Physiologic changes of pregnancy Prof. Aziza Tosson.
85
Physiologic changes of pregnancy Prof. Aziza Tosson
-
Upload
anthony-hampton -
Category
Documents
-
view
220 -
download
1
Transcript of Physiologic changes of pregnancy Prof. Aziza Tosson.
Physiologic changes of pregnancy
Prof. Aziza Tosson
AIMS
TO GAIN AN UNDERSTANDING OF THE PHYSIOLOGICAL CHANGES THAT OCCUR DURING PREGNANCY
LEARNING OUTCOMES IDENTIFY THE CHANGES THAT TAKE PLACE
WITHIN THE UTERUS AND BODY SYSTEMS DURING PREGNANCY
CONSIDER THE EFFECT THESE CHANGES HAVE ON THE WOMAN
EXPLORE THE ROLE OF THE MIDWIFE WHEN GIVING ADVISE TO THESE WOMEN
ObjectivesSymptoms and physical findings of each
organ systemPhysiologic versus pathologic changesDiagnostic tests and interpretations
during physiological changes
UNDERSTANDING NEEDED TO EXPLAIN THE PHYSIOLOGICAL
CHANGES THAT TAKE PLACE TO THE WOMAN
TO UNDERSTAND THE MINOR DISORDERS OF PREGNANCY
RECOGNISE PATHOLOGICAL CHANGES IN ORDER TO REFER APPROPRIATELY
[insert [insert presenter presenter
info]info]
Anatomical ChangesAnatomical Changes
PelvisPelvis
Pelvic Floor MusclesPelvic Floor Muscles
UterusUterus
Uterine LigamentsUterine Ligaments
CervixCervix
PlacentaPlacenta
Amniotic FluidAmniotic Fluid
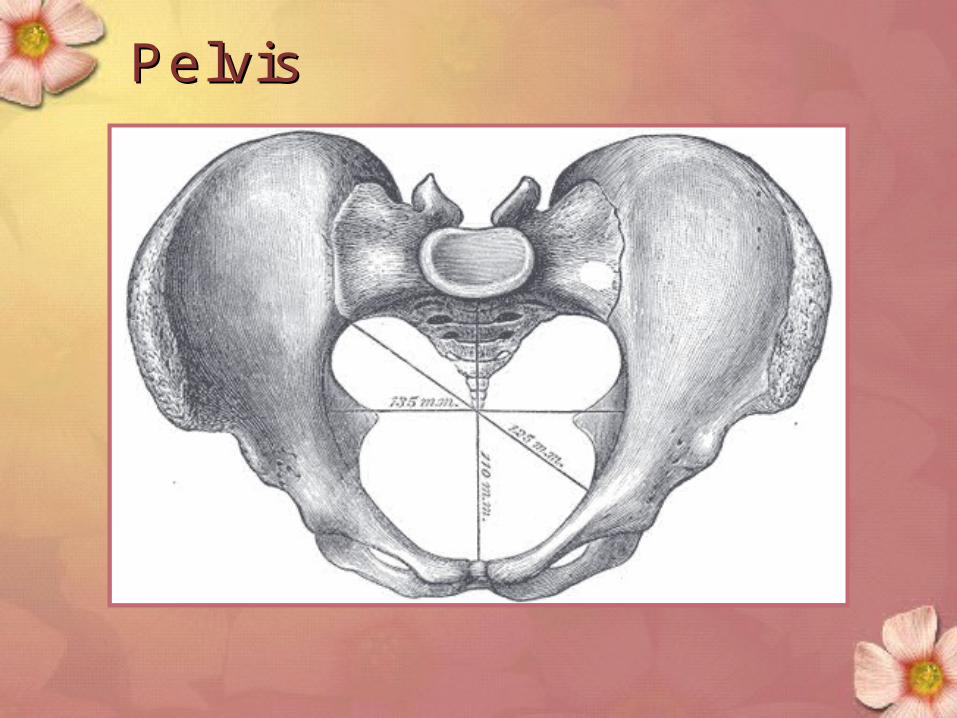
PelvisPelvis
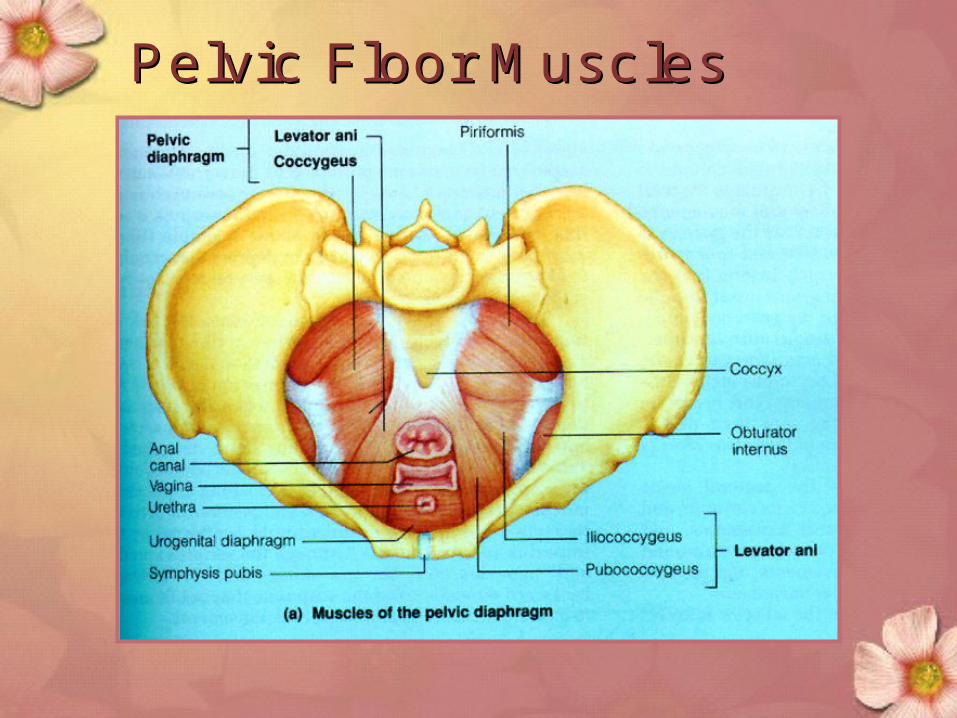
Pelvic Floor MusclesPelvic Floor Muscles
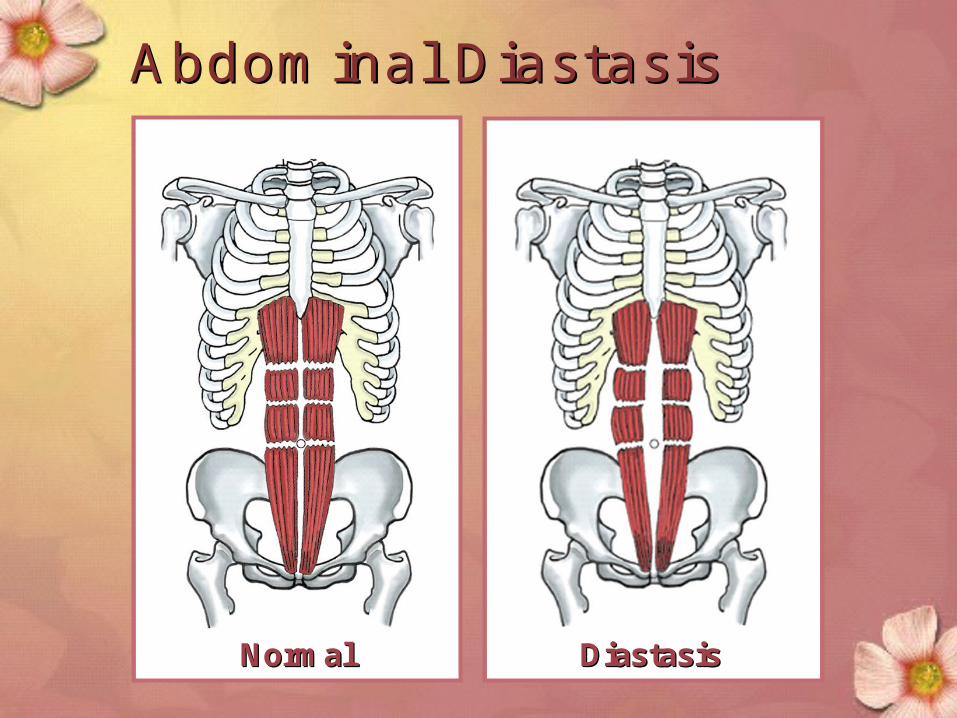
NormalNormal DiastasisDiastasis
Abdominal Abdominal DiastasisDiastasis
Physiological ChangesCirculatory
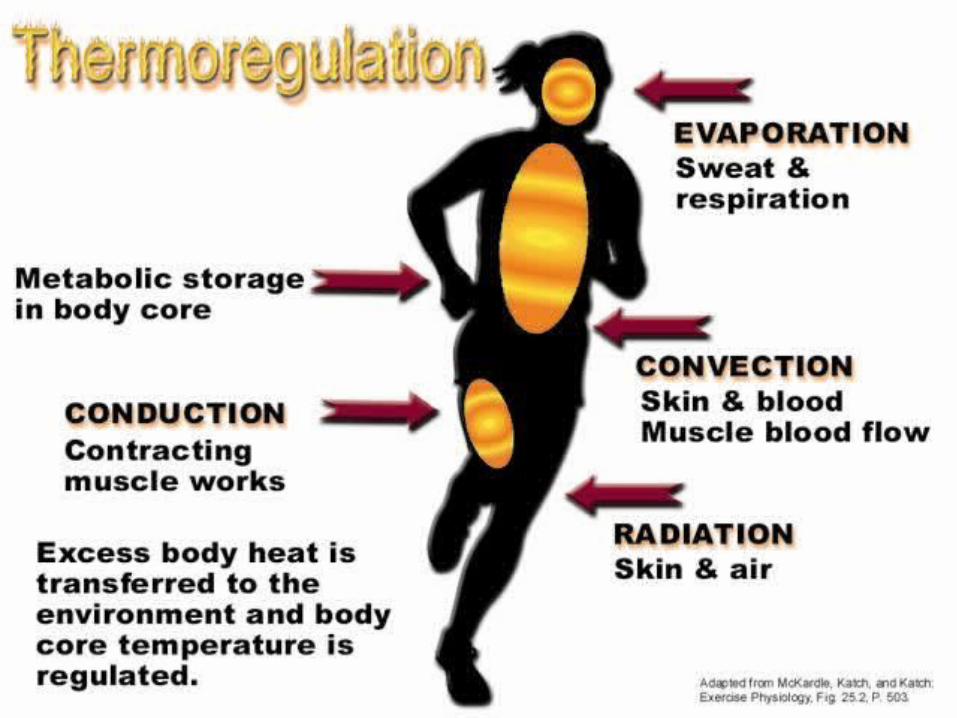
Thermoregulation
Metabolic
Respiratory
Digestive
Urinary
Skin
Breasts
Biomechanical
DEFINITIONTHE CHANGES THAT TAKE PLACE IN
THE MATERNAL ORGAN SYSTEM IN
RESPONSE TO PREGNANCY.
TO ACCOMADATE THE PREGNANCY
AND TO PREPARE THE WOMAN FOR
LABOUR
Organ systemsCardiovascular systemPulmonary systemGenital tractUrinary systemEndocrine systemGastrointestinal TractSkin
CHANGES ARE DUE TOALTERATIONS IN
HORMONAL PRODUCTION
CIRCULATION
METABOLISM
HORMONES
OESTROGEN
Produced in corpus luteum
Produced by placenta after 12 weeks
Responsible for growth particularly of uterus and breasts
progesterone Produced in corpus luteum and then the
placenta
Relaxes smooth muscle
Inhibits uterine contractions until uterus is prepared for labour
Regulates storage of body fat
Human chorionic gonadotrophicSecreted from trophoblast of the
developing embryo
Maintains corpus luteum until placenta takes over
Used in tests to confirm pregnancy
Human placental lactogenAlters maternal metabolism
Diverts glucose to fetus
Mobilises free fatty acids from maternal stores
RELAXIN
Released by corpus luteum then the Placenta
Softens pelvic ligaments
Reduces myometrial tone
Changes to Body SystemChanges to Body System
First TrimesterFirst Trimester Baby begins to growBaby begins to grow
Increased urinationIncreased urination
Changes with skin and Changes with skin and hairhair
Thickening waistlineThickening waistline
Nausea/fatigueNausea/fatigue
Second TrimesterSecond Trimester BabyBaby’’s weight increasess weight increases
Energy level improvesEnergy level improves
HeartburnHeartburn
Leg crampsLeg cramps
Pelvis relaxes causing SI Pelvis relaxes causing SI discomfortdiscomfort
Third TrimesterThird Trimester Baby has more rapid Baby has more rapid
growth & weight gaingrowth & weight gain
BackachesBackaches
Swelling of the hands, Swelling of the hands, legs, and feetlegs, and feet
BreathlessnessBreathlessness
More frequent More frequent urinationurination
Maternal changes - anatomical and physiological
Cardiovascular changes increase in SV increase in cardiac output increase in HR at given work load increase in blood volume (mostly during latter half
of pregnancy) Uterus may compress large blood vessels reducing
venous returnTotal Body water
Circulatory System
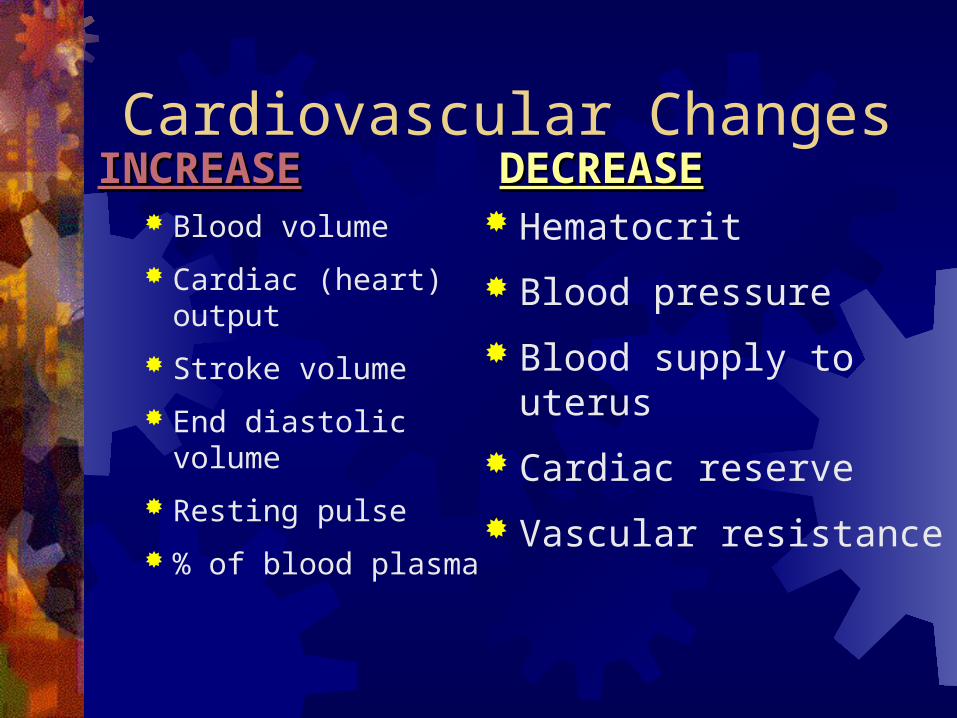
Cardiovascular Changes
Blood volume
Cardiac (heart) output
Stroke volume
End diastolic volume
Resting pulse
% of blood plasma
Hematocrit
Blood pressure
Blood supply to uterus
Cardiac reserve
Vascular resistance
DECREASEDECREASEINCREASEINCREASE
Wajed Hatamleh RN, MSN, PhD.Wajed Hatamleh RN, MSN, PhD.
Cardiovascular SystemCardiovascular System Heart shifts up and to the leftHeart shifts up and to the left
Hemoglobin stays the same (12-16 g/dL) initiallyHemoglobin stays the same (12-16 g/dL) initially May drop down to 10 g/dL and still be normal May drop down to 10 g/dL and still be normal
physiologic anemia.physiologic anemia. Normal pregnancy Hgb is 10-14 g/dL later in Normal pregnancy Hgb is 10-14 g/dL later in
pregnancypregnancy Decreased Hct (38-47%)Decreased Hct (38-47%)
Normal pregnancy Hct is 32-42 later in pregnancyNormal pregnancy Hct is 32-42 later in pregnancy Pulse rate may increase 10-15 beats.Pulse rate may increase 10-15 beats. Weight of uterus can cause supine hypotensive Weight of uterus can cause supine hypotensive
syndrome.syndrome.
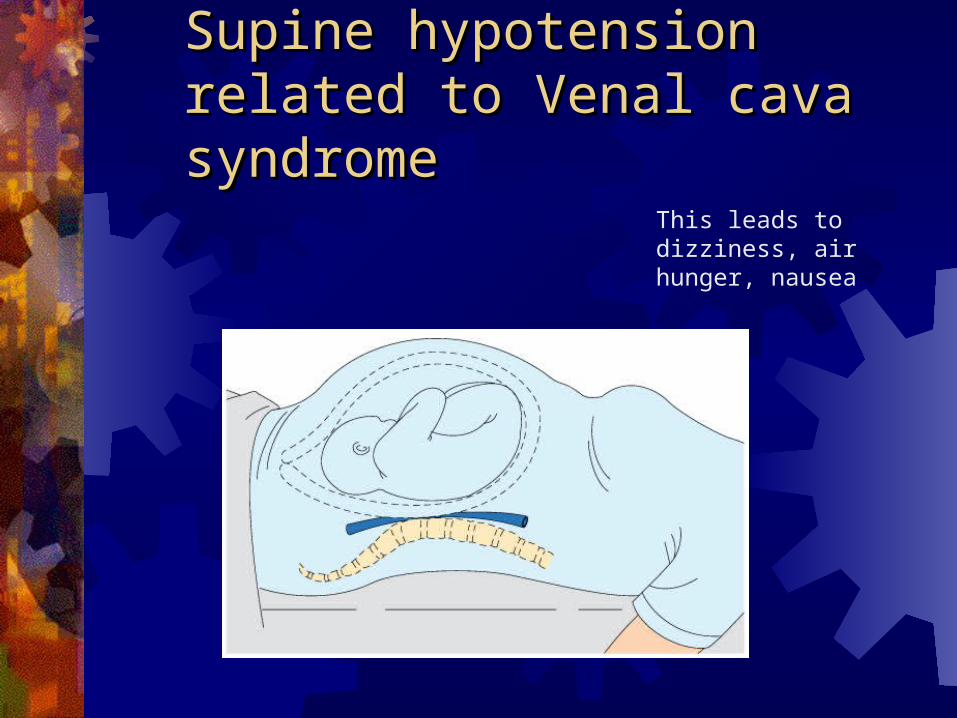
Supine hypotension related to Supine hypotension related to Venal cava syndromeVenal cava syndrome
This leads to dizziness, air hunger, nausea
Total body water Increases 6-8 L Increases by 40 %Normal body water
2/3 intracellular 1/3 extracellular
¾ interstitial ¼ intravasular
2/3 increase is extravascular
Physiologic anemia of pregnancy Physiologic intravascular change Plasma volume increases 50-70 %
Beginning by the 6th wk RBC mass increases 20-35 %
Beginning by the 12th wk Disproportionate increase in plasma volume
over RBC volume----Hemodilution Despite erythrocyte production there is a
physiologic fall in the hemoglobin and hematocrit readings
Iron deficiency anemia With erythropoiesis of pregnancy, iron
requirements increase. Because large amounts of iron may not be
available from body stores and may not be in the diet
Supplementation is recommended to prevent iron deficiency anemia
At term, Hemoglobin less than 10.0 is usually due to iron deficiency anemia rather than the hemodilution of pregnancy
Normal Iron Requirements Total body iron content average in normal adult
females is 2gm Iron requirement for normal pregnancy is 1 gm
200 mg is excreted 300 mg is transferred to fetus 500 mg is need for mom
Total volume of RBC inc is 450 ml 1 ml of RBCs contains 1.1 mg of iron 450 ml X 1.1 mg/ml = 500 mg
Daily average is 6-7 mg/day Small intervals between pregnancies are most
concerning
Respiratory systemMechanical
diaphragmConsumption
Increase in needed oxygenStimulation
Progesterone stimulation
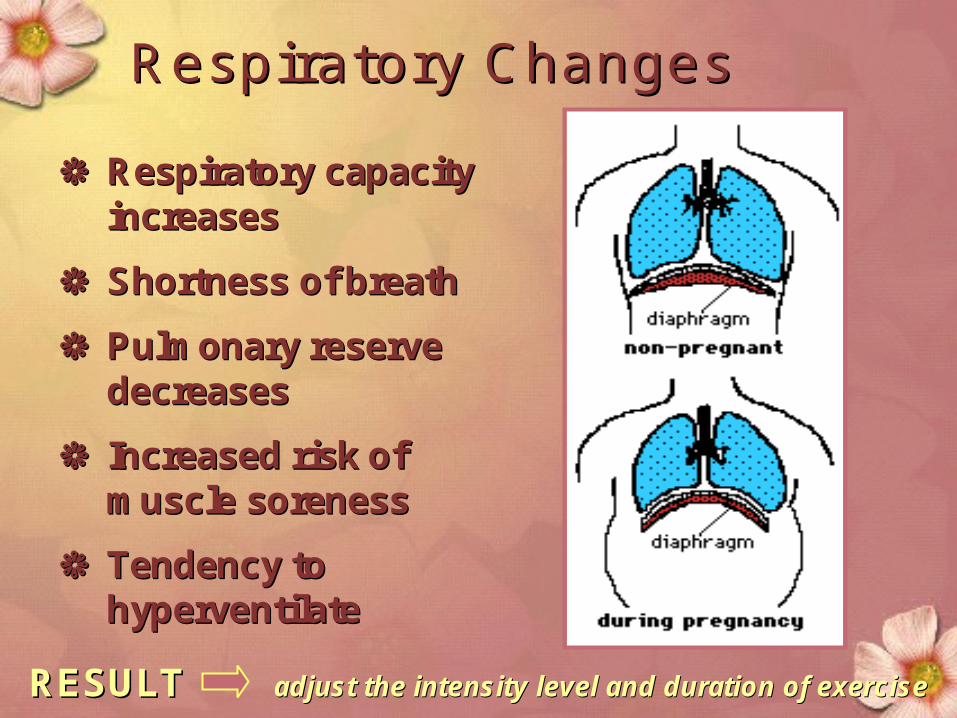
Respiratory ChangesRespiratory Changes
Respiratory capacity Respiratory capacity increasesincreases
Shortness of breathShortness of breath
Pulmonary reserve Pulmonary reserve decreasesdecreases
Increased risk of Increased risk of muscle sorenessmuscle soreness
Tendency to Tendency to hyperventilatehyperventilate
RESULT RESULT adjust the intensity level and duration of exerciseadjust the intensity level and duration of exercise
Physiologic changes - Physiologic changes -
RESPIRATORY SYSTEMRESPIRATORY SYSTEM
increase respiratory rateincrease respiratory rate increased oxygen consumptionincreased oxygen consumptioncommon are nasal stuffiness, common are nasal stuffiness,
nosebleeds due to nosebleeds due to Increased Increased vascular swelling to nosevascular swelling to nose
Respiratory Consumption
O2 consumption Increases 15-20 % 50 % of this increase is required by the uterus Despite increase in oxygen requirements, with the
increase in Cardiac Output and increase in alveolar ventilation oxygen consumption exceeds the requirements.
Therefore, arteriovenous oxygen difference falls and arterial PCO2 falls.
Physiologic changes -Physiologic changes - GASTROINTESTINALGASTROINTESTINAL
Digestive system slow due to progesteroneDigestive system slow due to progesteroneNausea and vomitingPtyalism: increase salivationHeartburn Hemorrhoids Prolonged gallbladder emptying time may lead Prolonged gallbladder emptying time may lead
to gall stonesto gall stones Bile salt buildup may lead to itching.Bile salt buildup may lead to itching.
Gastrointestinal Tract Displacement of the stomach and intestines Appendix can be displaced to reach the right
flank Gastric emptying and intestinal transit times are
delayed secondary to hormonal and mechanical factors
Pyrosis is common due to the reflux of secretions
Vascular swelling of the gums Hemorrhoids due to elevated pressure in veins
Digestive ChangesDigestive Changes
Digestive system slows Digestive system slows
Intestines are pushed up Intestines are pushed up and to the sides and to the sides
Smooth muscle of the Smooth muscle of the stomach relaxes and can stomach relaxes and can cause heartburncause heartburn
Constipation and hemorrhoids are Constipation and hemorrhoids are common during pregnancycommon during pregnancy
Morning sicknessMorning sickness
Physiologic changes -Physiologic changes - METABOLISMMETABOLISM
BMR increases by 20-25 % during pregnancy
Recommended weight gain – 25-35 lbOverweight – 15-25 lbUnderweight – 25-35 lb
Need for increased iron, calcium, fat, and protein
Metabolic Changes
Insulin level Carbohydrate utilization during exercise as
weight increasesEstrogen Progesterone RelaxinCaloric requirements by ~ 300 calories/dayProtein and fluid requirements
INCREASES IN:INCREASES IN:
Genital Tract Increased vascularity and hyperemia
Vagina Perineum Vulva
Increased secretions Characteristic violet color of the vagina
Chadwick’s sign Increased length to the vaginal wall Hypertrophy of the papillae of the vaginal
mucosa
Physiologic changes in Physiologic changes in pregnancy - Reproductive systempregnancy - Reproductive system
Uterus – Uterus – Enlarges : esp fundal area thickens, then Enlarges : esp fundal area thickens, then
thins later in pregthins later in preg Umbilicus by 20 weeksUmbilicus by 20 weeks Xyphoid by 36 weeks fundus, Braxton-Xyphoid by 36 weeks fundus, Braxton-
Hicks irregular contractions after 4 Hicks irregular contractions after 4 monthsmonths
Cervix – mucous plug, Goodell’s sign, Cervix – mucous plug, Goodell’s sign, Chadwick’s signChadwick’s sign
Ovaries –after 11 weeks, the plac prod Ovaries –after 11 weeks, the plac prod progesterone and estrogenprogesterone and estrogen
Changes in the cervixLength remains the same Increase in widthSoftening after third month due to
oestrogen Increased vascularity Increased cervical mucosa Increased glandular function
changes in sizeuterus grows to 30x23x20 at termweight increases to 900gms
hypertrophy.. Oestrogen causes cells to increase until 20 weeks gestation Hyperplasia:- number of cells increase under the influence of oestrogen.
After 20 weeks gestation
Uterine muscle tissue stretches to allow fetus to grow
Progesterone relaxes the smooth muscles enabling it to stretch
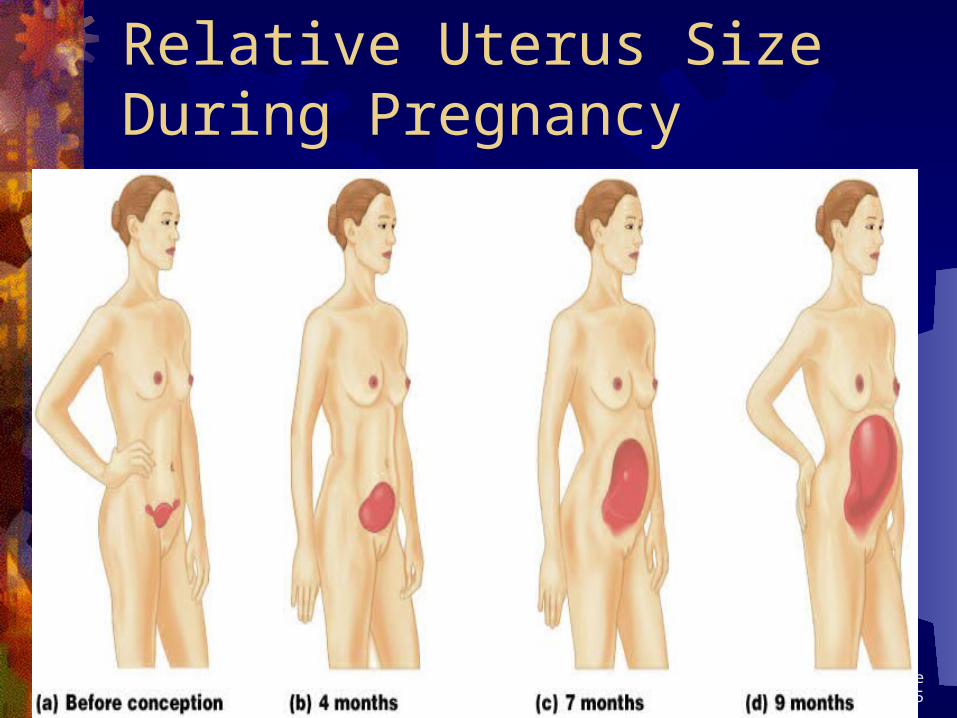
Relative Uterus Size During Pregnancy
Figure 28.15
Changes in the shape of the uterus
Isthmus elongates during the 1st 10 weeks like a stalk
From 7mm to 2.5cms at 10 weeks
Later becomes the lower segment with the globular uterus sitting on top
ORGANISATION OF MUSCLE FIBRES
Inner circular layer Surrounds cornua, lower uterine segment and
cervix
Middle layer Oblique, crisscross arrangement involved in
contractions to expel fetus
Outer longitudinal layer Contracts and retracts thickening the upper
segment
BY 12 WEEKSUterus is upright and leans slightly to the
rightNo longer a pelvic organUterus may be palpable above the pubic
boneFetus now occupies most of the uterine
cavityPlacenta now developed
2ND TRIMESTA Development of the upper and lower
uterine segmentUpper segment, thicker containing oblique
musclesLower segment formed from the isthmus
contains circular and longitudinal musclesUterus is pear shaped againBraxton Hicks contractions
3rd TRIMESTA
Lower segment formed from isthmus and contains longitudinal fibres
Upper segment thick and contains oblique muscle fibres
By 36 weeks lower segment measures 8-10cms
EngagementBy 38 weeks the cervix is taken up into
the lower segment
BLOOD CHANGES Increase in oestrogen:
new blood vessels formed
growth of existing ones
Therefore an increase in blood volume.
BLOOD SUPPLY TO UTERUS
Blood supply pre pregnancy = 10mls/min
At 40weeks 800 – 900mls/min
20% of cardiac output goes to uterus
Blood volume: from 5 litres to 7.5
total volume up by 40-50%
Red cell mass: rises constantly throughout
pregancy
Up by 20% by end of
pregnancy
PLASMA VOLUME
Increases from 10th week of pregnancy
variable related to parity, fetal weight and number
Reaches maximum level approx 50% above non-pregnant levels at 32-34 weeks then maintained
50% rise in plasma volume
20% rise in red cell mass
Heamodilution: Physiological anaemiaMost apparent at 32-34 weeks
RENAL SYSTEMDILATION OF THE RENAL VESSELSDUE THE EFFECTS OF
PROGESTERONE
INCREASED RENAL BLOOD FLOWGFR INCREASES BY 60% IN EARLY
PREGNANCYSIZE OF PORES INCREASED
Urinary Changes Kidneys grow and filter more
blood as the blood volume increases
Become more susceptible to bladder and kidney infections
Bladder becomes compressed causing frequent urination and incontinence
Wajed Hatamleh RN, MSN, PhD.Wajed Hatamleh RN, MSN, PhD.
Physiologic changes -Physiologic changes -
URINARY TRACTURINARY TRACT
Increased glomerular filtration rateIncreased glomerular filtration rateFrequencyFrequencyInfection : Infection : Smooth muscle of Smooth muscle of
bladder relaxes/stasisbladder relaxes/stasis
Endocrine Normal pregnancy physiology shows
“lower lows and higher highs” Postprandial hyperglycemia
To ensure sustained glucose levels for fetus Accelerated starvation
Early switch from glucose to lipids for fuels Insulin resistance promotes hyperglycemia
Resistance-Reduced peripheral uptake of glucose for a given dose of insulin
Mild fasting hypoglycemia occurs with elevated FFA, triglycerides,and cholesterol
WATER, WATER, WATER
Provide a ready source of water Encourage frequent water breaks
Hydration is a major concern Hydration is a major concern during maternal exercise.during maternal exercise.
Insulin resistanceAnti-insulin environment is aided by:placental lactogen
Like growth hormone Increases lipolysis and FFA Increases tissue resistance to insulin
Increased unbound cortisol Estrogen and Progesterone may also
exert some anti-insulin effects
Thyroid Estrogen stimulates Increase in TBG
Total T3 and T4 are increased However the active hormones remains unchanged
hCG stimulates thyroid TSH is reduced
Iodine deficient state Due to Increased renal clearance
To rule out pathologic changes Early in pregnancy TSH can be used Later free T4 is needed
LiverLiver morphology unchangedLab Tests similar to liver disease
Alkaline phosphatase doubles AST, ALT, GGT and bilirubin are slightly
lower Decreased plasma albumin
Gallbladder Impaired contractionHigh residual volumesPromotion of stasisStasis associated with increased
cholesterol saturation of pregnancy, supports predisposition of stones
Intrahepatic cholestasisRetained bile salts-pruritus gravidarum
Wajed Hatamleh RN, MSN, PhD.Wajed Hatamleh RN, MSN, PhD.
Physiologic changes -Physiologic changes -INTEGUMENTARY SYSTEMINTEGUMENTARY SYSTEMThese result from stretching of the skin and These result from stretching of the skin and
hormonal changeshormonal changesLinea nigra: pigmentation down middle line pigmentation down middle line
of abdof abdChloasma – “mask of pregnancy”Straie: stretch marks of abd, breasts, stretch marks of abd, breasts,
thighs and buttocksthighs and buttocksSweating
Skin changesChloasma or melasma gravidarumStriaeLinea nigra
Skin ChangesStretch marks
Dark pigmented line on there abdomen which is called Linea Nigra
Pigment changes on their face and neck
Small blood vessels in the face, neck and upper chest
MOST OF THESE RESOLVE AFTER PREGNANCY
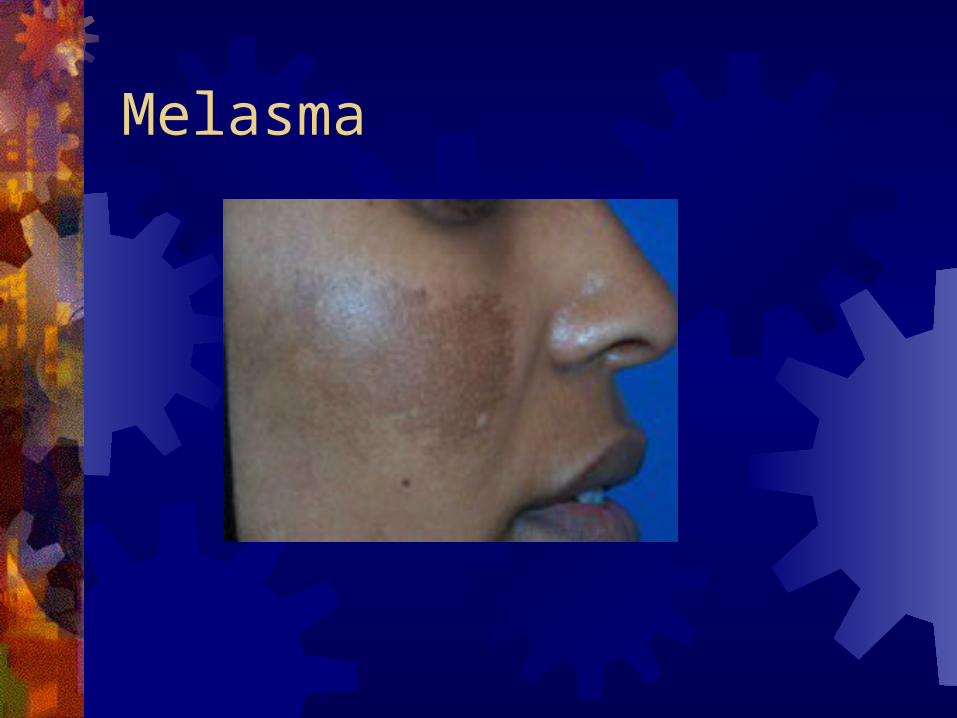
Melasma

Melasma
MelasmaAlso known as the mask of pregnancyMore common in dark skin peopleMore pronounced in the summerFades a few months after deliveryRepeated pregnancy can intensifyCan occur in normal non-pregnant
women with harmless hormonal imbalances or women on OCPs or depo
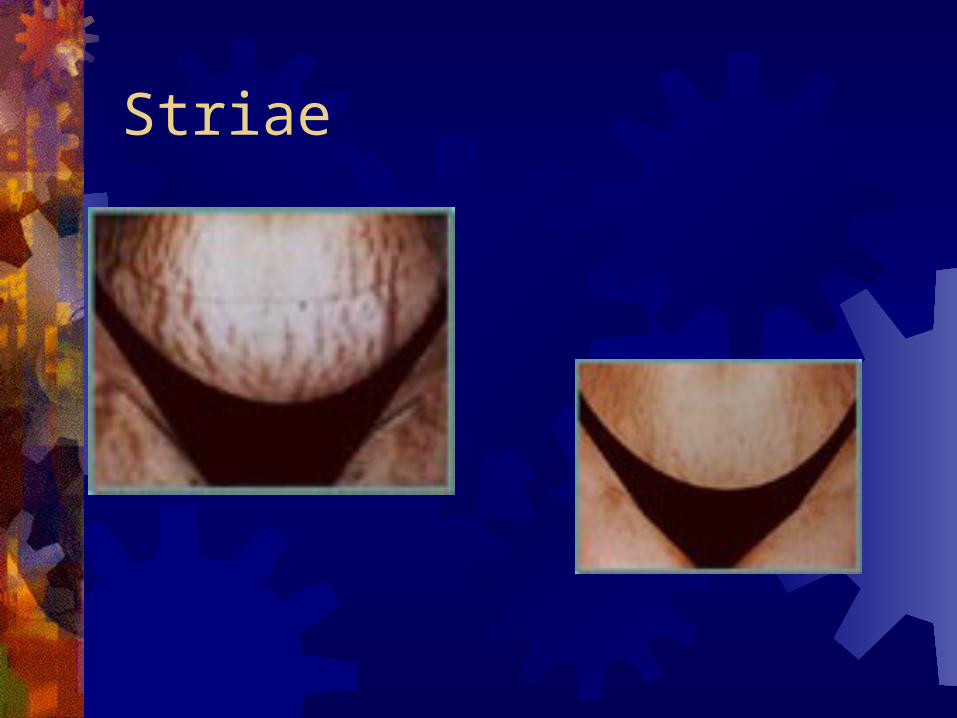
Striae
StriaeReddish slightly depressedBreasts, thighs, and abdomen In future pregnancies they appear as
glistening, silver lines
Linea nigra
HyperpigmentationMelasma and linea nigraEstrogen and progesterone Some melanocyte stimulating effect
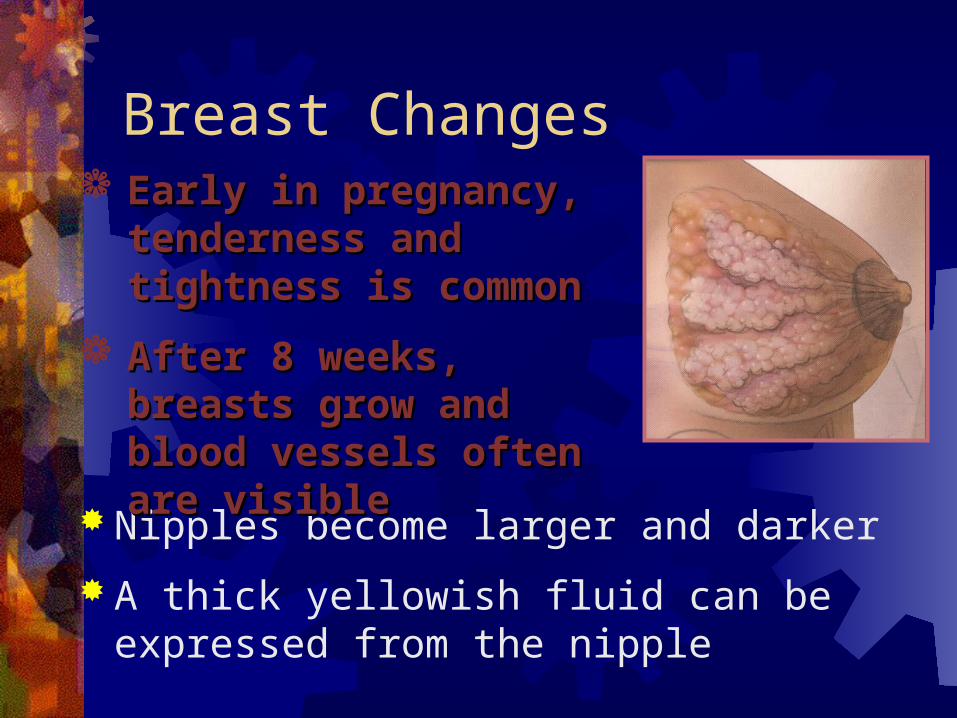
Breast Changes
Nipples become larger and darker
A thick yellowish fluid can be expressed from the nipple
Early in pregnancy, Early in pregnancy, tenderness and tightness tenderness and tightness is commonis common
After 8 weeks, breasts After 8 weeks, breasts grow and blood vessels grow and blood vessels often are visibleoften are visible
Wajed Hatamleh RN, MSN, PhD.Wajed Hatamleh RN, MSN, PhD.
MS systemMS system
Joint relaxationJoint relaxation Posture changesPosture changes -lordosis/center of -lordosis/center of
gravity gravity Back acheBack ache Diastasis recti: separation of rectus Diastasis recti: separation of rectus
abdominous abdominous Leg cramp due to calcium, and Leg cramp due to calcium, and
stretching stretching
Pelvic Floor Muscle Functions
Maintain alignment and support of internal organs
Control of urine flow
Sexual enhancement
Eliminate waste from rectum
Improve recovery from episiotomy
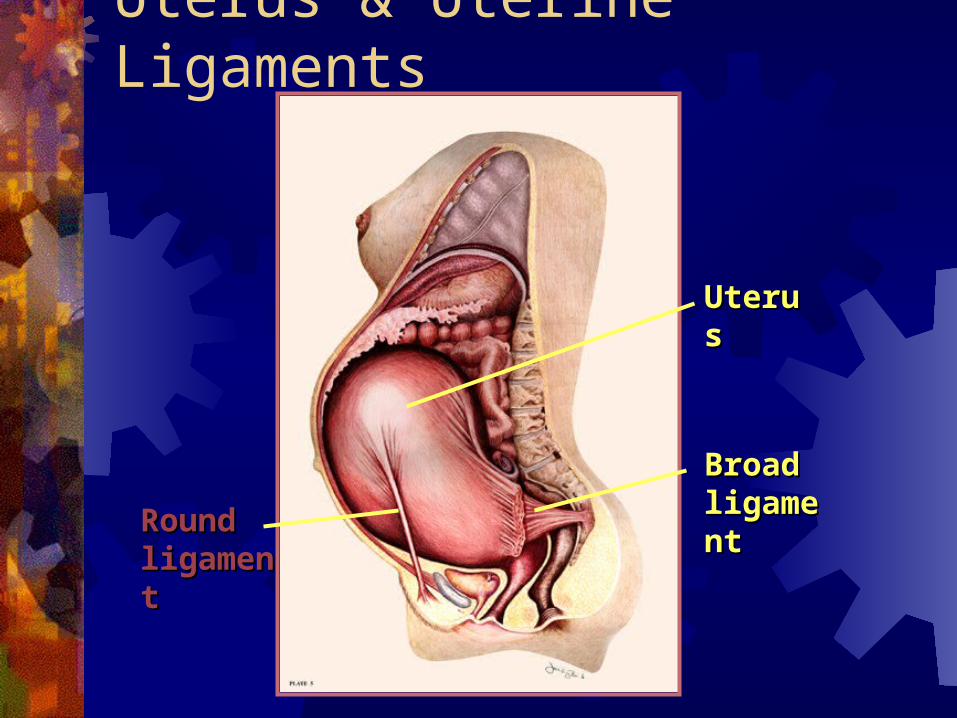
Uterus & Uterine Ligaments
UterusUterus
Broad Broad ligamentligament
Round Round ligamentligament
Biomechanical ChangesWeight distribution shifts
Joint movement
Balance of muscle strength
Spinal curves increase
Joint laxity becomes greater
More structural discomfort
Increased potential for nerve compression
Potential for InjuryNerve compression
syndromes
Low back discomforts or pelvic pain
Upper back fatigue
Lower extremity
Pelvic floor function
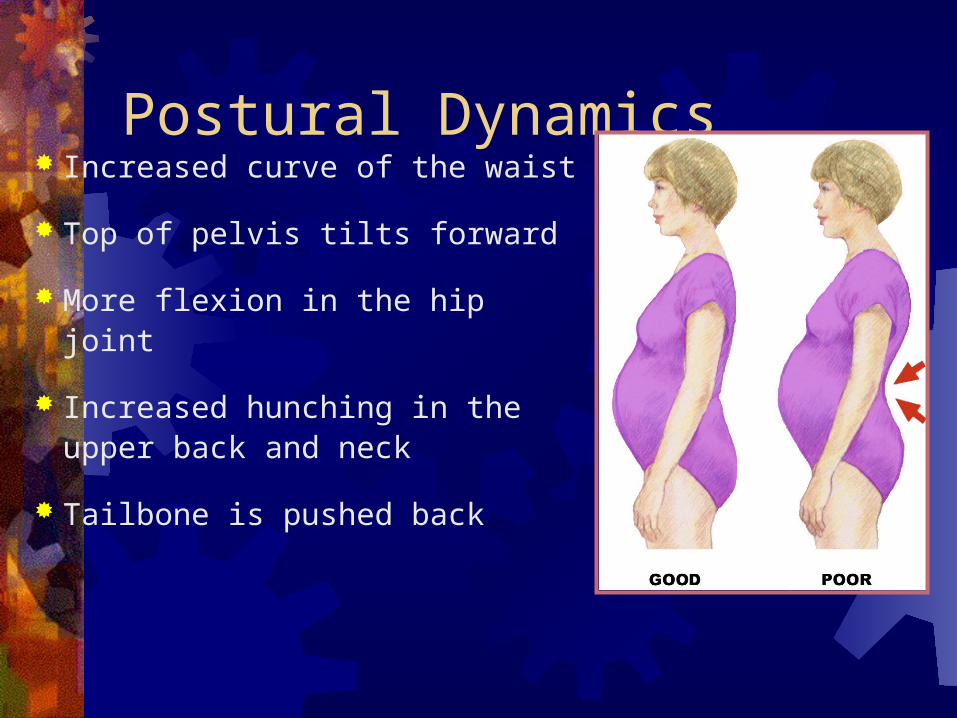
Postural Dynamics Increased curve of the waist
Top of pelvis tilts forward
More flexion in the hip joint
Increased hunching in the upper back and neck
Tailbone is pushed back
Muscles Affected Overstretching & weakening of gluteal muscles &
hamstrings Overstretching & weakening of abdominal
muscles & pelvic floor Overstretching & weakening of upper back
muscles Shortening and tightening of low back & hip
flexors muscles Shortening of upper back flexors & pectoral
muscles
Wajed Hatamleh RN, MSN, PhD.Wajed Hatamleh RN, MSN, PhD.
Neurological and sensoryNeurological and sensory
Decreased intraoccular pressureDecreased intraoccular pressure Corneal thickeningCorneal thickening Altered sense of smellAltered sense of smell Decreased attention spanDecreased attention span Problems with memoryProblems with memory Altered CNS physiology leading to Altered CNS physiology leading to
mood disturbance.mood disturbance.
Combat Effects of Gravity/ Hormones
Do pelvic tilts Alter the stance Shorten the jog stride Lower or eliminate the
step in aerobics Avoid rapid leg abduction Avoid breast stroke kick in
swimming Recognize tolerance for
activities will vary
Do pelvic floor exercises to prevent trauma
Emphasize strengthening & stretching exercises
Wear abdominal support/ sports bra when exercising for support
Changes to Body System First Trimester Baby begins to grow Increased urination Changes with skin and hair Thickening waistline Nausea/fatigue
Second Trimester Baby’s weight increases Energy level improves Heartburn Leg cramps Pelvis relaxes causing SI
discomfort
Third Trimester Baby has more rapid
growth & weight gain Backaches Swelling of the hands, legs,
and feet Breathlessness More frequent urination