Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of...
45
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology Objectives after studying this chapter, you should be able to . . . 1. Explain the genesis of resting membrane potential. 2. Describe the action potential of nerve, skeletal, cardiac, and smooth muscle fibers. 3. Expound the effect of extracellular fluid ion concentrations on the cell membrane potential. 4. Explain the mechanism of propagation of the action potential. 5. Describe rhythmicity of certain excitable tissues. 6. Expound the nerve fiber morphology, its myelination, and the nerve fiber classification. 7. Explain the synaptic transmission and neurotransmitters. 8. Expound transmission of impulses from nerves to skeletal muscle fibers: The neuromuscular junction. 9. Describe the histological appearance of the skeletal muscle fiber. 10. Explain the mechanism of muscle contraction. 11. Describe the source of energy for the muscle. 12. Characterize types of muscle contraction. 13. Expound different events-related to muscle contraction such as skeletal muscle tone, muscle fatigue, muscle hypertrophy, muscle atrophy, the staircase effect, and Relationship between muscle length and tension. 14. Describe the types of smooth muscles, and the mechanism of smooth muscle contraction. 15. Explain the difference between smooth, skeletal, and cardiac muscles. NERVES & MUSCLES PHYSIOLOGY
Transcript of Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of...
![Page 1: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/1.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology
Objectives after studying this chapter, you should be able to . . .
1. Explain the genesis of resting membrane potential. 2. Describe the action potential of nerve, skeletal, cardiac, and smooth muscle
fibers. 3. Expound the effect of extracellular fluid ion concentrations on the cell
membrane potential. 4. Explain the mechanism of propagation of the action potential. 5. Describe rhythmicity of certain excitable tissues. 6. Expound the nerve fiber morphology, its myelination, and the nerve fiber
classification. 7. Explain the synaptic transmission and neurotransmitters. 8. Expound transmission of impulses from nerves to skeletal muscle fibers: The
neuromuscular junction. 9. Describe the histological appearance of the skeletal muscle fiber. 10. Explain the mechanism of muscle contraction. 11. Describe the source of energy for the muscle. 12. Characterize types of muscle contraction. 13. Expound different events-related to muscle contraction such as skeletal muscle
tone, muscle fatigue, muscle hypertrophy, muscle atrophy, the staircase effect, and Relationship between muscle length and tension.
14. Describe the types of smooth muscles, and the mechanism of smooth muscle contraction.
15. Explain the difference between smooth, skeletal, and cardiac muscles.
NERVES & MUSCLES PHYSIOLOGY
![Page 2: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/2.jpg)
![Page 3: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/3.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 1
Electrical potentials exist across the membranes of virtually all cells of the body. In addition, some cells, such as nerve and muscle cells, are capable of generating rapidly changing electrochemical impulses at their membranes, and these impulses are used to transmit signals along the nerve or muscle membranes. In still other types of cells, such as glandular cells, macrophages, and ciliated cells, local changes in membrane potentials also activate many of the cells’ functions.
RReessttiinngg mmeemmbbrraannee ppootteennttiiaall ((RRMMPP)):: Is the potential difference between the inner and outer
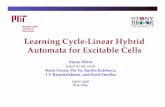
surface of a biological membrane during rest or inactivity at which the forces of concentration gradient and electrical gradient balance. RMP varies between –100 mV to -10 mV (on the inside relative to the outside of the membrane) depending on the type and the size of tissues (figure 4.1). This mean an excess of negative ions (anions) accumulates immediately inside the cell membrane along its inner surface and excess of positive ions (cations) accumulates immediately outside the membrane (table 1.1).
TThhee ggeenneessiiss aanndd tthhee mmaaggnniittuuddee ooff rreessttiinngg mmeemmbbrraannee ppootteennttiiaall ((RRMMPP)):: In humans the
genesis and the magnitude of the normal resting membrane potential is mainly due to: (1) Passive outward diffusion of K+ ions (diffusion potential) (figure 4.2) which alone is responsible for about 95% of RMP than will the inward diffusion of Na+ ions. This is because the permeability of the membrane to K+ ions is 100 times more than Na+ channels. This outward diffusion of K+ will create a state of electro-positivity outside the membrane and electronegativity on the inside (because of negative anions that remain behind). The outward diffusion of K+ ions will create more positivity on the outer side of the membrane that exactly counterbalances further passive diffusion of K+ ions down its concentration gradient. This counterbalance forces is called K+ equilibrium potential at which the chemical driving force and the electrical driving force on K+ ions are equal and opposite, and the net diffusion of K+ ions is stopped. Ex = - 61 log [x]i / [x]o, where i and o refer to intra- and extracellular concentration of the ion (x) in question, E = equilibrium potential. (2) Electrogenic pump (Na+-K+ pump) which pumps three Na+ ions out of for every two K+ ions pumped in. This pump utilizes energy for its action, which is derived from ATP. Thus, for every cycle of the pump the inside of the excitable cell losses one positive charge a process that leads to an excess of positive charges outside. Electrogenic pump is responsible for about 5% of the total resting membrane potential.
Figure 4.1: Diagrammatic representation for the membrane potential measurement.
Figure 4.2: The genesis for the establishment of RMP.
![Page 4: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/4.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 2
Excitable cell: Some cells (like muscle and nerve cells) are called excitable cells. This is because they have two essential properties: [1] Excitability: They are able to respond to certain stimuli by generating electrical impulses called action potentials. [2] Conductivity: They and able to transmit action potential over the surface of cell membrane. The action potential of the nerve and skeletal muscle fiber: Action potential (also called impulse in the nerve fiber) is a rapid and transient change in the membrane potential that can be transmitted across the surface of an excitable cell. Series of action potentials transmitted along the nerve to its ends is called nerve signal.
Similar to the electrical signal, nerve signal also consists of waves that can be recorded called action potentials (figure 4.3). Each action potential (spike potential) begins with a sudden change from the normal resting negative potential to a positive membrane potential and then ends with an almost equally rapid return to the negative potential. The duration of action potential is only a few 10,000ths of a second. The stages of an action potential are as fallow: [1] Resting stage: which represents a resting membrane potential (RMP) before the action potential occurs. The membrane is said to be polarized during this stage because of the very large membrane potential that is present (figure 4.3, circle 7). [2] Initiation of an action potential (generation of graded potential): Any event (chemical, mechanical, thermal, or electrical stimulation) that increases the membrane permeability to the Na+ ions by opening of Na+ channels will lead to Na+ influx and consequently an initial rise in the membrane potential toward the zero level (figure 4.3, circle 1). This initial local change in membrane potential (also called graded potential) (not transmittable, transient change in membrane potential) is resisted by increasing K+ efflux and Cl- influx with consequent restoration of the resting membrane potential. However, if this initial rise in membrane potential is rapid and enough in magnitude, it may approach a critical level called the threshold level (figure 4.3, circle 2) at which action potential will be generated. Therefore, the threshold level can be defined, as the level of membrane potential required to cause an action potential, which is between -50 to –70 mV. Action potential fails to occur if: [A]: The membrane potential rises very slowly so that the Na+ channels then have time to close while K+ channels will have the time to open. Therefore, the membrane potential will not reach the threshold level for eliciting an action potential. This phenomenon is called
Table 1.1 Magnitude of RMP in different tissues
Nerve cells - 70 mV
Skeletal muscle - 90 mV
Cardiac muscle - 90 mV
SA node - 70 mV
GI smooth muscle Variable; - 40 to - 75 mV
Red blood cells - 10 mV
Figure 4.3: Action potential of skeletal muscle and nerve fibers.
![Page 5: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/5.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 3
accommodation of the membrane to the stimulus. [B]: The stimulus is subthreshold in magnitude, with less number of Na+ channels to open.
Once action potential started, action potential waves occur with constant rate and amplitude regardless of the strength of the stimulus provided that the stimulus is at or above threshold intensity (the action potential is therefore is said to obey the all or none law). [3] Depolarization stage: When the membrane potential reaches the threshold level, the potential across the membrane rises suddenly and rapidly in the positive direction approaching zero or may overshoots and become positive (figure 4.3, circle 3). The cause of this depolarization is due to sudden opening of special type of membrane channels for Na+
ions (open the activated gated of the channel) which their opening depend on the voltage across the membrane (threshold level). Therefore, they are called voltage-gated Na+ channels and consequently increase the Na+ permeability of the membrane substantially allowing Na+ to pass from exterior to intracellular fluid (inward Na+ current). After the voltage-gated Na+ channel has remained open for short times, it suddenly closes by the inactivated gate of the channel, and Na+ ions can no longer pass to the inside of the membrane (figure 4.3, circle 4). At this point the membrane potential begins to recover back toward the resting membrane state, which is repolarization process. A very important characteristic of the voltage-gated Na+ channel is that the gates will not regain its original configuration again until the membrane potential returns either to on nearly to the original resting membrane potential level. [4] Repolarization stage: In which the normal resting membrane-polarizing state is re-established (figure 4.3, circles 5, 6). The causes of repolarization are: [A] Closure of voltage-gated Na+ channels preventing further inflow of Na+ ions inside the nerve fiber. [B] Opening of voltage-gated K+ channels which allow the passage of K+ ions from intracellular fluid (ICF) to extracellular fluid (ECF) (outward K+ current).
[C] The electrogenic pump. At the end of repolarization there is a delay in closure of K+ gates which allows excess K+ ions to diffuse out the nerve fiber making inside the cell more negative than the original resting membrane
Table 4.2: Comparison of action potential and conduction velocity
Excitable tissues Action potential duration
Speed of conduction
Skeletal muscle 5 msec 4 -5 m/sec
Cardiac muscle 200 msec 0.5 m/sec
Nerve fiber 1 msec Variable, 0.5 – 120 m/sec
![Page 6: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/6.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 4
potential for just a few milliseconds after the action potential is over. This is called hyperpolarization (figure 4.3, circle 6).
Almost everything regarding initiation and conduction of action potentials in nerve fibers applies equally well to skeletal muscle fiber except that the duration of action potential in skeletal muscle (5 msec) about five times longer and velocity of conduction is much slower than in the large myelinated nerve fiber (table 4.2).
Figure 4.3 is deliberately distorted in order to demonstrate the different phases of the local potential and action potential. The magnitudes of the local potential and hyperpolarization are exaggerated, the local potential is stretched out to make it seem longer, and the duration of hyperpolarization is shrunken so the graph does not run off the page. When these events are plotted on a more realistic timescale, they look like figure 4.4. The local potential is so brief it is unnoticeable, and hyperpolarization is very long but only slightly more negative than the RMP. An action potential is often called a spike; it is easy to see why from this figure.
Degree of excitability: We can label a particular tissue as highly excitable tissue when the value of resting membrane potential of it is very near to the threshold value for the action potential. This is because we only need a very small change in membrane potential to reach the threshold value and consequently to generate an action potential. On the other hand, when the resting membrane potential value moves in the opposite direction away from the threshold value, i.e. it becomes more negative, it becomes very difficult to excite such tissue because we need a large change in membrane potential to reach the threshold value in order to elicit an action potential. Therefore, such tissues are less excitable tissues.
Effect of ECF Na+, Ca2+ and K+ ions concentration on excitability level:
Decreasing the external Na+ ion concentration decreases the size of the action potential but has little effect on the excitability level.
Ca2+ ion concentration in ECF is important in modulating the activity of voltage-gated Na+ channels. The excess of positive charges of these Ca2+ ions (hypercalcemia) decreases the excitability of the nerve fiber by increasing the threshold level. On the other hand, when there is a deficit in Ca2+ ions in the ECF (hypocalcemia) increases the excitability of nerve fiber decreases the threshold level. Therefore, the nerve fiber becomes highly excitable; sometimes discharging repetitively and spontaneously without any provocation rather than remaining in the resting state causing a condition called muscle tetany in which there were contractions of the muscles of hands, causing them to assume the position illustrated in figure 4.6. Trousseau's sign is elicited by inflating a blood pressure cuff above systolic pressure for up to 3 minutes to induce ischemia in the arm through cuff, to exaggerate neuronal excitability to produce the characteristic sign. A positive sign is carpo-pedal spasm.
Figure 4.4: Actual time course for the action potential.
Figure 4.6: Trousseau's sign.
![Page 7: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/7.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 5
Both increases and decreases in the plasma (ECF) K+ concentration (normal concentration is between 3.5 and 5.0 mM) can alter the intracellular-to-extracellular K concentration gradient, which in turn can change the resting membrane potential. The most serious consequences of both K+ excess and K+ deficiency are related to their impact on the heart. Both conditions (excess or deficiency) result in decreased nerve and muscle excitability for different reasons.
1. A fall in ECF K+ concentration (hypokalemia) may associate with failure of eliciting an action potential. When the extracellular fluid K+ concentration falls, the RMP decreases below normal, i.e. hyperpolarization, and the membrane becomes less excitable). This shifting the membrane potential away from the threshold value is due to the following: The decrease in the extracellular concentration of K+ increases the K+ concentration gradient. As a result, the tendency for K+ to diffuse out of the cell increases, and a larger negative charge inside the cell is left. At this new equilibrium, the larger charge difference across the plasma membrane is a hyperpolarization.
In a hereditary disease known as familial periodic paralysis, the extracellular K+ ion concentration is often reduced that the person actually becomes paralyzed but reverts to normal after intravenous administration of K+. Hypokalemia is associated with skeletal, smooth, and cardiac muscle weakness and paralysis. 2. However, hyperkalemia, extracellular K is high prevent the passive flow more K retain in the cell RMP becomes less negative depolarization of the membrane. This decreases the excitability of these tissues because some of the voltage-gated sodium channels are inactivated and prevent the rapid sodium-induced spike of the action potential. Hyperkalemia causes heart to become dilated and flaccid with impaired cardiac conduction and arrest the heart in diastole. The inactivation of voltage-gated Ca++ at higher extracellular K+ concentration reduces the excitability of cardiac muscles and consequently the strength of myocardial muscles by reducing the release of Ca2+ into the sarcoplasm. Also it causes muscle weakness or paralysis, and depression of nerve excitability. Local anesthetics such as procaine and tetracaine and many other drugs act directly on the voltage-gated Na+ channels making them much more difficult for these gates to open and thereby reducing the membrane excitability and consequently the nerve impulse fails to pass through the anesthetized area. Table 4.3 summarizes the main differences between graded potential and an action potential.
![Page 8: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/8.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 6
Table 4.3: Differences of graded potential versus action potential.
Graded potentials Action potentials
Depending on the stimulus, graded potentials can be depolarizing or
hyperpolarizing.
Action potentials always lead to depolarization of membrane and reversal
of the membrane potential.
Amplitude is proportional to the strength of the stimulus.
Amplitude is all-or-none; strength of the stimulus determines the frequency of all-
or-none action potentials generated.
Amplitude is generally small (a few mV to tens of mV).
Large amplitude of ~100 mV.
Duration of graded potentials may be a few milliseconds to seconds.
Action potential duration is relatively short; 3-5 ms.
Ion channels responsible for graded potentials may be chemical, mechanical, or
electrical –gated channels
Voltage-gated Na+, Voltage-gated Ca++ and voltage-gated K+ channels are responsible
for the action potential.
The ions involved are usually Na+, K+, or Cl−.
The ions involved are Na+, Ca++ and K+ (for action potentials).
No refractory period is associated with graded potentials.
Absolute and relative refractory periods are important aspects of action potentials.
Graded potentials can be summed over time (temporal summation) and across
space (spatial summation).
Summation is not possible with action potentials (due to the all-or-none nature, and the presence of refractory periods).
Graded potentials travel by passive spread (electrotonic spread) to neighboring
membrane regions.
Action potential propagation to neighboring membrane regions is
characterized by regeneration of a new action potential at every point along the
way.
Amplitude diminishes as graded potentials travel away from the initial site
(decremental).
Amplitude does not diminish as action potentials propagate along neuronal
projections (non decremental).
In principle, graded potentials can occur in any region of the cell plasma membrane
Occur in plasma membrane regions where voltage-gated Na+ and K+ channels are
highly concentrated.
![Page 9: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/9.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 7
The action potential of the cardiac and smooth muscle fibers: However, in some tissues such as in cardiac muscles (atria, ventricles, and Purkinje fibers) and some smooth muscles, the excitable membrane does not repolarized immediately after depolarization but instead, the potential remains on a plateau near the peak of the spike for few millisecond before repolarization begins (figure 4.7). The causes of the action potential plateau seen in the cardiac and in some of smooth muscle fibers is due to the presence of voltage-gated Ca2+ channels.
In cardiac muscle fibers, there are voltage-gated Na+ channels responsible for the spike potential (i.e., the upstroke of action potential) (figure 4.7, circles 0), this is followed by the initial repolarization (figure 4.7, circles 1) which is due to opening of voltage-gated potassium channels. In addition, voltage-gated Ca2+ channels are responsible for the sustained depolarization, i.e. the plateau portion of action potential (figure 4.7, circle 2). Phase 3 (repolarization) results from an opening of voltage-gated potassium channels with consequent increase in K+ efflux and closure of voltage-gated Ca2+ channels with consequent decrease in Ca2+ influx. Phase 4 is a true resting potential that that remains near the equilibrium potential for K+. When heart rate is about 75 beats per minute, the mean duration of action potential in ventricular muscle cells is 200 msec.
In smooth muscle fibers such as intestinal smooth muscle, the spike potential and the plateau are both due to voltage-gated Ca2+ channels rather than sodium conductance. Consequently, the rates of rise of smooth action potentials are slow, and the durations are long relative to most neural action potentials. These channels are permeable mainly to Ca2+ ions (and much less to Na+) allowing Ca2+ ions to flow to the interior of the fiber. These channels are very slow (slow channels) to become activated (i.e. opened) in comparison to Na+ channel (fast channel). Activation of the fast channels causes the depolarized portion of the action potential; where as the slow and prolonged activation of the slow channels is mainly responsible for the plateau portion of this type of action potential. In cardiac muscles, repolarization is achieved by: [A] Closure of voltage-gated Na+ channels. [B] Closure of voltage-gated Ca2+ channels. [C] Activation of voltage-gated K+ channels. [D] Na+-K+ pump. [E] The Ca2+ pump. This pumps Ca2+ ions from the interior to the exterior of the cell membrane, creating a Ca2+ ion gradient of about 10,000-fold, leaving an internal concentration of Ca2+ ions of about 0.1 mM in contrast to an external concentration of about 1 mM. Re-establishment of the normal resting membrane potential: Transmission of each impulse by nerve decreases the concentration difference of Na+ and K+ across the cell membrane. After large number of impulses, the concentration difference will fall down to a point that action potential cannot be propagated. However, the concentration difference is re-established by the action of Na+-K+ pump. Activity of this pump is strongly stimulated when there is excess Na+ inside the cell. Re-establishment of normal concentration of Na+, K+ and Ca2+ ions across the membrane after the end of action potential is
Figure 4.7: The action potential of the cardiac and smooth muscle fibers.
![Page 10: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/10.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 8
an active metabolic process and is achieved by Na+-K+ pump and by Ca2+ pump. Both of which require energy extracted from ATP and causing a production of heat. Propagation of the action potential: An action potential elicited at any one point on an excitable membrane usually excites adjacent portion of the membrane, resulting in propagation of the action potential to all directions away from the stimulus until the entire membrane has become depolarized. This type of propagation of action potential is called continuous conduction. The mechanism of this propagation is as follow: When the stimulus induces an action potential at any point in an excitable membrane, it means that the membrane developed an increased permeability to Na+ at this point. Therefore, the positively charged Na+ ions flow inward through this depolarized point and spread to the adjacent resting membrane points along the core of the axon (figure 4.8). The inflow of Na+ ions through the first depolarized point of the membrane will create electropositivity on the inner side of the first depolarized point and also on the adjacent resting membrane points. This will change the membrane potential at the adjacent resting points to the threshold voltage value for initiating another new action potential adjacent to the first one, which in turn initiates another action potential, causing progressively more and more depolarization, causing progressively more and more depolarization. The transmission of the depolarization
process along a nerve or muscle fiber is called a nerve or muscle impulse. Repolarization of membrane occurs first at the point of original stimulus and then spreads progressively along the membrane, moving in the same direction that depolarization had previously spread. Rhythmicity (also called automaticity or spontaneous repetitive discharge) of certain excitable cells: Rhythmical cell is the cell that can generate action potential spontaneously (without external stimulus) and repetitively (repeats itself). The characteristics of cell membrane of the excitable cell are: [1] The threshold level for stimulation is low. [2] The cell membrane even in its natural resting state is more permeable to Na+/or Ca2+ ions than non-rhythmical cell. [3] The cell membranes show cyclic increase and decrease of the pumping of Na+ (by Na+-K+ ATPase pump) and Ca2+ ions (by Ca++
Figure 4.8: Diagrammatic representation for the propagation of the action potential.
Figure 4.9 A: RMP of the membrane of rhythmical cell.
![Page 11: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/11.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 9
ATPase pump) outward through the cell membrane. The membrane potential becomes more negative when the Na+ or Ca2+ ions are pumped rapidly and less negative when Na+ or Ca2+ pump becomes less active. This cyclic increase and decrease activity of Na+ or Ca2+ pump will lead to generate a continuous change in resting membrane potential locally (figure 4.9 A). This local wave-like change in resting membrane potential is of two types: Slow wave potential or pacemaker wave potential.
The high membrane
permeability in these tissues to Na+/or Ca2+ ions and the low activity of Na+ or Ca2+ pump will lead to increase concentration of these ions in the ICF and consequently increase the membrane potential progressively until the slow wave or pacemaker potential (pacemaker potential also called prepotential, and is synonym to graded potential in skeletal and nerve fiber) rises above the level of approximately -35 mV, the threshold level for the action potential. At threshold level, voltage-gated Na+ or voltage-gated Ca2+ channels become activated (as in the sinoatrial node, the atrioventricular node, and the bundle of His of the heart) and an action potential is elicited and spread over the rhythmical cell then contraction does occur. Toward the end of the depolarization, voltage-gated Ca2+ channels become inactivated and the membrane becomes excessively permeable to K+ due to activation of voltage-gated K+ channels. The excessive outflow of K+ ions carries tremendous numbers of positive charges to the outside of the membrane, creating inside the fiber considerably more negativity than would otherwise occur. This state is called hyperpolarization, which is the cause for the delay of the next depolarization to occur immediately after the end of first action potential. But shortly there after, the depolarization process begins again and a new action potential occurs spontaneously. Rhythmicity occurs normally in the sinoatrial node and atrioventricular node of the heart, in most smooth muscle, and in many of the neurons of the central nervous system (CNS). It is these rhythmical discharges that cause the heart to beat, that cause peristalsis, and that cause neuronal events as the rhythmical control of breathing. Noradrenalin released by the sympathetic nerve endings, or adrenaline circulating in the blood stimulate β1 receptors present on the SA node, the AV node, and the bundle of His of the heart causing an increase of inward Na+ and Ca2+ ions current. This increase in ions current causes a more steeper pacemaker potential slope (increased rate of upward drift of the membrane potential toward the threshold level) (figure 4.9 B). This causes acceleration of self-excitation (i.e. increase the rate of action potential generation). In contrast, acetylcholine released by the parasympathetic vagus nerve endings stimulates muscarinic receptors present on the SA node, the AV node, and the bundle of His of the heart. This stimulation greatly increases the permeability of the fiber membranes to potassium ions, which allows rapid leakage of potassium out of the conducting fibers. This causes increased negativity inside the fibers and less steeper of pacemaker potential slope (decreased rate of upward drift of the membrane potential toward the threshold level), an effect called hyperpolarization, which makes this excitable tissue much less excitable (figure 4.9 B). This causes deceleration of self-excitation (i.e. pecial the rate of action potential generation).
Figure 4.9 B: Effect of sympathetic and parasympathetic stimulation on pacemaker potential.
![Page 12: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/12.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 10
The Refractory Period: It is the period of time during which the second action potential is difficult or cannot occur in an excitable fiber as long as the membrane is still depolarized from the preceding action potential. The importances of refractory period are: (1) Limits how many action potentials can be produced during a given period of time and (2) Prevents an action potential from starting another action potential at the same point on the plasma membrane. This period can be of two types:
[1] Absolute refractory period: It is the period of time during which a second action potential in an excitable tissue cannot be elicited even with a very strong stimulus as long as the membrane is still depolarized from the preceding action potential. This period corresponds the period of depolarization and about one-third of repolarization (figure 4.10). The reason for this is that shortly after the action potential is initiated the voltage-gated Na+ channels become closed. And any amount of excitatory signal applied to these channels at this point will not reopen these channels. The only condition that will reopen them is for the membrane potential to return either to or almost to the original resting membrane potential level.
[2] Relative refractory period: It is the period of time during which a second action potential in an excitable tissue can be elicited if the strength of the applied stimulus is stronger than normal stimulus. This period follows the absolute refractory period and last from the end of the first 1/3 of repolarization to the end of hyperpolarization (figure 4.10). During this time, application of stronger than normal stimuli can excite the fiber. The causes of this relative refractory period are: A. During this time some the voltage-gated Na+ channels still have not been reversed from their closed state. B. The voltage-gated K+ channels are usually wide open at this time, so any tendency for Na+ ions to flow in is associated with K+ ions efflux. C. In addition, the end of this period of time is associated with the state of hyperpolarization that makes it more difficult to stimulate the fiber.
Figure 4.10: The refractory periods of skeletal and nerve fibers.
![Page 13: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/13.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 11
TThhee nneerrvvee:: The human nervous system contains about (100 billion) neurons. A typical nerve cell or
neuron has 5-7 processes called dendrites that extend out from the cell body (soma) and arborized extensively (figure 4.11). The dendrites are receptor membrane of the neuron which also has long cytoplasmic extension called the axon (nerve fiber) that originates from a thickened area of the cell body called axon hillock. The axon has a specialized function of conducting impulses away from the dendrites. To put this task into perspective, if we imagine the motor neuron cell body to be the size of a tennis ball, the axon running to a muscle in the hand would at this scale be about two kilometers long! The axon ends in a number of synaptic knobs (terminal buttons).
The cytosol of the terminal button has two important structures and these are the [1] mitochondria and [2] synaptic vesicles. In the synaptic vesicles, transmitter secreted by the nerve is stored. The mitochondria provide ATP, which is required to synthesize new transmitter substance. In addition, the wall of terminal button has two important structures and these are [1] voltage-gated Ca2+ channels and [2] Ca2+ pump (figure 4.11).
In association with “all” nerve fiber there are
cells called Schwann cells. In some nerves, a short distance from its origin, the axon acquires a sheath of myelin, which is multiple layers of cellular membrane of Schwann cells containing the lipid substance sphingomyelin. These types of nerve are called myelinated nerves. About once every mm along the axon, the myelin sheath is interrupted by nods of Ranvier. The end of axon is lack of myelin sheath. Schwann cells are found along peripheral nerves. In the CNS, most neurons are myelinated, but the cells that form the myelin are oligodendrogliocytes rather than Schwann cells. Furthermore, unlike Schwann cell, oligodendrogliocytes send off multiple processes that form myelin on many adjacent axons rather than wrapping one axon as in Schwann cell.
Sphingomyelin is an excellent insulator that prevents almost all flow of ions. However, at the juncture between each two successive Schwann cells along the axon, small and uninsulated areas remains (node of Ranvier) where ions can still flow with ease between the ECF and the ICF of the axon. In addition, voltage-gated Na+ channels are highly concentrated at the nodes of Ranvier. Neurotrophins: They are proteins that are necessary for survival and growth of neurons. Some of these are products of the muscles or other structures that the neurons innervate, but others are produced by
Figure 4.11: The nerve fiber and the terminal button.
![Page 14: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/14.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 12
Schwann cells and astrocytes. An example of neurotrophins is Nerve Growth Factor (NGF), Brain-Derived Neurotrophic Factor (BDNF). Each maintains a different pattern of neurons and preventing apoptosis. Myelination is important for the following reasons: [1] It increases the excitability of the nerve fiber: This is because the excellent insulation afforded by the myelin membrane substantially minimizes loss of ions and also decreases the membrane capacitance about fifty folds. Both of these effects allow depolarization and repolarization processes to occur with very little transfer of ions (i.e. increase excitability). Consequently, depolarization and repolarization is achieved mainly by the opening and closure of voltage-gated Na+ channels with very little contribution by K+ channels. The capacitance of the membrane per unit length determines the amount of charge required to achieve a certain potential and therefore affects the time needed to reach the threshold (i.e. increase excitability). Large capacitance values, with other parameters remaining the same, mean a slower conduction velocity. [2] It speeds up the conduction velocity of action potential along the nerve fiber by jumping from node to node. This is called saltatory conduction (figure 4.12). This mechanism increases the velocity of nerve transmission in myelinated fiber of an average of 5-50 times. [3] Saltatory conduction conserves energy for the axon, for only the nodes depolarize.
The number of Na channels per square micrometer of membrane in myelinated mammalian neurons is maximum in the Node of Ranvier. An axon can conduct in either direction when an action potential is initiated in the middle of it. One along the axon to the terminal buttons (orthodromic conduction) and the other along the axon back to the soma (antidromic conduction).
Various diseases of the central and peripheral nervous system (e.g., multiple sclerosis or Guillain-Barre Syndrome) cause groups of myelinated axons in certain areas to lose some or all of their myelin sheath. This demyelination of a segment of an axon causes slowed conduction velocity and, if severe, impulse conduction failure at the site of demyelination. Factors that affect the conduction velocity: 1. Myelination: myelinated nerve is about 50 times faster. 2. Axon diameter: in unmyelinated nerve axon, the conduction velocity is directly proportional to the square root of axon diameter while in the myelinated neuron conduction velocity increases directly with axon diameter, thus myelination saves considerable space in the nervous system. In small unmyelinated nerve axon, the conduction velocity is about 0.5 meter/second while in the largest myelinated nerve axon it is about 100 meter/second. As diameter increases, Velocity of conduction increases, Magnitude of electrical response increases, Threshold of excitation decreases, Duration of response decreases, Refractory period decreases. 3. Temperature.
Figure 4.12: Conduction of nerve impulse through myelinated nerve fiber.
![Page 15: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/15.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 13
Electrical properties of a nerve (nerve trunk): [1] Does not obey the all or none law: This mean that as the stimulus intensity increases, the amplitude of response (action potential) are increased. This is because the average nerve trunk contains about twice as many unmyelinated small nerve fibers as myelinated large nerve fiber. The velocity of conduction in nerve fibers varies from 0.5 m/s in very small unmyelinated fibers to up 100 m/s in very large unmyelinated fibers. The threshold of the individual axons in the nerve and their distance from the stimulating electrodes vary. With subthreshold stimuli, none of the axons are stimulated and no response occurs. When the stimuli are of threshold intensity, axons with low threshold fire and a small potential change is observed. As the intensity of the stimulating current is increased, the axons with higher thresholds are also discharged. The electrical response increases proportionately until the stimulus is strong enough to excite all of the axons in the nerve. This stimulus is called maximal stimulus. Further application of greater supramaximal stimuli produces no further increase in the size of the observed potential. [2] Generation of compound action potential: This mean that as the stimulus intensity increases, the duration of response (action potential) are increased with the appearance of multiple peaks (as opposed to single axons) in the action potential (called compound action potential) (figure 14.A). This is due to the fact a mixed nerve is made up of families of fiber with varying speeds of conduction. Glia: In addition to neurons, the nervous system contains glial cells (neuroglia). There are 10-50 times as many glial cells as neurons. In the peripheral nervous system there are two types of glial cells: [a] Schwann cells. [b] Satellite cells which are a type of glial cells that surround cell bodies of the neurons in ganglia. Satellite glial cells act as a regulator of neuronal microenvironment similar to astrocytes in the CNS.
In the central nervous system (CNS), there are four main types of glia (figure 4.13):
[a] Microglia (tissue macrophage) that are scavenger cells that enter the nervous system from the blood vessels. [b] Oligodendrogliocytes that are involved in myelin formation of the CNS neurons. [c] Astrocytes which are found throughout the brain (fibrous astrocytes in the white matter and protoplasmic astrocytes in the gray matter). The main functions of astrocytes are:
Figure 4.13: Different types of glial cells.
Figure 14.A: The graph is a reproduction of clinical recording of a monophasic compound action potential from a nerve that contains A, B, and C type fibers.
![Page 16: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/16.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 14
[1] Astrocytes send processes to the capillary blood vessels to form the tight junctions that contribute in the formation of the Blood-brain barrier (BBB) (figure 4.13). [2] They also send processes that envelop synapses and the surface of nerve cells. [3] They produce substances that are trophic (promoting cellular growth, differentiation, and
survival) to neurons. [4] They help maintain the appropriate concentration of substances in the interstitial fluid by taking up K+ ions and neurotransmitters (glutamate and GABA). Without rapid K+ reuptake, [K+] increases and depolarizes neuronal resting membrane potentials. [5] To provide neurons with lactate as an energy source. [6] To synthesize neurotransmitter precursors for neurons (e.g., glutamine synthesis for glutaminergic neurons).
[d] Ependymal cells are the epithelial-like cells that form a thin epithelial membrane lining the ventricular system of the brain and the spinal cord. It. Ependyma is one of the four types of neuroglia in the central nervous system. It is involved in the production of cerebrospinal fluid (CSF). Classification of nerve fibers:
[i] The fibers can be classified according to their
conduction velocity into the following general types: 1. Type A fibers: They are the typical have a large diameter and they are myelinated fibers of spinal nerves that conduct impulses at high velocities (6-120 m/sec). They include according to the conduction velocity, they subdivided in descending order into: Alpha (α) fibers (also called type 1a): They are motor fibers to the skeletal muscles (alpha motor neurons), also they the sensory fibers from the skeletal muscles (muscle spindle and Golgi tendon organ). Beta (β) fibers (also called type 1b): Act as secondary sensory fibers to the skeletal muscle spindle (this information would indicate the position of one's limb once it has stopped moving, i.e. conscious proprioception), and contribute to fine touch, pressure and vibration. Gamma (γ) fibers: They are typically motor neurons that control the intrinsic activation of the skeletal muscle spindle. Delta (δ) fibers: They are free nerve endings that conduct stimuli related to fast pain, touch, pressure, and cold temperature.
The susceptibility of the fibers to pressure, hypoxia, and local anesthesia is shown in the table. 2. Type B fiber: They are myelinated fibers that conduct impulses at lower velocity than type A nerve fibers. Generally, they are the preganglionic fibers of the autonomic nervous system (ANS), and have a low conduction velocity. 3. Type C fibers: They are very small unmyelinated nerve fibers that conduct impulses at low velocities. These fibers include: Postganglionic fibers in the ANS, nerve fibers at the dorsal roots of the spinal cord (these fibers carry the following sensory information: slow pain, warmth and cold temperature, touch, pressure, itch).
[ii] The fibers can be classified according to the direction in which they conduct impulses. Sensory, or
afferent neurons (figure 4.13 A), conduct impulses from sensory receptors into the CNS. Motor, or efferent neurons conduct impulses out of the CNS to effector organs (muscles and glands). Interneurons, are located entirely within the CNS and serve the associative, or integrative functions of
Susceptibility to Most
susceptible
Least
susceptible
Pressure A C
Hypoxia B C
Local anesthetics
C A
![Page 17: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/17.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 15
the nervous system. There are two types of motor neurons: somatic and autonomic. Somatic motor neurons are responsible for both reflex and voluntary control of skeletal muscles. Autonomic motor neurons innervate (send axons to) the involuntary effectors—smooth muscle, cardiac muscle, and glands. The cell bodies of the autonomic neurons that innervate these organs are located outside the CNS in autonomic ganglia.
[iii] The structural classification of neurons is
based according to the number of processes that extend from the cell body of the neuron (figure 4.13 B). Unipolar neurons (also called pseudounipolar neurons) have a single short process that branches like a T to form a pair of longer processes. Sensory neurons are unipolar. One of the branched processes receives sensory stimuli and produces nerve impulses; the other delivers these impulses to synapses within the brain or spinal cord. Anatomically, the part of the process that conducts impulses toward the cell body can be considered a dendrite, and the part that conducts impulses away from the cell body can be considered an axon. Functionally, however, the two branched processes behave as a single long axon; only the small projections at the receptive end of the process function as typical dendrites. Bipolar neurons have two processes, one at either end; this type is found in the retina of the eye. Multipolar neurons, the most common type, have several dendrites and one axon extending from the cell body; motor neurons are good examples of this type.
Regeneration of peripheral nerve fibers: The peripheral nervous system is able to repair and regenerate itself, but the central nervous system is incapable of doing so. Nerves can be easily damaged in a traumatic event due to their sometimes vulnerable positions in the body. However, if a nerve is damaged, it does have the ability to regenerate if its soma and a small portion of the neurilemma remain. The proximal segment can either die by apoptosis or attempts at repair The nerve begins the process by destroying the axon distal to the site of injury (Wallerian degeneration) allowing Schwann cells, basal lamina, and the neurilemma near the injury to begin producing a regeneration tube. Nerve growth factors are produced causing many nerve sprouts to bud. When one of the growth processes finds the regeneration tube, it
Figure 4.13 B: The structural classification of neurons.
Figure 4.13 A: Classification of nerve fiber
according to the direction in which they conduct impulses.
![Page 18: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/18.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 16
begins to grow rapidly towards its original destination guided the entire time by the regeneration tube. Nerve regeneration is very slow and can take up to several months to complete. While this process does repair some nerves, there will still be some functional deficit as the repairs are not perfect.
![Page 19: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/19.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 17
SSyynnaappttiicc ttrraannssmmiissssiioonn:: Impulses are transmitted from one nerve cell to another at synapses.
These are the junctions where a terminal of an axon of one cell (presynaptic cell) terminates on the soma or dendrites of another neuron (the postsynaptic cell) (figure 4.14). Transmission at most of junction is chemical; the impulse in the presynaptic axon liberates a chemical mediator from its terminals called (neurotransmitters). The chemical mediator binds to receptors on the surface of the postsynaptic cell, and this triggers intracellular events that alter the permeability of the membrane of the postsynaptic neuron. Almost all the synapses utilized for signal transmission in the CNS are chemical synapses which transmit the signals in one direction, that is from the neuron that secretes the transmitter (presynaptic neuron) to the neuron on which the transmitter acts (postsynaptic neuron). At some of the junction, however, transmission is electrical where the membrane of the presynaptic and postsynaptic neurons come close together forming a gab junctions which are low resistance bridges through which ions pass with relative ease. Only a few gap junctions have been found in the CNS. Through gap junctions the action potentials are transmitted in both directions from one smooth or cardiac muscle to the next.
Physiological anatomy of the synapse: The synapse composed of (figure 4.14):
1. An enlarged area of presynaptic terminal called terminal buttons or synaptic knobs. The synaptic vesicles contain a transmitter substance which when released into the synaptic cleft; either excites or inhibits the postsynaptic neuron. This excitation or inhibition depends on the type of the receptors at the postsynaptic neuron whether excitatory or inhibitory receptors. 2. Synaptic cleft that separate the two neurons by about 200-300 angstroms. 3. The cell membrane of the postsynaptic neuron which is soma, the dendrites, or some other portion of postsynaptic neuron. The cell membrane of the postsynaptic neuron contains receptor proteins, which interact with the neurotransmitter and bring about excitation or inhibition of the postsynaptic neuron. Transmission of signal or impulse across the synapse: When the action potential depolarizes the terminal, large number of voltage-gated Ca2+ channels at the terminal membrane open and consequently large number of Ca2+ ions flow into the terminal (figure 4.14). The influx of Ca2+ ions into the terminal initiates the process of exocytosis of the terminal vesicles, which fuse with the presynaptic membrane and release its content of the neurotransmitter. The quantity to transmitter substance that is released into the synaptic cleft is directly related to the number of Ca2+ ions that enter the terminal. Therefore, any condition that reduces the quantity of Ca2+ ions entering the presynaptic terminal also
Figure 4.14: Transmission of signal or impulse across the synapse.
![Page 20: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/20.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 18
will decrease the amount of transmitter released. The transmitter then diffuses across the synaptic cleft and interacts with receptors at the postsynaptic membrane. The result of interaction is one of the following:
[1] May leads to open the neurotransmitter-gated Na+ or Ca2+ channels that allow Na+ or Ca2+ ions to pass through the cell membrane resulting in bringing the membrane potential of the postsynaptic membrane to threshold level. This local change in membrane potential is a graded potential and is called excitatory postsynaptic potential (EPSP). Summation of many EPSPs causes change in the postsynaptic cell membrane potential to the threshold level with consequent generation of action potential and excitation of postsynaptic cell.
[2] May lead to open neurotransmitter-gated Cl- or K+-channels that allow mainly Cl- or K+ ions to pass through with consequent hyperpolarization of the membrane toward the Cl- or K+ ion equilibrium potential (-90 mV) resulting in inhibition of cell due to hyperpolarization of the membrane. This local change in membrane potential (hyperpolarization) is a graded potential and is called inhibitory postsynaptic potential (IPSP). The inhibitory neurotransmitters are γ-aminobutyric acid (GABA) and glycine.
[3] May lead to activate enzymes, which in turn activates an internal metabolic system “second messenger” of the cell resulting in either increase or decrease the number of receptors or prolonged changes in neurons. Such changes can alter the reactivity of the synapse for minutes, days, months or even years. Therefore, transmitter substances that cause such effects are called synaptic modulators.
The resting membrane potential in the soma of a motor neuron is about –65 mV. Any change in potential in any part of the intrasomal fluid causes an almost exactly equal change in potential at all other points inside the soma. This is because in the interior of the neuronal soma contains a very highly conductive electrolytic solution and there is almost no resistance to conduction of electrical current from one part of the soma interior to another part.
When neurotransmitter acts on a postsynaptic membrane excitatory receptor it will causes an opening of neurotransmitter-gated Na+ channels. The rapid influx of the positively charged Na+ ions to the interior of the neuron neutralizes part of the negativity of the resting membrane potential, i.e. increase in the resting membrane potential toward 0. This local increase in voltage above normal resting membrane potential is called excitatory postsynaptic potential (EPSP). Excitation of a single presynaptic terminal on the surface of a neuron will almost never excite the neuron because of insufficient transmitter released by a single terminal to cause an EPSP of a sufficient magnitude to elicit an action potential. In order to elicit an action potential in the postsynaptic neuron, the resting membrane potential of the soma of the postsynaptic neuron has to increase from –65 to the threshold level of –45 mV. This magnitude of change in potential (from –65 to –45 mV) in the soma of postsynaptic neuron requires the summation of many EPSP generated at the membrane of the postsynaptic neuron (figure 4.15, and 4.16). There are two types of summation: [1] Spatial summation: In which many presynaptic terminals that end (converge) on the membrane of a single soma are stimulated at the same time (figures 4.15 and 4.16). Therefore each EPSP/or IPSP will be added to the others. [2] Temporal summation: In which presynaptic terminals fire repetitively in rapid succession. Each time a terminal fire, the released transmitter substance opens the membrane channels causing EPSP or IPSP. A second opening of the same channel can increase the EPSP or IPSP to a still greater level so that the more rapid the rate of terminal stimulation, the greater the effective postsynaptic potential.
![Page 21: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/21.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 19
When summation of EPSPs has not raised high enough to reach the threshold for eliciting an action potential, the neuron is said to be facilitated. That is its membrane potential is nearer to the threshold for firing than normally but not yet to the firing level. A signal entering the neuron from soma of other source can then excite the neuron very easily. In order to change the postsynaptic membrane potential, summation of EPSPs should occur.
When the membrane potential inside the soma rises high enough, i.e. about –45 mV, action potential begins in the postsynaptic neuron at the axon hillock, and not on the soma membrane adjacent to the excitatory synapses. The main reason for this is that the soma has relatively few voltage-gated Na+ channels in its membrane, which are less than enough required to elicit an action potential. On the other hand, the membrane of the axon hillock has seven times as great a concentration of voltage-gated Na+ channels and therefore can generate an action potential. Once the action potential begins, it travels both peripherally along the axon and also backward over the soma and some of the dendrites. However, many dendrites fail to transmit action potentials because their membranes have relatively few voltage-gated Na+ channels, so that their thresholds for excitation are very high.
Chemical substances that function as neurotransmitters: More than 50 different chemical substances have been described as being synaptic neurotransmitter. Their excitatory or inhibitory effects are depending on location. These neurotransmitters are classified into two groups:
Small-molecule, rapidly acting transmitters.
Large-molecule, slowly acting transmitters (neuropeptides).
Figure 4.15: Convergence of many presynaptic terminals on single post synaptic neuron.
Figure 4.16: Spacial summation of EPSPs.
![Page 22: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/22.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 20
[1]. Small-molecule, rapidly acting transmitters which are usually synthesized in the cytosol of the presynaptic terminal and then are absorbed by active transport into the transmitter vesicles in the terminal. The small-molecule transmitters include four different classes of transmitter substances:
Class 1: Acetylcholine.
Class 2: Several different amines such as norepinephrine, epinephrine, dopamine, serotonin, and histamine.
Class 3: several different amino acids such as gamma-aminobutyric acid (GABA), glycine, glutamate, and aspartate. Most excitatory neurotransmission in the brain is mediated by glutamate. The common inhibitory amino acid neurotransmitter in the CNS is GABA that generates IPSPs due to chloride influx. Glycine is inhibitory amino acid neurotransmitters in the CNS and spinal cord. Strychnine blocks glycine receptors, resulting in uncontrolled convulsions and respiratory arrest. Glutamate, aspartate, and cysteine are three amino acids that excite our neurons and can be called "excitotoxins." They are now added in large amounts to our food supply.
Class 4: nitric oxide (NO). It is present in areas of brain that are responsible for long-term behavior and memory.
[2]. Large-molecule, slowly acting transmitters (neuropeptides): They are synthesized by the ribosomes in the in the soma. The vesicles containing the neuropeptide are transported slowly all the way to the tips of the nerve fibers by axonal streaming of axon cytoplasm. Finally, these vesicles release their transmitter in response to action potentials in the same manner as for small-molecule transmitters. They include (A) hypothalamic-releasing hormones, (B) pituitary peptides, (C) peptides that act on gut and brain ( pecial os, substance P, gastrin, CCK, VIP, insulin, glucagon), and (D) neuropeptides from other tissues (angiotensin II, bradykinin, carnosine, sleep peptides, calcitonin).
The primary inhibitory neurotransmitters of the CNS are γ-aminobutyric acid (GABA) and
glycine, examples of small molecule transmitters. Sedative-hypnotic drugs (e.g., benzodiazepines, barbiturates, and alcohols) target the GABA receptor, which, through the action of increased Cl− influx, results in membrane hyperpolarization. Caution must be used with these drugs because there is a dose-dependent depression of the CNS: sedation → anxiolysis → hypnosis → anesthesia → medullary depression (respiratory depression) → coma. Synergism with other CNS depressants occurs, increasing the risk for potentially lethal overdoses.
Removal of the transmitter from the synapse: After the transmitter agent binds with the receptors, is rapidly removed from the synaptic cleft. This is achieved in three different ways:
1. By diffusion of the transmitter out of the cleft into the surrounding fluids. 2. By enzymatic destruction within the cleft itself. For instance, in the case of acetylcholine, the
enzyme cholinesterase is present in the cleft and inactivates this transmitter substance. 3. By active transmitter re-uptake; many of the transmitters are actively transported back into the
presynaptic terminal itself and are then reused again and again. Fatigue of synaptic transmission: When excitatory synapses are repetitively stimulated at a rapid rate, the number of discharges by postsynaptic neuron is at first very great, but it becomes progressively less in succeeding milliseconds or second. This is called synaptic fatigue. Fatigue is an exceedingly important characteristic of synaptic transmission, for when areas of the nervous system become overexcited (e.g. epileptic fit), fatigue causes them to lose this excess excitability after a while (termination of the epileptic fit). The mechanism of fatigue is mainly due to exhaustion of the stores of the transmitter substance in the synaptic terminal.
![Page 23: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/23.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 21
Effect of acidosis and alkalosis on synaptic transmission: Alkalosis greatly increases neuronal excitability due to the reduction in the free ECF Ca2+ ions concentration (hypocalcaemia) (but not the total Ca2+ concentration), which modulates the activity of voltage-gated Na+ channels. A rise in arterial pH from normal of 7.4 to about 7.8 often causes cerebral convulsions because of increased excitability due to the decrease in the free ECF Ca2+ ions concentration (hypocalcaemia) (but not the total Ca2+ concentration), which modulate the activity of voltage-gated Na+ channels of the neurons. A fall in pH from 7.4 to below 7.0 usually causes greatly decreases neuronal excitability due to the increase in the free ECF Ca2+ ions concentration (hypercalcaemia) (but not the total Ca2+ concentration), which modulate the activity of voltage-gated Na+ channels and often causes comatose state as it occurs in diabetic or uremic acidosis. Effect of drugs on synaptic transmission: Cessation of oxygen supply for only few seconds can cause complete inexcitability of neurons. Caffeine, theophylline and theobromine, which are found in coffee, tea, and cocoa, respectively, all increase neuronal excitability, presumably by reducing the threshold for excitation of the neurons. However, strychnine does not reduce the threshold for excitation of the neurons but inhibits the action of some of the inhibitory transmitters on the neurons. In consequence, the effects of the excitatory transmitter become overwhelming, and the neurons becomes so excited that they go into rapidly repetitive discharge, resulting in sever convulsions. Tetrodotoxin inhibits the firing of action potentials in nerves by binding to the voltage-gated sodium channels in nerve cell membranes and blocking the passage of sodium ions (responsible for the rising phase of an action potential) into the nerve cell Most anesthetics increase the membrane threshold for excitation and thereby decrease synaptic transmission at many points in the nervous system. Synaptic delay: It is the minimum period of time required for transmission of an action potential from presynaptic neurons to a postsynaptic neuron which is about 0.5 ms. The causes of this delay are:
A. A time for discharge of the transmitter substance by the presynaptic terminal, B. A time for diffusion of the transmitter to the postsynaptic neuronal membrane, C. A time for the action of the transmitter on the membrane receptors, D. A time for the action of the receptor to increase the membrane permeability and E. A time for inward diffusion of Na+ to raise the excitatory postsynaptic potential to a high enough
value to elicit an action potential.
Synaptic plasticity: Synapses are not fixed for life; in response to experience, they can be added, taken away, or modified to make transmission easier or harder. This ability of synapses to change is called synaptic plasticity. It is the changes in the synaptic functions as a result of the history of discharging at a synapse, i.e. synaptic conduction can be strengthened or weakened on the basic of past experience. Think about when you learned as a child to tie your shoes. The procedure was very slow, confusing, and laborious at first, but eventually it became so easy you could do it with little thought—like a motor program playing out in your brain without requiring your conscious attention. It became easier to do because the synapses in a certain pathway were modified to allow signals to travel more easily across them than across “untrained” synapses. These changes can be presynaptic or postsynaptic. These changes are of the following forms:
1. Short-term post-tetanic potentiation (PTP): It is the production of short (few sec to few hours) postsynaptic potentials as a result of a brief (tetanizing) train of stimuli in the presynaptic neuron. It is due to the buildup of excess Ca2+ ions in the presynaptic neuron and consequently a continuous release of neurotransmitter.
![Page 24: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/24.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 22
2. Long-term potentiation (LTP): It is the production of long (days) postsynaptic potentials as a result of a brief (tetanizing) train of stimuli in the presynaptic neuron. It is due to the buildup of excess Ca2+ ions in the postsynaptic neuron and consequently alters the phosphorylation of intracellular proteins in a way that leads to greater EPSPs in response to stimulation of presynaptic terminals. Glutamate-induced increase in intracellular Ca++ is a key player in LTP. 3. Postsynaptic habituation: It is gradual decrease of postsynaptic response to a continuous presynaptic stimulation. It is due to decrease of the presynaptic neurotransmitter release as a result of inactivation of voltage-gated Ca2+ channels at the terminal button membrane with consequent reduction of Ca2+ influx and reduction of intracellular terminal button Ca2+ ion concentration.
![Page 25: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/25.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 23
TTrraannssmmiissssiioonn ooff iimmppuullsseess ffrroomm nneerrvveess ttoo sskkeelleettaall mmuussccllee ffiibbeerrss:: TThhee nneeuurroommuussccuullaarr
jjuunnccttiioonn:: The skeletal muscles are innervated by large myelinated nerve fibers that originated from
anterior horns of the spinal cord. As the axon supplying a skeletal muscle fiber approaches its termination, it losses its myelin sheath and divides into a number of branches. Each nerve fiber is divided many times to form a complex of branching nerve terminals which invaginates into an invaginated muscle fiber membrane called the synaptic gutter (figure 4.17). The junction between the nerve terminal and the muscle fiber is called the neuromuscular junction which is located at the fiber midpoint so that the action potential in the muscle fiber travels in both directions. The space between the terminal and the fiber membrane is called the synaptic cleft which is occupied by spongy reticular fibers called basal lamina through which diffuses ECF. The bottom of the gutter (which is the part of the muscle fiber membrane) adjoining the nerve terminal is called the motor end plate. In the motor end plate, there are numerous smaller folds of the muscle fiber membrane called subneural clefts, which greatly increase the surface area of motor end plate at which the synaptic excitatory acetylcholine (Ach) transmitter can act. The acetylcholine is synthesized in the cytoplasm of the nerve terminal but is rapidly absorbed into many small synaptic vesicles. Attached to the matrix of the basal lamina are large quantities of the enzyme acetylcholinestrase, which is capable of destroying acetylcholine.
When the action potential arrives at the nerve terminal (figure 4.17 circle 1), this opens many
voltage-gated Ca2+ channels at the nerve terminal (figure 4.17 circle 2). As a result, the Ca2+ ion concentration in the terminal increase about a hundred-fold, which in turn increases the rate of fusion of the Ach vesicles with the terminal membrane by about 10,00-fold. As each vesicle fuses, its outer surface ruptures through the cell membrane, thus causing exocytosis of Ach into the synaptic cleft (figure 4.17 circle 3).
Figure 4.17: Anatomy of thhee neuromuscular junction.
![Page 26: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/26.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 24
Within about 1 msec after Ach is released by the axon terminal (figure 4.17 circle 4), much of it has already diffused out of the synaptic gutter and no longer acts on the muscle fiber membrane, and all the remaining is destroyed by the acetylcholinestrase in the basal lamina lying between the nerve terminal and the subneural clefts. However, the very short period of time that Ach remains in contact with the muscle fiber membrane is almost always sufficient to excite the muscle fiber. The rapid removal of the Ach prevents re-excitation after the muscle fiber has recovered from the first action potential.
During this very short time of Ach release, it interacts with nicotinic Ach-gated ion channels (the name is due to the nicotinic type of receptors attached to the gated channel and to which Ach is interacted with). The interaction of Ach with the receptors causes conformational changes in these transmembrane channel proteins that lead to open the Ach-gated channels (figure 4.17 circle 5). These channels allow Na+ and K+ ions to flow though the channels. Because the channels opened by Ach conduct both Na+ and K+ ions, the postsynaptic membrane potential is depolarized to a value halfway between the Na+ and K+ equilibrium potential. This means that the membrane potential in the local area of the muscle fiber to increase in the positive direction, creating a local depolarizing potentials called the end-plate potential. This local change in membrane potential is graded potentials. If the summation of many end-plate potentials is sufficient enough, it may activate voltage-gated Na+ channel. Consequently, propagated action potential will occur (figure 4.17 circles 6, 7 and 8).
If a single vesicle releases its contents of Ach molecules (i.e., a quantum), the membrane will depolarize by approximately 1 mV. At rest, small quanta (packets) of acetylcholine are release randomly from the nerve cell membrane. Each producing a minute local depolarization of the membrane called a miniature end-plate potential.
Drugs that affect transmission at the neuromuscular junction: Drugs acting at the NMJ are used: i) as research tools; ii) therapeutically, as treatments for various neuromuscular disorders; and iii) cosmetically, e.g. ‘Botox’ for ironing-out wrinkling of facial skin. Clinical uses of neuromuscular blocking drugs (functional antagonists) include surgery to increase muscle relaxation under anesthesia. On the other hand, drugs that enhance neuromuscular function (functional agonists) are used clinically to treat diseases like myasthenia gravis or Lambert-Eaton Myasthenic Syndrome (LEMS). 1. Drugs that stimulate the muscle fiber by Ach-like action (agonists) or causing excessive release of Ach: Many different compounds including methacholine, carbachol, and nicotine, have the same effect on the muscle fiber, as does Ach. The difference between these drugs and Ach is that they are not or very slowly destroyed by acetylcholinestrase, so that when moderate quantities applied to the muscle fiber their action persists for many minutes to several hour causing repeated action potentials and consequently a state of muscle spasm. On the other hand, when extreme dose of these drugs are used it causes a state of flaccid paralysis rather than spasm. These effects are due to the fact that prolonged action of Ach or Ach-like drugs causes the Ach-gated ion channels to become desensitized and
Because entry of calcium from the extracellular medium is required for vesicle mobilization and fusion with the presynaptic membrane, altering the extracellular calcium concentration affects the number of vesicles released by each nerve action potential. Increasing extracellular calcium concentration increases the number of vesicles released. Conversely, decreasing extracellular calcium concentration decreases the number of vesicles released, and, if extracellular calcium is too low, can impair neuromuscular transmission. Extracellular magnesium acts just the opposite to calcium. Increasing extracellular magnesium decreases the number of vesicles released by a nerve action potential, most likely by inhibiting the entry of calcium into the nerve terminal. Thus, high extracellular magnesium, as might be seen in patients using large quantities of magnesium-containing salts (e.g., Maalox or Epsom salts) can lead to impaired neuromuscular transmission. Conversely, decreased extracellular magnesium increases the number of vesicles released.
![Page 27: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/27.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 25
inactivated. Black widow spider toxin causes an excessive release of vesicles. This causes muscle spasms, cramping pain, and generalized nervous excitation. Drugs belong to this group can also works by blocking presynaptic potassium channels, prolonging the duration of the presynaptic action potential. The prolonged depolarization allows excessive Ca2+ ions to enter the terminal through voltage-gated Ca-channels, increasing vesicular fusion rate and hence more Ach release and more EPSP generation.
2. Drugs that stimulate the neuromuscular junction by inactivating acetylcholinestrase: Such as neostigmine, physostigmine, and organophosphates (organophosphates include insecticides and so-called nerve gases, diisopropyl pecial osphates). Therefore, inactivated acetylcholinestrase (by anticholinesterase agents) in the synapses will not hydrolyse the acetylcholine released at the end-plate. As a result, acetylcholine increases in quantity with successive nerve impulses so those extreme amounts of acetylcholine can accumulate and then repetitively stimulate the muscle fiber (spastic paralysis, a state of continual contraction of the muscle). This causes muscular spasm when even a few nerve impulses reach the muscle, which can cause death due to laryngeal spasm.
3. Drugs that inhibit transmission at the neuromuscular junction and cause paralysis of the muscles: This can achieved by drugs that:
Inhibit Ach synthesis,
Prevent filling (storage) of the vesicles with acetylcholine,
Inhibit exocytosis of the ACH-containing vesicles (such Mg2+ ions which with compete with Ca2+).
Block vesicular release of Ach (such as Botulinus toxin) by preventing fusion of synaptic vesicles with the nerve terminal plasma membrane. Botulinum toxin is produced by the anaerobic bacillus Clostridium botulinum, which may be found in improperly canned food, and is one of the most potent toxins known. This toxin (the agent responsible for botulism) blocks the release of vesicles. This, of course, leads to muscle paralysis (flaccid paralysis, which is a state in which the muscles are limp and cannot contract) and, if the diaphragm becomes affected, can be fatal.
Compete with acetylcholine for the receptor sites of the end-plate membrane at the nerve terminal. Curariform drugs can prevent passage of impulses from the nerve terminal to the end-plate of the muscle fiber. This can be achieved by competing with acetylcholine for the receptor sites of the end-plate membrane, so that the acetylcholine cannot increase the permeability of the acetylcholine channels sufficiently to initiate a depolarization wave.
Myasthenia gravis: The disease of myasthenia gravis causes the person to become paralyzed because of inability of the neuromuscular junction to transmit signals from the nerve fibers to the muscle fibers due to the reduction in the Ach-gated ion channels. Consequently, the end-plate potentials developed in the muscle fiber are too weak to stimulate the muscle fibers adequately. Usually occurs in women between the ages of 20 and 40. It is an autoimmune disease in which antibodies attack the neuromuscular junctions. The effects often appear first in the facial muscle and commonly include drooping eyelids and double vision (due to weakness of the eye muscles). The initial symptoms are often followed by difficulty in swallowing, weakness of the limbs, and poor physical endurance. Lambert-Eaton syndrome is a neurologic condition resulting from autoantibodies that bind to and block Ca2+ channels on the presynaptic motor nerve terminals. By blocking the Ca2+ channels, the Ca2+-dependent exocytosis of vesicles filled with acetylcholine (a neurotransmitter needed for muscle contraction) is inhibited, resulting in muscle weakness.
![Page 28: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/28.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 26
TThhee sskkeelleettaall mmuussccllee:: All skeletal muscles are made of numerous of fibers (multinucleated muscle cells) ranging between 10 and 80 microns in diameter. In most muscles the fibers extend the entire length of the muscle and each of them is innervated by only one nerve ending, located near the middle of the fiber.
Properties of skeletal muscles: Excitability. The ability to respond to certain stimuli by producing electrical signals called action
potentials (or nerve impulses).
Contractility. When a muscle is stimulated above its threshold, it will start to contract, which generates tension between its origin and insertion points.
Conductivity. The ability to transmit action potential over the surface of cell membrane.
Tonicity. Even when muscles at rest, a certain amount of contraction usually remain. This residual degree of contraction in skeletal muscle is called muscle tone.
Each muscle fiber contains myofibrils suspended in the matrix (sarcoplasm). The fluid of the matrix contains K+, Mg2+, phosphate, protein enzymes, mitochondria, and an extensive endoplasmic reticulum (Sarcoplasmic Reticulum, SR). Sarcoplasmic reticulum composed of longitudinal tubules that terminate in large chambers called terminal cisternae that come very close to another tubular system called transverse tubules (T- tubules) (figure 4.18 A). T tubules originate from the cell membrane and are opened to ECF and penetrate all away through the muscle fiber from one side to the other and they branch among themselves and interlacing among all the separate myofibrils. The function of these T tubules is to transmit the action potential that spread over the surface of the skeletal muscle fiber to the deep interior within the fiber.
The sarcoplasmic reticulum and especially the cisternae contain high concentration of Ca2+ ions.
At the wall of the sarcoplasmic reticulum two important structure are present and these are: [1] Ryanodine Ca2+-releasing channel (as in skeletal and cardiac muscles) or IP3-Ca2+ releasing channel (as in smooth muscles) through which Ca2+ ions can pass from inside of SR to ICF and, [2] Ca2+ pump which pumps Ca2+ ions back from ICF to inside of SR. The wall of T tubule contains dihydropyridine (DHP) receptors (because they are blocked by the drug dihydropyridine) which act as:
Figure 4.18 A: Microscopic appearance of skeletal muscle fiber.
![Page 29: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/29.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 27
Voltage sensor in skeletal muscles fiber. Once these receptors activated, it will activate Ryanodine Ca2+-releasing channel at the wall of cisternae and consequently lead to efflux of Ca2+ from SR to sarcoplasm (ICF).
Voltage sensor and also Ca2+ channels in the cardiac muscle fiber. Once these channels are open as a result of the voltage change in wall of cardiac muscles; it allows Ca2+ to enter from ECF to ICF through DHP-Ca2+ channels. This calcium binds to Ryanodine Ca2+-releasing channel on the sarcoplasmic reticulum, opening them and releasing a greater quantity of Ca2+ from the SR into the cytosol (Ca2+-induce Ca2+-releasing channels). The SR provides 90% of the Ca2+ needed for myocardial contraction. In order to avoid confusion, it is worth to mentioned that ryanodine Ca2+-releasing channel on the sarcoplasmic reticulum can be activated and open its gate to the efflux of Ca2+ from inside of SR to the cytosol by two means:
Voltage-induce conformation change of DHP receptors at the wall of T tubule (as in skeletal muscles).
Ca2+ influx from ECF into the cytosol and induced a further increase in cytosolic Ca2+ through ryanodine Ca2+-induce Ca2+-releasing channels (as in cardiac muscles)
Each myofibril consists of: [1] Myosin filaments (thick filaments and each myosin filament is composed of about 200 myosin molecules). There are small projections from the sides of the myosin filaments along their entire extent (except in the very center) called cross-bridge (which are the heads of myosin molecules (figure 4.18 B). It is interaction between these cross-bridges and actin filaments that causes contraction. Myosin head can function as an ATPase enzyme to cleave ATP and to use the energy derived from ATP to energize the contraction process. [2] Actin filaments (thin filaments), which is composed of three different components: double-stranded F-actin protein, double-stranded
Figure 4.19: Muscle striations.
Figure 4.18 B: Myosin and actin filaments.
![Page 30: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/30.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 28
tropomyosin protein, and troponin (figure 4.18 B). Troponin protein holds F-actin and tropomyosin together so that the tropomysin protein covers the active sites (ADP molecules) that are present on the F-actin molecule (figure 4.18 B). Troponin protein is a complex of three globular protein molecules. Troponin I has strong affinity for actin. Troponin T has strong affinity for tropomyosin. Troponin C has strong affinity for Ca ions. Troponin I and T complex is believed to attach the tropomyosin to the actin. Troponin C is believed to initiate the contraction process. Active sites are the sites to which myosin heads are interact with. Under E.M. the myosin and actin filaments partially interdigitate and thus cause the myofibrils to have alternate light bands (contain only actin filaments and called I-bands) and dark bands (contain the myosin filaments as well as the end of the actin filaments overlapping the myosin and called A-bands) (figure 4.19). The actin filaments are attached to the so-called Z-disc, and extend on either side of the Z-disc to interdigitate with myosin filaments. Z-disc composed of filament proteins that also attaching the myofibrils to each other all the way across the muscle fiber. These bands give skeletal and cardiac muscle fiber that appearance. The portion of a myofibril or of the whole muscle fiber that lies between two successive Z-discs is called a sarcomere. When the muscle fiber is at its normal, fully relaxed resting length, the length of sarcomere is about 2 microns. At this length, the actin filaments completely overlap the myosin filaments and just beginning to overlap each other.
When a muscle fiber is overstretched beyond its resting length, the ends of the actin filaments pull apart; leaving a light area in the center of the A-band called the H-zone. On the other hand, in the contracted state these actin filaments have been pulled inward among the myosin filaments so that they now overlap each other to a major extent. Also, the Z-discs have been pulled by the actin filaments up to the ends of myosin filaments. This sliding is generated by the interaction of the cross-bridge of the myosin filaments with the actin filaments. Mechanism of muscle contraction (sliding filaments or walk along theory): Each skeletal muscle fiber is excited by one of the terminal of large nerve fiber which attach to the middle of skeletal muscle fiber at the neuromuscular junction. There is only one neuromuscular junction to each muscle fiber locates near the middle of the fiber. Muscle contraction occurs through the following sequence:
The action potential is transmitted from the nerve fiber to its nerve terminals and then across the neuromuscular junction to the surface of skeletal muscle fiber.
The T- tubules then transmit the surface action potential deep inside the muscle fiber.
This action potential in the T- tubules causes an activation of voltage sensors (DHP receptors).
Activation of DHP receptors lead to opening of Ca2+ channel (ryanodine Ca2+- channel) in the cisternae leading to rapid release of Ca2+ ions from the cisternae to the ICF of the muscle fibers.
The released Ca2+ to the ICF of the muscle fibers, then diffuse to the adjacent actin myofibrils where they bind strongly with troponin.
This Ca2+- troponin binding leads to move tropomyosin molecules away from the F-actin protein and consequently leads to exposure of the active sites (ADP). This is followed by interaction between actin protein active site and the cross-bridge of myosin (heads of myosin molecules). This interaction causes contraction to occur according to walk-along theory (or sliding filament theory) by sliding of thin filaments over the thick filaments. The sliding during muscle contraction in produced, according to walk-along theory by breaking and reforming of linkages between the cross-bridges of myosin and the actin active sites. It is postulated that when the head attached to actin, this attachment causes changes in the intermolecular forces in the head of the cross-bridge allowing the heads to be able to tilt and drags the actin filament along with it (power stroke). The energy that activates this tilt is derived from cleavage of ATP that is bind to the head by the ATPase activity of the head of the cross-bridges (ATP ADP + Pi+ E). Then, immediately
![Page 31: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/31.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 29
after tilting, the head binds with a new ATP molecule which causing the head to break away from active site and return to its normal position. In this position it combines with a new active site farther down along the actin filament, and then a similar tilt takes place again.
The width of the A-bands is constant, where as the Z lines move closer together when the muscle contracts and farther apart when it is stretched.
Muscle contraction will continue as long as the Ca2+ ions remain in high concentration in the sarcoplasmic fluid. However, a continually active Ca2+ pump located in the walls of the sarcoplasmic reticulum pumps Ca2+ ions out of the sarcoplasmic fluid back into the SR and returning the cytosolic Ca2+ concentration to normal level of about 0.1 mM. Once the Ca2+ ions concentration outside of the reticulum has been lowered sufficiently, Ca2+ ions will be released from troponin, and the chemical interaction between myosin and actin ceases and the muscle relax. It is during this Ca2+ pulse that muscle contraction occurs. If the contraction is to continue without interruption for longer intervals, a series of such pulses must be initiated by a continuous series of repetitive action potentials. If the actin filament has pulled all the way out to the end of the myosin filament with no overlap with myosin, the tension developed by the activated muscle is zero. This is because no cross-bridges involved in the contraction process. If the actin filament begins to overlap the myosin filament, the tension increases progressively as the overlap increases. This is because more cross-bridges come into action. On further overlapping, the actin filaments begin to overlap each other on the opposite side; at this point the strength of contraction starts to decrease again. This is because less number of cross-bridges involved in the contraction process. This support the idea that the greater the number of cross-bridges pulling the actin filaments, the greater the strength of contraction.
The calcium used in the excitation-contraction coupling process in skeletal muscle comes exclusively from the sarcoplasmic reticulum. This can be shown that extracellular calcium is not necessary, because skeletal muscle fibers can contract for up to 30 to 60 minutes in solutions that do not contain calcium. This contrasts with the heart or smooth muscle, which stop contracting immediately in calcium-free solutions. There appears to be a small net loss of calcium with each contraction. Thus a skeletal muscle fiber contracting longer than about 60 minutes in calcium-free medium will begin to grow weaker as the internal calcium stores are depleted.
Muscular dystrophy is a collective term for several hereditary diseases in which the skeletal muscles degenerate, lose strength, and are gradually replaced by adipose and fibrous tissue. This new connective tissue impedes blood circulation, which in turn accelerates muscle degeneration in a fatal spiral of positive feedback. The most common form of the disease is Duchenne15 muscular dystrophy (DMD), caused by a sex-linked recessive allele. Like other sex-linked traits, DMD is mainly a disease of males. The disease affects the hips first, then the legs, and progresses to the abdominal and spinal muscles. The muscles shorten as they atrophy, causing postural abnormalities such as scoliosis. DMD is incurable but is treated with exercise to slow the atrophy and with braces to reinforce the weakened hips and correct the posture. Patients are usually confined to a wheelchair by early adolescence and rarely live beyond the age of 20.
![Page 32: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/32.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 30
The source of energy for the muscle: All muscle contraction depends on ATP; no other energy source can serve in its place. The energy is needed for the following: [1] Most of the energy is required to activate the walk-along mechanism of muscle contraction (myosin ATPase). [2] Small amounts of energy are required to pump Ca2+ from the sarcoplasm into sarcoplasmic reticulum and to pump Na+ and K+ ions though muscle fiber membrane to maintain an appropriate ionic environment for the propagation of action potentials.
ATP supplies the energy required by the muscle. At rest and during light exercise, muscle fibers rely almost exclusively on the aerobic metabolism of fatty acids to generate ATP. When the muscle starts contracting, the mitochondria begin breaking down molecules of pyruvate instead of fatty acids. This is because lipids alone cannot supply energy fast enough; therefore, glucose becomes the predominant component in the muscle fuel mixture. The glucose can come either from the surrounding interstitial fluid or through the breakdown of glycogen reserves within the sarcoplasm. However, the concentration of ATP present in the muscle fiber (4 mM) is sufficient to maintain full contraction for only a few sec at most. Fortunately, after the ATP is broken into ADP, the ADP is rephosphorylated to form new ATP within a fraction of sec. Sources of the energy for the re-phosphorylation of ADP ATP (figure 4.22): During the course of exercise, different mechanisms of ATP synthesis are used depending on the exercise duration. We will view these mechanisms from the standpoint of immediate, short-term, and long-term energy, but it
Figure 4.22: Skeletal muscle sources of the energy.
![Page 33: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/33.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 31
must be stressed that muscle does not make sudden shifts from one mechanism to another like an automobile transmission shifting gears. Rather, these mechanisms blend and overlap as the exercise continues. [1] Immediate energy: In a short, intense exercise such as a 100 m dash, the energy released from cleavage of phosphocreatine is used to re-phosphorylate of ADP ATP. The cell phosphocreatine plus its ATP together can provide maximal muscle power for a period of 10-15 sec. Therefore, this energy system is used for maximal short bursts of muscle power. [2] Short-term energy: As the phosphagen system is exhausted, the muscles shift to anaerobic glycolysis to “buy time” until cardiopulmonary function can catch up with the muscle’s oxygen demand. During this period, the muscles obtain glucose from the blood and their own stored glycogen. The pathway from glycogen to lactic acid, called the glycogen–lactic acid system, produces enough ATP for 30 to 40 seconds of maximum activity. To play basketball or to run completely around a baseball diamond, for example, depends heavily on this energy-transfer system. [3] Long-Term Energy: After 40 seconds or so, the respiratory and cardiovascular systems “catch up” and deliver oxygen to the muscles fast enough for aerobic respiration to meet most of the ATP demand. The oxidative release of energy is exceedingly efficient thus allowing continued muscle activity for many hours. A disadvantage of aerobic metabolism is that it requires adequate blood circulation to deliver sufficient quantities of oxygen to the muscle cells, and to remove CO2 rapidly from those cells. When O2 supplies are insufficient, the pyruvic acid formed from glucose does not enter the citric acid cycle but reduced to lactic acid. This process of anaerobic glycolysis is more rapid than the aerobic glycolysis but associated with the net production of much smaller quantities of energy-rich phosphate bonds. Physical activity lasting over many minutes and hours cannot be supported by the limited bodily reserves of glucose and glycogen. Fatty acids from food and adipose tissue, therefore, supply most of the substrate used by muscle tissue working overtime. However, lightly loaded muscles manage to cover their energy needs for extended period of time through oxidation of circulating glucose and fatty acids.
When muscle fibers are completely depleted of ATP and phosphocreatine, they developed a state of
extreme rigidity called rigor due to continuous interaction between the cross bridge and the active sites on actin filaments. When this occurs after death, the condition is called rigor mortis. In rigor, almost all of the myosin heads attach to actin but in an abnormal, fixed, and resistant way due to complete loss of ATP required to cause separation of cross-bridge from the actin filaments during relaxation.
Muscle heat production: Due to ion pumping and cross bridge turnover, muscles produce heat as a by-product of ATP hydrolysis. This is true even in relaxed muscle, because ion pumps are working and some cross bridges are cycling. With contraction, when many cross bridges are cycling and the sarcoplasmic reticulum is vigorously pumping calcium, heat production is greatly elevated. Skeletal muscle is the most abundant tissue in the body. Thus, even at rest, skeletal muscle heat production helps maintain normal body temperature. With exercise the heat produced by the muscles increases dramatically. This can be advantageous if an individual is chilled until widespread shivering is invoked. In this case the muscles undergo uncoordinated contractions that do not lead to large-scale limb movements and thus not much mechanical work. Here, most of the energy liberated by ATP hydrolysis is converted into heat, which helps counteract any drop in body temperature. The motor unit: It is the combination of a single motor nerve cell (neuron) and all the muscle cells it innervates (figure 4.24). When an electrical impulse Figure 4.24: Motor unit
![Page 34: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/34.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 32
travel down the axon, all muscle cells attached to the motor unit contract simultaneously. In general, the large muscles that react slowly and do not require a very fine degree of control such as the gastrocnemius muscle may have several hundred muscle fibers in a motor unit is called slow motor unit. On the other hand, small muscle that react rapidly and whose control is exact have few muscle fibers (as laryngeal muscles) in each motor unit is called fast motor unit.
Types of muscle contraction: Muscle contraction is said to be isometric when the muscle does not shorten during contraction and isotonic when it shortens with a constant tension on the muscle (figure 4.25). There are several basic differences between isometric and isotonic contraction:
Isometric contraction does not require much sliding of myofibrils among each other.
Isometric contraction requires a smaller amount of energy used by the muscle.
Isometric contraction does not do work.
Isometric contraction is associated with less release heat and, therefore, isometric contraction is more energy efficient, whereas that of isotonic contraction is associated with more release of heat and, therefore, is less energy efficient.
Most contractions of the muscle in the body are actually a mixture of the two. Single muscle twitch and summation of contraction: The time delay between the application of stimulus and the beginning of muscle contraction is called the latent period. Muscle contraction can be elicited by exciting the nerve to a muscle or by passing a short electrical stimulus through the muscle it self, giving rise to a single sudden contraction lasting for a fraction of a second. This type of muscle contraction is called single muscle twitch (figure 4.26). The contractile mechanism does not have a refectory period because it depends on the availability of intracellular free Ca2+, therefore, repeated stimulation before relaxation has occurred produced additional activation of the contractile elements and a response that is added to the contraction already present. This phenomenon is known as summation of contractions (figure 4.26). The tension developed during summation is considerably greater than that during the single muscle twitch. In general, summation occurs in two different ways:
Figure 4.25: Types of muscle contraction.
![Page 35: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/35.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 33
1. By increasing the number of motor units contracting simultaneously ( pecial or multiple motor unit summation) and 2. By increasing the rapidity of contraction of individual motor units (temporal summation).
When a muscle is stimulated at progressively greater frequencies, frequency is finally reached at which the successive contraction fuse called tetanization (figure 4.26). It is a complete tetanization when there is no relaxation between stimuli. An incomplete tetanization when there are period of incomplete relaxation between the summated stimuli. During a complete tetanization, the tension developed is about four times that developed by individual twitch contractions.
Tetanus toxin, which is produced by the bacterium Clostridium tetani, can result in tetany throughout all the skeletal muscles of the body. The bacterium lives in the soil, and once it contaminates a dirty wound, the tetanus toxin is released. The toxin travels to the spinal cord where it blocks inhibitory nerves, allowing the excitatory motor neurons to fire rapidly. Rapidly firing motor neurons summate to produce tetany, a potentially fatal condition. Skeletal muscle tone: Even when muscles at rest, a certain amount of contraction usually remain. This residual degree of contraction in skeletal muscle is called muscle tone. This tonic contraction in skeletal muscles is due to nerve impulses coming from gamma motor neurons in the spinal cord. These in turn are controlled partly by impulses transmitted from the brain to the anterior motor neurons, and partly by impulses that originate in muscle spindles located in the muscle itself. In cardiac and smooth muscles, maintenance of tone is purely myogenic, i.e. the muscles themselves control the tone. The tone is not under nervous control in cardiac muscle. Muscle fatigue: Muscle fatigue is the progressive weakness and loss of contractility that results from prolonged use of the muscles. For example, if you hold a book at arm’s length for a minute, you will feel your muscles growing weaker and eventually you will be unable to hold it up. Repeatedly squeezing a rubber ball, pushing a video game button, or trying to take lecture notes from a fast-talking professor produces fatigue in the hand and finger muscles. Fatigue has multiple causes:
Figure 4.26: Single muscle twitch and summation of contraction.
![Page 36: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/36.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 34
• ATP synthesis declines as glycogen is consumed due to interruption of blood flow through a contracting muscle and the loss of nutrient supply. This will results in slow down the mechanism of muscle contraction and the sodium-potassium pumps (which are needed to maintain the resting membrane potential and excitability of the muscle fibers). • Accumulation of lactic acid lowers the pH of the sarcoplasm, which inhibits the enzymes involved in contraction, ATP synthesis, and other aspects of muscle function. • Motor nerve fibers use up their acetylcholine, which leaves them less capable of stimulating muscle fibers. This is called junctional fatigue. Muscle hypertrophy: Forceful muscular activity causes the muscle size to increase, a phenomenon called hypertrophy. Most hypertrophy results from increase in the diameter of fiber already present in the muscle, and partly due to hyperplasia (increase in the number of fiber). As the diameter of the muscle fiber increases, the sarcoplasm increases and the fiber gain in various nutrients such as glycogen, lipids, ATP, phosphocreatine, increase in the synthesis of contractile proteins and in addition, more additional mitochondria. All these will increase the motive power of muscle and maintains it for longer period of time. Hypertrophy results mainly from very forceful muscle activity even this activity is for only few minutes each day. Weak muscular activity, even when sustained over long periods of time, does not result in significant hypertrophy. On the other hand, prolonged muscle activity does increase muscle endurance due to an increase in muscle metabolism caused by an increase in the oxidative enzymes, myoglobin, and even blood capillaries. Muscle atrophy: Muscle atrophy is the reverse of muscle hypertrophy. It results from non-using muscle for prolonged period of time. It also results from muscle denervation. Skeletal muscle continuously remodels in response to its level of use. When a muscle is inactive for an extended period, the rate of synthesis of the contractile proteins in individual muscle fibers decreases, resulting in an overall reduction in muscle mass. This reversible reduction in muscle mass is called atrophy. Changes in muscle strength at the onset of contraction (the staircase effect or treppe): When a muscle begins to contract after a long period of rest, its initial strength of contraction may be as little as one-half its strength 30 to 50 muscle twitches later. That is the strength of contraction increases to a plateau, this phenomenon is called the staircase effect or treppe. It is believed to be caused primarily by electrolyte changes, an increase in the cytosolic Ca2+ concentration that occurs when a series of contraction begins. Relationship between muscle length and tension: The preload is the amount of force applied to a resting muscle before stimulation, creating passive tension. When the muscle is stimulated, active tension is added to the passive tension. The amount of active tension produced is the difference between passive tension and total tension. Active tension is considered as the real tension that is generated in the muscle during contractile process. It can be determined by the length-tension curve. The isometric tension developed in a muscle fiber on neural stimulation depends on the extent to which the muscle was stretched before stimulation. The length of the muscle at which the active tension is maximal is usually at its resting length (figure 4.27). Increase or decrease the muscle length from its resting length will leads reduction in its tension. At a sarcomere length of 2.2 μm, overlap between thick and thin filaments is optimal and force development is maximal. At lengths greater than 2.2 μm, force decreases because cross-bridge overlap is lessened. At lengths less than 2.2 μm, force is diminished because the thin filaments meet at the center of the sarcomere, causing an increased resistance to shortening. Skeletal muscles operate at the plateau of their length-tension relation because preload is set at the optimal level by bony attachments at each end of the muscle. By contrast, preload is not fixed in cardiac muscle but varies according to the amount of venous return. Preload is a key determinant of the force of cardiac muscle contraction.
![Page 37: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/37.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 35
The resting length of skeletal muscles is close to ideal, so that significant stretching decreases contraction strength. This is not true of the heart. Prior to filling with blood during diastole, the sarcomere lengths of myocardial cells are only about 1.5 μm). At this length, the actin filaments from each side overlap in the middle of the sarcomeres, and the cells can contract only weakly (figure 4.27). As the ventricles fill with blood, the myocardium stretches (increase the preload) so that the actin filaments overlap with myosin only at the edges of the A bands. This increases the number of interactions between actin and myosin, allowing more force to be developed during contraction. This phenomenon is called the Frank–Starling law. Cardiac muscle, unlike skeletal muscle, does not display a descending limb on the active tension curved because the greater stiffness of cardiac muscle normally prevents its sarcomeres from being stretched beyond 2.2 microns.
The length-tension relationship of smooth muscle is very different. If you’ll recall back to skeletal muscle, when we stretch the skeletal muscle, we get a decrease in the active tension (what the cross-bridges are doing) and an increase in passive tension (the non-contractile elements like the membrane behave like stretched rubber bands, cause passive tension). If we stretch smooth muscle, we see a small, temporary increase in passive tension, but that rapidly returns to normal. The ability of the smooth muscle cell to generate active tension remains normal over a very wide range of changes in length. Smooth muscle can do this because it has no striations and the thick and thin filaments are not lined up in the rigid way that we see in skeletal muscle. This lack of a rigid structure means that smooth muscle fiber can be stretched and there will still be some myosin head able to bind to the active site and the rest of the cross-bridge cycle continues normally, allowing for force generation. Types of muscle fibers: Depending upon contraction time and myosin ATPase activity the muscle fibers are divided into two types: 1. Type I fibers or slow fibers or slow twitch fibers, which have small diameter. 2. Type II fibers or fast fibers or fast twitch fibers, which have large diameter. Most of the skeletal muscles in human beings contain both the types of fibers. Types of muscles: Based on contraction time, the skeletal muscles are classified into two types: 1. Red muscles 2. Pale (white) muscles.
Figure 4.27: Relationship between muscle length and tension.
![Page 38: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/38.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 36
Table 4.4: Comparison between red and pale muscles.
Red (slow twitch) muscles Pale (fast twitch) muscle
Type I fibers are more Twitch contraction is long designed for sustained contraction
Type II fibers are more Twitch contraction is short designed for short contraction
More Myoglobin content, so it is red, More blood vessels, More mitochondria aerobic glycolysis for ATP production less liable to fatigue.
Less myoglobin content, so it is pale, Less blood vessels, Less mitochondria anaerobic glycolysis for ATP production more liable to fatigue.
Sarcoplasmic reticulum is less extensive Contraction is less powerful
Sarcoplasmic reticulum is more extensive Contraction is more powerful
Response is slow with long latent period Response is rapid with short latent period
Example: Back muscles and gastrocnemius muscles
Examples: Hand muscles and ocular muscles
Electromyogram (EMG): If many muscle fibers contract simultaneously, the summated electrical potentials can be recorded at the skin or from the muscle directly and this recording is called electromyogram (EMG). EMG can be recorded after a proper electrical stimulation of the muscle. EMG are frequently used clinically to diagnose abnormalities of muscle excitation including the abnormalities of the muscle it self, motor and sensory nerve conduction, and studies of neuromuscular transmission. Such of these abnormalities are: [A]- Alteration in amplitude of motor unit potential: In primary muscle diseases, the amplitude of motor unit potential will be reduced. Conversely, in chronic partial denervation of the muscle, the amplitude of motor unit potential will be increased due to collateral sprouting of the nerve terminals with reinnervation of the neighbor muscle fibers. [B]- Muscle fasciculation: is due to spontaneous motor unit contractions, which can be visible by the slight movement of the skin over the muscle. Muscle fasciculation occurs especially following destruction of anterior motor neurons or the motor nerve. As the peripheral nerve fibers die, spontaneous impulses are generated during the first few days, and fasiculatory muscle movements result in the muscle. [C]- Muscle fibrillation: is due to spontaneous activity of individual muscle fibers, which cannot be visible through the skin and can only be detected by EMG. Fibrillation is a feature of denervation, occurring 10-20 days after the interruption of the nerve supply, but it is also seen in primary muscle disease.
![Page 39: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/39.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 37
TThhee ssmmooootthh mmuusscclleess:: Smooth muscle can generally be divided into two major types, the multi-unit
and the single unit smooth muscle (figure 4.28) and (table 4.1): Single-unit smooth muscle cells can be found in the gut and blood vessels. Because these cells are linked together by gap junctions, they are able to contract as a syncytium. Single-unit smooth muscle cells contract myogenically, which can be modulated by the autonomic nervous system.
Unlike single-unit smooth muscle cells, multi-unit smooth muscle cells are non-rhythmical and found in the muscle of the eye and in the base of hair follicles. Multi-unit smooth muscle cells contract by being separately stimulated by nerves of the autonomic nervous system. As such, they allow for fine control and gradual responses, much like motor unit recruitment in skeletal muscle.
The junction between the nerve terminals and smooth muscles are either contact junction (morphologically more like skeletal muscle neuromuscular junction) as in multiunit smooth muscles or diffuse junction (figure 4.28) as in single unit smooth muscles. In these junctions, the nerve fiber of autonomic nervous system branch diffusely on top of a sheet of muscle fiber without making an actual direct contact with single unit smooth muscle fibers as in diffuse junction or making a direct contact with multi-unit smooth muscle fibers as in contact junction. The multiple branches of the nerve fibers are beaded with enlargements (called varicosities) from which neurotransmitter substance is released from the nerve fiber which is then diffused into the interstitial fluid and then to the smooth muscle fiber.
Initiation of smooth muscle contraction and relaxation: Smooth muscles can contract or relax as a consequence of the following factors:
[1]. Action potential-smooth muscle contraction: Smooth muscle action potentials arise from membrane that is autonomously active and tonically modulated by autonomic neurotransmitters. Therefore, conduction velocities and action potential shapes are labile. Depolarization of the plasma membrane opens voltage-gated Ca2+ channels. Calcium ions diffuse through the Ca2+ channels from ECF to ICF. The generation of action potential can be due to:
The rhythmicity,
Stretching the smooth muscles, or the
Generation of excitatory junctional potential (EJP) as in multiunit smooth muscles. EJP results from the interaction between neurotransmitters from autonomic nervous system and excitatory receptors at the multiunit smooth muscle membrane lead to generation of discrete partial depolarization that look like small end-plate potentials and called excitatory junctional potentials (EJPs). The action potential does not develop. This type of depolarization is called local depolarization or excitatory junctional potential (EJP). This local depolarization travels throughout the entire multiunit smooth muscle fiber and causes contraction. Local depolarization is developed because the multiunit smooth muscle fibers are too small to develop action potential. Smooth muscle relaxation can be result
Figure 4.28: Histological arrangement of multi-unit and single-unit smooth muscles
![Page 40: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/40.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 38
of the generation of inhibitory junctional potentials (IJPs) if interaction between a neurotransmitter and inhibitory receptors occurs with consequent hyperpolarization of the membrane. [2]. Non action potential-smooth muscle contraction: Smooth muscle contraction can be initiated without the generation of an action potential as a result of local tissue factors or humeral factors.
The smooth muscles of the arterioles, metarterioles, and precapillary sphincters have little or no nervous supply. Yet, the smooth muscle is highly contractile, responding rapidly to change in local condition in the surrounding interstitial fluid (local tissue factors). Some of the specific control factors are: ↓oxygen, ↓Ca++, ↓body temperature, ↑CO2, ↑[H+], ↑Lactic acid, ↑[K+], ↑adenosine & phosphate compounds, in the local tissues all cause smooth muscle relaxation and therefore vasodilatation. The mechanisms by which the local tissue factors excite or inhibit the smooth contraction not clear. It is possible that these factors cause change in the cell membrane potential, changes in the permeability of the membrane to Ca2+ ions, and/or changes in the intracellular contractile process.
Humeral factors mechanism is the result of interaction between hormones, chemical agents or any other factors (norepinephrine, epinephrine, acetylcholine, angiotensin, vasopressin, oxytocin, serotonin, and histamine) with excitatory receptors of G protein at the surface of smooth muscle fibers. Mechanism of smooth muscle excitation: Propagated action potentials (through activation of voltage-gated Ca++ channels), or chemical substances (Humeral factors through activation of G protein) can initiate smooth muscle contraction. All cause smooth muscle contraction by increase the intracellular Ca2+ concentration. Activated G protein can activate:
G protein-gated Ca channels at the smooth muscle cell membrane or
Membrane phospholipase C Release of IP3 Activates IP3-gated Ca channels at the membrane of endoplasmic reticulum (figure 4.29):
As the ICF Ca2+ concentration increases, it binds with a regulatory protein called calmodulin (instead of troponin that present in skeletal muscle). This calmodulin-Ca2+ complex activate a phosphorylating enzyme called myosin light chain kinase (MLCK), which leads to phosphorylation of myosin head. This phosphorylation of the head of the cross-bridge will bring about the interaction between the head of myosin with the actin filament and preceding the same as occurs for skeletal muscle, thus causing muscle contraction. When the Ca2+ ion concentration falls below a critical level, all aforementioned processes reverse and the presence of an enzyme myosin phosphatase is required to dephosphorylate the head of the cross-bridge and consequently disengagement of the head from the actin filament (relaxation) (figure 4.29). However, myosin dephosphorylation does not necessarily lead to immediate smooth muscle relaxation due to the presence of latch bridge mechanism by which the dephosphorylated myosin cross-bridges remain attached to actin for some time after the cytoplasmic Ca2+ ion concentration falls. This produce sustained contraction with little expenditure of energy.
![Page 41: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/41.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 39
Drugs such as nifedipine and related newer compounds are calcium channel blockers. These drugs block Ca2+ channels in the membrane of smooth muscle cells within the walls of blood vessels, causing the muscles to relax and the vessels to dilate. This effect, called vasodilation, may be helpful in treating some cases of hypertension (high blood pressure). Calcium-channel-blocking drugs are also
Figure 4.29: Mechanism of smooth muscle excitation and relaxation.
![Page 42: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/42.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 40
used when spasm of the coronary arteries (vasospasm) produces angina pectoris, which is pain caused by insufficient blood flow to the heart.
The difference between smooth, skeletal, and cardiac muscles: 1. Histological differences (figure 4.30):
Smooth muscle cells are small, no striations seen in smooth muscle cells (absence of sarcomeres).
No T-tubules.
No troponin (except cardiac muscles).
The thick and thin filaments are dispersed throughout the cell. Thin filaments (actin) are anchored into dense bodies (a Z-line equivalent) which are either anchored to the cell membrane but most of them float within the cytoplasm and hold together by intermediate filaments (figure 4.31).
The junction between the nerve terminal (somatic nerve fiber) and skeletal muscle fiber is called neuromuscular junction while those between the nerve terminals (autonomic nervous system) and smooth muscles are called contact or diffuse junction.
The neurotransmitter at the neuromuscular junction of skeletal muscle is only acetylcholine; while of smooth muscle is acetylcholine or norepinephrine. Smooth muscle is innervated by the autonomic and enteric nervous systems while skeletal muscles are innervated by somatic sensory and motor neurons.
2. Differences in muscle contraction: In smooth muscles are rhythmical tissues, the contraction time is longer, less energy is required to sustain the same tension of contraction relative to skeletal muscles, can be shorten a far greater percentage of its length compare to skeletal muscle. In addition, the maximum force of smooth muscle contraction per cm cross-sectional area is greater than the skeletal muscle contraction. However, the cross-bridge cycle in smooth muscle is considerably slower than in skeletal muscle, which allows for a longer contraction time and higher maximal force of contraction. An important characteristic of visceral smooth muscle is its ability to contract in response to stretch. 3. Differences in membrane potential:
In normal resting state, the membrane potential of smooth muscle is less negative than in skeletal muscle and some of them have no fixed value but actually have a slow wave potential. The action potentials of visceral smooth muscle occur in two different forms: (1) Spike potential as those seen in skeletal muscle and (2) Action potential with plateau. The smooth muscle cell membrane has far more voltage-gated Ca2+ channels and few voltage-gated Na+ channels than skeletal muscle fiber. Therefore, Na+ participates little in the generation of the action potential in most smooth muscle. Instead, the flow of Ca2+ ions to the interior of the fiber is mainly responsible for the action potential and the initiation of the smooth muscle contraction.
Figure 4.31: Smooth muscle and its contractile apparatus.
![Page 43: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/43.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 41
CCaarrddiiaacc mmuussccllee:: Cardiac muscle physiology can best be understood through reviewing the differences
with skeletal muscles. 1. Histological differences: Cardiac muscle is striated like skeletal muscle but otherwise differs from it in many structural and physiological ways. Cardiac myocytes (muscle cells), or cardiocytes, are relatively short, thick, branched cells. They usually have one centrally placed nucleus (but it can be more) (skeletal muscle cell is multinucleated). The sarcoplasmic reticulum (SR) lacks terminal cisternae (it has foot-like sacs associated with the T tubules). The cardiac muscles are made up of many cardiac muscle cells connected in series with each other at the intercalated discs, which are the cell membranes that separate individual cardiac muscle cell from each other. At the intercalated disc free diffusion of ions and action potential from one cardiac cell to another occurs through gap junctions. It also has especially large mitochondria, which fill about 25% of the myocyte; skeletal muscle fibers, by comparison, have much smaller mitochondria that occupy only 2% of the fiber. 2. The action potentials of the cardiac muscle fibers (atria, ventricles and Purkinje fibers) characterized by the presence of plateau, which causes the prolongation of action potential in the cardiac muscle. The myocytes contract as long as the action potential is in its plateau. The duration of cardiac action potential is much longer (calcium influx prolongs the duration of the action potential and produces a characteristic plateau phase) than in nerve or skeletal muscle fiber. In a typical nerve, the action potential duration is about 1 ms. In skeletal muscle cells, the action potential duration is approximately 2-5 ms. In contrast, the duration of cardiac action potentials range from 200 to 400 ms. In nerve and muscle cells, the depolarization phase of the action potential is caused by an opening of sodium channels. This also occurs in non-pacemaker cardiac cells (atrial and ventricular muscles). However, in cardiac pacemaker cells (sinoatrial and atrio-venticular nodes), calcium ions are involved in the initial depolarization phase of the action potential. 3. The cardiac muscle is absolutely refractory during most of the action potential (recall figure 4.7). Therefore, tetanization of the type seen in skeletal muscle cannot occur. An electrical stimulus can sometimes initiate a new spike at the very end of the action potential, i.e. at the relative refractory period. 4. The strength of cardiac contraction depends on the concentration of Ca2+ ions in the ECF that pass through T-tubules and on the Ca2+ released from endoplasmic reticulum. In contrast, the strength of skeletal muscle contraction is hardly affected by the ECF Ca2+ concentration because its contraction is caused almost entirely by Ca2+ ions released from sarcoplasmic reticulum inside the skeletal muscle fiber itself. 5. Metabolism of cardiac muscle: Cardiac muscle depends almost exclusively on aerobic respiration to make ATP. It is very rich in myoglobin (a short-term source of stored oxygen for aerobic respiration) and glycogen (stored energy). Cardiac muscle, therefore, is more vulnerable to an oxygen deficiency. Because it makes little use of anaerobic fermentation or the oxygen debt mechanism, it is not prone to fatigue.
![Page 44: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/44.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 42
Table 4.2 summarizes the main differences among the three types of muscles.
: summary of the differences among the three types of muscles 2Table 4. Skeletal muscles Cardiac muscles Smooth muscles
Microscopic appearance
Striated; Cylindrical and unbranched cells, actin and myosin arranged in sarcomeres, more than
one nucleus
Striated; branched cells, actin and myosin
arranged in sarcomeres, usually one nucleus
Not striated; Spindle-shaped, unbranched cells,
no sarcomeres, actin anchored into dense
bodies and cell membrane, only one
nucleus
Length 1 cm to 4 cm 80 μ to 100 μ 50 μ to 200 μ
Innervation Somatic nervous system (alpha motor neurons)
Autonomic nervous system
Autonomic nervous system
Level of Control
Under voluntary control,
Only neurogenic
Under involuntary Control, Myogenic in
nature
Under involuntary Control, Neurogenic and
myogenic in nature
Initiation of Contraction
Upon stimulation Spontaneous Spontaneous
Role of Nervous Stimulation
Initiates contraction Modifies contraction; can excite or inhibit
Initiates or modifies contraction;
can excite or inhibit;
Modifying Effect of Hormones
No Yes Yes
Fatigue Possible Not possible Not possible
Summation & Tetanus Possible Not possible Possible
RMP Stable Stable Unstable
For trigger of contraction, calcium binds with
Troponin Troponin Calmodulin
Contraction grade The grading depends on
the number of cells stimulated
The grading depends on the initial length of the cell before contraction
and changes in contractility
Can be graded in single-unit smooth muscle by
varying the cytosolic Ca2+
concentration
Presence of Myofibrils, Sarcomers, Troponin, T tubules
Yes Yes No
Level of Development of Sarcoplasmic Reticulum
Well developed Moderately developed Poorly developed
Source of Increased Cytosolic Ca
2+
Sarcoplasmic reticulum
From ECF and from sarcoplasmic reticulum
From ECF and from sarcoplasmic reticulum
Site of Ca2+
regulation Troponin in thin
filaments Troponin in thin
filaments Myosin in thick
filaments
Presence of Gap Junctions
No Yes Yes in single-unit smooth
muscle
Length–Tension Relationship
Yes but limited Yes No
![Page 45: Physiology of muscles and nerves - Al-Mustansiriya University10_09... · Describe rhythmicity of certain excitable tissues. ... have two essential properties: [1] ... Skeletal muscle](https://reader039.fdocuments.in/reader039/viewer/2022030815/5b2590fa7f8b9af7778b4871/html5/page/45.jpg)
Al-Mustansiriya College of Medicine/Nerve & Muscles Physiology 43