Physiology and Clinical Applications of Cardiopulmonary Exercise Testing in Lung Cancer Surgery
13
Click here to load reader
Transcript of Physiology and Clinical Applications of Cardiopulmonary Exercise Testing in Lung Cancer Surgery

Physiology and ClinicalApplications ofCardiopulmonary ExerciseTesting in Lung Cancer Surgery
Nha Voduc, MD, FRCPCKEYWORDS
� Preoperative assessment � Exercise physiology � Cardiopulmonary exercise testing� VO2 (oxygen uptake)
KEY POINTS
� Cardiopulmonary exercise testing (CPET) permits measurement of oxygen uptake (VO2), an indi-cator of overall cardiopulmonary fitness and a useful measurement in the assessment of operativerisk for lung resection patients.
� CPET should be considered for the risk stratification of potential lung resection patients with FEV1
(forced expiratory volume in first second of expiration) or diffusion capacity of carbon monoxide ofless than 80% predicted.
� Predicted postoperative peak VO2 measurements of less than 10 mL/kg/min are associated withsignificantly increased risk of mortality and morbidity after lung resection.
� CPET is not indicated or appropriate for all patients; clinicians ordering CPET should be aware ofthe contraindications and limitations of this test.
m
INTRODUCTION
Pulmonary resection is the cornerstone of mana-gement for patients with localized primary lungcancer. However, given that tobacco smoking isa common risk factor for lung cancer, chronicobstructive pulmonary disease, and cardiovas-cular disease, many patients who have lungcancer have preexisting cardiorespiratory disease.Consequently, many patients with surgicallyresectable lung cancer disease may not be oper-able. The surgeon must weigh the potential bene-fits of surgery with the risk of postoperativecomplications.
Cardiopulmonary exercise testing (CPET) hasbeen shown to be an invaluable diagnostic toolin the preoperative assessment of the patientwho has lung cancer. It can be used to measure
Division of Respirology, University of Ottawa, Ottawa HosOttawa, Ontario K1H 8L6, CanadaE-mail address: [email protected]
Thorac Surg Clin 23 (2013) 233–245http://dx.doi.org/10.1016/j.thorsurg.2013.01.0051547-4127/13/$ – see front matter � 2013 Elsevier Inc. All
disability, distinguish between cardiovascularand respiratory causes of exercise limitation, andaid in the risk stratification of potential candidatesfor pulmonary resection. Exercise is unique in thatit simultaneously places demands on both thecardiovascular and respiratory systems. This char-acteristic makes exercise testing an ideal tool forevaluating cardiovascular and respiratory func-tion. However, CPET is neither required by norapplicable to all patients who have lung cancer.This article provides an overview of cardiopulmo-nary exercise physiology, describes the nature ofCPET, and discusses the evidence supporting itsrole in the preoperative assessment of the patientwho has lung cancer. It also discusses the contra-indications and limitations to CPET, the effects ofsurgical resection on exercise physiology, andpotential alternatives to formal CPET.
pital, General campus, 501 Smyth Road, Mailbox 211,
rights reserved. thoracic.th
eclinics.co

Voduc234
BASICS OF EXERCISE PHYSIOLOGY
Under normal circumstances, our cardiovascularand respiratory systems have tremendous cap-acity to respond to the increased metabolic de-mands associated with physical activity. At rest,an individual uses only a small fraction of theirpotential cardiovascular and respiratory output.Therefore, it is not surprising that many patientswith clinically significant respiratory or cardiacdisease may not have clinically obvious findingsat rest. By increasing demands on both the cardio-vascular and respiratory systems, exercise testingrepresents a useful modality for uncovering thepresence of disease and assessing disability.Arguably, the single bestmeasurement of overall
cardiopulmonary fitness is the maximum oxygenuptake (VO2 max). This measurement is often ex-pressed asmilliliters of oxygen (uptake) perminute.Oxygen is required to meet the increased energyrequirements of exercise, and consequently thebody must increase its oxygen uptake. The pro-cess requires the coordinated function of multiplesystems. Oxygen uptake is determined by multiplefactors: respiratory function, cardiac function,oxygen-carrying capacity in the blood, distributionof blood, and extraction and use of oxygen in theperipheral tissues.Theoretically, impairment of any of these sys-
tems can impair the uptake and use of oxygen.However, in health, the relative capacity or reserveof the respiratory system is greater than thecardiovascular reserve. At the maximum exercise,the average healthy individual is limited by theircardiovascular system (oxygen transport anduse) and uses only 60% to 70% of their maximumventilatory capacity. Ventilatory limitation to exer-cise occurs only in patients with respiratorydisease or in elite athletes. Elite athletes’ cardio-vascular systems may have greater than normalcapacity, resulting in use of their entire respiratorycapacity at peak exercise.The fact that only a portion of the respiratory
capacity is used at peak exercise for most healthyindividuals has major clinical implications. First,this situation means that mild respiratory diseaseis not associated with a reduction in exercisecapacity. It also means that interventions thatreduce lung function, such as pulmonary resec-tion, do not necessary have a proportional impacton overall functional capacity.
PRINCIPLES OF CPET
CPET differs from conventional cardiac stresstesting in that it uses a pneumotachograph andgas analyzers, which enable the measurement of
key metabolic variables: ventilation, oxygen pro-duction, and carbon dioxide. These variables, inaddition to heart rate, provide the cornerstonesfor CPET. They allow CPET to simultaneouslyassess cardiovascular and respiratory responsesduring exercise. This section reviews selectedcardiopulmonary exercise measurements andprinciples that are essential for the preoperativeassessment of the patient undergoing thoracicsurgery. Those readers interested in other applica-tions of CPET or more details on the methodologyand interpretation of CPET are referred to theAmerican Thoracic Society (ATS)/American Col-lege of Chest Physicians (ACCP) guidelines forCPET and as well as an excellent textbook editedby Weisman and Zeballos.1
Key Exercise Measurements
VO2
Possibly the most important and unique feature ofCPET is that it permits direct measurement ofVO2. VO2 max refers to the highest VO2 attainableby the patient. Provided that exercise testing isconducted under consistent conditions, VO2 maxis a highly reproducible measurement.2 Duringexercise, VO2 increases with work load. VO2 maxis attained when further increases in work loadare no longer associated with any further increasesin work load (a plateau is seen on the VO2 vs workgraph). Consequently, determination of the VO2
max requires significant effort on behalf of thepatient: the patient has to continue exercising attheir maximum capacity for long enough to visu-alize this plateau. Although this goal can be accom-plished by highly motivated patients (particularlythose who exercise regularly and who are accus-tomed to experiencing significant levels of dyspneaand fatigue), many patients are not able to sustainexercise long enough to discern a clear VO2 max.For thesepatients, the termpeakVO2 is convention-ally used. Peak VO2 is the highest VO2 measuredduring theexercise test. If a patient showsevidenceof approaching cardiovascular or respiratory limita-tion, the peak VO2 obtained is likely close to thepatient’s maximum VO2.Maximum VO2 is influenced by patient size and
muscle mass used during exercise, as well asfitness; larger individuals have a higher VO2 thansmaller individuals. To help standardize VO2 forindividuals of different sizes and make it a betterreflection of relative fitness, VO2 is often reportedas VO2 per kilogram. This strategy has obviouslimitations: the VO2/kg is disproportionally low inobese individuals and disproportionally high inpatients who are underweight. Alternative esti-mates of fitness have been suggested, such as

Cardiopulmonary Exercise Testing in Lung Cancer Surgery 235
VO2/height, VO2/body mass index, or even VO2/leanbody weight. None of these alternatives have beenformally evaluated in the preoperative literature.
Heart rate and cardiovascular limitationAs work load demands increase during exercise,cardiovascular output must increase. During earlyexercise, this goal is accomplished by increasesin both heart rate and stroke volume. Strokevolume reaches a plateau early, and subsequentincreases in cardiac output are reflected by linearincreases in heart rate. For most individuals,the cardiac output is limited by heart rate. Themaximum attainable heart rate can be predictedusing the equation: 210 – (0.65 � age), althoughthere is some degree of variation between individ-uals. At the end of exercise, if a patient’s heartrate is at least 90% of their predicted maximumheart rate, it is reasonable to conclude that theirexercise capacity is limited by cardiovascularfactors.
Other signs of cardiovascular limitation includearrhythmias or decreases in systolic blood pres-sure. During exercise, systolic blood pressureincreases, reflecting increases in stroke volume.A drop in systolic blood pressure is an ominoussign and may reflect failure of the cardiac pumpor severe pulmonary vascular disease.
Patients with heart disease or conditions thatreduce oxygen transport or use (such as anemiaor deconditioning), typically show proportionallygreater heart rate increases for a given VO2
(increased HR/VO2 slope).
Ventilation and ventilatory limitationAnother of the unique measurements obtainedduring CPET is minute ventilation. Ventilation mustincrease during exercise, to meet the increasedmetabolic need for oxygen and to eliminate carbondioxide. In health, themain stimulus for ventilation iscarbon dioxide production. Increases in ventilationare accomplished by increases in both tidal volumeand respiratory rate. Similar to stroke volume, theincrease in tidal volume reaches a plateau earlyduring exercise, after which further increases inventilation are reflected by increases in respiratoryrate. The peak tidal volume attained during exerciseis influenced by lung mechanics and respiratorymuscle strength. It is approximately 60% of theresting vital capacity.
Maximum ventilatory capacity during exercisecan be estimated using a variety of predictiveequations. Exercise is limited by ventilatory factorsif peak ventilation attained during exercise is atleast 85% of the predicted maximum ventilation.The reliability of predictive equations for maximumventilation is variable, depending on the equation
used and patient population. Flow volume loopassessments can also be obtained during exercisetesting and may potentially offer a more reliablemethod of identifying ventilatory limitation. Theinterested reader is referred to the ATS/ACCPguidelines for CPET2 for an overview of alternativemethods of assessing ventilatory limitation.
Lung disease may have 2 potential effects onventilatory responses during exercise. Alterationsin lung mechanics seen in either obstructive orrestrictive lung diseases lead to reductions in themaximum ventilatory capacity. If severe enough,these reductions result in early exercise limitation.Furthermore, lung disease may also be associatedwith increased physiologic dead space, whichmust be compensated for by increases in ventila-tion. This situation is reflected by an increasedventilation/VO2 slope during exercise.
Anaerobic thresholdAs exercise intensity increases, aerobic mecha-nisms for energy production are not adequateand anaerobic mechanisms must be recruited tomeet metabolic energy demands. The disadvan-tage to anaerobic energy pathways is the produc-tion of lactic acid, which is metabolized to CO2 andwater. The CO2 produced by anaerobic mecha-nisms stimulates increased ventilation. The termanaerobic threshold (AT) refers to the point atwhich there is a rapid increase in arterial lactatelevels. Although it is possible to directly measurelactate levels by blood tests performed duringexercise, this is not typically measured in clinicalsettings. The AT is most often estimated to occurwhen there is a change in the VO2/VCO2 slopeduring exercise (V-slope method).
The AT is expressed as a percentage of the pre-dicted maximum VO2, and typically occurs at 40%to 70% of the predicted maximum VO2. Work loadslower than the AT can be sustained indefinitely(provided there are adequate energy stores),whereas work loads greater than AT cannot besustained.
Any condition that could impair oxygen trans-port or use could potentially affect the AT.Common causes of a reduced AT include decon-ditioning and cardiovascular disease. Anemia or,rarely, mitochrondrial myopathies may also beassociated with reductions in AT. AT is anappealing measurement because it reflects overallcardiovascular fitness and its determination doesnot require a maximal effort from the patient.However, it does have limitations: a clear AT maynot be discernable from the exercise data for allpatients. Furthermore, patients with severe respi-ratory disease may be limited by respiratoryfactors before attaining an AT.

Box 1Indications for exercise termination
Chest pain suggestive of ischemia
Ischemic EKG changes
Complex ectopy
Second-degree or third-degree heart block
Decrease in systolic pressure by more than20 mm Hg from highest value during test
Hypertension (>250 mm Hg systolic and >120mm Hg diastolic)
Severe desaturation (<80%)
Sudden pallor
Loss of coordination
Mental confusion
Dizziness or presyncope
Signs of respiratory failure
Data from American Thoracic Society, AmericanCollege of Chest Physicians. ATS/ACCP Statement oncardiopulmonary exercise testing. Am J Respir CritCare Med 2003;167:211–77.
Voduc236
Exercise Methodology
To conduct CPET, an exercise machine is used toprovide a standardized resistance. The 2 mostwidely used exercise devices for this purpose area treadmill and cycle ergometer. Although bothmodalities have their proponents, one is notnecessary superior to the other for all patients,and it is important to be aware of their relativestrengths and weaknesses.Treadmill testing is advantageous because it
usesmotions that are familiar to almost all patients:walking/running. Because the work load on tread-mill exercise is shared amongmore muscle groupsthan cycling, patients are able to achieve a 10%higher VO2 and are less likely to terminate treadmillexercise because of quadriceps fatigue.3,4 Onoccasion, it may be advantageous for the patientto achieve a higher VO2 to detect certain physio-logic abnormalities (eg, ischemic heart disease).Given the ubiquitous nature of cardiac stresstesting, which primarily uses treadmill exercise,most hospitals already have a treadmill available.The disadvantages to treadmills include no directmeasurement of work load, increased motion arti-fact, and (theoretically) reduced safety. For tre-admill testing, a work load is established byadjusting the treadmill speed and incline. However,for a given speed, there can be significant varia-tions in the work load placed on the patient, de-pending on gait and length of stride. Whenpatients are running on a treadmill, there is greaterbody motion, which can potentially affect thequality of electrocardiographic (EKG) tracings andmake the measurement of blood pressure morechallenging (this can be offset by the use of auto-mated blood pressure cuffs). Treadmill exercisedoes place greater demands on patients’ coordi-nation and balance than a stationary cycle ergom-eter. This situation may be problematic for moreelderly and frail patients.Cycle ergometry is advantageous because it
provides a more stable platform for exercise thantreadmill testing. Because patients exercise ina seated position on a stationary cycle, there isgenerally less motion artifact and fewer demandson the coordination of the patient. Furthermore,because the patient’s weight is supported, cycleergometry can be used to measure exerciseperformance in patients whose exercise capacityis too low to permit ambulation. Cycle exercisefor CPET is typically performed on an electronicallybraked cycle ergometer, which allows the workload to be directly set by the laboratory personnel.The software in the cycle ergometer varies theresistance based on the cycling speed, to maintaina specified work load. The disadvantage to cycle
ergometry is that the motion may not be as familiaras walking for some patients.Regardless of which exercise modality is used, it
is important for the clinician to be aware that peakVO2measured on cycle ergometry is typically lowerthan the peak VO2 measured during treadmilltesting. Although normal ranges for exercise para-meters such as VO2 and VE have been establishedspecifically for cycle ergometry, this discrepancymakes it difficult to compare results for cycle ergo-metry with treadmill testing for a given patient.Most studies evaluating CPET in preoperative riskassessment used cycle ergometry.Most clinical CPETs should be symptom limited
to record the highest attainable results for meta-bolic measurements. This criterion means thatduring the test, the patient is given standardizedverbal encouragement to exercise as long aspossible. The test is usually terminated onlywhen the patient cannot exercise further becauseof intolerable symptoms (usually leg fatigue ordyspnea). On occasion, CPET may be stoppedby the laboratory personnel before the develop-ment of symptom limitation because of safetyconcerns. Indications to stop CPET include signif-icant ventricular arrhythmias, severe hypertension,hypotension, reduced consciousness, inability tofollow commands, and profound oxygen desatu-ration (Box 1). This situation emphasizes theneed for clinical CPET to be conducted by

Cardiopulmonary Exercise Testing in Lung Cancer Surgery 237
appropriately trained medical personnel who arecapable of recognizing the need for early termina-tion of the test.
A variety of exercise protocols have been estab-lished for CPET. These protocols vary in rate ofincrease in work load (or increase in speed andincline in treadmill protocols) and how much timeis spent at a given work load (duration of eachstage). The choice of protocol should be dictatedby the patient population and clinical circum-stances. For most clinical CPETs, there is noneed to compare CPET results between differentpatients, and consequently a protocol is chosenby the laboratory personnel before the exercisetest, based on estimations of the patient’s exercisecapacity. Ideally, the duration of exercise shouldbe 8 to 12 minutes.2,5 Tests that are shorter than8 minutes may not provide enough exercise data(although this might be unavoidable in patientswith severe cardiac or respiratory disease). Incontrast, tests that are too long may result inpatients terminating exercise because of musclefatigue, before cardiovascular or pulmonary limitscan be reached.
In cycle ergometry, most clinical CPETs are con-ducted using a simple incremental program: thework load is increased by 5 to 20 W, every 1 or 2minutes. Given that most patients with lung resec-tion undergoing exercise testing have comorbid-ities, a work load increase of 10 W/min (or 20 Wincreases at 2-minute intervals) has been typicallyused in the preoperative literature. A 2-minutewarm-up period with pedaling at a low resistance(20 W) may be used.
CPET IN PREOPERATIVE ASSESSMENTRelationship Between Exercise Parametersand Operative Risk
Numerous studies have established a link betweencardiopulmonary fitness, asmeasured by peak VO2
and poor surgical outcomes. The first study toshow this relationship for patients with pulmonaryresection was published by Eugene in SurgeryForum in 1982.6 This study reported that a lowpeak VO2 was associated with increased post-operative mortality in patients with pulmonaryresection. The investigators retrospectively re-viewed preoperative peak VO2 measurements in19 patients who went on to undergo pneumonec-tomy. These investigators found that that a peakVO2 of less than 1 L/min was associated with100% mortality, whereas no mortality was identi-fied in patients who achieved a peak VO2 of morethan 1 L/min. Furthermore, the investigators alsodid not identify a relationship between preopera-tive FEV1 (forced expiratory volume [FEV] in first
second of expiration) and surgical outcome. De-spite the small sample size and retrospectivenature of this study, its results did provoke signifi-cant interest in the role of CPET for the evaluationof patients undergoing thoracic surgery.
In 1984, Smith and colleagues7 reported that VO2
was also able to predict the likelihood of postoper-ative complications. These investigators evaluated22 patients undergoing lung resection surgery.In contrast to the Eugene study, Smith andcolleagues did standardize VO2 for patient size.They found that a VO2/kg of less than 15 mL/kg/min was associated with a 100% complicationrate whereas a VO2/kg of more than 20 was associ-ated with only a 10% complication rate. Bechardand Wetstein8 reported similar results when theycompared pulmonary function and exerciseparameters in 50 patients undergoing lung surgerywho did and did not experience postoperativecomplications. These investigators found no differ-ence in mean FEV1 between the 2 groups butsignificant differences in exercise performance.The group who developed complications hada significantly lower peak VO2 than the group whodid not. There were no complications in patientswith a peak VO2/kg greater than 20 mL/kg/min,whereas patients with a peak VO2/kg of less than10 had a 71% complication rate. In addition, theonly deaths in their study occurred in patientswith a peak VO2 of less than 10 (mortality was29% for patients with a peak VO2/kg <10).
Not all studies have reported an associationbetween exercise performance and risk of opera-tive complications. However, a meta-analysis of14 studies performed by Benzo and colleagues9
reported differences in peak VO2 (as well as peakVO2/kg) in patients with lung resection who didand did not develop postoperative complications.
Although peak VO2/kg is a good reflection ofexercise capacity, it is also dependent on ageand is affected by obesity. It is possible that usingpeak VO2/kg as the only measure of operabilitymay unfairly bias the assessment against older orobese individuals. Bolliger and colleagues10 evalu-ated the % predicted peak VO2 as an alternativemeasure. They compared the receiver-operatorcurves for VO2/kg and percent predicted VO2
against complication rates. Because the patient’sresults are compared against a predicted refer-ence based on their age, age was excluded asa factor. Similarly, the results are not directlyaffected by the patient’s weight. Bolliger andcolleagues found that the area under the curve(AUC) for % predicted VO2 was slightly greaterthan the AUC for VO2/kg. A peak VO2 greater than75% predicted was associated with only a 10%complication rate. One limitation to this approach

Voduc238
is that most patients for whom exercise testingis conducted have a peak VO2 that is less than75% of predicted. Despite evaluating a relativelyhealthy patient population (mean FEV1 anddiffusion capacity of carbon monoxide [DLCO]were >80% for the study group), only 49% of theirpatients attained a peak VO2 of more than 75% ofpredicted.One of the key studies to establish the role of
CPET in the preoperative evaluation of the high-risk patient undergoing thoracic surgery waspublished by Morice and colleagues.11 Theseinvestigators prospectively performed CPET in 37high-risk patients. These patients were all deemedhigh-risk because of preexisting respiratory impair-ment, at least by traditional standards. To beincluded in the study, all patients had to have either:FEV1 less than 40%, a predicted postoperativeFEV1 of less than 33% or a respiratory acidosis(PCO2 [partial pressure of carbon dioxide] >43).Eight of 37 patients showed a peak VO2 of greaterthan 15 mL/kg/min, despite their baseline respira-tory impairment. Those patients were offeredsurgery (lobectomy or segmentectomy) and hada 0% postoperative mortality. This study showedthat CPET was able to identify a subset of high-risk patientswho could still undergo surgical resec-tion safely.AT has also been evaluated as a predictor of
postoperative complications, and may furtherrefine the predictive results obtained by peakVO2/kg measurements. Torchio and colleagues12
found that among patients with a peak VO2/kg ofless than 20 mL/kg/min, no patients with an ATof more than 14.5 mL/kg/min experienced severecomplications, whereas 92% of patients with anAT less than 14.5 mL/kg/min experienced severecomplications. The main limitation of using AT isthat it may not be identifiable in all patients. Be-chard and Wetstein8 previously recognized anassociation between AT and postoperativecomplications but did not focus on AT, becausethey found that it could be identified in only 58%of their patients.There has been little study on the association
between ventilatory limitation during exercisetesting and risk of operative complications. Dalesand colleagues13 in a retrospective analysis foundthat a ventilatory reserve of less than 25 L at peakexercise was associated with an increased risk ofrespiratory complications, but this has not beenvalidated in a prospective study.
Preoperative Assessment Algorithms
Traditionally, CPET was used a last resort test inthe preoperative evaluation of the patient with
lung resection. CPET was performed only onhigh-risk patients, with the goal of identifying thesubset of patients who could still undergo surgerywith a low risk of complications. CPET was notused unless patients had already undergonepulmonary function testing (PFT) and quantitativeperfusion scanning and if their postoperative pre-dicted (ppo) FEV1 or DLCOwas less than 40%.14,15
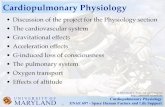
Over the last decade, this approach has beenchallenged. Wyser and Bolliger16 evaluated theusefulness of an algorithm that used CPET beforenuclear perfusion scanning. When they comparedtheir algorithm with the traditional approach, theyfound that both approaches excluded a compa-rable number of patients, but the algorithm usingCPET immediately after PFTs and before nuclearscanning was associated with a lower complica-tion rate. Because of these results, recent guide-lines have adopted this algorithm.17 The 2009European Respiratory Society (ERS)/EuropeanSociety of Thoracic Surgeons guidelines forradical therapy in lung cancer, suggested thefollowing approach for the respiratory evaluationof potential patients for lung resection (Fig. 1):
1. Measurement of FEV1 and DLCO. If both aregreater than 80%, may proceed to surgery.
2. If either FEV1 or DLCO is less than 80%, CPETshould be performed. If the peak VO2 is greaterthan 75% of predicted or VO2/kg is greater than20 mL/kg/min, then may proceed to surgery.
3. If peak VO2 less than 35% of predicted orVO2/kg is less than 10, surgical resection isnot recommended.
4. If the VO2 or VO2/kg are between theses ranges,then ppo values for FEV1, DLCO, and peak VO2
should be calculated. Surgical resection thatleaves a ppo FEV1 and ppo DLCO both greaterthan 30% and a ppo VO2 greater than 10mL/kg/min may proceed.
Safety and Clinical Limitations of CPET
Clinicians ordering CPET must be familiar with thepotential complications and contraindications toCPET. Exercise testing is generally safe, withsevere complication rates of less than 1:10 00010.Absolute contraindications to CPET include severeor uncontrolled cardiac disease (cardiomyopathy,unstable angina, and arrhythmias), uncontrolledasthma, significant infection or metabolic derange-ment, or an uncooperative patient (Box 2). Conse-quently, CPET should not be ordered beforea clinical assessment.CPET can diagnose cardiac disease, but CPET
may be less sensitive and specific than other formsof cardiac stress testing. The diagnosis of ischemicheart disease with CPET (as with conventional

Fig. 1. ERS/ESTS preoperative assess-ment algorithm. (From Bolliger CT,Perruchoud AP. Functional evaluationof the lung resection candidate. EurRespir J 1998;11:206; with permissionfrom the European RespiratorySociety.)
Cardiopulmonary Exercise Testing in Lung Cancer Surgery 239
cardiac stress testing) is based on the presence ofST depressions on EKG tracings. Gianrossi andcolleagues18 published a meta-analysis of 147studies comparing exercise-inducedST abnormal-ities with coronary angiography. They founda substantial variation in the published literature,but the overall sensitivity and specificity of STchanges for significant coronary artery diseasewas 68% and 77%, respectively. CPET can detectother abnormalities associated with cardiacdisease, such as an increased heart rate to VO2
slope and a reduced AT. However, these CPETmeasurements are not specific to cardiac disease:they can be affected by other conditions thatreduce oxygen delivery or use, such as decondi-tioning or anemia. Consequently, if the clinicalpreoperative evaluation suggests a high likelihoodof cardiac disease, the patient should be sent formore specific testing, such as a dobutamine echo-cardiogram, in addition to PFT and CPET.
Not all patients undergoing thoracotomy arecapable or willing to perform preoperative exercisetesting, but this factor itself may be a harbinger of
increased risk. Epstein and colleagues19 prospec-tively evaluated 74 thoracotomy cases at theircenter. Nineteen percent were unable to undergoCPET. These patients had similar resting pulmo-nary function compared with most who underwentCPET, but scored higher on the cardiac risk index(described later). They had significantly morecomplications and significantly higher mortality.
ALTERNATIVES TO CPET FOR PREOPERATIVEEVALUATION
Compared with other forms of exercise testing,CPET is the most resource intensive, and con-sequently, CPET is not available in all centers per-forming lung resection. Other forms of exercisetesting havebeen used for preoperative evaluation.
Stair Climbing
Stair climbing has been used for preoperativeassessment for decades. For this test, the patientis asked to climb as many flights of stairs aspossible. The test is self-paced: there is no

Box 2Absolute and relative contraindications for CPET
Absolute:
Myocardial infarction within previous 3 to 5 days
Unstable angina
Uncontrolled arrhythmias, causing symptoms or hemodynamic instability
Syncope
Active endocarditis, myocarditis, or pericarditis
Symptomatic aortic stenosis
Uncontrolled heart failure or pulmonary edema
Acute pulmonary embolus or pulmonary infarction
Thrombosis of lower extremities
Suspected dissecting aneurysm
Uncontrolled asthma
Respiratory failure
Acute noncardiopulmonary disorder, which may affect exercise performance or be aggravated byexercise
Room air oxygen saturation less than 85% at rest
NB: although CPETcan be performedwith supplemental oxygen in these cases, reliable measurementof VO2 is not possible with supplemental oxygen use
Relative:
Left main coronary stenosis or equivalent
Moderate stenotic valvular disease
Severe untreated systemic hypertension (>200 mm Hg systolic, >120 mm Hg diastolic)
Tachyarrhythmias or bradyarrhythmias
High-degree atrioventricular block
Hypertrophic cardiomyopathy
Significant pulmonary hypertension
Advanced or complicated pregnancy
Electrolyte abnormalities
Orthopedic impairment that compromises exercise performance
Data from American Thoracic Society, American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonaryexercise testing. Am J Respir Crit Care Med 2003;167:211–77.
Voduc240
required speed or time limitation. The primarymeasurement is number of flights of stairs cli-mbed. In 1968, Van Nostrand and colleagues20
published a chart review of patients undergoingpneumonectomy and found that inability to climb2 flights of stairs without severe dyspnea wasassociated with a 50%mortality after pneumonec-tomy. Although this study is widely cited, amongthe 91 patients with stair climbing data, only 4were unable to climb 2 or less flights of stairswith severe dyspnea.
Stair climbing is appealing because of itssimplicity, but it is difficult to standardize, forboth the patient and the health facility conductingthe test. There are no well-accepted standards fordetails such as climbing pace, use of railing forsupport, height of each step, or numbers of stairsin each flight. There are no established normalranges for stair-climbing distance. Furthermore,stair climbing provides no direct physiologic infor-mation. Pollock and colleagues21 did report anapproximate correlation between number of stairs

Cardiopulmonary Exercise Testing in Lung Cancer Surgery 241
climbed and peak VO2 measured via cycle ergom-eter but did not specifically assess for a relation-ship between stair-climb results and operativeoutcomes. Brunelli and colleagues22 have pub-lished several studies on stair climbing in patientsundergoing thoracic surgery. Brunelli and Salati23
evaluated prospectively 160 patients and foundthat altitude attained on stair climbing was a supe-rior predictor of postoperative complications thaneither resting FEV1 or predicted postoperativeFEV1. Only 6.5% of patients able to climb 14 mof stairs developed postoperative complications,whereas 50% of patients who climbed 12 m orless developed complications. This study did notdirectly compare stair climbing with formal CPET.Because of the low cost and simplicity of stairclimbing, Brunelli and Salati have suggested stairclimbing be used before CPET during preoperativeevaluation. In their algorithm, patients who wereable to climb 22 m (or climb at least 12 m andhad ppo FEV1 and ppo DLCO >40%) couldproceed to operation without need for CPET.CPET would be used only for patients who wereunable to climb 22 m and had a ppo FEV1 or ppoDLCO of less than 40%. Although this approachis appealing, its usefulness requires validation.
Six-Minute Walk Test
The conduct of the 6-minute walk test (6MWT) isreflected in its name: the patient is asked to walkas far as possible over a period of 6 minutes. Theprimary outcome of interest is distance walked.The concept and usefulness of a timed walkingtest were originally validated by Cooper24 withthe 12-minute walk test; however, Butland andcolleagues25 subsequently reported close correla-tion between results from a 6MWT and a 12-minutewalk test. They also reported slightly less variancein the results of the 6MWT on repeated testing.Consequently, the 6MWT has largely replaced itslonger counterpart. Similar to stair climbing, the6MWT does not provide direct physiologic infor-mation, although the distance walked duringa 6MWT has been shown to correlate with qualityof life measures as well as aerobic capacity (VO2)in patients with lung disease.26,27 Furthermore,standardized protocols have been published toimprove the reproducibility of 6MWT.28
The 6MWT can be used to assess responses totherapy (particularly pulmonary rehabilitation) andis validated as a prognostic indicator for chroniclung disease. Holden and colleagues29 found a sig-nificant difference in preoperative 6MWT distancebetween patients who died within 90 days ofsurgery compared with those who survived. How-ever, data for 6MWT in preoperative patients are
limited and inconsistent. Consequently, it is notrecommended for preoperative assessment.17,30
Risk Indices
Some investigators have suggested the use ofscoring systems for assessing the risk of postoper-ative complications. One of the first to be specifi-cally developed for patients with lung resectionand possibly the most widely cited was publishedby Epstein and colleagues.31 They combined thecardiac risk index developed by Goldman withadditional respiratory factors to create the cardio-pulmonary risk index (CPRI). Patients receiveda CPRI score of 1 to 10, based on the sum of theircardiac risk index score (1–4; 1 for a Goldmanscore of 0–5, 2 for 6–12, 3 for 12–25, and 4for >25) and pulmonary risk index score (1 pointeach for the presence of obesity, smoking within8 weeks of surgery, productive cough within5 days of surgery, diffuse wheezing within 5 daysof surgery, FEV1/FVC (forced vital capacity) <0.7,and PaCO2 [partial pressure of carbon dioxide, arte-rial] >45 mm Hg). These investigators found thatpatientswith aCPRI of 4 or greater weremore likelyto experience postoperative complications (posi-tive predictive value of 79% and negative predic-tive value of 86%). In addition, when CPRI scoreand peak VO2 were evaluated in a multiple regres-sion model, peak VO2 did not add any additionalpredictive value for postoperative complications.The limitations to using the CPRI are its relativecomplexity as well as reliance on some subjectivefactors. A subsequent study by Ferguson con-firmed a difference in mean CPRI scores forpatients who did and did not experience postoper-ative complications but found that the differencewas small (less than half a point on the 10-pointCPRI scale).32
More recently, Falcoz and colleagues33 deriveda scoring system designed to predict in-hospitalmortality for thoracic surgery. Their system (Thor-acoscore) was based on the outcomes of 15,183patients from 59 French hospitals between 2002and 2005. These investigators found that thefollowing factors were associated with anincreased risk of mortality: age, sex, AmericanSociety of Anesthesiologists score, performancestatus, dyspnea score, priority of surgery (urgentor not), procedure (pneumonectomy or other),diagnosis (benign or malignant), and number ofcomorbidities score (0, 1–2, or 31). The Thoraco-score has been validated in other hospitalsettings.34 As with Epstein’s CPRI, the limitationsof the Thoracoscore are its complexity and useof potentially subjective factors (eg, priority ofsurgery, number of comorbidities). However, it is

Voduc242
appealing, because it can provide an estimation ofmortality risk.
POSTOPERATIVE OUTCOMES
Although CPET is not routinely used after lungresection surgery, a few studies have used CPETin the postoperative period to assess the effectof surgery on exercise capacity. Brunelli andcolleagues35 performed CPETs on patients under-going lobectomy and pneumonectomy at dis-charge and 1 month and 3 months afterresection. Lobectomy was associated with a 12%reduction in peak VO2 at discharge, but thisimproved to 3% at 3 months (not statisticallydifferent from preoperative exercise capacity).Pneumonectomy was associated with an 18%reduction in peak VO2 at time of discharge. Threemonths later, patients who underwent a pneumo-nectomy still had a peak VO2 that was 11% lowerthan their preoperative measurements. Althoughstatistically significant, the reduction in peak VO2
is smaller than reductions in lung function afterpneumonectomy (at 3 months after pneumonec-tomy, FEV1 andDLCOwasstill 34%and20% lowerthan preoperative values).Bolliger and colleagues36 compared postope-
rative VO2/kg with predictions of postoperativeVO2/kg calculated using the same methodologyas ppo FEV1: ppo VO2/kg 5 preoperative VO2 �(1 – number of segments to be resected/19). Theseinvestigators found that calculations of ppo VO2/kgsignificantly overestimated the degree of exercisecapacity loss after an operation. At 6 months aftersurgery, the loss in exercise capacity was onlyabout half the loss predicted by equation. Thisfinding is not surprising, because the relationshipbetween VO2 loss and lung function loss is notlinear. Although Bolliger and colleagues did notfind that ppo VO2/kg accurately predicted postop-erative exercise capacity, they did find that it wasthe best predictor for both postoperative morbidityand mortality. Mortality in patients with a ppo VO2
of less than 10mL/kg/min (3 of 25 patients studied)was 100%.Although preoperative peak VO2/kg measure-
ments can help predict likelihood of complicationsin the postoperative period, its value in the predic-tion of long-term outcomes or postoperativedisability has not been well established. Beccariaand colleagues37 reviewed the outcomes of 62patients with lung cancer resection. Sevenpatients had a ppo FEV1 of less than 40% butunderwent surgical resection because their peakVO2/kg was greater than 10 mL/kg/min. Of these7 patients, 2 became oxygen-dependent andexperienced marked limitation of daily living.
CONTROVERSIES AND LIMITATIONS OF THEEXISTING RESEARCH
Although a preponderance of data and expertopinion support a role for CPET in the evaluationof the preoperative patient, there are limitationsto the existing literature and controversies withthis approach.
Lack of Focus on High-Risk Patients
Most of the exercise literature does not focusspecifically on the higher-risk patient. Currentpractice recommendations suggest CPET beused only on higher-risk patients (who are believedto be at increased risk for poor outcomes becauseof low ppo lung function). Most studies performedCPET on all patients undergoing resection, regard-less of their preoperative risk. Only a few studiesfocused exclusively on high-risk patients.11,16
Although this oversight is understandable forstudies published before the role of CPET in preop-erative evaluation became well established, moremodern studies still remain too inclusive in theirstudy population.
Extent of Surgical Resection
Much of the existing literature does not take intoaccount the extent of surgical resection. Forexample, the original article by Eugene6 as well asthemore recent studybyWyser16 includedpatientsundergoing segmentectomy, single lobectomy, bi-lobectomy, and pneumonectomy. The physiologicimpact and risk from a segmentectomy would beexpected to be less than a pneumonectomy, andso it would intuitively be expected to use differentpeak VO2/kg thresholds, depending on the extentof surgery. These thresholds remain to be estab-lished. The use of a ppo VO2/kg greater than 10,as suggested by Bolliger and colleagues,10 mayrepresent the best method of taking into accountthe extent of surgical resection, but this requiresconfirmation.
Long-Term Outcomes
It remains to be proved whether preoperative exer-cise performance has any influence on long-termclinical outcomes. Most of the literature hasfocused on clinical outcomes within 30 days ofsurgery. Long-term outcomes are more likely tobe dependent on factors other than cardiopulmo-nary physiology. Therefore, it may be unrealistic toexpect pre-VO2 (or any other exercise finding) tohave any major predictive value in long-termoutcomes.

Cardiopulmonary Exercise Testing in Lung Cancer Surgery 243
Clinical Relevance of PostoperativeComplications
There has been an attempt by many investigatorsto use a consistent definition for postoperativecomplications. The original study establishinga link between peak VO2/kg and complications bySmith7 focused on cardiopulmonary complica-tions: PaCO2 greater than 45 mm Hg, greater than48 hours’ mechanical ventilation, myocardialinfarction, arrhythmias, pneumonia, lobar ate-lectasis, pulmonary embolus, and death. Manysubsequent investigators have used similar defini-tions for postoperative complications in theirstudies.10–12 Studies that have included a broaderrange of complications such as excessive bloodloss or wound infection have not identified a rela-tionship between complications and exerciseperformance.38
The clinical significance of these cardiopulmo-nary complications is highly variable. For example,postoperative atelectasis may have no adverselong-term sequelae, even if bronchoscopy is re-quired in the postoperative period. Most of thecomplications are likely preferable to unresectedlung cancer, provided that the patient is not leftwith major permanent disability. Consequently,some investigators have argued that it would beincorrect to exclude patients solely because ofan increased risk of complications.39
Consequences of Not Operating
Much of the existing literature focuses on theoutcomes of patients who undergo surgery,without the context of clinical outcomes for early-stage cancer that is left unresected. Consequently,it is difficult to establish whatmortality or complica-tion rate should be prohibitive for surgery. Althougha patient with moderate chronic obstructivepulmonary disease may be at increased risk forpostoperative complications and even mortality, itis difficult to know at what point these risksoutweigh the potential benefits of cancer resec-tion. A recent study by Loewen and colleagues40
showed the value and limitations of CPET inpatients undergoing surgery for lung cancer. Theyused an algorithm similar to that suggested byWyser and colleagues. Patients with a ppo FEV1
less than 33% or greater than 900 mL underwentCPET. If their peak VO2/kg was at least 15, thepatient was offered surgery. If the peak VO2/kgwas less than 15, patients were categorized asvery high risk. These patients could still undergosurgery depending on the discretion of the thoracicsurgeon (the use of additional testing such asDLCO or perfusion scanning was not described).Of the 403 patients with adequate data, 86 were
categorized as very high risk (ppo FEV1 <33% or<900 mL and peak VO2 <15). Of these patients,68 underwent some form of thoracotomy. Althoughthe study did confirm that peak VO2 was a predictorof both postoperative complications and pooroutcome (death or respiratory failure), the mortalityin the subset of the very-high-risk patient groupwas only 4% (3 of 68). Although the selection ofpatients for surgery was not randomized (thusleaving the outcomes vulnerable to confoundingby other patient factors), the investigators didnote that the 5-year survival of the 68 high-riskpatients who underwent surgery was superior tothat of patients who did not undergo resection.This study shows the importance of not basingoperative decisions solely on a fixed thresholdvalue for peak VO2. The threshold for operating isa moving target; it is influenced by improvementsin surgical technique and postoperative care aswell as the development and refinement of effec-tive nonsurgical treatment of early-stage lungcancer (eg, radical radiotherapy).
SUMMARY
CPET is a valuable tool in the preoperative assess-ment of the patient who has lung cancer. It canidentify patients at increased risk for mortality aswell as postoperative complications. However, itis neither required nor appropriate for all patients.It should not be a substitute for a careful clinicalassessment. The results obtained from cardiopul-monary exercise should be used to aid, notreplace, clinical judgment. As with any other diag-nostic test in medicine, its value is dependent onthe ability of the clinician to use it judiciously.
REFERENCES
1. Weisman IM, Zeballos RJ. Clinical exercise testing.
Progress in Respiratory Research, vol. 32. Basel
(Switzerland): Karger; 2002.
2. American Thoracic Society, American College of
Chest Physicians. ATS/ACCP statement on cardio-
pulmonary exercise testing. Am J Respir Crit Care
Med 2003;167:211–77.
3. Miyamura M, Honda Y. Oxygen intake and cardiac
output during maximal treadmill and bicycle exer-
cise. J Appl Physiol 1972;32(2):185–8.
4. Hermansen L, Saltin B. Oxygen uptake during
maximal treadmill and bicycle exercise. J Appl
Physiol 1969;26(1):31–7.
5. Balady GJ, Arena R, Sietsema K, et al. Clinician’s
guide to cardiopulmonary exercise testing in adults:
a scientific statement from the American Heart Asso-
ciation. Circulation 2010;122(2):191–225.

Voduc244
6. Eugene J, Brown SE, Light RW, et al. Maximum
oxygen consumption: a physiologic guide to pulmo-
nary resection. Surg Forum 1982;33:260–2.
7. Smith TP, Kinasewitz GT, Tucker WY, et al. Exercise
capacity asapredictorofpost-thoracotomymorbidity.
Am Rev Respir Dis 1984;129(5):730–4.
8. Bechard D, Wetstein L. Assessment of exercise
oxygen consumption as preoperative criterion for
lung resection. Ann Thorac Surg 1987;44(4):344–9.
9. Benzo R, Kelley GA, Recchi L, et al. Complications
of lung resection and exercise capacity: a meta-
analysis. Respir Med 2007;101(8):1790–7.
10. Bolliger CT, Jordan P, Soler M, et al. Exercise
capacity as a predictor of postoperative complica-
tions in lung resection candidates. Am J Respir
Crit Care Med 1995;151(5):1472–80.
11. Morice RC, Peters EJ, Ryan MB, et al. Exercise
testing in the evaluation of patients at high risk for
complications from lung resection. Chest 1992;
101(2):356–61.
12. Torchio R, Gulotta C, Parvis M, et al. Gas exchange
threshold as a predictor of severe postoperative
complications after lung resection in mild-to-
moderate chronic obstructive pulmonary disease.
Monaldi Arch Chest Dis 1998;53(2):127–33.
13. Dales RE, Dionne G, Leech JA, et al. Preoperative
prediction of pulmonary complications following
thoracic surgery. Chest 1993;104(1):155–9.
14. Gilbreth EM, Weisman IM. Role of exercise stress
testing in preoperative evaluation of patients
for lung resection. Clin Chest Med 1994;15(2):
389–403.
15. Datta D, Lahiri B. Preoperative evaluation of patients
undergoing lung resection surgery. Chest 2003;
123(6):2096–103.
16. Wyser C, Stulz P, Soler M, et al. Prospective evalua-
tion of an algorithm for the functional assessment of
lung resection candidates. Am J Respir Crit Care
Med 1999;159(5 Pt 1):1450–6.
17. Brunelli A, Charloux A, Bolliger CT, et al. ERS/ESTS
clinical guidelines on fitness for radical therapy in
lung cancer patients (surgery and chemo-radio-
therapy). Eur Respir J 2009;34(1):17–41.
18. Gianrossi R, Detrano R, Mulvihill D, et al. Exercise-
induced ST depression in the diagnosis of coronary
artery disease. A meta-analysis. Circulation 1989;
80(1):87–98.
19. Epstein SK, Faling LJ, Daly BD, et al. Inability to
perform bicycle ergometry predicts increased
morbidity and mortality after lung resection. Chest
1995;107(2):311–6.
20. Van Nostrand D, Kjelsberg MO, Humphrey EW. Pre-
resectional evaluation of risk from pneumonectomy.
Surg Gynecol Obstet 1968;127(2):306–12.
21. Pollock M, Roa J, Benditt J, et al. Estimation of venti-
lator reserve by stair climbing. Chest 1993;104:
1378–83.
22. Brunelli A, Al Refai M, Monteverde M, et al. Stair
climbing test predicts cardiopulmonary compli-
cations after lung resection. Chest 2002;121(4):
1106–10.
23. Brunelli A, Salati M. Preoperative evaluation of lung
cancer: predicting the impact of surgery on physi-
ology and quality of life. Curr Opin Pulm Med
2008;14(4):275–81.
24. Cooper KH. A means of assessing maximal oxygen
intake. Correlation between field and treadmill
testing. JAMA 1968;203(3):201–4.
25. Butland RJ, Pang J, Gross ER, et al. Two-, six-, and
12-minute walking tests in respiratory disease.
Br Med J (Clin Res Ed) 1982;284(6329):1607–8.
26. Guyatt GH, Townsend M, Keller J, et al. Measuring
functional status in chronic lung disease: conclu-
sions from a randomized control trial. Respir Med
1991;85(Suppl B):17–21 [discussion: 33–7].
27. Cahalin L, Pappagianopoulos P, Prevost S, et al. The
relationship of the 6-min walk test to maximal oxygen
consumption in transplant candidates with end-
stage lung disease. Chest 1995;108(2):452–9.
28. ATS Committee on Proficiency Standards for Clinical
Pulmonary Function Laboratories. ATS statement:
guidelines for the six-minute walk test. Am J Respir
Crit Care Med 2002;166(1):111–7.
29. Holden DA, Rice TW, Stelmach K, et al. Exercise
testing, 6-min walk, and stair climb in the evaluation
of patients at high risk for pulmonary resection.
Chest 1992;102(6):1774–9.
30. Brunelli A, Pompili C, Salati M. Low-technology exer-
cise test in the preoperative evaluation of lung
resection candidates. Monaldi Arch Chest Dis
2010;73(2):72–8.
31. Epstein SK, Faling LJ, Daly BD, et al. Predicting
complications after pulmonary resection. Preopera-
tive exercise testing vs a multifactorial cardiopulmo-
nary risk index. Chest 1993;104(3):694–700.
32. Ferguson MK, Durkin AE. A comparison of three
scoring systems for predicting complications after
major lung resection. Eur J Cardiothorac Surg
2003;23(1):35–42.
33. Falcoz PE, Conti M, Brouchet L, et al. The Thoracic
Surgery Scoring System (Thoracoscore): risk model
for in-hospital death in 15,183 patients requiring
thoracic surgery. J Thorac Cardiovasc Surg 2007;
133(2):325–32.
34. Chamogeorgakis T, Toumpoulis I, Tomos P, et al.
External validation of the modified Thoracoscore in
a new thoracic surgery program: prediction of in-
hospital mortality. Interact Cardiovasc Thorac Surg
2009;9(3):463–6.
35. Brunelli A, Xiume F, Refai M, et al. Evaluation
of expiratory volume, diffusion capacity, and exer-
cise tolerance following major lung resection: a
prospective follow-up analysis. Chest 2007;
131(1):141–7.

Cardiopulmonary Exercise Testing in Lung Cancer Surgery 245
36. Bolliger CT, Wyser C, Roser H, et al. Lung scanning
and exercise testing for the prediction of postopera-
tive performance in lung resection candidates at
increased risk for complications. Chest 1995;108(2):
341–8.
37. Beccaria M, Corsico A, Fulgoni P, et al. Lung cancer
resection: the prediction of postsurgical outcomes
should include long-term functional results. Chest
2001;120(1):37–42.
38. Colman NC, Schraufnagel DE, Rivington RN,
et al. Exercise testing in evaluation of patients
for lung resection. Am Rev Respir Dis 1982;
125(5):604–6.
39. Lim E, Beckles M, Warburton C, et al. Cardiopulmo-
nary exercise testing for the selection of patients
undergoing surgery for lung cancer: friend or foe?
Thorax 2010;65(10):847–9.
40. Loewen GM, Watson D, Kohman L, et al. Preoper-
ative exercise Vo2 measurement for lung resection
candidates: results of Cancer and Leukemia
Group B Protocol 9238. J Thorac Oncol 2007;
2(7):619–25.