Methadone Pain Management: Physician's guidelines Ontario Canada
Upload
physicians-weeklyCategory
view
223download
0description
updatesCardiology
Surviving Heart Failure
High BP & CKd
& PadWomen
www.physweekly.com/cardio

2
don’t Miss another issue
Visit www.physweekly.com/register
Sign Up for our eNewsletterToday
visit www.physiciansweekly.com 3
Director, Business Dev. dave dempsey Mark elms dennis turner
Project Manager diana Marganski
Director of Finance tom Campbell
Sales
President Clay Romweber
VP, Product Marketing & Development tom Richards
VP, Operations & Infrastructure derek Mirdala
Management
Editorial Director Keith d’Oria
Senior Editor Janine anthes
Associate Editor Chris Cole
Creative Director Jonathan Nichol
Associate Art Director timothy Hodges
Interactive Marketing Spc sally Ladd
Production Director George Camba
Production Specialist Lacey archer
Administrative Assistant erika Kaufman
Editorial
Vice President denise Halverson
Project Administrator Lauri Hutchinson
Mngr Hospital Relations Jacquie Jacovino
Institutional Relations amy Johnson Michelle McKenna sadie steib Judy Wengryn
Customer Service
Table of Contents
a Message From the Editor
Physician’s Weekly is proud to present this monograph with feature stories on several important topics in cardiology. In recent months, we have published a variety of news articles covering this disease state. Focusing on clinical and evidence-based information, the content in these features relies on the expertise of our contributing physician authors. Physician’s Weekly will continue to feature cardiology news in the coming months. In the meantime, we hope you find this information useful in your practice. Feel free to give us feedback and opinions by emailing me at [email protected].
sincerely,
Keith d’Oria Editorial Director, Physician’s Weekly
4
a New guideline for Treating Hypertriglyceridemia — Lars Berglund MD, PhD
12
Calculating risk for CVd — Matthew C. Tattersall, DO
8
improving Survival after Heart Failure — Gregg C. Fonarow, MD
16
Women & Pad: a Call to action — Alan T. Hirsch, MD
20
Blood Pressure & End-Stage renal disease in Patients With CKd — Carmen A. Peralta, MD, MAS
Physician’s Weekly™ (ISSN 1047-3793) is published by Physician’s Weekly, LLC, a division of M/C Holding Corp. The service is free for qualifying institutions. Please contact us at [email protected] for more information. Offices: Physician’s Weekly, LLC, 5 Commerce Way, Suite 202, Hamilton, NJ 08691; and 180 Mount Airy Road, Suite 102, Basking Ridge, NJ 07920. Reproduction without written permission from the publisher is prohibited. Copyright 2012, Physician’s Weekly, LLC.
Publication of an advertisement or other product mention in Physician’s Weekly should not be construed as an endorsement of the product or the manufacturer’s claims. The appearance of or reference to any person or entity in this publication (including images) does not constitute an expressed or implied endorsement of the product mentioned. The reader is advised to consult appropriate medical literature and the product information currently provided by the manufacturer of each drug to verify indications, dosage, method, duration of administration, and contraindications. All editorial is developed independent of influence from advertising brands/companies.

4
H ypertriglyceridemia can substantially increase the likelihood of patients developing heart disease when compared with those who
have normal triglyceride levels. While treatment strategies for this condition are well established, its causes differ from patient to patient, as do the risks they pose to each individual. Clinical practice guidelines from the endocrine society on hypertriglyceridemia were published in the september 2012 Journal of Clinical Endocrinology & Metabolism. They recommend that more attention be paid to how personal history, physiology, and lifestyle interact to affect risk.
“In recent years, much of the focus surrounding lipids has concentrated on cholesterol,” explains Lars Berglund, Md, phd, who chaired the endocrine society task force that developed the most recent guidelines. “although there are evidence–based guidelines from respected medical associations that address lipids, data on the complex role of triglycerides in heart disease continue to accumulate. Considering this recent emergence of data on triglycerides, it was important to have a guideline that specifically discusses this component of heart disease care.”
a New guideline for Treating Hypertriglyceridemia The Endocrine Society has released a clinical practice guideline on hypertriglyceridemia that stresses the importance of individualizing treatments based on patient factors.
lars Berglund Md, PhdProfessor of MedicineSenior Associate Dean for ResearchDirector, Clinical and Translational Science Center
University of California, Davis Health System
visit www.physiciansweekly.com 5
Taking an individualized approachdr. Berglund stresses that clinicians should not view elevated fasting triglyceride levels as a standalone factor. “triglycerides should be looked at in the context of other risk factors for cardiovascular disease (CVd) and metabolic dis-ease,” he says. “assessment should include the evalu-ation of secondary causes of hyperlipidemia, includ-ing endocrine conditions and medications [table 1]. Central obesity, hypertension, abnormalities of glucose metabolism, liver dysfunction, and family history of dyslipidemia and CVd should be assessed.” For example, patients
a New guideline for Treating Hypertriglyceridemia
6
with triglyceride levels in the moderate range— 200 mg/dl to 999 mg/dl—may have changes in HdL and LdL cholesterol levels and properties, which are associated with cardiovascular risk, but insulin resistance and other factors should also be considered during patient management. patients with isolated hypertriglyceridemia (eg, familial type) are more likely to have larger particles, which are less likely to cause cardiovascular risk.
Fatty foods, smoking, and poor exercise also contribute to the risk for high triglyceride levels. “simple carbohydrates that can be broken down and absorbed quickly, such as sugar-sweetened beverages, white rice, and white bread, contribute to an increase in fat formation and triglyceride levels,” says dr. Berglund. While alcohol can increase HdL cholesterol levels, it can also lead to high triglyceride levels. Certain prescription medications (eg, bile acid sequestrants for high LdL) can also interact to raise blood triglyceride levels. “understanding the importance of specific risk factors requires that clinicians ascertain a full profile of each patient,” dr. Berglund adds.
Considering Treatment options defining the level of hypertriglyceridemia for indi-vidual patients is crucial to determining the goal of treatment and should be based on fasting levels. The endocrine society guidelines define normal triglyceride levels as less than 150 mg/dl (table 2). Mild and moderate hypertriglyceridemia are catego-rized by levels below 999 mg/dl, which are primarily associated with a risk for CVd. When levels rise above 1,000 mg/dl, patients should be categorized as having severe and very severe hypertriglyceride-mia. The risk for these individuals is associated more often with pancreatitis.
Because weight, diet, and exercise play particularly important roles in triglyceride levels, the endocrine society guidelines recommend that initial treatment for mild-to-moderate hypertriglyceridemia be lifestyle therapy, consisting of dietary counseling, physical activity, and a weight reduction program for overweight and obese patients. “Overweight or obese patients may feel overwhelmed when asked to lose weight,” dr. Berglund says, “but clinicians should reassure them that even modest reductions in weight can have highly beneficial effects on their triglyceride levels.”
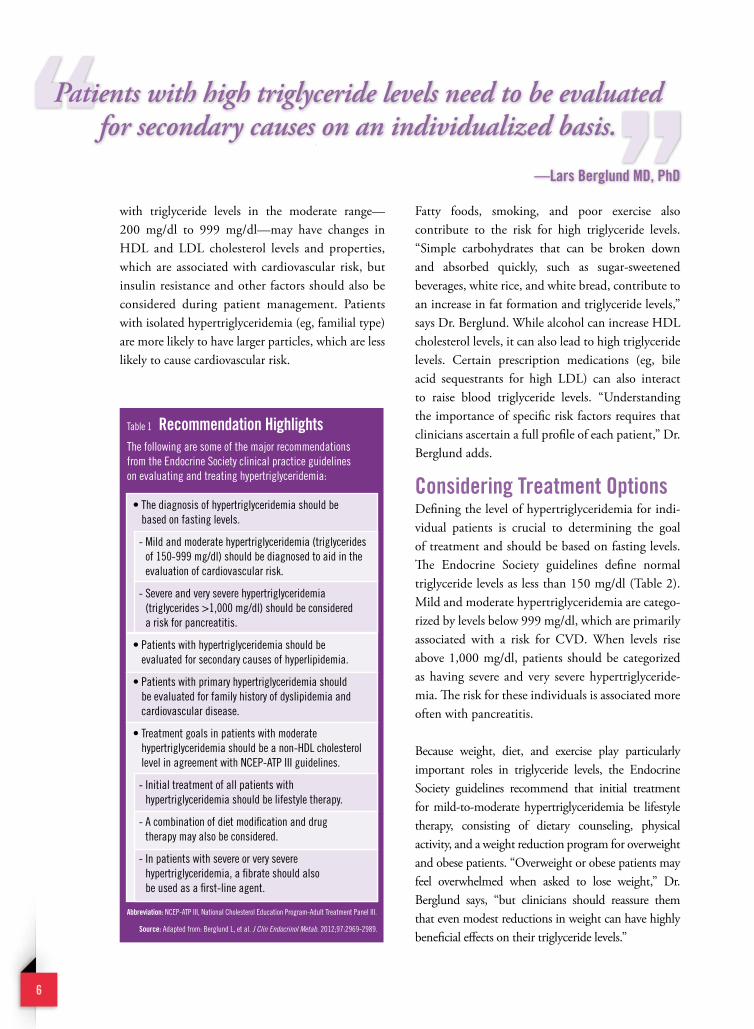
Table 1 recommendation HighlightsThe following are some of the major recommendations from the Endocrine Society clinical practice guidelines on evaluating and treating hypertriglyceridemia:
• The diagnosis of hypertriglyceridemia should be based on fasting levels.
- Mild and moderate hypertriglyceridemia (triglycerides of 150-999 mg/dl) should be diagnosed to aid in the evaluation of cardiovascular risk.
- Severe and very severe hypertriglyceridemia (triglycerides >1,000 mg/dl) should be considered a risk for pancreatitis.
• Patients with hypertriglyceridemia should be evaluated for secondary causes of hyperlipidemia.
• Patients with primary hypertriglyceridemia should be evaluated for family history of dyslipidemia and cardiovascular disease.
• Treatment goals in patients with moderate hypertriglyceridemia should be a non-HDL cholesterol level in agreement with NCEP-ATP III guidelines.
- Initial treatment of all patients with hypertriglyceridemia should be lifestyle therapy.
- A combination of diet modification and drug therapy may also be considered.
- In patients with severe or very severe hypertriglyceridemia, a fibrate should also be used as a first-line agent.
abbreviation: NCEP-ATP III, National Cholesterol Education Program-Adult Treatment Panel III.
Source: Adapted from: Berglund L, et al. J Clin Endocrinol Metab. 2012;97:2969-2989.
Patients with high triglyceride levels need to be evaluated for secondary causes on an individualized basis.
—lars Berglund Md, Phd

visit www.physiciansweekly.com 7
For patients at risk for triglyceride-induced pan-creatitis and for whom lifestyle changes have been ineffective, the guideline recommends that fibrates be the first line of drug treatment. although statins have some triglyceride-lowering effects, they are not overly effective in patients with very high lev-els, according to dr. Berglund. The guideline rec-ommends that statins not be used as monotherapy for severe or very severe hypertriglyceridemia, but that they may be useful for moderate hyper-triglyceridemia when indicated to modify cardio-vascular risk. Fibrates, niacin, and n-3 fatty acids
are recommended for use alone or in combination with statins in patients with moderate-to-severe triglyceride levels.
“The key take-home message for all clinicians is that patients with high triglyceride levels need to be evaluated for secondary causes on an individualized basis,” says dr. Berglund. “Only then can we determine the causes and direct our focus of treatment. The endocrine society guidelines can serve as a helpful aid for physicians as they manage patients from diagnosis to treatment.”
Lars Berglund, MD, PhD, has indicated to physician’s Weekly that he has served as a consultant for Merck and Danone and received grants/research aid from the NIH. He is also a shareholder of Pfizer and Novo Nordisk.
readings & resources
Berglund l, Brunzell J, goldberg a, et al. Evaluation and treatment of hypertriglyceridemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97:2969-2989.
Ford E, li C, Zhao g, et al. Hypertriglyceridemia and its pharmacologic treatment among US adults. Arch Intern Med. 2009;169:572-578.
di angelantonion E, Sarwar N, Perry P, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993-2000.
Muller-riemenschneider F, Nocon M, Willich S. Prevalence of modifiable cardiovascular risk factors in German adolescents. Eur J Cardiovasc Prev Rehabil. 2010;17:204-210.
Mora S, rifai N, Buring J, ridker P. Fasting compared with nonfasting lipids and apolipoproteins for predicting incident cardiovascular events. Circulation. 2008;118:993-1001.
* These criteria focus on the ability to assess risk for premature cardiovascular disease (CVD) versus risk for pancreatitis. The designations of mild and moderate hypertriglyceridemia correspond to the range of levels predominant in risk assessment for premature CVD. This range includes the vast majority of subjects with hypertriglyceridemia. Severe hypertriglyceridemia carries a susceptibility for intermittent increases in levels >2,000 mg/dl and subsequent risk of pancreatitis; very severe hypertriglyceridemia is indicative of risk for pancreatitis. In addition, these levels suggest different etiologies. Presence of mild or moderate hypertriglyceridemia is commonly due to a dominant underlying cause in each patient, whereas severe or very severe hypertriglyceridemia is more likely due to several contributing factors.
Source: Adapted from: Berglund L, et al. J Clin Endocrinol Metab. 2012;97:2969-2989.abbreviation: NCEP-ATP III, National Cholesterol Education Program-Adult Treatment Panel III.
NCEP-aTP iii Endocrine Society*
<150 mg/dl
150-199 mg/dl
200-999 mg/dl
1,000-1,999 mg/dl
≥2,000 mg/dl
Normal
Borderline-high triglycerides
High triglycerides
Very severe hypertriglyceridemia
<150 mg/dl
150-199 mg/dl
200-499 mg/dl
≥500mg/dl
Normal
Mild hypertriglyceridemia
Moderate hypertriglyceridemia
Severe hypertriglyceridemia
Very severe hypertriglyceridemia
Table 2 Proposed Criteria for diagnosing Elevated Triglyceride levels Under Fasting Conditions

8
H eart failure (HF) is among the leading causes of hospitalization in the united states, afflicting more than 5.8 million men and women each
year. The disease has been associated with substantial morbidity, mortality, and healthcare expenditures. The 5-year mortality rate for HF has been estimated at more than 50%, and roughly $40 billion is spent annually in costs related to HF.
previous studies have shown that there are gaps, variation, and disparities in the use of evidence-based, guideline-recommended therapies for HF. Regardless of the clinical setting, many eligible HF patients do not receive one or more of the therapies that have been proven to be effective in reducing all-cause mortality in clinical trials and analyses. Non-adherence to recommended HF therapies can significantly reduce quality of life and lifespan in sufferers with the disease.
Examining Benefits of Proven HF Therapiesa study published in the February 21, 2012 Journal of the American Heart Association: Cardiovascular
gregg C. Fonarow, MdEliot Corday Professor of Cardiovascular
Medicine and ScienceDavid Geffen School of Medicine Ronald Reagan UCLA Medical CenterDirector Ahmanson–UCLA Cardiomyopathy Center

visit www.physiciansweekly.com 9
New data show that a combination of several key guideline-recommended therapies for heart failure treatment can improve the odds of survival by up to 90% over 2 years.
improving Survivalafter Heart Failure
and Cerebrovascular Diseases evaluated the indi vidual and incremental benefits of guideline-recommended therapies. “While certain therapies are recommended for HF patients in national guidelines from the american College of Cardiology and the american Heart association, our study was the first to examine the specific incremental contribution of each of these therapies in improving survival when combined in a real-world clinical practice,” says Gregg C. Fonarow, Md, who was the lead author on the investigation.
The study by dr. Fonarow and colleagues utilized a nested case-control design that included HF patients who were enrolled in the Registry to Improve the use of evidence-Based Heart Failure Therapies in the Outpatient setting (IMpROVe HF) cohort. The
analysis involved 1,376 patients who died within 24 months; 2,752 patients who survived to 24 months were included in the control group. The key guideline-recommended therapies evaluated were:
• Three types of HF medications: β-blockers, aldosterone antagonists, and aCe inhibitors or angiotensin receptor blockers.
• Cardiac resynchronization therapy (CRt).
• anticoagulant therapy for atrial fibrillation.
• Implantable cardioverter-defibrillators (ICds).
• HF patient education.
each individual guideline-recommended therapy

10
for HF analyzed in the study was associated with an important survival benefit, with the lone exception being use of aldosterone antagonists (table 1). The greatest individual benefits were observed with the use of β-blockers and CRt. use of β-blockers reduced the odds of HF mortality by 58% over 24 months, while CRt use was linked to a 56% reduction in the odds of HF mortality over 24 months.
The finding on aldosterone antagonist use contra-dicted the results of multiple randomized clinical trials that demonstrated efficacy and an association with lower mortality risk. according to dr. Fonarow, this finding may have resulted from confounding
by indication or other forms of observational bias. alternatively, aldosterone antagonist use may be less effective or less safe as dosed and monitored in actual clinical practice. “More studies of the clinical effec-tiveness of aldosterone antagonists in HF are needed,” dr. Fonarow says. “Nevertheless, eligible HF patients should continue to be treated with this evidence-based, guideline-recommended therapy.”
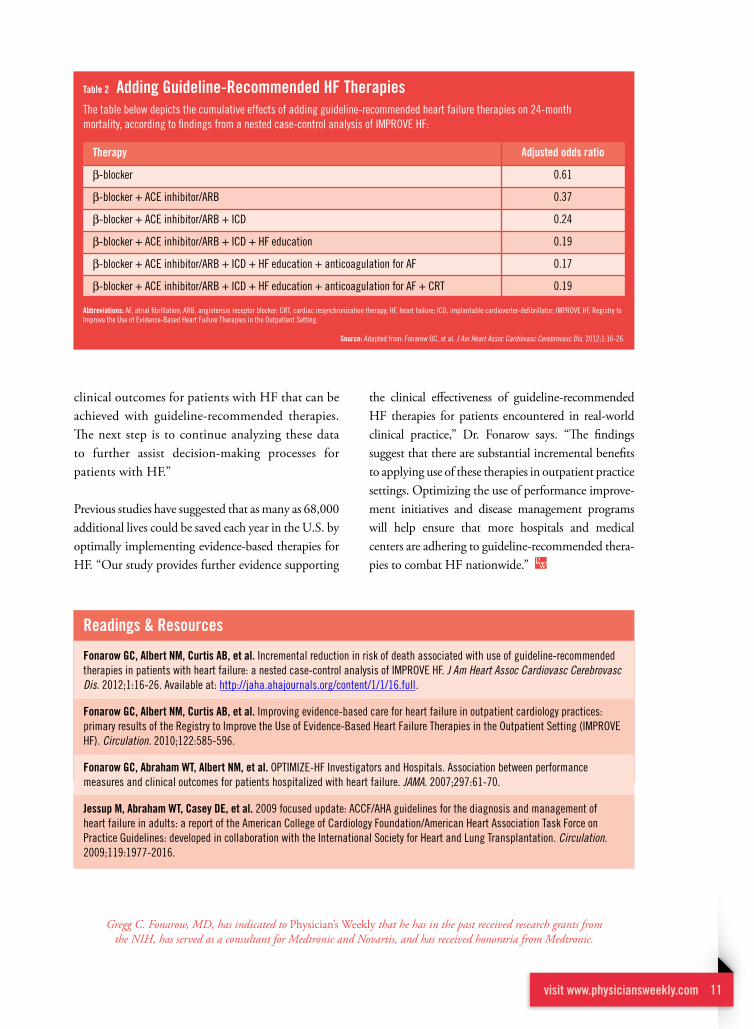
incremental improvements Matteras each guideline-recommended therapy for HF was added in the study, the overall survival rate increased incrementally. When compared with no treatment at all, up to a 90% reduction in mortality rate was observed in 24 months of observation (table 2). “This is a remarkable improvement in clinical outcome for patients with HF and reduced ejection fraction,” says dr. Fonarow.
It should be noted that the study revealed that there appeared to be a plateau in survival benefit after any four or five guideline-recommended HF therapies were applied. “This may be the result of relatively few patients qualifying for and being treated with all seven of the guideline-recommended therapies we analyzed in the study,” explains dr. Fonarow. “This potential plateau will require further confirmation in future studies.”
looking into the FutureHigh-quality, patient-centered outcomes research is a national priority, dr. Fonarow says, and may better inform clinical decision-making in patients with HF. “Our study provides patients, clinicians, purchasers, and policymakers with compelling evidence of the incremental improvements in
There are substantial incremental benefits to applying use of these therapies in outpatient practice settings.
— gregg C. Fonarow, Md
Table 1 guideline-recommended Therapies for HF & MortalityThe table below depicts the association between treatment with guideline therapies at baseline and mortality at 24 months, according to findings from a nested case-control analysis of IMPROVE HF:
guideline-recommended therapy
ACE inhibitor/angiotensin receptor blocker
β-blocker
Aldosterone antagonists
Anticoagulation for atrial fibrillation
Implantable cardioverter-defibrillators
Cardiac resynchronization therapy
Heart failure education
abbreviations: HF, heart failure; IMPROVE HF, Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting.
Source: Adapted from: Fonarow GC, et al. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. 2012;1:16-26.
adjusted odds ratio
0.56
0.42
1.05
0.73
0.62
0.44
0.73
visit www.physiciansweekly.com 11
clinical outcomes for patients with HF that can be achieved with guideline-recommended therapies. The next step is to continue analyzing these data to further assist decision-making processes for patients with HF.”
previous studies have suggested that as many as 68,000 additional lives could be saved each year in the u.s. by optimally implementing evidence-based therapies for HF. “Our study provides further evidence supporting
the clinical effectiveness of guideline-recommended HF therapies for patients encountered in real-world clinical practice,” dr. Fonarow says. “The findings suggest that there are substantial incremental benefits to applying use of these therapies in outpatient practice settings. Optimizing the use of performance improve-ment initiatives and disease management programs will help ensure that more hospitals and medical centers are adhering to guideline-recommended thera-pies to combat HF nationwide.”
Gregg C. Fonarow, MD, has indicated to physician’s Weekly that he has in the past received research grants from the NIH, has served as a consultant for Medtronic and Novartis, and has received honoraria from Medtronic.
Table 2 adding guideline-recommended HF TherapiesThe table below depicts the cumulative effects of adding guideline-recommended heart failure therapies on 24-month mortality, according to findings from a nested case-control analysis of IMPROVE HF:
Therapy
β-blocker
β-blocker + ACE inhibitor/ARB
β-blocker + ACE inhibitor/ARB + ICD
β-blocker + ACE inhibitor/ARB + ICD + HF education
β-blocker + ACE inhibitor/ARB + ICD + HF education + anticoagulation for AF
β-blocker + ACE inhibitor/ARB + ICD + HF education + anticoagulation for AF + CRT
abbreviations: AF, atrial fibrillation; ARB, angiotensin receptor blocker; CRT, cardiac resynchronization therapy; HF, heart failure; ICD, implantable cardioverter-defibrillator; IMPROVE HF, Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting.
Source: Adapted from: Fonarow GC, et al. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. 2012;1:16-26.
adjusted odds ratio
0.61
0.37
0.24
0.19
0.17
0.19
Fonarow gC, albert NM, Curtis aB, et al. Incremental reduction in risk of death associated with use of guideline-recommended therapies in patients with heart failure: a nested case-control analysis of IMPROVE HF. J Am Heart Assoc Cardiovasc Cerebrovasc Dis. 2012;1:16-26. Available at: http://jaha.ahajournals.org/content/1/1/16.full .
Fonarow gC, albert NM, Curtis aB, et al. Improving evidence-based care for heart failure in outpatient cardiology practices: primary results of the Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVE HF). Circulation. 2010;122:585-596.
Fonarow gC, abraham WT, albert NM, et al. OPTIMIZE-HF Investigators and Hospitals. Association between performance measures and clinical outcomes for patients hospitalized with heart failure. JAMA. 2007;297:61-70.
Jessup M, abraham WT, Casey dE, et al. 2009 focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:1977-2016.
readings & resources

12
Calculating risk for CVd
Clinicians deciding on which risk model to use should be aware that the Framingham CVD risk score will likely increase the number of
people who qualify as moderate and high risk.
in guidelines on primary prevention of cardiovas-cular disease (CVd), the Framingham coronary heart disease (CHd) risk score has long been
recommended for assessing 10-year risk of myo-cardial infarction (MI) or cardiac death. In 2008, the Framingham group developed the Framingham CVd risk score, which added new endpoints of angina, cerebrovascular disease, peripheral vascular disease, and heart failure to the CHd risk score. The Framingham CVd risk score has since been adopted and favored by the latest guidelines for cardiovascu-lar risk assessment.
Significant implications on CVd riskLittle is known about the population level effects of switching from the Framingham CHd risk score to the Framingham CVd risk score. In the May/June 2011 Journal of Clinical Lipidology, my col-leagues and I conducted a study to determine the impact of switching to the Framingham CVd risk score from the Framingham CHd risk score on the united states population. For our study, 1,020 patients from NHaNes were analyzed to define the changes in risk category distribution and corre-sponding changes to lipid goal achievements. When the Framingham CVd risk score was used, 63% of men and 74% of women moved up by at least one risk category when compared with the Framingham CHd risk score. additionally, the low-risk popula-tion decreased from 52% to 16%, and the high-risk population increased from 4% to 20%.
Significant implications on CVd risk
Matthew C. Tattersall, doCardiovascular Medicine FellowDivision of Cardiovascular MedicineDepartment of Medicine
University of Wisconsin School of Medicine and Public Health

visit www.physiciansweekly.com 13
In February 2011, the american Heart association released recommendations on CVd prevention in women. It modified 10-year risk thresholds and rec-ommended using the Framingham CVd risk model for routine risk assessment. In the updated guidelines, the “high-risk” threshold for a woman’s 10-year cardiovascular risk was lowered from 20% to 10%. When we used the updated thresholds and applied the Framingham CVd risk score—as opposed to the Framingham CHd risk score—we found that 44% of women aged 55 to 74 with no prior cardiac disease would now be classified as high risk for CVd.
Treatment implications for CVdWhen subjects in NHaNes were reclassified based on the Framingham CVd risk score, about 30% of those previously meeting lipid goals by the Framingham CHd risk score no longer met lipid goals. This means that pharmacotherapy would likely need to be initi-ated or intensified for many more patients. published research has consistently documented that statin ther-apies can reduce CHd mortality, the endpoint of the
Framingham CHd, by 25% to 30%. The effects of statins on lowering the risks associated with the other endpoints—stroke, peripheral vascular disease, and heart failure—included in the Framingham CVd risk score are not as clear. More data are needed to assess the potential benefits of therapies for patients based on the additional components that are accounted for in the Framingham CVd risk score.
increase awareness of CVd ModelIt’s important to note that the Framingham CVd risk score is a valuable tool in the fight against heart disease. Current primary prevention guidelines recommend routine assessment of cardiovascular risk using a mul-tivariate risk model. Clinicians deciding on which risk model to use should be aware that the Framingham CVd risk score will likely increase the number of people who qualify as moderate and high risk. The treatment effects of statin therapy, while known to reduce cardiac death and MI, have less certain and differing treatment effects on other endpoints.
Matthew C. Tattersall, DO, has indicated to physician’s Weekly that he has no financial disclosures to report.
Little is known about the effect of switching from the Framingham CHD risk score to the Framingham CVD risk score.
readings & resources
Tattersall M, Karmali K, gangnon r, Keevil J. The population effects of the global cardiovascular risk model in United States adults: findings from the National Health and Nutrition Surveys 2005-2006. J Clin Lipidol. 2011;5:166-172.
Mosca l, Benjamin E, Berra K, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women— 2011 update: a guideline from the American Heart Association. Circulation. 2011;123:1243-1262.
Unverzagt F, McClure l, Wadley V, et al. Vascular risk factors and cognitive impairment in a stroke-free cohort. Neurology. 2011;77:1729-1736.
defilippis a, Blaha M, Ndumele C, et al. The association of Framingham and Reynolds risk scores with incidence and progression of coronary artery calcification in MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol. 2011;58:2076-2083.
yoshida M, Mita T, yamamoto r, et al. The combination of Framingham risk score and carotid intima-media thickness improves the prediction of cardiovascular events in patients with type 2 diabetes. Diabetes Care. 2011;35:178-180.

14
about 8 million people in the united states have peripheral artery disease (pad), a condition that, if left untreated, increases heart attack
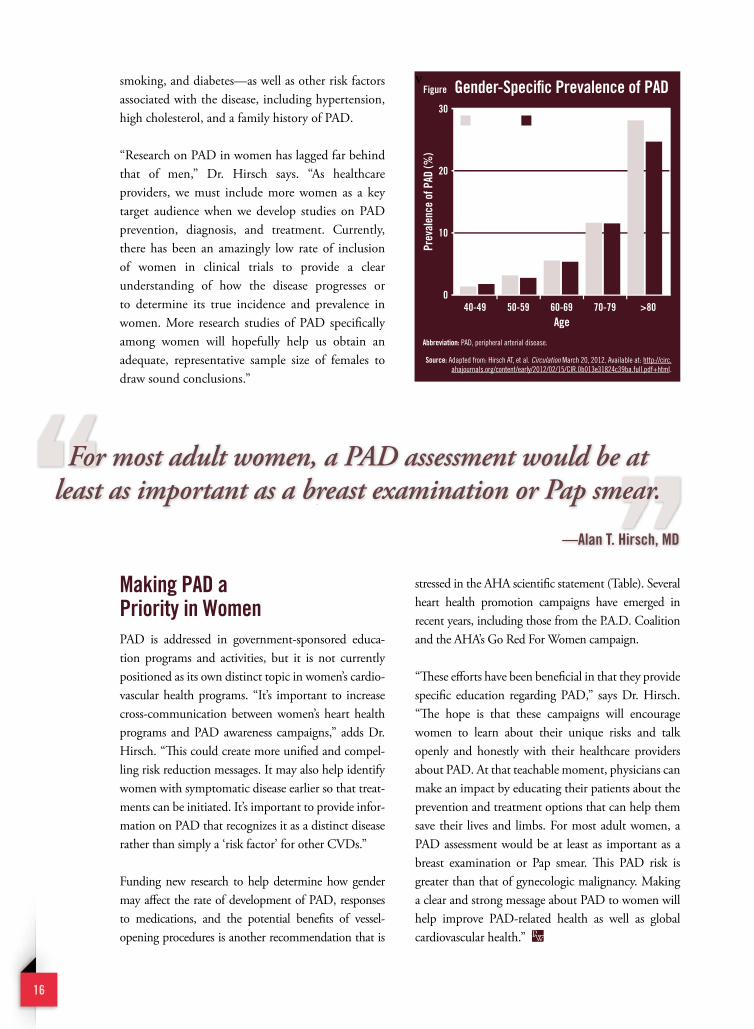
and stroke risks, severely limits walking ability, and causes tissue death requiring limb amputation. The prevalence of pad is nearly equal between men and women (Figure). Only about 10% of individuals with pad experience classic, recognized exertional
claudication, and many people experience no symptoms at all. as a result, few individuals with pad receive prompt diagnosis or treatment. “The mortality rate and healthcare costs associated with pad are comparable to those of heart disease and stroke,” says alan t. Hirsch, Md. “Women, in particular, suffer an immense burden from pad, but current data suggest that most women remain unaware of their risk. pad continues to go largely unrecognized and untreated in women.”
an important Scientific Statement on PadIn the March 20, 2012 issue of Circulation, the american Heart association (aHa), in collaboration
Women suffer the consequences of peripheral arterial disease (PAD)at rates at least as high as those observed in men. A scientific statement encourages physicians to proactively increase awareness of and test women at risk for PAD.
alan T. Hirsch, MdProfessor of Medicine, Epidemiology, and
Community HealthDirector, Vascular Medicine Program
Lillehei Heart Institute University of Minnesota Medical School
Women & Pad a Call to action
visit www.physiciansweekly.com 15
with the Vascular disease Foundation and the p.a.d. Coalition, released a scientific statement on women and pad. It recommends that healthcare providers proactively increase awareness of and test women at risk for pad. It also calls for more women-focused research into the disease.
“There is a great need to identify women with pad and those who are at risk for it, especially african-american women, so that we can help lower cardiovascular ischemic event rates,” says dr. Hirsch, who was the chair of aHa writing group that developed the call-to-action statement. “This may also reduce the loss of independent functional capacity and ischemic amputation rates.” He notes that women in the united states visit physicians
for pad at a rate that is similar to that of men, confirming the large burden of the disease in women.
Pad awareness Continues to lagawareness of pad in women and men is strikingly low when compared with knowledge of other cardiovascular diseases (CVds) and other conditions. according to current data, women may be somewhat more aware of pad and its risk than their male counterparts. That said, improving or eliminating knowledge gaps would provide a major opportunity to enhance the health of women significantly. Greater efforts are needed to increase awareness of the major risk factors of pad—including age over 50,
Women & Pad a Call to action
16
smoking, and diabetes—as well as other risk factors associated with the disease, including hypertension, high cholesterol, and a family history of pad.
“Research on pad in women has lagged far behind that of men,” dr. Hirsch says. “as healthcare providers, we must include more women as a key target audience when we develop studies on pad prevention, diagnosis, and treatment. Currently, there has been an amazingly low rate of inclusion of women in clinical trials to provide a clear understanding of how the disease progresses or to determine its true incidence and prevalence in women. More research studies of pad specifically among women will hopefully help us obtain an adequate, representative sample size of females to draw sound conclusions.”
Making Pad a Priority in Womenpad is addressed in government-sponsored educa-tion programs and activities, but it is not currently positioned as its own distinct topic in women’s cardio-vascular health programs. “It’s important to increase cross-communication between women’s heart health programs and pad awareness campaigns,” adds dr. Hirsch. “This could create more unified and compel-ling risk reduction messages. It may also help identify women with symptomatic disease earlier so that treat-ments can be initiated. It’s important to provide infor-mation on pad that recognizes it as a distinct disease rather than simply a ‘risk factor’ for other CVds.”
Funding new research to help determine how gender may affect the rate of development of pad, responses to medications, and the potential benefits of vessel-opening procedures is another recommendation that is
stressed in the aHa scientific statement (table). several heart health promotion campaigns have emerged in recent years, including those from the p.a.d. Coalition and the aHa’s Go Red For Women campaign.
“These efforts have been beneficial in that they provide specific education regarding pad,” says dr. Hirsch. “The hope is that these campaigns will encourage women to learn about their unique risks and talk openly and honestly with their healthcare providers about pad. at that teachable moment, physicians can make an impact by educating their patients about the prevention and treatment options that can help them save their lives and limbs. For most adult women, a pad assessment would be at least as important as a breast examination or pap smear. This pad risk is greater than that of gynecologic malignancy. Making a clear and strong message about pad to women will help improve pad-related health as well as global cardiovascular health.”
vFigure gender-Specific Prevalence of Pad
abbreviation: PAD, peripheral arterial disease.
Source: Adapted from: Hirsch AT, et al. Circulation March 20, 2012. Available at: http://circ.ahajournals.org/content/early/2012/02/15/CIR.0b013e31824c39ba.full.pdf+html.
Prev
alen
ce o
f Pad
(%)
age40-49 50-59 60-69 70-79 >80
Men Women30
20
10
01.3 1.7
3.1 2.75.5 5.3
11.8 11.5
28.4
24.7
For most adult women, a PAD assessment would be at least as important as a breast examination or Pap smear.
—alan T. Hirsch, Md
visit www.physiciansweekly.com 17
readings & resources
Hirsch aT, allison Ma, gomes aS, et al. A call to action: women and peripheral artery disease: a scientific statement from the American Heart Association. Circulation 2012;125:1449-1472. Available at: http://circ.ahajournals.org/content/early/2012/02/15/CIR.0b013e31824c39ba.full.pdf+html.
Hirsch aT, Murphy TP, lovell MB, et al; Peripheral Arterial Disease Coalition. Gaps in public knowledge of peripheral arterial disease: the first national PAD public awareness survey. Circulation. 2007;116:2086-2094.
rooke TW, Hirsch aT, Misra S, et al. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:2020-2045.
Higgins JP, Higgins Ja. Epidemiology of peripheral arterial disease in women. J Epidemiol. 2003;13:1-14.
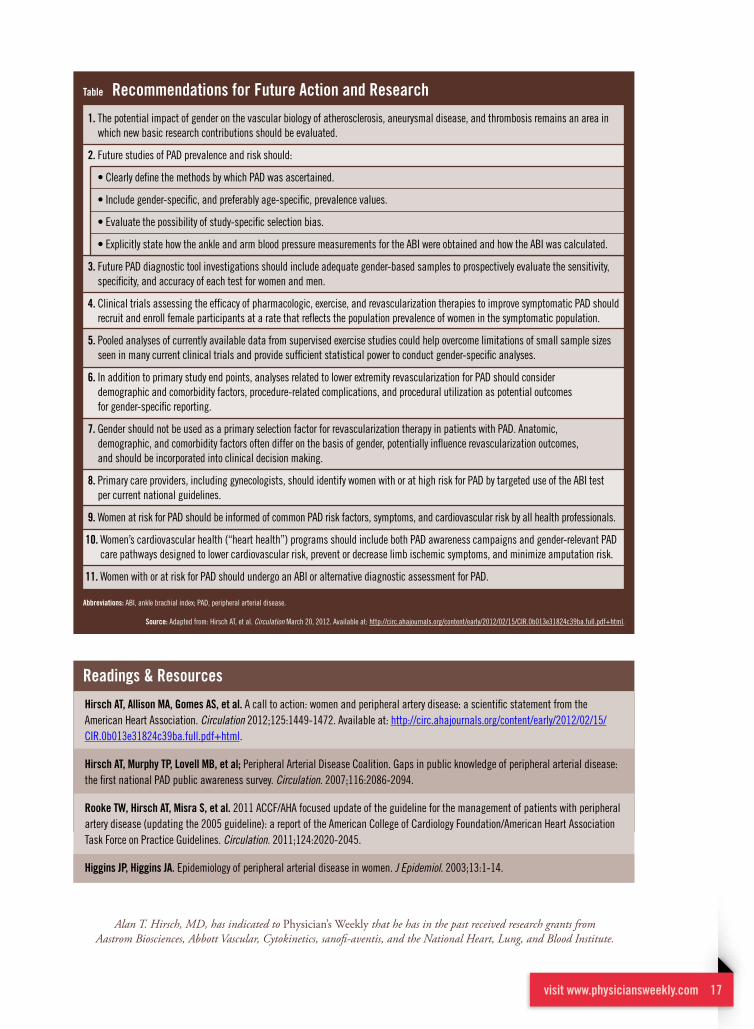
Table recommendations for Future action and research
1. The potential impact of gender on the vascular biology of atherosclerosis, aneurysmal disease, and thrombosis remains an area in which new basic research contributions should be evaluated.
2. Future studies of PAD prevalence and risk should:
• Clearly define the methods by which PAD was ascertained.
• Include gender-specific, and preferably age-specific, prevalence values.
• Evaluate the possibility of study-specific selection bias.
• Explicitly state how the ankle and arm blood pressure measurements for the ABI were obtained and how the ABI was calculated.
3. Future PAD diagnostic tool investigations should include adequate gender-based samples to prospectively evaluate the sensitivity, specificity, and accuracy of each test for women and men.
4. Clinical trials assessing the efficacy of pharmacologic, exercise, and revascularization therapies to improve symptomatic PAD should recruit and enroll female participants at a rate that reflects the population prevalence of women in the symptomatic population.
5. Pooled analyses of currently available data from supervised exercise studies could help overcome limitations of small sample sizes seen in many current clinical trials and provide sufficient statistical power to conduct gender-specific analyses.
6. In addition to primary study end points, analyses related to lower extremity revascularization for PAD should consider demographic and comorbidity factors, procedure-related complications, and procedural utilization as potential outcomes for gender-specific reporting.
7. Gender should not be used as a primary selection factor for revascularization therapy in patients with PAD. Anatomic, demographic, and comorbidity factors often differ on the basis of gender, potentially influence revascularization outcomes, and should be incorporated into clinical decision making.
8. Primary care providers, including gynecologists, should identify women with or at high risk for PAD by targeted use of the ABI test per current national guidelines.
9. Women at risk for PAD should be informed of common PAD risk factors, symptoms, and cardiovascular risk by all health professionals.
10. Women’s cardiovascular health (“heart health”) programs should include both PAD awareness campaigns and gender-relevant PAD care pathways designed to lower cardiovascular risk, prevent or decrease limb ischemic symptoms, and minimize amputation risk.
11. Women with or at risk for PAD should undergo an ABI or alternative diagnostic assessment for PAD.
abbreviations: ABI, ankle brachial index; PAD, peripheral arterial disease.
Source: Adapted from: Hirsch AT, et al. Circulation March 20, 2012. Available at: http://circ.ahajournals.org/content/early/2012/02/15/CIR.0b013e31824c39ba.full.pdf+html.
Alan T. Hirsch, MD, has indicated to physician’s Weekly that he has in the past received research grants from Aastrom Biosciences, Abbott Vascular, Cytokinetics, sanofi-aventis, and the National Heart, Lung, and Blood Institute.
18
Blood Pressure & End-Stage renal disease in Patients With CKdNew data suggest that blood pressure targets in patients with chronic kidney disease, or CKD, may need to be adjusted to avoid progression to end-stage renal disease.
18

visit www.physiciansweekly.com 19
Carmen a. Peralta, Md, MaSAssistant Professor of Medicine
University of California, San Francisco School of Medicine
Attending Physician San Francisco VA Medical Center
visit www.physiciansweekly.com 19
S tudies have shown that treating high blood pressure (Bp) is one of the most important strategies to slowing the progression from
chronic kidney disease (CKd) to end-stage renal disease (esRd). Currently, a Bp goal of less than 130/80 mm Hg is recommended for patients with CKd, a target that is lower than the goal that is recommended for people without CKd (less than 140/90 mm Hg). despite the dissemination of clinical guidelines, meeting Bp targets in people with CKd may be difficult in clinical practice.
“The most recent evidence supporting the use of lower Bp targets in people with CKd has been
conflicting,” explains Carmen a. peralta, Md, Mas. “The
association of Bp levels and esRd risk in a large,
national, community-based setting of persons with established CKd has not been well studied. In addi-tion, some recent reports have found that higher pulse pressure and lower diastolic Bp (dBp) may lead to adverse cardiovascular outcomes. This can make it especially challenging for clinicians to control Bp aggressively in patients with CKd.”
analyzing important associationsFew studies have investigated the association of each Bp component with esRd risk. In the January 9, 2012 Archives of Internal Medicine, dr. peralta and colleagues had a study published that investigated the independent association of systolic Bp (sBp) and dBp with esRd risk in patients with CKd who participated in the Kidney early evaluation program (Keep), a nationwide kidney health screening program offered by the National Kidney Foundation. More than 16,000 patients in Keep were studied in the analysis, and all participants had at least stage III CKd.
“In the past, questions have been raised about the established Bp targets for preventing

20
esRd because they’ve been studied mostly in randomized control trials, where participants tend to be healthier than the general population,” says dr. peralta. “The Keep cohort gave us the opportu-nity to look at a community-based sample of regular americans who have CKd.”
The results confirm that higher Bp levels are associ-ated with higher risk to develop esRd. Most strik-ingly—despite dissemination of guidelines—the study found that more than one-third of patients with CKd had Bps of 150/90 mm Hg or higher, mostly due to isolated high sBp (table 1). “The prev-alence of uncontrolled hypertension was very high among people with CKd,” dr. peralta adds. “This was largely explained by isolated systolic hyperten-sion.” Higher sBp was associated with higher esRd
risk, and this risk appeared to start at 140 mm Hg rather than at 130 mm Hg (the current target sBp for CKd). Furthermore, higher pulse pressure was associated with higher esRd risk. people with sBps of 150 mm Hg or higher and dBps of less than 90 mm Hg were more likely to be older, non-Hispanic black and have diabetes and albuminuria (table 2).
important implicationsa better understanding of the association of Bp and esRd risk among people with CKd might help physicians provide better care for their patients with CKd, says dr. peralta. “The issue is daunting when more than one-third of persons with CKd are walking around with Bps higher than 150 mm Hg. Our study suggests that trying to get Bp to less than 140 mm Hg may be beneficial in reducing esRd risk.”
More attainable BP goals may ease some of the challenges faced by physicians.
—Carmen a. Peralta, Md, MaS
Table 1 BP Components & incident ESrdIncreases in systolic blood pressure (BP) were associated with a hazard ratio (HR) for end-stage renal disease (ESRD) of 1.66 in age- and sex-adjusted models and an HR of 1.23 after full adjustment. Below is a breakdown of the associations between systolic and diastolic BPs and HRs for ESRD:
*Adjusted for age, sex, race/ethnicity, insurance, access to a physician, current smoking, diabetes mellitus, body-mass index, baseline estimated glomerular filtration rate, albumin-uria, and prevalent cardiovascular disease.
Source: Adapted from: Peralta CA, et al. Arch Intern Med 2012;172:41-47.
Systolic BP
<130 mm Hg 1.00 [Reference] 1.00 [Reference]
130-139 mm Hg 1.08 0.71
140-149 mm Hg 1.72 1.27
≥150 mm Hg 3.36 1.36
diastolic BP
<60 mm Hg 1.40 1.12
60-74 mm Hg 1.00 [Reference] 1.00 [Reference]
75-89 mm Hg 0.90 0.91
≥90 mm Hg 1.67 1.81
BP Hr adjusted Hazard*

visit www.physiciansweekly.com 21
Randomized trials have shown that lower goals (less than 130/80 mm Hg) reduce esRd risk for patients with proteinuria, notes dr. peralta. “However, this lower goal can be especially hard for patients to achieve in clinical practice. Clinicians should focus more on patients with the highest and most uncon-trolled Bps rather than be compelled to reach a goal of 130/80 mm Hg in everyone with CKd. More attainable Bp goals may ease some of the challenges faced by physicians.” Bp goal revisions might also enable physicians to prescribe fewer Bp medications and focus more on other aspects of care. Greater efforts on patient education regarding Bp control may also be of benefit.
More research Warrantededucational strategies on Bp control should focus on lowering sBp. More research is necessary to identify agents that lower arterial stiffness, dr. peralta says. “Our study had relatively few people with high degrees of proteinuria, and these individuals may benefit from even lower targets. Ideally, we should be working toward increasing our knowledge and understanding of the long-term associations of Bp and esRd risk as well as associations between Bp components and risk for mortality or cardiovascular events. as these data emerge in subsequent studies, it’s hoped that we’ll get a better picture of how we can optimize the manage-ment of Bp in patients with CKd.”
Carmen A. Peralta, MD, MAS, has indicated to physician’s Weekly that she has no financial interests to report.
readings & resources
Peralta Ca, Norris KC, li S, et al. BP components and end-stage renal disease in persons with chronic kidney disease. The kidney early evaluation program (KEEP). Arch Intern Med 2012;172:41-47. Available at: http://archinte.ama-assn.org/cgi/reprint/172/1/41 .
agarwal r. Blood pressure components and the risk for end-stage renal disease and death in chronic kidney disease. Clin J Am Soc Nephrol. 2009;4:830-837.
Peralta Ca, Hicks lS, Chertow gM, et al. Control of hypertension in adults with chronic kidney disease in the United States. Hypertension. 2005;45:1119-1124.
Peralta Ca, Shlipak Mg, Wassel-Fyr Cl, et al. Association of antihypertensive therapy and diastolic hypotension in chronic kidney disease. Hypertension. 2007;50:474-480.
Hsu Cy, iribarren C, McCulloch CE, darbinian J, go aS. Risk factors for end-stage renal disease: 25-year follow-up. Arch Intern Med. 2009;169:342-350.
Table 2 Characteristics linked With isolated Systolic Hypertension in CKd*
* Systolic blood pressure 150 mm Hg or higher and diastolic blood pressure lower than 90 mm Hg.
abbreviations: ACR, albumin-to-creatinine ratio; CKD, chronic kidney disease.
Source: Adapted from: Peralta CA, et al. Arch Intern Med 2012;172:41-47.
Characteristic odds ratio
age
<60 years 1.00 [Reference]
60-75 years 2.24
>75 years 3.69
Sex
Male 0.81
race/ethnicity
White 1.00 [Reference]
African-American 1.13
Asian 0.76
Hispanic 1.12
Other 0.87
Diabetes 1.31
ACR >30 mg/g 1.72
insurance status
Both private and public 1.00 [Reference]
Private only 0.74
Public only 0.97
Neither 0.92
Saw physician in last 2 years 1.07

don’t Miss another issue
Visit www.physweekly.com/register
Sign Up for our eNewsletterToday