Physio Article
23
1 EFFICACY OF THREE PHYSIOTHERAPY INTERVENTIONS IN INFLUENCING CLINICAL AND BIOCHEMICAL CHANGES OF DELAYED ONSET MUSCLE SORENESS(DOMS) IN RECREATIONAL ATHLETES Synopsis Submitted to SAVEETHA UNIVERSITY For the award of the degree of DOCTOR OF PHILOSOPHY in PHYSIOTHERAPY by S. SUDHAKAR Research Supervisor Dr. G. Arun Maiya, Ph.D DEPARTMENT OF PHYSIOTHERAPY SAVEETHA UNIVERSITY CHENNAI-602105 October 2010
-
Upload
dr-krishna-n-sharma -
Category
Documents
-
view
230 -
download
0
Transcript of Physio Article

1
EFFICACY OF THREE PHYSIOTHERAPY INTERVENTIONS IN
INFLUENCING CLINICAL AND BIOCHEMICAL CHANGES OF
DELAYED ONSET MUSCLE SORENESS(DOMS) IN RECREATIONAL
ATHLETES
Synopsis Submitted to
SAVEETHA UNIVERSITY
For the award of the degree of
DOCTOR OF PHILOSOPHY
in
PHYSIOTHERAPY
by
S. SUDHAKAR
Research Supervisor
Dr. G. Arun Maiya, Ph.D
DEPARTMENT OF PHYSIOTHERAPY
SAVEETHA UNIVERSITY
CHENNAI-602105
October 2010

2
CONTENTS
S.No CHAPTERS Page No
1. CHAPTER 1 –INTRODUCTION 4
1.1 Introduction 4
1.2 Problem Statement 5
1.3 Recent trends in the scientific study of the importance of
Physiotherapy Modalities in ameliorating the delayed onset muscle
soreness (DOMS) of recreational athletes.
6
1.4 Need for the study 6
1.5 Significance of the proposed study in the context of current status 6
1.6 Operational Definitions 7
2. CHAPTER 2: OBJECTIVES, PLAN AND SCOPE 7
2.1 Aim of the study 7
2.2 Objectives of the study 7
2.3 Relevance and Scope of the study 8
3. CHAPTER 3: MATERIALS AND METHODS 8
3.1 Study Procedure 10
3.2 Induction Of Delayed Onset Muscle Soreness 10
3.3 Treatment Protocols 11
3.4 Post test Measurements 11
4. CHAPTER 4: STATISTICAL ANALYSIS AND RESULTS 13
4.1 Creatine kinase (CK) 13

3
4.2 Lactate dehydrogenase (LDH) 15
4.3 Maximum isometric voluntary contraction (MIVC) 18
4.4 Repeated measures ANOVA results for dependent variables CK,
LDH and MIVC 19
4.5 Pain score 19
5. CHAPTER 5: DISCUSSION 20
6. CHAPTER 6: CONCLUSION 21
7. CHAPTER 7: REFERENCES 22
8. List of Publications 23

4
INTRODUCTION
1.1 INTRODUCTION
Delayed Onset Muscle Soreness (DOMS) is a common phenomenon experienced by
individuals who perform unaccustomed exercise that typically involves an eccentric
component. The soreness begins to occur at approximately 8 - 24 hours post-exercise and
peaks at approximately 48 hours post exercise. Perception of soreness is generally reduced at
72 hours with residual soreness remaining beyond that time frame. After the exercise, the
symptoms usually appear a couple of hours to a day, peak between 1 and 3 days, and may
subside within 5 to 7 days, (Clarkson and Hubal, 2002).This constellation of symptoms is
often called “Delayed Onset Muscle Soreness (DOMS)”.
DOMS PHYSIOLOGICAL CAUSES:
By mid 80’s the thought of lactic acid build up in the muscles as a cause for DOMS
was put to rest. Likewise from the 80's and early 90's the main theories that seem to be still
active are DOMS is due to muscle cell damage (ruptured cells spilling contents), where the
repair process makes nerve endings sensitive to the pain signal, or it is due to an
inflammatory response ( Tidball 1995). The latter suggests that the 48 hour period when
DOMS hits is the peak time for cell death (Armstrong 1984).From the reviews it is assumed
that the pain is actually the building up of the new muscle fiber material where other fibers
are getting pushed out of the way as new tissue comes in.
PATHOPHYSIOLOGY OF DELAYED ONSET MUSCLE SORENESS (DOMS):
Five hypotheses are used to explain the pathophysiology of DOMS.
1. Structural damage from high tension.
2. Metabolic waste product accumulation.
3. Increased temperature.
4. Spastic contracture.
5. Myofibrillar remodeling.
WHY DOMS NEED TO BE TREATED: DOMS can temporarily reduce muscle
performance. The diminished performance results from reduced voluntary effort due to the
sensation of soreness and from the muscle's lowered capacity to produce force. DOMS hurts
and the consequent effects are decreased range of motion, increased size from swelling, and

5
less power to work in the affected muscles. Negative implications of DOMS include minimal
to severe soreness, the inability to continue safe and effective training or performance,
biomechanical alterations predisposing individuals to injury, decrease in strength and power,
interruption of activities of daily living (ADL’S) and a decreased motivation and willingness
to continue training due to negative experiences of the soreness( Weber servedio et al.1994).
In order to minimize negative experiences associated with DOMS and potential detrimental
effects on performance, it is necessary to identify a successful treatment intervention.
HOW DOMS CAN BE TREATED:
DOMS can be treated either by advising complete rest from the participation, by medical
management and various physiotherapy approaches to reduce the soreness symptoms.
VARIOUS PHYSIOTHERAPY APPROACHES: Physiotherapy Interventions play a major
role both in prevention and treatment for the negative effects associated with DOMS. Many
treatments have been investigated which include massage, electrical stimulation, ultrasound,
acupuncture (Barlas, 2000), cryotherapy, repeat bout exercise, stretching (Johansson 1999),
Low intensity Laser therapy (Craig 1999), Iontophoresis (Hasson 1992), Transcutaneous
electrical nerve stimulation (TENS) (Craig 1996), preventative training, and even hyperbaric
oxygen therapy (Mekjavic, 2000).
1.2 PROBLEM STATEMENT:
Strength, range of motion, and a feeling of competence are important factors in
performing sports and exercise. Unaccustomed eccentric exercise causes adverse effects on
these factors (Bourgeois, MacDougall, 1999).Eccentric exercise, therefore may cause
significant reduction in performance during training and competition and/or increase the risk
of further injury. If athletes perform eccentric exercise with several muscles during training,
it is possible that the exercise efficiency on the subsequent day might be impaired. To date, a
sound and consistent treatment for DOMS has not been established. Although multiple
practices exist for the treatment of DOMS, few have scientific support. Suggested treatments
for DOMS are numerous and include pharmaceuticals, herbal remedies, stretching, massage,
nutritional supplements, and many more. As DOMS has been shown to alter biomechanics of
movement (Ebbeling and Clarkson 1989) and predispose participants to injury, it is important
to determine an effective treatment intervention that will reduce the negative impacts of

6
DOMS. The present research is done on recreational athletes as they usually begin a
new exercise programme, increase their exercise intensity and commonly change their
sports activity.
1.3 RECENT TRENDS IN THE SCIENTIFIC STUDY OF THE IMPORTANCE
OF PHYSIOTHERAPY MODALITIES IN AMELIORATING THE DELAYED
ONSET MUSCLE SORENESS (DOMS) OF RECREATIONAL ATHLETES:
In the past, gentle stretching was one of the recommended ways to reduce
exercise related muscle soreness, but a study by Australian researchers published in 2007
found that stretching is not effective in avoiding muscle soreness. Recently study was done
on better attenuation effects of compression in DOMS, compression (and compression suits)
have been studied over the past 8 years. In another recent study Rhea, Bunker (2009),
investigated DOMS pain reduction with Vibration, Perceived pain was measured at 12, 24,
48, and 72 hours post workout. Many studies have been done to find out the significance
effects of modalities on DOMS, but none of the studies so far have been shown much
significant results in the markers of DOMS and in relieving the symptoms of muscle
soreness.
1.4 NEED FOR THE STUDY: The extensive reviews of the literature reveal that, there is
paucity of studies on role of various Physiotherapy modalities in ameliorating the DOMS.
Coaches, athletes, and medical practitioners are well aware of the symptoms of muscle
damage after eccentric exercise because it clearly affects subsequent exercise or performance
(i.e., strength, power, range of motion and probably exercise economy). Muscle weakness
requires a longer recovery and might have more impact on performance than soreness
sensation. Therefore the present study is needed to help for the athletes to be safe from the
above problems arising out of muscle damage.
1.5 SIGNIFICANCE OF THE PROPOSED STUDY IN THE CONTEXT OF
CURRENT STATUS:
INTERNATIONAL STATUS: Developed countries with their modern “Know how” are
progressing rapidly in exploring the possibilities of various physiotherapy modalities to
supplement the medical management thereby to facilitate early recovery.

7
NATIONAL STATUS: The wealth of knowledge that has been provided by our researchers
regarding the use of various physiotherapy modalities for DOMS has to be collaborated with
detailed well organized study. Such a scientific study will facilitate Indian researchers and
clinicians to use these modalities to treat DOMS effectively.
1.6. OPERATIONAL DEFINITIONS:
Delayed onset muscle soreness (DOMS) Muscle soreness experienced by individuals
Who perform unaccustomed exercise that involves an eccentric component
Eccentric action Lengthening of a muscle under tension (Hall, 1991)
RECREATIONAL ATHLETE: “Recreational athlete" means an individual participating in
fitness training and conditioning, sports or other athletic competition, practices or events
requiring physical strength, agility, flexibility, range of motion, speed or stamina and who is
not affiliated with an amateur, educational or professional athletic organization or any
association that sponsors athletic programs or events in the State.
2. OBJECTIVES PLAN AND SCOPE OF THE STUDY
2.1 AIM OF THE STUDY:
To investigate the effects of three physiotherapy interventions in delayed onset muscle
soreness and its influence on biochemical markers in recreational athletes.
2.2 OBJECTIVES OF THE STUDY:
1. To investigate creatine kinase (CK) and Lactate dehydrogenase (LDH) enzymatic activity
taken at repeated time measures in 3 different physiotherapy interventions and compared
with a control group.
2. To evaluate the effect of 3 physiotherapy modalities on Maximum isometric voluntary
contraction (MIVC) in experimentally induced delayed onset muscle soreness in
recreational athletes
3. To determine the effect of physiotherapy on pain parameters using VAS scale.
4. To compare the effectiveness of physiotherapy modalities on biochemical parameters(CK
& LDH), maximum isometric voluntary contraction and pain scale taken at different

8
times after experimentally inducing delayed onset muscle soreness in recreational
athletes.
2.3 RELEVANCE AND SCOPE OF THE STUDY:
Delayed onset muscle soreness (DOMS) is a familiar experience for the elite as well as
the novice athlete. Symptoms can range from muscle tenderness to severe debilitating pain.
The mechanisms, treatment strategies, and impact on athletic performance remain uncertain,
despite the high incidence of DOMS (Cheung, Hume, Maxwell Sports Med. 2003). DOMS is
most prevalent at the beginning of the sporting season when athletes are returning to training
following a period of reduced activity. Several theories have been proposed to explain the
underlying cause of delayed onset muscle soreness, however none is universally accepted.
There are also many anecdotal claims that the effects of DOMS can be reduced with various
treatment modalities. Again no method has any conclusive, empirical support for the
prevention of delayed onset muscle soreness. In India, recently increasing numbers are
participating in athletic activities and are taking a more active approach to achieve health and
wellness. This increase in activity exposes individuals to DOMS and the associated negative
effects. Even though the benefits of regular exercise are well known, many of us don't do it.
One reason may be that pain or discomfort sometimes goes along with fitness activities.
Starting or continuing an exercise program may be easier if you understand what muscle
soreness is and what to do about it. Interventions such as physiotherapy play a major role
both in prevention and treatment for the negative effects associated with DOMS. Most of the
individuals and athletes experience muscle soreness after unaccustomed exercises due to lack
of training, this highly demands some intervention, and not much research have been done in
India to meet those demands. Also, the exact role of a physiotherapist in alleviating the
DOMS and therapeutic interventions is also not successful in India.
3. MATERIALS AND METHODOLOGY
SUBJECTS: 160 normal collegiate recreational athlete subjects in the age group 18-25 years
who were not under any training protocols and with no history of upper arm injury were
recruited after approval from the Institutional Ethics committee. The number of subjects was
determined by a power analysis with 90% power and a 1-tailed level of significance of P
<.0.5 based on data from the pilot study. During the experimental period, subjects were

9
requested not to take any medication, change their diet, or perform any strenuous exercise.
All subjects were informed about the meaning of the study.
SAMPLING: Quota sampling technique was used and all the subjects were randomized
equally in to four groups, each group having forty subjects.
STUDY PERIOD: The study was conducted for a total period of two years and eight months.
STUDY CENTER: The whole study was conducted in Saveetha University.
PILOT STUDY: A pilot study was performed prior to data collection for the present study.
The goal of the pilot study was to: (1) to collect data that will provide an opportunity to gain
some practical experience in carrying out the proposed protocol, (2) ensure that instructions
to subjects are clear and concise, and make modifications where necessary, (3) determine
whether or not the soreness inducing exercise session would elicit the expected level of
perceived soreness, (4) collect and analyze preliminary data.
After the approval of ethical clearance from university, the pilot study was
conducted. The main objective of the pilot study was to know the percentage of 1 RM to be
selected for inducing delayed onset muscle soreness (DOMS) and to know their recovery
from DOMS. In the pilot study, 9 college athletes were selected, and they were divided in to
3 groups, each group having 3 participants.70 % of 1 RM for group A, and 80 % of 1 RM for
group B, and 90 % of 1 RM for group C have been taken to induce DOMS experimentally.
Subjects were then given a VAS scale with specific instructions on how to record information
regarding their level of soreness. From the results it was found that group B (80% of 1 RM)
recovered faster when compared to group C. Group A did not developed the symptoms of
DOMS. Group C took much time for pain recovery. Pain by VAS scale is the outcome
measure taken at 24 hours and after 96 hours.
GROUP A (70% of 1RM) GROUP B (80% of 1RM) GROUP C (90 % of 1 RM)
Mean SD Mean SD Mean SD
24 Hours 3 1 7 1 8.3 0.57
96 Hours 0.6 1.15 4.3 0.57 7.3 0.57
From the results of the pilot study it was found that 80 % of 1 RM was enough to induce
DOMS experimentally when compared to 70% and 90% of 1 RM.
STUDY DESIGN: The research design consisted of Pre test- Post test true experimental
study design with two factors (Groups and time) with repeated measures on time.

10
3.1 STUDY PROCEDURE
160 collegiate athletes Participated in the study
Study divided in to 4 phases
PHASE-I BASELINE
MEASUREMENT
Serum CK, LDH, MIVC
and Pain measurement
were taken at the baseline
before inducing DOMS.
PROCEDURE
PHASE-2 DOMS
INDUCTION
All participants were
induced DOMS by an
eccentric loading
protocol with barbell
after calculating 1 RM.
PHASE-3
TREATMENT
After inducing DOMS,
Participants were
allocated randomly in
to four groups. Each
group consisting of 40
participants.
PHASE -4 POST
TESTMEASUREMENT
Serum CK,
LDH,MIVC and Pain
measurement were
taken at 24, 48, 72 and
96 hours before the
treatment intervention
Group ICryotherapy
Group IIUltrasound
Group IIIExercises
Group IVControl
Treatment was applied at 24, 48, 72 and 96 hours.
3.2 INDUCTION OF DELAYED ONSET MUSCLE SORENESS:
All the subjects were induced delayed onset muscle soreness (DOMS) by an eccentric
loading protocol with a barbell (Tiidus and Ianuzzo, 1983)
Eccentric Loading Protocol:
1 RM Calculation:
The subject was asked to lift a fixed weight in his hand from a fully extended to a fully flexed
position in standing position. The amount of weight was determined by subject's perception.
Initially 1 Repetitive maximum (RM) was calculated by using the formula
[Number of repetitions + 1] X Weight used.
30
80 % of 1 RM was calculated and used for inducing DOMS. Concentric contractions were
followed by eccentric contractions for 7 seconds. Assistance was given for concentric
contractions and no assistance given for eccentric contractions and all the subjects were
verbally encouraged. The subjects were instructed to perform 4 sets, 1 set consisting of 10

11
repetitions, with a rest period of 3-5 minutes between each set. After inducing DOMS the
subjects were divided into one of four treatment groups.
3.3 TREATMENT PROTOCOLS
Treatments were administered at 24, 48, 72, and 96 hours post exercise.
The following protocols outline the treatment that subjects received in their respective
groups.
Group I: Cryotherapy-Ice massage was given by a method of direct application with ice bag
technique for duration of ten to fifteen minutes after 24, 48, 72 and 96 hours.
Group II: Phonophoresis- Participants in group II received Phonophoresis ( Phyaction 190i
ultrasound), Intensity of 0.8 watts/cm2 for a duration of 8 minutes given after 24, 48, 72 and
96 hours.
Group III: Participants in group III were instructed to do an exercise protocol. The
individuals in the exercise group performed mild full ROM elbow flexion and extension
exercises, with only the gravitational pull on the hand and arm providing resistance. The
repetitions were performed continuously during a 20-second period and then rested for 40
seconds. This exercise /rest interval was continued for a total treatment time of 15 minutes.
Group IV: Control-No therapy was administered. Rest advised for them.
3.4 POST TEST MEASUREMENTS
DEPENDENT VARIABLES:
Maximum isometric voluntary contraction (MIVC) of elbow flexors by modified hand held
dynamometer, Plasma Creatine kinase (CK) and Lactate dehydrogenase (LDH) activity were
measured from blood samples taken from Cubital veins. Pain assessment was made from
VAS scale. All measurements were taken at the baseline, 24, 48, 72 and 96 hours after
inducing delayed onset muscle soreness (DOMS).
DATA COLLECTION:
SERUM CK AND LDH LEVELS:
The analysis is done in Erba Chem 5 plus v2 instrument, Blood samples of 2 ml were
collected from all the subjects using a disposable syringe and the serum separated. Than 50
micro liters of serum added to1 ml of CK reagent, and incubated at 37 degree Celsius for 100
seconds in an incubator. Similarly 50 micro liters of serum added to 1 ml of LDH reagent,
and incubated at 37 degree Celsius for 1 minute in an incubator.

12
Test has been done by using the kits from Agappe diagnosis following the standard protocol
and readings displayed in the instrument were noted. This procedure was done at baseline,
24, 48, 72 and 96 hours and the values were noted.
MAXIMUM ISOMETRIC VOLUNTARY CONTRACTION (MIVC):
INSTRUMENT: The dynamometer is a modified Wika pressure gauge (van der Ploeg, 1984)
the pressure range is 0-300 Newton (N). The meter is equipped with a maximum indicating
pointer with a resetting knob and a curved applicator.
MEASUREMENT TECHNIQUE AND TEST PROCEDURE: At least one practice trial was
given to the participants to familiarize them with the feel of pushing against the
dynamometer. The participants then performed the action actively until they performed it
correctly. Participants were asked to build their force gradually to a maximum voluntary
effort over a self-determined 2-second period. They then maintain maximum effort for 5
additional seconds during which dynamometer was held stationary against the limb segment.
A rest period lasting 1 or 2 minutes was provided before a second (repeat) measure of an
action was taken. Peak force values were recorded for each trial from the digital readout on
the dynamometer. The test was repeated three times and an average measure was taken.
SUBJECT POSITION- Shoulder at neutral, elbow flexed at 900, Forearm supinated.
Dynamometer placement- elbow just proximal to styloid process. Stabilization of subject-
Superior aspect of shoulder or arm.
PAIN MEASUREMENT: The VAS consists of a 10-cm line with the two endpoints labeled
with verbal descriptors. The patient is required to place a mark on the 10 cm line at a point
that corresponds to the level of pain intensity he or she presently feels (Turk and Melzack
1992). VAS consists of a 10 cm line with descriptors at each end. At the left end there was
the number zero with the descriptor "no soreness at all", and at the right end there was the
number ten with the descriptor "soreness as bad as it could be". Each subject placed an x
dong a 10 cm line to describe the amount of muscle soreness he/she was presently
experiencing. Data was collected at baseline and at 96 hours.
The Outcome measurements Creatine Kinase (CK), Lactate Dehydrogenase (LDH), Pain
measurement, and Maximum Isometric voluntary contraction (MIVC) were taken at the
baseline before inducing DOMS, and taken at 24, 48, 72 and 96 hours after inducing delayed
onset muscle soreness (DOMS).

13
4. STATISTICAL ANALYSIS AND RESULTS
4.1 CREATINE KINASE (Normal level =60-180 I Units/Liter)
To find out the difference between the groups in each measure ONE WAY ANOVA is done.
CREATINE KINASE VALUES IN CONTROL AND IN 3 EXPERIMENTAL GROUPS
TAKEN AT DIFFERENT TIMES POST EXERCISE
Groups Baseline 24 hours 48 hours 72 hours 96 hours
Mean SD Mean SD Mean SD Mean SD Mean SD
Cryotherapy 86.38 23.33 276.55 66.21 606.50 156.18 921.48 222.80 1134.18 342.42
Phonoporesis 81.50 18.67 252.10 71.58 589.95 146.07 905.98 305.10 1043.70 430.79
Exercise 94.70 28.93 327.78 122.16 558.70 242.53 544.00 368.53 479.60 448.04
Control 86.80 21.05 313.08 80.07 661.00 147.65 1003.05 254.28 1244.65 414.39
Anova f
value
2.19 6.14 2.32 19.44 27.49
p value .091 NS
.001*** .077NS
.000*** .000***
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
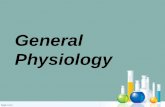
RESULTS: From the above table values, it is noted that at baseline and at 48 hours, there is
no significant difference seen in creatine kinase elevation between the four groups (p >0.05),
But significant difference were observed at 24 hours, and after 72 hours and 96 hours
(p<0.001)
PAIRED t TEST ANALYSIS: To find out the changes between baseline-24 hours, 24-48
hours, 48-72 hours, 72-96 hours for all the four groups paired t test was used.
CREATINE KINASE VALUES ANALYSIS WITHIN THE GROUPS AT DIFFERENT TIMES
CK measures Cryotherapy Phonoporesis
Mean SD
t value p value Mean SD t value p value
Baseline-24 hrs 190.17 67.20 17.89 .000*** 170.6 71.6 15.06 .000***
24-48 hrs 329.95 146.65 14.22 .000*** 337.85 121.20 17.62 .000***
48-72 hrs 314.97 157.74 12.62 .000*** 316.02 250.905 7.96 .000***
72-96 hrs 212.69 241.00 5.58 .000*** 137.72 259.74 3.35 .002**

14
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
RESULTS: In the above table it is observed that changes between baseline-24 hours, 24-48
hours, 48-72 hours, 72-96 hours for group 1 (Cryotherapy), group 2 (phonophoresis) and
group 4 (control) were showing significant difference statistically (p<0.001), where as in
group 3 (exercise) alone, the CK measures between baseline-24 hours and 24-48 hours were
having significant difference (p<0.001) but measures between 48-72 hours and 72-96 hours
were not showing significant difference statistically (p>0.05)
ONE WAY ANOVA RESULTS: To find out the significant difference of changes of
Creatine kinase measure from baseline- 24 hours, 24-48 hours, 48-72 hours, 72-96 hours
(within the period) between the groups, One-way ANOVA test was used.
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.005)
RESULTS: From the above table it is found that changes of creatine kinase measure from
baseline- 24 hours, 24-48 hours, 48-72 hours, 72-96 hours (within the period) between the
groups, were having statistical significant difference (p<0.001).
CK
measures
Exercise Control
Mean SD t value p value Mean SD t value p value
Baseline-
24 hrs
233.0 113.48 12.98 .000*** 226.27 79.48 18.00 .000***
24-48 hrs 230.92 175.24 8.33 .000*** 347.92 119.03 18.48 .000***
48-72 hrs 14.70 225.67 0.411 .683 NS
342.04 185.64 11.65 .000***
72-96 hrs 64.39 175.54 2.320 .026 NS
241.60 293.98 5.19 .000***
CK
measures
Cryotherapy Phonoporesis Exercise Control f
value
p value
Mean SD
Mean SD
Mean SD
Mean SD
0-24 hrs 190.17 67.20 170.6 71.6 233.0 113.48 226.27 79.48 4.88 .003**
24-48 hrs 329.95 146.65 337.85 121.20 230.92 175.24 347.92 119.03 5.82 .001***
48-72 hrs 314.97 157.74 316.02 250.90 14.70 225.67 342.04 185.64 26.68 .000***
72-96 hrs 212.69 241.00 137.72 259.74 64.39 175.54 241.60 293.98 12.54 .000***

15
CREATINE KINASE MEANS VALUES OF THE CONTROL AND 3 EXPERIMENTAL
GROUPS TAKEN AT DIFFERENT TIME MEASURES
4.2 LACTATE DEHYDROGENASE (Normal level = 220-400 I Units/Liter)
I.PAIRED t TEST ANALYSIS: To find out the changes between baseline-24 hours, 24-48
hours, 48-72 hours, 72-96 hours for all the four groups paired t test was used.
LACTATE DEHYDROGENASE VALUES ANALYSIS WITHIN THE GROUPS IN
DIFFERENT TIMES POST EXERCISE
LDH measures
Exercise Control
Mean SD t value p value Mean SD t value p value
Baseline-24 hrs 177.77 85.15 13.20 .000*** 210.67 85.14 15.64 .000***
24-48 hrs 97.89 90.79 6.81 .000*** 189.77 87.12 13.77 .000***
48-72 hrs 85.0 120.55 4.45 .000*** 122.14 94.92 8.13 .000***
72-96 hrs 87.19 77.26 7.13 .000*** 4.85 171.91 0.17 .859 NS

16
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
RESULTS: In the above table it is observed that changes between baseline-24 hours, 24-48
hours, 48-72 hours for all the four groups the LDH measures were showing significant
difference (p<0.001), but the changes between 72-96 hours also were showing significant
difference statistically only in group 3 (exercises), but in other 3 groups between 72-96 it was
not having significant difference (p>0.05).
II. ONE WAY ANOVA: To find out the difference between the groups in each measure one
way ANOVA is done.
LACTATE DEHYDROGENASE VALUES IN CONTROL AND IN 3 EXPERIMENTAL
GROUPS TAKEN AT DIFFERENT TIMES POST EXERCISE
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
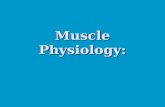
RESULTS: The above table shows that at baseline, 24hours, 48 hours,72 hours and at 96
hours the LDH values between the four groups were statistically having significant difference
(p<0.001).
LDH measures Cryotherapy Phonoporesis
Mean SD t value p value Mean SD
t value p value
Baseline-24 hrs 174.25 53.04 20.77 .000*** 171.62 74.15 14.63 .000***
24-48 hrs 200.79 100.96 12.57 .000*** 191.799 78.88 15.37 .000***
48-72 hrs 84.72 79.03 6.77 .000*** 87.12 130.03 4.23 .000***
72-96 hrs 14.32 121.28 0.74 .460NS
25.19 137.48 1.15 .253NS
Groups Baseline 24 hours 48 hours 72 hours 96 hours
Mean SD Mean SD Mean SD Mean SD Mean SD
Cryotherapy 256.35 35.77 430.6 56.56 631.4 122.35 716.12 126.09 730.45 171.23
Phonoporesis 288.5 28.53 460.12 75.99 651.92 94.22 739.05 131.17 713.85 207.03
Exercise 275.2 46.88 452.97 102.82 550.87 143.96 465.87 141.39 378.67 119.97
Control 288.6 35.85 499.35 89.05 689.12 118.39 811.27 136.77 806.42 249.70
ANOVA f
value
6.67 4.77 9.31 50.38 38.82
p value .000*** .003** .000***
.000*** .000***

17
III.ONE WAY ANOVA: To find out the significant difference of changes of lactate
dehydrogenase measure from baseline- 24 hours, 24-48 hours, 48-72 hours, 72-96 hours
(within the period) between the groups, One-way Anova test was used.
LDH
measures
Cryotherapy
Phonoporesis Exercise Control f value p value
Mean SD
Mean SD Mean
SD
Mean SD
Baseline-
24 hrs
174.25 53.04 171.62 74.15 177.77 85.15 210.67 85.14 2.33 .076Ns
24-48 hrs 200.79 100.96 191.799 78.88 97.89 90.79 189.77 87.12 11.59 .000***
48-72 hrs 84.72 79.03 87.12 130.03 85.0 120.55 122.14 94.92 29.68 .000***
72-96 hrs 14.32 121.28 25.19 137.48 87.19 77.26 4.85 171.91 4.48 .005**
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
RESULTS: One way ANOVA results shows that the LDH changes between the four groups
were found to have significant difference statistically at 24-48 hours, 48-72 hours and at 72-
96 hours.
LACTATE DEHYDROGENASE MEAN VALUES OF THE CONTROL AND 3
EXPERIMENTAL GROUPS TAKEN AT DIFFERENT TIME MEASURES

18
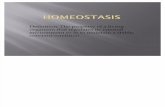
4.3. Maximum Isometric Voluntary Contraction(MIVC):
MIVC MEAN VALUES OF THE CONTROL AND 3 EXPERIMENTAL GROUPS TAKEN
AT DIFFERENT TIME MEASURES

19
4.4 REPEATED MEASURES ANOVA RESULTS:
To find out the overall changes within the group Repeated ANOVA was adopted.
REPEATED MEASURES ANOVA FOR DEPENDENT VARIABLES CK, LDH AND MIVC
BY GROUP AND TIME
Groups Creatine Kinase IU/L (CK) Lactate dehydrogenase IU/L
(LDH)
Maximum Isometric
Voluntary contraction
(MIVC) lbs
Repeated
measures
ANOVA f value
P value Repeated
measures
ANOVA f value
P value Repeated
measures
ANOVA f value
P value
Cryotherapy 844.63 0.000*** 1947.39 0.000*** 1531.01 0.000***
Phonophoresis 512.93 0.000*** 2333.43 0.000*** 1790.19 0.000***
Exercise 136.23 0.000*** 840.49 0.000*** 2226.80 0.000***
Control 759.53 0.000*** 1599.87 0.000*** 2600.80 0.000***
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.005)
RESULTS: Repeated measures ANOVA results shows that the CK, LDH and MIVC
measures overall changes within the groups for all the four groups were found to have
difference statistically significant (p<0.001)
4.5 Pain Score: To find out the difference between the groups in each measure one way
ANOVA is done.
PAIN VAS SCORES FOR FOUR GROUPS TAKEN AT PRE AND POST
TREATMENT LEVELS
Groups 24 hours 96 hours
Mean SD Mean SD
Cryotherapy 5.08 0.512 2.90 0.49
Phonoporesis 5.12 0.51 1.145 0.258
Exercise 5.07 0.52 1.94 0.33
Control 5.13 0.62 2.915 0.459
Anova f value 0.110 183.4
p value . 954NS .000***

20
The above table shows that pain scores at 24 hours between the groups were not found to
have significant difference (p>0.05) but at 96 hours the pain scores were showing statistically
significant difference (p<0.001).
To find out the significant difference of changes of Pain measure from 24-96
hours (within the period) between the groups, One-way ANOVA test was used.
Note: *p<0.05, **p<0.01, ***p<0.001, NS- Not significant (p>0.05)
The differences of change in pain measure from 24-96 hours between the groups were found
to be statistically significant in between the four groups (p<0.001)
5. DISCUSSION:
The onset of muscle pain in all the four groups occurred within the first 24 hours
following the eccentric exercise protocol, which is consistent with other studies, investigated
the onset of DOMS resulting from exercise-induced muscle damage. (Nosaka, 1995)
In the present study, three different Physiotherapy modalities were compared to
facilitate the recovery of DOMS. In the present study, we found that electrotherapy
modalities Cryotherapy and Phonophoresis do not have direct influence on reducing the
biochemical markers like Creatine kinase (CK) and Lactate Dehydrogenase (LDH). However
the modalities are useful in reducing the pain. When we compared the maximum isometric
voluntary contraction (MIVC), Ultrasound is found to be better in improving the muscle
Pain
measures
Cryotherapy
Phonoporesis Exercise Control
f value
p value
Mean SD
Mean SD
Mean SD
Mean SD
24-96
hours.
2.18 0.41 3.98 0.55 3.13 0.38 2.21 0.50 133.19 .000***

21
contraction at 72 hours as compared to cryotherapy. The probable reason may be pain gate
mechanism and anti-inflammatory action of Ultrasound is better than cryotherapy.
In the present study, we compared exercises and electro modalities; exercise
is effective in all the four parameters-CK, LDH, MIVC and pain. The probable reason may be
breakup of adhesions from the injured, sore muscles takes place during exercise. Increased
blood flow or temperature in the muscle helps to decrease the accumulation of noxious waste
products. Endorphin release by neurons in the central nervous system increases during
exercise. Increased afferent input is noted from large, low-threshold sensory units in the
muscles (muscle group-Ia, Ib, and II fibers [gate control theory]). The training effect appears
to be highly specific, not only for the particular muscles involved in the exercise, but also for
the type of contractions performed. For example, Schwane and Armstrong (1983) found that
in rats, the muscle damage that occurs during downhill running is prevented by downhill or
level training but not by uphill training. The eccentric protocol causes more DOMS and rise
in the plasma CK and LDH activity. Subjective enzymatic values (CK & LDH) remained
elevated for at least 4 days after exercise induced muscle damage in group1 (cryotherapy),
group 2 (phonophoresis) and in group 4 (control), but in group 3 (exercises), the values
remained elevated for 2 days only, than the values start to decrease at 72 hours and the values
were reaching near to the baseline values in day 4. Maximum Isometric voluntary contraction
(MIVC) scores were found to be decreasing until 48 hours in all the groups, But however in
group 3 (Exercises), the scores started to increase after 48 hours and in group 2
(Phonophoresis) the scores started to increase after 72 hours. In group 1 (Cryotherapy) and
Group 4 (Control) the MIVC scores were not much improving even till 96 hours. Therefore
we strongly recommend that exercises can be advised for the early recovery of DOMS in
recreational athletes to facilitate their early participation.
6. CONCLUSION:
In conclusion, the eccentric protocol causes more muscle soreness and rise in the plasma
CK and LDH activity. Subjective enzymatic values remained elevated for at least 4 days after
exercise induced muscle damage in group1 ( cryotherapy), group 2 ( phonophoresis ) and in
group 4 ( control), but in group 3 ( exercises), the values remained elevated for 2 days only,
than the values reached near to the baseline values in day 4. But in the variables MIVC and
VAS scores, both phonophoresis (group 2) and exercises (group 3) were found to be effective
when compared to cryotherapy (group 1) and control groups.

22
7. REFERENCES:
Armstrong, R. B. (1984). Mechanisms of exercise-induced delayed onset muscular soreness:
a brief review- Medicine and Science in Sports and Exercise 16(6): 529-538.
Arnheim DD. Modern Principles of Athletic Training. 7th ed. St Louis, MO: Times
Mirror/Mosby; 1989:198-231.
Barlas P, Robinson J, Allen J, et al. Lack of effect of acupuncture upon signs and symptoms
of delayed onset muscle soreness [In Process Citation]. Clin Physiol. Nov 2000; 20(6):449-
56.
Cannavino CR, Abrams J, Palinkas LA, et al. Efficacy of transdermal ketoprofen for delayed
onset muscle soreness. Clin J Sport Med. Jul 2003; 13(4):200-8.
Clarkson PM, Hubal MJ. Exercise-induced muscle damage in humans. Am J Phys Med
Rehabil. 2002 Nov; 81(11):S52-S69.
Cobb CR, deVries HA, Urban RT, et al. Electrical activity in muscle pain. Am J Phys
Med. Apr 1975; 54(2):80-87.
Connolly DA, Lauzon C, Agnew J, et al. The effects of vitamin C supplementation on
symptoms of delayed onset muscle soreness. J Sports Med Phys Fitness. Sep 2006;
46(3):462-7.
Craig JA, Barron J, Walsh DM, et al. Lack of effect of combined low intensity laser
therapy/phototherapy (CLILT) on delayed onset muscle soreness in humans. Lasers Surg
Med. 1999; 24(3):223-30.
Davis WJ, Wood DT, Andrews RG, et al. Elimination of delayed-onset muscle soreness by
pre-resistance cardio acceleration before each set. J Strength Cond Res. Jan 2008; 22(1):212-
25.
Friden, j, sjostrom, m. & ekblom, b. (1981). A Morphological study of delayed muscle
soreness. Experientia 37, 506–507.
Friden, j., seger, j., sjostrom, m. & ekblom, b. (1983). Adaptive response in human skeletal
muscle subjected to prolonged eccentric training. International Journal of Sports Medicine 4,
177–183.

23
Hedayatpour N, Falla D, Arendt-Nielsen L, et al. Sensory and electromyography mapping
during delayed-onset muscle soreness. Med Sci Sports Exerc. Feb 2008; 40(2):326-334.
Hough.T. (1902). Ergographic studies in muscular soreness. American Journal of Physiology
7, 76–92.
Johansson PH, Lindstrom L, Sundelin G, et al. The effects of preexercise stretching on
muscular soreness, tenderness and force loss following heavy eccentric exercise. Scand J
Med Sci Sports. Aug 1999; 9(4):219-25.
McAnulty S, McAnulty L, Nieman D, et al. Effect of NSAID on muscle injury and oxidative
stress. Int J Sports Med. Nov 2007; 28(11):909-15.
Mekjavic IB, Exner JA, Tesch PA, et al. Hyperbaric oxygen therapy does not affect recovery
from delayed onset muscle soreness. Med Sci Sports Exerc. Mar 2000; 32(3):558-63.
Smith LL. Acute inflammation: the underlying mechanism in delayed onset muscle soreness?
Med Sci Sports Exerc. 1991; 23:542-551.
Tidball, 3. G. (1995). Inflammatory ce11 response to acute muscle injury. Medicine and
Science in Sports and Exercise 27: 1022-1032.
Warren GL, Ingalls CP, Lowe DA, Armstrong RB. Excitation-contraction uncoupling: major
role in contraction-induced muscle injury. Exercise and Sport Sciences Reviews. 2001;
29:82–87.
Weber, M. D., F, J. Servedio, et al. (1994). The effects of three modalities on delayed onset
muscle soreness. The Journal of Orthopaedic and Sports Physical Therapy 20(5): 236-242.
LIST OF PUBLICATIONS:
1. Role of Physiotherapy in Ameliorating the Delayed Onset Muscle Soreness (DOMS)
and Influence on Biochemical Markers of Recreational Athletes. The Journal of
Indian Physiotherapists April 2010 Volume 4, Issue 1: 20-28.