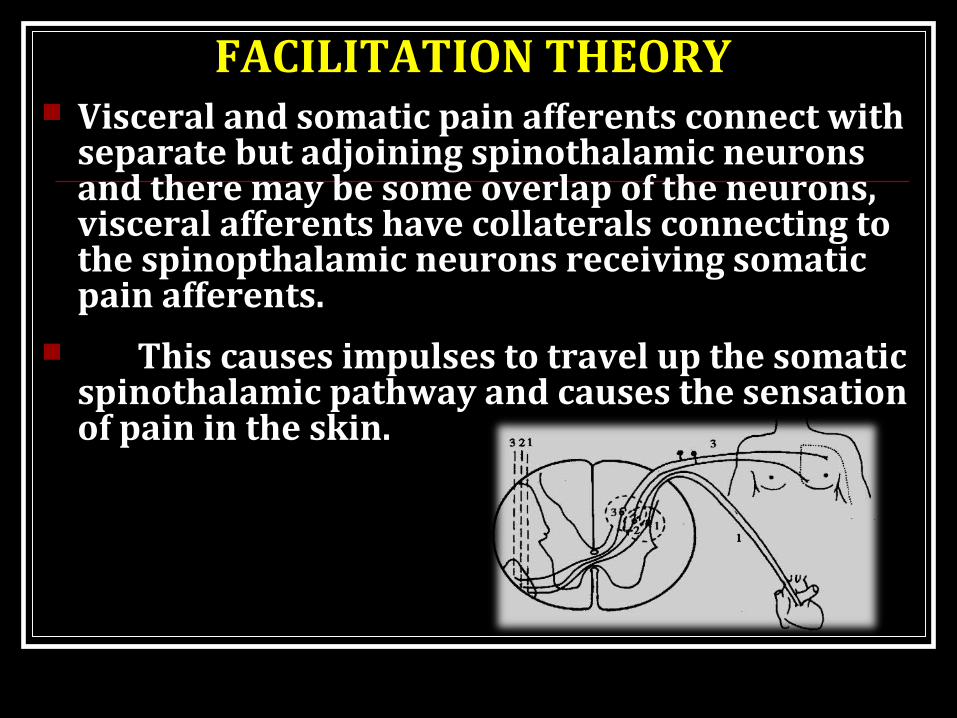
FACILITATION THEORY Visceral and somatic pain afferents connect with
separate but adjoining spinothalamic neurons and there may be some overlap of the neurons, visceral afferents have collaterals connecting to the spinopthalamic neurons receiving somatic pain afferents.
This causes impulses to travel up the somatic spinothalamic pathway and causes the sensation of pain in the skin.

How pain is transmitted to brain

Process of painphysiology
TRANSDUCTIONTRANSMISSIONPERCEPTIONMODULATION

Transduction:
Pain stimuli is converted to electrical energy. This electrical energy is known as Transduction. This stimulus sends an impulse across a peripheral nerve fiber (nociceptor).

Transmission
A delta fibers (myelinated) send sharp, localized and distinct sensations.
C fibers (unmyelinated) relay impulses that are poorly localized, burning and persistent pain.
Pain stimuli travel- spinothalamic tracts.
Perception Person is aware of pain –
somatosensory cortex identifies the location and intensity of pain
Person unfolds a complex reaction-physiological and behavioral responses is perceived.

Modulation Inhibitory neurotransmitters like
endogenous opioids work to hinder the pain transmission.
This inhibition of the pain impulse is known as modulation

Receptors for Pain The receptors in the skin and other tissues are
free nerve endings of small myelinated A δ and non myelinated C fibres.
They are widespread in the superficial layers of skin as well as in certain internal tissues such as the periosteum, arterial walls, joint surfaces, falx and tentorium of cranial vault.

Pain receptors (Nociceptors) Free nerve endings More in
Superficial layers of skin Periosteum Arterial walls Joint surfaces Falx, tentorium
Sparse in other deep tissues.
Non-adapting in nature.
Effects of painSympathetic responses Pallor Increased blood pressure Increased pulse Increased respiration Skeletal muscle tension Diaphoresis

Effects of painParasympathetic responses Decreased blood pressure Decreased pulse Nausea & vomiting Weakness Pallor Loss of consciousness
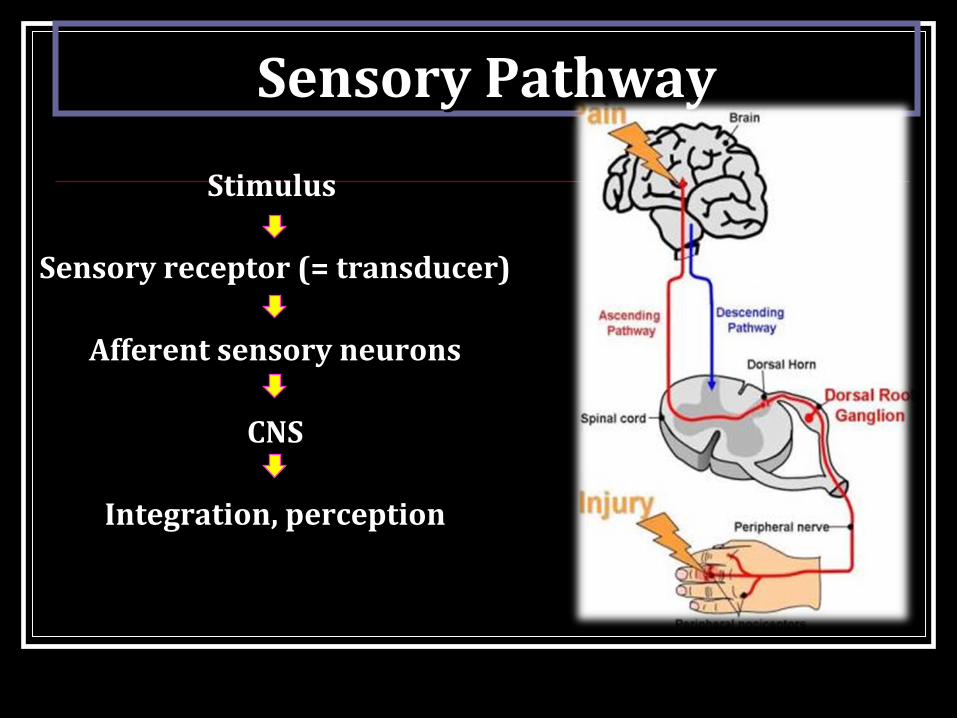
Sensory PathwaySensory Pathway
Stimulus Stimulus
Sensory receptor (= transducer)Sensory receptor (= transducer)
Afferent sensory neuronsAfferent sensory neurons
CNSCNS
Integration, perceptionIntegration, perception

Somatic Senses Primary sensory neurons
from receptor to spinal cord or medulla
Secondary sensory neurons always cross over (in spinal cord or medulla) → thalamus
Tertiary sensory neurons → somatosensory cortex (post central gyrus)

Dual pathways for pain transmission From peripheral receptors to spinal cord:
Aδ fibers (fast fibers) – for fast pain C fibers (slow fibers) – for slow pain
From spinal cord to brain: via Anterolateral (Spinothalamic) tract Neo-spinothalamic tract – for fast pain Paleo-spinothalamic tract – for slow pain

•Thalamus – ventrobasal complex•Reticular formation
Spinothalamic tract
Spinal cord(lamina I – lamina marginalis)
Peripheral fibersAδ fibers
Pain receptor(Free nerve endings)
•Somatosensory cortex•Other basal areas of brain

Pain pathwayPain pathway

•Reticular nuclei,Tectal area & periaqueduvtal grey region •Thalamus
Spinothalamic tract
Spinal cord(lamina II & III – substantia gelatinosa)
Peripheral fibersC fibers
Pain receptor(Free nerve endings)
•Thalamus (IL & VL nuclei)•Hypothalamus•Other basal areas of brain

CENTER FOR PAIN SENSATION The center for pain sensation is in the post central gyrus of parietal cortex. Fibres reaching Hypothalamus are concerned with arousal mechanism due to pain stimulus.
Substance P is the neurotransmitter involved in pain sensation. It is secreted by the ending of pain nerve fibres in dorsal grey horn.

DESCENDING NEURONS Descending Pain Modulation (Descending Pain
Control Mechanism) Transmit impulses from the brain (corticospinal
tract in the cortex) to the spinal cord (lamina) Periaquaductal Gray Area (PGA) – release
enkephalins Nucleus Raphe Magnus (NRM) – release serotonin The release of these neurotransmitters inhibit
ascending neurons Endogenous opioid peptides - endorphins &
enkephalins causes analgesia.

PHYSIOLOGY OF PAIN PERCEPTION
InjuryInjury
Descending Descending PathwayPathway
PeripheralPeripheralNerveNerve
Dorsal Dorsal RootRootGanglionGanglion
C-FiberC-Fiber
A-beta FiberA-beta Fiber
A-delta FiberA-delta Fiber
AscendingAscendingPathwaysPathways
Dorsal Dorsal HornHorn
BrainBrain
Spinal CordSpinal Cord
42

Physiological Basis of Medical measures to relieve pain
The CNS has its own control system which inhibits the impulse of pain sensation. This is also called Analagesia system. This control system is present in both brain and spinal cord.
Pain control system in spinal cord: This is in dorsal grey horn. The dorsal grey horn is considered as the gateway for pain impulses to reach the brain (via) spinothalamic tract.
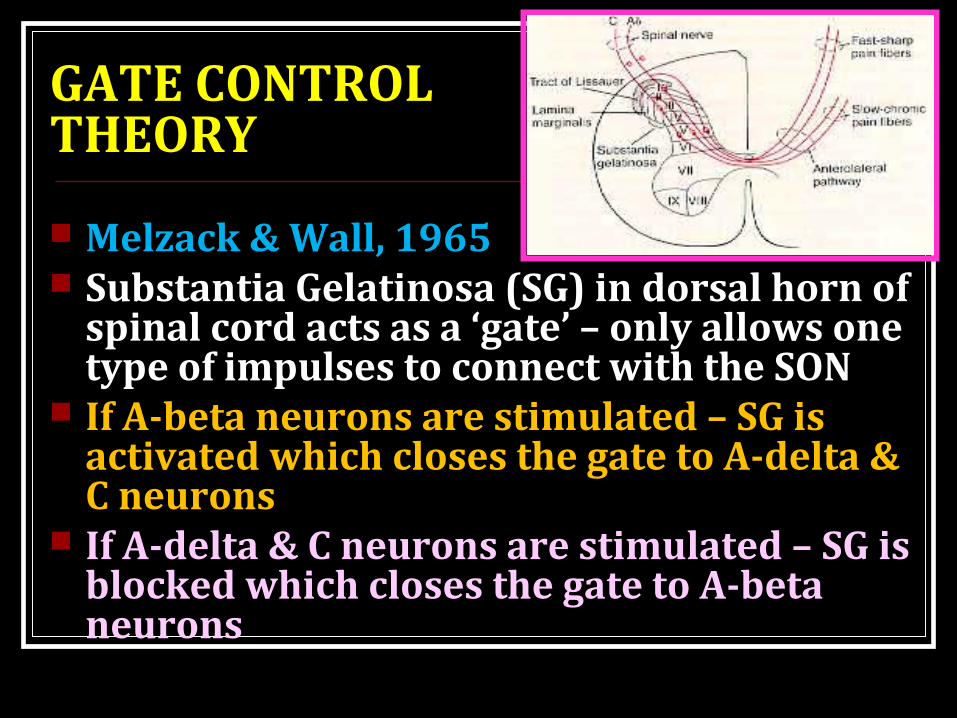
GATE CONTROL THEORY
Melzack & Wall, 1965 Substantia Gelatinosa (SG) in dorsal horn of
spinal cord acts as a ‘gate’ – only allows one type of impulses to connect with the SON
If A-beta neurons are stimulated – SG is activated which closes the gate to A-delta & C neurons
If A-delta & C neurons are stimulated – SG is blocked which closes the gate to A-beta neurons

GATE CONTROL THEORY Gate - located in the dorsal horn of the spinal cord Smaller, slower n. carry pain impulses Larger, faster n. fibers carry other sensations Impulses from faster fibers arriving @ gate 1st inhibit
pain impulses (acupuncture/pressure, cold, heat, chem. skin irritation).
Brain
Pain
Heat, Cold, Mechanical
Gate (T cells/ SG)

Gate control theory When pain sensation is produced-- other afferents
particularly the touch fibres reaching the posterior column of spinal cord are also activated.
These dorsal column fibres send collaterals to the cells of substantia gelatinosa in the dorsal grey horn.
Thus impulses ascending via dorsal column fibres pass through the collaterals and reach substantia gelatinosa.
Here these impulses inhibit the release of substance P by the pain nerve endings. So that the pain sensation is suppressed.
Thus the gating of pain in dorsal grey horn level is similar to presynaptic inhibition.

•Periaqueductal grey•Periventricular nuclei
Raphe magnus nucleusNucleus reticularis paragigantocellularis
Spinal cord(pain inhibiting complex in dorsal horn)
Hypothalamus(periventricular nucleus & MFB)
Pain suppression (Analgesia) system of brain & spinal cord
NeurotransmittersNeurotransmittersSerotoninSerotoninOpiates (enkephalins)Opiates (enkephalins)


Pain control system in Brain Acupuncture is also used to relieve pain. This
is based upon the pain inhibitory mechanism of encephalins and endorphins released by this procedure.
Pain control NSAIDs (inhibit COX)NSAIDs (inhibit COX)
Opiates (inhibit NT release)Opiates (inhibit NT release)

Inhibition of pain transmission by tactile sensory signals
Rubbing the skin near painful areas and applying liniments often relieves pain.
This is due to the stimulation of Aβ sensory fibres from peripheral tactile receptors depress transmission of pain signals.
This results from a type of local lateral inhibition.

Surgical procedure that relieve pain
Different surgical procedures are done in the course of pain pathway to relieve pain. They are
-Sympathectomy-Cordotomy-Thalamotomy-Prefrontal lobotomy

Applied Terminology
Algesia = pain Analgesia = dec./loss of sensitivity to painful stimuli Hyperalgesia = inc. sensitivity to painful stimuli Allodynia = sensation of pain in response to an
innocuous stimulus
Brown-Sequard syndrome (hemisection of the spinal cord.
Syringomyelia (loss of pain & temp. with sparing of touch & vibration.

Applied Tic douloureux- electric shock like pain in
sensory distribution of V or IX CN. Trigeminal neuralgia Glassopharyngeal neuralgia
Headache – Dura Cerebral blood vessels CSF pressure Nasal & accessory nasal structures Eye disorders Muscle spasm of head & neck muscles Alcohol constipation

Applied Treatment for pain
Remove the cause NSAID (Non-Steroidal Anti-
Inflammatory drugs) Opioid analgesics

APPLIED PHYSIOLOGYAbnormal prolonged pain: Injuries and disease
process cause damage to peripheral nerves cause severe debilitating and persistent abnormalities of pain sensation.
Hyperpathia : Threshold for stimulation is increased causing burning pain.
Phantom limb: Pain in absent limb.Causalgia: spontaneous burning pain long after
trivial injuries.Hyperalgesia is a condition in which pain is
produced by minor stimuli which normally do not cause pain eg: Touch
If a normal innocuous tactile or thermal stimulus evokes pain, the condition is called Allodynia.

RECAP
Definition of pain Types of pain Varieties of pain Pain pathway, pain inhibiting pathway , central analgesia Referred pain Applied physiology

Thank You