Physiology of ‘Normal’ Labour
23
Physiology and Mechanics Physiology and Mechanics of ‘Normal’ Labour and of ‘Normal’ Labour and Pregnancy Pregnancy
-
Upload
prabhakar-kumar -
Category
Documents
-
view
40 -
download
6
description
hjf
Transcript of Physiology of ‘Normal’ Labour

Physiology and Mechanics of Physiology and Mechanics of ‘Normal’ Labour and Pregnancy‘Normal’ Labour and Pregnancy

AimsAims
• Understand the physiological changes that Understand the physiological changes that occur in a normal pregnancyoccur in a normal pregnancy
• Understand the physiology and mechanics Understand the physiology and mechanics influencing the four stages of a normal influencing the four stages of a normal labour.labour.
• Pass the DRCOGPass the DRCOG

Physiology of PregnancyPhysiology of Pregnancy
(From 38 weeks after conception or 40 weeks (From 38 weeks after conception or 40 weeks after first day of last period)after first day of last period)

Cardiovascular ChangesCardiovascular Changes
• Cardiovascular output increases by 30-50%, peaking at Cardiovascular output increases by 30-50%, peaking at approx 24/40approx 24/40
• Mediated by increased pulse and stroke volumeMediated by increased pulse and stroke volume• Renin level increase Renin level increase angiotensin I level increase angiotensin I level increase• Blood volume increases in proportion to COBlood volume increases in proportion to CO• Circulation becomes Circulation becomes hyperdynamichyperdynamic, i.e. it reacts more , i.e. it reacts more
strongly to exercise etc. This leads to murmurs strongly to exercise etc. This leads to murmurs becoming more apparentbecoming more apparent
• At term, blood flow to uterus is approx 1L/minAt term, blood flow to uterus is approx 1L/min• Most changes are reversed by 6 weeks postpartumMost changes are reversed by 6 weeks postpartum

Respiratory ChangesRespiratory Changes• Progesterone-mediated increase in tidal Progesterone-mediated increase in tidal
volume + resp rate volume + resp rate reduced pCO reduced pCO22
• OO22 consumption increases by approx 20% to consumption increases by approx 20% to
meet additional metabolic needsmeet additional metabolic needs• Hyperaemia and oedema of respiratory tractHyperaemia and oedema of respiratory tract
Increased Decreased No Change
Tidal volume Inspiratory reserve Vital capacity
Respiratory rate Expiratory reserve PO2
Minute volume Residual volume
PCO2

Renal + Urological ChangesRenal + Urological Changes
• GFR increased in proportion to CO, leading to GFR increased in proportion to CO, leading to decreased urea + creatininedecreased urea + creatinine
• Marked hydroureter + dilatation of renal Marked hydroureter + dilatation of renal pelvises due to influence of progesterone and pelvises due to influence of progesterone and pressure of foetus. This persists for 6-12 weeks pressure of foetus. This persists for 6-12 weeks after deliveryafter delivery
• RF heavily influenced by blood supply, hence RF heavily influenced by blood supply, hence it increases markedly in positions that relieve it increases markedly in positions that relieve uterine pressure on IVC e.g. lateral.uterine pressure on IVC e.g. lateral.

GI System ChangesGI System Changes
• Mechanical constipation occursMechanical constipation occurs• Hormone-mediated relaxation of all smooth Hormone-mediated relaxation of all smooth
muscle muscle decreased GI motility decreased GI motility• Increase in ALP due to placental productionIncrease in ALP due to placental production• Heartburn common, due to pressure of Heartburn common, due to pressure of
uterus, decreased motility, and relaxation of uterus, decreased motility, and relaxation of sphincter.sphincter.
• Reduced HCl production Reduced HCl production GI ulcers much GI ulcers much less common in pregnancyless common in pregnancy

Haematological ChangesHaematological Changes
• White cell count increased.White cell count increased.• Plasma volume increases more than cell count, Plasma volume increases more than cell count,
thus Hb tends to lower by dilutionthus Hb tends to lower by dilution• Total iron requirement (in addition to normal) Total iron requirement (in addition to normal)
= 1G for duration of pregnancy (easily = 1G for duration of pregnancy (easily obtained in diet)obtained in diet)
• Reduced protein C and protein S and increase Reduced protein C and protein S and increase in other clotting factors in other clotting factors tendency to clot tendency to clot
• ESR raisedESR raised

Endocrine ChangesEndocrine Changes• Pregnancy alters systemic protein binding, subtly Pregnancy alters systemic protein binding, subtly
altering all hormone systemsaltering all hormone systems• Placenta secretes hormone similar to TSH, leading to Placenta secretes hormone similar to TSH, leading to
increased thyroid function (and sometimes Sx increased thyroid function (and sometimes Sx resembling hyperthyroid)resembling hyperthyroid)
• Metabolic rate rises by approx 25%Metabolic rate rises by approx 25%• Placenta secretes CRH Placenta secretes CRH ACTH production ACTH production
increased aldosterone + cortisol which contribute to increased aldosterone + cortisol which contribute to oedema of pregnancyoedema of pregnancy
• Pituitary enlarges and prolactin increases tenfoldPituitary enlarges and prolactin increases tenfold• Increased corticosteroids and progesterone lead to Increased corticosteroids and progesterone lead to
increased insulin resistanceincreased insulin resistance

Physiology of LabourPhysiology of Labour

Late PregnancyLate Pregnancy
• Braxton-Hicks contractions start around 26 Braxton-Hicks contractions start around 26 weeks but may not be felt until much laterweeks but may not be felt until much later
• CO becomes more sensitive to body CO becomes more sensitive to body position, e.g. especially recumbentposition, e.g. especially recumbent
• Marked leucocytosis just prior to and Marked leucocytosis just prior to and during labourduring labour

First Stage – Latent PhaseFirst Stage – Latent Phase
• Few days leading up to active labourFew days leading up to active labour• Prostaglandin mediated ‘ripening’ of cervixProstaglandin mediated ‘ripening’ of cervix• Irregular contractions begin effacementIrregular contractions begin effacement• ‘‘Bloody show’ – mucous and blood which previously Bloody show’ – mucous and blood which previously
plugged cervix liquefies. Likely also mediated by plugged cervix liquefies. Likely also mediated by prostaglandins.prostaglandins.
• Membranes can rupture at any time (often assisted but Membranes can rupture at any time (often assisted but ARM is NOT part of normal labour). This event tends to ARM is NOT part of normal labour). This event tends to trigger active labour, again likely due to the release of trigger active labour, again likely due to the release of prostaglandins (true mechanism not fully understood)prostaglandins (true mechanism not fully understood)

First Stage – Active PhaseFirst Stage – Active Phase
• Said to begin once regular contractions Said to begin once regular contractions established, or effaced cervix 3cm dilatedestablished, or effaced cervix 3cm dilated
• Cervix dilates at approx 1cm/hr and is Cervix dilates at approx 1cm/hr and is incorporated into lower segmentincorporated into lower segment
• Upper segment progressively shortens and Upper segment progressively shortens and thickens, due to spirals of smooth muscle thickens, due to spirals of smooth muscle contractingcontracting
• Lower segment stretches and thinsLower segment stretches and thins• Ends when cervix is 10cm dilated (‘Fully’)Ends when cervix is 10cm dilated (‘Fully’)

Second StageSecond Stage
• Begins when cervix fully dilatedBegins when cervix fully dilated• Lasts about 1hr in primip, 30mins in multip but Lasts about 1hr in primip, 30mins in multip but
lenthened by epidural analgesialenthened by epidural analgesia• Upper segment continues to shorten and thicken. Upper segment continues to shorten and thicken.
Majority of fetus in lower segmentMajority of fetus in lower segment• Head passes intraspinous diameter – the narrowest part Head passes intraspinous diameter – the narrowest part
of the pelvisof the pelvis• Perineum softened by congestion with blood (not unlike Perineum softened by congestion with blood (not unlike
arousal)arousal)• Delivery accomplished by the following six Delivery accomplished by the following six
manoeuvres:manoeuvres:

Six manoeuvres of deliverySix manoeuvres of delivery1.1. EngagementEngagement of the fetal head in the transverse position. The of the fetal head in the transverse position. The
baby is looking across the pelvis at one or other of the baby is looking across the pelvis at one or other of the mother's hips. mother's hips.
2.2. Descent and flexionDescent and flexion of the fetal head of the fetal head 3.3. Internal rotationInternal rotation. The fetal head rotates 90 degrees to the . The fetal head rotates 90 degrees to the
occipito-anterior position so that the baby's face is towards the occipito-anterior position so that the baby's face is towards the mother's rectum. mother's rectum.
4.4. Delivery by extensionDelivery by extension. The fetal head passes out of the birth . The fetal head passes out of the birth canal. Its head is tilted backwards so that its forehead leads the canal. Its head is tilted backwards so that its forehead leads the way through the vagina. way through the vagina.
5.5. RestitutionRestitution. The fetal head turns through 45 degrees to restore . The fetal head turns through 45 degrees to restore its normal relationship with the shoulders, which are still at an its normal relationship with the shoulders, which are still at an angle. angle.
6.6. External rotationExternal rotation. The shoulders repeat the corkscrew . The shoulders repeat the corkscrew movements of the head, which can be seen in the final movements of the head, which can be seen in the final movements of the fetal head.movements of the fetal head.

Third StageThird Stage
• From delivery of fetus to delivery of placentaFrom delivery of fetus to delivery of placenta• Usually within 15-30 mins (depends on choice of active or Usually within 15-30 mins (depends on choice of active or
expectant management)expectant management)• Immediately after delivery, contractions tend to stop for brief Immediately after delivery, contractions tend to stop for brief
periodperiod• Placenta separated due to ‘shearing effect’ of uterus contracting Placenta separated due to ‘shearing effect’ of uterus contracting
after foetus delivered, thereby reducing size of site of attachmentafter foetus delivered, thereby reducing size of site of attachment• Retroplacental haematoma forms, exuding downwards pressureRetroplacental haematoma forms, exuding downwards pressure• Active management is now so common to be considered Active management is now so common to be considered
NORMALNORMAL• Oxytotic (commonly syntocinon) given by IM injection to stimulate Oxytotic (commonly syntocinon) given by IM injection to stimulate
uterine contractionuterine contraction• Placenta can be delivered by maternal effort or by controlled cord traction Placenta can be delivered by maternal effort or by controlled cord traction
(CCT)(CCT)• Active Management has been shown to reduce PPHActive Management has been shown to reduce PPH

Past DRCOG QuestionsPast DRCOG Questions
• http://www.drcog-mrcog.info/mcq%20papehttp://www.drcog-mrcog.info/mcq%20papers%201%20-%205.htmrs%201%20-%205.htm

Regarding Labour:Regarding Labour:
• the latent phase may last for more than four hours the latent phase may last for more than four hours • the active phase should be associated with cervical the active phase should be associated with cervical
dilatation at a rate of at least 1 cm. per hour dilatation at a rate of at least 1 cm. per hour • the active phase starts when the cervix is effaced and the active phase starts when the cervix is effaced and
2 cm. dilated 2 cm. dilated • involves artificial rupture of the membranes involves artificial rupture of the membranes • is best charted using a partogram is best charted using a partogram • epidural anaesthesia has an adverse effect on the rate epidural anaesthesia has an adverse effect on the rate
of progress in the 1st. stage of labourof progress in the 1st. stage of labour
T
T
F
F
T
F

The second stage:The second stage:
• starts with the onset of maternal expulsive effort starts with the onset of maternal expulsive effort and ends with the delivery of the baby. and ends with the delivery of the baby.
• should not last more than one hour in the should not last more than one hour in the primigravida. primigravida.
• continuous electronic monitoring should be used continuous electronic monitoring should be used in all cases. in all cases.
• opiates should be used for pain relief. opiates should be used for pain relief. • may be prolonged in association with regional may be prolonged in association with regional
anaesthesia.anaesthesia.
F
F
F
F
T

Active management of the third Active management of the third stage:stage:
• always involves the use of an intravenous always involves the use of an intravenous oxytocic oxytocic
• signs of placental separation should be awaited signs of placental separation should be awaited before cord traction is used before cord traction is used
• the cord should be clamped immediately to the cord should be clamped immediately to prevent haemorrhage from the baby prevent haemorrhage from the baby
• reduces the incidence of retained placenta reduces the incidence of retained placenta • reduces the incidence of post-partum haemorrhagereduces the incidence of post-partum haemorrhage
F
F
F
F
T

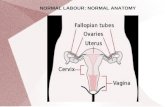
Normal Labour:Normal Labour:
• is associated with internal rotation of the head is associated with internal rotation of the head • is associated with extension of the delivered head is associated with extension of the delivered head • does not occur with mento-posterior position does not occur with mento-posterior position • does not occur with brow presentation does not occur with brow presentation • should not be attempted after two Caesarean sections should not be attempted after two Caesarean sections • carries less risk to the mother than Caesarean section carries less risk to the mother than Caesarean section • involves episiotomy involves episiotomy • involves physiological management of the third stage involves physiological management of the third stage • is associated with blood loss < 350 ml is associated with blood loss < 350 ml
T
T
T
T
F
T
F
F
F

Normal pregnancy:Normal pregnancy:• the key stages of organogenesis occur between 10 and 12 the key stages of organogenesis occur between 10 and 12
weeksweeks• maternal metabolic rate increases by about 25%maternal metabolic rate increases by about 25%• increased maternal metabolic rate is mainly caused by the increased maternal metabolic rate is mainly caused by the
foetus and placentafoetus and placenta• blood volume increases by about 30%blood volume increases by about 30%• red cell mass increases by about 40%red cell mass increases by about 40%• erythrocyte sedimentation rate remains within the non-erythrocyte sedimentation rate remains within the non-
pregnant rangepregnant range• cardiac output increasescardiac output increases• glomerular filtration rate increases by up to 50%glomerular filtration rate increases by up to 50%• ureters and renal pelves dilate, but return to normal within ureters and renal pelves dilate, but return to normal within
two weeks of deliverytwo weeks of delivery• iron supplementation should be given routinelyiron supplementation should be given routinely
F
T
T
T
F
F
T
T
F
F

ReferencesReferences
• http://www.merck.com/mmpe/sec18/ch260/http://www.merck.com/mmpe/sec18/ch260/ch260b.htmlch260b.html
• http://www.uptodate.com/patients/content/thttp://www.uptodate.com/patients/content/topic.do?topicKey=labordel/10159opic.do?topicKey=labordel/10159
• www.accd.edu/sac/nursing/rnsg2261/www.accd.edu/sac/nursing/rnsg2261/PDFWH/PDFWH/StageStagesOfsOfLaborLabor.pdf.pdf